
Abstract
Prior to widespread use of vaccine, Haemophilus influenzae type b (Hib) was the leading cause of bacteremia, pneumonia, and meningitis among US infants and young children. Invasive Hib disease was estimated to infect 1 in 200 children younger than 5 years of age in the USA. Hib vaccines were introduced into the national pediatric immunization schedule in the late 1980s. Almost immediately following their widespread use, there was a dramatic decline in disease incidence. While developed countries were early adopters of the conjugate Hib vaccine, developing countries were slower to do so for a variety of reasons, including but not limited to the perceived lack of disease burden to justify adding another vaccine to the schedule and the associated financial constraints of being able to do so. The African nation of Gambia, however, introduced Hib vaccine in 1997, being among the first African countries to routinely immunize their children against this infection. Prior to vaccine initiation, the incidence of Hib meningitis in The Gambia was 297 per 100,000 children younger than 1 year of age and 60 per 100,000 children younger than 5 years of age. Only 55% of infected children fully recovered (Bijlmer et al., J Infect Dis 161:1210–5, 1990). Although the incidence of Hib meningitis in The Gambia was similar to that in the USA, Gambian children were significantly more likely to have devastating outcomes (Bijlmer et al., J Infect Dis 161:1210–5, 1990). Five years after introduction of conjugate Hib vaccine in The Gambia, the incidence of Hib meningitis decreased to zero in children less than 5 years of age (Oluwalana et al., J Pediatr 163:S4–7, 2013; Adegbola et al., Lancet 366:144–50, 2005). In addition, Hib nasopharyngeal carriage among toddlers decreased from 12% to 0.25% during this time period (Adegbola et al., Lancet 366:144–50, 2005). The data from The Gambia highlight the effectiveness of conjugate Hib vaccines in the prevention of invasive disease. Observations regarding the effectiveness of Hib vaccine are not isolated to the USA and The Gambia. Similar impressive results have been achieved in every part of the world where Hib vaccination has been introduced.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Haemophilus influenzae type b
- Hib
- Polysaccharide vaccine
- Conjugate vaccine
- Bacterial meningitis
- Epiglottitis
Haemophilus influenzae Type B
Etiology
In 1892, German bacteriologist, Richard Pfeiffer, first isolated Haemophilus influenzae from the sputum of patients with flu-like illnesses , mistaking this newly discovered Gram-negative pleomorphic coccobacillus for the cause of influenza. Influenza viruses weren’t discovered as the cause of influenza until 4 decades later. In the meantime, Margaret Pittman further characterized H. influenzae showing that isolates of the bacterium could be encapsulated (types a–f) or nonencapsulated (non-typeable). She found that H. influenzae type b was the most common type isolated from the cerebrospinal fluid and blood of children. The bacterial polyribosylribitol phosphate (PRP) polysaccharide capsule was identified early on as a primary virulence factor capable of facilitating hematogenous spread of infection and preventing phagocytes from engulfing and killing the bacteria. Antibodies directed against PRP were subsequently found to correlate with both short-term and long-term protection from invasive disease.
Pre-vaccine epidemiology
Hib infection occurs worldwide, in both developing and developed countries. While nearly all invasive Hib diseases occur in children younger than 5 years, the majority of infection is seen in those younger than 18 months of age. Globally, each year during the pre-vaccine era, Hib caused an estimated eight million cases of invasive disease and more than 370,000 deaths among children younger than 5 years [4]. In the early and mid-1980s, in the USA, it was estimated that 20,000 cases of invasive Hib disease occurred each year. Infecting 1 in 200 children younger than 5 years of age, Hib was the leading cause of bacterial meningitis among US children.
Table 12.1 lists the factors associated with an increased risk of acquiring invasive Hib infection [5]. One subpopulation known to be in this category is the Alaskan Natives. While the incidence of invasive Hib disease among children less than 5 years old in the general US population was 40–50 per 100,000, the incidence among the Alaskan Native population was closer to 332 per 100,000 [6, 7]. On the other hand, breastfeeding has been found to protect against invasive Hib disease, particularly in the first six months of life. Secondary cases of infection may occur among under- or unimmunized children residing in the same house or attending the same childcare center as an infected person; however, these account for less than 5% of all invasive Hib diseases.
