
Abstract
The complex problem of clinician distress, a prevalent condition found across the spectrum of health professionals, has deleterious effects on quality of healthcare. Multiple factors contribute to this growing problem, including the increasingly complex nature of the management and organization of medical care delivery. This chapter describes Mindful Practice, an empirically studied educational program designed to enhance well-being, quality of care, and flourishing of physicians. A skills-based training program, Mindful Practice uses the technologies of one’s innate capacity for awareness, faculty to reflect on clinical experiences as narratives, and ability to learn one’s own capacities and strengths in the midst of the challenging dynamics experienced in the practice of medicine. Thus, the contemplative practices, narrative medicine, and appreciative inquiry that are woven into this educational experience energizes physicians and other health professionals through real-life relevance, an increased sense of meaning, and a growing capacity for health professionals to connect meaningfully across the divides that exist between individual clinicians and the organizations of health system delivery. Ultimately, clinician distress calls for an ethical mandate that requires courage and commitment, and eventual transformation, personally and collectively.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Looking back on my experience as a clinician, teacher, mentor, researcher, and family caregiver what stands out vividly are my memories of presence. By this I mean the intensity of interacting with another human being that animates being there for, and with, that person. Presence is a calling forward or a stepping toward the other. It is active. It is looking into someone’s eyes, placing your hand in solidarity on their arm, speaking to them directly and with authentic feeling. Presence is built out of listening intensely, indicating that the person and their story matter, and explaining carefully so that you are understood. (Kleinman, 2017)
Good patient care is found not in a computer screen but in being truly present with patients. (Verghese, 2016)
1 Mindful Practice: An Overview
Mindful Practice, a mindfulness-based program developed by a team of physicians at the University of Rochester School of Medicine and Dentistry (Rochester, New York, USA) was designed to enhance clinical health professionals’ resilience and well-being, improve the clinician-patient relationship, and advance the quality of medical care they provide. This educational intervention, built on a strong biopsychosocial foundation, contains three major components—mindfulness meditation, narrative medicine, and appreciative inquiry. These components are integrated in a series of theme-based modules to address key challenges facing clinicians and educators in a seamless experiential, interactive, and relational pedagogy (Epstein, 2014; Krasner, 2016; Krasner et al., 2009).
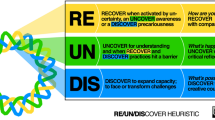
Mindful Practice as described by Epstein in 1999 refers to qualities of exemplary clinicians that transcend clinical specialty and clinical experience (Epstein, 1999): moment-to-moment purposeful attentiveness to one’s own physical and mental processes during every day work with the goal of practicing with clarity and compassion. These same qualities, first identified as promotion of individual flourishing, also apply to qualities of organizations and leadership and can guide organizational change within the culture of medicine. Clinician distress, which contributes to burnout and lower quality of care (Shanafelt, 2003), is related to both individual and health systems factors (Montgomery, 2014), and thus, steps needed to promote clinician well-being must address individual vulnerability, as well as organizational structure, function, leadership and culture (Shanafelt et al., 2019). Applying the qualities that Mindful Practice focuses on within the culture of medicine at both the individual and organizational levels may be a useful approach for promoting positive change, a healthier working and learning environment, and improved quality of care (see Fig. 15.1).
The qualities central to Mindful Practice-attentive observation, critical curiosity, beginner’s mind, and presence-not only inform the moment by moment lived experience of clinicians, but also that of the relationships among individuals and groups within the organization (Epstein, 2017). Those relationships occur at the intrapersonal, interpersonal, team, departmental and institutional levels, and include the sociopolitical environment that affects and is affected by the health care system, as well as the nested interactions among these levels within organizations. Mindfulness in organizations, thus, refers to the capacity of the members and of the organization themselves to have awareness of intrapersonal, interpersonal and environmental dynamics. Mindfulness, furthermore, enhances a universal capacity for clear thinking and open-heartedness through embodied awareness, contributing to a greater sense of emotional balance and well-being. Health professionals, leaders and educators world-wide have resonated with the goals, objectives and methods used in the Mindful Practice program; over the last decade more than a thousand of such individuals have participated in 2, 3 and 4-day Mindful Practice programs that have been held on every continent.
