
Abstract
Behavioral variant frontotemporal dementia (bvFTD) is a syndrome defined by a set of core clinical criteria, which include disinhibition; apathy or inertia; loss of sympathy or empathy; perseverative, stereotyped, or compulsive/ritualistic behavior; and hyperorality. The clinical features of bvFTD overlap substantially with those of psychiatric disease, particularly major depressive disorder and bipolar affective disorder. The similarities between bvFTD and primary psychiatric disease results in a significant diagnostic challenge for clinicians. Understanding the neuropsychiatric aspects of bvFTD may assist in differentiating bvFTD from a primary psychiatric disorder.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Frontotemporal dementia
- Frontotemporal lobar degeneration
- Behavioral symptoms
- Neuropsychiatry
- Psychiatric disorders
- Dementia
Introduction
Frontotemporal dementia (FTD) is a clinically and neuropathologically heterogenous neurodegenerative disorder characterized by disturbances in behavior, personality, and language associated with degeneration of frontal and temporal brain regions [1]. FTD consists of three clinical variants distinguished by the predominant presenting symptoms: behavioral variant FTD (bvFTD), semantic variant primary progressive aphasia (svPPA), and nonfluent/agrammatic variant primary progressive aphasia (nfvPPA) [2, 3]. Additionally, there are several related disorders which share features with FTD, including FTD with motor neuron disease (FTD-MND), corticobasal syndrome (CBS), and progressive supranuclear palsy (PSP).
Behavioral variant FTD is the most common form of FTD and comprises over 50% of all FTD cases [4]. The syndrome has an early age of onset with a mean of 58 years of age. The time between disease onset and the initial evaluation is approximately 3 years and the duration of the illness is approximately 8 years [2].
Behavioral variant FTD is characterized by a set of core diagnostic criteria proposed by Rascovsky et al. in 2011, which include behavioral disinhibition; apathy or inertia; loss of sympathy or empathy; perseverative, stereotyped, or compulsive/ritualistic behavior; hyperorality; and executive dysfunction (Table 1) [2]. All but one of these criteria (executive dysfunction) are behavioral in nature and have overlapping features with many psychiatric syndromes, including schizophrenia, obsessive-compulsive disorder (OCD), bipolar disorder (BPD) and major depressive disorder (MDD). Not surprisingly, many patients with bvFTD are mistakenly diagnosed with a primary psychiatric condition [5].
The neuroanatomical correlates of bvFTD typically show a pattern of atrophy in the frontal and anterior temporal lobes, with the right hemisphere being predominately affected. The earliest structures involved include the anterior cingulate cortex (ACC), anterior insula (AI), and orbitofrontal cortex (OFC). As the disease progresses, atrophy is found in the dorsolateral prefrontal cortex (dlPFC), frontal poles, dorsal insula (DI), striatum, thalamus, and anterior hippocampus. In later stages of the disease, atrophy becomes more widespread and involves the posterior hippocampi, posterior insula (PI), and parietal lobes, regions that are prominently involved in Alzheimer’s disease (AD) [6]. For that reason, in the late stages of bvFTD, there is considerable overlap with AD.
Neuropsychiatric Features of bvFTD
The bvFTD syndrome has substantial overlap with the symptomology of multiple primary psychiatric conditions, which presents a significant diagnostic challenge for clinicians. The difficulty in diagnostic accuracy is delineated in a study by Woolley et al. [5], who performed a systematic, retrospective, blinded chart review of 252 patients at the University of California, San Francisco Memory and Aging Center in order to identify the rate of psychiatric diagnoses which precede that of a neurodegenerative disorder. Of this population, 71 patients (28.2%) received a psychiatric diagnosis prior to ultimately being diagnosed with a neurodegenerative disorder, and approximately 50% with bvFTD were first diagnosed with a primary psychiatric disorder [5]. This study highlights the importance of understanding the key features of bvFTD in order to make an accurate diagnosis.
In this section, we will outline the neuropsychiatric features of bvFTD followed by a brief review of the overlap between bvFTD and primary psychiatric conditions, namely, MDD and BPD.
Disinhibition
Disinhibition is an early symptom of bvFTD and is present in 76% of cases at the time of the initial evaluation [2]. Disinhibition is often the most salient feature of bvFTD as patients frequently exhibit impulsivity, socially inappropriate behavior, and loss of social decorum attributable to aberrant reward processing and a lack of regard for potential consequences of inappropriate actions [2, 7, 8].
The most common manifestation of behavioral disinhibition is impulsivity [9], such as new-onset gambling or substance use, excessive spending, reckless behavior, or oversharing of personal information [2, 9, 10]. Violation of social norms often includes overfamiliarity, inappropriate touching, and inappropriate sexual acts [2, 11, 12]. Additionally, criminal behaviors occur in approximately 50% of cases [13]. A general lack of etiquette may be demonstrated by inappropriate laughing at a serious event, touching others, unbridled profanity, or making offensive jokes [2, 12].
Studies exploring the neuroanatomical correlates of disinhibition have largely implicated dysfunction of the right subgenual cingulate cortex (SGC) and the posteromedial aspect of the right OFC [14,15,16]. In addition to SGC and OFC involvement, Franceschi et al. also found that the bilateral inferior temporal cortex, hippocampus, amygdala, and nucleus accumbens were hypometabolic on fluorodeoxyglucose positron emission tomography (FDG-PET) in those with bvFTD who predominately exhibited disinhibition [15].
