
Abstract
Groin and scrotal pathologies are a common occurrence in children and one of the common reasons for referral to the Paediatric Urologist. The descent of the testis to the scrotum along with the role of the patent processus vaginalis (PPV) results in formation of inguinal hernias and hydroceles in children. Management of varicocele remains controversial within the adults and now increasingly is being seen and managed by the paediatric urologist. Long term functional outcomes of the condition are still a matter of debate. Abdomino-scrotal hydrocele is a recognised congenital problem. Uncommon conditions like spermatoceles may cause diagnosis dilemmas. The aim is to look at the practical aspects of diagnosis and evidence-based approach to management.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Inguinal hernia
- Hydrocele
- Patent processus vaginalis (PPV)
- Groin
- Testis
- Varicocele
- Spermatocele
- Abdomino-scrotal hydrocele (ASH)
- Paediatric urologist
-
1.
To differentiate between the common groin/scrotal conditions that present in the paediatric age group.
-
2.
To recognize the emergency/urgent vs elective cases and to deal with it appropriately.
-
3.
To understand the investigation pathway to assist with the differential diagnosis.
-
4.
To keep updated with current management options of groin/scrotal conditions.
-
5.
To understand the nuances associated with difficult scenarios in groin/scrotal pathologies.
17.1 Inguinal Hernia
Baby boy born at 32 weeks’ gestation is on NICU. He is now 4 weeks old and the neonatal doctor has noted a lump in the left groin. It is reducible.
-
Q1. What is the most likely diagnosis?
-
Q2. What is the incidence of this condition?
-
Q3. What clinical findings help differentiate it from other conditions?
-
Q4. When is the best time to operate?
A1. The most likely diagnosis is an inguinal hernia.
A2. Inguinal hernia in children is a common presentation to the paediatric urologist. The incidence of an inguinal hernia in a term neonate is 3–5%. This increases to 10–30% with the degree of prematurity [1,2,3]. It is nearly 5 times more prevalent in boys, the right-side hernias being twice as common as the left side ones. 15% occur bilaterally [4]. Conditions that increase the risk of inguinal herniae include cystic fibrosis, hydrocephalus, peritoneal dialysis, abdominal wall defects connective tissue disorders (Ehlers Danlos syndrome) mucopolysaccharidosis (Hunter or Hurlers syndrome), ascites, cryptorchidism, congenital hip dislocation and myelomeningocele.
A3. An inguinal hernia in a child is usually an indirect hernia. The aetiology is the persistence of the patent processes vaginalis (PPV) after birth, which allows peritoneal contents like bowel and omentum to come through to present as a lump in the groin. Most parents will give a history of a bulge in the groin especially after straining or crying.
On clinical examination, positive ‘silk glove sign’ (thickened PPV in the cord) is palpated. One may feel the testis separately from the lump but cannot get above the swelling (difference from hydrocele). This lump is reducible. Large hernia may extend into the scrotum in boys. Ultrasonography may demonstrate a PPV with peritoneal contents through it but radiological investigations are not commonly used.
A4. Timing of surgery plays a key role in decision making in children. Most surgeons would prefer to repair the hernia in premature infants once they are ready to discharge from the neonatal unit [5]. Infants under the age of 6 months are operated on the next available operating list. Asymptomatic children over the age of 1 year can be operated electively. Parents are advised about the risk of incarceration and the signs and symptoms to watch for during the waiting time till surgery.
9-month-old boy is brought to the Accident and emergency department by his parents with a red tender lump in the right groin, which is irreducible.
-
Q1. What is the diagnosis?
-
Q2. What are the risks/ complications of this condition?
-
Q3. What is the management strategy for this patient?
-
Q4. What are the advantages and disadvantages of open vs laparoscopic technique of repair?
A1. This patient has an incarcerated right inguinal hernia.
A2. The complications of incarceration and bowel obstruction along with compression of cord structure is possible. Torsion and ischemia of the ovary (in females) is also known to complicate the inguinal hernia.
A3. In emergency cases of incarceration, every attempt should be made to reduce the hernia as soon as possible. In infants <3 months of age that have required manual reduction, the inguinal herniotomy should be done before discharge as these have a 15% reincarceration incidence with delayed repair after 5 days [5, 6]. In older children, the procedure can be done electively. However, in an irreducible inguinal hernia the patient should be taken to theatres for reduction and inspection of the hernial contents followed by the inguinal herniotomy.
