
Summary
Introduction: Assessment of the individual safest minimal mean arterial pressure (MAP) during cardiac surgery remains empirical. The objective of this study was to evaluate the lower limit of autoregulation (LLA) within a short period (15 min).
Methods: After developing autoregulation software (OptiMAP) incorporated into transcranial Doppler ultrasound (Waki-Atys®, Lyon, France), we monitored the mean blood flow velocity (MV) and MAP. Thirty successive values of MV and MAP were automatically analysed to calculate the correlation (Mx) between the two parameters. We compared two methods of Mx sampling during a period of 15 min: Mx10s = long averaging windows (one MAP/MV pair recorded every 10 s), and Mx2s = short averaging windows (one MAP/MV pair recorded every 2 s). The LLA value calculated from the whole recording (Mx10s) was used as the reference. Autoregulation was considered impaired at an Mx value >0.35.
Results: Five patients were included in the study. The surgery lasted for 138 ± 32 min and cardiopulmonary bypass lasted for 72 ± 33 min. MAP and MV were recorded for 117 ± 24 min. MAP varied from 33 ± 10 to 92 ± 10 mmHg. LLA calculated from the whole recording (Mx10s) was similar to LLA calculated from the 15-min recording (Mx2s): 70 ± 2.5 versus 73 ± 3.5 mmHg. MAP remained below LLA during 48 ± 12% of the recording. During the 15-min recording, Mx10s was not able to calculate the LLA value.
Conclusion: In cases of haemodynamic instability, decreasing the Mx sampling window seems to accurately detect LLA.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Cerebral autoregulation
- Cardiac surgery
- Mean arterial pressure
- Cardiopulmonary bypass
- LLA
- Lower limit of autoregulation
- Mx
Introduction
Setting the mean arterial pressure (MAP) during cardiopulmonary bypass (CPB) in cardiac surgery remains a real challenge. A recent trial tested two levels of MAP (70–80 versus 40–50 mmHg) to prevent cerebral injury [1] but did not find any differences between the two treatment groups and concluded that MAP had to be individualized for each patient. This concept was largely explained in a recent review [2]. Both hypotension and hypertension during cardiac surgery are detrimental to cardiac surgical patients. Blood pressure management based on a personalized target is promising in further improving neurological outcomes after cardiac surgery [2]. The remaining question is how to identify this target in an individual patient. Currently, the best tool to determine this target is probably cerebral autoregulation monitoring, as was concluded in a recent randomized trial [3].
The cerebral autoregulation status can be measured by the mean velocity index (Mx), which is a moving Pearson correlation coefficient between paired MAP and cerebral blood flow velocity values. It is able to give the autoregulation status on a continuous basis. Other indices have been developed for use during cardiac surgery, such as the cerebral oximetry index (COx), using near-infrared spectroscopy (NIRS) technology [2, 4]. Overall, Mx is considered the best noninvasive tool to assess autoregulation in the operating room [5], and it was evaluated in a recent randomized trial where its use to set MAP during CPB decreased postoperative delirium.
Currently, in a large majority of publications, Mx is calculated as a continuous, moving Pearson’s correlation coefficient between MAP and transcranial Doppler ultrasound (TCD) mean velocity (MV). Consecutive, paired, 10-s averaged values over a 300-s duration are used for each calculation, incorporating 30 data points to display an Mx value. When autoregulation is intact, there is no correlation between cerebral blood flow (CBF) and MAP, and the Mx value approaches 0. When autoregulation is impaired, the Mx value approaches 1. The length of the average window is seldom discussed in the literature. However, Mx was first developed in neurointensive care with small and slow variations in MAP and very long data recordings (lasting for several days). In the cardiac surgery field, there are bigger and faster MAP variations. Therefore, the aim of this study was to test a new setting of Mx calculation with shorter average periods. We kept the same sample with 30 data points being used to calculate Mx, but we decreased the average period from 10 to 2 s. Our hypothesis was that in cardiac surgery, the arterial pressure modification amplitude and its consequences for CBF would be better assessed with these more rapid settings.
Materials and Methods
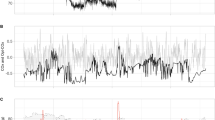
In patients under general anaesthesia, after induction, TCD (Waki-Atys®) monitoring of the middle cerebral arteries was performed using a smart automatic robotic probe. Digitized arterial blood pressure and TCD signals were processed using OptiMAP software. OptiMAP was developed to monitor autoregulation and was installed in the TCD device (Fig. 1).