Sturm et al. found that atrophy of the right pregenual ACC in subjects with bvFTD was associated with a lower degree of self-conscious emotional reactivity [17], which suggests that this brain region may play a role in disinhibited behavior. In another study, Perry et al. found that the inability of participants to subjectively differentiate between pleasant and unpleasant odors was correlated with atrophy of the right ventral mid-insula and right amygdala, suggesting that the lack of aversion to negative stimuli may be a component of reward-seeking behavior seen in those with disinhibited behavior [8].
Pharmacological treatments targeting disinhibited behavior are limited, though some studies demonstrate that selective serotonin reuptake inhibitors (SSRI) may be effective. In a small open-label study by Swartz et al., 11 subjects with FTD were treated with fluoxetine, sertraline, or paroxetine for three months and were found to have a reduction in the degree of disinhibition [18]. In another open-label study by Herrmann et al., 15 subjects with FTD were treated with citalopram 30 mg daily for six weeks and were found to have significant decreases on the neuropsychiatric inventory (NPI) questionnaire total score and on the disinhibition subscore of the NPI [19].
Apathy
Apathy is the most common presenting symptom of bvFTD, occurring in 84% of cases at the time of the initial evaluation [2]. It is characterized by the reduction of goal-directed behavior, diminished emotional reactivity, and a decrease in social engagement [20]. Apathy initially manifests as a reduction of spontaneous activity and a general sense of indifference [20,21,22]. In later stages of the disease process, apathy may result in substantial functional impairment with limited ability to perform instrumental and basic activities of daily living (ADL) [23]. The functional impairment resulting from apathy is often very difficult for those caring for the patient and can lead to substantial emotional distress [24].
A diagnostic framework for the diagnosis of apathy was proposed by Marin in 1991 [21]. Marin described apathy as a distinct neuropsychiatric syndrome defined by a lack of motivation, a decrease in goal-directed behavior, and a loss of interest [21]. Despite Marin’s proposed diagnostic criteria describing the apathy syndrome, the concept of apathy has varied throughout the literature leading to confusion due to lack of a formal definition. Levy and Dubois defined apathy as a “quantitative reduction of voluntary, goal-directed behaviors” and defined three subtypes, emotional-affective, cognitive, and autoactivation. This definition was important for delineating three different behavioral syndromes associated with three different anatomical correlates [25]. A more recent set of diagnostic criteria describing the apathy syndrome has been proposed by a consensus panel of 23 experts (Table 2) in order to formally define the concept of apathy [20, 22].
The neuroanatomical correlates of apathy in those with bvFTD have been largely associated with dysfunction of the frontal lobes. Studies utilizing voxel-based morphometry (VBM) demonstrate predominately right-sided atrophy of the medial prefrontal cortex (mPFC) [14, 16, 26] and the ACC [14, 16, 26, 27]. Other areas of involvement include the dlPFC [16, 26], OFC [14, 16, 27], insula [26, 28], and the caudate [28].
Pharmacological treatments targeting apathy are limited. Psychostimulants may result in some improvement, though careful patient selection is essential due to the potential for significant side effects, including insomnia, hypertension, irritability, and psychosis. Methylphenidate has shown benefit in multiple small studies [29]. In several randomized controlled trials (RCT), methylphenidate was associated with significant improvement in apathy in those with AD [30, 31, 32]. One small RCT of eight patients diagnosed with bvFTD found that treatment with dextroamphetamine resulted in an improvement in neuropsychiatric inventory (NPI) subscales of apathy by 2.8 points [33]. Despite some improvement in symptoms, these small studies do not justify treating FTD with stimulants in most cases given the potential for significant adverse events.
Loss of Empathy or Sympathy
Loss of empathy is a presenting symptom in 73% of bvFTD cases [2]. Symptoms manifest as emotional detachment and a decrease in social interest, as well as a lack of concern for the feelings of others [2, 34]. This indifference can profoundly impact relationships early in the disease course and often results in substantial caregiver burden by disruption the emotional connection between the caregiver, often the patient's spouse, and the patient [35, 36]. In extreme cases, lack of empathy may manifest as sociopathic behavior [37]. When coupled with disinhibition and impulsivity commonly demonstrated by those with bvFTD, loss of empathy may lead to criminal behavior, ranging from petty theft to homicide [38].
Empathy is a complex construct in which an observer is able to identify with the feelings, thoughts, or emotions of another individual, leading to a change in the observer’s affective state [39]. The ability to empathize is a fundamental aspect of social interaction and involves affective perspective taking and affect sharing [39]. The affective perspective taking and affect sharing of empathy are broken down into cognitive components and affective components, each of which has multiple subcomponents that are beyond the scope of this chapter [40, 41]. The cognitive components of empathy involve the observer understanding what others may be thinking or feeling, while the affective components involve sharing and responding to the emotional experience of others [40]. This paradigm allows for a better understanding of the empathy deficits demonstrated in bvFTD.
The underlying neuroanatomy implicated in the loss of empathy is largely related to the widespread dysfunction of structures that are associated with both cognitive and affective empathy. A lesional study by Shamay-Tsoory et al. demonstrated that cognitive empathy and affective empathy were associated with distinct neuroanatomical substrates. Deficits in cognitive empathy were found to be associated with lesions of the right ventromedial PFC (vmPFC) , while deficits in affective empathy were found to be associated with lesions of the left inferior frontal gyrus (IFG) [42]. A by Dermody et al. in subjects with bvFTD correlated well with the earlier study by Shamay-Tsoory et al. Dermody et al. found that the diminished cognitive empathy in bvFTD was associated with predominately right-sided atrophy of the mPFC, OFC, insular cortices, and lateral temporal lobes. Diminished affective empathy was associated with predominately left-sided atrophy of the OFC, (IFG), insula, thalamus, putamen, and the bilateral mid-cingulate gyrus [43].