2 Challenges Facing Clinicians
The context and the practice of medicine just seems to be accelerating, and the number of things competing for our attention is just incredible…David Hatem MD, Professor of Medicine, University of Massachusetts School of MedicineFootnote 1
The hustle and bustle of residency training, it’s quite a fast pace, it’s very grueling…Chiezetam Ekekeze MD, Chief Resident, Internal Medicine Residency Program, Brown University
It is a relentless exposure to suffering…Frederick Marshall MD, Professor of Neurology, University of Rochester School of Medicine and Dentistry
No matter what happens to you or your patients, or anything like that, that you’re not allowed to, sort of, even have an emotion, let alone express it…Andrew Czuchwicki MD, Anesthesiologist, Queens Hospital, Adelaide, Australia
Recent epidemiologic studies suggest that clinician distress is common, that it is related to individual, micro-environmental and institutional issues, and that it is a precursor to the high levels of burnout reported among physicians, nurses and other health professionals. The first published reports describing burnout in the United States appeared in the mid-1970s (Freudenberger, 1975; Maslach, 1976). Since then, burnout has been defined as a work-related syndrome involving emotional exhaustion, depersonalization/cynicism, and a low sense of personal accomplishment, and epidemiologic studies suggest that burnout affects over half of physicians in training and practicing physicians, and over a third of nurses (McHugh, Kutney-Lee, Cimiotti, & Sloane, 2011; West, Dyrbye, & Shanafelt, 2018). The medical specialties most at risk for burnout are those on the “front lines” such as family medicine, general internal medicine, and emergency medicine (Shanafelt et al., 2012).
Affecting 25–55% of physicians worldwide, burnout has been linked to poorer quality of care, patient dissatisfaction, increased medical errors and lawsuits, and decreased empathic capacity (Shanafelt, 2003; Shanafelt et al., 2012). The consequences of burnout among practicing physicians include not only poorer quality of care but also poorer quality of life, accidents, and suicide, as well as leaving clinical practice (Sinsky et al., 2017; Williams et al., 2001). There is concern that early retirement due to burnout will have a significant effect on patient access to health care services (AAMC, 2018; Bodenheimer, 2006; Treadway, 2008).
The factors contributing to physician burnout are complex and numerous. Throughout history, practitioners have often felt that their clinical tools were inadequate to address patients’ health problems. Currently, though, structural and organizational factors within the healthcare environment threaten health professionals’ identity, well-being and perceived effectiveness to a far greater degree (Zuger, 2004). These include the cumbersome information technology demands, burdensome administrative and documentation requirements, a pervasive sense of loss of control and meaning, and a lack of alignment of individual and organizational values (Dunn, Arnetz, Christensen, & Homer, 2007; Shanafelt & Noseworthy, 2017; Sinsky et al., 2016).
The problem of physician burnout seems an expected side-effect of contemporary medical practice. The pace, complexity, and ongoing challenges of the chronic and multiple medical conditions that physicians care for in which management requires not only a biomedical focus but increasingly psychological and socioeconomic considerations contribute significantly to the risks for burnout. Medical science has successfully addressed many of the public-health related diseases that once threatened one’s survival or the survival of one’s family. Now, stress-related maladies increasingly challenge modern medicine, which by their nature add complexity to diagnosis and treatment. Individuals and organizations of healthcare simultaneously struggle with these complexities as they attempt to address them for patients, for the public at large, and for the health of those working within the health care delivery system.
3 What Is Mindful Practice?
Mindful Practice® is an educational program designed for physicians and other health professionals that engages the physical, emotional and cognitive aspects of clinical experience through cultivating intrapersonal and interpersonal awareness. It supports collegial relationships and helps health professionals reflect on and learn from the most challenging clinical experiences in a manner that recognizes their intrinsic strengths and capacities for efficacy and quality in their work. It offers tangible skills that can be used at every level not only to build individual resilience but to change the health care system through awareness-building, from leadership down to the rank-and-file.
Mindful practice depends on developing a capacity for mindfulness. Mindfulness involves the awareness of the present moment that includes awareness of one’s inner life (sensations, emotions, thoughts, feelings) as well as sensations and stimuli from the outside world. Mindfulness might incorporate experiences from the past and anticipating the future, but, importantly, the awareness of all of these experiences is grounded in the present moment—it can be described as being experienced in the unfolding now. Mindfulness is a human capacity that fosters clear thinking and receptivity and responsiveness to others’ distress. Its historical role, that of relieving suffering and cultivating compassion, makes it a quality essential to medical care (Ludwig & Kabat-Zinn, 2008). We believe that mindfulness is a naturally occurring human capacity which can be cultivated in a variety of ways. Over the past 30 years, mindfulness has been closely associated with meditation practices and empirically validated and widely disseminated “mindfulness-based” interventions such as mindfulness-based stress reduction (MBSR) or mindfulness-based cognitive therapy (MBCT). We believe that there are many ways to cultivate mindfulness, including practices that can be incorporated into the workplace.
