
Abstract
Safe and effective management of procedure-related pain and anxiety in the emergency department (ED) has become expected. It facilitates controlled accomplishment of therapeutic and diagnostic procedures, reduces psychological trauma and its sequelae, reduces healthcare provider and parental distress, and improves parental acceptance of rendered care. Many advances in procedural sedation and analgesia (PSA) for nonelective procedures in non-fasted patients in the ED have occurred over the past 30 years as a result of intense interest in this concept and the development of general and pediatric emergency medicine specialties, for whom PSA is now considered core training. This chapter reviews some of the PSA techniques shown to safely and effectively decrease children’s pain and anxiety associated with procedures in the ED. Since pain and anxiety are frequently indistinguishable, the combination will often be referred to as distress.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Emergency department
- Procedural sedation and analgesia (PSA)
- Local anesthesia
- Psychological intervention
- Pain
- Anxiety
- Motion
- Adverse events
- Upper airway obstruction
- Laryngospasm
- Emesis
- Pulmonary aspiration
- Eutectic Mixture of Local Anesthetics (EMLA)
- Nil per os (NPO)
- American Society of Anesthesiologists (ASA)
- American College of Emergency Physicians
- Capnography
- Moderate sedation
- Deep sedation
- Naloxone (Narcan)
- Flumazenil
- Atropine
- Succinylcholine
- Ketamine
- Ondansetron (Zofran)
- Gamma-aminobutyric acid (GABA)
- Chloral hydrate
- Barbiturates
- Diazepam
- Etomidate
- Fentanyl
- Dexmedetomidine (Precedex)
- Ketofol
- Lorazepam
- Meperidine (Demerol)
- Methohexital (Brevital)
- Midazolam (Versed)
- Morphine
- Nitrous oxide
- Pentobarbital (Nembutal)
- Propofol
- Remifentanil
- S-ketamine
- Sufentanil
- Lidocaine
- Metoclopramide (Reglan)
- Scopolamine
- Diphenhydramine (Benadryl)
- Dexamethasone (Decadron)
- Codeine
- Oxycodone
- Glycopyrrolate
- Mallampati
Introduction
Why Procedural Sedation and Analgesia (PSA)?
Painful therapeutic procedures are frequently necessary during emergency care of children, many of whom already have a painful and frightening injury or illness. Immobility for diagnostic radiological procedures in young children is also often required. These procedures are distressful for the children, their parents, and their healthcare providers. Inadequately relieved procedure-related pain and distress produces physiological and psychological reactions that have acute and long-term consequences [1,2,3,4,5,6].
Safe and effective management of procedure-related pain and anxiety in the emergency department (ED) has become expected [7]. It facilitates controlled accomplishment of therapeutic and diagnostic procedures [3, 8, 9], reduces psychological trauma and its sequelae [3, 5, 8, 10], reduces healthcare provider and parental distress, and improves parental acceptance of rendered care [11]. Many advances in PSA for nonelective procedures in non-fasted patients in the ED have occurred over the past 30 years as a result of intense interest in this concept and the development of general and pediatric emergency medicine specialties, for which PSA is now considered core training [12]. Family and third-party payer’s desire for definitive management of acute injuries during initial ED visits also seems to be increasing. This chapter reviews some of the PSA techniques shown to safely and effectively decrease children’s pain and anxiety associated with procedures in the ED. Since pain and anxiety are frequently indistinguishable, the combination will often be referred to as distress.
Long-Term Negative Impact of Painful Procedures
Elimination or relief of pain and suffering, whenever possible, is an important responsibility of physicians caring for children [13], as unmanaged pain can result in a variety of negative long-term consequences [14]. Accumulating evidence indicates that by the middle of the third trimester of human gestation, ascending pain fibers fully connect to the primary somatosensory cortex of the brain [15, 16]. Descending inhibitory pain pathways , on the other hand, appear to require postnatal development. Rather than being less sensitive to pain, young infants may actually experience pain more intensely than older children [17]. As the brain rapidly matures during the first weeks to months after birth, recurrent painful stimuli may alter the formation of new neuronal circuits, resulting in children’s hypersensitivity and increased behavioral response to noxious stimuli [15, 18,19,20,21,22,23].
Inadequately controlled procedure-related pain has been correlated to increased distress and maladaptive behaviors during subsequent healthcare interactions. Boys circumcised at birth without effective anesthesia had increased distress at their 4- and 6-month routine vaccinations compared to uncircumcised controls [24]. Similarly, toddlers who had painful postoperative care during the first 3 months of life demonstrated greater pain responses at their 14-month immunizations compared with controls [25]. In older children, painful therapeutic procedures have been associated with negative memory and greater pain during similar future procedures [26,27,28], even when those future procedures are performed with adequate analgesia [5]. Although the mechanisms underlying these observations have yet to be fully elucidated, these studies show that painful episodes can be encoded into children’s implicit and explicit memories [23]. While praising a child following a painful procedure, in an effort to modify negative memories, may lessen these memories and reduce distress during subsequent procedures [29], prevention of negative memories by employing effective sedation–analgesia for intensely painful procedures is likely a crucial part of preventing the negative feedback loop that can then cause greater anxiety and pain during future procedures and healthcare interactions [30, 31].
When May PSA Not Be Needed?
PSA requires substantial and frequently scarce healthcare resources in a busy ED and has significant, albeit rare, risks. Emergency healthcare providers therefore increasingly are employing strategies that provide effective minimally painful techniques for local anesthesia or systemic analgesia. Combined with psychological or behavioral approaches to reduce patient anxiety, these strategies may greatly reduce the need for PSA as well as diminish the need for deeper sedation [32].
Nearly Painless Local Anesthesia
Topical Anesthetics
Use of topical anesthesia for children’s lacerations has become standard in many EDs. Locally compounded solutions or gels containing 4% lidocaine, 0.1% epinephrine (adrenaline), and 0.5% tetracaine (LET or LAT) provide local anesthesia when instilled for 20–30 min into an open wound or abscess [33,34,35]. These solutions are more effective in scalp and facial lacerations than those on extremities or the trunk, but their initial use markedly reduces the pain of subsequent injection of lidocaine, if such is needed. Careful application of limited amounts of these solutions onto lip or mucous membrane lacerations (e.g., using a cotton-tip swab) has been shown safe and can be quite effective [36]. Caution must be taken, especially in small children, as rapid absorption of the anesthetics could cause toxicity. A recent study also found use of LET on finger lacerations safe and effective [37].
Buffering Injected Lidocaine
Pain associated with injection of lidocaine can be markedly reduced by buffering the anesthetic, injecting slowly through fine needles (e.g., 30-gauge) subcutaneously instead of intradermally, and warming the anesthetic to body temperature [38,39,40,41,42]. Buffering lidocaine , with or without epinephrine, to pH 7.0–7.2 by mixing 1 part of 1 mEq/mL sodium bicarbonate with 9–10 parts of 1% lidocaine markedly decreases the pain of injection [43, 44]. Buffering also decreases onset time for anesthesia [44] without affecting efficacy or duration [44,45,46]. The buffered mixture is stable for at least 3 weeks when stored at room temperature [45] and longer when refrigerated [47]. Buffered lidocaine injected subcutaneously using a 30-gauge needle rapidly and effectively minimizes the pain of intravenous catheter insertion [462].
Psychological Interventions Reduce Distress and Need for PSA
Acute injury or illness causes significant anxiety and stress for most children and their parents. Lack of understanding of ED routines for care, ongoing pain, prolonged waits, preconceived notions about emergency care, and numerous other known and unknown factors interfere with effective preparation of the child and use of the child’s and parents’ coping mechanisms [48]. Consequently, many young children are frightened and unwilling to cooperate with necessary procedures , even when little or no pain is involved. A warm smile and a slow respectful and sometimes playful approach may reduce the frightened child’s perception of the provider as a threat and increase the likelihood of cooperation without need for sedation. Approaching infants, toddlers, and young children should incorporate techniques adjusted for stranger anxiety, fear of separation, and other key developmental stages [463]. Addressing parental concerns and providing them with an explanation of the plan for care, along with age-specific suggestions on how they can allay some of their child’s fears and anxieties, allows them to prepare their child as well as themselves [371].
Having their parent at their side during painful procedures in the ED is of utmost importance for school-aged and younger children, despite realizing their parent can do little to alleviate procedural pain [49]. Parents likewise believe their presence during procedures is important and beneficial to their children [50,51,52]. EDs increasingly are enacting policies to give parents the option of staying with their child during all procedures and resuscitations, usually with a staff member dedicated to explain the care provided and to monitor the parent for signs of extreme distress, syncope, etc. [53,54,55]. When suggestions are given to parents on how to help their child (e.g., touching, distracting with stories, reciting the alphabet, counting, etc.), parents can provide significant assistance in accomplishing anxiety-provoking procedures without sedation [56, 57]. In addition, nonthreatening language should be used to characterize anticipated sensations, e.g., “freezing, poking, or squeezing” instead of “burning, bee sting, or hurting.” Simply allowing young children to sit in their willing parent’s lap, with parents providing distraction and hugs for mild restraint, markedly reduces the child’s distress during minor procedures [58]. Combining this technique with LET for topical wound anesthesia, supplemented as needed with buffered lidocaine injected via a 30-gauge needle, the author rarely finds it necessary to employ PSA for suturing lacerations in young children.
What Makes PSA in the Emergency Department Different?
Children often exhibit significant distress when faced with emergency department (ED) procedures despite administration of analgesic medications and psychological interventions . They may be anxious about sounds and sights they do not understand, fearful because of prior experience or hearsay, or in pain because of incomplete analgesia or local anesthesia. Furthermore, their usual coping mechanisms may be in disarray because of the unexpected nature of their illness or injury and their perception that they have no control over the impending treatment. When children refuse or are unable to cooperate with necessary procedures or if effective local anesthesia is not possible, safe and effective pharmacologic sedation can avert detrimental patient, parent, and practitioner sequelae and facilitate accomplishment of the procedure [5, 59, 60].
ED PSA in children, however, has greater inherent risks when contrasted to elective sedation. Patients frequently have not fasted for traditional periods and consequently may have “full stomachs” [61,62,63]. Postponement of procedures to allow fasting in the ED may be impractical due to limited resources. More importantly, postponement to allow gastric emptying is likely ineffective because painful injuries and serious illnesses unpredictably delay emptying of stomach contents; moreover, necessary administration of opioids for pain management likely exacerbates this problem. Compounding these issues, children undergoing painful or anxiety-provoking procedures typically require deeper levels of sedation than adults or teenagers who may be able to better control their behavior [1]. Unanticipated arrival or deterioration of other ED patients and overextended ED staff may result in the sedating physician unpredictably being pulled away or distracted by other patients’ emergencies. Finally, therapeutic procedures performed by trainees in academic EDs frequently are more prolonged and require longer periods of sedation.
Deciding Whether to Perform PSA
The first and foremost goal of pediatric PSA is assurance of the patient’s safety and welfare during the sedation and recovery. With this in mind and the limitations noted earlier, the clinician considering PSA must carefully consider the following:
-
1.
Is the procedure necessary? Some procedures that would require PSA in many children may be unnecessary. For example, it is likely that, as in adults, many lacerations of the hand and feet heal as well with bandaging as with suturing [64]. Similarly, virtually all tongue lacerations heal well without suturing [65].
-
2.
Do I have the resources and skills to rescue if rare but serious adverse events occur? For example, would I be able to administer a paralytic drug for severe laryngospasm or secure the airway by intubation?
-
3.
What if an unexpected patient with a critical emergency arrives? Do I have the resources to continue the PSA and procedure? Or, if I had to leave the patient, do I have the resources to safely recover the patient?
Systematic Approach to Safe ED PSA
Knowledge of Clinical Policies Specific to Emergency Department
Although each facility and institution may have their own specific policies, procedures, and guidelines, it is important that the sedation provider in the emergency department is familiar with the clinical policies of their specialty. In 2014 the American College of Emergency Physicians updated its clinical policy, Procedural Sedation and Analgesia in the Emergency Department, and in 2018 approved a detailed multidisciplinary guideline for unscheduled procedural sedation [67, 101].
Goals of PSA
Pediatric PSA by experienced providers has low but inevitable risks of adverse events including respiratory depression, apnea, airway obstruction, vomiting, hypotension, and dysphoria [372]. The first and foremost goal of pediatric PSA is assurance of the patient’s safety and welfare during the sedation and recovery [59, 68]. Within this context, additional goals include control of behavior (muscle relaxation or relative immobility) and minimization of procedure-related pain, anxiety, memory, and negative psychological responses [59, 95]. Safe attainment of these goals requires careful patient screening for factors associated with increased sedation-related risk of adverse events or difficult airway management, preparation for management of possible adverse events, and meticulous assurance of effective patient cardiopulmonary and other vital functions during and after the procedural sedation.
By developing a routine or systematic approach for ED PSA, the emergency physician reduces risks for the patient by identifying children at increased risk of adverse events and increasing preparedness for safe and effective management of adverse events should they occur [69]. The systematic approach should include the following steps:
-
1.
Pre-sedation patient assessment
-
2.
Informed consent
-
3.
Plan for sedation
-
4.
Documentation/sedation record
-
5.
Recovery/discharge
-
6.
Quality improvement
Pre-sedation Patient Evaluation and Risk Assessment
Children should be screened for factors that may be associated with increased risk of adverse events or difficult management of these events during sedation. Identification of these risks allows for better preparation for management of untoward events or development of alternative plans to reduce the likelihood of undesired effects. In addition to general sedation screening in preparation for an ED procedure , a focused physical exam immediately prior to sedation should be repeated to detect any acute changes in the child’s physiological status such as acute onset of wheezing or fever.
Pre-sedation history and physical examination should focus upon the patient’s cardiorespiratory status and airway to determine the sedator’s ability to rescue breathe for this individual, if necessary [59, 70, 71]. A focused history may be guided by the mnemonic AMPLE:
-
(A) Allergies to medications, latex, CT contrast, and food (e.g., egg allergy prohibits use of propofol; shellfish allergies are associated with CT contrast reactions).
-
(M) Current medications or illicit drugs that might interact with PSA medications; these often reveal concurrent diagnoses that may impact PSA choices, e.g., psychiatric medications.
-
(P) Past medical history, including any complications with sedation or anesthesia and chronic illnesses; history of snoring/stridor, recent URI/respiratory infections or asthma exacerbations, GERD, cardiac history, prematurity, any neuromuscular disease (may contraindicate succinylcholine), and history of airway surgery/tumors/malformations.
-
(L) Last meal/fluid intake.
-
(E) Events leading to a need for procedure, e.g., associated injuries:
-
(a)
ASA physical status classification
The patient physical status classification endorsed by the American Society of Anesthesiologists (ASA) [71] to predict risk for adverse events during general anesthesia [73, 74] is helpful in assessing sedation risks and is summarized in Table 22.1. ASA Class I and II children are at low risk for serious adverse events when carefully monitored. Events that are initially minor, such as upper airway obstruction during deep sedation, usually can be easily addressed with simple interventions and catastrophic sequelae prevented. However, children with underlying illnesses often have less cardiopulmonary reserve and thus a greater risk for adverse responses to sedative and analgesic medications, and their rescues often are more difficult and complex. Therefore, when possible, it is suggested an experienced sedation provider or anesthesiologist be consulted for planning sedation of ASA Class III patients and an anesthesiologist consulted for Class IV or V patients (Table 22.1).
-
(b)
Airway assessment: comorbid risk factors, Mallampati classification
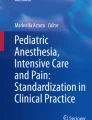
Factors associated with difficulty in airway management include those that make it hard to visualize the larynx or partially or completely obstruct the upper airway. Examples include history of previous problems with anesthesia or sedation including prolonged intubation or unplanned hospitalization; stridor, snoring, or sleep apnea; chromosomal abnormality (e.g., trisomy 21); history of prematurity with prolonged intubation; significant obesity; short neck or limited neck mobility; receding mandible (small lower jaw) or decreased hyoid-mental distance; dysmorphic facial features (e.g., Pierre–Robin syndrome); small mouth opening; protruding incisors; loose teeth; dental appliances; high, arched, and narrow palate or history of cleft palate repair ; large tongue; tonsillar hypertrophy; or no visible uvula (Fig. 22.1; Mallampati airway classifications III, IV) [70, 71]. Note, in one study, children with Mallampati scores III/IV were found to require increased airway repositioning during sedation with ketamine [374].

Mallampati airway classification. (Adapted with permission from Mallampati [357])
Problems associated with increased risk of adverse events and for which consultation with an experienced sedation practitioner or anesthesiologist is suggested include:
-
ASA physical status Class III or IV
-
Current upper respiratory illness (URI)Footnote 1
-
Pulmonary: wheezing not cleared by a bronchodilator, obstructive sleep apnea
-
Morbid obesity (>2 × ideal body weight)
-
Cardiovascular conditions: cyanosis, congestive heart failure
-
Neurological conditions: poorly controlled seizures, central apnea
-
Gastrointestinal conditions: uncontrolled gastroesophageal reflux
-
Prematurity with residual pulmonary, cardiovascular, gastrointestinal, and neurological problems
-
Age < 3 months
-
Pregnancy or suspected pregnancy
-
Neuromuscular disease
-
Severe developmental delay
-
Patients who are difficult to control
-
History of failed sedation, oversedation, or paradoxical response to sedatives
Screening for Acute Illness
Patients should be screened for acute illnesses that may increase their risk for sedation-related adverse effects. Most children undergoing ED PSA are American Society of Anesthesiologists’ Physical Status (ASA-PS) Class I or II and at low risk for serious adverse events when closely monitored and simple rescue interventions quickly applied [372]. Children with acute illnesses, however, may have less cardiopulmonary reserve and are more likely to have adverse responses to sedative and analgesic medications. A study of 83,000 children undergoing elective and nonelective sedation found that those with a current or recent (within 2 weeks) upper respiratory illness (URI) were more likely to experience adverse airway events such as obstruction, oxygen desaturation, snoring, coughing, secretions requiring suctioning, laryngospasm, stridor, or wheezing but not apnea. URIs with thick and/or green secretions were more likely to cause adverse airway events. Rates of major adverse events (laryngospasm, aspiration, unplanned intubation/admission) were <1% regardless of URI status [373]. When acute illness is detected, the sedation provider must weigh the increased risk against the need for the diagnostic or therapeutic procedure.
-
(c)
Fasting status and risk of aspiration
To decrease the risk of pulmonary aspiration of gastric contents in healthy children undergoing general anesthesia for elective procedures, fasting from clear liquids a minimum of 2 h and from milk or solid food 6–8 h is a well-established consensus-based practice [77]. However, as noted in these guidelines, “Published evidence is silent on the relationship between fasting times, gastric volume, or gastric acidity and the risk of emesis/reflux or pulmonary aspiration in humans.” Increasing evidence suggests there is not a clear association between fasting status and risk for pulmonary aspiration during procedural sedation [78, 375, 466]. It is difficult to extrapolate directly to PSA from the long experience with safe general anesthesia. It is likely that risk of aspiration is less during ED PSA compared to general anesthesia in the operating room for several reasons. First, protective airway reflexes are generally preserved at the depth of moderate sedation [77, 79]. Second, airway reflexes are also relatively intact during sedation with the commonly used dissociative agent ketamine during deep sedation or even light general anesthesia [79]. Of concern, however, these reflexes are likely blunted during deep sedation with opioids, benzodiazepines , barbiturates, propofol, and etomidate, especially if sedation is deep enough to cause apnea [358]. Third, intubation of the trachea, rarely performed in children undergoing ED PSA, likely increases the risk of pulmonary aspiration due to pharmacological abolition of protective reflexes to facilitate intubation and mechanical interference with these reflexes during passage of the endotracheal tube into the trachea [72, 73, 82]. Fourth, the great majority of children receiving ED PSA meet ASA physical status Class I or II criteria [9, 61,62,63, 81, 372] and, compared to those in ASA physical status Classes III and IV, are associated with less risk of adverse events during anesthesia [59, 375]. It is the combination of these differences—i.e., moderate sedation , common use of dissociative ketamine for deep sedation, lack of manipulation of the larynx, and healthy patients—that likely results in ED PSA having lower risk of aspiration compared to general anesthesia.
A more robust literature on identification of risk factors for aspiration in children undergoing general anesthesia has found no benefit from routine preoperative administration of antacids or pharmacological agents to increase gastric motility [75, 82]. Gastric fluid volume and pH were not different with NPO periods of 2, 4, and 12 h after drinking apple juice in one study [83] or after 30 min to 3 h, 3–8 h, or more than 8 h after clear liquid ingestion in another trial [84]. No studies have examined gastric emptying in children after solid intake, but one small study of adult women after a light breakfast found 3 of 8 had emptied their stomachs by 2 h and all by 6 h [85].
Vomiting, although not likely to result in aspiration when protective airway reflexes are intact, is a common adverse event during ED PSA in children, occurring in as much as 25% of patients, especially when opioids are coadministered prior to sedation [9, 88]. As supported by literature reviews [77, 89, 91], recent series of children receiving ketamine or nitrous oxide for ED PSA suggest there is poor correlation between the length of time of preprocedural fasting and vomiting [62, 63, 78]. No significant difference in frequency of vomiting was found between children that fasted between 0, 2, 4, 6, 8, and greater than 8 h. This may be because the vomiting is medication induced and gastric contents have little effect on likelihood of vomiting.
Gastric emptying may also be unpredictably delayed in ill or injured patients due to development of ileus [91]. ED management of pain with opioids likely exacerbates this problem. Whether brief delay (1–6 h) of PSA decreases vomiting is undetermined. Coadministration of ondansetron has been found to reduce vomiting associated with ketamine-based ED PSA but only from 12.6 to 4.7% with 13 patients needing to be treated to prevent 1 episode of vomiting [92]. No effect of ondansetron on vomiting was found when nitrous oxide was coadministered with fentanyl for PDSA [430]. This and other strategies need further investigation. It is the practice of the author to consider all sedated ED patients to have “full stomachs” and to manage them with vigilance and preparation for assisting them in clearing their oropharynx by rolling them to their side or assisting them in leaning forward. Suctioning of the mouth is then used, if needed, to “mop up.”
Pregnancy
Since many medications administered for ED PSA have the potential for causing harm to a fetus, it is recommended that the menstrual status be reviewed with post-menarchal girls and a urine pregnancy test performed prior to sedation. The US Food and Drug Administration (FDA) has categorized medications based upon known or possible risk to a developing fetus as listed in Table 22.2. Increasing uterine size , greater tendency for vomiting, and many other changes also increase the complexity of PSA during pregnancy.
Informed Consent
The physician responsible for the sedation should provide to the patient and/or parents information concerning the objectives of the sedation, behavioral changes associated with the sedative regimen (especially important when the parent/guardian plans to remain with the patient during the sedation/procedure), and potential adverse effects during and after the sedation [59, 69, 93]. Parents should understand that, albeit rare, there is a risk of pulmonary aspiration, cardiopulmonary compromise, hypoxic brain injury, and/or death. It is also recommended to discuss with them the possible need for muscle relaxation , intubation, hospitalization, and unsuccessful sedation with inability to perform the procedure. These issues that have been discussed with the parent/guardian (and patient when appropriate) and that they have given their informed consent to proceed with the sedation should be documented on the sedation record.
Adverse effects/events generally discussed include:
-
Incomplete analgesia and/or amnesia
-
Respiratory depression/apnea
-
Pulmonary aspiration
-
Psychosis and recovery dysphoria
-
Catatonia/nystagmus
-
Dysrhythmias
Plan for Sedation
-
(a)
Selection of a medication plan
Selection of medications and dosages should be guided by the desired key effect(s). An ideal regimen would provide acceptable analgesia, sedation, and amnesia for residual awareness of procedure-related pain or anxiety, cause minimal adverse effects, and work reliably with a wide therapeutic index; i.e., small differences in dose would not cause oversedation or adverse events, have rapid onset and recovery, and be easy to titrate to effect. No single agent or combination of agents fully achieves these goals. Selection of procedural sedation medications therefore is based upon balancing desired effects with the potential for adverse effects. For procedures that are very painful (e.g., fracture reduction), control of the pain will be paramount. For procedures that require the child to be motionless—e.g., computerized tomography (CT) or magnetic resonance imaging (MRI) scans—immobility may be most important. Most procedures in children require some combination of analgesia and immobility along with anxiolysis; therefore, sedation planning can be broadly organized into categories of these parameters.
Analgesia, Hypnosis, Anxiolysis, or Amnesia? Balanced Sedation
Medication selection and dose can be organized by anticipation of whether the procedure is (1) nonpainful/noninvasive or associated with (2) low level of pain and high anxiety or (3) high level of pain, high anxiety, or both, (4) whether local anesthesia can be used, and (5) whether the patient needs to be motionless; i.e., for some procedures, some motion is acceptable during painful and/or invasive procedures to the extent that the motion neither causes risk to the patient nor hinders the successful performance of the procedure, whereas in others (e.g., MRI), any movement prevents completing the procedure (see Table 22.3) [61, 94, 95].
Principal and secondary effects of sedative–analgesic medications are summarized in Table 22.4. Although combining sedative–analgesic medications generally increases the risks of adverse effects [98, 99], the actual depth of sedation is likely to be a better predictor of these risks [96, 100]. Thoughtful “balanced sedation” with anxiolytic and analgesic drugs, carefully titrated to effect, can achieve very satisfactory sedation and typically results in smaller effective doses of individual drugs than if a single drug is used. For example, fentanyl is a potent analgesic but has little or no anxiolytic or amnestic effect, whereas midazolam is a potent anxiolytic and amnestic agent with no analgesic effect. Combining fentanyl and midazolam results in effective procedural sedation, but the combination causes significantly greater respiratory depression than either fentanyl or midazolam alone [96].
Depth of Sedation
Since increasing depth of sedation is associated with increasing frequency of adverse events [59], use of the lightest effective sedation is usually preferred . However, frequently the depth of sedation required for a particular procedure cannot be accurately predicted in a specific patient [95]. Incompletely appreciated anxiety and lack of comprehension in younger children or those with developmental delay often cause need for deeper-than-anticipated sedation for procedures in which local anesthesia or mild sedation would suffice in a self-controlled adolescent or adult. For intensely painful procedures, deep sedation is typically required. Clinicians providing sedation, therefore, ideally should be trained and prepared to administer increasingly deeper sedation as guided by the patient’s response to the procedure. It is important, too, for the clinician to realize that many sedative analgesic agents also induce varying degrees of amnesia. When midazolam, ketamine, or propofol, and to a lesser extent nitrous oxide, is administered, the patient is unlikely to recall clearly procedure-related pain despite occasional moaning or crying out during intensely painful parts of the procedure [9]. However, it is unwise to promise complete amnesia during the informed consent process. The extent of procedural amnesia can be assessed in part by asking the patient if he/she “recalls anything hurting” after they have recovered ; a negative answer is reassuring to parents who have remained with the patient during the procedure. Because of amnesia for procedure-related pain, lighter and presumably safer levels of sedation may be acceptable when patient motion does not interfere with accomplishment of the procedure.
For this reason, the amnestic agent midazolam is combined with fentanyl for PSA because completely effective analgesia cannot be achieved with fentanyl without marked respiratory depression. Of note, deeper sedation with ketamine is usually much less associated with adverse cardiopulmonary effects in comparison to other agents and, in addition, ketamine induces moderate amnesia. Some older children may prefer not to be deeply sedated; in the same way, many adults fear general anesthesia. As an example, a 13-year-old boy sedated by the author with nitrous oxide in conjunction with a lidocaine fracture hematoma block recalled the next day the details of the reduction of his displaced distal radius and ulnar fractures. Yet, he was adamant that he would not have preferred to have been “put to sleep” and unaware of the reduction. Since the hematoma block was very effective and he recalled no pain, he was very satisfied with his experience of altered awareness during the fracture reduction. When local anesthesia or other analgesic technique can be achieved, some children may prefer lighter levels of sedation without loss of awareness, a concept that needs further investigation.
-
(b)
Staffing
For moderate sedation, a sedation provider trained in the sedation protocol and skilled in pediatric advanced life-support techniques is responsible for the procedural sedation–analgesia, including monitoring of the patient’s status. In the ED, this is typically the emergency physician. If, after induction of adequate sedation, that individual then performs the procedure for which sedation is provided, a second individual, typically a registered nurse, with sedation training and knowledgeable in pediatric basic life support must be at the bedside and responsible for monitoring the patient’s cardiopulmonary status and the need for interventions to manage adverse events. This second individual often is responsible for recording the patient’s status on the sedation record and may assist with minor, interruptible tasks once the patient’s level of sedation and cardiopulmonary functions have stabilized, provided that adequate monitoring of the patient is maintained [59, 68, 101].
For deep sedation in the ED, a sedation provider, again, typically the emergency physician, with training in the pharmacology of the agents to be administered and skilled in pediatric advanced life support must be in the procedure room and is responsible for the procedural sedation–analgesia, including monitoring of the patient’s status. At least one clinician must be assigned to monitor and record the patient’s airway patency and cardiorespiratory status and, in contrast to moderate sedation planning, should have no other responsibilities during induction of sedation, the procedure, and the early postprocedure period when the patient is at greatest risk for respiratory depression, partial upper airway obstruction, and aspiration. If an experienced sedation provider has induced adequate sedation and will then perform the procedure, primary responsibility for monitoring the patient’s cardiopulmonary status may be designated to a second sedation-trained clinician, typically a registered nurse, if the responsible provider can easily interrupt performance of the procedure to assist with or assume management of adverse events. It should not be planned that the clinician monitoring the patient would assist with the procedure as that may distract this clinician from monitoring the patient’s vital signs and clinical status or interfere with rapid intervention [59, 67, 68, 101]. Brief, interruptible assistance with the procedure may be provided by this person but with caution and with assured concurrent attention to the patient’s vital functions. Safe use of deep sedation is dependent upon this clinician’s meticulous attention to the patient’s airway and breathing and anticipation and early recognition of adverse events. Threats to ventilation and oxygenation usually are easily managed when rapidly recognized and interventions immediately implemented. Experience with deep sedation has shown that some patients (~5–25%) will develop oxygen desaturation of <90% and partial upper airway obstruction, both of which are usually easily managed when rapidly recognized.
Since deeper-than-intended sedation may occur or be necessary in any patient, it is recommended that all but the lightest sedations (e.g., use of nitrous oxide) be staffed and monitored as if deep sedation may occur, particularly when gaining initial experience with sedation protocols or using agents with narrow therapeutic indices (e.g., propofol, midazolam + fentanyl, or etomidate). This usually means a third provider is needed if assistance will be necessary in performing the procedure. In addition, at least one provider should be present who is intimately familiar with location of resuscitation and other necessary medical equipment.
In most hospitals, physician sedation providers and nurses must be credentialed to administer PSA. Credentialing typically includes didactic sessions on use of specific PSA medications, demonstration of safe and effective administration of PSA, and competency in skills needed for rescue from adverse events [93].
-
(c)
Monitoring and equipment
Direct Patient Observation
In addition to electrophysiological monitoring, airway patency, rate and depth of respiration, and the child’s color (nail beds, mucosa) should be checked frequently by vigilant direct observation, especially after each medication administration and in the early postprocedure period when painful procedural stimuli have ended. This enables essential immediate interventions for adverse events such as marked respiratory depression, positional obstruction of the upper airway as muscle relaxation occurs (snoring, paradoxical chest wall motion without exhaled breaths may be noted), or vomiting. Opening of the airway by realignment or jaw thrust, applying painful stimulation to awaken and induce breathing, administering supplemental oxygen, or turning and suctioning to clear vomit often are usually all that is needed to correct problems that can otherwise rapidly deteriorate to life-threatening situations.
Direct monitoring during recovery should continue by a designated healthcare provider until the patient emerges to a level of moderate sedation; thereafter direct monitoring can be designated to the child’s parent or another responsible adult with the healthcare provider immediately available until the patient returns to the pre-sedation level of responsiveness [59, 68, 101].
Patients undergoing sedation should wear a loose-fitting top or hospital gown to ensure easy direct observation of the chest. The patient’s mouth and nose should not be obscured and skin should be visible for monitoring of color. A stethoscope should be immediately available.
For moderate sedation , in addition to direct observation, measurement of oxygen saturation by pulse oximetry is strongly recommended [59, 68, 101]. Additional continuous electrophysiological monitoring throughout sedation and recovery of ECG-based heart rates, respiratory rates, and noninvasive automated blood pressures measured after each medication bolus and/or every 5 min add further measures of safety.
For deep sedation , in addition to direct observation, routine use of noninvasive physiologic monitoring should include continuously measured oxygen saturation, heart rate , and respiratory rate and, in addition, noninvasive automated blood pressure measurements after each medication bolus and/or every 5 min throughout sedation and recovery [59, 68, 101].
Pulse oximetry has been demonstrated to detect hypoxemia well before cyanosis occurs and is therefore critical for monitoring for respiratory compromise. In one study of infants, O2 saturations were ≤ 83% before perioral cyanosis was detected by experienced emergency pediatricians [102]. Monitoring of oxygen saturation with pulse oximetry has been suggested as the most important means of reducing sedation-related injury and should be used for all but minimal sedations [59, 68, 70]. The pulse oximeter audible tone should be activated to alert providers to changes without the need to frequently read the monitor instead of observing the patient.
End-tidal CO 2 capnography provides breath-to-breath information on the effectiveness of ventilation . Assessment of ventilation by continuous end-tidal CO2 capnography has been found more sensitive than either direct observation or decreases in oxygen saturation in detecting respiratory depression or airway obstruction [103]. Changes in capnographic waveform and/or changes in end-tidal CO2 are frequently noted well before changes in oxygen saturation , including in patients’ breathing room air [103,104,105,106,107,108,109,110,111]. Problematically, the sedation provider must repeatedly observe the monitor screen to note the end-tidal CO2 waveform as, unlike pulse oximetry, there is no audible alert tone. Of note, no changes in end-tidal CO2 were found in children sedated with ketamine alone [110, 111].
Changes in end-tidal CO2 capnography can aid in early recognition of respiratory depression and/or airway obstruction and allow initial interventions that may avert the need to administer positive-pressure ventilations, e.g., limitation of further administration of sedative medications or opening of the airway. Assisted ventilation during oxygen desaturation due to apnea or periods of respiratory depression should be administered as needed. However, positive-pressure ventilation increases gastric pressures due to insufflation of air into the stomach. At a depth of sedation that induces apnea or significant respiratory depression, there is likely concurrent relaxation of esophageal muscle tone and significant blunting of protective airway reflexes. Thus, there is likely increased risk of pulmonary aspiration associated with positive-pressure ventilation due to gastroesophageal reflux into the oropharynx.
Routine administration of supplemental oxygen has been recommended to prevent hypoxemia during deep and moderate sedation [103]. However, sedation providers should recognize that administration of supplemental oxygen may delay oxygen desaturation for several minutes during respiratory depression or apnea [113]. Therefore, use of supplemental oxygen may delay recognition of these adverse events with their likely concurrent depression of protective airway reflexes, unless the patient is also monitored by end-tidal CO2 with capnography [115]. Similarly, recognition of airway obstruction is likely delayed [105,106,107,108,109, 112, 114, 116]. When capnography is unavailable, consideration should be given to monitoring patients by pulse oximetry as they breathe room air. Although an indirect and less-sensitive measure of ventilation than capnography, decreases in oxygen saturation alert the clinician to decreases in ventilation and facilitate interventions before hypoxemia and a need for positive-pressure ventilation occurs. With this strategy, administration of supplemental oxygen may be reserved for patients whose oxygen saturations drop below 90% without rapid rise in response to airway maneuvers such as head tilt/jaw thrust and/or stimulation. Respiratory depression is sufficiently commonplace during sedation with propofol that many providers recommend as routine administration of supplemental oxygen during propofol PSA [107, 108, 117].
Equipment
Resuscitation equipment must be immediately available. A self-inflating (Ambu-type) bag–mask positive-pressure device with a PEEP attachment and appropriately sized mask , continuous oxygen supply, and an airway suctioning device with a large rigid suction tip should be prepared for each sedation. Anesthesia-style CPAP bags, endotracheal intubation equipment, and resuscitation medications, with a dosing guide, including reversal agents such as naloxone and flumazenil, a paralytic agent such as succinylcholine , and antiepileptic and antiarrhythmic medications for drug-induced seizures and dysrhythmias should be immediately available for all sedations [59, 68, 70].
No suction apparatus can clear the oropharynx during active vomiting. The patient must be helped to turn or roll to the side or to sit upright to clear his airway. The suction device is used to clear residual emesis from the mouth after active vomiting has stopped . If the patient is unresponsive and emesis is noticed in the posterior pharynx or mouth, the patient should be rapidly rolled to the side to allow emesis to passively flow out as suctioning of the posterior pharynx is performed; there is significant risk for pulmonary aspiration in this situation.