Transmission
Hib transmission occurs from person to person through respiratory droplets or direct contact with respiratory secretions. Neonatal acquisition of infection through contact with genital tract secretions has also been reported. Pharyngeal colonization is thought to precede infection (through subsequent bacteremia and seeding of distal sites or contiguous spread of respiratory mucosa) and contribute to community spread.
Clinical presentation
The six most common presentations of invasive Hib disease include meningitis, bacteremic pneumonia, epiglottitis, septicemia, cellulitis, and osteoarticular infections [8]. Prior to the use of vaccine, more than half of all invasive Hib infections resulted in meningitis . In fact, Hib was the leading cause of bacterial meningitis among children younger than 5 years old. Of children who developed Hib meningitis, 4 % succumbed to disease, despite appropriate therapy. Of those who survived, 15–30% still suffered from hearing impairment or other neurologic sequelae. Less common manifestations of Hib infection include purulent pericarditis, endocarditis, and peritonitis.
Management
The treatment for invasive Hib disease includes intravenous administration of either ampicillin (if the isolate is beta-lactamase negative) or a third-generation cephalosporin (ceftriaxone, cefotaxime, if the isolated is beta-lactamase positive) for 7–10 days. For patients with Hib meningitis, administering dexamethasone before or at the same time as the first dose of antibiotics has been shown to reduce the rates of sensorineural hearing loss.
Prevention
The primary approach to community-wide Hib prevention includes the routine administration of Hib vaccine to infants starting at 2 months of age. Some circumstances require that close contacts of an index case of invasive Hib disease receive antibiotic prophylaxis to prevent secondary spread of infection (Table 12.2). Rifampin is the drug of choice for most individuals who require chemoprophylaxis. Rifampin (and other antibiotics like ceftriaxone) is effective at eradicating nasopharyngeal colonization of Hib in 95% of carriers and is effective in reducing the number of secondary cases of infection.
Hib Vaccine
Vaccine characteristics
There are currently three monovalent and one combination conjugate Hib vaccines available for use in the USA (Table 12.3). These vaccines contain Hib PRP covalently linked to a carrier protein, either tetanus toxoid (PRP-T) or the outer membrane protein complex from Neisseria meningitidis (PRP-OMP). The timing of administration and number of doses required to complete the primary conjugate Hib vaccine series is determined by the vaccine product used. It is important to note that immunization with a vaccine conjugated with a tetanus toxoid is not a substitute for a tetanus vaccine.
Vaccine storage, preparation, administration
PedvaxHib is provided in ready-to-use vials. There is no reconstitution required. ActHIB and Hiberix are provided as lyophilized powder which is to be reconstituted with the provided saline diluent. Pentacel consists of a liquid component (diphtheria-tetanus-acellular pertussis-inactivated polio [DTaP-IPV]) and a lyophilized powder (ActHIB). The supplied lyophilized powder is to be reconstituted with the supplied liquid component just before administration. All Hib vaccines should be maintained at refrigerator temperature (2–8 °C). When ready for use, a 0.5 mL dose of vaccine is administered intramuscularly.
Vaccine recommendations
Routine Hib immunization consists of a primary vaccine series and a subsequent booster. The primary vaccine series is typically initiated at 2 months of age but can be started as early as 6 weeks. The timing and the number of doses administered in the primary vaccine series is dependent on the vaccine product used and the age of the patient when the vaccine series is initiated (Table 12.4). The booster dose, for which any of the Hib vaccine products can be used, is administered between 12 and 15 months of age and must be given more than 8 weeks after the last dose of the primary series. Children younger than 5 years of age who have not yet been immunized against Hib should be vaccinated according to the catch-up recommendation schedule (Table 12.4).