The Mindful Practice program at the University of Rochester School of Medicine and Dentistry was designed in 2005–2007 as a mindfulness-based intervention for medical students, physician trainees, practicing physicians and other clinicians to address burnout and build resilience through a contemplative, self-care-oriented approach. In addition to its effects on personal well-being, observational data suggest that clinician mindfulness is associated with greater patient safety and error reduction (Dierynck, Leroy, Savage, & Choi, 2017; Ludwig & Kabat-Zinn, 2008; Crosskerry, 2003; Sibinga & Wu, 2010; Vogus & Sutcliffe, 2007a, 2007b), as well as patients’ assessments of physicians’ communication skills and satisfaction with care (Beach et al., 2013). In addition, mindfulness is one quality that can help raise awareness of cognitive biases, such as avoiding or mitigating diagnostic and medical decision-making problems engendered by premature closure, and availability and anchoring biases (Crosskerry, 2003). Ron Epstein, who along with Mick Krasner designed the Mindful Practice program at the University of Rochester, outlined several core qualities of effective clinicians in his seminal 1999 JAMA article Mindful Practice (Epstein, 1999). For heuristic reasons, we have distilled the qualities of mindful practice to four attributes, or habits of mind: attentive observation, critical curiosity, beginner’s mind, and presence. We chose these qualities because they are intuitively simple to understand, have relevance to medical practice, and are qualities thought to be teachable. For example, the concept of beginner’s mind has to do with setting aside preconceptions and cultivating an openness to surprise; these qualities have been suggested as helpful in avoiding diagnostic bias and premature closure (Crosskerry, 2003). The Mindful Practice program endeavors to assist clinicians in cultivating these qualities, applying them to their practice of medicine, whether in the clinic, the operating room, or the board room, and has relevance for public health and leadership within health care organizations.

Schematic of Mindful Practice as an intervention that connects together clinician well-being, quality of care, and quality of caring
Three components that make up the core experience of Mindful Practice are:
-
Formal and Informal Mindfulness Practices: Cultivation of an open, receptive, and non-judgmental orientation to one’s present experience, which helps promote physical, emotional and cognitive stability. The formal practices—such as meditation—and what are called informal practices—such as strategically employing the breath or body awareness during the work day—are central to the skills used when building the qualities of attention, curiosity, openness, and presence.
-
Narratives from the Practice of Medicine: Our approach to using narratives is informed by Rita Charon’s transformative work on how the use of personal stories can enrich and humanize health care (Charon, 2001). In addition, we incorporate into narrative exercises some of the skills developed in formal and informal mindfulness practices. In these exercises, participants reflect on and share personal stories about significant challenges in clinical practice and in clinicians’ professional development (e.g., meaningful experiences, errors, grief and loss, conflict, resilience and compassion). Particularly important is cultivation of a quality of deep listening that emphasizes curiosity and inquiry into the storyteller’s experience, while avoiding providing advice, making judgments and comparing one’s own stories to those of the speaker. Equally important is the cultivation of self-reflection and interpersonal awareness for the speaker while sharing their story. Thus, these narrative exchanges have a contemplative quality that deepens both the storyteller’s self-awareness as well as the listener’s understanding of the storyteller’s experience. These experiences often help connect the clinicians with sources of professional satisfaction, meaning and personal capacities for managing the challenges of medical practice. While in the training workshops, participants practice sharing narratives in structured settings with the goal for participants to bring the same skills of self-awareness and deep listening to encounters with patients, to teaching venues and to administrative roles.
-
Appreciative Dialogues: Based on Appreciative Inquiry (Cooperider, 2005), a strength-based approach to individual and organizational change that alters habitual patterns of thinking and behavior, appreciative dialogues are designed to help participants discover capacities and resources within themselves for positive potential. The dialogues are structured so as to incorporate an intentional focus on recognizing strengths of the clinician within the challenging experiences through the very act of discussing with a colleague. Participants are encouraged to bring the same skills of eliciting, naming and promoting individual strengths and capabilities to their work with patients, students and colleagues to complement the more common problem-oriented approaches in medical settings, to foster effective teamwork, and to increase patient motivation and self-reliance.