Pharmacological treatments targeting loss of empathy in bvFTD are limited, though studies evaluating the therapeutic effects of oxytocin have shown positive results. Hurlemann et al. assessed the effect of intranasal oxytocin in a randomized, double-blind, placebo-controlled trial of 48 healthy male volunteers and demonstrated that intranasal oxytocin enhanced emotional empathy but not cognitive empathy [44]. Subsequent randomized, double-blind, placebo-controlled trials regarding the effects of oxytocin were performed by Jesso et al. (n = 20) and Finger et al. (n = 46) in subjects with bvFTD. Both studies demonstrated significant improvement in measures of empathy [45, 46].
Perseverative, Stereotyped, or Compulsive/Ritualistic Behaviors
Repetitive behaviors occur in bvFTD at the time of initial evaluation in 71% of cases [2] and may be related to deficits in suppressing urges to perform an action [47]. These behaviors can present as simple repetitive movements or vocalizations, such as eye blinking, throat clearing, or tapping, among others. More complex behaviors are also frequently observed, including collecting and hoarding behavior, repetitive storytelling, and frequent unnecessary trips to the bathroom [2, 48, 49, 50].
Some of the repetitive behaviors seen in bvFTD have features related to deficits in impulse control. Compulsions, as typically seen in OCD, are characterized in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as purposeful repetitive motor acts that are associated with obsessive thoughts and performed to reduce anxiety or distress [51]. In those with OCD, performing the behavior results in relief from distress, though the action is not intrinsically pleasurable [52, 53]. In contrast to that seen in OCD, impulsivity typically seen in bvFTD is characterized by the inability to resist urges due to deficits in response inhibition and delayed gratification, as well as a lack of consideration for potential consequences. This leads to an act performed due to the need to immediately satisfy a desire rather than to alleviate anxiety or distress [54, 55]. In a study by Moheb et al., it was demonstrated that typical repetitive behaviors seen in bvFTD were complex and included stereotypic speech, hoarding, and frequent unnecessary trips to the restroom. In contrast, symptoms typical of OCD, such as checking, counting, and ordering, were infrequent. Furthermore, repetitive behaviors in bvFTD were not associated with anxiety, and were able to be stopped on command without causing distress [50].
In contrast to the study by Moheb et al., other studies have found that symptoms typical of OCD are prominent in bvFTD [47, 56, 57, 58].
The neuroanatomical correlates of repetitive behaviors in bvFTD are largely related to the dysfunction of structures in the left temporal lobe and striatum. A study by Rosso et al. performed computed tomography (CT) and/or MRI on 87 subjects and found that left temporal lobe atrophy was associated with complex compulsive behaviors, which included preoccupation with ideas or activities, strict adherence to a fixed schedule, frugality, arranging items in a particular order, and cleaning rituals [59]. Similarities were found in a functional imaging study using single-photon emission computed tomography (SPECT), which correlated hypoperfusion of the left temporal lobe with compulsive behavior, and hypoperfusion of the right frontal lobe with stereotypical behavior [60]. The role of the striatum in stereotypical behavior associated with bvFTD was further described in a study utilizing VBM by Josephs et al., who demonstrated disproportionate atrophy of the putamen and caudate head bilaterally [61]. Additionally, atrophy of the dorsal ACC and right supplementary motor area was found to be associated with repetitive behavior in a study by Rosen et al. [14]
The pharmacological treatments specifically targeting repetitive behaviors in those with bvFTD are limited, though some studies have demonstrated modest improvement in symptoms. In a small open-label study published by Swartz et al., previously described in this chapter, a reduction in compulsive behaviors was noted after treatment with an SSRI [18]. A case series of three patients reported improvement in compulsive behavior associated with bvFTD with the use of clomipramine [62]. A case report indicated that topiramate was effective in helping to reduce alcohol use in an individual with bvFTD [63]. Lastly, a small study by Mendez et al. found that those with FTD who were treated with donepezil were more likely to experience worsening of disinhibition and compulsive behavior, which returned to baseline after donepezil was discontinued [64].
Hyperorality and Dietary Changes
Hyperorality and dietary changes have long been recognized as a feature of neurodegenerative disease [65] and have been considered a core feature of bvFTD since the diagnostic criteria proposed in 1998 by Neary et al. [66]. Significant changes in eating behavior are present in 59% of those with bvFTD at the initial evaluation [2] and increase with the progression of disease [67]. A range of disordered eating behavior has been described, including increased appetite, excessive eating regardless of satiety, alterations in food preferences often with a preference for carbohydrates, and, in severe cases, oral exploration, chewing, or ingestion of inedible objects [2, 68, 69, 70]. The potential degree of insatiability that may be seen in those with bvFTD was clearly demonstrated in a study by Woolley et al., where participants were given sandwiches for lunch and allowed to eat as many as they wished for up to one hour. Sandwiches were continuously brought to the participants, regardless of their requests, in order to maintain a constant volume of sandwiches in front of the participant. Those with bvFTD were much more likely to eat more sandwiches than controls. In some cases, participants with bvFTD requested that sandwiches stop being brought to them, despite continuing to eat the sandwiches [70].