Intravenous access adds an additional invasive procedure to the patient’s treatment, but it enables easily controlled and rapid titration of medications and provides an increased margin of safety by enabling rapid administration of reversal and resuscitation agents, if needed. When medications are administered intravenously, the intravenous access should be maintained throughout sedation and recovery. When medications are administered by a non-intravenous route (e.g., by intramuscular injection), whether to establish intravenous access should be decided on an individual basis. If vascular access is not established, the ability to immediately accomplish such must exist for all sedations, especially when a multiple drug sedation regimen is used. For agents that frequently cause hypotension (e.g., propofol), it is recommended that intravenous access be established with an indwelling catheter and maintained with a resuscitation fluid (lactated Ringer’s solution or normal saline). Patients who have been NPO for an extended period may benefit from an infusion of 10–20 mL/kg of LR or NS to counter any hypotensive effects of sedation medications. A stopcock near the hub of the IV catheter (e.g., on the tail of a T-connector inserted into the hub of the catheter and in line with the IV fluids) facilitates controlled and complete administration of sedation medications. This setup allows a syringe containing the sedative to be connected to the stopcock and the medication injected near the hub as the IV fluids infuse. This reduces the possibility of uncertain medication infusion amount and rate that might occur if the medication is added considerably upstream of the catheter hub. For agents such as ketamine that do not frequently cause hypotension, an indwelling “saline lock” is typically sufficient; the ketamine can be flushed into the bloodstream with 5–10 mL boluses of saline following ketamine administration.
A mnemonic some find helpful in preparing equipment is MS MAID: Machine Suction – Monitors Airway (oral airway, bag–mask, ETT, blade) IV Drugs.
Preparation for and Management of Adverse Events
Anticipation
The rarity of serious adverse events in ED PSA can lull the provider into complacency [116, 117, 132, 372]. It is suggested that the possibility of a life-threatening event during PSA should be thought of as inevitable, as a matter of “when” rather than “if.” Since these events are so infrequent and variations in individuals’ responses to a medication are not always predictable, the provider must always be prepared.
Effective management of adverse events begins first and foremost with preparation for the planned sedation. Thorough pre-sedation evaluation to identify patients at increased risk for adverse events or difficult airway management, monitoring and staffing based upon intended sedation depth, and immediate availability of resuscitation equipment and medications are critical. Factors associated with serious adverse outcomes include late recognition of hypoxemia and inadequate resuscitation, thus emphasizing the importance of preparation and continual monitoring during the sedation and recovery periods [101]. If recognized early , most adverse effects can be addressed effectively with relatively minor interventions. Stimulation, airway realignment, jaw thrust, and supplemental oxygen are usually all that is needed to avoid further deterioration to life-threatening events [117].
Management of Respiratory Depression and Apnea
Respiratory depression is one of the most common potentially serious effects of pediatric PSA [66, 118, 372]. A critical incident analysis of serious adverse outcomes in pediatric sedation found 80% initially presented with respiratory depression [97, 98]. Widespread use of pulse oximetry has since dramatically improved early recognition of respiratory depression. Agents commonly associated with respiratory depression include the sedative–hypnotics (barbiturates, benzodiazepines, chloral hydrate, propofol), particularly when used in conjunction with opioids [116, 117]. Apnea has also been rarely reported with administration of ketamine [120, 121].
Avoiding Respiratory Depression (See Also Basic Pharmacokinetics)
Most sedative medications variably blunt brainstem receptor response to increases in plasma levels of CO2. Since response to rising levels of CO2 determines breathing rate and depth, significant increases in sedative concentrations in the brainstem quickly lead to respiratory depression or apnea. The more rapidly a sedative drug is infused, the higher its initial brainstem concentration and the greater the respiratory depression. A primary strategy for reducing respiratory depression and maintaining adequate ventilation (and, in association, oxygenation) is slow administration of PSA drugs, often achieved by repeatedly infusing half or less of the total expected dose until the desired effect is achieved (titration). Ketamine can be an exception to the recommended slow administration approach because of its unique relative lack of respiratory depression. Taking advantage of first-pass kinetics, experienced sedators may choose to administer smaller doses rapidly for very brief procedures (see section “Ketamine”) [376].
At-Risk Periods
Patients may experience respiratory depression at any time during the sedation, but the greatest risks are immediately after medication administration and again after cessation of painful procedural stimuli [122].
Recognition of Ineffective Ventilation
As detailed previously, direct observation of the patient including general color and chest wall movement continues to be one of the most important means of recognizing respiratory depression and/or airway obstruction. The patient’s oropharynx and chest wall should be directly visible at all times to facilitate observation for lack of respiratory effort or respiratory effort without air exchange. In addition, pulse oximetry with audible tone and end-tidal capnography facilitate detection of ventilatory changes before they are clinically apparent.
Airway and Ventilation Maintenance
Initial management of hypoventilation may simply require verbal encouragement to the patient to breathe as his or her sensitivity to rising CO2 has been blunted by the sedation medications. Patients who have received opioids such as fentanyl may be awake but “forget” to breathe. Stimulation, painful if necessary, to arouse the patient may improve muscle tone and prompt breathing. If oxygen saturations are falling despite these maneuvers, supplemental oxygen administration and airway-opening maneuvers and/or positive-pressure ventilation may be necessary. See section below for management of “Upper Airway Obstruction.”
Treatment: Respiratory Depression and Apnea
When monitors alarm (e.g., indicating dropping oxygen saturation), ASSESS THE PATIENT. DO NOT presume the pulse oximeter probe slipped off, BP cuff inflating proximal to the probe, monitor malfunction, etc. Evaluate equipment later!
First Line (in Rapid Succession, If Needed)
-
1.
Verbally encourage or stimulate patient to breathe deeply (patients may require intensely painful stimuli, e.g., squeezing the fracture site or a hard sternal rub with knuckles); if insufficient, then do number 2.
-
2.
Reposition airway (chin lift/jaw thrust); if insufficient, then do number 3.
-
3.
Administer supplemental oxygen.
-
4.
If spontaneous ventilation continues to be inadequate, administer positive-pressure ventilation via bag–mask.
-
5.
If patient is on a continuous infusion (e.g., propofol)—slow down or stop medication infusion, and then do number 6.
-
6.
Call for help, if needed.
Second Line: Reversal Medications for Opioids and Benzodiazepines
If respiratory depression occurs after administration of an opioid or benzodiazepine and does not readily resolve after the above supportive measures, or requires continued positive-pressure ventilation, consider use of reversal agents. Slow, titrated reversal is preferred if positive-pressure ventilation is effective. The desired endpoint is lessening of the respiratory depression with slightly lighter sedation. Rapid, full reversal may lead to severe pain, hypertension, and agitation or seizure [123]. Reversal agents are rarely needed by experienced sedation providers.
Naloxone (Narcan®)
Indications
Opioid-induced apnea , respiratory depression, or “wooden/rigid chest syndrome” not responding to stimulation, airway-opening maneuvers, supplemental oxygen, and/or positive-pressure ventilations.
Dose
1–2 mcg/kg (0.001–0.002 mg/kg) IV push repeated every 1–3 min until the patient begins to have spontaneous respirations. Doses of 1–2 mcg/kg are recommended to “gently” reverse opioid-induced respiratory depression yet maintain analgesia. Larger doses , such as 10–100 mcg/kg, may awaken the patient and reverse the analgesic effects resulting in significant pain, hypertension, pulmonary edema, vomiting, or seizures [123].
During the interval of apnea, the patient is supported with assisted ventilations until adequate spontaneous respirations are restored. Thereafter, the patient is observed closely as the reversal effects of naloxone may be briefer than the opioid-induced respiratory depression . For “wooden chest syndrome,” if the patient cannot be ventilated and oxygen saturations are dropping rapidly, naloxone may be given in 1 or 2 mg boluses for convenience. Alternatively, succinylcholine 1–2 mg/kg may be used to paralyze the patient.
Caution
Opioid-induced respiratory effects may outlast the duration of naloxone, and patients must be closely monitored for recurrence of respiratory depression, typically at least 2 h after naloxone administration [123, 124].
Flumazenil (Romazicon®)
Indications
Benzodiazepine (e.g., midazolam)-induced apnea or respiratory depression not responding to stimulation, airway-opening maneuvers, supplemental oxygen, and/or positive-pressure ventilation.
Dose
0.01–0.04 mg/kg (maximum 0.5 mg) IV over 30 s. Repeat every 60 s to desired response. A cumulative dose of 3 mg may be necessary. Flumazenil may reverse midazolam-induced hypnotic and amnestic effects but may not reverse ventilatory depression [127]. When appropriate, naloxone should be used as the first line in reversal therapy. Drug therapy does not obviate the need to protect the airway and support ventilation.
Caution
Flumazenil may cause seizures in patients chronically on benzodiazepine medications and should be used cautiously in patients on medications that can lower seizure threshold. Also, benzodiazepine-induced respiratory effects may outlast the duration of flumazenil, and patients must be closely monitored for recurrence of respiratory depression, typically at least 2 h after flumazenil administration [126, 127]. Recurrence of sedation has been reported in up to 7% of cases, most commonly in children under 5 years of age [126] (Table 22.5).
Upper Airway Obstruction
The pediatric airway is particularly prone to dynamic obstruction due to the relatively large size of the tongue and tonsillar tissues. As sedation depth increases, the muscles of the tongue, jaw, and oropharynx lose tone in a manner similar to deep sleep. Sedation-induced “obstructive sleep apnea” may result in partial or complete airway obstruction, exacerbated by the supine position and nasal passage obstruction. A history of snoring or obstructive sleep apnea alerts the clinician to the increased likelihood of this occurrence. Placement of a shoulder roll in infants and a head roll in older children and adolescents to align the oropharynx, posterior pharynx, and trachea may help align the patient’s airway and relieve this obstruction. Markedly, obese patients also may benefit from a large head or shoulder roll to compensate for their large trunk.
A jaw thrust or chin lift may be necessary to open the upper airway by pulling the tongue and related muscles away from the posterior pharynx. Patients who are very deeply sedated or have inadvertently reached the depth of general anesthesia may benefit from placement of an oro- or nasopharyngeal airway, but because oropharyngeal airways may induce a gag reflex and vomiting, these devices should be used with caution. Laryngospasm is a special type of upper airway obstruction and is addressed later in this chapter.
At-Risk Periods
Positional airway obstruction may occur at any time during sedation but, in association with respiratory depression, it may more likely be shortly after medication administration or after the painful procedural stimulus has ended.
Recognition of Upper Airway Obstruction
Signs of partial upper airway obstruction include stridor or noisy breathing. Paradoxical chest wall movement (sucking in of the chest and distention of the abdomen with inspiration) may be seen with partial or complete obstruction. Hypoxemia is a late sign. An obstructive pattern is seen on capnography well before changes in oxygen saturation and allows early detection of airway obstruction (or apnea).
Treatment
-
1.
Align airway and open with chin lift or jaw thrust; provide supplemental oxygen as needed.
-
2.
Suction airway if excessive secretions are present.
-
3.
If not responding to repositioning, consider continuous positive airway pressure (CPAP) with bag–mask (CPAP or anesthesia-type bag is preferable to self-inflating-type bag as CPAP can be delivered more effectively to open the airway by distending the posterior pharynx).
-
4.
If having difficulty maintaining an open airway, consider an oral airway (unconscious patient) or nasal airway.
-
5.
If unable to ventilate with CPAP, rapidly consider treatment for laryngospasm with succinylcholine.
Laryngospasm
Laryngospasm is an uncommon but potentially life-threatening sedation-related adverse event. It is a partial or complete upper airway obstruction, with oxygen desaturation, caused by involuntary and sustained closure of the vocal cords and is not relieved by routine airway repositioning maneuvers, suctioning, or insertion of a nasal or oral airway. Laryngospasm may be intermittent or sustained and brief or prolonged [133, 136].
The incidence of laryngospasm during pediatric ED PSA is difficult to determine as it is a rare event, estimated to occur in 1–3/1000 sedations [117, 137, 372]. Relative preservation of upper airway protective reflexes during ketamine-based sedation reduces the risk of pulmonary aspiration and thus makes ketamine one of the safest agents for ED PSA in unfasted children, yet, paradoxically, ketamine PSA may have increased risk for laryngospasm [133,134,135]. A meta-analysis of pediatric ketamine-based ED PSA found an incidence of laryngospasm of 0.3%; the only identifiable association with increased risk of laryngospasm was an initial intravenous dose of greater than 2.5 mg/kg, but data was unable to be analyzed for associations with URI, wheezing, or other risk factors found to be associated with increased risk during general anesthesia [137]. Of particular interest, young age and oropharyngeal procedures (excluding endoscopy) were not associated with increased risk, but prospective larger data sets are needed to better clarify these risks.
Laryngospasm in almost 50,000 non-intubated children undergoing elective propofol sedation/anesthesia was noted to occur at a rate of 21/10,000 (0.2%) [86]. Laryngospasm associated with general anesthesia has been estimated as high as 14% in younger children and as low as 0.1%, with lower likelihood reported in non-intubated children [138, 139]. The wide variability may be due to differences in definition and study design, patient populations, anesthetic techniques, and airway manipulation [140]. However, consistently noted risk factors for laryngospasm with general anesthesia include young age, upper respiratory infection, asthma, manipulation of the airway, and exposure to smoking in the home [141, 142].
It is unclear whether prophylactic administration of atropine or glycopyrrolate with ketamine to reduce hypersalivation reduces the risk of laryngospasm [143, 144]. The meta-analysis of pediatric ketamine-based ED PSA, noted earlier, found that overall airway and respiratory adverse events (but not laryngospasm) were actually increased in children who received concurrent anticholinergics [137]; this unexpected association was also found in a later report on 22,645 ketamine sedations [377].
At-Risk Periods
Laryngospasm may occur at any time during sedation, including recovery. In one report of non-intubated children undergoing sedation/general anesthesia, laryngospasm occurred most frequently during emergence (48%) but was also seen during induction (29%) and maintenance (24%) phases [139]. Increased risk for ketamine-related laryngospasm may occur in children with current URI, especially if febrile, if secretions/emeses pool in the posterior pharynx, or if a procedure such as endoscopy stimulates the gag reflex [142, 145, 146].
Recognition of Laryngospasm
Early signs of laryngospasm may include coughing. A characteristic stridulous noise can be heard with partial laryngospasm. Chest wall movement is noted, but there is a mismatch between the patients’ respiratory effort and the small amount of air exchange. If complete laryngospasm occurs, no stridulous noise will be heard and no air exchange or breath sounds will be noted despite chest wall movement. No ventilation with a bag–mask device will be possible.
Oxygen saturations will drop rapidly if the patient is breathing room air, typically within 30–60 s. If the patient has been preoxygenated, saturations may remain above 90% for 1–5+ min, dropping more rapidly in younger children and infants [112]. Capnographic changes are a very sensitive means of diagnosing laryngospasm. During partial laryngospasm, turbulence affects expiratory flow, but the amplitude of the capnogram will correlate with the extent of hypoventilation. During complete laryngospasm the CO2 waveform will be lost despite chest wall movement [108] (Fig. 22.2).

Laryngospasm treatment algorithm. (Modified for sedation from Hampson-Evans et al. [136], with permission from John Wiley and Sons)
If the patient develops stridor during sedation:
-
1.
Remove stimulus to posterior oropharynx; consider gentle suction of excessive secretions and emesis.
-
2.
Reposition airway with jaw thrust; vigorous, painful intrusion of the thumbs in the laryngospasm notch may help.
-
3.
Apply CPAP (continuous positive airway pressure) with 100% O 2 with anesthesia-type bag–mask; CPAP may reduce partial obstruction by distending the posterior pharynx, which exerts pull to open the partially closed larynx and vocal cords.
-
4.
Assess air movement, if unable to oxygenate with CPAP.
-
5.
Rapidly consider atropine 0.02 mg/kg IV followed by low-dose succinylcholine (0.1–0.25 mg/kg IV) with ventilatory support as needed [147]; consider an additional dose of propofol if propofol sedation is underway.
-
6.
If still unable to oxygenate, administer full-dose succinylcholine (1–2 mg/kg IV or 3–4 mg/kg IM) followed by intubation.
Attempts to provide intermittent positive-pressure ventilation with a face mask may distend the stomach and make subsequent ventilation more difficult. In complete laryngospasm CPAP may worsen the obstruction by forcing the area just above the false cords closed. Therefore, if complete spasm cannot be broken, early IV agents should be considered [136].
When laryngospasm occurs in the midst of propofol PSA, deepening the sedation with administration of an additional 0.5 mg/kg of propofol has been shown to be an effective treatment for laryngospasm [148]. Transient apnea with this technique should be anticipated.
Low-dose succinylcholine (0.1 mg/kg IV) may be effective in relaxing laryngospasm [147]. Onset of neuromuscular blockade is generally more rapid at the larynx compared with the peripheral muscles [149]. Relaxation of the larynx induced with this small dose will be brief but may allow the patient to be oxygenated by CPAP and intubation avoided. Alternatively, administration of a fully paralyzing dose (1–3 mg/kg IV) followed by intubation should be considered if the patient is rapidly becoming severely hypoxic [136]. The intravenous route is preferred for administration of succinylcholine, but if there is no vascular access, it can be administered intramuscularly at a dose of 3–4 mg/kg. Although full effect may take about 4 min, onset of relaxation of the larynx occurs earlier than maximum suppression of the muscle twitch response and enables ventilation [150].
Succinylcholine administration following hypoxia may be associated with severe bradycardia and even cardiac arrest. Atropine 0.02 mg/kg IV administered prior to succinylcholine is recommended [151].
Emesis
Nausea and vomiting occur in 5–25% of children during or after ED PSA. Use of opioids before or during sedation increases the likelihood of vomiting [88, 152], whereas concurrent use of midazolam with an opioid [9], ketamine [87], or nitrous oxide [10] reduces the incidence of PSA-related vomiting. Propofol appears to be less emetogenic and may not benefit from addition of midazolam to the regimen. Coadministration of ondansetron (Zofran®) with ketamine reduces vomiting both in the ED and after discharge [92]. However, ondansetron does not reduce emesis when given with nitrous oxide/fentanyl [430]. Children with a history of prior postoperative nausea and vomiting or with a history of motion sickness are at increased risk for vomiting [153]. Further investigations are needed to better predict sedation-associated nausea and vomiting and to determine strategies to significantly reduce this relatively minor but very undesirable adverse effect.
At-Risk Periods
Emesis may occur at any point during procedural sedation but most commonly is seen during the postprocedure recovery period [9, 10, 88]. Since emesis can occur at any point and with every systemic agent used for procedural sedation, the provider responsible for monitoring the patient’s airway should always be vigilant for signs of impending retching and prepared to turn the patient to the side to clear the airway. Suction equipment should be prepared and immediately available during and after all sedations. This equipment is used to finish clearing the emesis from the mouth after the patient stops vomiting. It is also advisable to have a large emesis basin at the bedside during each ED PSA.
Treatment: Emesis During Procedural Sedation
-
Position patient’s head to side, allow patient to clear own mouth during active vomiting, and suction oropharynx with rigid large bore Yankauer-type suction tip.
-
If using nitrous oxide, immediately remove the mask to allow clearing of emesis and discontinue nitrous, at least temporarily. Some providers prefer to allow the patient to hold the face mask during sedation with nitrous oxide so that the patient can immediately remove the mask if feeling nauseated.
Ondansetron (Zofran®)
An anti-serotonin agent, ondansetron is not routinely administered to prevent emesis during ED PSA. However, one study of children receiving ketamine for ED PSA showed that vomiting in the ED or after discharge was less frequent with ondansetron coadministration: 8% versus 19%, with nine patients needing to be treated to prevent one episode of vomiting [92]. A randomized trial of ondansetron in children undergoing nitrous oxide with intranasal fentanyl sedation , however, did not find a reduction of emesis [430]. Ondansetron also may be considered in a child with significant prior history of postoperative nausea and vomiting. Further evaluation of the effectiveness of this antiemetic agent during ED PSA is needed. Other antiemetic agents such as prochlorperazine (Compazine®) and promethazine (Phenergan®) usually are not used because of sedating effects and increased risk for causing dystonic reactions.
Dose
IV, PO; 0.1–0.15 mg/kg, maximum dose 4 mg. Rapidly dissolving 4 mg oral tabs (ODT) are available and can be split in half for easy administration to young children. Dosing can be simplified by administering ondansetron ODT 2 mg to children 3 years of age and younger and 4 mg to children 4 years of age and older.
Cautions
May rarely cause bronchospasm, tachycardia, headaches, and lightheadedness. Life-threatening torsades de pointes has been reported with very large (32 mg) intravenous doses; ondansetron should not be given to patients with prolonged QT intervals [465].
Not Requiring Patients to Drink Fluids Prior to Discharge Also May Reduce Vomiting
Historically, assuring patients can drink prior to discharge has been done to prevent postoperative “dehydration.” Given shortened fasting times and the common practice of administration of IV fluids during sedation, the risk of dehydration is low compared to the risk of inducing vomiting [101, 152].
Pulmonary Aspiration
Clinically significant or life-threatening pulmonary aspiration of gastric contents during pediatric procedural sedation is extremely rare. Aspiration occurs in approximately 0.1% of cases under general anesthesia and was noted to have occurred in 4 of 49,836 children undergoing elective propofol sedation/anesthesia, but it has not been reported in association with ED PSA [72, 73, 77, 78, 86]. Patients with ASA physical status Class III or higher and those requiring intubation are likely at higher risk. Risk for aspiration is likely greater, too, in patients who experience brief periods of apnea or significant respiratory depression as esophageal tone and protective airway reflexes may be absent during these periods and gastric contents may reflux into the trachea with little or no initial patient response. Because of the potential gravity of this adverse event, it is suggested clinicians consider using ketamine or nitrous oxide that better preserves protective airway reflexes or, when possible, lighter sedation combined with local anesthesia for non-fasted emergency patients [79].
Recognition
Clinical symptoms of pulmonary aspiration may include cough, crackles/rales, decreased breath sounds, tachypnea, wheeze, rhonchi, and respiratory distress that were not present before the sedation and present before the end of the ED recovery phase. These are usually accompanied by a decrease in oxygen saturation from baseline , requiring supplemental oxygen, and, if obtained, focal infiltrate, consolidation, or atelectasis on chest radiograph [132]. As noted previously, clinically significant pulmonary aspiration may more likely occur in the unresponsive patient when gastric contents passively flow out of the stomach to the larynx. As the aspiration occurs, there may be little or no immediate signs due to the depth of sedation/anesthesia. The aspiration may become evident as the patient emerges from sedation.
Treatment
If emesis is seen, turn patient to side, allow to retch, and suction posterior pharynx as needed. Administer supplemental oxygen by nasal cannula or mask as needed. Many cases of transient hypoxia will resolve with this simple maneuver. CPAP may improve oxygenation in cases of severe aspiration with alveolar collapse. The majority of children who experience pulmonary aspiration require only close observation and simple supportive care with supplemental oxygen with or without CPAP and recover without sequelae [72, 73, 80, 86]. Endotracheal intubation should be considered if definitive protection of the airway or tracheal suctioning is required; RSI (rapid sequence induction) may be necessary. Uncommonly, severely symptomatic patients may need to be taken to the OR for emergent bronchoscopy with bronchial lavage of particulate matter. Arrange for appropriate continued monitoring, support, and work-up as needed including chest radiograph. For symptomatic patients, this usually means inpatient admission to an intensive care unit.
Medications
Basic Pharmacokinetics: Simplified
Parenteral drugs effective for PSA are small, hydrophobic lipophilic compounds that rapidly diffuse out of the bloodstream into the lipophilic tissues of the brain and spinal cord where they cause sedation/anesthesia.
Since the brain receives a disproportionately high percentage of the cardiac output (15–25%) [155], a large portion of a sedative drug injected into the bloodstream circulates on first-pass out of the heart into the brain’s circulation and quickly crosses the blood–brain barrier to exert its clinical effects within a single circulation time (first-pass or “one arm–brain” kinetics). As the drug circulates throughout the body and diffuses into muscle, bone, and, at a slower rate, poorly perfused fat, the blood plasma concentration falls. The concentration gradient between the brain and the blood then favors drug diffusion out of the brain. As the brain’s drug concentration falls, the drug effect lessens. This secondary reequilibration (“biphasic redistribution”) causes the patient to awaken or respiratory depression to lessen. These effects are relatively independent of metabolic clearance of the drug from the body. PSA drugs’ metabolic half-lives tend to be on the order of hours, whereas their sedative effect half-lives or “wake-up times” are on the order of minutes [155].
The duration of action of a single intravenous dose is similar for all these anesthetic/hypnotic drugs and is determined by redistribution of the drugs out of the brain. However, after repeated doses or prolonged infusions, a drug’s duration of action is determined by complex interactions between the rate of redistribution of the drug, the amount of drug accumulated in fat, and the drug’s metabolic clearance. The wake-up time of some drugs such as etomidate, propofol, and ketamine increases only modestly with prolonged infusions, while others such as diazepam and thiopental increase dramatically and midazolam less so [155].
A rapidly injected drug travels as a more concentrated bolus on the first-pass out of the heart into the brain circulation than a slowly injected drug that is diluted by the passing blood. Thus, with rapid infusion , the initial concentration gradient between the plasma and the brain is greater. Consequently, the brain’s concentration of the drug rises more rapidly, and a greater portion of the administered dose enters the brain with resultant deeper sedation than when the same drug dose is slowly infused.
Thus, small doses of medications can have significant clinical effect if administered rapidly. Since the blood–brain concentration gradient also reverses more rapidly with these smaller doses, “wake-up” time may be shorter, making this strategy beneficial for brief procedures. Importantly, however, clinicians must be aware that rapid changes in the brainstem’s concentration of opioid and sedative drugs markedly increase the potential for respiratory depression and apnea. As a practical point, this technique can be used only for ketamine administration because it causes markedly less respiratory depression than opioid and GABAergic drugs [376] (Fig. 22.3).

Plasma drug concentration and CNS drug concentrations and effects after a single IV dose
A drug’s therapeutic window is used to describe the difference between the dose of that drug that results in the desired sedative or analgesic effect and the dose that results in adverse effects. A drug with a wide therapeutic window has a greater margin of safety for use for ED PSA. For example, accidental administration of a tenfold greater-than-intended dose of ketamine will likely result in prolonged recovery but relatively little cardiopulmonary depression [157], whereas the same error with propofol will result in apnea and hypotension [156].
Many reasonable medication options exist for ED PSA [95, 159]. Use of analgesic medication when pain is the primary cause of distress is the key, and balancing analgesia with anxiolysis makes sedations more pleasant for patients. For nonpainful procedures when immobility is the primary objective, sedative–hypnotic medications may be chosen. It is recommended that the clinician initially become familiar with a few specific agents or combination of agents that provide the desired effects of analgesia, sedation, and/or anxiolysis. Limiting one’s experience to a few agents better enables one to anticipate and manage adverse effects and events associated with those agents. One’s pharmacologic armamentarium then can be gradually increased and refined with tailoring of regimens to a specific patient’s characteristics. The following section summarizes medication effects and pharmacology in healthy children. Abnormalities in renal and hepatic function can significantly alter these parameters, particularly the duration of effects. In addition, significant variability in effect may occur between individuals due to genetically determined factors such as differences in drug receptor sites, metabolic activation, or clearance. Patients with ASA physical status Class III and higher also have less physiological reserves and therefore are more likely to have adverse effects with smaller doses.
Dosing Details
Titration to Desired Effect
Careful intravenous “titration” of medications using repeatedly administered small doses to achieve the desired clinical effect enables the practitioner to use the smallest effective dose and reduce the peril of oversedation with its increasing risks of respiratory depression and aspiration and, furthermore, hasten recovery [59, 69, 96, 160]. Individual variation in sensitivity to the medication can also be detected; thus a smaller-than-expected dose may be found adequate for a given individual.
Knowledge of the time to peak effect of the specific medication is necessary to avoid “stacking” of doses when first gaining experience with titration. That is, if, to achieve deeper sedation, a subsequent dose is administered before the peak effect of the preceding dose has occurred, deeper-than-intended sedation can easily occur. For example, morphine has a peak effect of approximately 10 min. If an additional dose of morphine is administered after 5 min because the patient is still in significant pain, by 15 min after the original dose, when both the first and second doses are near peak effects, the patient may have significant respiratory depression due to an excessive accumulative dose. For this reason, titration is difficult with drugs that have longer than 1–3 min to peak effect time.
When a “typical” total dose for a specific procedure is known, that total dose may be divided and the increments administered at intervals shorter than “the time to peak effect” without likely overshoot. This strategy of repeated administration of fractional doses for fixed dose protocols—e.g., half of the anticipated total dose administered twice with administration separated by a short interval—reduces the risk for significant respiratory depression induced by some agents such as the combined technique using fentanyl and midazolam. This approach is suggested for providers who have less experience with a specific medication.
Intravenous Administration at the Hub
Injecting medications at or near the hub of the indwelling venous catheter allows one to know more precisely when the drug enters circulation and when the entire dose has been administered. This can avoid unintended continued infusion of residual drug in the intravenous tubing when adverse effects are occurring.
Intramuscular Administration
While IM administration avoids the need for placement of an IV catheter, it still requires a feared needlestick and makes titration to effect difficult. More importantly, if a serious adverse event occurs (e.g., severe laryngospasm), an emergent IV for resuscitation medications or fluids may be difficult to place. Specifically, ketamine-administered IM has been shown to be effective in achieving sedation. However, the IM route requires either use of a dose large enough to sedate all children—e.g., 4 mg/kg, which will oversedate some and result in greater frequency of adverse events [137]—or painful repeat administration of a smaller dose if the original dose is insufficient. Since the onset of IM ketamine is 5–15 min, titration without oversedation is difficult. Due to the large dose typically administered IM, recovery is prolonged [161].
Sedative–Hypnotic Agents
Commonly used sedative–hypnotic medications for procedural sedation include barbiturates, chloral hydrate, propofol, and etomidate. These drugs induce general depression of the central nervous system (CNS) by stimulation of inhibitory gamma-aminobutyric acid (GABA) receptors or other mechanisms that are not yet fully elucidated. None of these drugs have an analgesic effect. While deeply induced sedation (e.g., with propofol) may enable painful procedures to be accomplished, lighter sedation with less respiratory depression may be facilitated by the addition of an analgesic agent as described in subsequent sections. This chapter will review the common sedatives used in the ED with particular focus on their clinical applications and supporting literature from the speciality.
Chloral Hydrate [76]
Indications
Chloral hydrate is a sedative hypnotic drug that may be used to provide ED PSA in children less than 2–3 years of age, including those with congenital cardiac anomalies and who are undergoing painless diagnostic studies such as CT or MRI scans, ECHOs, eye exams, and locally anesthetized facial lacerations [154, 382,383,384,382]. Sedation is achieved in >80% of young children with an oral dose of 50–75 mg/kg. Chloral hydrate should not be considered a first-line agent in children older than 48 months because of decreased efficacy as compared with younger children. The drug may be administered orally or rectally. The oral preparation has a bitter taste that frequently requires administration in a flavored vehicle to disguise its taste; approximately a third of children may vomit soon after oral administration.
Contraindications/Cautions/Adverse Effects
Children receiving chloral hydrate should be properly monitored and managed by appropriately trained personnel due to the risk of respiratory depression and hypoxia. Chloral hydrate should not be used in children with neurodevelopmental disorders due to an increased incidence of adverse effects and decreased efficacy as compared with healthy children. Chloral hydrate has the potential for resedation and may produce residual effects up to 24 h after administration. The elimination half-life is age-dependent, with much longer effects in infants. These effects may occur long after the procedure is finished; reports describe infant deaths due to slumping in car seats and other causes of obstruction of the airway after discharge [383]. Many infants may have unsteady gait, hyperactivity, or irritability the day after sedation. Other adverse effects include respiratory depression, hypotension, paradoxical excitement (0–15%), vomiting (10–30%), and, rarely, hepatic failure, areflexia, jaundice, gastrointestinal hemorrhage, and esophageal stricture [76, 162, 163]. These disadvantages along with its highly variable effects on older children and inherent difficulty with titration of oral medications make this agent less than ideal for children older than 1–2 years of age. Interestingly, children who have been fasted may have increased PSA failure rates.
Pregnancy Category C
-
Dose: PO or PR; 50–125 mg/kg; typical initial dose 75 mg/kg. A second dose may be given, if needed, to a maximum of 2 g or 100–125 mg/kg total dose.
-
Onset/duration: sedation within 30–60 min, recovery by 60–120 min.
-
Mechanism of action: halogenated hydrocarbon with sedative–hypnotic but no analgesic effects.
-
Metabolization: rapidly metabolized by hepatic alcohol dehydrogenase to its active compound trichloroethanol and subsequently excreted in the urine [155]. The elimination half-life is age-dependent: 40 h in preterm infant, 28 h in term infant, and 6–8 h in toddler.
Barbiturates
Barbiturates are pure sedatives with no analgesic effect. They potentiate the effect of GABA, the principal inhibitory neurotransmitter in the CNS, by binding to the GABAA receptor and prolonging the open time of the membrane chloride ion channel. In addition, barbiturates block the excitatory AMPA receptor [155]. Barbiturates have been used in the ED for painless radiological procedures such as CT and MRI scans. Newer rapid CT scans do not require prolonged motionlessness, and new medications with fewer adverse effects have become available for MRI scans; thus, barbiturates are now less frequently used for ED procedural sedation.
Methohexital (Brevital®)
Indications
Methohexital administered by either the intravenous, intramuscular, or rectal route can provide effective sedation for children undergoing painless diagnostic studies such as CT or MRI scans [384]. However, because of the readily induced respiratory depression associated with this medication, methohexital has not been used or studied extensively for procedural sedation in children, and thus its use should be considered only by experienced and knowledgeable clinicians.
Adverse Effects
Respiratory depression and apnea are dose- and infusion rate-dependent and are readily induced with intravenous administration but may occur with any route of administration. Hangover-like residual effects may last for 24 h.
Pregnancy Category B
-
Dosages: 1 mg/kg IV, 10 mg/kg IM, 25 mg/kg PR.
-
Onset/duration:
-
Mechanism of action: ultrashort-acting , highly lipid-soluble barbiturate with rapid CNS uptake and redistribution. It has marked sedative–hypnotic but no analgesic effects.
-
Metabolization: Hepatic degradation with renal excretion results in an elimination half-life of 3.5 h and less accumulation of drug in body tissues compared to other barbiturates.
Pentobarbital (Nembutal®)
Indications
Pentobarbital is a short-acting barbiturate that induces relative immobility and can be safely used to sedate children to facilitate nonpainful diagnostic studies such as CT and MRI scans; redundant but supportive measures may include head positioning, supplemental oxygen, and occasional bag–valve–mask ventilatory support [159]. Pentobarbital successfully sedates >97% of children for CT or MRI scans with higher success rates in children younger than 8 years of age [167,168,169, 206]. Pentobarbital is more effective in providing sedation than midazolam [170] or etomidate [171] and causes fewer adverse respiratory events than propofol [172]. The addition of midazolam with pentobarbital does not appear to increase success rates and prolongs time to discharge [168].
Oral pentobarbital (4 mg/kg) has been found similar to oral chloral hydrate (50 mg/kg) in time to sedation and length of sedation; overall adverse event rate, including oxygen desaturation , was slightly lower with pentobarbital (0.5%) than with chloral hydrate (2.7%) [173, 174]. Of note, a database review found infants younger than 12 months of age sedated for elective CT or MRI with PO pentobarbital (4–8 mg/kg) had comparable effectiveness and fewer respiratory complications compared with IV pentobarbital (2–6 mg/kg); time to sedation was slightly longer with PO than with IV pentobarbital (18 versus 7 min), but time to discharge (~1 h 45 min) was similar. Total adverse event rate was similar (0.8% [PO] versus 1.3% [IV]), but oxygen desaturation was slightly more frequent for IV (0.2% [PO] versus 0.9% [IV]). Sedation effectiveness was comparable (99.5% [PO] versus 99.7% [IV]), leading the author to recommend consideration of PO administration for this age group, even when an IV is in place [175]. In a randomized comparison of IV pentobarbital (maximum 5 mg/kg in incremental doses) or oral chloral hydrate (75 mg/kg) prior to MRI, children who received pentobarbital had a higher incidence of paradoxical reaction (14% versus 9%) and prolonged recovery with a similar failure rate [174].