A4. The incidence of incarceration of inguinal hernia ranges between 6 and 18%. It is much higher in infants with the risk increasing up to 30% [7]. Surgery is therefore an indication to all children presenting with an inguinal hernia. The traditional open inguinal approach still remains popular amongst Paediatric Urologists. The PPV is separated from the vas and vessels, high ligation with absorbable sutures (up to the deep ring) and divided. The risks following this procedure are low (<1%) but the potential injury to the vas and vessels remains, including wound infection, haematoma, testicular atrophy and recurrence of hernia.
Laparoscopic inguinal hernia repair has been in practice since 1993, first described by Montupet. The initial description has been of an intracorporeal repair consisting of a purse string suture in the peritoneum at the level of the internal ring [8]. Since then various modifications and variations have been introduced [9]. It can be an intracorporeal or extracorporeal/percutaneous. There is insufficient evidence to support one technique from the other [10]. The benefits of laparoscopic approach vs the traditional open technique includes visualisation of contralateral open ring, improved cosmesis and post-operative pain. However, with every laparoscopic procedure increase in length of operative timing, cost and introduction of pneumoperitoneum in small infants still remains the potential disadvantages.
Many surgeons advocate the advantage of laparoscopic approach in the oedematous groin following an episode of incarceration with subsequent manual reduction. It allows inspection of the hernial contents, viability of bowel and avoids the risk of damage to the vas and vessels, which in the open inguinal technique can prove be very challenging and associated with increased morbidity and complications.
Laparoscopy has over the years evolved with fine instruments and sophisticated technical details. It definitely has its benefits in bilateral inguinal hernia repairs, visualising uncommon conditions like direct or femoral hernia and reducing the occurrence of metachronous contralateral hernia. However, the evidence does not show either approach to be superior from one another [11]. Parents should be made aware of both techniques with advantages and disadvantages of each.
17.2 Hydrocele
2-year-old boy is seen in Accident and Emergency Department. He had a viral upper respiratory tract illness and 2 days later they have noticed a swelling in the scrotum.
-
Q1. What is the differential diagnosis of a swelling in the scrotum in a 2-year old presenting to the Accident & Emergency Department?
-
Q2. What is the usual presentation and clinical examination findings of this condition?
-
Q3. How common is this condition? Is it a congenital problem?
-
Q4. What is the best management approach?
-
Q5. Name some other types of hydrocele.
A1. The differential diagnosis of an acute scrotum would include torsion of the testis, torsion of hydatid cyst of Morgagni, inguinal hernia, hydrocele and idiopathic scrotal oedema.
A2. Most boys will present with a scrotal swelling usually noticed by the parents. It may precede a viral infection. In girls, there is a groin lump. Some parents of the toddlers give a good history of it being small first thing in the morning and noticeably bigger at the end of the day suggesting a communicating hydrocele. Non-communicating hydroceles are not as common and usually occur in older boys.
It is a painless swelling and, in most cases, the underlying testis can be felt separately. In the tense hydroceles, the testes are difficult to palpate. The ability to get above the irreducible swelling distinguishes it from an inguinal hernia. Transillumination test is positive but not a reliable test in children as the incarcerated bowel may also transilluminate. Clinical examination is enough to make a diagnosis. In some cases of doubt, ultrasonography is a reliable investigation.
A3. Hydrocele is a collection of peritoneal fluid within the tunica vaginalis testis. It is the result of persistence of the processus vaginalis, allowing fluid to communicate to the scrotum via the patent processus vaginalis (PPV). It is a common cause of swelling in the scrotum and occurs in 2–5% of boys, usually before the age of 5 years [12]. It is uncommon in girls and when present is called Hydrocele of the canal of Nuck.
Hydroceles can be classified as congenital or acquired. The acquired or secondary causes may be due to infection, trauma, torsion, tumour, or iatrogenic like following varicocele surgery. Children with indwelling ventriculo-peritoneal shunts or peritoneal dialysis have increased intraperitoneal fluid which may exacerbate a hydrocele.
A4. PPV ligation is a common procedure performed by the Paediatric Urologist. However, the surgical indications unlike that of inguinal hernia is age dependent. In a recent UK survey, most paediatric surgeons/urologists would manage hydroceles conservatively for the first 2 years of life and offer surgery if it persists beyond the age of 2–3 years [13]. However, a significant number of surgeons deferred it until 4 years and offered surgical intervention prior to the child starting school.