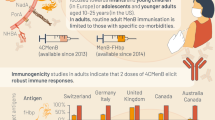
Hib vaccination is not recommended for healthy children over 5 years old because of the low risk for acquiring invasive Hib disease in this age group. There are certain risk factors , however, that increase the risk for invasive Hib disease even among older children, adolescents, and adults. Hib vaccine recommendations for these individuals are listed in Table 12.5. In particular, vaccines administered within two weeks of starting chemotherapy are not considered to be effective. In such instances, the children should be re-immunized at least 3 months after completing chemotherapy.
Contraindications to vaccines
Hib vaccine is contraindicated in patients who have had an anaphylactic or severe allergic reaction to a prior dose of Hib vaccine or to a vaccine component. If Guillain-Barre syndrome occurred within 6 weeks of receipt of a prior vaccine containing tetanus toxoid, the benefits and risks of giving a Hib vaccine product conjugated to a tetanus toxoid (ActHIB, Hiberix, Pentacel) should be discussed. The contraindications to the combination vaccine are similar to those of the vaccine components when separately administered.
Adverse events
Most reactions to Hib vaccine are mild and last for less than a day. Self-limiting injection site complaints such as pain, redness, and swelling are common. The adverse reactions following combination vaccines are similar to those of the vaccine components when separately administered. Severe adverse reactions to the Hib vaccine are very rare.
Immunogenicity
Antibodies to the Hib capsular polysaccharide, PRP, at a concentration of 0.15 μg/mL and 1 μg/mL confer short- and long-term protection, respectively, against invasive disease. More than 95% of infants will develop protective antibody concentrations after completion of the Hib primary vaccine series. PedvaxHib (PRP-OMP) administration results in a robust antibody response after the first dose, with a boost in titers after the second dose, thus leading to the need for only two doses of vaccine to complete the primary series with this vaccine formulation . On the other hand, ActHIB (PRP-T) requires a three-dose primary series of vaccine to achieve protective antibody concentrations. As the antibody levels decline following completion of the primary series, a booster dose administered at 12–15 months is needed to maintain protection from disease.
Impact of Vaccine on Disease Burden
The first H. influenzae vaccine to be developed was a monovalent polysaccharide vaccine composed of the purified PRP capsule from Hib strains that became available in the mid-1980s. As with other pure polysaccharide vaccines, this formulation of Hib vaccine was poorly immunogenic in young infants and children, failed to elicit a T-cell-dependent immune response , did not induce immune memory, and had no effect on reducing nasopharyngeal carriage [8]. Post-marketing studies in the USA found the effectiveness of this polysaccharide vaccine to range between 69% and 88% among children less than 18 months of age [9]. In addition, uptake of the polysaccharide vaccine never reached higher than 35% among US children [10]. The biochemical process of conjugating (covalently linking) the PRP polysaccharide to a protein carrier changes the manner in which the immunogen is recognized by, and processed by, the immune system. Instead of being processed in a T-cell-independent manner like pure polysaccharide antigens, conjugated PRP vaccines are processed in a T-cell-dependent manner. They are, therefore, highly immunogenic in young infants, they induce immune memory, and their use is associated with marked reductions in nasopharyngeal carriage. Monovalent conjugate Hib vaccines were first licensed by the FDA in the USA in 1987 [9] and subsequently recommended by the Advisory Committee on Immunization Practices in 1990 for use in all infants starting at 2 months of age.
Although conjugate Hib vaccines were introduced into the pediatric immunization schedule in 1990, coverage rates among infants in the USA did not reach 90% until 1995 [10]. Since then, there has been a sustained reduction in the prevalence of Hib carriage among preschool-aged children to less than 1% and a decline in disease incidence exceeding 99%. In fact, the incidence of invasive Hib infection among children younger than 5 years of age has remained below the Healthy People 2020 goal of 0.27 per 100,000 for the past decade [11]. Currently, invasive Hib disease occurs primarily in un- or under-immunized children younger than 5 years and among children who are later found to have an inherited humoral immunodeficiency . Fully immunized individuals who develop severe Hib disease should undergo a detailed diagnostic evaluation for conditions that may have predisposed them to invasive disease.