The Mindful Practice curriculum, taught in a modular fashion, presents themes of professional relevance and challenge as the ground upon which participants bring mindful attention and awareness as they reflect upon and then share clinical experiences that connect with the theme. Among the themes include the following (Epstein & Krasner, 2017):
-
Noticing—improving clinicians’ capacity for attentive observation, and increased awareness of blind spots and implicit biases.
-
Responding to suffering—exploring how clinicians notice and respond to suffering in patients and themselves
-
Compassion—the role of empathy and actions to relieve suffering, including the patient-clinician relationship
-
When things go wrong—building awareness and resourcefulness when confronted with errors and bad outcomes
-
Grief and loss—investigation of how clinicians’ awareness of and responses to the inevitable experience of grief and loss in patient care, as well as their own attitudes toward their own illnesses and mortality can enrich their work
-
Resilience—building skills, relationships and community resources to help clinicians flourish—being more effective in their work with patients and colleagues while also living a more balanced sustainable work life.
-
Uncertainty—an examination of how clinical work can be enriched by adopting an improvisational stance when confronted with challenging situations
-
Professionalism—consideration of training knowledge, skills, virtue, character, ethics and behavior in the culture of medicine
The acquisition of medical knowledge, assimilation of clinical information, and continued honing of manual skills are vital to professional competence. Likewise, the continual honing of interpersonal skills, steady development of increased intrapersonal and interpersonal awareness, and capacity to attend to patients with presence are also central tasks toward the goal of practicing high quality, relationship-centered medical care. A central objective of Mindful Practice has been the integration of these skills into the practitioner’s clinical understanding and individual expression in much the same way that the understanding of organ systems and their physiology and pathology become integrated into an approach to solving problems in a clinical encounter.
Becoming Mindful: Getting Started in the Workplace
-
1.
Take a moment to orient yourself to your workday as you arrive at work. Use the walk from arrival to the office from the parking lot bus or train to step into your life. Acknowledge where you are, where you are going, and inquire about your intention for the day
-
2.
While sitting at your desk periodically pay attention to bodily sensations, noticing the state of tension or relaxation.
-
3.
Bring awareness to transitions—from the office to the patient encounter, from the patient encounter to clinical workspaces, from the hallway into the exam room. Take a moment for a conscious breath when crossing the threshold into an exam room.
-
4.
Close your door for 5 min at lunch, set your cell phone down, turn off the screen of the computer, and simply bring awareness to the moment
-
5.
Practice STOP: Stop, Take a breath, Observe, and Proceed as often as you can during the workday
-
6.
Download and use cell phone apps like Headspace and Insight Timer to support contemplative practice
-
7.
Consider further training such as those available through Mindful Practice (www.mindfulpratice.urmc.edu)
Mindful practice training for individuals and teams of health care providers (nurses, physicians, advanced practice providers, support staff) does not require large cultural or philosophical changes. Yet, developing habits of the informal and formal contemplative practices, sharing experiences using narratives, deep listening, awareness of one’s own actions, biases and emotions all require practice and reinforcement. We believe that small adjustments in practice style through the incremental introduction of simple practices can lead to positive shifts in the lived experience of those delivering health care; when groups of colleagues share common experiences of practicing mindfully, it can change organizational culture and promote (and be promoted by) a collective vision that features the importance of self-awareness and self-care among all the stakeholders who are engaged in health care enterprise. Here, leadership, educational interventions and opportunities for reinforcement are key.
4 What Are the Effects of Mindful Practice?
The Mindful Practice program in its original form involved recruiting 70 primary care physicians to participate in a year-long study involving 8 weekly sessions with an all-day retreat after week 6, and 10 monthly sessions (Krasner & Epstein, 2010; Krasner et al., 2009). With grant support from the Physicians Foundation for Health System Excellence, we designed a program of individual modules, each of which addressed key aspects and challenges of professional life. Participants completed questionnaires at baseline, at the beginning of the program, at 8 weeks, at the end of the program, and at 3 months after completing the program. In general, participants were moderately burned out at baseline and showed significant and enduring improvements in physician well-being (lower burnout and mood disturbance), attentiveness (increased mindfulness), and attitudes toward clinical care (increased empathy, psychosocial orientation and interest in patients as people) (Krasner et al., 2009). We also noted that these changes were all mediated by changes in mindfulness, and, furthermore, noted personality changes—participants were more conscientious and experienced greater emotional stability, an unexpected finding in mid-career physicians (average age 46). This intervention has been repeated among primary care providers in Spain with similar results demonstrated on burnout, empathy, mood and mindfulness (Asuero, 2012).