Surgery is performed as a day case via a groin incision, with separation of the PPV from the vas and vessels and high ligation with an absorbable suture. Laparoscopic repairs similar to inguinal hernias with aspiration of the scrotal fluid is also practised.
A5. Encysted hydrocele occurs when the fluid gets trapped within its layers during the natural closure of the processus vaginalis. Meconium hydrocele is a neonatal condition secondary to the gastrointestinal perforation leading to meconium staining of the hydrocele fluid. Non-communicating hydroceles in older boys can be approached via the scrotum and a Lord procedure (excision of excess of processus vaginalis) [13, 14] or a Jaboulay procedure (marsupialisation of the free edge of tunica vaginalis) is performed. Recurrent hydrocele is rare. Ultrasound is performed to exclude a recurrent inguinal hernia and these children may need re exploration of the groin combined with the scrotal approach.
17.3 Varicocele
15-year boy is referred to the urology clinic with 4-month history of dull ache in the left testis.
-
Q1. What is the differential diagnosis?
-
Q2. What clinical findings and investigations are key to the diagnosis?
-
Q3. What is the pathophysiology of this condition?
-
Q4. What are the indications for a surgical intervention?
-
Q5. What are the different modalities of treatment?
-
Q6. What is the effect on fertility?
A1. The differential diagnosis should always exclude torsion of the testis with careful history and clinical examination. The others include inguinal hernia, hydrocele, epididymal cyst and varicocele.
A2. The majority of boys and young adult men present with a painless scrotal swelling. At times however, there may be a dull ache or dragging sensation, exacerbated by exercise or in hot weather conditions.
On examination, the dilated veins are palpated like a ‘bag of worms’. It is imperative that the genitalia are examined in both standing and lying down positions to confirm disappearance of the dilated veins in supine position. The clinical grading system of Dublin and Amelar was recently expanded by the World Health Organisation (WHO) to include an additional ‘subclinical’ grade 0.
-
Grade 0: Subclinical, detected on ultrasound only.
-
Grade 1: Palpable on Valsalva’s manoeuvre
-
Grade 2: Palpable (not visible) without Valsalva’s manoeuvre
-
Grade 3: Visible, negating the need for palpation
-
Testicular size or volume should also be assessed as baseline during the physical examination. This is useful for assessing size and volume discrepancy between the two sides to direct further follow up. Various methods such as Prader orchidometer, Rochester (Takihara) orchidometer, rulers and callipers have been used to evaluate the testicular size and volume. Lambert’s formula is widely used for calculating the testis volume (in millilitres) when applying a two-dimensional measuring system. As described by Lambert, the volume is calculated by multiplication of width x length x depth in centimetres by a constant usually 0.71 [15].
Ultrasonography is now increasing being used to confirm the diagnosis and accurately document the testicular size. Ultrasound is a more reliable method as compared to an orchidometer as there are less inter-observer differences with the imaging modality [15, 16].
It is to be noted that right sided varicoceles are rare. Varicocele in a young child is equally rare. An abdominal ultrasound is recommended to rule out neoplasms such as Wilms tumour in very young children as a varicocele may be a secondary finding in such cases due to venous congestion.
A3. Varicocele is described as an abnormal enlargement of the pampiniform venous plexus that drains blood from the testis. The prevalence in children and adolescents is estimated to be between 10 and 15% [17] and it is uncommon in boys under 10 years of age [18].
The pampiniform plexus drains mainly into the testicular vein which drains further into the inferior vena cava on the right and into the renal vein on the left. The testicular vein draining into the left forms an approximately 90-degree angle that leads to the left renal vein being easily compressed between the adjacent superior mesenteric artery and the aorta, thus resulting in impeded venous drainage from the left testis, described as the nutcracker effect [18, 19]. This anatomical difference between the right and the left venous drainage can explain the predominant left sided varicocele formation.
A4. In the year 2016, The European Urology Pediatric Guidelines made the following recommendations with regards criteria for varicocele treatment in children and adolescents: varicocele associated with low testicular volume, presence of an additional testicular condition with affected fertility, varicoceles that are bilateral and palpable, abnormal sperm quality in older adolescents with varicoceles, or symptomatic varicoceles- irrespective of the grade of the varicocele. Regular follow up with clinical examination and ultrasound to measure the testicular size is recommended.