Two screenshots from OptiMAP software (the post-treatment analysis screen) during cardiac surgery in the same patient. Left panel: Quick assessment of the lower limit of autoregulation (LLA) with Mx2s (grey bars) and Mx10s (white bars) during 15 min of recording. Right panel: LLA assessment with Mx10s (grey bars) during the whole recording. The top graphs (A) show the mean arterial pressure (MAP) and mean velocity trends during the whole procedure; the middle graphs (B) show the Mx2s and Mx10s trends; and the bottom graphs (C) show the Mx values versus MAP clustered in 5-mmHg intervals, with the Mx value 0.35 shown in each graph by a horizontal white line
The clinicians did not use the OptiMAP software and autoregulation data to optimize haemodynamic status during the surgery. They had access only to the absolute values of MV and other traditional markers (the systolic velocity, diastolic velocity, pulsatility index and their trends). MAP management was at the discretion of the clinicians, who could change the goals on the basis of the monitoring data.
We compared two methods of Mx calculation offline to assess the lower limit of autoregulation (LLA): Mx10s, with long averaging windows of 10 s [2, 3, 5], and Mx2s, with short averaging windows of 2 s. Mx10s requires a minimum recording of 5 min of data to calculate the first value, and this value is refreshed every 10 s. With Mx2s, the first value is available after 1 min, and this is refreshed every 2 s. Mx2s and Mx10s were used during a short 15-min recording to assess LLA. As described in the literature, Mx10s was used as the gold standard to determine LLA on the overall recording during the surgery. Autoregulation was considered lost (defining the LLA) when Mx increased to >0.35.
Demographic and general data on the patient were collected (age, sex, and data on the timing of different aspects of the surgery), as well as haemodynamic data. The recordings were post-analysed by one investigator not involved in patient care. After the artefacts were cleaned up, the whole monitoring was analysed with Mx10s and the 15-min sample was analysed with Mx2s and Mx10s. The Mx values were plotted as a function of MAP in 5-mmHg bins with the number of MAP values used to construct each bin (Fig. 1).
Results
Five patients (three men and two women) were enrolled in our preliminary pilot study. All results are expressed as mean ± standard deviation. The age of the patients was 71 ± 6 years. The surgery lasted for 138 ± 32 min and CBP lasted for 72 ± 33 min. MAP and MV on TCD were recorded continuously for 117 ± 24 min. MAP was very labile, varying between 33 ± 10 and 92 ± 10 mmHg throughout the entire CPB recording. During the 15-min recording, MAP was also very labile, varying from 40 ± 6.3 to 90 ± 5.5 mmHg.
During a period of 15 min with huge and rapid variations in MAP, LLA could not be calculated with Mx10s in any patient (the Mx value was never under 0.35), whereas LLA was able to be calculated with Mx2s in all patients.
The LLA value calculated from the whole CPB recording with Mx10s was similar to that calculated using Mx2s in 15 min (70 ± 2.5 versus 73 ± 3.5 mmHg).
During the whole recording, the MV value below LLA was lower than the MV value above LLA (33 ± 9 versus 40 ± 11 cm/s, P = 0.004). The MV value at LLA (38 ± 10 cm/s) did not differ from that at higher MAP values (40 ± 11 cm/s), pleading also for a correct LLA assessment detection with the Mx10s.
In our cohort, the MAP value remained under LLA for 48 ± 12% of the recording period.
Discussion
These data show that during acute variations in MAP (from 40 ± 6.3 to 90 ± 5.5 mmHg during a 15-min recording), Mx2s can rapidly provide a minimal acceptable MAP value to preserve CBF, whereas Mx10s is unable to help clinicians in this way. In the area of patient-centred care, use of Mx as a tool to personalize MAP in each patient is promising.
Rapid cerebral autoregulation assessment at the start of the procedure may lead the clinician to consider LLA as a possible MAP target. Decreasing the average window exposes this marker to an increase in artefact noise on the signal; thus, it is less efficient for longer trends, such as those observed in the intensive care unit. However, in this specific setting of haemodynamic instability, Mx2s can analyse cerebral autoregulation, unlike Mx10s. Furthermore, despite its short period of analysis, the LLA value observed with Mx2s was also comparable to that observed with Mx10s during the whole recording period.
