
Abstract
Operative time is the most reported outcome to measure learning curve and proficiency in robotic surgery. Furthermore, little attention is paid to procedure-independent variables. Consequently, the gently descending trend line of ‘console time’ will reassure operators that their times are improving, but no information as to the number of cases to competence, assessment on their technical ability to place ports or dock the robot, nor any appraisal of inflections in the curve are presented. As they are involved heavily with positioning of the patient and of the robot, the effect of the fluidity of the ‘robotic team’ is also underrated when purely operative durations are considered.
Cumulative summation curve analysis (CUSUM) is a straightforward way to present data in a different fashion, with the result that information becomes usable, both for predicting learning curves and retrospective analyses. It can define when the switch from learning to maintenance phases occurs, in turn aiding training programs. The inflections seen when plotting the data can be revisited to investigate why progress stalled or improved. In addition, as it is vital to see every robotic case as a team effort, we encourage data from both procedure-dependent and independent sources be analysed in a similar way, to inform and improve the entire programme.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
As this piece is written, a PubMed search for “learning curve” and “robotic surgery” yields 1222 results. The latest study into the effect of 23 years of paediatric fellowship programs on the robotic learning curve shows that in 17 articles comprising 721 procedures, operative time is the most reported outcome to measure learning curve and proficiency [1]. Furthermore, the literature is replete with examples of procedure-specific advances within robotics but less well represented by procedure-independent variables. These factors are often removed from analyses so as not to distort the primary outcome measure of console time—the time it takes to perform the procedure [2]. When a surgeon begins robotic surgery, it can be reasonably assumed that the procedures being performed have been previously practised laparoscopically or in an open fashion, so essentially all that is being measured is how slick the surgeon is at using the console. The effects of an ever-increasing body of work with simple procedure duration curves are that there is limited accurate information available on the number of procedures that should be performed for the learning curve to have been completed and that the effect of the robotic team is negated. The solution to this issue is twofold. First, data should be interpreted in a different way, with the aim to define when the switch from learning to maintenance phases occurs, which can in turn aid training programs. Second, it is vital to see every robotic case as a team effort, and so data from both procedure-dependent and independent sources must be analysed. The approach we have taken in Leeds is to use CUSUM analysis.
2 CUSUM Analysis
Cumulative Summation curve analysis was first described by Page in 1954 [3], as a method to represent data from consecutive procedures, transforming the variability of raw data into a cumulative sum of differences between each value and the mean [4]. The process is straightforward. First, the mean of all the values (X1, X2, X3 etc.) is calculated (X). The first CUSUM value starts at zero (S0) and subsequent CUSUM values are calculated by adding the difference between the current value and the average value to the previous CUSUM:
\( {\mathrm{CUSUM}}_{(4)}={\mathrm{CUSUM}}_{(3)}+\left({X}_{(4)}-\underline{X}\right) \)
If values are above average, CUSUM is positive and the slope is upward, whereas if values are below average, CUSUM is negative and the slope is downward. Therefore, the perfect learning curve would follow a bell-shaped curve pattern, shown in Fig. 111.1, with the upward slope (learning phase) representing the time during which outcomes exceeded the mean and the downward slope (maintenance phase) representing the time where the procedure took less time than the mean, towards achieving proficiency when the graph is continuously declining or maintained at zero.

Idealised CUSUM curve
The asymptote represents the number of cases required to achieve competence. Inflections in the curve represent moments of deviation of progression. CUSUM charts can therefore be used to take a retrospective look at the data to identify time points where progress was interrupted; such analysis is extremely difficult in a simple case/duration chart. Consider the graph in Fig. 111.2 for the time it takes a person to run a given distance 50 times.

Time to complete run
The graph shows a general improvement in time consistent with improved fitness and technique. A trendline has been added to prove that the runner is getting faster over the 50 races. However, when the runner looks back on their achievement, there are no clues as to whether any factors specifically affected races. If we apply CUSUM analysis to this data, the graph in Fig. 111.3 appears.

CUSUM
Broadly, this follows a bell-shaped curve, as expected. However, the runner notices that the downward curve to proficiency is interrupted by an inflection point (arrowed). Looking at the date of run 35, they recall this was when they sustained a sprained ankle, which affected them for the next few runs, before improving steadily once again.
Applying this process to robotic surgery, the benefits of the CUSUM curve include the ability to monitor surgical performance by smoothing natural data variance, identifying when trainees should be becoming competent by the asymptote, and making trends more apparent and to provide early and sensitive detection of small process changes by inspecting curve inflection points.
Figure 111.4 shows the robotic time for one surgeon’s first 37 pyeloplasties (RS). The trendline shows an improvement in speed at the console.