Of note, in a study by Cervellione et al., 28% of their subclinical varicocele cohort progressed on to a clinically detectable varicocele at 4 year follow up, and 67% remained unchanged [20].
A5. Varicoceles can be treated by various techniques. The basic principle of treatment is to interrupt the venous return through the internal spermatic vein. Angiographic occlusion of the internal spermatic veins can be performed by retrograde or antegrade injection of a sclerosing agent. This technique is considered as lymphatic and internal artery sparing technique, which in turn prevents hydrocele formation. Failure rate varies between 5 and 20% [21].
Surgical approach may either be an inguinal approach (Ivanissevich), the high approach (Paloma) or the microsurgical approach. The microsurgical repair technique is considered to have fewer complications and lower recurrence rates of all but does require extensive microsurgical training.
The Paloma technique is widely adopted in clinical practice. It is an open surgical approach with access achieved proximally on the spermatic vessels.
Laparoscopic varicocelectomy follows the same principles as the Paloma procedure. Its advantages include early post-operative recovery, better optic magnification and cosmesis, though the success rates are reported to be similar to the open procedure.
Published meta-analysis in children show that results after laparoscopic technique are similar to open with recurrence rates of 8.6 and 4.7% respectively and post-operative hydrocele rate of 6.7 and 7.1% respectively. Laparoscopic lymphatic sparing approach has a lower incidence of hydrocele (4.3 vs. 17.6%) but higher incidence of recurrence (3.5 vs. 2.2%) than the Paloma procedure [21, 22]. There is low level of evidence in support of radiological or surgical intervention for varicoceles in children and adolescents to improve testicular volume or sperm concentration [23].
A6. There is a normal 10% size variation between the two testes [24]. Studies by Diamond et al. showed that relative testicular size discrepancy greater than 10% in Tanner stage 5 adolescents is associated with decreased sperm concentration and total sperm count [25]. Further, sperm abnormality was greater for volume differences in excess of 20% between the two sides [25, 26]. Also to note, small ipsilateral testis has shown that corrective surgery may result in catch up growth in 80% of those testes [27]. The cause and relationship between varicocele and fertility is not fully clear or understood. Studies have shown that the prevalence of varicocele is 20–40% in men seeking investigations for fertility reasons [27,28,29]. However, only 15–20% of men with varicocele require treatment for infertility, suggesting that most men with varicocele do not report any adverse fertility issues [30]. This fact is important to emphasise during counselling of adolescent boys and their parents and post pubertal boys should be offered semen analysis to confirm appropriate sperm count and motility as baseline.
17.4 Abdomino-Scrotal Hydrocele
6-month-old boy is referred to the clinic with a large inguinal scrotal lump. He is asymptomatic.
-
Q1. What is the differential diagnosis?
-
Q2. What clinical examination and radiological investigations help with the diagnosis?
-
Q3. Is this a congenital abnormality? What is the pathophysiology of this condition?
-
Q4. (a) What are the indications for surgical management?
-
(b) What is the surgical approach?
A1. The differential diagnosis includes inguinal scrotal hernia, lymphatic malformation and Abdomino-Scrotal Hydrocele (ASH).
A2. On clinical examination, a combination of a scrotal swelling with an abdominal swelling just above the inguinal ligament, ASH should be suspected. The cross fluctuant between the tense hydrocele and abdominal mass is the ‘Springing back ball’ sign [31]. A cough impulse may be present. It can be partially reduced or emptied on lying supine. Trans-illumination test is positive. Ultrasound is diagnostic. Contrast enhanced compute tomography or magnetic resonance imaging are useful investigations to demonstrate the extension of the hydrocele. Other commonly associated pathologies that occurs in nearly 20% of cases include ipsilateral or contralateral cryptorchidism, contralateral inguinal hernia or simple hydrocele [32].
A3. Abdomino-scrotal hydrocele (ASH) is a rare congenital abnormality of the processes vaginalis. It is characterised by a fluid filled mass in the inguinal scrotal area with a hidden, often deep intra-abdominal component that communicates in an hour glass fashion through the inguinal canal. The incidence is between 1.25 and 3.1% of all hydroceles noted in infancy [32, 33]. The incidence of ASH increasing with the expanding use of Ultrasonography. Bilateral ASH is rare.