The underlying neuroanatomical correlates of eating behavior are likely multifactorial, though multiple studies have implicated orbitofrontal-insular-striatal networks as a mediator of eating behavior and satiety [70, 71, 72]. A study by Woolley et al. utilizing VBM demonstrated that atrophy of the right ventral insular cortex, striatum, and anterior OFC was associated with increased food consumption [70]. A similar study by Whitwell et al. demonstrated that increased food consumption was associated with atrophy of the anterolateral OFC bilaterally [71]. Whitwell et al. correlated the increase in carbohydrate craving associated with bvFTD with the right AI and the posterolateral OFC bilaterally [71]. There is also evidence that changes in the hypothalamus may lead to disturbance in eating behavior. In a study by Piguet et al., significant atrophy of the hypothalamus was present on structural MRI as well as on postmortem analyses in patients with bvFTD who demonstrated a significant disturbance in eating behavior [72].
Treatment modalities targeting hyperorality and dietary changes are limited, though there have been a small number of medications that have resulted in improvement. Serotonergic medications are the most widely studied in bvFTD. In a small open-label study performed by Swartz et al., previously described in this chapter, treatment with an SSRI resulted in a decrease in carbohydrate craving [18]. Additional studies found that fluvoxamine and trazodone were also effective at improving eating behaviors [73,74,75].
Given the limited number of available pharmacological treatment options, close caregiver supervision is often necessary in order to mitigate the potential for overeating, weight gain, and possible attempts to ingest inedible objects [11].
Overlapping Characteristics of bvFTD and Psychiatric Disorders
Neurodegenerative disorders, particularly bvFTD, and primary psychiatric disorders have many features in common, which presents a significant diagnostic challenge for clinicans. Recognizing these overlapping features is an essential first step in uncovering the etiology of the patient's presenting symptoms. A thorough evaluation, including an exhaustive history, neuroimaging, and neuropsychological testing, can aid in narrowing the differential diagnoses and may result in findings that would have otherwise be missed, such as severe executive dysfunction noted on neuropsychological testing or frontotemporal atrophy demonstrated on MRI of the brain. In this section, we will briefly discuss some of the similarities between bvFTD, MDD, and BPD.
Overlapping Symptomatology
Early symptoms of bvFTD can mimic those found in late-life primary mood disorders, and are often experienced by those with MDD and BPD [5].
Major depressive disorder is a common psychiatric disorder characterized by intermittent episodes of depressed mood with several clinical features with bvFTD, which can potentially congtribute to diagnostic uncertainty, particularly in complicated or atypical cases. The diagnostic criteria for MDD are defined in DSM-5 by nine characteristic features: (1) depressed mood, (2) diminished interest or pleasure in activities, (3) a significant change in weight or appetite, (4) insomnia or hypersomnia, (5) psychomotor agitation or retardation, (6) fatigue or loss of energy, (7) feelings of worthlessness or guilt, (8) diminished concentration, and (9) recurrent thoughts of death or suicide [51]. Anhedonia is often present in those with MDD, though it can appear very similar to that of apathy associated with bvFTD as both often present clinically as decreased motivation. In this case, other symptoms would likely aid in clarifying the underlying diagnosis, however, differentiating bvFTD and MDD can become increasingly difficult in those with atypical or severe cases of depression. In those with atypical depression, appetite is often signficantly increased and may appear similar to the increase in appetite commonly associated with bvFTD. Severe cases of depression may present as emotional disengagement and social withdrawal which can be mistaken for lack of empathy associated with bvFTD. [5, 76,77,79]. Despite the overlapping symptomatology between bvFTD and MDD, clinicians generally consider MDD much more prevalent than bvFTD [80, 81]. Clinician’s familiarity with similarities and differences between bvFTD and MDD, as well as a thorough evaluation, can improve diagnostic accuracy and help to avoid a delay in care.
Bipolar disorder is a psychiatric disorder characterized by intermittent episodes of mania and depression. The diagnostic criteria for BPD are defined in DSM-5 as a distinct period of abnormally and persistently elevated or irritable mood in addition to seven characteristic features: (1) inflated self-esteem or grandiosity, (2) decreased need for sleep, (3) more talkative than usual or pressure to keep talking, (4) flight of ideas or racing thoughts, (5) distractibility, (6) increased goal-directed activity or psychomotor agitation, and (7) excessive involvement in activities that have a high potential for negative consequences. As in MDD, the symptoms of BPD have a large overlap with those of bvFTD. One of the most salient features in both BPD and bvFTD is excessive impulsivity, however, in BPD it is predominantly associated with manic episodes, though this is not the case in bvFTD. Psychomotor agitation (i.e., engaging in purposeless movements) is another common feature of BPD that may be mistaken for repetitive movements which may be seen in bvFTD [5, 76,77,79].
Neuroimaging Correlates Between bvFTD and Psychiatric Disorders
Neuroimaging plays an important role in helping to distinguish bvFTD from a primary psychiatric disorder, but it has also been instrumental in helping to establish the underlying neuroanatomical correlates of psychiatric symptoms. In those with MDD and BPD, evidence suggests that structural changes in the brain impact regions involved in bvFTD [6, 82]. Two large meta-analyses examined gray matter abnormalities in MDD and BPD via VBM [82, 83]. Redlich et al. found that in subjects with MDD, there was a reduction in gray matter volume of the vmPFC, dorsomedial PFC (dmPFC), hippocampus, caudate, and precuneus. In subjects with BPD, there was a reduction in the dlPFC, insula, bilateral hippocampi, amygdala, caudate, thalamus, and putamen [84].