Adverse Effects
Respiratory depression is dose- and infusion rate-dependent and is generally less than that seen with equivalently sedating doses of opioids or chloral hydrate [173, 174, 176]. Mild respiratory depression is usually seen at doses required for hypnotic effect. The following adverse events and frequencies have been reported: transient respiratory depression with oxygen desaturation of ≥10% below the baseline in 1–8%; vomiting in ≤1% [168, 177, 178]; increased airway secretions, airway obstruction, coughing, and bronchospasm [168,169,170, 174, 179]; emergence reactions (hyperactivity in 5–7%) [178, 179] of 8.4% in children older than 8 years [179]; and paradoxical reaction (sustained inconsolability and severe irritability and combativeness for more than 30 min) in 0.01% with oral pentobarbital [174] and in 1.5% with intravenous pentobarbital [169]. Up to 35% of children will have increased sleeping or hangover-like effects in the 24 h following pentobarbital sedation [174, 179]. Pentobarbital should be avoided in children with porphyria.
Pregnancy Category D
-
Dosages:
-
IV (protocol used by author): first dose, 2.5 mg/kg; if needed, subsequent doses, 1.25 mg/kg, may repeat × 3 to maximum of 7.5 mg/kg or 200 mg maximum.
-
IM: 2–6 mg/kg, to a maximum of 100 mg.
-
PO or PR (<4 years): 3–6 mg/kg, to a maximum of 100 mg.
-
PO or PR (>4 years): 1.5–3 mg/kg, to a maximum of 100 mg.
-
-
Onset/duration: The onset of action is related to the route of administration and subsequent absorption. The duration of hypnotic effect is dependent upon redistribution with recovery occurring within 50–75 min after IV or IM administration, even though the biologic half-life in plasma is 15–20 h [176].
-
Mechanism of action: short-acting barbiturate with sedative–hypnotic but no analgesic effects; it induces relative immobility through nonselective depression of the CNS via facilitation of GABA receptors.
-
Metabolization: hepatic degradation with elimination half-life 15–20 h [176]. This may explain why many parents note it may take their children up to a day to return to normal behavior.
Anxiolytic–Amnestic–Sedative Agents
Benzodiazepines
Benzodiazepines produce a range of hypnotic (sedative), anxiolytic, amnestic, anticonvulsant, and muscle relaxant effects via modulation of the GABAA receptor, the most common inhibitory receptor within the brain. The GABAA receptor is composed of five subunits, each of which has multiple subtypes. The varying combinations of subunit subtypes result in different pharmacological and clinical effects (Table 22.6). When benzodiazepine binds to its site on the GABA receptor, it causes the receptor to have a much higher affinity for the GABA neurotransmitter. This results in the associated chloride ion channel opening more frequently, causing the neuronal membrane to become hyperpolarized. Benzodiazepines have no analgesic effect. Benzodiazepines administered without other medications rarely cause severe adverse effects [180]. However, when benzodiazepines are combined with other drugs such as opiates, marked respiratory depression and apnea can readily occur [96]. Midazolam (Versed®) and diazepam (Valium®) are commonly used benzodiazepines for procedural sedation because of their shorter duration and potent anxiolytic and amnestic effects.
Paradoxical Reactions
Severe behavioral changes, typically during recovery, resulting from benzodiazepines as well as barbiturates have been reported including mania, anger, and impulsivity. Individuals with borderline personality disorder appear to have a greater risk of experiencing severe behavioral or psychiatric disturbances from benzodiazepines. Paradoxical rage reactions from benzodiazepines are thought to be due to partial deterioration from consciousness, generating automatic behaviors, fixation amnesia, and aggressiveness from disinhibition with a possible serotonergic mechanism playing a role [181, 182]. In the context of ED PSA, parents should be forewarned about the possibility of excitability, increased anxiety, and agitation in response to midazolam. Recommendations for management of this adverse effect include protecting patients from self-harm while allowing further recovery, deepening sedation with fentanyl or diphenhydramine or administration of caffeine [181, 183].
Midazolam (Versed®)
Indications
Midazolam is a water-soluble benzodiazepine that induces anxiolysis and mild sedation. Most children will not fall asleep with midazolam alone, even at higher doses. Consider another agent or combine with another agent (e.g., pentobarbital) if procedure requires patient to remain motionless (e.g., MRI scan). Midazolam has more potent amnestic effects, quicker onset, and shorter duration of action compared to diazepam [184,185,186,187]. Since it is water soluble, midazolam can be administered intramuscularly, as well as PO, IV, or intranasally (IN). Midazolam may be used for seizure control, but longer-lasting agents such as lorazepam are typically used. Midazolam also has antiemetic effects, an additional benefit when coadministered with opioids or ketamine [188].
Intranasally administered midazolam, 0.4–0.5 mg/kg, using an atomizer and a volume of 0.2–0.5 mL, results in mild sedation and anxiolysis with few adverse reactions in many young children undergoing laceration repair [100, 189,190,191, 249, 459, 467, 468]. For brief CT scans in infants and toddlers, only 30% were sedated sufficiently using a dose of 0.5 mg/kg [385]. IN midazolam 0.2 mg/kg combined with IN fentanyl 2 mcg/kg was found effective and with minimal minor adverse effects during laceration repair in young children [394]. Onset of mild sedation occurs within 4–5 min and peak sedation 20–25 min. The author experience is that IN midazolam works better if administered before the young child becomes upset. Use of a mucosal atomizer decreases the burning sensation of IN midazolam . Some providers administered a small dose of intranasal lidocaine to minimize the discomfort of IN midazolam [467].
Contraindications/Cautions/Adverse Effects
Midazolam causes minimal hemodynamic effects (mild hypotension with compensatory tachycardia), but dose- and infusion rate-dependent respiratory depression and apnea occur when midazolam is administered in concert with opioids [96]. An important adverse reaction to benzodiazepines in children is the disinhibitory reaction, possibly mediated by central cholinergic mechanisms [181]. Paradoxical excitement or dysphoria during recovery may be increased in older children when midazolam is coadministered with ketamine [87].
Pregnancy Category D
-
Dosages:
-
IV/IM: anxiolysis, 0.05 mg/kg IV with maximum of 2 mg; sedation, 0.1 mg/kg IV with maximum of 5–10 mg. If titrating to effect, administer doses at 3 min or greater intervals to avoid stacking effects. However, the anticipated dose (e.g., 0.1 mg/kg) may be divided and administered at 1–2 min intervals to reduce respiratory depression.
-
PO: 0.2–0.75 mg/kg.
-
IN: 0.2–0.4 mg/kg (use 5 mg/mL IV solution to reduce volume, use atomizer, or drip slowly); more rapid onset and shorter duration than oral. When administered with an atomizer device, this technique achieves mild to moderate sedation. If the intravenous solution is dripped into the nares without atomization, most children complain of a burning sensation.
-
PR: 0.3–0.5 mg/kg, may not be preferred by older children [192, 193].
-
-
Onset/duration:
-
IV: sedation within 1 min, peak effect by 2–6 min, recovery by 30–60 min [194].
-
IM: sedation within 5–15 min, peaks by 30 min, recovery by 30–60 min [195].
-
PO: anxiolysis and mild sedation peak within 15–20 min, recovery by 60–90 min.
-
IN: effect within 5–10 min, duration 45–60 min. Use of atomizer results in faster onset.
-
-
Mechanism of action: See benzodiazepine introduction.
-
Metabolization: Midazolam is degraded almost completely by cytochrome P450-3A4 in the liver and excreted in the urine. Midazolam metabolites have little CNS activity , unlike those of diazepam.
-
Reversal: Midazolam-induced apnea or respiratory depression may be counteracted by administration of flumazenil 0.01–0.04 mg/kg (maximum 0.5 mg) IV over 30 s and repeated every 60 s to desired response. A cumulative dose of 3 mg may be necessary. Flumazenil may reverse midazolam-induced hypnotic and amnestic effects but not ventilatory depression [125]. The patient must be closely monitored, typically for 2 h after flumazenil administration, for resedation and respiratory depression. Recurrence of sedation has been reported in up to 7% of cases, most commonly in children under 5 years of age [126]. Flumazenil may cause seizures in patients chronically on benzodiazepine medications and should be used cautiously in patients on medications that can lower seizure threshold.
Diazepam (Valium®)
Indications
Diazepam has excellent antianxiety, skeletal muscle relaxation, and amnestic properties, but because its duration of effect is longer than that of midazolam, diazepam is seldom used for ED PSA or preprocedure anxiolysis. It is considered 2–4 times less potent than midazolam.
Contraindications/Cautions/Adverse Effects
Drowsiness may last 2–6 h with resedation occurring at 6–8 h due to enterohepatic recirculation and formation of active metabolites. Like other benzodiazepines, diazepam readily causes respiratory depression with rapid administration.
Diazepam’s propylene glycol carrier causes burning sensations on intramuscular and intravenous injection and erratic absorption with intramuscular administration. Administer with caution in patients with liver and kidney dysfunction.
Pregnancy Category D
-
Dosages: IV, 0.04–0.2 mg/kg/dose q 2–4 h. PR: 0.5 mg/kg/dose.
-
PO: 0.12–0.8 mg/kg.
-
Onset/duration: IV, within 1.5–3 min. PR: 7–15 min.
-
PO: 30–60 min.
-
Mechanism of action: See benzodiazepine introduction.
-
Metabolization: Diazepam undergoes hepatic microsomal oxidation with renal excretion. Liver and kidney dysfunction, as well as active metabolites including desmethyldiazepam and oxazepam, may prolong effects.
Other Non-analgesic Sedative Agents
Propofol (Diprivan®)
Propofol is a sedative hypnotic agent with no analgesic properties [155]. It is the most commonly used parenteral agent for induction and maintenance of general anesthesia in the United States, due in large part to rapid and pleasant recovery from anesthesia induced by this potent agent. Little or no nausea is associated with propofol, and its amnestic effect is similar to that from midazolam [196]. Many adults and older children remark on awakening that they feel as if they have just had a good nap. These characteristics have resulted in propofol’s rapid increase in popularity as an agent for scheduled [86, 197] and ED PSA for children [159, 198]. A recent review and update of propofol use for ED PSA has been published [156].
Propofol has a narrow therapeutic window, which makes PSA titration to desired effect without oversedation more difficult than with many other agents. Significant respiratory depression and hypotension are relatively common (see “Adverse Effects” section) [86, 156, 199]. Propofol can be used alone for painless procedures such as MRI or CT scans, or, at greater doses, for painful procedures . However, because significant respiratory depression or apnea is associated with doses necessary for painful procedures, smaller doses of propofol have been combined with analgesic opiates or ketamine for ED PSA [200,201,201, 363,364,365,366,367,368,369,370,368]. (Please see “Ketofol” section under Ketamine for further details.)
Use of propofol for ED PSA should be preceded by specific training and supervised experience [156]. It is recommended that when propofol is administered, an experienced provider with advanced airway skills be dedicated to administering the sedation and managing the airway and cardiorespiratory status of the patient. In-depth knowledge of adverse effects and advanced airway skills are essential for safe use of this drug.
Pharmacology
The exact mechanism by which propofol exerts global CNS depression has not been fully elucidated . However, there is evidence that propofol potentiates GABAA receptor activity by slowing the channel-closing time, with lesser effects on GABAB receptors, modestly inhibits the N-methyl-d-aspartate (NMDA) receptor, modulates calcium influx through slow calcium-ion channels, and locks sodium channels [204].
Pharmacokinetics
Propofol is highly lipophilic and rapidly diffuses from plasma into body tissues, particularly the highly perfused brain. The onset of action of propofol as determined by time to unconsciousness (i.e., loss of response to voice command) is within 1 arm–brain circulation time (the time required for the drug to travel from the site of injection to the site of action in the brain) and can be as brief as 15–30 s, but is more typically 40–60 s, dependent upon the rate of administration. Since propofol is rapidly distributed from CNS to inactive storage sites such as muscle and fat, recovery from anesthesia is rapid with duration of action about 5–10 min. The short duration of sedation after repeated doses can be explained by rapid metabolic clearance from blood and slow redistribution of the drug from the peripheral tissues . Thus, the pharmacokinetics of propofol after IV administration are best described by a three-compartment model with rapid distribution of the drug from blood into the brain and other tissues, rapid metabolic clearance from blood, and slow redistribution of the drug from the peripheral compartment back into the bloodstream, resulting in sub-hypnotic plasma levels of drug [155].
Propofol is rapidly and extensively metabolized in the liver to less active conjugates, which are excreted mainly in the urine. Since plasma clearance exceeds hepatic blood flow, it appears that the drug also is metabolized at extrahepatic sites. Mean total body clearance of propofol appears to be proportional to body weight; obese patients have a substantially higher body clearance than leaner individuals.
Indications
Propofol sedation of children in the ED has been reported primarily for fracture reduction with fentanyl, morphine, or ketamine coadministered [199, 201, 205]. Sedation or distress scores were low during fracture reduction with propofol + morphine or fentanyl and similar to ketamine + midazolam or morphine + midazolam [199, 200]. Mean recovery times after propofol for these studies were 15–23 min. Unlike other PSA techniques, with the exception of nitrous oxide, repeated or continuous dosing of propofol causes little prolongation of recovery when administered for less than 1–2 h. Thus, after longer procedures, such as complex laceration repair or emergent MRI scans during which either repeated doses or continuous infusion of propofol is required, recovery typically is still within 15–30 min [205]. Note, however, that intermittent bolus dosing appears to be associated with increased risk of respiratory and cardiovascular depression in comparison to continuous infusions [156].
Contraindications/Cautions/Adverse Effects
Transient respiratory depression, apnea, upper airway obstruction, or laryngospasm may occur in up to 10% of children, especially during induction of sedation [86, 156, 199, 207]. Administration of induction dosages of propofol slowly over 3 min decreases the incidence of respiratory depression [208]. Increasing upper airway narrowing due to muscle relaxation, especially at the level of the epiglottis, has been shown with increasing depth of propofol sedation/anesthesia [209]. Loss of protective airway reflexes during apneic periods may place patients at increased risk of pulmonary aspiration as the ensuing bag–mask positive-pressure ventilation increases gastric pressure and risk of passive regurgitation [378]. Pulmonary aspiration during propofol sedation has been found to be rare, but candidates for propofol sedation must be carefully screened for risks of “full stomachs,” URIs, and difficult airways [156, 210]. Respiratory depression and apneic events are frequent enough when sedating with propofol that routine administration of supplemental oxygen and monitoring with end-tidal capnography, in addition to having a functioning anesthesia or CPAP ventilation bag at the bedside, is recommended [107, 108, 115, 156].
The main adverse cardiovascular effect of propofol is hypotension, in part related to decreases in peripheral vascular resistance [211]. In spontaneously breathing patients, as much as a 30% decrease in blood pressure may be seen with little or no changes in heart rate [205, 212]. The decrease in blood pressure is dose- and infusion rate-dependent and is potentiated by coadministration of opioids such as fentanyl [211, 213]. Propofol may rarely induce profound bradycardia and cardiac arrest in hypovolemic patients or in those at risk for hypotension or with cardiac dysfunction [86, 214]. Administration of additional fluids and a cautious rate of IV infusion may help reduce the risk of propofol-induced hypotension.
Because of the increased risk of apnea and hypotension compared to other agents for PSA, many providers avoid use of propofol in ED patients determined to have difficult airways, cardiac dysfunction, brief fasting, or ASA physical status Class III, IV, or V [115, 199].
Propofol is formulated as an emulsion in soybean oil, glycerol, and purified egg products because it is essentially insoluble in aqueous solutions. Historically it was recommended to avoid propofol administration to patients with allergies to eggs or soy. However, propofol has been reported to have been administered without allergic reactions to adults and children with egg or soy allergies and is considered safe to use in these patients [158].
Despite the addition of disodium EDTA or sodium metabisulfite to inhibit bacterial growth, significant bacterial contamination of open containers has been associated with serious patient infection. Using aseptic technique, propofol should be administered shortly after removal from sterile packaging.
Injection site pain is common with propofol but often may not be recalled due to propofol’s amnestic effects. In ED PSA , coadministration of morphine or fentanyl for procedural analgesia may reduce this effect [115]. Lidocaine 0.5 mg/kg administered intravenously immediately prior to propofol infusion and use of large antecubital veins also may help ameliorate this minor adverse effect [156].
Involuntary movement (myoclonus) has been reported in 15–20% of pediatric patients undergoing propofol anesthesia, typically during induction [156]. Myoclonus significant enough to interrupt the procedure, the majority of which were radiological, however, occurred only at a rate of 2/10,000 in elective sedations with propofol [86].
Pregnancy Category B
-
Dosages: Propofol dosing varies by age. In children 3 years and younger, an initial dose of 2 mg/kg and in older children and adolescents 1.5 mg/kg is recommended to achieve sedation [156, 386]. Continuous infusion of 100–250 mcg/kg/minute (6–15 mg/kg/hour) can then be started to maintain longer sedation. Note, however, administration of 2–3.5 mg/kg followed by continuous infusion of 100–300 mg/kg/min is commonly used for induction of general anesthesia [117, 156, 200,201,201, 205, 215, 216].
-
Published studies of pediatric ED PSA for fracture reduction used an initial bolus of 1 mg/kg propofol administered over 1–2 min followed by additional doses of 0.5 mg/kg every 1–3 min based on patient response [199, 201, 205]. Mean total propofol doses in these studies were 2.5–4.5 mg/kg. Alternatively, one study followed the initial 1 mg/kg bolus immediately with a propofol infusion at 67–100 mg/kg/min until cast completion; most children required an additional bolus of propofol during the infusion to achieve the desired level of sedation [201]. In each of these studies, propofol was administered shortly after morphine or fentanyl administration.
-
Administration [156]: Commercially available 1% propofol injectable emulsion (10 mg/mL) may be used without dilution. If dilution is necessary, the drug may be diluted with 5% dextrose injection to a concentration of not less than 0.2% (2 mg/mL) in order to maintain the emulsion. Propofol should be discarded if there is evidence of separation of the emulsion. The emulsion should be shaken well just prior to administration.
-
Using aseptic technique, contents of a vial may be transferred into a sterile, single-use syringe and administered shortly after removal from sterile packaging. The manufacturers state that propofol is compatible with several IV fluids (e.g., 5% dextrose, 5% dextrose and lactated Ringer’s, 5% dextrose, and 0.2 or 0.45% sodium chloride) when a Y-type administration set is used.
Etomidate
Indications
Etomidate is an ultrashort-acting, imidazole-derived, sedative-hypnotic agent with amnestic but no analgesic effects [230]. Because etomidate rapidly induces unconsciousness with little hemodynamic effect and clinical recovery occurs within minutes, it is frequently used in the emergency setting to induce unconsciousness prior to neuromuscular blockade during endotracheal intubation [218,219,219]. However, etomidate inhibits adrenal steroid synthesis for 6–8+ h causing concern for worsening septic shock [230,231,232,232]. This adverse effect has led many to use ketamine to induce unconsciousness prior to intubation in ill patients [388].
Etomidate has been shown to be safe and effective for brief nonpainful procedures such as CT scans and can be combined with fentanyl for fracture reductions. Early reports were inconclusive about the safety and effectiveness of etomidate for ED PSA in children [159, 221,222,223,223]. However, a small study of ED pediatric patients sedated for head and neck CT found successful completion of the CT in 57% with etomidate doses up to 0.3 mg/kg and 76% with doses up to 0.4 mg/kg, in contrast to a success rate of 97% for pentobarbital [171]. Etomidate 0.2 mg/kg IV was infused over 30 s, with additional doses, if needed, of 0.1 mg/kg IV over 30 s at 1 min intervals, to a maximum total dose of 0.4 mg/kg. Duration of sedation was 13 min, and parents felt their children returned to normal behavior much earlier than with pentobarbital. A more rapid infusion technique in another study reported a 99% successful completion of CT scans with etomidate in 446 fasted ASA-PS Class I and II children ; duration of sedation was 34 min [224]. With a proximal tourniquet in place, 0.5 mg/kg lidocaine (maximum dose 25 mg) was first administered through the intravenous catheter to mitigate burning from the subsequent etomidate infusion, a “mini-Bier block” technique. After 1 min, the tourniquet was removed and etomidate 0.3 mg/kg was infused over 2–3 s. If sedation was not adequate, an additional 0.15 mg/kg bolus was administered within 1 min of the initial dose. If needed, an additional 0.15 mg/kg bolus was given during scans requiring multiple views or repositioning. Median total etomidate dose was 3.3 mg/kg. With this technique, one patient had apnea and the CT scan was not completed; otherwise significant respiratory depression did not occur. Although most of these children were not ED patients, it suggests this agent may be used successfully for this purpose.
For fracture reduction, etomidate 0.2 mg/kg infused intravenously over 60–90 s resulted in effective sedation in 92% of children compared to 36% with midazolam 0.1 mg/kg IV [225]. Both were combined with fentanyl 1 mcg/kg IV. Median recovery time in those reaching adequate sedation was 12 min with etomidate and 24 min with midazolam. Desaturation occurred in 22% of children in both groups; all responded quickly to free flow oxygen administration or head repositioning; no patient experienced apnea or required positive-pressure ventilation. Myoclonus occurred in 22% of patients who received etomidate, but it was described as mild and brief and did not interfere with the fracture reduction. Pain on injection of etomidate was noted in 46% of children. More recent studies of etomidate 0.2 mg/kg in conjunction with fentanyl found similar effectiveness for brief painful procedures; 32–36% of children required brief interventions for respiratory adverse events. Median times to discharge readiness were 21–23 min [387, 389, 390]. A small randomized trial found similar dosing of etomidate with fentanyl was less effective than ketamine with midazolam for fracture reduction in children [387]. Further studies of etomidate are needed to define better safety and efficacy parameters for PSA, in emergency patients.
Contraindications/Cautions/Adverse Effects
Similar to midazolam, transient apnea with rapid infusion may rarely occur when etomidate is administered alone [224], but respiratory depression may occur in 20–40% or more of children receiving etomidate coadministered with fentanyl or morphine [225]. Pain with injection in 2–20% and myoclonus in 8–40% of patients are associated with etomidate infusion [221, 226, 227]. When present, myoclonus that can resemble seizures usually lasts less than 1 min and can be decreased by the coadministration redundant of other drugs. These tremors are benign and not epileptiform activity [226, 228].
Although trials investigating etomidate-induced adrenal suppression associated with PSA in noncritically ill children are not available, studies in adults and children have demonstrated cortisol depression for up to 24 h with as little as a single dose of etomidate . This suppression may be clinically significant in patients with hemorrhagic or septic shock, leading some to suggest consideration of alternative agents such as ketamine for induction of unconsciousness for tracheal intubation or PSA in these patients [229, 232, 388].
Pregnancy Category D
-
Dosages: 0.2 mg/kg IV for sedation; 0.3 mg/kg IV for intubation.
-
Onset/duration: onset of sedation within 30–60 s, with duration of deep sedation 3–12 min when using a dose of 0.2–0.3 mg/kg [71]. Sufficient recovery for discharge may take 20–30 min [224, 389, 390].
-
Mechanism of action: Etomidate , like propofol, is structurally unrelated to other anesthetics. It is an imidazole derivative that is thought to induce sedation through enhanced gamma-aminobutyric acid (GABA) neurotransmission [230].
-
Metabolization: Etomidate is highly protein bound in blood and is degraded by hepatic and plasma esterases to inactive products. It exhibits a bi-exponential decline, with a redistribution half-life of 2–5 min and an elimination half-life of 68–75 min [230].
Sedative–Analgesic Agents
The following are primary analgesic agents. Sedation generally requires higher doses of opioids or addition of sedative–hypnotic agents, both of which significantly increase respiratory depression. Ketamine induces sedation and amnesia, but opioid agents cause little amnesia.
Opiates (Narcotics) (Table 22.7): Fentanyl (Sublimaze®)
Indications
Fentanyl is a high-potency synthetic opiate with minimal hemodynamic effects. Due to its lipophilic nature and rapid biphasic redistribution, onset of analgesia and sedation occur rapidly with intravenous administration but are of short duration, making it a favorable agent for ED PSA. Fentanyl, by weight, is 80–100 times more potent than morphine. It provides significant analgesia and mild sedation for painful procedures but is not recommended for anxiety control or for control of spontaneous movement. Since fentanyl, unlike morphine, does not cause clinically significant histamine release, it is the opiate of choice in patients who have increased potential for hypotension, e.g., trauma or sepsis [233].
Atomized intranasal (IN) administration of fentanyl (1.5–2 mcg/kg) in children provides significant pain relief by 5–10 min for painful conditions including orthopedic injures, sickle-cell pain, abscess incision and drainage, and abdominal pain [239,240,241,241, 394,395,393]. IN fentanyl (2 mcg/kg) has been combined with IN midazolam (0.2 mg/kg) to facilitate laceration repair [394]. IN fentanyl (1.5 mcg/kg) combined with 50–70% nitrous oxide was found effective for reduction of mildly/moderately displaced fractures [395]. A retrospective study found IN fentanyl (1.7 mcg/kg) plus 50% nitrous oxide to have similar efficacy to intravenous ketamine plus midazolam for fracture reduction [396]. However, a prospective comparison of IN fentanyl (1.5 mcg/kg) plus 70% nitrous oxide to 70% nitrous oxide alone found similar distress reduction between the two groups but increased emesis in those receiving fentanyl [397]. IN administration is facilitated by devices that create a fine mist to increase broad distribution of the drug onto nasal mucosa [398].
Fentanyl has been administered in oral lozenges (oral transmucosal fentanyl citrate (OTFC)) for ED PSA for laceration repair. However, titration to effect is difficult with this technique, and it has been associated with frequent nausea, vomiting (20–50%), and pruritus [235,236,237,237].
Fentanyl Plus Midazolam
A primary goal with most painful ED PSA is attenuated or blocked unpleasant recall of the procedure. Since fentanyl induces minimal amnesia and cannot completely block procedure-related pain without extreme respiratory depression, it is typically combined with midazolam to induce amnesia for residual procedural pain. Although the combination of fentanyl and midazolam can cause significant respiratory depression [96], both agents have competitive antagonists that readily reverse undesirable effects. Typically, stimulation of the patient or commands to take deep breaths will overcome respiratory depression, but if necessary, a small dose of naloxone, 1 mcg/kg (0.001–0.015 mg/kg/dose IV), repeated as needed, will reverse respiratory depression but retain much of the analgesia effect.
The dose of midazolam that maximizes amnestic effect is not well established. Furthermore, while the onset of peak amnestic effect is indistinct, the duration of action appears to be fairly long, hence a broad window within which to administer the analgesic agent, fentanyl. Thus, it is recommended to maximize the capability to administer sufficient amnestic agent by infusing the midazolam before the fentanyl is given, since the synergistic respiratory depressant effects of the two medications may limit the ability to administer sufficient amnestic agent if it is given after the fentanyl.
Adequate analgesia for painful procedures always requires sufficient narcotic to cause some degree of respiratory depression (assuming narcotic-naive patients). Use of local anesthesia for the procedure (e.g., a hematoma block for fracture reduction) can significantly reduce the amount of systemic analgesic agent needed and thus reduce respiratory depression. It is important to time the “peak analgesia effect” (peak brain concentration) with “maximal analgesia need” (at time of the maximally painful part of the procedure); hence the analgesic agent is administered after the amnestic agent. The respiratory depression is typically counteracted by the pain of the procedure. Particular attention to ventilatory sufficiency should occur after the painful procedural stimulus ends, since respiratory depressant effects will persist for minutes to hours after the last dose of medication [122]. This adverse effect may be exacerbated by oral or parenteral opioid analgesics administered prior to the PSA.
Contraindications/Cautions/Adverse Effects
Fentanyl, like other opioid analgesics, causes dose- and infusion rate-dependent respiratory depression characterized by decreases in respiratory rate , tidal volume, minute ventilation, and ventilatory response to carbon dioxide. Hypotension and bradycardia may also occur with rapid infusion or larger doses. Although return to relative alertness typically occurs within 20–30 min after IV administration, respiratory depressant effects may last several hours. Patients may be awake but need to be reminded to breathe due to the drug’s depression of the brainstem response to rising plasma CO [120, 124, 241].
Respiratory depression can be lessened by administering the expected total dose in divided amounts, e.g., 0.5 mcg/kg/dose (0.0005 mg/kg/dose), and infusing each dose over 30–60 s at 1–2 min intervals. Respiratory depression is markedly increased by coadministration of sedative–hypnotic medications such as midazolam or barbiturates [9, 98]. At the level of deep sedation, many children will have respiratory depression or partial upper airway obstruction due to muscle relaxation and may require airway-opening maneuvers, supplemental oxygen, or painful stimulation [9].
Respiratory depression is readily reversed by the competitive antagonist naloxone. Titration of naloxone in small doses of 1–2 mcg/kg stopping at the endpoint of reversal of respiratory depression will retain much of the analgesia effect. Repeated doses may be necessary as respiratory effects may outlast the reversal effects of naloxone. Administration of a “full” dose of naloxone may cause significant pain, hypertension, tachycardia, vomiting, and other undesirable adverse effects.
Chest wall rigidity may occur with rapid infusion of large doses (usually >5 mcg/kg (0.005 mg/kg)), especially in infants. This life-threatening adverse effect will manifest by lack of spontaneous chest wall movement, dropping oxygen saturations, loss of ETCO2 waveforms, and an inability to ventilate the patient with positive pressure by bag and mask. Reversal with naloxone or paralysis with succinylcholine may be needed to manage this life-threatening adverse event.
Pregnancy Category C
-
Dosages: for analgesia; 1–2 mcg/kg (0.001–0.002 mg/kg), intravenously. Titrate to effect by administering doses of 0.5 mcg/kg over 15–30 s, repeated every 1–2 min. A total dose of 1–2 mcg/kg usually can be administered without causing significant respiratory depression, unless coadministered with midazolam. For significantly painful injuries, an initial dose of 1 mcg/kg usually may be administered safely over 30 s.
-
Intranasal administration of 1.5–2 mcg/kg provides analgesia in 5–10 min. Using an atomizer device, divide the dose repeatedly between nares administering 0.1–0.2 mL/spray until full dose is administered.
-
For ED PSA: fentanyl + midazolam; midazolam, 0.05–0.1 mg/kg intravenously over 1–2 min, is administered first, titrated to an endpoint of drooping eyelids and slurred speech . A total dose of 10 mg likely is sufficient for amnesia in large adolescents. Then fentanyl, 0.5 mcg/kg intravenously over 30 s, is repeated to an endpoint of decreased patient responsiveness to a relevant painful stimulus such as squeezing the fracture site or palpating the abscess. If local anesthesia is used for the procedure, approximately 1 mcg/kg fentanyl may be sufficient. For intensely painful procedures, such as fracture reduction without a hematoma block, up to 2 mcg/kg may be necessary [9]. Respiratory depression is likely at this dose; therefore, time the end titration of fentanyl as the painful part of the procedure is begun; the procedure-related pain will stimulate the patient and counteract some of the respiratory depression. Additional doses of fentanyl may be administered after about 10 min if the patient becomes agitated or manifests significant pain during longer procedures. Alternatively, midazolam may be administered intranasally, 0.2 mg/kg, maximum 10 mg and then intranasal fentanyl 1.5–2 mcg/kg when local anesthesia is also used for the procedure.
-
Fentanyl comes in 2 mL vials of 50 mcg/mL. Titration is easier and safer if the concentrated fentanyl is diluted to 10 mcg/mL by adding 2 mL of fentanyl to 8 mL of normal saline, resulting in 10 mL of 10 mcg/mL.
-
Onset/duration : Analgesia with mild sedation after IV administration of fentanyl is within 30–60 s, with greatest sedative–analgesic effects lasting 5–10 min. Although return to relative alertness typically occurs within 20–30 min after IV administration, respiratory depressant effects may last several hours. Patients may be awake but “forget to breathe” due to the drug’s depression of the brainstem response to rising plasma CO2 [120, 124, 242].
-
Mechanism of action: Fentanyl is a high-potency mu agonist opiate 50–100 times more potent than morphine [233].
-
Metabolization: Fentanyl is metabolized in the liver and excreted in the urine. There are no active metabolites [233].
Morphine
Indications
While the “standard” for analgesia, morphine is typically not used for procedural sedation because its slow onset of peak analgesic effect (~10 min) makes titration difficult. Repeating a dose before 10 min leads to “stacking”; i.e., administering a second dose before the peak effect of the first dose results in unnecessary excess medication administration, overshooting the intended level of analgesia, and is associated with excess adverse effects such as respiratory depression. Morphine is commonly administered to provide baseline analgesia if the patient is in pain from an injury, abscess, etc. Additional analgesia, typically with a different agent such as fentanyl or ketamine, is then administered for the procedure.
Contraindications/Cautions/Adverse Effects
Additional administration of a benzodiazepine for anxiolysis increases the respiratory depression associated with morphine administration. Morphine induces histamine release and may result in hypotension, nausea/vomiting, dizziness, and pruritus; histamine release may exacerbate asthma. Pruritus can be treated with diphenhydramine.
Pregnancy Category C
-
Dosages: IV; 0.05–0.1 mg/kg, titrated to the effect of pain relief. Opioid-naive patients may experience less nausea if the expected dose is divided. For example, an 80 kg teenager will likely better tolerate two 4 mg doses administered 10–15 min apart.
-
Onset/duration: 1–3 min, peak 10–20 min ; duration of significant analgesia 1–2 h.
-
Mechanism of action: mu agonist (analgesia) and weak kappa agonist (respiratory depression).
-
Metabolization: glucuronidated in the liver and excreted in the urine; 10% metabolized to active metabolite, which can accumulate in children with renal failure.
Meperidine (Demerol®)
Indications
Although a potent opioid, meperidine , like morphine, is seldom used for procedural sedation because its long time to peak effect (~10 min) makes it difficult to titrate without overshooting (stacking) the intended level of analgesia and sedation. In addition, meperidine causes histamine release at a greater frequency than do other opioids, and its atropine-like effects may cause tachycardia and euphoria.
Contraindications/Cautions/Adverse Effects
Interaction with MAO inhibitors may be catastrophic resulting in hypertension, excitation, tachycardia, seizure, and hyperpyrexia . Biodegradation to the active metabolite normeperidine (elimination half-life of 15–40 h) results in prolongation of effects. With large or repeated doses, accumulation of normeperidine may cause nervous system excitation with tremors, muscle twitches, and seizures.
Pregnancy Category C
-
Dosages: IV/IM; 1 mg/kg.
-
Onset/duration: IV, 1–5 min, peak by 10 min; duration of 1–2 h. IM, peak effect by 10 min, duration 1–2 h.
-
Mechanism of action: a phenylpiperidine opioid with potent analgesic effects.
-
Metabolization: Hepatic degradation forms active metabolite normeperidine (elimination half-life of 15–40 h), which results in prolongation of effects and has adverse effects as noted earlier.
Codeine
Codeine is well absorbed after oral administration, but the drug must be metabolized by the liver to morphine to have an analgesic effect. Since up to 35% or more of people are slow or non-metabolizers, codeine is an ineffective analgesic agent for many [243, 244]. Conversely, ultrarapid metabolizers may experience reduced analgesic effect but increased adverse effects from relatively small doses [245]. For these reasons, oxycodone is the oral analgesic of choice in the author’s ED.
Oxycodone
Indications
Oxycodone , an opioid analgesic medication originally synthesized from opium-derived compounds, is readily absorbed by oral route and is often administered for painful conditions when no IV access is established, e.g., at triage for possible fractures or burns [246]. It can also be used to augment sedation for painful procedures, e.g., with nitrous oxide for abscess I&D or fracture reduction [88]. Oxycodone is preferred because, unlike codeine, it does not require metabolism to an active form. Oxycodone may cause less nausea than codeine [2], but one comparison found no difference in vomiting or other adverse effects at analgesically similar doses [246].
Contraindications/Cautions/Adverse Effects
Oxycodone, as do other opiates, significantly increases frequency of vomiting when combined with other analgesic regimens, e.g., with ketamine or nitrous oxide. Vomiting prior to ED discharge after PSA increased from approximately 10% with ketamine + midazolam [9] or nitrous oxide [10] to 25% when oxycodone had been administered in triage [88]. Oxycodone also causes dose-dependent respiratory depression by blunting the brainstem response to increasing levels of carbon dioxide. A dose of 0.2 mg/kg administered to children with painful injuries caused tiredness but no clinically apparent changes in ventilation or oxygenation [246]. At a dose of 0.3 mg/kg administered to young children in preparation for painful abscess I&D, we have observed many patients become sleepy but are easily aroused with verbal stimuli and oxygen saturations usually remain within normal ranges as they breathe room air; however, these children should routinely be monitored for respiratory depression after this larger dose.