By the year 2000, conjugate Hib vaccines were routinely used only in the Americas and European region of the WHO. While developed countries were early to incorporate conjugate Hib vaccine into their immunization programs , most underdeveloped nations were faced with insurmountable barriers to do so. Obstacles to adding Hib to existing vaccine programs included the paucity of data on country-specific disease burden, a lack of awareness of the potential for a major public health impact of vaccine, and costs associated with its routine administration [12]. Globally, the annual invasive Hib disease burden of more than eight million cases and 363,000 deaths was responsible for 3% of all-cause mortality in children under 5 years of age [13].
In this same year, the Global Alliance for Vaccines and Immunizations, or GAVI , initiated a program to provide Hib vaccines to eligible low-income countries. Despite the financial support, engagement in the program remained low, suggesting that a general lack of awareness about Hib disease was, perhaps, an even greater barrier to vaccination than vaccine costs [14]. In 2006, the WHO formally recommended that conjugate Hib vaccines be routinely administered to all infants and children of all nations. In an intensive effort to support widespread uptake of Hib vaccine, GAVI partnered with international public health organizations to support research aimed at addressing gaps in understanding disease burden ; improving communication and coordination with local, regional, national, and global partners; and advocating for the adoption of Hib vaccine in countries around the world [12]. By early 2020, all but three countries, China, Russia, and Thailand, have incorporated routine Hib vaccination into their national immunization programs with ongoing efforts to optimize their rates of vaccine coverage (Fig. 12.1).

2018 conjugate Hib vaccination rates by country
Following widespread global use of conjugate Hib vaccine, invasive Hib disease burden around the world decreased dramatically. Between 2000 and 2015, corresponding to the increasing number of countries routinely administering Hib vaccine, the number of global Hib deaths had declined by 90% (Fig. 12.2). By 2015, annual estimates of invasive Hib disease among children younger than 5 years old (excluding those with HIV) were down to 340,000 cases (from eight million) and 29,500 deaths (from 363,000) [15]. In 2015, more than 80% of all global Hib deaths were reported from four countries India, Nigeria, China, and Sudan [15].

The number of countries routinely using Hib vaccine in their pediatric immunization schedule versus the number of global Hib-related deaths among children younger than 5 years of age
India first introduced conjugate Hib vaccine in the southern state of Tamil Nadu in 2011. Within 2 years of routine vaccine use, they found a 78% decline in confirmed cases of Hib meningitis [16]. Shortly after, conjugate vaccine uptake increased nationwide. Despite an 81% decline in estimated Hib deaths in Indian children between 2000 (82,600 deaths) and 2015 (15,600 deaths), invasive Hib disease still accounted for 3% of all-cause mortality in this age group, largely because of suboptimal vaccine coverage rates in many areas. One state, Uttar Pradesh, did not adopt Hib vaccine until the end of 2015. Of the Hib deaths in this report, 60% were reported from this region in India [17].
Conjugate Hib vaccine has proven safe and effective in preventing invasive Hib disease everywhere it is used across the globe. It is estimated that Hib vaccines prevented 1.2 million infant and childhood deaths between 2000 and 2015. The efforts and commitments of global partnerships between individual nations and GAVI, the US Centers for Disease Control and Prevention, and several agencies of the World Health Organization have been highly successful in reducing global morbidity and mortality from invasive Hib disease.
References
Bijlmer HA, van Alphen L, Greenwood BM, Brown J, Schneider G, Hughes A, Menon A, Zanen HC, Valkenburg HA. The epidemiology of Haemophilus influenzae meningitis in children under five years of age in the Gambia, West Africa. J Infect Dis. 1990;161:1210–5.
Oluwalana C, Howie SRC, Secka O, Ideh RC, Ebruke B, Sambou S, Erskine J, Lowe Y, Corrah T, Adegbola RA. Incidence of Haemophilus influenzae type b disease in the Gambia 14 years after introduction of routine Haemophilus influenzae type b conjugate vaccine immunization. J Pediatr. 2013;163:S4–7.