Lu et al. found that in subjects with MDD, there was a reduction of gray matter volume in the vmPFC, ACC, anterior superior temporal gyrus, left caudate, and left hippocampus when compared to healthy controls. In subjects with BPD, there was a reduction in the bilateral insula, superior temporal gyrus, mPFC, ACC, bilateral medial frontal gyrus, and the right medial and inferior temporal gyrus [83].
Regions of volume loss described in these meta-analyses have overlapped with regions involved with bvFTD, described elsewhere in this chapter. The overlapping brain regions of bvFTD, MDD, and BPD may explain the commonality between specific features of these conditions.
Conclusions
Behavioral variant FTD often presents predominately as a neuropsychiatric syndrome early in the disease course. The symptomology of bvFTD and underlying neuroanatomical correlates have overlap with those of primary psychiatric conditions. The commonalities between bvFTD in the early stages, and primary psychiatric conditions, may lead to a misdiagnosis of bvFTD. Clinicians should be aware of this pitfall and be diligent in the evaluation of patients who present with complaints that appear to be psychiatric in nature, especially those who present in late life.
Cases 1
Ms. BH is a right-handed woman with 16 years of education who was employed by the United States government. At baseline, BH was very involved with family and friends and enjoyed volunteering for local community organizations. In her mid-50s, BH began consuming an excessive amount of alcohol at a far greater extent than she had previously. Around this time, she began performing simple repetitive movements which manifested as constantly rubbing her hands together. More complex compulsive behaviors were also noted as she began collecting discarded aluminum cans and other items from the roadside. BH's hygiene progressive worsened and she began showering only once every two weeks.
One year after symptom onset, she was noted by her husband to be increasingly withdrawn socially and not meeting her obligations in the community organizations which she was involved. She became less interested in socializing with family and friends and was less engaged with her husband. On one notable occasion, after the death of a close friend, she did not reach out to her friend’s family or attend the funeral. BH stopped completing household chores and began spending most of her day on the sofa watching television. Additionally, she began exhibiting some degree of disinhibition as she began engaging strangers in conversation and disclosing personal details.
Neurological exam revealed difficulty with the Luria sequence, mild postural tremor, and global, symmetric hyperreflexia without clonus.
Neuropsychological testing revealed impairment in verbal and visual memory, visuospatial ability, confrontation naming, working memory, set switching, and response inhibition.
Laboratory studies and electroencephalogram were unremarkable.
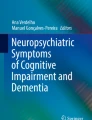
FDG-PET was notable for decreased glucose metabolism in the right anterior temporal lobe. Florbetapir [18F] PET was negative for amyloid aggregates. Structural MRI of the brain demonstrated disproportionate volume loss in the right frontotemporal region (Figs. 1 and 2).

Axial view in radiological orientation showing asymmetric atrophy of the right anterior temporal lobe (a) and the insular cortex (c). Other areas of degeneration include the bilateral orbitofrontal cortex with prominence of the orbital fissures bilaterally and the longitudinal cerebral fissure (b), the lateral prefrontal cortex (d), and the medial prefrontal cortex (e)

Coronal view (left and middle) and sagittal view (right) in radiological orientation showing significant areas of atrophy in the lateral prefrontal cortex (f), medial prefrontal cortex and anterior cingulate gyrus (g), right anterior temporal lobe (h), medial prefrontal cortex (i), subgenual cingulate gyrus (j), and orbitofrontal cortex (k)
Given BH’s symptoms of disinhibition, apathy, loss of empathy, repetitive/compulsive behavior, hyperorality, and executive dysfunction in addition to atrophy of the frontal and anterior temporal lobes, BH was ultimately diagnosed with bvFTD.
Case 2
Mr. KC is a right-handed man with 16 years of education who was employed as a photographer. In his early-50s, KC began experiencing difficulty performing tasks related to his job, and was noted to be repeatedly purchasing incorrect items for his camera. Additionally, the quality of KC's photography began to decline and he became increasingly rigid, often arguing with clients and insisting that his ideas were better.
Approximately 1 year after KC began to experience difficulty at work, he began to experience word-finding difficulty. His speech became increasingly generalized and non-specific, often referring to objects as a “thing” rather than the specific name of the object. Over the following year, KC experienced substantial progressive of word-finding difficulty. He began taking pictures of objects that he was unable to name and used the pictures to communicate. For example, he took pictures of multiple types of fruit and would send the pictures to his wife via text message in order to let her know that they needed more fruit from the store. Further progression of symptoms led to KC being unable to recall the meaning of words or conceptual knowledge making it difficult to use objects. For example, he was unable to identify what broccoli was or what to do with it. He also had been found performing activities inappropriately on mulitple occasions, such as washing his hands in the toilet rathger than the sink. In addition to language deficits, KC also exhibited memory impairment, visuospatial impairment, and behavioral changes, which included apathy and disinhibition. Notably, his cognition was impaired to the degree that he was unable to work and his wife had to help with most chores.