A follow-up investigation of the participants in Rochester, designed to determine what aspects of this educational intervention contributed to participants’ well-being and the care they provided, incorporated structured interviews and standard qualitative thematic analytic methods (Beckman et al., 2012). Participants reported three main themes: (1) the importance of a professional community: sharing personal experiences from medical practice with colleagues reduced professional isolation; (2) the importance of trainable skills: mindfulness skills improved the participants’ ability to be attentive and listen deeply to patients’ concerns, respond to patients more effectively, and to have sufficient resources to adapt to stressful circumstances; and (3) the importance of physician self-care: while participants valued developing greater self-awareness and found it positive and transformative, they still had difficulty granting themselves permission to attend to their own personal growth.
Although the first two themes seem to have face-validity for this kind of intervention, this final theme was more unexpected. We attribute physicians’ difficulty recognizing their vulnerability and need for self-care in the service of being more available to patients as reflecting the values of commitment to service, clinical excellence and altruism within the culture of medicine. These values when carried to a more extreme can lead to over-commitment, self-deprivation and perfectionism and can undermine physicians’ well-being and clinical effectiveness. Since the publication of these findings, and as the link between health professional well-being and quality of care becomes stronger through empirical evidence (Dewa, Loong, Bonato, & Trojanowski, 2016; Linzer, 2018; Panagioti et al., 2018), there are now mandates from licensing bodies that undergraduate and graduate medical education address self-care and well-being of students and residents, and many health care organizations have developed wellness programs for practicing clinicians. With time, we are hopeful that organized medicine will address clinician burnout more systematically and make it more culturally normative for physicians and other health professionals to engage in activities that promote self-awareness and mindfulness.
Since its development, the Mindful Practice curriculum has been adapted to provide training experiences for health professionals in many different settings. The most prominent of these trainings involve 4 and 5-day intensive retreat-like experiences facilitated by the original developers along with additional clinician faculty who are experienced in mindfulness, narrative and appreciative interview practices and dedicated to promoting professional flourishing in healthcare. Advanced teacher training and internship opportunities have allowed Mindful Practice to reach physicians and other healthcare professionals in North and South America, Asia, Europe, Africa, the Middle East, and Australia. Participants include clinicians from all clinical specialties (and a few veterinarians), as well as those in healthcare administration, hospital executive suites, medical and nursing school deans’ offices, malpractice insurance carriers, public health agencies, and government regulatory bodies.
5 Courageous Conversations and Conclusions
It does create this camaraderie and friendship and community which is so supportive and sustaining…Andrew Czuchwicki MD, Anesthesiologist, Queens Hospital, Adelaide, Australia
There’s a lot of power in telling your own story, and that’s so much of what we’ve been doing here at this retreat is strangers sharing their own stories, and then something magical happening where you feel like you’re no longer strangers… ChiezetamEkekeze MD, Chief Resident, Internal Medicine Residency Program, Brown University
It allows me, I think, to embrace more of this human kind of vulnerability in a way that feels very courageous, so I see it now as more of a strength, as opposed to something that I kind of need to protect myself from…I think that enables me to actually engage in a different way, a way that’s actually a little clearer, and I think really through Mindful Practice that’s actually helped me to be a better physician… Joanna McDermid MD, Consulting psychiatrist, BC Children’s Hospital, Vancouver, BC Canada
Mindful Practice has been well-received among participants from a wide-variety of medical specialties who have attended the training programs, as well as among participants in specific health-care teams who have invited Mindful Practice training within their organizations such as surgical teams. Leaders in health care are increasingly aware of the high costs due to attrition, early retirement and medical errors associated with burnout among health professionals in their organizations. By comparison, the cost of a mindfulness program or other programs to try to mitigate burnout is incredibly inexpensive. In 2017, Shanafelt et al clearly described a business case for interventions to reduce burnout (Shanafelt, Goh, and Sinsky, 2017).