Pyeloplasty robotic time
Converting the same data into a CUSUM curve shows a double bell-shaped curve, which was surprising given the raw data. The asymptote reveals that competence in the procedure occurred after 13 cases, but the descending slope was interrupted by a major inflection, resulting in another period of learning, or adaption, then another maintenance phase (Fig. 111.5).

CUSUM robotic time for pyeloplasty
Looking back at around case 21, this correlated with a period where some of the pyeloplasties prior to this had returned obstructed, requiring redo procedures. It was discovered that the cause of this had been the use of V-lock suture, which had caused an intense inflammatory reaction in the renal pelvises, a complication which we have since published [5]. It had taken a number of weeks to discover the cause, during which many variables were investigated, including operator technique, and this in turn was clearly reflected in the CUSUM curve.
3 Procedure-Independent Variables
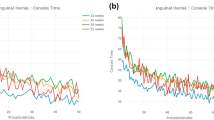
Assessment of the purely surgical components of robotic surgery ignores procedure-independent variables and appraisal of how well the team works together. Examples of such factors include patient positioning, port placement, manipulation of the robot into a suitable position adjacent to the patient and docking the robot arms. These ‘soft’ factors are vital to the smooth running of a robotic case and rely on interactions with the entire surgical team. We postulated that these factors may have a learning curve of their own, perhaps more important than the console time, as they are more powerfully linked to the development of new practice in the theatre. To assess this, we looked at case duration and CUSUM curves for the ‘docking time’, which is the time it takes from first incision to docking the robot (Fig. 111.6). This is important because it occurs in every robotic case, no matter which operation is to be performed. The first 137 cases for the same surgeon (RS) were analysed, which included pyeloplasty, nephrectomy, Mitrofanoff, ureteric reimplantation, detrusorotomy, heminephroureterectomy, varicocele ligation, and second-stage orchidopexy.

(a) Docking time. (b) CUSUM docking time
Again, the case duration curve is relatively meaningless in comparison to the CUSUM curve, which reveals a learning curve of 30 cases. It is perhaps not surprising that this is greater than the time to competence for an actual robotic operation, because the robotic time demands brand new technical skills required of the team. The major inflection in the graph at case 77 represented a period of time when two new operations were introduced (Mitrofanoff with detrusorotomy and ureteric reimplant), both requiring different port positioning to the frequently performed procedures. In addition, a new member of the team (AT) began to learn the concepts of robotics by performing the placement of the ports and docking of the robot for the more basic procedures.
4 Summary
CUSUM analysis allows the data collected to be presented in a fashion which allows assessment of progression of learning and retrospective interpretation of deviations from that progression. It allows robotic training programs to be devised and pitfalls to be anticipated. The ‘noise’ produced by a simple duration curve, often utilised to demonstrate temporal efficiency, is too great to reveal the subtleties of our practice, resulting in little meaningful data being gleaned from them. Our experience also highlights the importance of a dedicated robotic team, for planning and execution of individual tasks, where the need for special training to meet defined standards is essential for safe and successful robotic practice [6].
References
Pio L, Musleh L, Paraboschi I, Pistorio A, Mantica G, Clermidi P, et al. Learning curve for robotic surgery in children: a systematic review of outcomes and fellowship programs. J Robot Surg [Internet]. 2019 Sep 17 [Cited 2019 Sep 28];Epub ahead. Available from: http://www.ncbi.nlm.nih.gov/pubmed/31531753
Tasian GE, Wiebe DJ, Casale P. Learning curve of robotic assisted pyeloplasty for pediatric urology fellows. J Urol. 2013;190(4 Suppl):1622–6.
Page ES. Continuous inspection schemes. Biometrika. 1954;41(1–2):100–15.
Cundy TP, Rowland SP, Gattas NE, White AD, Najmaldin AS. The learning curve of robot-assisted laparoscopic fundoplication in children: a prospective evaluation and CUSUM analysis. Int J Med Robot Comput Assist Surg. 2015;11(2):141–9.
Radford A, Turner A, Ashraf J, Subramaniam R. Robotic pyeloplasty in children: a “barbed” shortcut. J Laparoendosc Adv Surg Tech. 2018;28(4):486–9.
Van Batavia JP, Casale P. Robotic surgery in pediatric urology. Curr Urol Rep [Internet]. 2014 May [Cited 2019 Sep 28];15(5):402. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24658829
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Turner, A.M., Subramaniam, R. (2021). CUSUM Analysis and the Learning Curve. In: Gharagozloo, F., Patel, V.R., Giulianotti, P.C., Poston, R., Gruessner, R., Meyer, M. (eds) Robotic Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-53594-0_111
Download citation
DOI: https://doi.org/10.1007/978-3-030-53594-0_111
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-53593-3
Online ISBN: 978-3-030-53594-0
eBook Packages: MedicineMedicine (R0)