On neurological examination, KC did not engage in conversation unless directly questioned. He demonstrated echolalia and laughed inappropriately. He was perseverative and stimulus-bound, demonstrating utilization behaviors throughout the evaluation. His thought process was tangential, and he rarely answered questions directly. He could not describe his mood, however, his affect was borderline euphoric. He did not demonstrate appropriate concern or emotion given the nature of some of the topics of discussion. His speech was fluent and grammatically intact but generalized and vague. He was unable to name any items on a task of confrontational naming but was able to correctly describe the function of some of the words. He made semantic paraphasic errors. He was unable to read short, simple sentences. He was unable to write words or draw an animal when asked.
Neuropsychological testing revealed profound impairment in language, most notably impaired confrontation naming, impaired single-word comprehensionm impaired object knowledge. He was also noted to have impaired verbal and visual memory and executive functioning. Structural MRI demonstrated profound asymmetric left temporal atrophy (Fig. 3).

Axial (left) and sagittal (right) views in radiological orientation showing profound asymmetric left temporal lobe atrophy (a)
KC was ultimately diagnosed with semantic variant primary progressive aphasia (svPPA) based on the presence of impaired confrontation naming, impaired single word comprehension, impaired object knowledge, alexia, and agraphia. Additionally, MRI demonstrated left anterior temporal lobe atrophy consistent with svPPA.
Case 3
Ms. KA is a right-handed woman with 14 years of education who worked as an accountant. In her early-50s, KA began experiencing slowed speech and was noted to be omitting prepositions and conjunctions when communicating with her children via text message, though there were no spelling errors. The following year, KA began to have difficulty with grammar and using appropriate sentence structure predominantly when writing, resulting in shorter, more simple sentences. KA also began experiencing word-finding difficulty which impacted her ability to communicate.
Three years after the onset of symptoms, she began exhibiting halting, effortful speech. Reading and verbal comprehension was impaired, particularly to long, syntactically complex sentences. Writing was much more difficult than speaking, though she was still able to compose letters and emails with the help of her family.
Despite her language impairment, she remained fully independent and continued to work as an accountant without additional difficulty.
On neurological examination, KA was exhibited halting, effortful speech, with agrammatism and frequent phonological errors. When she spoke, her sentences were short and grammatically simplistic. Comprehension of syntactically complex sentences was impaired. Single-word comprehension and object knowledge were spared. She exhibits subtle nondominant limb apraxia and orobuccal apraxia.
On neuropsychological testing, she demonstrated severely impaired sentence repetition, diminished verbal agility, and agrammatism with relatively preserved naming, comprehension, and semantic knowledge. Additionally, she exhibited impaired lexical fluency, markedly impaired design fluency, executive dysfunction, and mild visual memory deficits.
Ms. KA was ultimately diagnosed with nonfluent variant primary progressive aphasia (nfvPPA) on the basis of her effortful, halting speech with agrammatism, spared single-word comprehension and object knowledge, and neuroimaging demonstrating predominant left fronto-insular atrophy (Fig. 4).

Axial structural MRI (left) view in radiological orientation showing asymmetric left insular cortex (a) and left operculum (b) atrophy. Voxel-based morphometry* (VBM) (right) showing the greatest degree of atrophy in the left insular/opercular region (c). *Map of this patient’s brain volume compared to 534 healthy older controls (age range 44–99 y.o., M ± SD: 68.7 ± 9.1; 220 male/302 female) from the UCSF MAC Hillblom Cohort, adjusted for age, sex, total intracranial volume, and magnet strength. W-scores are interpreted like z-scores, with mean = 0/standard deviation = 1. Negative W-scores represent below-average volume. <−1.50 are below 7th %ile compared to healthy controls and might be considered clinically abnormal. VBM analyses were performed using the open-source Brainsight system, developed at the University of California, San Francisco, Memory and Aging Center by Katherine P. Rankin, Cosmo Mielke, and Paul Sukhanov, and powered by the VLSM script written by Stephen M. Wilson, with funding from the Rainwater Charitable Foundation and the UCSF Chancellor’s Fund for Precision Medicine
References
Rabinovici GD, Miller BL (2010) Frontotemporal lobar degeneration. CNS Drugs 24(5):375–398
Rascovsky K, Hodges JR, Knopman D et al (2011) Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 134(9):2456–2477
Gorno-Tempini ML, Hillis AE, Weintraub S et al (2011) Classification of primary progressive aphasia and its variants. Neurology 76(11):1006–1014