Mindful Practice training cultivates qualities that most clinicians and educators recognize as qualities of excellent practitioners—attentiveness, self-monitoring, curiosity, beginner’s mind, commitment, resilience, presence, empathy, acceptance and awareness of one’s biases. However, while attention to these qualities has grown over the past 30 years, still, it is generally an afterthought in the formal education of health professionals. Mindfulness training, in whatever form, does present challenges. It requires exercising parts of oneself that have not been exercised for a long time. It involves awareness of—and questioning about—personal attitudes, values and blind spots that can be uncomfortable. When clinicians are very busy, distressed and burned out, the challenges of developing self-awareness can seem daunting; narrowly focused clinicians may find themselves unable to discern that self-care may be one of the best uses of their limited time and energies. Furthermore, health care teams, not just individuals, may benefit from the implementation of mindfulness training; yet team-based mindfulness training has not been rigorously studied. Recently, the popularity of mindfulness in the media has fostered preconceptions and distortions among the general public that mindfulness merely is an escape, a form of relaxation, only for the well-heeled and new age, or a luxury that they can ill-afford while they are struggling just to keep up. Here, education is essential. Finally, institutional support is key. Reports from Fortune 500 companies that have developed mindfulness programs demonstrate that in organizations where being mindful has positive valence and seen as a virtue, and where programs are offered, people are more likely to be drawn to it (Tan, 2012). Health care organizations should emphasize that even the busiest physicians are guided by principles of service and compassion, and endeavor to bring skill and wisdom to their work; that finding themselves struggling in their work, questioning the value of their efforts, or searching for professional meaning can bring a wide range of health professionals to recognize and find ways to address their needs; and that the organization values and supports the efforts of their constituencies to adopt practices that help them to be more mindful.
At a symposium in 2014 at Johns Hopkins University, Dr. John Kabat-Zinn, the founder of the Mindfulness-Based Stress Reduction program, offered an updated definition of mindfulness that included a more explicit ethical intention: Mindfulness is the awareness that arises by paying attention, on purpose in the present moment, non-judgmentally, in the service of self-understanding, wisdom, and compassion (Kabat-Zinn, 2014). This clarification mirrors a growing recognition within the medical community for the need to be more explicit about the professional ethics that not only support the provision of quality health care, but also support the needs of the providers of that care.
This ethical mandate has deep implications for the structure and systems within the medical culture. It calls on everyone involved in the enterprise of providing scientifically rational, ethically sound and exquisitely empathic care to communicate together, turning toward the most difficult issues while holding close the ideas of self-understanding, wisdom and compassion (Epstein, 2017). Mindful Practice asks participants to do just that. At its core is the fierce honesty of being able to see things not as we desire, but as they truly are, and then to ask, together, as a community, what capacities do we already have that can help us negotiate these turbulent waters? Whether it is a patient suffering deep loss and grief, a colleague challenged by fatigue and error, an administrator attempting to manage resources wisely and fairly, or a leader seeing threats to institutional existence looming while envisioning a better, safer, kinder and more effective learning and working environment.
Courage is required to initiate and engage in conversations that help individuals and organizations examine the ethical underpinnings of their work and implement behaviors and programs that support those ethical underpinnings. Once those conversations are underway, individuals and organizations require skills: skills of attentively observing what is, skills of applying critical curiosity to how things appear and are, skills at reframing and re-visioning the current situations with a beginner’s mind, and skills of simply being present with acceptance and without judgment to the unfolding now, in the service of making the most skillful and effective decisions. This commitment to noticing, clear thinking, generosity and growth was the initial inspiration behind our work, and we believe that Mindful Practice offers a roadmap to move the conversations along a path of positive change.
Key Messages for Researchers
-
Physician well-being and quality of care are strongly connected.
-
Further research, qualitative and quantitative, is required to evaluate the impact of investing in physician and health professional well-being.
-
Mindfulness-Based Interventions vary in so many aspects. For them to be compared, a research agenda for assessing efficacy should include a number of standard individual, team and systemic measures.
-
The ethical dimensions within healthcare are of great interest but are challenging to assess. Research should include explorations of this aspect of physician and health professional well-being, institutional health, and the larger public health.
-
One objective of continued research on mindfulness interventions designed to improve professional well-being and quality of care should be the identification of best practices and how these can be tailored to local environments.
Key Messages for Healthcare Delivery
-
Physician and other health professional well-being should be considered a primary quality indicator within the healthcare system.
-
Healthcare teams should consider reflections on patient narratives, as shared by members of the team, as a way of supporting meaning and purpose at work.