Our study had several limitations. First, we chose as a definition of autoregulation an Mx value lower than 0.35. The Mx cut-off value indicating loss of autoregulation (and thus providing the LLA) is not clearly known and has been described as being between 0.25 and 0.5 [6]; a recent prospective intervention study chose a value of 0.4 [3]. In that study, the authors suggested that individualizing MAP during CPB on the basis of cerebral autoregulation monitoring could be effective in reducing the incidence of postoperative delirium. They used LLA as the minimal tolerable MAP value during CPB. They assessed LLA during the first part of the surgery (before CPB was started). During CPB, the patient’s MAP was targeted to be greater than the LLA value. In the control group, the MAP targets were determined according to institutional practice. The LLA value was determined prior to CPB on the basis of the highest MAP value at which Mx increased from <0.4 to ≥0.4. When Mx did not cross 0.4 clearly, LLA was defined as the blood pressure with the lowest Mx value (the MAP value with the best autoregulation). This methodological detail is very relevant. Indeed, like those authors, we experienced some difficulties in assessing LLA quickly in the first part of the procedure with the classic Mx as was described by Czosnyka et al. [5] more than 10 years ago.
The main limitation of our study was definitely the small number of patients. It was only a preliminary pilot study to provide a proof of concept. Further studies are planned to test this concept in a larger cohort.
Finally, a technical limit of Doppler measurement is the recording of surgical artefacts. Indeed, we observed that the surgeon’s electrosurgical knife generated noise during the first part of the procedure. These artefacts interfere with use of TCD and compromise use of Mx in the pre-CPB period. To avoid this problem, it would be interesting to develop an automatic ‘signal cleaner’ at some stage.
These difficulties in recording a good signal in the operating room provide a strong argument for developing quicker LLA assessment techniques that could be used before the surgery is started. With this new specific setting of Mx and LLA calculation within a shorter period (15 min), we have proposed a new tool to help clinicians use autoregulation monitoring. With a MAP value below the LLA value 50% of the time in this observational study, traditional management of MAP may not be aggressive enough to avoid ischaemic consequences for the brain.
Conclusion
Cardiac surgery is characterized by acute haemodynamic variations. Use of a shorter Mx sampling window (2 s versus 10 s) allows accurate LLA detection within 15 min. Such rapid and sophisticated detection could assist clinicians with better MAP target management during CPB. Further studies should be performed to validate these initial findings.
References
Vedel AG, Holmgaard F, Rasmussen LS, Langkilde A, Paulson OB, Lange T, Thomsen C, Olsen PS, Ravn HB, Nilsson JC (2018) High-target versus low-target blood pressure management during cardiopulmonary bypass to prevent cerebral injury in cardiac surgery patients: a randomized controlled trial. Circulation 137(17):1770–1780
Liu Y, Chen K, Mei W (2019) Neurological complications after cardiac surgery: anesthetic considerations based on outcome evidence. Curr Opin Anaesthesiol 32(5):563–567
Brown CH, Neufeld KJ, Tian J et al (2019) Effect of targeting mean arterial pressure during cardiopulmonary bypass by monitoring cerebral autoregulation on postsurgical delirium among older patients: a nested randomized clinical trial. JAMA Surg 154(9):819–826. https://doi.org/10.1001/jamasurg.2019.1163
Ono M, Zheng Y, Joshi B, Sigl JC, Hogue CW (2013) Validation of a stand-alone near-infrared spectroscopy system for monitoring cerebral autoregulation during cardiac surgery. Anesth Analg 116(1):198–204
Caldas JR, Haunton VJ, Panerai RB, Hajjar LA, Robinson TG (2018) Cerebral autoregulation in cardiopulmonary bypass surgery: a systematic review. Interact Cardiovasc Thorac Surg 26(3):494–503
Joshi B, Ono M, Brown C, Brady K, Easley RB, Yenokyan G, Gottesman RF, Hogue CW (2012) Predicting the limits of cerebral autoregulation during cardiopulmonary bypass. Anesth Analg 114(3):503–510
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Ethics declarations
The authors have no conflicts of interest.
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Gergelé, L., Khadraoui, Y., Manet, R., Desebbe, O. (2021). Quick Assessment of the Lower Limit of Autoregulation by Use of Transcranial Doppler Ultrasound During Cardiac Surgery. In: Depreitere, B., Meyfroidt, G., Güiza, F. (eds) Intracranial Pressure and Neuromonitoring XVII. Acta Neurochirurgica Supplement, vol 131. Springer, Cham. https://doi.org/10.1007/978-3-030-59436-7_30
Download citation
DOI: https://doi.org/10.1007/978-3-030-59436-7_30
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-59435-0
Online ISBN: 978-3-030-59436-7
eBook Packages: MedicineMedicine (R0)