Pregnancy Category B (D for Prolonged Use)
-
Dosages: 0.05–0.15 mg/kg for out-of-hospital analgesia; for procedural analgesia, 0.2 mg/kg, with the larger end of the range for younger children for fracture reduction, burn debridement , or abscess management. Since absorption after gastric administration has large interindividual variation in the rate and extent of absorption [247], the higher dose is not recommended for home use due to the potential for oversedation. Similarly, oxycodone should be used with caution in infants younger than 6 months of age due to marked variation in clearance [248].
-
Onset/duration: Analgesia begins within 30 min and peaks at ~1 h; duration 2–3 h.
-
Mechanism of action: mu agonist (analgesia) and weak kappa agonist (respiratory depression).
-
Metabolization: Oxycodone is metabolized by the cytochrome P450 enzyme system in the liver with up to 20% excreted unchanged in the urine. Thus, patients with poor renal function may accumulate higher plasma levels.
Hydrocodone
Indications
Hydrocodone is also an oral opioid analgesic often administered for painful conditions at 0.1–0.15 mg/kg. However, like codeine, hydrocodone requires metabolic conversion by cytochrome P450 2D6 (CYP2D6) to hydromorphone to exert analgesic effect. The CYP2D6 gene is highly polymorphic, with variant alleles that result in decreased, absent, or ultrarapid enzyme conversion of hydrocodone and thus affect its analgesia [399]. Moreover, co-ingestion of many other drugs such as ondansetron, which are also metabolized by CYP2D6, can saturate the enzyme making hydrocodone less effective [400].
NMDA Antagonists
Ketamine (Ketalar®)
Ketamine is a phencyclidine-derived lipophilic dissociative agent with rapid biphasic redistribution. Potent analgesic and amnestic effects with relative lack of cardiopulmonary depression make ketamine quite likely the most widely used and appropriate agent for ED PSA [79, 372]. The American College of Emergency Physicians (ACEP) Clinical Practice Guideline for Emergency Department Ketamine Dissociative Sedation: 2011 Update is summarized in Table 22.8 [79]. During fracture reduction , children receiving ketamine demonstrate significantly less distress and less respiratory depression than those receiving fentanyl or propofol coadministered with midazolam [9, 201]. Ketamine also induces significant amnesia and effective PSA for other intensely painful ED procedures such as burn debridement and abscess incision and drainage, as well as relative immobility for procedures during which occasional spontaneous movement is tolerated, such as complex laceration repair, and brief radiological procedures such as CT scans or joint aspiration [79, 159].
Ketamine has unique and diverse mechanisms of action with beneficial and potentially adverse effects. Ketamine interacts with multiple binding sites including NMDA and non-NMDA glutamate receptors, nicotinic and muscarinic cholinergic and opioid receptors, and, less so, peripheral neuronal sodium channels [250]. Ketamine’s primary site of anesthetic action is in the CNS in thalamocortical pathways and the limbic system where it binds to a site on postsynaptic NMDA channels that regulate transmembrane calcium, sodium, and potassium flux . This binding inhibits glutamate activation of the channel in a noncompetitive manner and is time- and concentration-dependent [119, 250, 251].
Circulatory Effects
In contrast to other sedative and analgesic agents, cardiac output, including heart rate and blood pressure , is usually well maintained with ketamine administration, even at deeper levels of sedation or anesthesia. Ketamine causes 10–30% increases in blood pressure and heart rate by blocking reuptake of catecholaminergic hormones norepinephrine, epinephrine, dopamine, and serotonin. These effects may increase intracranial pressure, and caution has been suggested with its use in patients with known intracranial pathology causing increased intracranial pressure. However, use of ketamine in ventilated patients with head trauma has been shown safe and not to impact intracranial pressure differently from opioids [252, 253]. Use of ketamine in the ED for rapid sequence intubation of patients with head trauma has also been advocated as safe [254]. Of note, ketamine also has a direct negative inotropic effect on the heart that is usually clinically inapparent due to the sympathetic stimulation [255]. In critically ill patients whose catecholamines are depleted due to maximal compensation for hypovolemia, hypoxemia, fluid–electrolyte, acid–base, and other physiologic insults, administration of ketamine may cause marked hypotension and bradycardia [256].
Ventilatory Effects
In marked contradistinction to other sedative–analgesic agents, doses of ketamine typically used for ED PSA rarely cause depression of pulmonary gas exchange or relaxation of upper airway muscles [79, 257]. Intravenous infusion of 2 mg/kg of ketamine over 1 min characteristically causes no significant effect on respiratory rate, tidal volume, minute ventilation, or end-tidal CO2, thus maintaining adequate gas exchange during unobstructed spontaneous room air breathing [258]. A study of intravenous administration over 5 seconds or less of up to 1 mg/kg found no significant respiratory or circulatory adverse effects [376]. Furthermore, ketamine does not significantly decrease thoracic or airway muscle activity [257, 259, 260], or impair lung ventilation distribution, functional residual capacity, or minute ventilation with intravenous doses of 2 or 4 mg/kg [134]. These effects and maintenance of positive end-expiratory pressure (PEEP) [261] result in lack of peripheral alveolar collapse and regional hypoventilation seen with propofol and opioid agents. Interestingly, relatively low-dose ketamine (1 mg/kg administered intravenously over 5 min, i.e., 0.2 mg/kg/min) to adults caused respiratory stimulant effects with three distinct phases: Increased tidal volumes (deep breathing) were followed by increased respiratory rates and then large tidal volumes with low respiratory rates and occasional brief apnea, possibly compensating for hypocarbia due to the preceding hyperventilation [262]. These findings are consistent with the mild increase in respiratory rate with maintenance of normal oxygen saturation and end-tidal CO2 noted in children receiving intravenous ketamine 1.5 mg/kg over 1 min for ED PSA [111].
Reduced responsiveness to increased CO2 and hypoxemia, however, have been demonstrated during the initial period after a bolus of ketamine when plasma levels are high and resolving as levels decrease [258, 263, 264]. This suggests the possibility of apnea in sensitive individuals or a delayed response to hypercarbia if airway obstruction occurs during induction of sedation and may explain the case reports of brief respiratory arrest after administration of intramuscular ketamine for ED PSA [120, 265, 266]. A case series of 18 children who inadvertently received 5–100-fold larger-than-intended doses of ketamine described respiratory depression and prolonged recovery but no residual effects except for 1 critically ill infant who died [157]. A meta-analysis of more than 8000 children who received ketamine for ED PSA found that the overall incidence of airway and respiratory adverse events (upper airway obstruction, apnea, oxygen desaturation ≤90%, or laryngospasm) was 4%. Increased risk was found in younger children and teenagers, those receiving more than 2.5 mg/kg initial or 5 mg/kg total doses, and those receiving coadministered anticholinergic or benzodiazepine medications [137]. Airway and respiratory adverse events occurred at twice the overall rate in children younger than 2 years, except for laryngospasm and apnea, which were not increased. The overall frequency of airway and respiratory adverse events in adolescents 13 years or older was almost three times greater with more apnea but less laryngospasm. The overall frequency of apnea was 0.8% in this series. Coadministration of other sedative–analgesic agents such as midazolam or morphine and young age also have been found by others to be associated with greater respiratory depression [87, 267].
Protective Airway Reflexes
Preservation of upper airway protective reflexes , even at deeper levels of sedation or anesthesia, reduces the risk of pulmonary aspiration and thus makes ketamine one of the safest agents for ED PSA in unfasted children, yet, paradoxically, it may increase the risk for one of the most significant life-threatening sedation-related adverse events: laryngospasm [134,135,136]. The incidence of laryngospasm in ketamine-based pediatric ED PSA is difficult to determine as it is a rare event and large sedation databases are not available for estimation. The meta-analysis of pediatric ketamine-based ED PSA found an incidence of laryngospasm of 0.3%; the only identifiable association with greater risk was an initial intravenous dose of greater than 2.5 mg/kg, but data was unable to be analyzed for URI, wheezing, or other risk factors noted with general anesthesia. Young age and oropharyngeal procedures (excluding endoscopy) were not associated with increased risk [137]. Although in the past, the prophylactic administration of anticholinergics was believed to reduce the incidence of secretions, laryngospasm, and respiratory complication , this is no longer held true. Rather, a recent matched case–control analysis of 8282 ketamine procedures in the emergency department revealed no association between age, dose, procedure, medical status, route of delivery, and the administration of anticholinergics with the occurrence of laryngospasm [268]. This data is important because it identifies the occurrence of laryngospasm as an unpredictable and idiosyncratic reaction. All practitioners, thus, who administer ketamine should be prepared to identify and treat laryngospasm.
Initial management of laryngospasm should include airway-opening maneuvers (straightening, jaw thrust) and administration of supplemental oxygen, preferably by CPAP. If these are insufficient to maintain oxygenation, low-dose succinylcholine should be considered (~0.1–0.2 mg/kg IV); if this low dose does not improve oxygenation, a full paralytic dose of 1–3 mg/kg succinylcholine should be administered. Laryngospasm induced by ketamine may be brief or it may be recurrent and it may occur during emergence as well as induction or mid-procedure [133]. Please see section on “Management of Laryngospasm.”
Sedative–Analgesic Effects
Sedation and dissociation induced by ketamine likely occur primarily from blockade of the excitatory effects of glutamate, the most prevalent CNS excitatory neurotransmitter. By binding to the neuronal membrane’s NMDA glutamate receptor complex associated with transmembrane calcium channels, ketamine prevents or reduces neurotransmission of pain and other stimuli by interfering with the calcium influx necessary for electrical propagation [250].
Subdissociative Ketamine
Administration of ketamine at low (subdissociative) doses of 0.1–0.4 mg/kg IV over 15 min has been shown in adults to provide pain relief similar to that of morphine or to augment opioid-associated analgesia [412, 413]. Infusion over 15 min provides effective analgesia with fewer minor adverse effects than faster administration[414]. Similar studies have yet to be performed in children.
Intranasal Ketamine
Needleless administration of potent sedative or analgesic medications has been a focus for distress and pain management in children. Bioavailability of intranasal (IN) ketamine is described as 20–50% with significant variability in plasma concentrations and absorption times. In 20 children, aged 1–7 years, 2 mg/kg of S-ketamine administered either IN or intravenously (IV) resulted in peak plasma concentrations of ketamine in the IN group at 20% of the IV group with the IN peak at 18 ± 13 min [415]. One child in the IN group experienced a rapid and high level of ketamine absorption with a peak plasma concentration twice the mean. In an earlier study, ketamine was administered IN at 3 mg/kg (IN3), 9 mg/kg (IN9), or 3 mg/kg (IV3) [416]. Mean plasma concentrations of ketamine peaked at 496 ng/mL in group IN3 and 2104 ng/mL in group IN9, both within 21 min. Calculated bioavailability was 50% in both IN groups. The peak ketamine plasma level in IN9 was similar to that of IV3, but the author concluded the large volume of ketamine required for IN9 was partly swallowed and led to an unacceptable variability of effect that precluded the IN route for induction of anesthesia.
IN ketamine (1 mg/kg) has been found to provide effective analgesia similar to that of IN fentanyl (1.5–2 mcg/kg) but with somewhat more common minor adverse effects such as bad taste, dizziness, or minimal sedation [240, 420,421,419]. Many studies have found IN ketamine 2–10 mg/kg, with or without additional sedatives, to provide adequate sedation in children undergoing dental procedures [417]. However, the high degree of variability of sedation onset, depth of sedation, and prolonged recovery make IN ketamine a less desirable sedation technique for ED procedures. An interim analysis of sedation for laceration repair in children compared 3, 6, or 9 mg/kg of IN ketamine [420]. The 3 and 6 mg/kg doses did not achieve adequate sedation. At 9 mg/kg, three of four patients were adequately sedated with recovery by 35–70 min. A small preliminary report of sedation for reduction of simple forearm fractures found 8 mg/kg IN ketamine effective in only 57% of children [421]. Of note, 1 mg/kg IN ketamine administered to 20 children who resisted venipuncture or venous catheter placement resulted in significantly reduced pain and anxiety and 90% successful procedure completion on first attempt [422].
Oral Ketamine
Ketamine administered orally (PO) also has been investigated for procedural sedation. PO ketamine 10 mg/kg administered 30–45 min prior to laceration repair, compared to placebo, resulted in 67% being cooperative (vs 7% with placebo) during lidocaine injection and during suturing (73% vs 20%); 80% in the ketamine group did not need continuous physical restraints. Half of the children were deeply sedated, and a quarter reached moderate sedation . No significant adverse cardiopulmonary effects occurred. Mean time to discharge was 104 ± 33 min [423]. A comparison of PO ketamine 10 mg/kg to PO midazolam 0.7 mg/kg prior to laceration repair found the ketamine group had greater tolerance of the local anesthetic injection but no difference in the tolerance of the suturing. Children receiving ketamine were more quickly sedated, 20 versus 43 min, but median times to discharge were similar, 105–110 min. Inconsolable agitation was the most prominent adverse effect in the midazolam group (21%), whereas vomiting (20%) occurred more frequently in the ketamine group [424]. A comparison of PO ketamine 5 mg/kg to PO midazolam 0.7 mg/kg found similar levels of sedation, but 32% of the ketamine group required additional IV sedation (vs 6% for midazolam) [425]. Combining PO ketamine 5 mg/kg with PO midazolam 0.5 mg/kg resulted in mean time to mild sedation of 15 min and 94% with effective sedation, but mean time to discharge was 3 h [426].
Dissociative Effects
Ketamine is classified as a dissociative general anesthetic agent because EEG and functional MRI (fMRI) recordings demonstrate electrical activity of the thalamus that is no longer synchronized with or is “dissociated” from the limbic system after ketamine administration [269]. The thalamus is believed to process and relay sensory information selectively to specific areas of the cerebral cortex and plays a major role in regulating arousal, the level of awareness , and activity as well as processing auditory, somatic, visceral, and visual sensory input [135]. It is thought this dissociative effect is the primary mechanism for preventing patients’ response to pain or other sensory stimuli after ketamine administration. More precise understandings of the mechanisms are under investigation. The patient who has received ketamine without an adjunctive sedative agent may have his/her eyes open but be unresponsive to the environment, described by some as if “the lights are on but nobody’s home.” This catatonic stare may be frightening to unprepared observers such as family members.
Prolonged Analgesic Effects
A relatively unexplored potential analgesic benefit of ketamine use for ED PSA is reduction of windup and central sensitization [270]. Brief noxious stimulation of peripheral tissue receptors initiates rapid neural transmission along myelinated and unmyelinated axons to the nerve’s central terminus located within the dorsal horn of the spinal cord and induces release of excitatory neurotransmitters, primarily glutamate, into the dorsal horn synapse. The glutamate initiates rapid firing of postsynaptic AMPA and kainate receptors, resulting in sharp “first” pain and reflex withdrawal from the stimulus, soon followed by dull, aching, burning, and poorly localized “second” pain. Persistent noxious stimulation of these peripheral nerves induces pre- and postsynaptic neurons in the dorsal horn to undergo changes in function , chemical profile, and structure that result in propagation of neural impulses at lower-than-normal thresholds, prolonged discharge, and widening of receptive fields. These changes have been termed “windup” and “central sensitization” hyperalgesia wherein successive similar stimuli cause increasing pain or normally subthreshold stimuli, such as light touch, produce intense pain at and adjacent to the site of original injury. Windup and central sensitization occur primarily by greater and more prolonged opening of postsynaptic NMDA channels to allow Ca2+ influx, which reduces transmembrane potential and facilitates postsynaptic depolarization [271]. This central facilitation manifests within seconds of a nociceptive stimulus and can outlast the stimulus for hours, days, or longer if the stimulus is maintained, even at low levels [272, 273, 283]. Experimental and clinical studies in adults have demonstrated that a single small dose of ketamine reduces the magnitude of hyperalgesia and windup-like pain [276,277,278,277]. Adults undergoing elective orthopedic or abdominal operations, for example, had reduced postoperative pain and marked reduction of opiate medication use for hours to days when as little as 50 mg of ketamine was added to their general anesthetic regimen [135, 278, 279]. Continued low-dose infusion of ketamine has also been shown to markedly augment morphine for analgesia after musculoskeletal injury in adults [280].
Paradoxically, opiates have been found to induce short-lasting analgesia and long-lasting hyperalgesia [281]. This opiate-induced hyperalgesia is also under the influence of excitatory neurotransmission and is similarly reduced by ketamine blockade of the NMDA glutamate receptor [282, 284]. Whether these prolonged beneficial effects occur with ketamine administration for ED PSA after an acute traumatic injury has yet to be explored.
Neurotoxicity
Concern has been raised about use of ketamine in children due to evidence of neurotoxicity in animals after high doses. Toxicity manifested as neuronal vacuolization has been found within specific areas of the midbrain of rats after administration of 40 mg/kg ketamine, but not after doses of 5, 10, or 20 mg/kg [285]. Other investigators found no evidence of neuronal injury (apoptosis) in 7-day-old rat pups after single doses of 25, 50, or 75 mg/kg; only with repeated injections of ketamine 25 mg/kg every 90 min for 9 h was any evidence of toxicity noted [286]. Of possible pediatric relevance, neuronal vacuolization was not found even with large doses of a potent ketamine-like drug (MK-801) in animals prior to puberty [287]. In addition, GABAergic drugs (e.g., diazepam) and alpha agonists (e.g., clonidine) markedly reduce the excitotoxic effects of ketamine-like drugs ; it has been suggested these should be coadministered with ketamine as a neuroprotective strategy.
A marked increase in normal CNS apoptosis or programmed cell death and some evidence of subsequent learning disabilities in association with administration of ketamine, ethanol, benzodiazepines, propofol, and volatile anesthetics also have been found in rodent animal models [291,292,290]. Of potential importance, the brain area most affected may vary by species. In rodents, key regions for learning are targeted , whereas in the monkey perhaps less-essential cortical redundant cells are more affected [291]. While it is difficult to compare the effect of specific dosages across species, doses that achieve similar clinical effects as PSA have been shown to increase CNS apoptosis in infant mice [292]. Although ketamine has been used extensively in children without apparent ill effect, these studies raise serious concerns that are the targets of ongoing investigations.
Psychotomimetic Effects
Transient ketamine-induced schizophrenia-like symptoms including hallucinations, delusions, illogical thinking, poverty of speech and thought, agitation, disturbances of emotion and affect, withdrawal, decreased motivation, decreases in memory, and dissociation are well described in adults and a major constraint to use of the drug [296,297,298,296]. These symptoms occur when plasma levels of ketamine are relatively low and thus are seen during recovery from sedation. Similar to onset of schizophrenia, these symptoms are thought to be more common in adults and adolescents than in prepubertal children , but this has not been confirmed in children or in association with ED PSA [87, 251, 255, 300,301,299]. Dependent upon definitions, overall emergence phenomena are well tolerated and occur in approximately 5–25% of children recovering from ED PSA with ketamine, as well as with other drug regimens , and in similar frequency at home within days of discharge [9, 87, 298, 300]. However, significantly unpleasant and disturbing phenomena (i.e., nightmares, hallucinations, and severe agitation) occur unpredictably in approximately 5% or fewer children and are also seen with other drug regimens such as fentanyl plus midazolam [9, 87]. Midazolam routinely administered after ketamine or mixed within the same syringe does not appear to reduce significant recovery dysphoria and may increase agitation in postpubertal children [87, 301]. Of interest, preinduction anxiety and agitation have been correlated with emergence delirium for both ED PSA and general anesthesia [301, 302]. Whether pre-sedation midazolam for anxiolysis may reduce recovery dysphoria in significantly anxious children undergoing ED PSA, as has been shown with general anesthesia, is unclear [300, 303].
A potentially effective strategy to reduce emergence delirium, and one regularly employed by the author and others , is to inform the patient to expect transient funny dreams, diplopia, blindness, etc. and to have pleasant thoughts during induction of sedation [304].
Beneficial Psychiatric Effects
Over the past decade, increasing studies in adults with mood and anxiety disorders that were previously resistant to treatment have found ketamine to produce rapid and robust antidepressant effects [401, 402]. Antidepressant medications that increase the activity of monoamine neurotransmitters, including serotonin, norepinephrine, and dopamine, typically take weeks to work, whereas the effects of ketamine on depression occur within hours. Most studies administered 0.5 mg/kg of ketamine intravenously over 40 min, but alternative doses and intervals are being investigated. Infusions repeated weekly have been found more effective in providing desired effects [403]. These treatments typically are conducted in a hospital or clinic setting but also have been performed in the ED or in collaboration with emergency physicians [404, 405]. A systematic review of ten controlled trials of treatment of depressed adults with suicidal ideation found ketamine rapidly reduced suicidal thoughts, within 1 day and for up to 1 week [406]. A trial in 13 adolescents with treatment-resistant depression administered 6 ketamine infusions of 0.5 mg/kg over 2 weeks. While the first five who received lower doses did not have benefit, five of eight who received doses based on actual body weight rather than idealized weight responded. Two of the responders were still in remission at the 6-month follow-up [405]. A later report of a 15-year-old with treatment-resistant depression and suicidal ideation noted improvement after repeated infusions of ketamine over 3 weeks [407]. An analysis of data from 188 adults who participated in 4 trials of ketamine for treatment-resistant major depressive disorder or bipolar disorder found 50–80% experienced feeling strange, spacey, woozy, loopy, dissociated, floating, visual distortions, difficulty speaking, and numbness during the infusion. Most side effects peaked within an hour of ketamine administration and resolved completely by 2 h post-infusion. No serious drug-related adverse events were observed, and at 3-month follow-up, no serious adverse events, such as cravings, memory problems , or cognitive deficits, were found [408]. Trials of orally or intranasally administered S-ketamine (approved by the FDA in 2019) are also being investigated [409, 410]. Because of adverse effects, as well as the potential for abuse, ketamine administration needs to be administered under medical supervision. Whether ketamine or S-ketamine can be used in emergency departments as a part of a comprehensive approach to reduce the risk of suicide in patients presenting with urgent suicidal thoughts requires further research [411].
Other Adverse Effects
Ketamine administration occasionally causes an evanescent erythematous rash shortly after infusion and, more commonly, double vision and dizziness during emergence from sedation; hypersalivation, typically with repeated or larger doses; and vomiting [9]. Vomiting in children who receive ketamine without adjunctive medications for ED PSA has been reported in 10–20% of children [87, 92]. Fortunately, vomiting almost always occurs during the recovery period and after discharge from the ED [9, 305].
Coadministration of opioids such as morphine or oxycodone increases emesis, whereas coadministration of midazolam with ketamine significantly reduces the likelihood of vomiting (19% versus 10%) [87] as does ondansetron (13% versus 5%) [92]. Since vomiting may be more likely to occur in older children, ondansetron should be especially considered in children older than 5 years [92]. Vomiting does not appear to be linked to the length of pre-sedation fasting or the dose of ketamine administered [63, 90, 306].
Ketamine-associated hypersalivation is thought to be mediated via cholinergic effects [135]. Because of concern that excess saliva may trigger laryngospasm and other adverse airway events, anticholinergic antisialagogues such as atropine or glycopyrrolate have traditionally been coadministered with ketamine [119, 251]. However, an unblinded observational study of approximately 1000 children receiving intravenous ketamine without an antisialagogue for ED PSA, mean dose 2 mg/kg, found no significant hypersalivation or adverse airway effects [144]. In contrast, a randomized blinded trial of intramuscular ketamine, 4 mg/kg, with or without atropine, found increased salivation but no adverse airway events in those receiving ketamine [143]. These studies suggest hypersalivation may be dose related. Importantly, a meta-analysis and a subsequent study of 22,645 ketamine-based sedations found an increased occurrence of respiratory adverse events associated with antisialagogues [137, 377]. Because of these studies and that “dry mouth” is a common complaint after atropine or glycopyrrolate, the author no longer routinely administers an antisialagogue when a single intravenous ketamine dose or total doses of 2 mg/kg or less are used for ED PSA.
Contraindications/Cautions/Adverse Effects
Please see specific effects.
While much less common than with other ED PSA regimens, respiratory depression, apnea, and upper airway obstruction may occur with ketamine administration [266]. When identified by close monitoring and direct observation, these adverse effects are usually easily managed with simple maneuvers such as jaw thrust and airway straightening [305]. Ketamine preserves cardiac output in healthy patients but should be used with caution in patients manifesting shock as it may cause cardiac depression and profound hypotension [256].
Psychotomimetic effects—e.g., hallucinations, paranoia, and other schizophrenia-like symptoms—occur unpredictably and usually become manifested as dysphoria during recovery. Some believe these symptoms may occur more frequently in postpubertal children and in children with psychiatric disorders. Since the pathologic mechanisms of schizophrenia appear to be similar to ketamine-induced effects, it is recommended to avoid use of ketamine in patients with psychiatric disorders and those whose close relatives carry these disorders. Although not well studied, children with attention deficit and hyperactivity disorders (ADHD) do not appear to have increased susceptibility to psychotomimetic effects. Ketamine is used routinely with and without midazolam in the author’s ED for intensely painful procedures in adolescents; all verbal children are informed prior to sedation of what they might experience during recovery and given the suggestion to think of pleasant circumstances as sedation is induced. Midazolam routinely administered after ketamine or mixed within the same syringe does not appear to reduce dysphoria during recovery from ketamine sedation and may increase dysphoria in teenagers [87, 301]. Highly anxious children may benefit from receiving anxiolytic doses of midazolam well before ketamine, as has been shown with general anesthesia [303, 307, 308].
Ketamine is available in concentrations of 10, 50, or 100 mg/mL. For intravenous sedation, it is recommended only the 10 mg/mL concentration be used in order to reduce the risk of overdose and to facilitate titration to desired effect. It is also recommended that only one concentration be routinely available in the ED to reduce the likelihood that a more concentrated solution and, thus, larger dose than intended be inadvertently administered.
Pharmacokinetics
In unpremedicated children and adults, approximate ketamine distribution half-life is 24 s, redistribution half-life 4.7 min, and elimination half-life 2.2 h [309, 310]. The redistribution half-life of 5 min is consistent with the typical deepest sedation period of 5–10 min observed with single-dose ketamine for ED PSA. Midazolam or diazepam coadministration with ketamine may delay hepatic metabolism, yet it does not seem to prolong recovery although the midazolam sedative effects may prolong discharge [87, 311].
To reliably achieve the dissociated state for ED PSA, a minimum dose of ketamine 1.5–2 mg/kg administered intravenously over 30–60 s or 4–5 mg/kg administered intramuscularly is generally recommended [79]. However, studies have found smaller intravenous or intramuscular doses to be effective, particularly when coadministered with midazolam [9, 88, 161, 312, 313]. Recent pharmacokinetic studies of ketamine ED PSA in children have helped elucidate why these different dosing strategies can be effective.
Age-specific ketamine pharmacokinetic profiles based upon measurement of plasma concentrations of ketamine in children 1.5–14 years of age who were undergoing ketamine ED PSA have been determined [314]. These profiles were then used to simulate several dosing strategies and recovery periods designed to achieve 15 min of very deep sedation/anesthesia (unresponsive or arouses, but not to consciousness , with painful stimulus) [160]. They predict a typical 6-year-old child would recover (drowsy, eyes open or closed but easily arouses to consciousness with verbal stimulus) by 70 min after a 2 mg/kg infusion over 30–60 s. An alternative strategy of an initial bolus of 1.25 mg/kg with a subsequent half dose (0.625 mg/kg) “top-up” at 8 min would achieve recovery by 30 min. Finally, an initial dose of 0.3 mg/kg followed by an infusion of 3 mg/kg/h for 15 min would result in recovery by 20 min after the infusion was stopped. These and doses for other ages are listed in Table 22.9.
As with most drugs, between-subject variability has been found in ketamine effect and clearance. The mean target ketamine plasma concentration of 0.65 mg/L would only be effective in 50% of children; a concentration of 1.59 mg/L would be required to achieve a similar effect, with longer recovery, in 95% of children [160]. The rate of plasma clearance in children is similar to that in adults and correlates with hepatic blood flow. Clearance increases in a nonlinear function with decreasing age and is reflected by higher dose requirements (mg/kg) to maintain the desired effect in younger children. Size accounts for only about half of the clearance variability; it is unknown what impact pharmacogenomics add. In an individual child, titration to the desired depth of sedation must be gauged clinically.
Concern has been raised that very rapid intravenous administration of ketamine may increase the risk for apnea or marked respiratory depression, presumably due to rapid changes in brain ketamine concentrations [79]. However, a recent small study of ketamine intravenous administration over 5 seconds or less of up to 1 mg/kg found no significant respiratory or circulatory adverse effects and mean recovery to discharge criteria in 20–25 min [376]. Rapid infusion of small doses has long been the author’s practice, enabling effective sedation with smaller doses and more rapid recovery for brief painful procedures such as a simple fracture reduction or abscess incision and drainage. The same technique is used for titration of additional doses as needed.
Indications
Ketamine is particularly effective as PSA for intensely painful procedures such as fracture reduction, dislocated joint reduction, burn debridement, or abscess I&D [9, 79]. Ketamine is also an effective PSA technique for brief painful radiological procedures such as guided joint aspiration or nonpainful CT scans and repair of complex lacerations. Procedures that involve the oropharynx, such as peritonsillar abscess I&D or endoscopy, may be performed with light ketamine sedation (see case examples), but the sedating physicians must be prepared for an increased risk of laryngospasm [146, 315, 316].
Pregnancy Category B
-
Dosages: When administered in doses greater than 2 mg/kg, ketamine readily induces general anesthesia with unresponsiveness to painful stimuli yet with continued spontaneous respirations and good cardiac output. However, initial intravenous doses ≥2.5 mg/kg or total dose ≥5.0 mg/kg after repeated dosing have been associated with increased risk of adverse respiratory events [137]. It is recommended that ketamine be titrated to the desired degree of blunted response to intense pain. Complete lack of responsiveness to painful stimuli is unnecessary with ketamine as it is a potent amnestic agent [9, 79]. Providers and parents can be reassured (but not guaranteed) that most patients will have little or no memory of the painful procedure, even if moans occur during the most painful parts. It helps parents if providers confirm procedural amnesia by asking the patient what is remembered after recovery, especially when the parents have remained in the room during the procedure.
-
IV: Total dose 1–2 mg/kg when used alone is sufficient for the most intensely painful procedures lasting less than 5–15 min (see “Pharmacokinetics” section). If coadministered with midazolam, 1–1.5 mg/kg is often sufficient. The total dose can safely be administered as a single dose over 30–60 s, but many sedators begin with an initial dose of 0.5 mg/kg administered over 15–30 s and repeated every minute until the desired blunted response to pain is achieved. For prolonged procedures, additional doses of 0.25–0.5 mg/kg may be administered as needed (about every 5–10 min), depending on individual patient response to stimulus [9, 312]. The smaller initial dose with additional doses as needed may shorten time for recovery [160]. Use of local anesthetics, when applicable, is highly encouraged to decrease the amount of ketamine needed. For an intensely painful but very brief procedure in which patient movement can be tolerated, e.g., moving a patient with a femur fracture off the spine board onto the ED bed, or repositioning a fractured extremity for an optimum radiograph, a small dose (0.2–0.3 mg/kg) administered rapidly by IV (over less than 5 s) can enable the patient to tolerate the procedure without losing consciousness; patients should be warned of feeling “weird” and monitored for possible sedation with this technique.
-
IM: 2–4 mg/kg, with smaller dose used for brief procedures in which local anesthesia is also used, e.g., laceration repair [313, 317].
-
IN: 1–2 mg/kg intranasally provides analgesia, but sedation likely requires 9–10 mg/kg. The variability of sedation makes this route less practical (see intranasal section above).
-
-
Onset/duration:
-
IV: sedation–analgesia within 15–30 s with initial deeper effects lasting 5–10 min and recovery by 60 min, depending upon dose administered.
-
IM: sedation–analgesia within 5–15 min, duration 30–150 min, depending upon dose administered.
-
IN: 1–2 mg/kg for analgesia, onset within 10–20 min, duration 60+ minutes.
-
-
Metabolization: Hepatic degradation of ketamine within the cytochrome systems results in norketamine, which has one-third the analgesic potency of ketamine. Norketamine has a shorter elimination half-life (1.13 h) than ketamine (2.1 h) [318].
Adjuncts
Note: Studies have found an increased occurrence of respiratory adverse events associated with coadministration of antisialagogues with ketamine [137, 377].
Glycopyrrolate (Robinul®)
Indication
Antisialagogue is used by some clinicians before initial dose of ketamine. It is preferred by some over atropine because it does not cross the blood–brain barrier, thus not causing possible undesirable CNS effects. Antisialagogues prior to single doses of 1–2 mg/kg of ketamine are likely unnecessary [79, 137, 143, 144]. It is unclear whether use of antisialagogues is beneficial in children with active URIs. Many children complain of “cottonmouth” for 6–8 h after glycopyrrolate administration [9].
Concentration
200 μg/mL.
Dose
5 μg/kg IV. Maximum dose is 200 mg. Administer at least 5–15 min before the initial dose of ketamine.
Atropine
Indication
Antisialagogue is used by some clinicians in conjunction with initial dose of ketamine (instead of glycopyrrolate). Concern has been raised about potential CNS adverse effects with atropine (e.g., excitation), but this appears uncommon [143]. Antisialagogues prior to single doses of 1–2 mg/kg of ketamine are likely unnecessary [79, 137, 143, 144]. It is unclear whether the use of antisialagogues is beneficial in children with active URIs.
Dose
0.01 mg/kg (minimum 0.1 mg, maximum 0.5 mg).
Ketamine with Sedatives or Analgesics
Other sedative or analgesic medications coadministered with ketamine, including propofol, midazolam, fentanyl, or barbiturates, increase the likelihood of adverse respiratory events [372, 377].
Ketamine Plus Propofol (Ketofol)
Although combining ketamine with propofol may have theoretical benefit by using lower doses of each agent to reduce the undesirable adverse effects of both agents, published studies in adults and children find the combination had not demonstrated superior clinical efficacy compared with propofol alone. A randomized trial comparing ketamine alone to ketofol found ketamine alone slightly more effective for fracture reduction (99 vs 90%) but the ketofol group had less vomiting [427]. A 2018 multicenter study of ED PSA in children found combining propofol with ketamine or fentanyl reduced the risk of adverse events compared to propofol alone, but all three techniques had greater risk than ketamine alone [372]. Studies conflict regarding reduced hemodynamic and respiratory adverse effects with the combination compared with propofol monotherapy [202]. A comparison of propofol + ketamine to propofol + fentanyl for PSA in toddlers undergoing burn dressing changes found similar minimal impact on blood pressure and respiratory rate but less restlessness with the addition of ketamine [203].
Coadministering ketamine and propofol (ketofol) intravenously has been shown to be an effective and efficient technique for ED PSA with fewer adverse effects than when both drugs are used as single agents [360, 361]. The decreased respiratory depression with ketofol may be due to the smaller doses of propofol needed to achieve sedation when coadministered with ketamine [362]. Moreover, use of ketamine for analgesia reduces the need for opioid coadministration with propofol, a combination that potentiates respiratory depression. Less frequent vomiting is also reported in patients receiving ketofol, when compared to use of ketamine alone, an effect similar to ondansetron [362]. Four studies of children receiving ketofol for ED PSA, primarily for fracture reductions, have been published to date [366,367,365, 427]. The optimum relative doses of ketamine and propofol are unclear.
A well-designed trial compared ketofol to ketamine alone in 136 children [363]. Children received either (1) an initial dose of ketamine followed by propofol (“ketofol”), 0.5 mg/kg each, and then propofol 0.5 mg/kg every 2 min as needed to achieve deep sedation or (2) an initial 1.0 mg/kg of ketamine followed by 0.25 mg/kg of ketamine every 2 min, as needed. The median total doses of propofol and ketamine were 0.5 mg/kg for those receiving ketofol and 1.0 mg/kg of ketamine for those receiving ketamine alone. The ketofol group had shorter recovery time by 3 min (13 vs 16 min) and fewer children experienced vomiting (2% vs 12%). Unpleasant recovery (agitation, hallucinations, delirium) occurred in 8% with ketofol and 13% with ketamine alone. Other adverse events were similar between the two groups.
A case series described use of intravenous ketofol (ketamine–propofol mixed 1:1 in a single syringe) titrated to deep sedation for ED PSA in 219 children [364]. The median dose was 0.8 mg/kg each of ketamine and propofol. Median recovery time was 14 min . Two patients required brief vigorous stimulation for central apnea, and positive pressure ventilation was needed to manage laryngospasm in an infant with croup who had undergone laryngoscopy to look for a foreign body.