-
Cultivating awareness of self, awareness of others, and awareness of relationship can assist health professionals to work effectively and flourish within the complex world of healthcare delivery.
-
Social connectivity among health professionals support quality of care delivery, and mitigate the effects of isolation.
-
Mindful Practice creates a growing and learning work environment that can translate into improvements in personal well-being, patient-centeredness, team function, and improved quality.
Notes
- 1.
All quotes not otherwise noted in references are from: Mead, J. September 30, 2019. Mindful Practice for Medical Clinicians. https://www.youtube.com/watch?v=MGliZssn-Ps&fbclid=IwAR3ns0U8bfdmjD5lt4MV1i10HEdINYLaD89XkJ3t06hUzUbXUexqKLhEgkQ
References
AAMC. (2018). 2018 update: The complexities of physician supply and demand: Projects from 2016-2030. Washington, DC: Association of American Medical Colleges.
Asuero, A. (2012). Effectiveness of an educational program on mindfulness to reduce burnout and improve empathy in primary care professionals. Barcelona, Spain: Universidad Autónoma de Barcelona.
Beach, M., Roter, D., Korthuis, P., Epstein, R., Sharp, V., Ratanawongsa, N., et al. (2013). A multicenter study of physician mindfulness and health care quality. Annals of Family Medicine, 11(5), 421–428.
Beckman, H., Wendland, M., Mooney, C., Krasner, M., Quill, T., Suchman, A., et al. (2012). The impact of a program in mindful communication on primary care physicians. Academic Medicine, 87(6), 815–819.
Bodenheimer, T. (2006). Primary care—Will it survive? New England Journal of Medicine, 355(9), 861–864.
Charon, R. (2001). Narrative medicine: form, function, and ethics. Annals of Internal Medicine, 134(1), 83–87.
Cooperider, D. (2005). Appreciative inquiry: A positive revolution in change. San Francisco, CA: Berrett-Koehler.
Crosskerry, P. (2003). The importance of cognitive errors in diagnosis and strategies to minimize them. Academic Medicine, 78(8), 775–780.
Dewa, C., Loong, D., Bonato, S., & Trojanowski, L. (2016). The relationship between physician burnout and quality of healthcare in terms of safety and acceptability: a systematic review. BMJ Open, 7(6), e015141.
Dierynck, B., Leroy, H., Savage, G., & Choi, E. (2017). The role of individual and collective mindfulness in promoting occupational safety in Health Care. Medical Care Research and Review, 74(1), 79–96.
Dunn, P., Arnetz, B., Christensen, J., & Homer, L. (2007). Meeting the imperative to improve physician wellbeing: assessment of an innovative program. Journal of General Internal Medicine, 22(11), 1544–1552.
Epstein, R. (1999). Mindful practice. Journal of the American Medical Association, 282, 833–839.
Epstein, R. (2014). What will it take for physicians to practice mindfully? Promoting quality of care, quality of caring, resilience, and well-being. In A. Le, C. Ngnoumen, & E. Langer (Eds.), The Wiley Blackwell handbook of mindfulness (1st edn). Hoboken, NJ: Wiley.
Epstein, R. (2017). Attending: Medicine, mindfulness, and humanity. New York: Scribner.
Epstein, R., & Krasner, M. (2017). Mindful practice workshop facilitator manual, 3rd edn. Rochester, NY: University of Rochester School of Medicine and Dentistry.
Freudenberger, H. (1975). The staff burnout syndrome in alternative institutions. Psychotherapy Theory Research and Practice, 12, 72–83.
Kabat-Zinn, J. (2014). Mindfulness and learning: An interdisciplinary symposium. Baltimore, MD: Johns Hopkins University.
Kleinman, A. (2017). The art of medicine: Presence. The Lancet, 2466–2467.
Krasner, M. S. (2016). Teaching health care professionals. In D. McCown, D. Reibel, & M. Micozzi (Eds.), Resources for teaching mindfulness: An international handbook (pp. 391–407). Cham: Springer.
Krasner, M., & Epstein, R. (2010). Mindful communication: Bringing intention, attention, and reflection to clinical practice: Curriculum Guide. Rochester, NY: University of Rochester School of Medicine and Dentistry.
Krasner, M., Epstein, R., Beckman, H., Suchman, A., Mooney, C., & Quill, T. (2009). Association of an educational program in mindful communication with burnout, empathy and attitudes among primary care physicians. Journal of the American Medical Association, 302(12), 1284–1293.