There is only one sonographic report of prenatal detection [34]. The first paediatric case was reported by Syme, though the term ASH was termed by Bickel in 1919. Dupuytren described it a ‘hydrocele en bisac’ in 1834. The aetiology is unclear. Many theories are postulated including the valve theory, diverticulum theory and displacement as per Laplace’s theory [35]. The most popular and accepted theory is that of Dupuytren’s which suggests that excessive intracystic pressure causes cephalad extension of the scrotal swelling through the deep inguinal ring [35].
A4 (a) Recent Systematic review (Doudt et al) showed there were no cases of complete spontaneous resolution [32]. The potential for compressive or secondary effects like lower extremity oedema, hydronephrosis, torsion, haemorrhage, infection and the tangible chance of malignant transformation are indications for surgical intervention [31, 32].
(b) Various surgical approaches have been described in the literature. The inguinal approach is the most common, however given individual presentations combined inguinal+ extra peritoneal, combined inguinal+ scrotal approach is also described. A standard inguinal skin crease incision and the external oblique fascia and muscles are opened. The inguinal component of ASH is exposed. The tense hydrocele makes it difficult to separate it from the surrounding stricture. Aspiration of fluid from the scrotum rather than the inguinal area facilitates the procedure [32]. A patch of tunica vaginalis can be left attached to the spermatic cord structures when the hydrocele is associated with a thickened wall as separation of vas and vessels will be difficult and results in bleeding. The key principle is to excise the abdominal and scrotal component. The PPV is not always seen. Pre-operative clinical grading (simple and complex with further subclasses) has been proposed that may support differentiation of severity of the associated cumulative risks [32, 36].
17.5 Spermatocele
15-year-old boy is referred to the Urology clinic. The GP had arranged an ultrasound of the scrotum for another pathology and it showed a 1 cm extra testicular cystic structure. The patient is asymptomatic.
-
Q1. What is the differential diagnosis?
-
Q2. What is the difference between the two diagnoses?
-
Q3. (a) What are the typical clinical findings?
-
(b) What are the characteristic features seen on ultrasound to help with the diagnosis?
-
Q4. How should this patient be managed?
-
Q5. What is the effect on fertility with surgical intervention?
A1. The differential diagnosis includes Epididymal cyst or a Spermatocele.
A2. Spermatocele or spermatic cyst is a fluid-filled sac within the epididymis. It is a common type of extra testicular cyst and represents cystic dilatation of the tubules of the efferent ductules in the head of the epididymis. They sometimes can develop in varying locations from the testicle to locations along the course of vas deferens [37]. These are benign cysts and similar to epididymal cysts. The difference being the spermatocele contains fluid and sperm cells. Spermatoceles are not common in children but when they occur, they usually present around puberty.
A3. (a) Spermatoceles present with a painless lump felt just above and separate to the testicle. It is usually small in size ranging from a few mm to 2 cm, however large lesions up to 8 cm have been reported. Transillumination may be possible to differentiate it from solid lesions [37, 38].
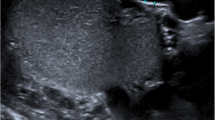
(b) Ultrasound shows typical appearances of spermatocele. MRI is therefore not indicated. These cystic lesions show no arterial or venous blood flow within them on colour Doppler [38]. It appears as a unilocular or a multilocular hypoechoic cystic lesion. They may show low level echogenic internal echoes due to proteinaceous fluid containing dead sperms [38, 39].
A4. Small cysts are best left alone. Large asymptomatic cysts can be regularly followed up. The cyst if become symptomatic and causes discomfort or is increasing in size should be considered for removal [40]. Spermatocelectomy or excision of the cyst under general anaesthetic is performed in young boys. Aspiration of the fluid followed by injection of sclerosing agent (99.5% alcohol, phenol, 5% ethanolamine) is an alternative to surgery [41].
A5. The surgical procedure itself does not improve fertility. Sclerosing agents should be used with caution in reproductive-aged men for the risk of inducing chemical epididymitis which further may cause epididymal damage and possible future infertility.
References
Harper RG, Garcia A, Sia C. Inguinal hernia: a common problem of premature infants weighing 1,000 grams or less at birth. Pediatrics. 1975;56:112–5.