Johnson JK, Diehl J, Mendez MF et al (2005) Frontotemporal lobar degeneration: demographic characteristics of 353 patients. Arch Neurol 62(6):925–930
Woolley JD, Khan BK, Murthy NK et al (2011) The diagnostic challenge of psychiatric symptoms in neurodegenerative disease: rates of and risk factors for prior psychiatric diagnosis in patients with early neurodegenerative disease. J Clin Psychiatry 72(2):126–133
Seeley WW, Crawford R, Rascovsky K et al (2008) Frontal paralimbic network atrophy in very mild behavioral variant frontotemporal dementia. Arch Neurol 65(2):249–255
Eckart JA, Sturm VE, Miller BL et al (2012) Diminished disgust reactivity in behavioral variant frontotemporal dementia. Neuropsychologia 50(5):786–790
Perry DC, Datta S, Sturm VE et al (2017) Reward deficits in behavioural variant frontotemporal dementia include insensitivity to negative stimuli. Brain J Neurol 140(12):3346–3356
Le Ber I, Guedj E, Gabelle A et al (2006) Demographic, neurological and behavioural characteristics and brain perfusion SPECT in frontal variant of frontotemporal dementia. Brain J Neurol 129(Pt 11):3051–3065
Lanata SC, Miller BL (2016) The behavioural variant frontotemporal dementia (bvFTD) syndrome in psychiatry. J Neurol Neurosurg Psychiatry 87(5):501–511
Manoochehri M, Huey ED (2012) Diagnosis and management of behavioral issues in frontotemporal dementia. Curr Neurol Neurosci Rep 12(5):528–536
Miller B, Llibre Guerra JJ (2019) Frontotemporal dementia. Handb Clin Neurol 165:33–45
Diehl-Schmid J, Perneczky R, Koch J et al (2013) Guilty by suspicion? Criminal behavior in frontotemporal lobar degeneration. Cogn Behav Neurol Off J Soc Behav Cogn Neurol 26(2):73–77
Rosen HJ, Allison SC, Schauer GF et al (2005) Neuroanatomical correlates of behavioural disorders in dementia. Brain J Neurol 128(11):2612–2625
Franceschi M, Anchisi D, Pelati O et al (2005) Glucose metabolism and serotonin receptors in the frontotemporal lobe degeneration. Ann Neurol 57(2):216–225
Massimo L, Powers C, Moore P et al (2009) Neuroanatomy of apathy and disinhibition in frontotemporal lobar degeneration. Dement Geriatr Cogn Disord 27(1):96–104
Sturm VE, Sollberger M, Seeley WW et al (2013) Role of right pregenual anterior cingulate cortex in self-conscious emotional reactivity. Soc Cogn Affect Neurosci 8(4):468–474
Swartz JR, Miller BL, Lesser IM et al (1997) Frontotemporal dementia: treatment response to serotonin selective reuptake inhibitors. J Clin Psychiatry 58(5):212–216
Herrmann N, Black SE, Chow T et al (2012) Serotonergic function and treatment of behavioral and psychological symptoms of frontotemporal dementia. Am J Geriatr Psychiatry Off J Am Assoc Geriatr Psychiatry 20(9):789–797
Robert P, Lanctôt KL, Agüera-Ortiz L et al (2018) Is it time to revise the diagnostic criteria for apathy in brain disorders? The 2018 international consensus group. Eur Psychiatr 54:71–76
Marin RS (1991) Apathy: a neuropsychiatric syndrome. J Neuropsychiatry Clin Neurosci 3(3):243–254
Robert P, Onyike CU, Leentjens AFG et al (2009) Proposed diagnostic criteria for apathy in Alzheimer’s disease and other neuropsychiatric disorders. Eur Psychiatry 24(2):98–104
Clarke DE, Ko JY, Lyketsos C et al (2010) Apathy and cognitive and functional decline in community-dwelling older adults: results from the Baltimore ECA longitudinal study. Int Psychogeriatr 22(5):819–829
Merrilees J, Dowling GA, Hubbard E et al (2013) Characterization of apathy in persons with frontotemporal dementia and the impact on family caregivers. Alzheimer Dis Assoc Disord 27(1):62–67
Levy R, Dubois B (2006) Apathy and the functional anatomy of the prefrontal cortex-basal ganglia circuits. Cereb Cortex 16(7):916–928
Sheelakumari R, Bineesh C, Varghese T et al (2019) Neuroanatomical correlates of apathy and disinhibition in behavioural variant frontotemporal dementia. Brain Imaging Behav.
Zamboni G, Huey ED, Krueger F et al (2008) Apathy and disinhibition in frontotemporal dementia: insights into their neural correlates. Neurology 71(10):736–742
Eslinger PJ, Moore P, Antani S et al (2012) Apathy in frontotemporal dementia: behavioral and neuroimaging correlates. Behav Neurol 25(2):127–136
Dolder CR, Nicole Davis L, McKinsey J (2010) Use of psychostimulants in patients with dementia. Ann Pharmacother 44(10):1624–1632
Rosenberg PB, Lanctôt KL, Drye LT et al (2013) Safety and efficacy of methylphenidate for apathy in Alzheimer’s disease: a randomized, placebo-controlled trial. J Clin Psychiatry 74(8):810–816
Padala PR, Padala KP, Lensing SY et al (2018) Methylphenidate for apathy in community-dwelling older veterans with mild Alzheimer’s disease: a double-blind, randomized, placebo-controlled trial. Am J Psychiatry 175(2):159–168
Scherer RW, Drye L, Mintzer J et al (2018) The apathy in dementia methylphenidate trial 2 (ADMET 2): study protocol for a randomized controlled trial. Trials 19(1):46
Huey ED, Garcia C, Wassermann EM et al (2008) Stimulant treatment of frontotemporal dementia in 8 patients. J Clin Psychiatry 69(12):1981–1982
Carr AR, Mendez MF (2018) Affective empathy in behavioral variant frontotemporal dementia: a meta-analysis. Front Neurol 9
Hsieh S, Irish M, Daveson N et al (2013) When one loses empathy: its effect on carers of patients with dementia. J Geriatr Psychiatry Neurol 26(3):174–184