An earlier case series of 20 children evaluated ketamine 0.5 mg/kg followed 1 minute later by propofol 1 mg/kg [365]. Second doses of ketamine, 0.25 mg/kg, and/or propofol, 0.5 mg/kg, were permitted if the level of sedation was deemed inadequate . The median time of recovery was 38 min. Transient mild oxygen desaturation occurred in three patients (15%) and responded easily to airway repositioning. No assisted ventilation or supplemental oxygen was needed. One patient vomited.
A blinded randomized trial compared ketofol to propofol for ED PSA in children and adults (median ages 20 and 22 years) [366]. All received 0.5–1 mcg/kg fentanyl 5 min prior to sedation. Then either 0.5 mg/kg of ketamine or saline was infused followed by propofol 1 mg/kg. Repeated doses of propofol 0.5 mg/kg were administered as needed to attain or maintain deep sedation. Respiratory depression was similar between the groups (22% vs 28%). They found the combination of ketamine and propofol resulted in greater provider satisfaction and perhaps better sedation quality.
Finally, a randomized trial compared ketamine alone to ketofol for fracture reduction in 183 children [427]. Ketamine 1 mg/kg or ketamine + propofol, 0.5 mg/kg each, was administered with additional doses as needed. There was no difference in adverse events except nausea was more common with ketamine alone. Efficacy of sedation was higher in the ketamine alone group (99 vs 90%). These studies found similar results to trials in adults [370,371,369].
Although coadministration of ketamine with propofol enables use of smaller doses of both propofol and ketamine to achieve effective sedation, it is unclear that the slightly faster recovery with this more complex technique in children is clinically significant and needs further evaluation.
Ketamine Plus Dexmedetomidine (Ketadex)
Coadministration of ketamine and dexmedetomidine has been found to reduce or prevent the tachycardia , hypertension, salivation, and emergence phenomena seen with ketamine and the bradycardia and hypotension/hypertension seen with dexmedetomidine in children undergoing cardiac procedures and lithotripsy [370]. However, no studies have been conducted to date evaluating this combination for ED PSA in children, perhaps because recovery is prolonged.
Nitrous Oxide (N2O)
Nitrous oxide (N2O) is a colorless, odorless, and tasteless gas that, in a linear dose–response pattern, induces dissociative euphoria, drowsiness, anxiolysis, and mild to moderate amnesia and analgesia with onset and offset of effects within 2–5 min [319, 320]. N2O is blended with oxygen (N2O/O2) and typically is described by the N2O component: “70 % N2O” is 70% N2O = 30% O2 [321]. At a specific concentration of N2O, however, depth of sedation can vary considerably. One study of N2O for ED PSA found 90% of children receiving 50–70% N2O were mildly sedated (drowsy, eyes open or closed, but easily aroused to consciousness with verbal stimulus), whereas moderate or deep sedation occurred in 3% receiving 70% N2O and in none receiving 50% [322]. Others report 2–10% of children may be poorly sedated during ED PSA with N2O [10, 322, 323].
Since N2O sedation and analgesia are usually mild to moderate, children are partially aware, and strategies to enhance the gas’s anxiolytic, dissociative, and euphoric effects are vital to successful use for PSA. Guided imagery significantly augments N2O’s efficacy and helps allay anxiety [320, 324]. Children naive to intoxication are frequently frightened by the floating or tingling sensations caused by the gas, but they readily accept these effects when incorporated into non-frightening scenarios. The author often encourages preschool and school-aged children to imagine flying to a favorite or imaginary place, “soaring with eagles, past clouds and stars to check out the moon,” guiding the child during the sedation by detailed descriptions of what might be “seen” along the way. Alternatively, some children like describing their own imaginings, allowing the author to figuratively “tag along,” as with a 5-year-old girl who portrayed in great detail her “chocolate ponies” as her radius fracture was being reduced. Finally, some older children and teenagers prefer the partial awareness with N2O sedation as they, like many adults, fear loss of vigilance or control associated with potent sedation or anesthesia.
Effective pain reduction by concurrent use of local anesthesia and/or systemic analgesia for painful procedures is also crucial for successful N2O ED PSA [325]. For example, forearm fractures can be reduced with minimal distress when N2O sedation is augmented by a lidocaine hematoma block [88, 326, 327] or lacerations repaired calmly in young children when they have also received topical anesthetic [10]. The lack of painful administration or need for venous access and the rapid onset and offset of effects make N2O ED PSA an attractive option for many clinical situations.
N2O can safely be administered by specially trained nurses to healthy children for ED PSA [62, 328, 329].
Indications
N2O , along with local anesthesia and/or oral analgesics, primarily is used for anxiolysis, mild analgesia, and amnesia during brief (<5–10 min) procedures, such as laceration repair, abscess incision and drainage, lumbar puncture, IV placement, and some fracture reductions [431, 436,437,435]. Use of 60–70% N2O or coadministration of opioids such as intranasal fentanyl or oral oxycodone or sedatives may deepen sedation and improve efficacy [129,130,131, 343,344,342, 428]. Coadministration of an opioid with N2O, however, increases the likelihood of emesis from about 10% to about 25% [88, 428]. However, N2O sedation for very painful procedures is limited unless local anesthesia can be used [325]. The author frequently administers oxycodone 0.2 mg/kg orally 30–60 min prior to N2O sedation for I&D of an abscess in toddler and preschool children. Although seldom seen, these children are monitored for respiratory depression before, during, and after the sedation.
Many find the gas more effective in children old enough to cooperate and use imagination, but significant reduction of procedure-related distress has been observed in 2-year-old and younger children [10]. In the author’s ED, N2O sedation is regularly used effectively in infants of 3 months of age and older by administering with a continuous-flow system, described later.
Suturing-related distress in children can be reduced by N2O [10, 323, 333,334,332]. We found 2- to 6-year-old children who had received topical anesthetic and were viewing cartoons with a parent at the bedside had less distress during wound cleaning, supplemental lidocaine injection, and suturing if receiving 50% N2O instead of oral midazolam. Children who received N2O alone recovered rapidly without ataxia or dizziness, but did have more vomiting (10%) [10]. Of note, 30% N2O was found insufficient in children younger than 8 years old in another study [330].
Mid to distal forearm fracture reduction can be effectively performed with N2O sedation, particularly when combined with a local anesthetic hematoma block [88, 326, 327, 336,337,335, 398,399,397, 432]. We found N2O plus 1% lidocaine hematoma block (2.5 mg/kg, maximum 100 mg) as effective as intravenous ketamine in reducing distress during fracture reductions in children aged 5–17 years. This technique is often most effective in displaced mid to distal forearm fractures that have large fracture site hematomas that enable effective hematoma blocks, whereas torus or greenstick fractures that require reduction likely have small or no fracture hematomas making the lidocaine block less effective; an effective fracture hematoma block is the key for maximum success. For these incomplete fractures, hematoma blocks may provide partial pain relief and, combined with 70% nitrous oxide along with prior oral oxycodone or another potent analgesic, enable many children to tolerate fracture reduction with acceptable distress. The child usually recalls less pain related to the fracture reduction performed with N2O sedation than an observer would expect based upon the child’s response during the procedure [326]. It is usually reassuring to ask the child after recovery, with the parent(s) present, what he or she recalls of the procedure, especially when the parent was present during the reduction and the child had manifested some distress. Recovery is markedly faster from N2O compared to ketamine-based sedation for fracture reduction (16 versus 83 min) [88]. If the N2O is turned off as soon as any painful molding of the cast at the fracture site after reduction is completed, the patient is typically recovered to near baseline before the casting or splinting is finished.
Children’s distress during other painful ED and outpatient procedures such as lumbar puncture, abscess drainage, dressing change, and intravenous catheter placement likewise can be reduced by N2O [322, 332, 339,340,341,342,343,341]. Recovery from N2O sedation typically is very rapid, with the child able to sit alone within 5 min and ready for discharge within 15 min.
Technique
As described previously, successful N2O sedators engage the child in imaginative stories throughout the procedure. Distraction, imagery, and storytelling significantly enhance desired effects by giving the child a nonthreatening construct in which to place the sensations caused by the gas. While breathing N2O , children are able to follow commands, describe sensations of floating, frequently laugh, and occasionally chew or lick masks that have been scented with bubblegum spray or flavored lip-balm to enhance acceptance of the mask. Adolescent and school-aged children often begin giggling if it is suggested to them that this is expected, and their parents typically also begin laughing when this occurs, presumably easing their own anxiety. Coaxing children as young as 2 years of age to hold the mask on their face adds a measure of safety by allowing them to remove the mask quickly if vomiting occurs. Their ability to hold the mask also indicates their depth of sedation and may reduce anxiety related to the mask covering their mouth/nose. When the mask is held in place by a sedator, that person must be vigilant for evidence of vomiting and quickly remove the mask to allow the child to clear the emesis.
Titration of the gas beginning at 30%, the anxiolytic dose, and increasing the concentration to 50–70% over 2 min may reduce children’s fear during induction. Others find when children have been prepared with explanations about what effects they are likely to feel, they tolerate beginning at 50–70%. With either technique, the child should breathe the maximum concentration desired for 1–2 min, allowing full effect, before beginning the procedure.
Administration of 100% oxygen after cessation of N2O to prevent “diffusion hypoxia” is unnecessary unless the patient is emerging from deep sedation or general anesthesia. N2O diffusing from the bloodstream into the alveoli and displacing oxygen is readily exhaled without causing hypoxia in patients recovering from sedation with N2O alone [128, 342, 343]. However, continuing 100% oxygen for 2–3 min after cessation of N2O is recommended to scavenge the N2O being exhaled by the patient [429]. As with any sedation technique, children should be monitored with pulse oximetry until alert, usually less than 3–5 min after ending N2O administration.
Delivery System
Delivery of N2O (fixed at 50%) in the ED historically has been by demand-valve systems designed for adult use (Nitronox/Entonox®). Children have difficulty generating the negative inspiratory pressure required to initiate gas flow with these devices. Continuous-flow systems, such as those used by dentists, oral surgeons, and anesthesiologists, in contrast, provide free flow of gases with the ability to deliver up to 70% N2O. These systems allow normal respirations and are easily used by patients of all ages [321, 344]. Dental systems with nasal hoods can be adapted for use with a full face mask by adding into the expiratory limb an open gas interface designed for anesthesia machines. Note, however, delivery systems that utilize dental nasal masks do not deliver N2O effectively. A study of children breathing N2O through a nasal mask found that end-expired alveolar N2O concentrations were, on average, 63% below flowmeter settings [429]. With administration of 50% N2O, an end-expired N2O saturation maximum of only 11% was attained after 90 seconds. Continuous-flow systems that use a full face mask have recently become available in the United States. N2O concentration is limited to a maximum of 70–75% as concentrations exceeding 79% (+21% O2) would cause hypoxia. Accidental administration of 100% N2O due to machine or system failure can be rapidly lethal [345, 346]. Providers must be very familiar with the mechanisms of the N2O delivery system used. A machine or systems check should be performed before each use of N2O to assure proper function of the machine and monitors.
A scavenging device should be an integral part of the delivery system to minimize ambient levels of N2O gas exposure to healthcare workers since chronic and repeated exposure to N2O may cause abnormalities in hematologic, neurologic, and reproductive systems (see cautions). The N2O delivery device and the treatment area in which it is used should be in compliance with National Institute of Occupational Safety and Health Standards and state safety guidelines and regulations [347]. It is beneficial to have room air exchanges of at least 10–20/h in treatment rooms to remove any N2O that has escaped the scavenging process.
Monitoring
An in-line oxygen analyzer should be used to assure proper equipment functioning/adequate oxygen delivery during N2O administration [59]. A gas analyzer that measures inspiratory and expiratory N2O and end-tidal CO2 concentrations adds additional assurance of patient safety and equipment function.
Administration of ≤50% N2O, without any other sedative , narcotic, or respiratory depressant drugs, to children ASA-PS Class I or II is considered minimal sedation, and the patient may be monitored by direct visualization and intermittent assessment of their level of sedation [59]. The child should be able to be verbally interactive throughout the sedation. If >50% N2O is administered or if the patient receives concurrent narcotic or other sedative drugs, the patient should be observed for moderate sedation and monitoring escalated accordingly if that should occur. Since oxygen is blended with N2O, even mild hypoxemia is very unlikely and should cause immediate investigation to determine the cause.
Contraindications/Cautions
At normal atmospheric pressure, N2O cannot induce general anesthesia, unless combined with other agents. N2O at 30–70% has been safely used widely for more than a century to reduce distress in children during dental procedures [348]. Review of nearly 36,000 administrations of 50% N2O for nondental procedures, 82% of which were in children, found 9 (0.03%) serious adverse events (somnolence, vomiting, bradycardia, vertigo, headache, nightmares, sweating) that may have been attributed to the N2O [349]. In healthy patients (ASA-PS I, II), N2O has minimal cardiovascular or respiratory effects [78, 130, 342]. N2O, however, may enhance the depressed response to hypoxia and hypercarbia induced by other agents [129,130,131, 322, 350].
N2O diffuses rapidly into air-filled cavities causing volume and/or pressure increases proportional to concentration and duration of N2O inhaled. Therefore, N2O should not be administered to patients with areas of trapped gas such as pneumothorax, obstructive pulmonary disease, or bowel obstruction. Albeit seemingly rare, patients with acute otitis media may experience painful increase in middle ear pressure. Other relative contraindications include significant head injury (N2O mildly increases intracranial blood flow), altered mental status, and psychiatric disorder (N2O may cause dysphoric effects similar to ketamine).
Bone marrow suppression; liver, CNS, and testicular dysfunction; decreased fertility and increased spontaneous fetal loss; and peripheral neuropathy may possibly occur with repeated and chronic exposure [331, 431]. None of these adverse effects have been found when scavenging devices are integrated into the system. Therefore, use of a scavenging device is essential to minimize ambient levels of gas and exposure to healthcare workers.
Deaths associated with N2O use have been due to inadvertent administration of 100% nitrous oxide, with subsequent hypoxia [345, 346]. These occurrences primarily were in patients already sedated with other drugs as part of anesthetic regimens. These tragedies point out the essential need for clinicians to understand all aspects, including mechanical, of the gas delivery device being used.
Pregnancy Category C
-
Adverse effects : Vomiting occurs in approximately 10% of children receiving 50% N2O, along with transient dizziness and headache in some [78]. These effects usually resolve within 5 min of cessation of N2O administration. Vomiting frequency increases with opiate and decreases with midazolam coadministration [10, 88]. Some providers believe the risk of vomiting increases when the duration of administration exceeds 5–10 min, especially with greater than 50% concentrations, but this is yet to be substantiated. Coadministration of ondansetron has been found to have no effect on the frequency of emesis when nitrous oxide is administered with intranasal fentanyl [430]. Protective airway reflexes are largely intact when N2O is used alone [354,355,353]. Whether combining N2O with other sedatives or analgesics increases risk for aspiration and other adverse events is unknown, but the risk likely correlates with the patient’s depth of sedation and effects of the coadministered drug.
-
Dosages : Concentrations of 30–50%, blended with oxygen, achieve minimal to light moderate sedation in most children without adverse cardiopulmonary effects [59]. More recently, routine use of 60–70% has been recommended and found safe in children undergoing sedation in the ED [322]. In the author’s ED, 50–70% concentrations are typically used with initial higher concentrations and then reduced as the most painful part of the procedure is accomplished.
-
Onset/duration : Patients experience the effects of N2O within 1 min, but for optimum effect, they should inhale the gas for 2–3 min before beginning a procedure to allow brain concentrations to equilibrate with the delivered concentration of gas. Recovery occurs rapidly with children being able to sit alone by 3–5 min after cessation, but initially they should be assisted with walking as ataxia may occur for a bit longer.
-
Mechanism of action : N2O has NMDA glutamate receptor antagonist, opioid agonist, and GABAergic effects [357,358,356].
-
Metabolization : N2O is excreted unchanged by exhalation.
Dexmedetomidine
Dexmedetomidine is an alpha-2 adrenergic agonist that binds CNS and peripheral receptors to mimic natural sleep with anxiolytic, amnestic, and mild analgesic effects without impacting ventilation [436, 437]. Patients sedated with lower doses of dexmedetomidine can be readily aroused to a comprehensible state, unlike with that from benzodiazepines or barbiturates. It can cause initial depression and then elevation (up to 30%) of blood pressure and heart rate, neither of which usually result in need for intervention. Effective ventilation is maintained during deep sedation. Airway tone is maintained resulting in children with obstructive apnea needing less airway support than during sedation with other agents [440,441,439]. Dexmedetomidine infusions do not appear to affect intracranial perfusion, including in patients with severe head trauma. Of note, unlike other agents used for sedation and anesthesia, dexmedetomidine may have neuroprotective effects against central nervous system neuronal apoptosis.
Despite lack of formal approval for use in children, pediatric applications of dexmedetomidine are increasing. Most commonly used intranasally for preoperative anxiolysis and intravenously as a continuous infusion in regimens for general anesthesia or sedation of intubated patients, it is also increasingly used intravenously as a single agent or coadministered with other sedatives for prolonged nonpainful procedures which require children to be motionless such as MRI or CT scans [436, 437, 440]. Dexmedetomidine can be administered by intramuscular, intranasal, buccal, or oral routes although bioavailability by the oral route is poor [444,445,446,447,445]. Intranasal and buccal routes have been found to be effective in children with developmental delay including autism [449,450,451,449]. IN dexmedetomidine 3 mcg/kg plus buccal midazolam 0.2 mg/kg was more effective in autistic children than dexmedetomidine alone [450]. Dexmedetomidine has some opioid-sparing effects, but as a single agent, it is generally ineffective for painful procedures. Coadministration of ketamine or use of local anesthetics with dexmedetomidine may be an option for ED PSA, but this technique needs further investigation [370].
Techniques
Intravenous Administration
Dexmedetomidine, usually 2–3 mcg/kg, is recommended to be infused intravenously over 10 min to minimize changes in blood pressure and heart rate. This induction dose is then followed by a maintenance infusion of 1–2 mcg/kg/hour for longer procedures such as MRI studies [436, 440, 451]. For short procedures, a single dose of 2 mcg/kg has shown to be effective. More rapid infusion of smaller doses has been reported to be well tolerated in children under general anesthesia, but this needs further study [452, 453]. Overall, the beneficial effects of dexmedetomidine make it an attractive option for sedation, but prolonged onset , typically 12–14 min, and recovery, typically 25–35 min, make it less desirable for many short procedures in the busy ED environment [436, 440, 448].
Intranasal Administration
Intranasal (IN) dexmedetomidine, unlike midazolam, is not irritating to the nasal mucosa. A systematic review of studies of IN dexmedetomidine in children identified 19 trials and concluded IN dexmedetomidine is more likely to provide effective sedation than oral chloral hydrate or oral midazolam [454]. Compared to intravenous infusion over 5 min , bioavailability of dexmedetomidine administered to adults was estimated for the following routes: intranasal (65%), buccal (82%), intramuscular (104%), and oral (16%) [455]. Also in adults, IN dexmedetomidine plasma concentrations peaked at 38 min with onset of sedation at 48–60 min [456]. In 18 children in the preoperative setting, plasma concentrations peaked by 47 min after 1 or 2 mcg/kg IN dexmedetomidine with bioavailability of 84% compared to intravenous infusion over 10 min [457]. The plasma concentrations in infants and toddlers neared the minimum concentration for sedation within 20 min of IN administration of 1 mcg/kg and within 10 min with 2 mcg/kg.
Effective sedation for CT studies occurred with IN dexmedetomidine 2.5 mcg/kg in 60 children, mean age 17 months [445]. The average time to sedation was 13 min and to recovery was 90 min. Decreases greater than 20% in heart rates occurred in 15% of children and in blood pressures in 2%, whereas increases greater than 20% in heart rates and blood pressures occurred in 3%. No child required intervention for these changes. In 50 children undergoing MRI studies, ages 4 months–11 years, IN dexmedetomidine 2–3 mcg/kg found that older children had lower peak concentrations and 94% of all children needed additional sedation with thiopental indicating IN dexmedetomidine insufficient as a single technique for these longer studies which lasted an average of 40–45 min [458]. It is unknown whether IN dexmedetomidine as a single technique may be sufficient for recently developed shorter MRI studies.
A comparison of IN dexmedetomidine 2 mcg/kg to IN midazolam 0.4 mg/kg for anxiolysis for laceration repair in 40 children 1–5 years of age found 70% of children who received dexmedetomidine were not anxious when positioned for the procedure compared to 11% of those who received midazolam [459, 464]. Topical and local anesthesia were used, and time to discharge was similar in both groups.
IN dexmedetomidine has been shown to reduce distress during venous catheter insertion. A preoperative study of children, mean ages 4 years, compared IN dexmedetomidine 1 mcg/kg to placebo for distress reduction during venous catheter insertion through topical anesthetic [460]. Of those who received IN dexmedetomidine, 94% became satisfactorily sedated (asleep but responding, or not, to mild prodding) with a mean onset time of 25 min and duration of 85 min. At the time of catheter insertion, 82% of the children were anxious but reassurable or calm and cooperative versus 57% in the placebo group. In the dexmedetomidine groups, the maximum mean drop in blood pressure was 13%, peaking at 60 min, and in heart rate was 15%, peaking at 75 min. A comparison of IN dexmedetomidine 2.5 mcg/kg to oral midazolam 0.5 mg/kg also found less distress with IN dexmedetomidine during venous catheter insertion in children undergoing CT studies [461].
Intramuscular Administration
IM dexmedetomidine, mean dose 2.4 mcg/kg for CT scans and 2.9 mcg/kg for MRI scans, provided adequate sedation in 65 children, mean ages 2–3 years, by 13 min for scans not requiring intravenous contrast. Mean length for CT scan was 3 min and for MRI scan 20 min. Recovery occurred within 20 min after the scans. A 2nd dose was needed in one patient in the MRI group and three in the CT group. A drop in blood pressure of 20% or more occurred in 14% without bradycardia, hypertension, or oxygen desaturation [439]. IM dexmedetomidine can also provide effective sedation for EEG without interfering with the EEG measurements [443].
Monitoring
All patients sedated with dexmedetomidine should be monitored as recommended for the depth of sedation achieved. Decreases and increases in blood pressure and heart rates are to be expected and do not require intervention unless signs of poor perfusion are present. Administration of normal saline prior to sedation may reduce these changes in children who have been fasted for prolonged periods.
Pregnancy Category C
Metabolism
Dexmedetomidine is metabolized by glucuronidation in the liver to inactive metabolites. A small fraction is excreted unchanged in the urine and feces [437].
Contraindications/Cautions/Adverse Effects
Dexmedetomidine should be administered with caution or avoided in children receiving digoxin, ß-adrenergic blockers, calcium channel blockers, or other agents that predispose to bradycardia or hypotension. Treatment of dexmedetomidine-induced bradycardia with glycopyrrolate or atropine has been reported to cause significant hypertension and asystole in one adult. Dexmedetomidine may also increase pulmonary vascular resistance in children with pulmonary hypertension [436]. Tenfold and 60-fold overdoses in two children have been reported with neither case developing cardiorespiratory demise, but recovery was prolonged [437].
Ketamine + Midazolam or Fentanyl + Midazolam Techniques for Deep Sedation
Providers utilizing these regimens should be thoroughly familiar with these medications and sedation guidelines outlined in text. Sedation should be performed in an area fully equipped for resuscitation.
Pre-sedation Assessment and Preparation
-
1.
Initial assessment : Determine patient’s ASA classification, airway risks, and time of last oral intake, and obtain informed consent.
-
2.
Establish indwelling venous access maintained with normal saline or Ringer’s lactate.
-
3.
Attach patient monitors to continuously measure patient’s oxygen saturation (with variable pitch indicator), heart rate, and respiratory rate and intermittently measure blood pressure . Consider preoxygenation and supplemental oxygen delivery during the sedation if capnography is available and staff trained in use.
-
4.
Prepare CPAP ventilation bag and mask; assure ability to deliver supplemental oxygen.
-
5.
Prepare oral suctioning device with rigid tip.
During Sedation
-
1.
Assign a provider whose sole responsibility is to monitor patient safety.
-
2.
Continuously monitor patient by direct observation; monitor oxygen saturation (with variable pitch indicator), HR, and RR; and monitor blood pressure after each medication infusion and at 5 min intervals. Patient monitoring and direct observation at increasing intervals is continued during recovery until discharge criteria are met.
-
3.
Infuse medications near the hub of the catheter over 10–20 s, in small incremental doses to titrate to desired endpoint of analgesia, sedation. Use of dilute solutions and precalculated dosage tables based upon patient weight is recommended.
-
4.
Administer medications when supportive staff is present and prepared to render support if necessary and provider prepared to begin and perform the procedure.
Fentanyl Technique
-
(a)
Midazolam: 0.05–0.1 mg/kg (0.05–0.1 mL/kg) at 2–3 min intervals; endpoint, decreased patient anxiety, mildly slurred speech, drooping eyelids; typically effective dose, not more than 0.1 mg/kg to induce marked amnesia along with sedation.
-
(b)
Fentanyl (10 mg/mL): 0.5 mg/kg (0.05 mL/kg) at 2–3 min intervals; endpoint, decreased patient responsiveness to painful stimulus or decreasing oxygen saturations; typically effective dose, 1–1.5 mg/kg.
Ketamine Technique
-
(a)
Midazolam may be reserved for anxious patients undergoing ketamine sedation. For anxiolysis, dose, 0.05 mg/kg; maximum dose, 2 mg; single administration, 5–15 min prior to initiation of sedation.
-
(b)
Ketamine (10 mg/mL): dose, 0.5–1 mg/kg (0.05–0.1 mL/kg), maximum dose ~50 mg, can be rapidly infused; infuse additional doses at 1 min intervals if needed; endpoint, decreased patient responsiveness to painful stimulus; typically effective total dose, 1–2 mg/kg. Supplemental doses of 0.5 mg/kg may be administered as indicated by patient distress.
Consider using an antisialagogue (e.g., glycopyrrolate 5 mg/kg or atropine 0.01–0.02 mg/kg) prior to ketamine administration if it is an anticipated procedure that will require multiple supplemental doses of ketamine.
Caution
Suggested doses may readily result in oxygen saturation falling below 90% in patient’s breathing room air, particularly when fentanyl is used. Providers must be prepared to immediately turn the patient to his side if vomiting, reposition or suction patient’s airway, and provide supplemental oxygen or positive-pressure ventilation until patient has returned to baseline physiological status and recovered from sedation.
Conclusion: Final Thoughts
This chapter has presented the sedation provider with a range of sedation techniques and options for painful and nonpainful procedures that may need to be performed on an urgent basis. There is no doubt that sedation and analgesia are important components of the emergency department care and should be an integral component of the emergency medicine physician’s practice. The training and credentialing process for sedation is an area of recent interest from the American College of Emergency Physicians. In July 2011, the American College of Emergency Physicians released a policy statement entitled Procedural Sedation and Analgesia in the Emergency Department: Recommendations for Physician Credentialing, Privileging, and Practice [359]. This policy iterated that the chief of the emergency medicine service at each institution will be responsible for establishing criteria for credentialing and recommending emergency physicians for sedation privileges. Sedation training should “focus on the unique ED environment.” This policy is important, because it empowers the chief of emergency medicine with the responsibility of establishing sedation training and credentialing requirements for the emergency medicine specialty. Furthermore, the policy expands the role of the emergency physicians as well as emergency medicine nurses by condoning the capability of qualified ED nurses to “administer propofol, ketamine, and other sedatives under the direct supervision of a privileged emergency physician.” The policy also recognizes that there may be occasions whereby the emergency medicine environment may not lend itself to having a separate physician administer the sedative and another to perform the procedure: For these situations, the policy states “Deep sedation may be accomplished…by the same emergency physician both administering sedation and performing the procedure.”
As the practice of sedation evolves, one can anticipate that the American College of Emergency Physicians will continue to survey the landscape, evaluate the literature, and recommend policies and guidelines to promote the safe and efficacious delivery of sedation in the emergency medicine environment.
Case Studies
Case 1
A 12-year-old boy has closed displaced metaphyseal fractures of his distal right radius and ulna and numbness in his 3rd and 4th fingers. He fell 30 min ago running in gym class and has no other injuries. He takes methylphenidate for attention deficit hyperactivity disorder (ADHD). He otherwise is healthy and has never received sedation or anesthesia. He ate lunch 2 h prior to arrival and was given ibuprofen by his mother on the way to the hospital. He is anxious and crying in triage.
Issues
Pain relief now and during radiographs and exams; PSA for fracture reduction with consideration of his fasting status, anxiety, ADHD, and neurovascular status of his injury:
-
1.
Pain relief will facilitate imaging of the fractures, accurate assessment of the injury, and preparation of the patient for PSA for fracture reduction. Options include:
-
(a)
Splinting the injured area to prevent movement of the fractured bones provides significant pain relief.
-
(b)
Systemic analgesia: Administer before radiographs, even if the child indicates less pain after splinting. Repositioning of the injured limb for radiographs and subsequent exams will be quite painful. Options include:
-
Oxycodone orally: In our ED, nurses follow standing orders to administer a first dose of oxycodone 0.2 mg/kg orally (maximum dose 10 mg) in triage to children with a potential isolated extremity fracture or another painful injury. This allows rapid and effective attention to the reduction of pain and high patient, family, and staff satisfaction. Noticeable analgesia occurs by 20–45 min with peak effect by an hour and with duration of 2–4 h. This dose is unlikely to cause sedation in children with painful injuries. Doses for home use are 0.05–0.15 mg/kg. Oxycodone is preferred over codeine because it does not require metabolic conversion for analgesic effect. Codeine is slowly or poorly converted to morphine in 2–40% of patients and thus provides poor or no pain relief to such children. If codeine previously has been effective for a specific child, a first dose of codeine 2 mg/kg orally is effective for these painful injuries with subsequent or home doses of 1 mg/kg.
-
Fentanyl intranasally, 1.5–2 mg/kg, achieves significant pain relief within 5–10 min with duration of 30–90 min. Use atomizer to spray small volumes of concentrated intravenous fentanyl solution (50 mg/mL) to improve absorption. Divide total dose into repeated sprays of ~0.1–0.2 mL/nostril. Use of small volumes reduces drainage of drug into posterior pharynx where it is less absorbed. If a wide margin of safety is determined after more extensive use of this technique, it might be performed by nurses in triage, but currently it is performed by a physician in a treatment room with patient monitoring for respiratory depression.
-
Opioids intravenously titrated to effect will provide the greatest pain relief. Fentanyl 1–2 mg/kg IV will provide analgesia within 1–2 min, lasting 30–60 min, whereas morphine 0.1 mg/kg IV will provide initial analgesia within 5–10 min with peak effect at 10–20 min and lasting 2–3 h. This strategy requires IV insertion, typically in a treatment room after physician assessment and orders. Anxiety and pain associated with catheter insertion are significant for many children and are greatly reduced by use of local anesthesia such as buffered lidocaine injected subcutaneously via a 30-gauge needle at the site of insertion.
-
Nitrous oxide 50–70% provides rapid pain relief. However, because continued analgesia requires ongoing administration and N2O scavenging systems are not mobile, a longer-acting systemic analgesic usually is needed. One strategy is to use N2O to reduce the patient’s pain and distress while an IV catheter is inserted for subsequent opioid administration. This strategy typically requires physician assessment and orders, access to N2O, and IV catheter insertion in a treatment room.
-
-
(a)
-
2.
Fasting status: This child ate lunch 2 h prior to his arrival. Pain from injury and opioid analgesics unpredictably slow intestinal motility. It is uncertain if delaying sedation for 2–4 h in these patients will allow significant additional gastric emptying. Vomiting with PSA does not correlate with the length of fasting. Furthermore, ED PSA does not involve tracheal intubation, a procedure that significantly increases risk of pulmonary aspiration during general anesthesia. Of note, pulmonary aspiration has not been reported in children undergoing ED PSA, despite most being incompletely fasted. As with general anesthesia, no studies have determined if pulmonary aspiration risk is reduced in non-fasted patients by pre-sedation administration of medications to enhance gastric emptying, inhibit gastric acid production, or decrease pH of gastric contents, and such strategies are not recommended. The author’s practice is to use PSA techniques that preserve airway reflexes as described herein, to be prepared for vomiting in all patients, and to perform PSA when the full complement of providers is available to perform the procedure and monitor the patient.
-
3.
PSA techniques: Since this non-fasted patient has potentially increased risk of pulmonary aspiration of gastric contents, a sedation technique that better preserves protective airway reflexes may increase patient safety. Ketamine and N2O are NMDA receptor antagonists that blunt protective airway reflexes less than the opioid and GABAergic agents such as fentanyl, midazolam, and propofol:
-
(a)
Nitrous oxide (50–70%) plus lidocaine fracture hematoma block, along with oxycodone administered at triage, is as effective in reducing distress associated with fracture reduction as intravenous ketamine, provided an effective hematoma block is placed. To reduce risk of nerve and vascular injury from injection, hematoma blocks are typically reserved for mid to distal forearm and, occasionally, ankle fractures. We administer 50% N2O to the child as the orthopedic surgeon, using sterile technique and a dorsal approach, injects 1% buffered lidocaine (2.5 mg/kg or 0.25 mL/kg, maximum dose 100 mg or 10 mL) into the fracture hematoma. N2O 70% is usually administered for the subsequent fracture reduction. Aspiration of hematoma blood into the lidocaine-containing syringe confirms proper location of the needle for injection. Perhaps counterintuitively, the worse the fracture, the more effective is fracture site anesthesia due to larger hematomas. The provider must be prepared for as yet unreported but potential seizure or dysrhythmia due to rapid intraosseous absorption of lidocaine. This theoretical risk is low since the injected lidocaine is within the drug’s therapeutic dose range. Some orthopedic surgeons prefer not to use this technique if the fracture and swelling cause numbness in the hand, typically median nerve distribution, because of inability to reassess nerve function immediately postreduction. Use of lidocaine instead of longer-acting local anesthetics such as bupivacaine enables postreduction neurologic assessment within 1–2 h. Variable patient awareness is present with N2O PSA; thus distraction and guided imagery are crucial to improve efficacy of this technique. Some older children and teenagers, as many adults, prefer not to be unconscious during a procedure if pain is sufficiently reduced.
-
(b)
Ketamine IV with or without midazolam more effectively reduces patient distress during intensely painful procedures and causes less respiratory depression than fentanyl- or propofol-based techniques. Intravenous administration is preferred because multiple attempts likely will be needed to align both the radius and ulna, thus increasing potential need for additional doses of ketamine. Time of recovery is reduced by administering a smaller initial dose followed by a half dose. For a child of this age, an initial ketamine dose 1 mg/kg followed by 0.5 mg/kg at 8 min likely results in approximately 15 min of very deep sedation with recovery to drowsiness and easy arousal by verbal stimulation by about 30 min. If longer deep sedation is needed for repeated reduction attempts, additional dose of 0.5 mg/kg can be given as needed. Alternatively, an initial ketamine dose of 1.75 mg/kg will result in 15 min of deep sedation, but recovery likely will take 60–70 min.
-
Intramuscular ketamine 4 mg/kg provides effective PSA without vascular access, but additional doses, if necessary, will require 4–5 min to determine if sufficient. Recovery is significantly longer than with intravenous ketamine, and vomiting is more frequent (26% versus 12%). Ability to obtain vascular access emergently (intraosseous, if necessary) must be present to manage life-threatening adverse events should they occur.
-
Midazolam 2 mg total dose may reduce the child’s anxiety as preparations are made for PSA. Although yet unconfirmed with PSA, reduced anxiety at induction correlates with reduced dysphoria during recovery from general anesthesia. This small dose is not likely to cause respiratory depression or prolong recovery. Midazolam administered in the same syringe or immediately after ketamine does not appear to reduce recovery dysphoria.
-
Glycopyrrolate or atropine to reduce ketamine-associated increased salivation is recommended by some to reduce the low risk of laryngospasm. Hypersalivation is usually not significant with these doses of ketamine but may occur with repeated doses for prolonged procedures . The author no longer routinely administers an antisialagogue because these agents have been associated with increased likelihood of adverse respiratory events, and patients complain of dry mouth after recovery.
-
Vomiting: Administration of opioids such as morphine or oxycodone with ketamine increases emesis (10% versus 25%), whereas administration of midazolam decreases vomiting (19% versus 10%) as does ondansetron (13% versus 5%).