Kumar VHS, Clive J, Rosenkrantz TS, Bourque MD, Hussain N. Inguinal hernia in preterm infants (≤32-week gestation). Pediatr Surg Int. 2002;18:147–52.
Grosfeld JL. Current concepts in inguinal hernia in infants and children. World J Surg. 1989;13:506–15.
Six thousand three hundred sixty-one pediatric inguinal hernias: a 35-year review. In: Paperpile. https://paperpile.com/app/p/65f11b78-2cb5-0c7a-9594-0c05d5a7c824. Accessed 18 Mar 2019.
Groff DB. Inguinal hernias in premature infants operated on before discharge from the neonatal intensive care unit. Arch Surg. 1985;120:962.
Koivusalo A, Pakarinen MP, Rintala RJ. Laparoscopic herniorrhaphy after manual reduction of incarcerated inguinal hernia. Surg Endosc. 2007;21:2147–9.
Parelkar SV, Oak S, Gupta R, Sanghvi B, Shimoga PH, Kaltari D, Prakash A, Shekhar R, Gupta A, Bachani M. Laparoscopic inguinal hernia repair in the pediatric age group—experience with 437 children. J Pediatr Surg. 2010;45:789–92.
Esposito C, St. Peter SD, Escolino M, Juang D, Settimi A, Holcomb GW. Laparoscopic versus open inguinal hernia repair in pediatric patients: a systematic review. Journal of Laparoendoscopic & Advanced Surgical Techniques. 2014;24:811–8.
Ostlie DJ, Ponsky TA. Technical options of the laparoscopic pediatric inguinal hernia repair. Journal of Laparoendoscopic & Advanced Surgical Techniques. 2014;24:194–8.
Esposito C, Escolino M, Farina A, Settimi A. Two decades of history of laparoscopic pediatric inguinal hernia repair. J Laparoendosc Adv Surg Tech A. 2014;24:669–70.
Esposito C, Escolino M, Turrà F, Roberti A, Cerulo M, Farina A, Caiazzo S, Cortese G, Servillo G, Settimi A. Current concepts in the management of inguinal hernia and hydrocele in pediatric patients in laparoscopic era. Semin Pediatr Surg. 2016;25:232–40.
Madden N (2008) Testis, hydrocoele and varicocoele. Essen Paediatr Urol, 2nd ed, p 247–263.
Jobson M, Hall NJ. Current practice regarding timing of patent processus vaginalis ligation for idiopathic hydrocele in young boys: a survey of UK surgeons. Pediatr Surg Int. 2017;33:677–81.
Koutsoumis G, Patoulias I, Kaselas C. Primary new-onset hydroceles presenting in late childhood and pre-adolescent patients resemble the adult type hydrocele pathology. J Pediatr Surg. 2014;49:1656–8.
Paltiel HJ, Diamond DA, Di Canzio J, Zurakowski D, Borer JG, Atala A. Testicular volume: comparison of orchidometer and US measurements in dogs. Radiology. 2002;222:114–9.
Diamond DA, Paltiel HJ, DiCanzio J, Zurakowski D, Bauer SB, Atala A, Ephraim PL, Grant R, Retik AB. Comparative assessment of pediatric testicular volume: orchidometer versus ultrasound. J Urol. 2000:1111–4.
Meacham RB, Townsend RR, Rademacher D, Drose JA. The incidence of varicoceles in the general population when evaluated by physical examination, gray scale sonography and color Doppler sonography. J Urol. 1994;151:1535–8.
Akbay E, Çayan S, Doruk E, Duce MN, Bozlu M. The prevalence of varicocele and varicocele-related testicular atrophy in Turkish children and adolescents. BJU Int. 2000;86:490–3.
Stassen CM, Weil EH, Janevski BK. Left renal vein compression syndrome (“nutcracker phenomenon”). Rofo. 1989;150:708–10.
Cervellione RM, Corroppolo M, Bianchi A. Subclinical Varicocele in the pediatric age group. J Urol. 2008;179:717–9.
Clarke SA, Agrawal M, Reidy J. Percutaneous transfemoral testicular vein embolisation in the treatment of childhood varicocoele. Pediatr Radiol. 2001;31:515–7.
Borruto FA, Impellizzeri P, Antonuccio P, Finocchiaro A, Scalfari G, Arena F, Esposito C, Romeo C. Laparoscopic vs open varicocelectomy in children and adolescents: review of the recent literature and meta-analysis. J Pediatr Surg. 2010;45:2464–9.