Adegbola RA, Secka O, Lahai G, Lloyd-Evans N, Njie A, Usen S, Oluwalana C, Obara S, Weber M, Corrah T, Mulholland K, McAdam K, Greenwood B, Milligan PJ. Elimination of Haemophilus influenzae type b (Hib) disease from the Gambia after the introduction of routine immunization with a Hib conjugate vaccine: a prospective study. Lancet. 2005;366:144–50.
Watt JP, Wolfson LJ, O’Brien KL, Henkle E, Deloria-Knoll M, McCall N, Lee E, Levine OS, Hajjeh R, Mulholland K, Cherian T. Burden of disease caused by Haemophilus influenzae type b in children younger than 5 years: global estimates. Lancet. 2009;374:903–11.
Wilfert CM. Epidemiology of Haemophilus influenzae type b infections. Pediatrics. 1990;85:631–5.
CDC. Progress toward elimination of Haemophilus influenzae type b disease among infants and children - United States, 1987-1995. MMWR. 1996;45:901–6.
Singleton R, Bulkow LR, Levine OS, Butler JC, Hennessy TW, Parkinson A. Experience with the prevention of invasive Haemophilus influenzae type b disease by vaccination in Alaska: the impact of persistent oropharyngeal carriage. J Pediatr. 2000;137:313–20.
Peltola H. Worldwide Haemophilus influenzae type b disease at the beginning of the 21st century: global analysis of the disease burden 25 years after the use of polysaccharide vaccine and a decade after the advent of conjugates. Clin Microbiol Rev. 2000;13:302–17.
CDC. Prevention and control of Haemophilus influenzae type b disease: recommendations of the advisory committee on immunization practices (ACIP). MMWR Recomm Rep. 2014;63:1–14.
Wegner JD. Epidemiology of Haemophilus influenzae type b disease and impact of Haemophilus influenzae type b conjugate vaccines in the United States and Canada. Pediatr Infect Dis J. 1998;17:S132–6.
CDC. Active Bacterial Core Surveillance Reports. https://www.cdc.gov/abcs/reports-findings/surv-reports.html. Accessed 1 June 2020.
Hajjeh R. Progress towards demonstrating the impact of Haemophilus influenzae type b conjugate vaccines globally. J Pediatr. 2013;163:S1–3.
World Health Organization. Estimated Hib and pneumococcal deaths for children under 5 years of age. 2000. https://www.who.int/immunization/monitoring_surveillance/burden/estimates/Pneumo_hib_2000/en/. Accessed 1 June 2020.
CDC. Progress toward introduction of Haemophilus influenzae type b vaccine in low-income countries – worldwide, 2004-2007. MMWR. 2008;57:148–51.
Wahl B, O’Brien KL, Greenbaum A, Majumder A, Liu L, Chu Y, Luksic I, Nair H, McAllister DA, Campbell H, Rudan I, Black R, Knoll MD. Burden of Streptococcus pneumoniae and Haemophilus influenzae type b disease in children in the era of conjugate vaccines: global, regional, and national estimates for 2000-2015. Lancet. 2018;6:e744–57.
Fitzwater SP, Ramachandran P, Kahn GD, Nedunchelian K, Suresh S, Santosham M, Chandran A. Impact of the introduction of the Haemophilus influenzae type b conjugate vaccine in an urban setting in southern India. Vaccine. 2019;37:1608–13.
Wahl B, Sharan A, Md K, Kumar R, Liu L, Chu Y, McAllister DA, Nair H, Campbell H, Rudan I, Ram U, Sauer M, Shet A, Black R, Santosham M, O’Brien KL, Arora NK. National, regional, and state-level burden of Streptococcus pneumoniae and Haemophilus influenzae type b disease in children in India: modelled estimates for 2000-15. Lancet. 2019;7:e735–47.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Suryadevara, M. (2021). Haemophilus influenzae Type B. In: Domachowske, J., Suryadevara, M. (eds) Vaccines. Springer, Cham. https://doi.org/10.1007/978-3-030-58414-6_12
Download citation
DOI: https://doi.org/10.1007/978-3-030-58414-6_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-58413-9
Online ISBN: 978-3-030-58414-6
eBook Packages: MedicineMedicine (R0)