-
Cautions: Although unlikely to occur, providers must be prepared for hypoventilation , apnea, or laryngospasm with ketamine. As with all deep sedations, this child must be monitored for adverse effects by an experienced dedicated provider during induction, sedation, and recovery. If vomiting occurs, the procedure immediately is interrupted and the child turned to his side to assist his clearing emesis. Observers (e.g., parents) should be forewarned about nystagmus and catatonic stare during sedation and possible dysphoria during recovery. Similarly, patients should be prepared for possible diplopia, dizziness, hallucinations, and a brief period of blindness during recovery. Getting the child to focus on pleasant thoughts during induction and recovery may reduce some of these psychotomimetic effects. Most patients will have no memory of even intensely painful procedures, even if they occasionally moan, but some will have partial recall, usually quite vague. It may help reassure observers if the child indicates no recall when asked after recovery.
-
-
(c)
Fentanyl + midazolam or propofol provides effective PSA but blunts protective airway reflexes more than ketamine. This child’s recent food intake makes these techniques less desirable. It is unknown whether delaying PSA will improve gastric emptying. Please see Fasting Status mentioned previously.
-
(d)
Reduction under general anesthesia may be considered. However, reduction should not be delayed long because of the apparent median nerve impingement. Of interest, general anesthesia with endotracheal intubation in non-fasted children may have greater risk of pulmonary aspiration than ED PSA.
-
(a)
Case 2
A 5-year-old girl has a closed distal radius fracture, dorsally angulated 30° but hinged at the cortex. She gets “car sick” and had multiple episodes of vomiting after an operation last year.
Issues
Pain management, history of motion sickness, and postanesthesia vomiting and optimum technique for a painful but brief fracture reduction. Of note, in young children, some orthopedic surgeons do not reduce metaphyseal fractures “minimally displaced” in the primary plane of motion because they will remodel to normal over the coming months. Standardized determination of how much displacement will successfully remodel remains to be developed:
-
1.
Pain relief: Please see Case 1. Splinting and oral oxycodone likely are sufficient.
-
2.
PSA technique options: Since this fracture reduction will take “one brief but painful push,” effective local anesthesia or brief deep sedation with rapid recovery is desirable:
-
(a)
Nitrous oxide (50–70%) plus fracture hematoma lidocaine block: This fracture may not have a significant hematoma, thus reducing the effectiveness of a hematoma block. Combining 70% N2O with oxycodone, 0.2 mg/kg orally without the hematoma block, may provide sufficient analgesia and partial amnesia for remaining pain. N2O should be administered for at least 2 min prior to reduction to maximize the gas’s effects. Balancing potentially incomplete PSA against the benefits of not needing vascular access and rapid recovery should be discussed with the parents. A downside to this technique is the 25% likelihood of vomiting when N2O is coadministered with an opioid. Coadministration of oral midazolam with N2O (without oxycodone) reduces vomiting but prolongs recovery. It is unknown if oral ondansetron significantly reduces vomiting with N2O and oxycodone.
-
(b)
Ketamine with or without midazolam intravenously: Since this fracture reduction will likely be very brief, experienced providers may consider rapid administration of ketamine 0.5–0.75 mg/kg (pushed over 3–5 s) to induce about 5 min of deep sedation, with additional ketamine given if necessary. The performer of the fracture reduction should be ready as the ketamine is infused. With the single small rapid dose, deep sedation will occur within 1 min, and recovery to being drowsy but responsive to verbal stimulation will occur by 10–15 min, often as casting is completed. Alternatively, administered over 30–60 s, ketamine 1.25 mg/kg provides deep sedation for 10–15 min with recovery by about 30 min or ketamine 2 mg/kg provides deep sedation for 15 min with recovery by an hour. Vomiting frequency after small dose ketamine is unknown. See Case 1 for additional information.
Intramuscular ketamine 4 mg/kg provides effective PSA, but recovery is significantly longer than with intravenous ketamine. See Case 1 for additional information.
-
(c)
Fentanyl with propofol or midazolam intravenously provides effective PSA for fracture reduction but with more respiratory depression than ketamine techniques (desaturation to less than 90% in approximately 25% FM versus 20% FP versus 5% KM). Since respiratory depression/apnea occur frequently, providers should be experienced with this technique and well prepared to provide ventilatory support. Vomiting is less frequent with propofol-based than ketamine-based techniques. Recovery is faster with propofol/fentanyl-based than with ketamine/midazolam-based PSA (23 versus 33 min in one study), especially if repeated doses are needed. Recovery is described as more pleasant after propofol sedation compared to ketamine. Time to discharge after fentanyl/midazolam is similar to that of ketamine/midazolam.
-
(a)
Case 3
A 3-year-old boy has blistering hot water burns to his right face and much of his anterior chest and abdomen, sustained when he pulled a pot with boiled water off the stove top. He was transported to the ED by EMS who was unable to insert an IV catheter, in part due to the child’s obesity (weight 23 kg). The child has a history of mild asthma without hospitalization, controlled with albuterol MDI as needed. He has had a runny nose and cough without fever for 1–2 days; his usual snoring while sleeping has worsened with the URI. The child is crying loudly and coughing as he is placed in a treatment room. Good air exchange with expiratory wheezes bilaterally is noted on auscultation.
Issues
Rapid pain relief, difficult vascular access, obesity, history of snoring, asthma with current wheezing, and upper respiratory infection:
-
1.
Rapid pain relief options:
-
(a)
Fentanyl intranasally 1.5–2 mg/kg achieves significant pain relief within 5–10 min . See Case 1 for additional information. Base dose on estimated lean body weight (~15 kg for 3-year-old); initial 2 mg/kg dose for this child is 30 mg or 0.6 mL. Divide the 0.6 mL total dose into four sprays of ~0.15 mL/nostril. The impact of an acute URI upon transmucosal absorption is unclear.
-
(b)
Nitrous oxide 50–70% will provide rapid pain relief, but its analgesic effect is lost within minutes when the gas is stopped. N2O can be administered while IV catheter insertion is attempted. Use of a continuous circuit or N2O delivery system easily activated by a young child is necessary.
-
(c)
Oxycodone orally, or other potent oral analgesics, will provide pain relief, but onset is 20–40 min. For this young patient with a very painful injury, an initial oxycodone dose of 0.3 mg/kg is given orally; based on estimated lean body weight of 15 kg, it is 4–4.5 mg. This dose may result in mild sedation as pain relief is achieved. See Case 1 for additional information.
-
(d)
Opioids intravenously titrated to effect will provide the greatest pain relief, if vascular access can be achieved . Fentanyl 1–2 mg/kg will provide analgesia within 1–2 min, lasting 30–60 min, whereas morphine 0.1 mg/kg will provide initial analgesia within 5–10 min with peak effect at 10–20 min and lasting 2–3 h.
-
(e)
Intramuscular ketamine 4 mg/kg provides rapid and marked pain relief and PSA without vascular access. Please see Case 1(b) for further information. If providers are available to monitor the patient and begin debridement, this may be a reasonable option. The greatest risk with this technique is that emergent vascular access to manage a life-threatening adverse event such as laryngospasm would be difficult, but an intraosseous needle could be placed, if necessary. IV catheter insertion for ongoing care can be attempted concurrently with the burn debridement.
-
(a)
-
2.
Difficult vascular access : Buffered lidocaine injected subcutaneously with a 30-gauge needle provides nearly painless rapid local anesthesia for IV insertion. Use of this or other local anesthetic techniques in this obese child will be especially important because multiple attempts likely will be needed. Because of the prolonged onset, topical anesthetic creams are not an optimum choice for local anesthesia. If available, N 2 O 50–70% will reduce IV insertion-related distress as well as provide systemic analgesia as described in (b).
-
3.
Obesity, snoring: As noted earlier, determine medication doses upon estimated lean body weight . Since fat is less perfused than brain and muscle, doses based upon total weight will result in higher initial plasma and brain concentrations and greater risk of adverse effects and prolonged recovery. Obesity also reduces lung functional residual capacity, increasing his risk of hypoxia with respiratory depression, and increases likelihood of upper airway obstruction as indicated by his history of snoring. Use of supplemental oxygen during sedation of this patient will provide a greater margin of safety by prolonging the time to hypoxia if decreased ventilation occurs. Monitoring with end-tidal capnography, in addition to pulse oximetry, will facilitate early detection of ventilatory insufficiency and allow supportive interventions before adverse consequences occur.
-
4.
History of asthma, currently wheezing, acute URI: If the patient’s wheezing clears readily with a single albuterol nebulization treatment, the increased risk of sedation-related adverse respiratory events likely is low, but providers should be prepared to administer additional asthma care if needed. The acute URI may increase the risk of laryngospasm, especially if the patient is febrile. It is unclear whether administration of a drying agent such as glycopyrrolate or atropine reduces this risk.
PSA Technique Options
-
(a)
Ketamine with or without midazolam: If vascular access is successful, the intravenous route is preferred as it allows titration to effect and use of the smallest effective dose, with repeat small doses as needed, thus decreasing length of recovery. Please see Case 1 for further information on ketamine dosing. It is likely this patient will need multiple subsequent painful burn debridements. Therefore, effective analgesia and amnesia for this initial burn care are especially important to establish the patient’s future expectations. A sedating dose of midazolam, 0.1 mg/kg, prior to ketamine infusion, may increase the probability of complete procedural amnesia. A potential additional benefit for this patient is ketamine-induced reduction of central sensitization and windup from continued burn pain. While the risk of laryngospasm associated with ketamine is quite low, the presence of an active URI may increase this risk, and the sedation providers should be prepared to manage this potentially life-threatening adverse event.
Intramuscular ketamine 4 mg/kg: Please see Case 1 for additional information.
-
(b)
Fentanyl + midazolam or propofol provides effective PSA but requires vascular access. Please see Case 2 for additional information.
-
(c)
Nitrous oxide 50–70% is unlikely to provide sufficient PSA for vigorous burn debridement in this young child unless it is coadministered with a potent systemic analgesic such as fentanyl or ketamine. These combinations can readily induce deep sedation and general anesthesia and should be considered only by providers experienced in such techniques.
Case 4
A 2-year-old boy has a complex forehead laceration that requires suturing. Topical anesthetic gel was applied in triage . Despite best efforts to calm him as he sits in his mother’s lap, he continues to cry and vigorously resists exam. His mother predicts he will not calm and indicates this is typical behavior during interactions with healthcare providers.
Issues
The laceration repair requires the patient’s forehead to be still; physical restraint will likely reinforce similar behavior during future healthcare; there are other ED patients waiting more than 4 h to be seen.
PSA Options
-
(a)
Nitrous oxide 50–70% provides effective calming for laceration repair in young children. A continuous circuit or another N2O delivery system with a standard mask that covers the patient’s mouth and nose and is designed for use by children is necessary for effective PSA with N2O. Dental-type nose masks are less effective since they allow mouth breathing that bypasses the N2O. If the laceration is on the chin or in an area covered by the standard mask, a neonatal size mask may be used as a nose mask and the child’s mouth gently held closed. If the mother is amenable, this technique can be enhanced by administering the N2O and suturing as the child sits in her lap with his head rested on her chest and her singing favorite songs or telling stories for distraction. A helper will need to help steady the child’s head and gently hold the mask in place over the patient’s mouth and nose. All must be vigilant for vomiting, often forewarned by abdominal or chest heaving. The N2O should be administered for about 2 min before attempting to provide additional anesthesia (buffered lidocaine injected with a half-inch 30-gauge needle recommended) or suturing.
-
(b)
Midazolam intranasally 0.2–0.4 mg/kg administered with atomizer to spray small volumes of concentrated intravenous solution (5 mg/mL) to improve absorption. Suggested dose for this 12 kg child is 5 mg or 1 mL. Divide the 1 mL total dose into four sprays of ~0.25 mL; alternate nostrils; allow about a minute between repeat sprays into a given nostril. Use of small volumes improves efficacy by reducing drainage of drug into posterior pharynx from which it is less well absorbed and causes an unpleasant taste. Onset of sedation occurs by 3–5 min with duration of 20–40 min. As with other routes of midazolam administration, some children become dysphoric instead of sedated. When administered with an atomizer, intranasal midazolam is well tolerated and achieves anxiolysis with mild sedation. If the intravenous solution is dripped into the nares without atomization, most children complain of a burning sensation.
-
(c)
Ketamine intramuscularly 2–3 mg/kg provides effective PSA for suturing when local anesthesia is also used. Minor restraint may be needed in a few children with this dose. Onset of sedation usually occurs by 5 min and recovery by 60–80 min.
-
(d)
Propofol, ketamine, or fentanyl/midazolam intravenously: Titration of any of these techniques will provide maximum effectiveness, but intravenous access is required. Placement of an IV catheter in this resistant child certainly will require physical restraint unless it is inserted after sedation with N2O, intranasal midazolam, or IM ketamine. Such strategy might be logical for a very complex laceration repair expected to last more than 20–30 min or involve a critical step that requires the patient to be motionless, such as approximating a lacerated eyelid margin.
Case 5
An otherwise healthy febrile 10-month-old infant needs incision and drainage of a large buttock abscess.
PSA Options
-
1.
Ketamine IV or IM: See Case 2 for additional information.
-
2.
Fentanyl + propofol or midazolam : See Case 2 for additional information.
-
3.
Nitrous oxide + oxycodone can provide acceptable PSA if effective local anesthesia of the abscess can be achieved. Field blocks with buffered lidocaine are variably effective for smaller abscesses but usually unsuccessful for large abscesses. For larger and deeper abscesses, the author has occasional success by partially draining the abscess through a small (~1 cm) incision through skin well anesthetized with subcutaneous lidocaine. The abscess cavity then is gently refilled with the topical anesthetic solution commonly used for anesthetizing lacerations (4% lidocaine, 1:100,000 epinephrine, and 0.5% tetracaine [LET]). After 30 min , the entire abscess cavity often is well anesthetized, and the patient tolerates widening the incision and debridement of the cavity under N2O sedation.
Case 6
You are asked to provide sedation for incision and drainage of a peritonsillar abscess in a very anxious 5-year-old boy who vigorously resists oropharyngeal exams. He has had a runny nose and cough with low-grade fever for 2–3 days.
Issues
Mild to light moderate PSA can safely be administered for I&D of peritonsillar abscesses in older children and teens who will cooperate with the procedure in the emergency department. However, this child will require deep sedation to overcome his resistance. Deep sedation by any technique carries increased risk of pulmonary aspiration due to variable blunting of protective airway reflexes. This patient will have blood and pus draining upon his larynx during the procedure. This patient should be considered for abscess drainage in the OR under general anesthesia, likely with endotracheal intubation.
For light PSA for peritonsillar abscess I&D in cooperative children, 30–45 min prior to the procedure, we administer morphine for baseline pain management and glycopyrrolate to dry secretions. Five to ten minutes prior to the procedure, we administer 2 mg of midazolam for anxiolysis. If the patient has difficulty tolerating the mucosal injection of buffered lidocaine with epinephrine at the site of the abscess, we may infuse 0.1–0.2 mg/kg of ketamine immediately prior to the surgeon’s incision, i.e., a small dose. The patient is able to follow commands but appears a bit dazed after the ketamine and usually is better able to tolerate the procedural pain. Laryngospasm has been found to occur more frequently during endoscopy with ketamine sedation, presumably due to direct stimulation of the larynx. Whether laryngospasm risk correlates directly with the dose of ketamine is unclear. Likewise, it is unclear whether risk of laryngospasm is increased with laryngeal stimulation by drainage from a peritonsillar abscess. Using this approach, none of our patients have developed laryngospasm during peritonsillar I&D in our ED.
Case 7
A 15-month-old boy has fallen through stair railings an hour ago and has a large hematoma on his left parietal area. He is irritable and restless. An emergent head CT scan to evaluate for intracranial injury has been ordered. The CT tech calls to state they cannot get the patient to lie still for the brief period of the scan and asks that the patient be sedated.
Issues
Need for emergent CT scan that requires motionless patient for about 1 min to conduct scan, potentially increased intracranial pressure from hemorrhage.
PSA Options
-
1.
Pentobarbital intravenously will sedate patient, but a full dose may cause mild reduction in blood pressure, which impacts brain perfusion. The prolonged recovery from pentobarbital makes monitoring patient for neurologic deterioration difficult and may complicate plans for general anesthesia if emergent craniotomy is needed.
-
2.
Ketamine intravenously 0.25–0.5 mg/kg, pushed rapidly, will provide brief sedation. Some restraint may be necessary. Blood pressure likely will be maintained, and brief increase in intracranial pressure probably is not critical.
-
3.
Propofol intravenously provides sedation, but brief hypotension and respiratory depression may rapidly worsen patient condition.
-
4.
Etomidate intravenously will provide sedation and recovery within 5–10 min with less risk of hypotension. Myoclonic jerks during induction of sedation tend to be brief but may interfere with scanning.
-
5.
Midazolam intravenously may be insufficient for sedation.
-
6.
Fentanyl intravenously for pain may be sufficient to coax patient to be still for the brief period, as needed.
Notes
- 1.
Note: Upper respiratory illness (URI) may increase the risk of laryngospasm, bronchospasm, and hypoxia during sedation. Mild URI symptoms alone (non-purulent rhinitis, afebrile, cough that clears) may not be an indication to cancel PSA, but management should reflect anticipation of above potential complications. Severe URI (febrile, purulent discharge, wet cough) should prompt consideration of cancellation of non-emergent or urgent procedures [376].
References
Carr D, et al. Acute pain management in infants, children, and adolescents: operative and medical procedures. Rockville: Agency for Health Care Policy and Research, Department of Health and Human Services; 1992.
Schechter NL, Berde C, Yaster M, editors. Pain in infants, children, and adolescents. 2nd ed. Philadelphia: Lippincott, Williams & Wilkins; 2003.
Terndrup TE. Pediatric pain control. Ann Emerg Med. 1996;27(4):466–70.
Walco GA, Cassidy RC, Schechter NL. Pain, hurt, and harm. The ethics of pain control in infants and children. N Engl J Med. 1994;331(8):541–4.
Weisman SJ, Bernstein B, Schechter NL. Consequences of inadequate analgesia during painful procedures in children. Arch Pediatr Adolesc Med. 1998;152(2):147–9.
Zeltzer LK, Altman A, Cohen D, LeBaron S, Munuksela EL, Schechter NL. American Academy of Pediatrics report of the subcommittee on the management of pain associated with procedures in children with cancer. Pediatrics. 1990;86(5):826–31.
Fosnocht DE, Heaps ND, Swanson ER. Patient expectations for pain relief in the ED. Am J Emerg Med. 2004;22(4):286–8.
Committee on Drugs. American Academy of Pediatrics. Guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures: addendum. Pediatrics. 2002;110(4):836–8.
Kennedy RM, Porter FL, Miller JP, Jaffe DM. Comparison of fentanyl/midazolam with ketamine/ midazolam for pediatric orthopedic emergencies. Pediatrics. 1998;102(4):956–63.
Luhmann JD, Kennedy RM, Porter FL, Miller JP, Jaffe DM. A randomized clinical trial of continuous-flow nitrous oxide and midazolam for sedation of young children during laceration repair. Ann Emerg Med. 2001;37(1):20–7.
Dollfus C, Annequin M, Adam M, et al. Analgesia with nitrous oxide for painful procedures in pediatric hematology-oncology. Ann Pediatr (Paris). 1995;42(2):115–21.
American College of Emergency Physicians. The use of pediatric sedation and analgesia. Ann Emerg Med. 2008;52(5):595–6.
American Academy of Pediatrics. Committee on psychosocial aspects of child and family health; task force on pain in infants, children, and adolescents. The assessment and management of acute pain in infants, children, and adolescents. Pediatrics. 2001;108(3):793–7.
Brennan F, Carr DB, Cousins M. Pain management: a fundamental human right. Anesth Analg. 2007;105(1):205–21.
Anand KJ, Scalzo FM. Can adverse neonatal experiences alter brain development and subsequent behavior? Biol Neonate. 2000;77(2):69–82.
Fitzgerald M, Anand KJS. Developmental neuroanatomy and neurophysiology of pain. In: Schechter NL, Berde C, Yaster M, editors. Pain in infants, children, and adolescents. Baltimore: Williams & Wilkins; 1993. p. 11–31.
Teng CJ, Abbott FV. The formalin test: a dose-response analysis at three developmental stages. Pain. 1998;76(3):337–47.
Grunau RV, Whitfield MF, Petrie JH. Pain sensitivity and temperament in extremely low-birth-weight premature toddlers and preterm and full-term controls. Pain. 1994;58(3):341–6.
Grunau RE, Whitfield MF, Petrie J. Children’s judgements about pain at age 8–10 years: do extremely low birthweight (< or = 1000 g) children differ from full birthweight peers? J Child Psychol Psychiatry. 1998;39(4):587–94.
Holsti L, Grunau RE, Oberlander TF, Whitfield MF. Prior pain induces heightened motor responses during clustered care in preterm infants in the NICU. Early Hum Dev. 2005;81(3):293–302.
Reynolds ML, Fitzgerald M. Long-term sensory hyperinnervation following neonatal skin wounds. J Comp Neurol. 1995;358(4):487–98.
Ruda MA, Ling QD, Hohmann AG, Peng YB, Tachibana T. Altered nociceptive neuronal circuits after neonatal peripheral inflammation. Science. 2000;289(5479):628–31.
Taddio A, Katz J. The effects of early pain experience in neonates on pain responses in infancy and childhood. Paediatr Drugs. 2005;7(4):245–57.
Taddio A, Katz J, Ilersich AL, Koren G. Effect of neonatal circumcision on pain response during subsequent routine vaccination. Lancet. 1997;349(9052):599–603.
Peters JW, Koot HM, de Boer JB, et al. Major surgery within the first 3 months of life and subsequent biobehavioral pain responses to immunization at later age: a case comparison study. Pediatrics. 2003;111(1):129–35.
Chen E, Zeltzer LK, Craske MG, Katz ER. Children’s memories for painful cancer treatment procedures: implications for distress. Child Dev. 2000;71(4):933–47.
Cohen LL, Francher A, MacLaren JE, Lim CS. Correlates of pediatric behavior and distress during intramuscular injections for invasive dental procedures. J Clin Pediatr Dent. 2006;31(1):44–7.
Okawa K, Ichinohe T, Kaneko Y. Anxiety may enhance pain during dental treatment. Bull Tokyo Dent Coll. 2005;46(3):51–8.
Chen E, Zeltzer LK, Craske MG, Katz ER. Alteration of memory in the reduction of children’s distress during repeated aversive medical procedures. J Consult Clin Psychol. 1999;67(4):481–90.
Pate JT, Blount RL, Cohen LL, Smith AJ. Childhood medical experience and temperament as predictors of adult functioning in medical situations. Child Health Care. 1996;25(4):281–98.
Cohen LL, Blount RL, Cohen RJ, Ball CM, McClellan CB, Bernard RS. Children’s expectations and memories of acute distress: short- and long-term efficacy of pain management interventions. J Pediatr Psychol. 2001;26(6):367–74.
Pierluisi GJ, Terndrup TE. Influence of topical anesthesia on the sedation of pediatric emergency department patients with lacerations. Pediatr Emerg Care. 1989;5(4):211–5.
Ernst AA, Marvez E, Nick TG, Chin E, Wood E, Gonzaba WT. Lidocaine adrenaline tetracaine gel versus tetracaine adrenaline cocaine gel for topical anesthesia in linear scalp and facial lacerations in children aged 5 to 17 years. Pediatrics. 1995;95(2):255–8.
Ernst AA, Marvez-Valls E, Nick TG, Mills T, Minvielle L, Houry D. Topical lidocaine adrenaline tetracaine (LAT gel) versus injectable buffered lidocaine for local anesthesia in laceration repair. West J Med. 1997;167(2):79–81.
Schilling CG, Bank DE, Borchert BA, Klatzko MD, Uden DL. Tetracaine, epinephrine (adrenalin), and cocaine (TAC) versus lidocaine, epinephrine, and tetracaine (LET) for anesthesia of lacerations in children. Ann Emerg Med. 1995;25(2):203–8.
Bonadio WA. Safe and effective method for application of tetracaine, adrenaline, and cocaine to oral lacerations. Ann Emerg Med. 1996;28(4):396–8.
White NJ, Kim MK, Brousseau DC, Bergholte J, Hennes H. The anesthetic effectiveness of lidocaine- adrenaline-tetracaine gel on finger lacerations. Pediatr Emerg Care. 2004;20(12):812–5.
Arndt KA, Burton C, Noe JM. Minimizing the pain of local anesthesia. Plast Reconstr Surg. 1983;72(5):676–9.
Brogan GX Jr, Giarrusso E, Hollander JE, Cassara G, Maranga MC, Thode HC. Comparison of plain, warmed, and buffered lidocaine for anesthesia of traumatic wounds. Ann Emerg Med. 1995;26(2):121–5.
Colaric KB, Overton DT, Moore K. Pain reduction in lidocaine administration through buffering and warming. Am J Emerg Med. 1998;16(4):353–6.
Krause RS, Moscati R, Filice M, Lerner EB, Hughes D. The effect of injection speed on the pain of lidocaine infiltration. Acad Emerg Med. 1997;4(11):1032–5.
Scarfone RJ, Jasani M, Gracely EJ. Pain of local anesthetics: rate of administration and buffering. Ann Emerg Med. 1998;31(1):36–40.
Christoph RA, Buchanan L, Begalla K, Schwartz S. Pain reduction in local anesthetic administration through pH buffering. Ann Emerg Med. 1988;17(2):117–20.
McKay W, Morris R, Mushlin P. Sodium bicarbonate attenuates pain on skin infiltration with lidocaine, with or without epinephrine. Anesth Analg. 1987;66(6):572–4.
Bartfield JM, Homer PJ, Ford DT, Sternklar P. Buffered lidocaine as a local anesthetic: an investigation of shelf life. Ann Emerg Med. 1992;21(1):16–9.
Orlinsky M, Hudson C, Chan L, Deslauriers R. Pain comparison of unbuffered versus buffered lidocaine in local wound infiltration. J Emerg Med. 1992;10(4):411–5.
Larson PO, Ragi G, Swandby M, Darcey B, Polzin G, Carey P. Stability of buffered lidocaine and epinephrine used for local anesthesia. J Dermatol Surg Oncol. 1991;17(5):411–4.
Siegel L. Preparation of children for hospitalization: a selected review of the research literature. J Pediatr Psychol. 1976;1(4):26–30.
Ross DM, Ross SA. Childhood pain: the school- aged child’s viewpoint. Pain. 1984;20(2):179–91.
Bauchner H, Waring C, Vinci R. Parental presence during procedures in an emergency room: results from 50 observations. Pediatrics. 1991;87(4):544–8.
Merritt KA, Sargent JR, Osborn LM. Attitudes regarding parental presence during medical procedures. Am J Dis Child. 1990;144(3):270–1.
Sacchetti A, Lichenstein R, Carraccio CA, Harris RH. Family member presence during pediatric emergency department procedures. Pediatr Emerg Care. 1996;12(4):268–71.
Mangurten J, Scott SH, Guzzetta CE, et al. Effects of family presence during resuscitation and invasive procedures in a pediatric emergency department. J Emerg Nurs. 2006;32(3):225–33.
O’Malley P, Brown K, Mace SE. Patient- and family-centered care and the role of the emergency physician providing care to a child in the emergency department. Pediatrics. 2006;118(5):2242–4.
O’Malley PJ, Brown K, Krug SE. Patient- and family-centered care of children in the emergency department. Pediatrics. 2008;122(2):e511–21.
Alcock DS, Feldman W, Goodman JT, McGrath PJ, Park JM. Evaluation of child life intervention in emergency department suturing. Pediatr Emerg Care. 1985;1(3):111–5.
Manne SL, Bakeman R, Jacobsen PB, Gorfinkle K, Redd WH. An analysis of a behavioral intervention for children undergoing venipuncture. Health Psychol. 1994;13(6):556–66.
Sparks LA, Setlik J, Luhmann J. Parental holding and positioning to decrease IV distress in young children: a randomized controlled trial. J Pediatr Nurs. 2007;22(6):440–7.
Coté CJ, Wilson S, American Academy of Pediatrics, American Academy of Pediatric Dentistry. Guidelines for monitoring and Management of Pediatric Patients before, during, and after sedation for diagnostic and therapeutic procedures. Pediatrics. 2019;143(6):e20191000.
Bijttebier P, Vertommen H. The impact of previous experience on children’s reactions to venepunctures. J Health Psychol. 1998;3(1):39–46.
Agrawal D, Manzi SF, Gupta R, Krauss B. Preprocedural fasting state and adverse events in children undergoing procedural sedation and analgesia in a pediatric emergency department. Ann Emerg Med. 2003;42(5):636–46.
Babl FE, Puspitadewi A, Barnett P, Oakley E, Spicer M. Preprocedural fasting state and adverse events in children receiving nitrous oxide for procedural sedation and analgesia. Pediatr Emerg Care. 2005;21(11):736–43.
Roback MG, Bajaj L, Wathen JE, Bothner J. Preprocedural fasting and adverse events in procedural sedation and analgesia in a pediatric emergency department: are they related? Ann Emerg Med. 2004;44(5):454–9.
Quinn J, Cummings S, Callaham M, Sellers K. Suturing versus conservative management of lacerations of the hand: randomised controlled trial. BMJ. 2002;325(7359):299.
Lamell CW, Fraone G, Casamassimo PS, Wilson S. Presenting characteristics and treatment outcomes for tongue lacerations in children. Pediatr Dent. 1999;21(1):34–8.
Roback MG, Wathen JE, Bajaj L, Bothner JP. Adverse events associated with procedural sedation and analgesia in a pediatric emergency department: a comparison of common parenteral drugs. Acad Emerg Med. 2005;12(6):508–13.
Godwin SA, Burton JH, Gerardo CJ, et al. American College of Emergency Physicians clinical policies subcommittee on procedural sedation and analgesia: clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2014;63:247–58.
Hoffman GM, Nowakowski R, Troshynski TJ, Berens RJ, Weisman SJ. Risk reduction in pediatric procedural sedation by application of an American Academy of Pediatrics/American Society of Anesthesiologists process model. Pediatrics. 2002;109(2):236–43.
American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96(4):1004–17.
McAllister JD, Gnauck KA. Rapid sequence intubation of the pediatric patient. Fundamentals of practice. Pediatr Clin N Am. 1999;46(6):1249–84.
Owens WD, Felts JA, Spitznagel EL Jr. ASA physical status classifications: a study of consistency of ratings. Anesthesiology. 1978;49(4):239–43.
Warner MA, Warner ME, Warner DO, Warner LO, Warner EJ. Perioperative pulmonary aspiration in infants and children. Anesthesiology. 1999;90(1):66–71.
Borland LM, Sereika SM, Woelfel SK, et al. Pulmonary aspiration in pediatric patients during general anesthesia: incidence and outcome. J Clin Anesth. 1998;10(2):95–102.
Cote CJ, Todres ID, Ryan JF, et al., editors. A practice of anesthesia for infants and children. 3rd ed. Philadelphia: WB Saunders; 2001.
Practice Guidelines for Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration: Application to Healthy Patients Undergoing Elective Procedures. An updated report by the American Society of Anesthesiologists task force on preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration. Anesthesiology. 2017;126:376–93.
Mace SE, Brown LA, Francis L, et al. Clinical pol- icy: critical issues in the sedation of pediatric patients in the emergency department. Ann Emerg Med. 2008;51(4):378–99; 399.e1–57.
Green SM, Mason KP, Krauss BS. Pulmonary aspiration during procedural sedation: a comprehensive systematic review. Br J Anaesth. 2017;118:344–54.
Bhatt M, Johnson DW, Taliaard M, et al. Association of preprocedural fasting with outcomes of emergency department sedation in children. JAMA Pediatr. 2018;172(7):678–85.
Green SM, Roback MG, Kennedy RM, Krauss B. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann Emerg Med. 2011;57:449–61.
Warner MA, Warner ME, Weber JG. Clinical significance of pulmonary aspiration during the perioperative period. Anesthesiology. 1993;78(1):56–62.
Green SM, Rothrock SG, Lynch EL, et al. Intramuscular ketamine for pediatric sedation in the emergency department: safety profile in 1,022 cases. Ann Emerg Med. 1998;31(6):688–97.
Engelhardt T, Webster NR. Pulmonary aspiration of gastric contents in anaesthesia. Br J Anaesth. 1999;83(3):453–60.
Maekawa N, Mikawa K, Yaku H, Nishina K, Obara H. Effects of 2-, 4- and 12-hour fasting intervals on preoperative gastric fluid pH and volume, and plasma glucose and lipid homeostasis in children. Acta Anaesthesiol Scand. 1993;37(8):783–7.
Ingebo KR, Rayhorn NJ, Hecht RM, Shelton MT, Silber GH, Shub MD. Sedation in children: adequacy of two-hour fasting. J Pediatr. 1997;131(1):155–8.
Soreide E, Hausken T, Soreide JA, Steen PA. Gastric emptying of a light hospital breakfast. A study using real time ultrasonography. Acta Anaesthesiol Scand. 1996;40(5):549–53.
Cravero JP, Beach ML, Blike GT, Gallagher SM, Hertzog JH. The incidence and nature of adverse events during pediatric sedation/anesthesia with propofol for procedures outside the operating room: a report from the Pediatric sedation research consortium. Anesth Analg. 2009;108(3):795–804.
Wathen JE, Roback MG, Mackenzie T, Bothner JP. Does midazolam alter the clinical effects of intravenous ketamine sedation in children? A double-blind, randomized, controlled, emergency department trial. Ann Emerg Med. 2000;36(6):579–88.
Luhmann JD, Schootman M, Luhmann SJ, Kennedy RM. A randomized comparison of nitrous oxide plus hematoma block versus ketamine plus midazolam for emergency department forearm fracture reduction in children. Pediatrics. 2006;118(4):e1078–86.
McGlone R, Carley S. Towards evidence-based emergency medicine: best BETs from the Manchester Royal Infirmary. BET 3: does the time of fasting affect complication rates during ketamine sedation? Emerg Med J. 2008;25(6):367–9.
Treston G. Prolonged pre-procedure fasting time is unnecessary when using titrated intravenous ketamine for paediatric procedural sedation. Emerg Med Australas. 2004;16(2):145–50.
Schreiner MS. Preoperative and postoperative fasting in children. Pediatr Clin N Am. 1994;41(1):111–20.
Langston WT, Wathen JE, Roback MG, Bajaj L. Effect of ondansetron on the incidence of vomiting associated with ketamine sedation in children: a double-blind, randomized, placebo-controlled trial. Ann Emerg Med. 2008;52(1):30–4.
Joint Commission on Accreditation of Healthcare Organizations. Standards and intents for sedation and anesthesia care. Revisions to Anesthesia Care Standards, Comprehensive Accreditation Manual for Hospitals. Oakbrook Terrace: Joint Commission on Accreditation of Healthcare Organizations; 2001. http://www.jcaho.org/standard/aneshap.html.
Dial S, Silver P, Bock K, Sagy M. Pediatric sedation for procedures titrated to a desired degree of immobility results in unpredictable depth of sedation. Pediatr Emerg Care. 2001;17(6):414–20.
Krauss B, Green SM. Sedation and analgesia for procedures in children. N Engl J Med. 2000;342(13):938–45.
Yaster M, Nichols DG, Deshpande JK, Wetzel RC. Midazolam-fentanyl intravenous sedation in children: case report of respiratory arrest. Pediatrics. 1990;86(3):463–7.
Cote CJ, Karl HW, Notterman DA, Weinberg JA, McCloskey C. Adverse sedation events in pediatrics: analysis of medications used for sedation. Pediatrics. 2000;106(4):633–44.
Cote CJ, Notterman DA, Karl HW, Weinberg JA, McCloskey C. Adverse sedation events in pediatrics: a critical incident analysis of contributing factors. Pediatrics. 2000;105(4 Pt 1):805–14.
Maxwell LG, Yaster M. The myth of conscious sedation. Arch Pediatr Adolesc Med. 1996;150(7):665–7.
Malia L, Laurich VM, Sturm JJ. Adverse events and satisfaction with use of intranasal midazolam for emergency department procedures in children. Am J Emerg Med. 2019;37:85–8.
American College of Emergency Physicians. Unscheduled procedural sedation: a multidisciplinary consensus practice guideline. https://www.acep.org/globalassets/sites/acep/media/policy-statement/unscheduled-procedural-sedation-sept-28-2018-cp.pdf.
Shaw KN, Bell LM, Sherman NH. Outpatient assessment of infants with bronchiolitis. Am J Dis Child. 1991;145(2):151–5.
Langhan ML, Shabanova V, Li F, Bernstein SL, Shapiro ED. A randomized controlled trial of capnography during sedation in a pediatric emergency setting. Am J Emerg Med. 2015;33(1):25–30.