Linzer, M. (2018). Clinician burnout and the quality of care. JAMA Internal Medicine, 178(10), 1331–1332.
Ludwig, D., & Kabat-Zinn, J. (2008). Mindfulness in Medicine. Journal of the American Medical Association, 300(11), 1350–1352.
Maslach, C. (1976). Burned out. Human Behavior, 5, 16–22.
McHugh, M., Kutney-Lee, A., Cimiotti, J., & Sloane, D. A. (2011). Nurses’ widespread job dissatisfaction, burnout, and frustration with health benefits signal problems for patient care. Health Affairs, 30(2), 202–210.
Montgomery, A. (2014). The inevitability of physician burnout: Implications for interventions. Burnout Research, 1, 50–56.
Panagioti, M., Geraghty, K., Johnson, J., Zhou, A., Panagopoulou, E., Chew-Graham, C., et al. (2018). Association between physician burnout and patient safety, professionalism, and patient satisfaction: A systematic review and meta-analysis. JAMA Internal Medicine, 178(10), 1317–1331.
Shanafelt, T. (2003). The well-being of physicians. American Journal of Medicine, 114(6), 513–519.
Shanafelt, T., & Noseworthy, J. (2017). Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clinic Proceedings, 92(1), 129–146.
Shanafelt, T., Boone, S., Tan, L., Dyrbye, L., Sotile, W., Satele, D., et al. (2012). Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Archives of Internal Medicine, 172(18), 1377–1385.
Shanafelt, T., Goh, J., & Sinsky, C. (2017). The business case for investing in physician well-being. JAMA Internal Medicine, 177(12), 1826–1832.
Shanafelt, T., Schein, E., Minor, L., Trockel, M., Schein, P., & Kirch, D. (2019). Healing the professional culture of medicine. Mayo Clinic Proceedings, 94, 81556–81566.
Sibinga, E., & Wu, A. (2010). Clinician mindfulness and patient safety. JAMA, 304(22), 2532-2533.
Sinsky, C., Colligan, L., Li, L., Prgomet, M., Reynolds, S., Goeders, L., et al. (2016). Allocation of physician time in ambulatory practice: A time and motion study in 4 specialties. Annals of Internal Medicine, 165(11), 753–760.
Sinsky, C., Dyrbye, L. N., West, C., Satele, D., Tutty, M., & Shanafelt, T. (2017). Professional satisfaction and the career plans of US physicians. Mayo Clinic Proceedings, 92(11), 1625–1635.
Tan, C.-M. (2012). Search inside yourself: The unexpected path to achieving success, happiness (and world peace). New York: HarperCollins.
Treadway, K. (2008). The future of primary care: Sustaining relationships. New England Journal of Medicine, 359(25), 2086.
Verghese, A. (2016, October). The importance of being. Health Affairs, 1924–1927.
Vogus, T., & Sutcliffe, K. (2007a). The impact of safety organizing, trusted leadership, and care pathways on reported medication errors in hospital nursing units. Medical Care, 45(10), 997–1002.
Vogus, T., & Sutcliffe, K. (2007b). The safety organizing scale: development and validation of a behavioral measure of safety culture in hospital nursing units. Medical Care, 45(1), 46–54.
West, C., Dyrbye, L. N., & Shanafelt, T. (2018). Physician burnout: contributors, consequences and solutions. Journal of Internal Medicine, 283, 515–529.
Williams, E., Conrad, T., Scheckler, W., Linzer, M., McMurray, J., & Schwartz, M. (2001). Understanding physicians’ intentions to withdraw from practice: The role of job satisfaction, stress, mental and physical health. Health Care Management Review, 26(1), 7–19.
Zuger, J. (2004). Dissatisfaction with medical practice. New England Journal of Medicine, 350(1), 69–75.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Krasner, M.S., Epstein, R. (2020). Mindful Practice: Organizational Change and Health Professional Flourishing Through Cultivating Presence and Courageous Conversations. In: Montgomery, A., van der Doef, M., Panagopoulou, E., Leiter, M.P. (eds) Connecting Healthcare Worker Well-Being, Patient Safety and Organisational Change. Aligning Perspectives on Health, Safety and Well-Being. Springer, Cham. https://doi.org/10.1007/978-3-030-60998-6_15
Download citation
DOI: https://doi.org/10.1007/978-3-030-60998-6_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-60997-9
Online ISBN: 978-3-030-60998-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)