Locke JA, Noparast M, Afshar K. Treatment of varicocele in children and adolescents: a systematic review and meta-analysis of randomized controlled trials. J Pediatr Urol. 2017;13:437–45.
Zachmann M, Prader A, Kind HP, Häfliger H, Budliger H. Testicular volume during adolescence. Cross-sectional and longitudinal studies. Helv Paediatr Acta. 1974;29:61–72.
Diamond DA, Zurakowski D, Bauer SB, Borer JG, Peters CA, Cilento BG Jr, Paltiel HJ, Rosoklija I, Retik AB. Relationship of varicocele grade and testicular hypotrophy to semen parameters in adolescents. J Urol. 2007;178:1584–8.
Kurtz MP, Zurakowski D, Rosoklija I, Bauer SB, Borer JG, Johnson KL, Migliozzi M, Diamond DA. Semen parameters in adolescents with Varicocele: association with testis volume differential and Total testis volume. J Urol. 2015;193:1843–7.
Costabile RA, Skoog S, Radowich M. Testicular volume assessment in the adolescent with a varicocele. J Urol. 1992;147:1348–50.
Organization WH, World Health Organization. The influence of varicocele on parameters of fertility in a large group of men presenting to infertility clinics**Supported by the Special Programme of Research, Development, and Research Training in Human Reproduction, World Health Organization, Geneva, Switzerland. Fertil Steril. 1992;57:1289–93.
Bogaert G, van den Heijkant M, Albersen M. Varicocele in children and adolescents: a challenge for diagnosis and treatment indications. Eur Urol Suppl. 2017;16:171–6.
Skoog SJ, Roberts KP, Goldstein M, Pryor JL. The adolescent Varicocele: What’s new with an old problem in young patients? Pediatrics. 1997;100:112–27.
Wlochynski T, Wassermann J, Generowicz Z. Abdominoscrotal hydrocele in childhood. J Pediatr Surg. 1993;28:248–50.
Doudt AD, Kehoe JE, Ignacio RC, Christman MS. Abdominoscrotal hydrocele: a systematic review. J Pediatr Surg. 2016;51:1561–4.
Avolio L, Chiari G, Caputo MA, Bragheri R. Abdominoscrotal hydrocele in childhood: is it really a rare entity? Urology. 2000;56:1047–9.
Sasidharan P, Crankson S, Ahmed S. Fetal abdominoscrotal hydrocele. Am J Obstet Gynecol. 1991;165:1353–5.
Kamble PM, Deshpande AA, Thapar VB, Das K. Large abdominoscrotal hydrocele: uncommon surgical entity. Int J Surg Case Rep. 2015;15:140–2.
Gadelkareem RA. Abdominoscrotal hydrocele: a systematic review and proposed clinical grading. Afr J Urol. 2018;24:83–92.
Rioja J, Sánchez-Margallo FM, Usón J, Rioja LA. Adult hydrocele and spermatocele. BJU Int. 2011;107:1852–64.
Tartar VM, Trambert MA, Balsara ZN, Mattrey RF. Tubular ectasia of the testicle: sonographic and MR imaging appearance. Am J Roentgenol. 1993;160:539–42.
Jain N, Chauhan U, Sethi S, Goel V, Puri SK. Tubular Ectasia of rete testis with Spermatocele. J Clin Diagn Res. 2015;9:TJ03–4.
Gray CL, Powell CR, Amling CL. Outcomes for surgical Management of Orchalgia in patients with identifiable intrascrotal lesions. Eur Urol. 2001;39:455–9.
Shan CJ, Lucon AM, Pagani R, Srougi M. Sclerotherapy of hydroceles and spermatoceles with alcohol: results and effects on the semen analysis. Int Braz J Urol. 2011;37:307–13.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kumar, N., Mushtaq, I. (2021). Inguinal Hernia, Hydrocele, Varicocele, Spermatocele and Abdomino-Scrotal Hydrocele. In: Godbole, P., Wilcox, D.T., Koyle, M.A. (eds) Practical Pediatric Urology. Springer, Cham. https://doi.org/10.1007/978-3-030-54020-3_17
Download citation
DOI: https://doi.org/10.1007/978-3-030-54020-3_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-54019-7
Online ISBN: 978-3-030-54020-3
eBook Packages: MedicineMedicine (R0)