Miner JR, Heegaard W, Plummer D. End-tidal carbon dioxide monitoring during procedural sedation. Acad Emerg Med. 2002;9(4):275–80.
Anderson JL, Junkins E, Pribble C, Guenther E. Capnography and depth of sedation during propofol sedation in children. Ann Emerg Med. 2007;49(1):9–13.
Yldzdas D, Yapcoglu H, Ylmaz HL. The value of capnography during sedation or sedation/analgesia in pediatric minor procedures. Pediatr Emerg Care. 2004;20(3):162–5.
Burton JH, Harrah JD, Germann CA, Dillon DC. Does end-tidal carbon dioxide monitoring detect respiratory events prior to current sedation monitoring practices? Acad Emerg Med. 2006;13(5):500–4.
Krauss B, Hess DR. Capnography for procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2007;50(2):172–81.
Kodali BS. www.capnography.com: an animated website. Anesth Analg. 2001;93(5):1364.
Tobias JD. End-tidal carbon dioxide monitoring during sedation with a combination of midazolam and ketamine for children undergoing painful, invasive procedures. Pediatr Emerg Care. 1999;15(3):173–5.
Kim G, Green SM, Denmark TK, Krauss B. Ventilatory response during dissociative sedation in children-a pilot study. Acad Emerg Med. 2003;10(2):140–5.
Patel R, Lenczyk M, Hannallah RS, McGill WA. Age and the onset of desaturation in apnoeic children. Can J Anaesth. 1994;41(9):771–4.
Keidan I, Gravenstein D, Berkenstadt H, Ziv A, Shavit I, Sidi A. Supplemental oxygen compromises the use of pulse oximetry for detection of apnea and hypoventilation during sedation in simulated pediatric patients. Pediatrics. 2008;122(2):293–8.
Rubin DM, Eisig S, Freeman K, Kraut RA. Effect of supplemental gases on end-tidal CO2 and oxygen saturation in patients undergoing fentanyl and midazolam outpatient sedation. Anesth Prog. 1997;44(1):1–4.
Miner JR, Burton JH. Clinical practice advisory: emergency department procedural sedation with propofol. Ann Emerg Med. 2007;50(2):182–7, 187. e181.
Pena BM, Krauss B. Adverse events of procedural sedation and analgesia in a pediatric emergency department. Ann Emerg Med. 1999;34(4):483–91.
Cravero JP, Blike GT, Beach M, et al. Incidence and nature of adverse events during pediatric sedation/ anesthesia for procedures outside the operating room: report from the Pediatric Sedation Research Consortium. Pediatrics. 2006;118(3):1087–96.
Bailey PL, Pace NL, Ashburn MA, Moll JW, East KA, Stanley TH. Frequent hypoxemia and apnea after sedation with midazolam and fentanyl. Anesthesiology. 1990;73(5):826–30.
Green SM, Johnson NE. Ketamine sedation for pediatric procedures: part 2, Review and implications. Ann Emerg Med. 1990;19(9):1033–46.
Mitchell RK, Koury SI, Stone CK. Respiratory arrest after intramuscular ketamine in a 2-year-old child. Am J Emerg Med. 1996;14(6):580–1.
Litman RS. Apnea and oxyhemoglobin desaturation after intramuscular ketamine administration in a 2-year-old child. Am J Emerg Med. 1997;15(5):547–8.
Newman DH, Azer MM, Pitetti RD, Singh S. When is a patient safe for discharge after procedural sedation? The timing of adverse effect events in 1367 pediatric procedural sedations. Ann Emerg Med. 2003;42(5):627–35.
Neal JM, Owens BD. Hazards of antagonizing narcotic sedation with naloxone. Ann Emerg Med. 1993;22(1):145–6.
Chamberlain JM, Klein BL. A comprehensive review of naloxone for the emergency physician. Am J Emerg Med. 1994;12(6):650–60.
Jones RD, Lawson AD, Andrew LJ, Gunawardene WM, Bacon-Shone J. Antagonism of the hypnotic effect of midazolam in children: a randomized, double-blind study of placebo and flumazenil administered after midazolam-induced anaesthesia. Br J Anaesth. 1991;66(6):660–6.
Ghouri AF, Ruiz MA, White PF. Effect of flumazenil on recovery after midazolam and propofol sedation. Anesthesiology. 1994;81(2):333–9.
Shannon M, Albers G, Burkhart K, et al. Safety and efficacy of flumazenil in the reversal of benzodiazepine-induced conscious sedation. The Flumazenil Pediatric Study Group. J Pediatr. 1997;131(4):582–6.
Dunn-Russell T, Adair SM, Sams DR, Russell CM, Barenie JT. Oxygen saturation and diffusion hypoxia in children following nitrous oxide sedation. Pediatr Dent. 1993;15(2):88–92.
Litman RS, Kottra JA, Berkowitz RJ, Ward DS. Breathing patterns and levels of consciousness in children during administration of nitrous oxide after oral midazolam premedication. J Oral Maxillofac Surg. 1997;55(12):1372–7; discussion 1378–9.
Litman RS, Berkowitz RJ, Ward DS. Levels of consciousness and ventilatory parameters in young children during sedation with oral midazolam and nitrous oxide. Arch Pediatr Adolesc Med. 1996;150(7):671–5.
Litman RS, Kottra JA, Verga KA, Berkowitz RJ, Ward DS. Chloral hydrate sedation: the additive sedative and respiratory depressant effects of nitrous oxide. Anesth Analg. 1998;86(4):724–8.
Bhatt M, Kennedy RM, Osmond MH, et al. Consensus-based recommendations for standardizing terminology and reporting adverse events for emergency department procedural sedation and analgesia in children. Ann Emerg Med. 2009;53(4):426–35.e424.
Cohen VG, Krauss B. Recurrent episodes of intractable laryngospasm during dissociative sedation with intramuscular ketamine. Pediatr Emerg Care. 2006;22(4):247–9.
von Ungern-Sternberg BS, Regli A, Frei FJ, et al. A deeper level of ketamine anesthesia does not affect functional residual capacity and ventilation distribution in healthy preschool children. Paediatr Anaesth. 2007;17(12):1150–5.
Lois F, De Kock M. Something new about ketamine for pediatric anesthesia? Curr Opin Anaesthesiol. 2008;21(3):340–4.
Hampson-Evans D, Morgan P, Farrar M. Pediatric laryngospasm. Paediatr Anaesth. 2008;18(4):303–7.
Green SM, Roback MG, Krauss B, et al. Predictors of airway and respiratory adverse events with ketamine sedation in the emergency department: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med. 2009;54(2):158–68.e151-4.
Murat I, Constant I, Maud’huy H. Perioperative anaesthetic morbidity in children: a database of 24,165 anaesthetics over a 30-month period. Paediatr Anaesth. 2004;14(2):158–66.
Burgoyne LL, Anghelescu DL. Intervention steps for treating laryngospasm in pediatric patients. Paediatr Anaesth. 2008;18(4):297–302.
Black AE. Laryngospasm in pediatric practice. Paediatr Anaesth. 2008;18(4):279–80.
Flick RP, Wilder RT, Pieper SF, et al. Risk factors for laryngospasm in children during general anesthesia. Paediatr Anaesth. 2008;18(4):289–96.
Olsson GL, Hallen B. Laryngospasm during anaesthesia. A computer-aided incidence study in 136,929 patients. Acta Anaesthesiol Scand. 1984;28(5):567–75.
Heinz P, Geelhoed GC, Wee C, Pascoe EM. Is atropine needed with ketamine sedation? A prospective, randomised, double blind study. Emerg Med J. 2006;23(3):206–9.
Brown L, Christian-Kopp S, Sherwin TS, et al. Adjunctive atropine is unnecessary during ketamine sedation in children. Acad Emerg Med. 2008;15(4):314–8.
Green SM, Klooster M, Harris T, Lynch EL, Rothrock SG. Ketamine sedation for pediatric gastroenterology procedures. J Pediatr Gastroenterol Nutr. 2001;32(1):26–33.
Novak H, Karlsland Akeson P, Akeson J. Sedation with ketamine and low-dose midazolam for short-term procedures requiring pharyngeal manipulation in young children. Paediatr Anaesth. 2008;18(1):48–54.
Chung DC, Rowbottom SJ. A very small dose of suxamethonium relieves laryngospasm. Anaesthesia. 1993;48(3):229–30.
Batra YK, Ivanova M, Ali SS, Shamsah M, Al Qattan AR, Belani KG. The efficacy of a subhypnotic dose of propofol in preventing laryngospasm following tonsillectomy and adenoidectomy in children. Paediatr Anaesth. 2005;15(12):1094–7.
Donati F, Meistelman C, Plaud B. Vecuronium neuromuscular blockade at the adductor muscles of the larynx and adductor pollicis. Anesthesiology. 1991;74(5):833–7.
Warner DO. Intramuscular succinylcholine and laryngospasm. Anesthesiology. 2001;95(4):1039–40.
Alalami AA, Ayoub CM, Baraka AS. Laryngospasm: review of different prevention and treatment modalities. Paediatr Anaesth. 2008;18(4):281–8.
Yaster M, Sola JE, Pegoli W Jr, Paidas CN. The night after surgery. Postoperative management of the pediatric outpatient–surgical and anesthetic aspects. Pediatr Clin North Am. 1994;41(1):199–220.
Thomas M, Woodhead G, Masood N, Howard R. Motion sickness as a predictor of postoperative vomiting in children aged 1–16 years. Paediatr Anaesth. 2007;17(1):61–3.
Koo SH, Lee DG, Shin H. Optimal initial dose of chloral hydrate in management of pediatric facial laceration. Arch Plast Surg. 2014;41:40–4.
Holzman RS, Mancuso TJ, Polaner DM, editors. A practical approach to pediatric anesthesia. Philadelphia: Lippincott, Williams & Wilkins; 2008.
Miller KA, Andolfatto G, Miner JR, Burton JH, Krauss BS. Clinical practice guideline for emergency department procedural sedation with propofol: 2018 update. Ann Emerg Med. 2019;73:470–80.
Green SM, Clark R, Hostetler MA, Cohen M, Carlson D, Rothrock SG. Inadvertent ketamine over-dose in children: clinical manifestations and outcome. Ann Emerg Med. 1999;34(4 Pt 1):492–7.
Pongdee T. Soy-allergic and egg-allergic can receive anesthesia. Available at: https://www.aaaai.org/conditions-and-treatments/library/allergy-library/soy-egg-anesthesia. Accessed 18 Dec 2019
Mace SE, Barata IA, Cravero JP, et al. Clinical policy: evidence-based approach to pharmacologic agents used in pediatric sedation and analgesia in the emergency department. Ann Emerg Med. 2004;44(4):342–77.
Dallimore D, Herd DW, Short T, Anderson BJ. Dosing ketamine for pediatric procedural sedation in the emergency department. Pediatr Emerg Care. 2008;24(8):529–33.
Roback MG, Wathen JE, MacKenzie T, Bajaj L. A randomized, controlled trial of i.v. versus i.m. ketamine for sedation of pediatric patients receiving emergency department orthopedic procedures. Ann Emerg Med. 2006;48(5):605–12.
Judisch GF, Anderson S, Bell WE. Chloral hydrate sedation as a substitute for examination under anesthesia in pediatric ophthalmology. Am J Ophthalmol. 1980;89(4):560–3.
Houpt MI, Sheskin RB, Koenigsberg SR, Desjardins PJ, Shey Z. Assessing chloral hydrate dosage for young children. ASDC J Dent Child. 1985;52(5):364–9.
Freyer DR, Schwanda AE, Sanfilippo DJ, et al. Intravenous methohexital for brief sedation of pediatric oncology outpatients: physiologic and behavioral responses. Pediatrics. 1997;99(5):E8.
Audenaert SM, Montgomery CL, Thompson DE, Sutherland J. A prospective study of rectal methohexital: efficacy and side effects in 648 cases. Anesth Analg. 1995;81(5):957–61.
Pomeranz ES, Chudnofsky CR, Deegan TJ, et al. Rectal Methohexital Sedation for Computed Tomography Imaging of Stable Pediatric Emergency Department Patients. Pediatrics. 2000;105:1110–4.
Karian VE, Burrows PE, Zurakowski D, Connor L, Mason KP. Sedation for pediatric radiological procedures: analysis of potential causes of sedation failure and paradoxical reactions. Pediatr Radiol. 1999;29(11):869–73.
Mason KP, Zurakowski D, Karian VE, Connor L, Fontaine PJ, Burrows PE. Sedatives used in pediatric imaging: comparison of IV pentobarbital with IV pentobarbital with midazolam added. AJR Am J Roentgenol. 2001;177(2):427–30.
Strain JD, Campbell JB, Harvey LA, Foley LC. IV Nembutal: safe sedation for children undergoing CT. AJR Am J Roentgenol. 1988;151(5):975–9.
Moro-Sutherland DM, Algren JT, Louis PT, Kozinetz CA, Shook JE. Comparison of intravenous midazolam with pentobarbital for sedation for head computed tomography imaging. Acad Emerg Med. 2000;7(12):1370–5.
Kienstra AJ, Ward MA, Sasan F, Hunter J, Morriss MC, Macias CG. Etomidate versus pentobarbital for sedation of children for head and neck CT imaging. Pediatr Emerg Care. 2004;20(8):499–506.
Zgleszewski SE, Zurakowski D, Fontaine PJ, D’Angelo M, Mason KP. Is propofol a safe alternative to pentobarbital for sedation during pediatric diagnostic CT? Radiology. 2008;247(2):528–34.
Rooks VJ, Chung T, Connor L, et al. Comparison of oral pentobarbital sodium (nembutal) and oral chloral hydrate for sedation of infants during radiologic imaging: preliminary results. AJR Am J Roentgenol. 2003;180(4):1125–8.
Malviya S, Voepel-Lewis T, Tait AR, et al. Pentobarbital vs chloral hydrate for sedation of children undergoing MRI: efficacy and recovery characteristics. Paediatr Anaesth. 2004;14(7):589–95.
Mason KP, Zurakowski D, Connor L, et al. Infant sedation for MR imaging and CT: oral versus intravenous pentobarbital. Radiology. 2004;233(3):723–8.
Strain JD, Harvey LA, Foley LC, Campbell JB. Intravenously administered pentobarbital sodium for sedation in pediatric CT. Radiology. 1986;161(1):105–8.
Greenberg SB, Adams RC, Aspinall CL. Initial experience with intravenous pentobarbital sedation for children undergoing MRI at a tertiary care pediatric hospital: the learning curve. Pediatr Radiol. 2000;30(10):689–91.
Egelhoff JC, Ball WS Jr, Koch BL, Parks TD. Safety and efficacy of sedation in children using a structured sedation program. AJR Am J Roentgenol. 1997;168(5):1259–62.
Slovis TL, Parks C, Reneau D, et al. Pediatric sedation: short-term effects. Pediatr Radiol. 1993;23(5):345–8.
Gaudreault P, Guay J, Thivierge RL, Verdy I. Benzodiazepine poisoning. Clinical and pharmacological considerations and treatment. Drug Saf. 1991;6(4):247–65.
van der Bijl P, Roelofse JA. Disinhibitory reactions to benzodiazepines: a review. J Oral Maxillofac Surg. 1991;49(5):519–23.
Gillies D, Beck A, McCloud A, Rathbone J. Benzodiazepines alone or in combination with antipsychotic drugs for acute psychosis. Cochrane Database Syst Rev. 2005;4:CD003079.
Rubin JT, Towbin RB, Bartko M, Baskin KM, Cahill AM, Kaye RD. Oral and intravenous caffeine for treatment of children with post-sedation paradoxical hyperactivity. Pediatr Radiol. 2004;34(12):980–4.
Cole SG, Brozinsky S, Isenberg JI. Midazolam, a new more potent benzodiazepine, compared with diazepam: a randomized, double-blind study of preendoscopic sedatives. Gastrointest Endosc. 1983;29(3):219–22.
Ghoneim M, Mewaldt S. Benzodiazepines and human memory: a review. Anesthesiology. 1990;72(5):926–38.
Ramoska EA, Linkenheimer R, Glasgow C. Midazolam use in the emergency department. J Emerg Med. 1991;9(4):247–51.
Wright SW, Chudnofsky CR, Dronen SC, et al. Comparison of midazolam and diazepam for conscious sedation in the emergency department. Ann Emerg Med. 1993;22(2):201–5.
Unlugenc H, Guler T, Gunes Y, Isik G. Comparative study of the antiemetic efficacy of ondansetron, propofol and midazolam in the early postoperative period. Eur J Anaesthesiol. 2004;21(1):60–5.
Lane RD, Schunk JE. Atomized intranasal midazolam use for minor procedures in the pediatric emergency department. Pediatr Emerg Care. 2008;24(5):300–3.
Connors K, Terndrup TE. Nasal versus oral midazolam for sedation of anxious children undergoing laceration repair. Ann Emerg Med. 1994;24(6):1074–9.
Theroux MC, West DW, Corddry DH, et al. Efficacy of intranasal midazolam in facilitating suturing of lacerations in preschool children in the emergency department. Pediatrics. 1993;91(3):624–7.
Saint-Maurice C, Meistelman C, Rey E, Esteve C, de Lauture D, Olive G. The pharmacokinetics of rectal midazolam for premedication in children. Anesthesiology. 1986;65(5):536–8.
Shane SA, Fuchs SM, Khine H. Efficacy of rectal midazolam for the sedation of preschool children undergoing laceration repair. Ann Emerg Med. 1994;24(6):1065–73.
Buhrer M, Maitre PO, Crevoisier C, Stanski DR. Electroencephalographic effects of benzodiazepines. II. Pharmacodynamic modeling of the electroencephalographic effects of midazolam and diazepam. Clin Pharmacol Ther. 1990;48(5):555–67.
Krauss B, Shannon M, Damian FJ, Fleisher GR, editors. Guidelines for pediatric sedation. 2nd ed. Dallas: American College of Emergency Physicians;1998.
Veselis RA, Reinsel RA, Feshchenko VA, Wronski M. The comparative amnestic effects of midazolam, propofol, thiopental, and fentanyl at equisedative concentrations. Anesthesiology. 1997;87(4):749–64.
Lalwani K, Michel M. Pediatric sedation in North American children’s hospitals: a survey of anesthesia providers. Paediatr Anaesth. 2005;15(3):209–13.
Sacchetti A, Stander E, Ferguson N, Maniar G, Valko P. Pediatric procedural sedation in the community emergency department: results from the ProSCED registry. Pediatr Emerg Care. 2007;23(4):218–22.
Bassett KE, Anderson JL, Pribble CG, Guenther E. Propofol for procedural sedation in children in the emergency department. Ann Emerg Med. 2003;42(6):773–82.
Havel CJ Jr, Strait RT, Hennes H. A clinical trial of propofol vs midazolam for procedural sedation in a pediatric emergency department. Acad Emerg Med. 1999;6(10):989–97.
Godambe SA, Elliot V, Matheny D, Pershad J. Comparison of propofol/fentanyl versus ketamine/midazolam for brief orthopedic procedural sedation in a pediatric emergency department. Pediatrics. 2003;112(1):116–23.
Slavik VC, Zed PJ. Combination ketamine and propofol for procedural sedation and analgesia. Pharmacotherapy. 2007;27(11):1588–98.
Tosun Z, Esmaoglu A, Coruh A. Propofol-ketamine vs propofol-fentanyl combinations for deep sedation and analgesia in pediatric patients undergoing burn dressing changes. Paediatr Anaesth. 2008;18(1):43–7.
Kotani Y, Shimazawa M, Yoshimura S, Iwama T, Hara H. The experimental and clinical pharmacology of propofol, an anesthetic agent with neuroprotective properties. CNS Neurosci Ther. 2008;14(2):95–106.
Skokan EG, Pribble C, Bassett KE, Nelson DS. Use of propofol sedation in a pediatric emergency department: a prospective study. Clin Pediatr (Phila). 2001;40(12):663–71.
Mallory MD, Baxter AL, Kost SI. Propofol vs pentobarbital for sedation of children undergoing magnetic resonance imaging: results from the Pediatric Sedation Research Consortium. Paediatr Anaesth. 2009;19(6):601–11.
Bell A, Treston G, McNabb C, Monypenny K, Cardwell R. Profiling adverse respiratory events and vomiting when using propofol for emergency department procedural sedation. Emerg Med Australas. 2007;19(5):405–10.
Dosani M, McCormack J, Reimer E, et al. Slower administration of propofol preserves adequate respiration in children. Paediatr Anaesth. 2010;20(11):1001–8.
Evans RG, Crawford MW, Noseworthy MD, Yoo SJ. Effect of increasing depth of propofol anesthesia on upper airway configuration in children. Anesthesiology. 2003;99(3):596–602.
Green SM. Propofol for emergency department procedural sedation–not yet ready for prime time. Acad Emerg Med. 1999;6(10):975–8.
Gan TJ. Pharmacokinetic and pharmacodynamic characteristics of medications used for moderate sedation. Clin Pharmacokinet. 2006;45(9):855–69.
Fulton B, Sorkin EM. Propofol. An overview of its pharmacology and a review of its clinical efficacy in intensive care sedation. Drugs. 1995;50(4):636–57.
Skues MA, Prys-Roberts C. The pharmacology of propofol. J Clin Anesth. 1989;1(5):387–400.
Tramer MR, Moore RA, McQuay HJ. Propofol and bradycardia: causation, frequency and severity. Br J Anaesth. 1997;78(6):642–51.
Smith I, White PF, Nathanson M, Gouldson R. Propofol. An update on its clinical use. Anesthesiology. 1994;81(4):1005–43.
Bryson HM, Fulton BR, Faulds D. Propofol. An update of its use in anaesthesia and conscious sedation. Drugs. 1995;50(3):513–59.
Zuckerbraun NS, Pitetti RD, Herr SM, Roth KR, Gaines BA, King C. Use of etomidate as an induction agent for rapid sequence intubation in a pediatric emergency department. Acad Emerg Med. 2006;13(6):602–9.
Guldner G, Schultz J, Sexton P, Fortner C, Richmond M. Etomidate for rapid-sequence intubation in young children: hemodynamic effects and adverse events. Acad Emerg Med. 2003;10(2):134–9.
Sokolove PE, Price DD, Okada P. The safety of etomidate for emergency rapid sequence intubation of pediatric patients. Pediatr Emerg Care. 2000;16(1):18–21.
Dickinson R, Singer AJ, Carrion W. Etomidate for pediatric sedation prior to fracture reduction. Acad Emerg Med. 2001;8(1):74–7.
Ruth WJ, Burton JH, Bock AJ. Intravenous etomidate for procedural sedation in emergency department patients. Acad Emerg Med. 2001;8(1):13–8.
Vinson DR, Bradbury DR. Etomidate for procedural sedation in emergency medicine. Ann Emerg Med. 2002;39(6):592–8.
Keim SM, Erstad BL, Sakles JC, Davis V. Etomidate for procedural sedation in the emergency department. Pharmacotherapy. 2002;22(5):586–92.
Baxter AL, Mallory MD, Spandorfer PR, Sharma S, Freilich SH, Cravero J. Etomidate versus pentobarbital for computed tomography sedations: report from the Pediatric Sedation Research Consortium. Pediatr Emerg Care. 2007;23(10):690–5.
Di Liddo L, D’Angelo A, Nguyen B, Bailey B, Amre D, Stanciu C. Etomidate versus midazolam for procedural sedation in pediatric outpatients: a randomized controlled trial. Ann Emerg Med. 2006;48(4):433–40, 440.e431.
Helmers JH, Adam AA, Giezen J. Pain and myoclonus during induction with etomidate. A double- blind, controlled evaluation of the influence of droperidol and fentanyl. Acta Anaesthesiol Belg. 1981;32(2):141–7.
McDowall RH, Scher CS, Barst SM. Total intravenous anesthesia for children undergoing brief diagnostic or therapeutic procedures. J Clin Anesth. 1995;7(4):273–80.
Modica PA, Tempelhoff R. Intracranial pressure during induction of anaesthesia and tracheal intubation with etomidate-induced EEG burst suppression. Can J Anaesth. 1992;39(3):236–41.
den Brinker M, Hokken-Koelega AC, Hazelzet JA, de Jong FH, Hop WC, Joosten KF. One single dose of etomidate negatively influences adrenocortical performance for at least 24h in children with meningococcal sepsis. Intensive Care Med. 2008;34(1):163–8.
Forman SA. Clinical and molecular pharmacology of etomidate. Anesthesiology. 2011;114:695–707.
Mohammad Z, Afessa B, Finkielman JD. The incidence of relative adrenal insufficiency in patients with septic shock after the administration of etomidate. Crit Care. 2006;10(4):R105.
Cotton BA, Guillamondegui OD, Fleming SB, et al. Increased risk of adrenal insufficiency following etomidate exposure in critically injured patients. Arch Surg. 2008;143(1):62–7; discussion 67.
McClain DA, Hug CC Jr. Intravenous fentanyl kinetics. Clin Pharmacol Ther. 1980;28(1):106–14.
Klein EJ, Diekema DS, Paris CA, Quan L, Cohen M, Seidel KD. A randomized, clinical trial of oral midazolam plus placebo versus oral midazolam plus oral transmucosal fentanyl for sedation during laceration repair. Pediatrics. 2002;109(5):894–7.
Schutzman SA, Burg J, Liebelt E, et al. Oral trans-mucosal fentanyl citrate for premedication of children undergoing laceration repair. Ann Emerg Med. 1994;24(6):1059–64.
Schutzman SA, Liebelt E, Wisk M, Burg J. Comparison of oral transmucosal fentanyl citrate and intramuscular meperidine, promethazine, and chlorpromazine for conscious sedation of children undergoing laceration repair. Ann Emerg Med. 1996;28(4):385–90.
Schechter NL, Weisman SJ, Rosenblum M, Bernstein B, Conard PL. The use of oral transmucosal fentanyl citrate for painful procedures in children. Pediatrics. 1995;95(3):335–9.
Roback MG, Carlson DW, Babl FE, Kennedy RM. Update on pharmacological management of procedural sedation for children. Curr Opin Anaesthesiol. 2016;29(Suppl 1):S21–35.
Borland M, Jacobs I, King B, O’Brien D. A randomized controlled trial comparing intranasal fentanyl to intravenous morphine for managing acute pain in children in the emergency department. Ann Emerg Med. 2007;49(3):335–40.
Graudins A, Meek R, Egerton-Warburton D, et al. The PICHFORK (Pain In Children Fentanyl Or Ketamine) trial: a randomized controlled trial comparing intranasal ketamine and fentanyl for the relief of moderate to severe pain in children with limb injuries. Ann Emerg Med. 2015;65:248–254.e1.
Frey TM, Florin TA, Caruso M, et al. Effect of intranasal Ketamine vs Fentanyl on pain reduction for extremity injuries in children. The PRIME randomized clinical trial. JAMA Pediatr. 2019;173(2):140–6.
Caspi J, Klausner JM, Safadi T, Amar R, Rozin RR, Merin G. Delayed respiratory depression following fentanyl anesthesia for cardiac surgery. Crit Care Med. 1988;16(3):238–40.
Williams DG, Hatch D, Howard RF. Codeine phosphate in paediatric medicine. Br J Anaesth. 2001;86(3):413–21.
Williams DG, Patel A, Howard RF. Pharmacogenetics of codeine metabolism in an urban population of children and its implications for analgesic reliability. Br J Anaesth. 2002;89(6):839–45.
Gasche Y, Daali Y, Fathi M, et al. Codeine intoxication associated with ultra-rapid CYP2D6 metabolism. N Engl J Med. 2004;351(27):2827–31.
Charney RL, Yan Y, Schootman M, Kennedy RM, Luhmann JD. Oxycodone versus codeine for triage pain in children with suspected forearm fracture: a randomized controlled trial. Pediatr Emerg Care. 2008;24(9):595–600.
Kokki H, Rasanen I, Reinikainen M, Suhonen P, Vanamo K, Ojanpera I. Pharmacokinetics of oxycodone after intravenous, buccal, intramuscular and gastric administration in children. Clin Pharmacokinet. 2004;43(9):613–22.
Pokela ML, Anttila E, Seppala T, Olkkola KT. Marked variation in oxycodone pharmacokinetics in infants. Paediatr Anaesth. 2005;15(7):560–5.
Mellion SA, Bourne D, Brou L, Brent A, Adelgais K, Galinkin J, Wathen J. Evaluating clinical effectiveness and pharmacokinetic profile of atomized intranasal midazolam in children undergoing laceration repair. J Emerg Med. 2017;53(3):397–404.
Sirinathsinghji D. NMDA antagonists as potential analgesic drugs. Basel: Birkhauser; 2002.
White PF, Way WL, Trevor AJ. Ketamine–its pharmacology and therapeutic uses. Anesthesiology. 1982;56(2):119–36.
Bourgoin A, Albanese J, Wereszczynski N, Charbit M, Vialet R, Martin C. Safety of sedation with ketamine in severe head injury patients: comparison with sufentanil. Crit Care Med. 2003;31(3):711–7.
Albanese J, Arnaud S, Rey M, Thomachot L, Alliez B, Martin C. Ketamine decreases intracranial pressure and electroencephalographic activity in traumatic brain injury patients during propofol sedation. Anesthesiology. 1997;87(6):1328–34.
Sehdev RS, Symmons DA, Kindl K. Ketamine for rapid sequence induction in patients with head injury in the emergency department. Emerg Med Australas. 2006;18(1):37–44.
Reich DL, Silvay G. Ketamine: an update on the first twenty-five years of clinical experience. Can J Anaesth. 1989;36(2):186–97.
Lippmann M, Appel PL, Mok MS, Shoemaker WC. Sequential cardiorespiratory patterns of anesthetic induction with ketamine in critically ill patients. Crit Care Med. 1983;11(9):730–4.
Drummond GB. Comparison of sedation with midazolam and ketamine: effects on airway muscle activity. Br J Anaesth. 1996;76(5):663–7.
Hamza J, Ecoffey C, Gross JB. Ventilatory response to CO2 following intravenous ketamine in children. Anesthesiology. 1989;70(3):422–5.
Mankikian B, Cantineau JP, Sartene R, Clergue F, Viars P. Ventilatory pattern and chest wall mechanics during ketamine anesthesia in humans. Anesthesiology. 1986;65(5):492–9.
Tokics L, Strandberg A, Brismar B, Lundquist H, Hedenstierna G. Computerized tomography of the chest and gas exchange measurements during ketamine anaesthesia. Acta Anaesthesiol Scand. 1987;31(8):684–92.
Shulman DL, Bar-Yishay E, Godfrey S. Respiratory mechanics and intrinsic PEEP during ketamine and halothane anesthesia in young children. Anesth Analg. 1988;67(7):656–62.
Morel DR, Forster A, Gemperle M. Noninvasive evaluation of breathing pattern and thoraco-abdominal motion following the infusion of ketamine or droperidol in humans. Anesthesiology. 1986;65(4):392–8.
Joly LM, Benhamou D. Ventilation during total intravenous anaesthesia with ketamine. Can J Anaesth. 1994;41(3):227–31.
Zsigmond EK, Matsuki A, Kothary SP, Jallad M. Arterial hypoxemia caused by intravenous ketamine. Anesth Analg. 1976;55(3):311–4.
Smith JA, Santer LJ. Respiratory arrest following intramuscular ketamine injection in a 4-year-old child. Ann Emerg Med. 1993;22(3):613–5.
Jonnavithula N, Kulkarni DK, Ramachandran G. Prolonged apnea with intramuscular ketamine: a case report. Paediatr Anaesth. 2008;18(4):330–1.
Bourke DL, Malit LA, Smith TC. Respiratory inter- actions of ketamine and morphine. Anesthesiology. 1987;66(2):153–6.
Green SM, Roback MG, Krauss B. Laryngospasm during emergency department ketamine sedation: a case-control study. Pediatr Emerg Care. 2010;26(11):798–802.
Rogers R, Wise RG, Painter DJ, Longe SE, Tracey I. An investigation to dissociate the analgesic and anesthetic properties of ketamine using functional magnetic resonance imaging. Anesthesiology. 2004;100(2):292–301.
Visser E, Schug SA. The role of ketamine in pain management. Biomed Pharmacother. 2006;60(7):341–8.
McMahon SB, Koltzenburg M, editors. Wall and Melzack’s textbook of pain. 5th ed. Philadelphia: Elsevier/Churchill Livingstone; 2005.
Woolf CJ, Thompson SW. The induction and maintenance of central sensitization is dependent on N-methyl-D-aspartic acid receptor activation; implications for the treatment of post-injury pain hypersensitivity states. Pain. 1991;44(3):293–9.
Ji RR, Kohno T, Moore KA, Woolf CJ. Central sensitization and LTP: do pain and memory share similar mechanisms? Trends Neurosci. 2003;26(12):696–705.
Ilkjaer S, Petersen KL, Brennum J, Wernberg M, Dahl JB. Effect of systemic N-methyl-D-aspartate receptor antagonist (ketamine) on primary and secondary hyperalgesia in humans. Br J Anaesth. 1996;76(6):829–34.
Warncke T, Stubhaug A, Jorum E. Ketamine, an NMDA receptor antagonist, suppresses spatial and temporal properties of burn-induced secondary hyperalgesia in man: a double-blind, cross-over comparison with morphine and placebo. Pain. 1997;72(1–2):99–106.
De Kock M, Lavand’homme P, Waterloos H. ‘Balanced analgesia’ in the perioperative period: is there a place for ketamine? Pain. 2001;92(3):373–80.
Willert RP, Woolf CJ, Hobson AR, Delaney C, Thompson DG, Aziz Q. The development and maintenance of human visceral pain hypersensitivity is dependent on the N-methyl-D-aspartate receptor. Gastroenterology. 2004;126(3):683–92.
Menigaux C, Fletcher D, Dupont X, Guignard B, Guirimand F, Chauvin M. The benefits of intraoperative small-dose ketamine on postoperative pain after anterior cruciate ligament repair. Anesth Analg. 2000;90(1):129–35.
Fu ES, Miguel R, Scharf JE. Preemptive ketamine decreases postoperative narcotic requirements in patients undergoing abdominal surgery. Anesth Analg. 1997;84(5):1086–90.
Gurnani A, Sharma PK, Rautela RS, Bhattacharya A. Analgesia for acute musculoskeletal trauma: low- dose subcutaneous infusion of ketamine. Anaesth Intensive Care. 1996;24(1):32–6.
Angst MS, Clark JD. Opioid-induced hyperalgesia: a qualitative systematic review. Anesthesiology. 2006;104(3):570–87.
Celerier E, Rivat C, Jun Y, et al. Long-lasting hyperalgesia induced by fentanyl in rats: preventive effect of ketamine. Anesthesiology. 2000;92(2):465–72.
Stubhaug A, Breivik H, Eide PK, Kreunen M, Foss A. Mapping of punctuate hyperalgesia around a surgical incision demonstrates that ketamine is a powerful suppressor of central sensitization to pain following surgery. Acta Anaesthesiol Scand. 1997;41(9):1124–32.
Joly V, Richebe P, Guignard B, et al. Remifentanil-induced postoperative hyperalgesia and its prevention with small-dose ketamine. Anesthesiology. 2005;103(1):147–55.
Olney JW, Labruyere J, Price MT. Pathological changes induced in cerebrocortical neurons by phencyclidine and related drugs. Science. 1989;244(4910):1360–2.
Farber NB, Wozniak DF, Price MT, Labruyere J, Huss J, St Peter H, et al. Age-specific neurotoxicity in the rat associated with NMDA receptor blockade: potential relevance to schizophrenia? Biol Psychiatry. 1995;38(12):788–96.
Farber NB, Price MT, Labruyere J, Nemnich J, St Peter H, Wozniak DF, et al. Antipsychotic drugs block phencyclidine receptor-mediated neurotoxicity. Biol Psychiatry. 1993;34(1-2):119–21.
Ikonomidou C, Bosch F, Miksa M, et al. Blockade of NMDA receptors and apoptotic neurodegeneration in the developing brain. Science. 1999;283(5398):70–4.
Fredriksson A, Archer T, Alm H, Gordh T, Eriksson P. Neurofunctional deficits and potentiated apoptosis by neonatal NMDA antagonist administration. Behav Brain Res. 2004;153(2):367–76.
Patel P, Sun L. Update on neonatal anesthetic neurotoxicity: insight into molecular mechanisms and relevance to humans. Anesthesiology. 2009;110(4):703–8.
Wang C, Sadovova N, Hotchkiss C, et al. Blockade of N-methyl-D-aspartate receptors by ketamine produces loss of postnatal day 3 monkey frontal cortical neurons in culture. Toxicol Sci. 2006;91(1):192–201.
Young C, Jevtovic-Todorovic V, Qin YQ, et al. Potential of ketamine and midazolam, individually or in combination, to induce apoptotic neurodegeneration in the infant mouse brain. Br J Pharmacol. 2005;146(2):189–97.
Krystal JH, Karper LP, Seibyl JP, et al. Subanesthetic effects of the noncompetitive NMDA antagonist, ketamine, in humans. Psychotomimetic, perceptual, cognitive, and neuroendocrine responses. Arch Gen Psychiatry. 1994;51(3):199–214.
Malhotra AK, Pinals DA, Weingartner H, et al. NMDA receptor function and human cognition: the effects of ketamine in healthy volunteers. Neuropsychopharmacology. 1996;14(5):301–7.
Adler CM, Goldberg TE, Malhotra AK, Pickar D, Breier A. Effects of ketamine on thought disorder, working memory, and semantic memory in healthy volunteers. Biol Psychiatry. 1998;43(11):811–6.
Newcomer JW, Farber NB, Jevtovic-Todorovic V, et al. Ketamine-induced NMDA receptor hypofunction as a model of memory impairment and psychosis. Neuropsychopharmacology. 1999;20(2):106–18.
Hollister GR, Burn JM. Side effects of ketamine in pediatric anesthesia. Anesth Analg. 1974;53(2):264–7.
Hostetler MA, Davis CO. Prospective age-based comparison of behavioral reactions occurring after ketamine sedation in the ED. Am J Emerg Med. 2002;20(5):463–8.
Lin C, Durieux ME. Ketamine and kids: an update. Paediatr Anaesth. 2005;15(2):91–7.
Kain ZN, Mayes LC, Wang SM, Hofstadter MB. Postoperative behavioral outcomes in children: effects of sedative premedication. Anesthesiology. 1999;90(3):758–65.
Sherwin TS, Green SM, Khan A, Chapman DS, Dannenberg B. Does adjunctive midazolam reduce recovery agitation after ketamine sedation for pediatric procedures? A randomized, double-blind, placebo-controlled trial. Ann Emerg Med. 2000;35(3):229–38.
Kain ZN, Caldwell-Andrews AA, Maranets I, et al. Preoperative anxiety and emergence delirium and post-operative maladaptive behaviors. Anesth Analg. 2004;99(6):1648–54.
Kennedy RM, McAllister JD. Midazolam with ketamine: who benefits? Ann Emerg Med. 2000;35(3):297–9.
Gorelick M, Nagler J, Losek JD. Pediatric sedation pearls. Clin Pediatr Emerg Med. 2007;8(4):268–78.
Gloor A, Dillier C, Gerber A. Ketamine for short ambulatory procedures in children: an audit. Paediatr Anaesth. 2001;11(5):533–9.
Thorp AW, Brown L, Green SM. Ketamine-associated vomiting: is it dose-related? Pediatr Emerg Care. 2009;25(1):15–8.
Vlajkovic GP, Sindjelic RP. Emergence delirium in children: many questions, few answers. Anesth Analg. 2007;104(1):84–91.
Kain ZN, Mayes LC, O’Connor TZ, Cicchetti DV. Preoperative anxiety in children. Predictors and outcomes. Arch Pediatr Adolesc Med. 1996;150(12):1238–45.
Domino EF, Domino SE, Smith RE, et al. Ketamine kinetics in unmedicated and diazepam-premedicated subjects. Clin Pharmacol Ther. 1984;36(5):645–53.
Grant IS, Nimmo WS, McNicol LR, Clements JA. Ketamine disposition in children and adults. Br J Anaesth. 1983;55(11):1107–11.
Atiba JO, Horai Y, White PF, Trevor AJ, Blaschke TF, Sung ML. Effect of etomidate on hepatic drug metabolism in humans. Anesthesiology. 1988;68(6):920–4.
Bleiberg AH, Salvaggio CA, Roy LC, Kassutto Z. Low-dose ketamine: efficacy in pediatric sedation. Pediatr Emerg Care. 2007;23(3):158–62.
McGlone RG, Howes MC, Joshi M. The Lancaster experience of 2.0 to 2.5 mg/kg intramuscular ketamine for paediatric sedation: 501 cases and analysis. Emerg Med J. 2004;21(3):290–5.
Herd D, Anderson BJ. Ketamine disposition in children presenting for procedural sedation and analgesia in a children’s emergency department. Paediatr Anaesth. 2007;17(7):622–9.
Luhmann JD, Kennedy RM, McAllister JD, Jaffe DM. Sedation for peritonsillar abscess drainage in the pediatric emergency department. Pediatr Emerg Care. 2002;18(1):1–3.
Bauer PW, Lieu JE, Suskind DL, Lusk RP. The safety of conscious sedation in peritonsillar abscess drainage. Arch Otolaryngol Head Neck Surg. 2001;127(12):1477–80.
Green SM, Hummel CB, Wittlake WA, Rothrock SG, Hopkins GA, Garrett W. What is the optimal dose of intramuscular ketamine for pediatric sedation? Acad Emerg Med. 1999;6(1):21–6.
Herd DW, Anderson BJ, Holford NH. Modeling the norketamine metabolite in children and the implications for analgesia. Paediatr Anaesth. 2007;17(9):831–40.
Parbrook GD. The levels of nitrous oxide analgesia. Br J Anaesth. 1967;39(12):974–82.
Benedetti C, Chapman CR, Colpitts YH, Chen AC. Effect of nitrous oxide concentration on event- related potentials during painful tooth stimulation. Anesthesiology. 1982;56(5):360–4.
Clark M, Bernick A. A handbook of nitrous oxide and oxygen sedation. 5th ed. St. Louis: Mosby; 2019.
Babl FE, Oakley E, Seaman C, Barnett P, Sharwood LN. High-concentration nitrous oxide for procedural sedation in children: adverse events and depth of sedation. Pediatrics. 2008;121(3):e528–32.
Burton JH, Auble TE, Fuchs SM. Effectiveness of 50% nitrous oxide/50% oxygen during laceration repair in children. Acad Emerg Med. 1998;5(2):112–7.
Clark MS, Campbell SA, Clark AM. Technique for the administration of nitrous oxide/oxygen sedation to ensure psychotropic analgesic nitrous oxide (PAN) effects. Int J Neurosci. 2006;116(7):871–7.
Babl FE, Oakley E, Puspitadewi A, Sharwood LN. Limited analgesic efficacy of nitrous oxide for painful procedures in children. Emerg Med J. 2008;25(11):717–21.
Hennrikus WL, Simpson RB, Klingelberger CE, Reis MT. Self-administered nitrous oxide analgesia for pediatric fracture reductions. J Pediatr Orthop. 1994;14(4):538–42.
Hennrikus WL, Shin AY, Klingelberger CE. Self- administered nitrous oxide and a hematoma block for analgesia in the outpatient reduction of fractures in children. J Bone Joint Surg Am. 1995;77(3):335–9.
Frampton A, Browne GJ, Lam LT, Cooper MG, Lane LG. Nurse administered relative analgesia using high concentration nitrous oxide to facilitate minor procedures in children in an emergency department. Emerg Med J. 2003;20(5):410–3.
Farrell MK, Drake GJ, Rucker D, Finkelstein M, Zier JL. Creation of a registered nurse-administered nitrous oxide sedation program for radiology and beyond. Pediatr Nurs. 2008;34(1):29–35; quiz 35–6.
Gamis AS, Knapp JF, Glenski JA. Nitrous oxide analgesia in a pediatric emergency department. Ann Emerg Med. 1989;18(2):177–81.
Bar-Meir E, Zaslansky R, Regev E, Keidan I, Orenstein A, Winkler E. Nitrous oxide administered by the plastic surgeon for repair of facial lacerations in children in the emergency room. Plast Reconstr Surg. 2006;117(5):1571–5.
Keidan I, Zaslansky R, Yusim Y, et al. Continuous flow 50:50 nitrous oxide:oxygen is effective for relief of procedural pain in the pediatric emergency department. Acute Pain. 2003;5(1):25–30.
Evans JK, Buckley SL, Alexander AH, Gilpin AT. Analgesia for the reduction of fractures in children: a comparison of nitrous oxide with intramuscular sedation. J Pediatr Orthop. 1995;15(1):73–7.
Gregory PR, Sullivan JA. Nitrous oxide compared with intravenous regional anesthesia in pediatric forearm fracture manipulation. J Pediatr Orthop. 1996;16(2):187–91.
Wattenmaker I, Kasser JR, McGravey A. Self- administered nitrous oxide for fracture reduction in children in an emergency room setting. J Orthop Trauma. 1990;4(1):35–8.
Babl FE, Belousoff J, Deasy C, Hopper S, Theophilos T. Paediatric procedural sedation based on nitrous oxide and ketamine: sedation registry data from Australia. Emerg Med J. 2010;27:607–12.
Babl FE, Oakley E, Sharwood LN. The utility of nitrous oxide. Emerg Med J. 2009;26(7):544–5.
Burnweit C, Diana-Zerpa JA, Nahmad MH, et al. Nitrous oxide analgesia for minor pediatric surgical procedures: an effective alternative to conscious sedation? J Pediatr Surg. 2004;39(3):495–9; discussion 495–9.
Ekbom K, Jakobsson J, Marcus C. Nitrous oxide inhalation is a safe and effective way to facilitate procedures in paediatric outpatient departments. Arch Dis Child. 2005;90(10):1073–6.
Henderson JM, Spence DG, Komocar LM, Bonn GE, Stenstrom RJ. Administration of nitrous oxide to pediatric patients provides analgesia for venous cannulation. Anesthesiology. 1990;72(2):269–71.
Kanagasundaram SA, Lane LJ, Cavalletto BP, Keneally JP, Cooper MG. Efficacy and safety of nitrous oxide in alleviating pain and anxiety during painful procedures. Arch Dis Child. 2001;84(6):492–5.
Stewart RD, Gorayeb MJ, Pelton GH. Arterial blood gases before, during, and after nitrous oxide:oxygen administration. Ann Emerg Med. 1986;15(10):1177–80.
Cheney FW. An early example of evidence-based medicine: hypoxemia due to nitrous oxide. Anesthesiology. 2007;106(1):186–8.
Luhmann JD, Kennedy RM, Jaffe DM, McAllister JD. Continuous-flow delivery of nitrous oxide and oxygen: a safe and cost-effective technique for inhalation analgesia and sedation of pediatric patients. Pediatr Emerg Care. 1999;15(6):388–92.
Duncan GH, Moore P. Nitrous oxide and the dental patient: a review of adverse reactions. J Am Dent Assoc. 1984;108(2):213–9.
Herff H, Paal P, von Goedecke A, Lindner KH, Keller C, Wenzel V. Fatal errors in nitrous oxide delivery. Anaesthesia. 2007;62(12):1202–6.
National Institute for Occupational Health. Criteria for a recommended standard: occupational exposure to waste anesthetic gases and vapors. Publication 77–120; 1977.
Ruben H. Nitrous oxide analgesia in dentistry. Its use during 15 years in Denmark. Br Dent J. 1972;132(5):195–6.
Onody P, Gil P, Hennequin M. Safety of inhalation of a 50% nitrous oxide/oxygen premix: a prospective survey of 35,828 administrations. Drug Saf. 2006;29(7):633–40.
Everett GB, Allen GD. Simultaneous evaluation of cardiorespiratory and analgesic effects of nitrous oxide-oxygen inhalation analgesia. J Am Dent Assoc. 1971;83(1):129–33.
Cleaton-Jones P. The laryngeal-closure reflex and nitrous oxide-oxygen analgesia. Anesthesiology. 1976;45(5):569–70.
Roberts GJ, Wignall BK. Efficacy of the laryngeal reflex during oxygen-nitrous oxide sedation (relative analgesia). Br J Anaesth. 1982;54(12):1277–81.
Rubin J, Brock-Utne JG, Greenberg M, Bortz J, Downing JW. Laryngeal incompetence during experimental “relative analgesia” using 50% nitrous oxide in oxygen. A preliminary report. Br J Anaesth. 1977;49(10):1005–8.
Jevtovic-Todorovic V, Todorovic SM, Mennerick S, et al. Nitrous oxide (laughing gas) is an NMDA antagonist, neuroprotectant and neurotoxin. Nat Med. 1998;4(4):460–3.
Gillman MA. Analgesic (sub anesthetic) nitrous oxide interacts with the endogenous opioid system: a review of the evidence. Life Sci. 1986;39(14):1209–21.
Dzoljic M, Van Duijn B. Nitrous oxide-induced enhancement of gamma-aminobutyric acid A-mediated chloride currents in acutely dissociated hippocampal neurons. Anesthesiology. 1998;88(2):473–80.
Benumof JL, editor. Airway management: principles and practice. St. Louis: Mosby-Yearbook; 1996. p. 132.
Oberer C, von Ungern-Sternberg BS, Frei FJ, Erb TO. Respiratory reflex responses of the larynx differ between sevoflurane and propofol in pediatric patients. Anesthesiology. 2005;103:1142–8.
O’Connor RE, Sama A, Burton JH, et al. Procedural sedation and analgesia in the emergency department: recommendations for physician credentialing, privileging, and practice. Ann Emerg Med. 2011;58(4):365–70.
Thomas MC, Jennett–Reznek AM, Patanwala AE. Combination of Ketamine and Propofol versus either agent alone for procedural sedation in the emergency department. Am J Health-Syst Pharm. 2011;68:2248–56.
Alletag MJ, Auerbach MA, Baum CR. Ketamine, Propofol, and Ketofol use for pediatric sedation. Pediatr Emer Care. 2012;28:1391–8.
Green SM, Andolfatto G, Krauss B. Ketofol for procedural sedation? Pro and Con. Ann Emerg Med. 2011;57(5):444–8.
Shah A, Mosdossy G, McLeod S, Lehnhardt K, Peddle M, Rieder M. A blinded, randomized controlled trial to evaluate Ketamine/Propofol Versus Ketamine alone for procedural sedation in children. Ann Emerg Med. 2011;57:425–33.
Andolfatto G, Willman E. A prospective case series of pediatric procedural sedation and analgesia in the emergency department using single-syringe Ketamine–Propofol Combination (Ketofol). Acad Emerg Med. 2010;17:194–201.
Sharieff GQ, Trocinski DR, Kanegaye JT, Fisher B, Harley JR. Ketamine-Propofol combination sedation for fracture reduction in the pediatric emergency department. Pediatr Emerg Care. 2007;23(12):881–4.
David H, Shipp JA. Randomized controlled trial of Ketamine/Propofol Versus Propofol alone for emergency department procedural sedation. Ann Emerg Med. 2011;57:435–41.
Andolfatto G, Abu-Laban RB, Zed PJ, Staniforth SM, Stackhouse S, Moadebi S, Willman E. Ketamine-Propofol Combination (Ketofol) Versus Propofol alone for emergency department procedural sedation and analgesia: A randomized double-blind trial. Ann Emerg Med. 2012;59:504–12.
Messenger DW, Murray HE, Dungey PE, van Vlymen J, Sivilotti ML. Subdissociative-dose Ketamine versus Fentanyl for analgesia during propofol procedural sedation: a randomized clinical trial. Acad Emerg Med. 2008;15:877–86.
Nejati A, Moharari RS, Ashraf H, Labaf A, Golshani K. Ketamine/Propofol Versus Midazolam/Fentanyl for procedural sedation and analgesia in the emergency department: A randomized, prospective, double-blind trial. Acad Emerg Med. 2011;18:800–6.
Tobias JD. Dexmedetomidine and ketamine: An effective alternative for procedural sedation? Pediatr Crit Care Med. 2012;13:423–7.
Leroy PL, van Beukering A, Costa LR, Emmanouil D, Franck LS. Beyond the drugs: Non-pharmacological strategies to optimize procedural care in children. Curr Opin Anesthesiol. 2016;29(suppl 1):S1–S13.
Bhatt M, Johnson DW, Chan J, et al. Risk factors for adverse events in emergency department procedural sedation for children. JAMA Pediatr. 2017;171(10):957–64.
Mallory MD, Travers C, McCracken CE, Hertzog J, Cravero JP. Upper respiratory infections and airway adverse events in pediatric procedural sedation. Pediatrics. 2017;140(1):e20170009.
Iyer MS, Pitetti RD, Vitale M. Higher mallampati scores are not associated with more adverse events during pediatric procedural sedation and analgesia. West J Emerg Med. 2018;19(2):430–6.
Green SM, Leroy PL, Irwin MG, et al. on behalf of the International Committee for the Advancement of Procedural Sedation. An international multidisciplinary consensus statement on fasting before procedural sedation in adults and children. Anaesthesia 2019 doi:https://doi.org/10.1111/anae.14892
Chinta SS, Schrock CR, McAllister JD, Jaffe DM, Liu J, Kennedy RM. Rapid administration technique of ketamine for pediatric forearm fracture reduction: a dose-finding study. Ann Emerg Med. 2015;65(6):640–8.
Grunwell JR, Travers C, McCracken CE, et al. Procedural sedation outside of the operating room using ketamine in 22,645 children: a report from the pediatric sedation research consortium. Pediatr Crit Care Med. 2016;17(12):1109–16.
Isono S, Eikermann M, Odaka T. Facemask ventilation during induction of anesthesia: how “gentle” is “gentle” enough? Anesthesiology. 2014;120(2):263–5.
Greenberg SB, Faerber EN, Aspinal CL, Adams RC. High-dose chloral hydrate sedation for children undergoing mr imaging: safety and efficacy in relation to age. AJR. 1993;161:639–41.
Napoli KL, Ingall CG, Martin GR. Safety and efficacy of chloral hydrate sedation in children undergoing echocardiography. J Pediatr. 1996;129:287–91.
Karaoui M, Varadaraj V, Munoz B, et al. Chloral hydrate administered by a dedicated sedation service can be used safely and effectively for pediatric ophthalmic examination. Am J Ophthalmol. 2018;192:39–46.
Fong CY, Tay CG, Ong LC, Lai NM. Chloral hydrate as a sedating agent for neurodiagnostic procedures in children. Cochrane Database of Systematic Reviews 2017, Issue 11. Art. No.: CD011786.
Institute for Safe Medication Practices. Chloral hydrate: is it still being used? Are there safer alternatives? 3 Nov 2016. https://www.ismp.org/resources/chloral-hydrate-it-still-being-used-are-there-safer-alternatives.
Sedik H. Use of intravenous methohexital as a sedative in pediatric emergency departments. Arch Pediatr Adolesc Med. 2001;155:665–8.
Chokshi AA, Patel VR, Chauhan PR, et al. Evaluation of intranasal Midazolam spray as a sedative in pediatric patients for radiological imaging procedures. Anesth Essays Res. 2013;7(2):189–93.
Young TP, Lim JJ, Kim TY, Thorp AW, Brown L. Pediatric procedural sedation with propofol using a higher initial bolus dose. Pediatr Emer Care. 2014;30:689–93.
Lee-Jayaram JJ, Green A, Siembieda J, Gracely EJ, Mull CC, Quintana E, Adirim T. Ketamine/Midazolam versus Etomidate/Fentanyl procedural sedation for pediatric orthopedic reductions. Pediatr Emer Care. 2010;26:408–12.
Gagnon DJ, Seder DB. Etomidate in sepsis: understanding the dilemma. J Thorac Dis. 2015;7(10):1699–701.
Mandt MJ, Roback MG, Bajaj L, et al. Etomidate for short pediatric procedures in the emergency department. Pediatr Emerg Care. 2012;28:898–904.
Disel NR, Yilmaz HL, Sertdemir Y, et al. Etomidate versus ketamine: effective use in emergency procedural sedation for pediatric orthopedic injuries. Pediatr Emerg Care. 2016;32(12):830–4.
Fenster DB, Dayan PS, Babineau J, Apone-Patel L, Tsze DS. Randomized trial of intranasal fentanyl versus intravenous morphine for abscess incision and drainage. Pediatr Emerg Care. 2016;34(9):607–12.
Quinn K, Kriss S, Drapkin J, et al. Analgesic efficacy of intranasal ketamine versus intranasal fentanyl for moderate to severe pain in children. A prospective, randomized, double-blind study. Pediatr Emer Care. 2018; In Press.
Fein DM, Avner JR, Scharbach K, Manwani D, Khine H. Intranasal fentanyl for initial treatment of vaso-occlusive crisis in sickle cell disease. Pediatr Blood Cancer, 64:e26332. https://doi.org/10.1002/pbc.26332.
Ryan PM, Kienstra AJ, Cosgrove P, et al. Safety and effectiveness of intranasal midazolam and fentanyl used in combination in the pediatric emergency department. Am J Emerg Med. 2019;37:237–40.
Hoeffe J, Trottier ED, Bailey B, et al. Intranasal fentanyl and inhaled nitrous oxide for fracture reduction: The FAN observational study. Am J Emerg Med. 2017;35:710–5.
Míguez MC, Ferrero C, Rivas A, et al. Retrospective comparison of intranasal fentanyl and inhaled nitrous oxide to intravenous ketamine and midazolam for painful orthopedic procedures in a pediatric emergency department. Pediatr Emer Care. 2019; In press.
Seiler M, Staubli G, Landolt MA. Combined nitrous oxide 70% with intranasal fentanyl for procedural analgosedation in children: a prospective, randomised, double-blind, placebo-controlled trial. Emerg Med J. 2019;36:142–7.
Wolfe T. Intranasal fentanyl for acute pain: techniques to enhance efficacy. Ann Emerg Med. 2007;49(5):721–2.
Yee MM, Josephson C, Hill CE, Harrington R, Castillejo MI, Ramjit R, Osunkwo I. Cytochrome P450 2D6 polymorphisms and predicted opioid metabolism in African American children with sickle cell disease. J Pediatr Hematol Oncol. 2013;35(7):e301–5.
Monte AA, Heard KJ, Campbell J, Hamamura D, Weinshilboum RM, Vasiliou V. The effect of CYP2D6 drug–drug interactions on hydrocodone effectiveness. Acad Emerg Med. 2014;21:879–85.
Sanacora G, Frye MA, McDonald W, et al. American Psychiatric Association (APA) council of research task force on novel biomarkers and treatments. A consensus statement on the use of ketamine in the treatment of mood disorders. JAMA Psychiatry. 2017;74(4):399–405.
Hashimoto K. Rapid-acting antidepressant ketamine, its metabolites and other candidates: A historical overview and future perspective. Psych Clin Neurosci. 2019;73:613–27.
Phillips JL, Norris S, Talbot J, et al. Single, repeated, and maintenance ketamine infusions for treatment-resistant depression: a randomized controlled trial. Am J Psychiatry. 2019;176:401–9.
Burger J, Capobianco M, Lovern R, et al. A double-blinded, randomized, placebo-controlled sub-dissociative dose ketamine pilot study in the treatment of acute depression and suicidality in a military emergency department setting. Military Med. 2016;181(10):1195–9.
Cullen KR, Amatya P, Roback MG, et al. Intravenous ketamine for adolescents with treatment-resistant depression: an open-label study. J Child Adolesc Psychopharmacol. 2018;28(7):437–44.
Wilkinson ST, Ballard ED, Bloch MH, Mathew SJ, et al. The effect of a single dose of intravenous ketamine on suicidal ideation: a systematic review and individual participant data meta-analysis. Am J Psychiatry. 2018;175:150–8.
Zarrinnegar P, Kothari J, Cheng K. Successful use of ketamine for the treatment of psychotic depression in a teenager. J Child Adolesc Psychopharmacol. 2019;29(6):472–3.
Acevedo-Diaz RR, Cavanaugh GW, Greenstein D, et al. Comprehensive assessment of side effects associated with a single dose of ketamine in treatment-resistant depression. J Affect Disord. 2019; https://doi.org/10.1016/j.jad.2019.11.028.
Arabzadeh S, Hakkikazazi E, Shahmansouri N, et al. Does oral administration of ketamine accelerate response to treatment in major depressive disorder? Results of a double-blind controlled trial. J Affect Disord. 2018;235:236–41.
Gálvez V, Li A, Huggins C, et al. Repeated intranasal ketamine for treatment resistant depression – the way to go? Results from a pilot randomised controlled trial. J Psychopharmacol. 2018;32(4):397–407.
Gordon J. New hope for treatment-resistant depression: guessing right on ketamine. https://www.nimh.nih.gov/about/director/messages/2019/new-hope-for-treatment-resistant-depression-guessing-right-on-ketamine.shtml.
Motov S, Rosenbaum S, Vilke GM, Nakajima Y. Is there a role for intravenous subdissociative-dose ketamine administered as an adjunct to opioids or as a single agent for acute pain management in the emergency department? J Emerg Med. 2016;51(6):752–7.
Sin B, Tatunchak T, Paryavi M, et al. The use of ketamine for acute treatment of pain: a randomized, double-blind, placebo-controlled trial. J Emerg Med. 2017;52(5):601–8.
Motov S, Mai M, Pushkar I, et al. A prospective randomized, double-dummy trial comparing IV push low dose ketamine to short infusion of low dose ketamine for treatment of pain in the ED. Am J Emerg Med. 2017;35:1095–100.
Weber F, Wulf H, Gruber M, Biallas R. S-ketamine and s-norketamine plasma concentrations after nasal and i.v. administration in anesthetized children. Pediatr Anesth. 2004;14:983–8.
Malinovsky JM, Servin F, Cozian A, et al. Ketamine and norketamine plasma concentrations after i.v., nasal and rectal administration in children. Br J Anaesth. 1996;77:203–7.
Poonai N, Canton K, Ali S, Hendrikx S, Shah A, Miller M, et al. Intranasal ketamine for procedural sedation and analgesia in children: a systematic review. PLoS ONE. 2017;12(3):e0173253.
Tsze DS, Steele DW, Machan JT, Akhlaghi F, Linakis JG. Intranasal ketamine for procedural sedation in pediatric laceration repair: a preliminary report. Pediatr Emer Care. 2012;28(8):767–70.
Poonai N, Canton K, Elsie S, et al. Intranasal ketamine for procedural sedation in children: a randomized controlled pilot study. Ann Emerg Med. 2017;70(4):S109.
Reynolds SL, Bryant KK, Studnek JR, et al. Randomized controlled feasibility trial of intranasal ketamine compared to intranasal fentanyl for analgesia in children with suspected extremity fractures. Acad Emerg Med. 2017;24:1430–40.
Quinn K, Kriss S, Drapkin J, et al. Analgesic efficacy of intranasal ketamine versus intranasal fentanyl for moderate to severe pain in children a prospective, randomized, double-blind study. Pediatr Emer Care. In Press;
Scheier E, Siman A, Balla U. Intranasal ketamine proved feasible for pain control in paediatric care and parental support was high. Acta Paediatr. 2017;106(10):1702.
Qureshi FA, Mellis PT, McFadden MA. Efficacy of oral ketamine for providing sedation and analgesia to children requiring laceration repair. Pediatr Emerg Care. 1995;11(2):93–7.
Younge PA, Kendall JM. Sedation for children requiring wound repair: a randomized controlled double blind comparison of oral midazolam and oral ketamine. Emerg Med J. 2001;18(1):30–3.
Rubinstein O, Barkan S, Breitbart R, et al. Efficacy of oral ketamine compared to midazolam for sedation of children undergoing laceration repair: a double-blind, randomized, controlled trial. Medicine (Baltimore). 2016;95(26):e3984.
Barkan S, Breitbart R, Brenner-Zada G, et al. A double-blind, randomised, placebo-controlled trial of oral midazolam plus oral ketamine for sedation of children during laceration repair. Emerg Med J. 2014;31(8):649–53.
Weisz K, Bajaj L, Deakyne SJ, et al. Adverse events during a randomized trial of ketamine versus co-administration of ketamine and propofol for procedural sedation in a pediatric emergency department. J Emerg Med. 2017;53(1):1–9.
Seiler M, Landolt MA, Staubli G. Nitrous oxide 70% for procedural analgosedation in a pediatric emergency department with or without intranasal fentanyl? Analgesic efficacy and adverse events if combined with intranasal fentanyl. Pediatr Emerg Care. 2019;35(11):755–9.
Klein U, Robinson TJ, Allshouse A. End-expired nitrous oxide concentrations compared to flowmeter settings during operative dental treatment in children. Pediatr Dent. 2011;33:56–62.
Fauteux-Lamarre E, McCarthy M, Quinn N, et al. Oral ondansetron to reduce vomiting in children receiving intranasal fentanyl and inhaled nitrous oxide for procedural sedation and analgesia: a randomized controlled trial. Ann Emerg Med. 2020;75(6):735–43.
Tobias JD. Applications of nitrous oxide for procedural sedation in the pediatric population. Pediatr Emer Care. 2013;29:245–65.
Jim’neez A, Bla’zquez D, Cruz J, et al. Use of combined transmucosal fentanyl, nitrous oxide, and hematoma block for fracture reduction in a pediatric emergency department. Pediatr Emer Care. 2012;28:676–9. Acad Emerg Med. 19:31–6.
Seith RW, Theophilos T, Babl FE. Intranasal fentanyl and high concentration inhaled nitrous oxide for procedural sedation: a prospective observational pilot study of adverse events and depth of sedation. Acad Emerg Med. 2012;19(1):31–6.
Heinrich M, Menzel C, Hoffmann F, Berger M, von Schweinitz D. Self-administered procedural analgesia using nitrous oxide/oxygen (50:50) in the pediatric surgery emergency room: effectiveness and limitations. Eur J Pediatr Surg. 2015;25:250–6.
Hee HI, Goy RWL, Ng ASB. Effective reduction of anxiety and pain during venous cannulation in children: a comparison of analgesic efficacy conferred by nitrous oxide, EMLA and combination. Paed Anaesth. 2003;13:210–6.
Mahmoud M, Mason KP. Dexmedetomidine: review, update, and future consideration of paediatric perioperative and periprocedural application and limitations. Br J Anaesth. 2015;115:171–82.
Mason KP, Lerman J. Review article: dexmedetomidine in children: current knowledge and future applications. Anesth Analg. 2011;113:1129–42.
Ebert TJ, Hall JE, Barney JA, et al. The effects of increasing plasma concentrations of dexmedetomidine in humans. Anesthesiology. 2000;93:382–94.
Mason KP, Lubisch NB, Robinson F, Roskos R. Intramuscular dexmedetomidine sedation for pediatric MRI and CT. AJR Am J Roetgenol. 2011;197:720–5.
Mason KP, Zurakowski D, Zgleszewski SE, et al. High dose dexmedetomidine as the sole sedative for pediatric MRI. Paediatr Anaesth. 2008;18:403–11.
Zub D, Berkenbosch JW, Tobias JD. Preliminary experience with oral dexmedetomidine for procedural and anesthetic premedication. Pediatr Anesth. 2005;15:932–93.
Iirola T, Vilo S, Manner T, et al. Bioavailability of dexmedetomidine after intranasal administration. Eur J Clin Pharmacol. 2011;67:825–31.
Mason KP, Lubisch N, Robinson F, et al. Intramuscular dexmedetomidine: an effective route of sedation preserves background activity for pediatric electroencephalograms. J Pediatr. 2012;161:927–32.
Yuen VM, Irwin MG, Hui TW, et al. A double-blind cross-over assessment of the sedative and analgesic effects of intranasal dexmedetomidine. Anesth Analg. 2007;105:374–80.
Mekitarian Fiho E, Robinson F, de Carvalho WB, et al. Intranasal dexmedetomidine for sedation for pediatric computed tomography imaging. J Pediatr. 2015;166:1313–5.
Lubisch N, Roskos R, Berkenbosch JW. Dexmedetomidine for procedural sedation in children with autism and other behavior disorders. Pediatr Neurol. 2009;41:88–94.
Makary L, Vornik V, Finn R, et al. Prolonged recovery associated with dexmedetomidine when used as a sole sedative agent in office-based oral and maxillofacial surgery procedures. J Oral Maxillofac Surg. 2010;68:386–91.
Mahmoud M, Gunter J, Donnelly LF, et al. A comparison of dexmedetomidine with propofol for magnetic resonance imaging sleep studies in children. Anesth Analg. 2009;109:745–53.
Ray T, Tobias JD. Dexmedetomidine for sedation during electroencephalographic analysis in children with autism, pervasive developmental disorders, and seizure disorders. J Clin Anesth. 2008;20:364–8.
Li BL, Yuen VM, Zhang N, et al. A comparison of intranasal dexmedetomidine and dexmedetomidine plus buccal midazolam for non-painful procedural sedation in children with autism. J Autism Dev Disord. 2019;49:3798–806.
Wong J, Steil GM, Curtis M, et al. Cardiovascular effects of dexmedetomidine sedation in children. Anesth Analg. 2012;114:193–9.
Dawes J, Myers D, Gorges M, et al. Identifying a rapid bolus dose of dexmedetomidine (ED50) with acceptable hemodynamic outcomes in children. Pediatr Anesth. 2014;24:1260–7.
Chen F, Wang C, Lu Y, Huang M, Fu Z. Efficacy of different doses of dexmedetomidine as a rapid bolus for children: a double-blind, prospective, randomized study. BMC Anesth. 2018;18:103.
Poonai N, Spohn J, Vandermeer B, et al. Intranasal dexmedetomidine for procedural distress in children: a systematic review. Pediatrics. 2020;145(1):e20191623.
Anttila M, Penttilä J, Helminen A, Vuorilehto L, Scheinin H. Bioavailability of dexmedetomidine after extravascular doses in healthy subjects. Br J Clin Pharmacol. 2003;56:691–3.
Li A, Yuen VM, Goulay-Dufay S, et al. Pharmacokinetic and pharmacodynamic study of intranasal and intravenous dexmedetomidine. Br J Anaesth. 2018;120(5):960–8.
Miller JW, Balyan R, Dong M, et al. Does intranasal dexmedetomidine provide adequate plasma concentrations for sedation in children: a pharmacokinetic study. Br J Anaesth. 2018;120(5):1056–65.
Uusalo P, Guillaume S, Siren S, et al. Pharmacokinetics and sedative effects of intranasal dexmedetomidine in ambulatory pediatric patients. Anesth Analg. 2019; in press
Neville DNW, Hayes KR, Ivan Y, McDowell ER, Pitetti RD. Double-blind randomized controlled trial of intranasal dexmedetomidine versus intranasal midazolam as anxiolysis prior to pediatric laceration repair in the emergency department. Acad Emerg Med. 2016;23:910–7.
Yuen VM, Hui TW, Irwin MG, et al. Optimal timing for the administration of intranasal dexmedetomidine for premedication in children. Anaesth. 2010;65:922–9.
Ghai B, Jain K, Saxena AK, Bhatia N, Sodhi KS. Comparison of oral midazolam with intranasal dexmedetomidine premedication for children undergoing CT imaging: a randomized, double-blind, and controlled Study. Pediatr Anesth. 2017;27:37–44.
McNaughton C, Zhou C, Robert L, Storrow A, Kennedy R. A randomized, crossover comparison of injected buffered lidocaine, lidocaine cream, and no analgesia for peripheral intravenous cannula insertion. Ann Emerg Med. 2009;54(2):214–20.
Krauss BS, Krauss BA, Green SM. Managing procedural anxiety in children. N Engl J Med. 2016;374:e19. (video)
American College of Emergency Physicians Policy Statement. Procedural sedation in the emergency department. Am Col Emerg Phys 2017.
FDA Drug Safety Communication: New information regarding QT prolongation with ondansetron (Zofran). https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-new-information-regarding-qt-prolongation-ondansetron-zofran. Accessed 18 Apr 2020.
Beach ML, Cohen DM, Gallagher SM, Cravero JP. Major adverse events and relationship to nil per os status in pediatric sedation/anesthesia outside the operating room. A report of the pediatric sedation research consortium. Anesthesiology. 2016;124:80–8.
Chiaretti A, Barone G, Rigante D, Ruggiero A, Pierri F, Barbi E, Barone G, Riccardi R. Intranasal lidocaine and midazolam for procedural sedation in children. Arch Dis Child. 2011;96(2):160–3.
Tsze DS, Ieni M, Fenster DB, Babineau J, Kriger J, Levin B, Dayan PS. Optimal volume of administration of intranasal midazolam in children: a randomized clinical trial. Ann Emerg Med. 2017;69:600–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kennedy, R.M. (2021). Sedation in the Emergency Department: A Complex and Multifactorial Challenge. In: Mason, MD, K.P. (eds) Pediatric Sedation Outside of the Operating Room. Springer, Cham. https://doi.org/10.1007/978-3-030-58406-1_22
Download citation
DOI: https://doi.org/10.1007/978-3-030-58406-1_22
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-58405-4
Online ISBN: 978-3-030-58406-1
eBook Packages: MedicineMedicine (R0)