Pomponi M, Ricciardi L, La Torre G et al (2016) Patient’s loss of empathy is associated with caregiver burden. J Nerv Ment Dis 204(9):717–722
Mendez MF (2010) The unique predisposition to criminal violations in frontotemporal dementia. J Am Acad Psychiatry Law 38(3):318–323
Liljegren M, Naasan G, Temlett J et al (2015) Criminal behavior in frontotemporal dementia and Alzheimer disease. JAMA Neurol 72(3):295–300
Singer T, Lamm C (2009) The social neuroscience of empathy. Ann N Y Acad Sci 1156(1):81–96
Rankin KP, Kramer JH, Miller BL (2005) Patterns of cognitive and emotional empathy in frontotemporal lobar degeneration. Cogn Behav Neurol 18(1):28–36
Baez S, Manes F, Huepe D et al (2014) Primary empathy deficits in frontotemporal dementia. Front Aging Neurosci 6:262
Shamay-Tsoory SG, Aharon-Peretz J, Perry D (2009) Two systems for empathy: a double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain 132(3):617–627
Dermody N, Wong S, Ahmed R et al (2016) Uncovering the neural bases of cognitive and affective empathy deficits in Alzheimer’s disease and the behavioral-variant of frontotemporal dementia. J Alzheimers Dis 53(3):801–816
Hurlemann R, Patin A, Onur OA et al (2010) Oxytocin enhances amygdala-dependent, socially reinforced learning and emotional empathy in humans. J Neurosci 30(14):4999–5007
Jesso S, Morlog D, Ross S et al (2011) The effects of oxytocin on social cognition and behaviour in frontotemporal dementia. Brain J Neurol 134(Pt 9):2493–2501
Finger EC, MacKinley J, Blair M et al (2015) Oxytocin for frontotemporal dementia: a randomized dose-finding study of safety and tolerability. Neurology 84(2):174–181
Mendez MF, Perryman KM, Miller BL et al (1997) Compulsive behaviors as presenting symptoms of frontotemporal dementia. J Geriatr Psychiatry Neurol 10(4):154–157
Olney NT, Spina S, Miller BL (2017) Frontotemporal Dementia. Neurol Clin 35(2):339–374
Mateen FJ, Josephs KA (2009) The clinical spectrum of stereotypies in frontotemporal lobar degeneration. Mov Disord: Off J Mov Disord Soc 24(8):1237–1240
Moheb N, Charuworn K, Ashla MM et al (2019) Repetitive behaviors in frontotemporal dementia: compulsions or impulsions? J Neuropsychiatry Clin Neurosci 31(2):132–136
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Association
Stein DJ (2002) Obsessive-compulsive disorder. Lancet 360(9330):397–405
Veale D, Roberts A (2014) Obsessive-compulsive disorder. BMJ 348
Robbins T, Curran H, de Wit H (2012) Special issue on impulsivity and compulsivity. Psychopharmacology 219(2):251–252
Berlin GS, Hollander E (2014) Compulsivity, impulsivity, and the DSM-5 process. CNS Spectr 19(1):62–68
Ames D, Cummings JL, Wirshing WC et al (1994) Repetitive and compulsive behavior in frontal lobe degenerations. J Neuropsychiatry Clin Neurosci 6(2):100–113
Perry DC, Whitwell JL, Boeve BF et al (2012) Voxel-based morphometry in patients with obsessive-compulsive behaviors in behavioral variant frontotemporal dementia. Eur J Neurol 19(6):911–917
Mitchell E, Tavares TP, Palaniyappan L et al (2019) Hoarding and obsessive-compulsive behaviours in frontotemporal dementia: clinical and neuroanatomic associations. Cortex 121:443–453
Rosso SM, Roks G, Stevens M et al (2001) Complex compulsive behaviour in the temporal variant of frontotemporal dementia. J Neurol 248(11):965–970
McMurtray AM, Chen AK, Shapira JS et al (2006) Variations in regional SPECT hypoperfusion and clinical features in frontotemporal dementia. Neurology 66(4):517–522
Josephs KA, Whitwell JL, Jack CR (2008) Anatomic correlates of stereotypies in frontotemporal lobar degeneration. Neurobiol Aging 29(12):1859–1863
Furlan JC, Henri-Bhargava A, Freedman M (2014) Clomipramine in the treatment of compulsive behavior in frontotemporal dementia: a case series. Alzheimer Dis Assoc Disord 28(1):95–98
Cruz M, Marinho V, Fontenelle LF et al (2008) Topiramate may modulate alcohol abuse but not other compulsive behaviors in frontotemporal dementia: case report. Cogn Behav Neurol 21(2):104–106
Mendez MF, Shapira JS, McMurtray A et al (2007) Preliminary findings: behavioral worsening on donepezil in patients with frontotemporal dementia. Am J Geriatr Psychiatry 15(1):84–87
Sourander P, Sjögren H (2008) The concept of Alzheimer’s disease and its clinical implications. In: Ciba foundation symposium – Alzheimer’s disease and related conditions. Wiley, p 11–36
Neary D, Snowden JS, Gustafson L et al (1998) Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology 51(6):1546–1554
Piguet O, Hornberger M, Shelley BP et al (2009) Sensitivity of current criteria for the diagnosis of behavioral variant frontotemporal dementia. Neurology 72(8):732–737
Miller BL, Darby AL, Swartz JR et al (1995) Dietary changes, compulsions and sexual behavior in frontotemporal degeneration. Dementia 6(4):195–199
Mendez MF, Licht EA, Shapira JS (2008) Changes in dietary or eating behavior in frontotemporal dementia versus Alzheimer’s disease. Am J Alzheimers Dis Other Demen 23(3):280–285
Woolley JD, Gorno-Tempini M-L, Seeley WW et al (2007) Binge eating is associated with right orbitofrontal-insular-striatal atrophy in frontotemporal dementia. Neurology 69(14):1424–1433
Whitwell JL, Sampson EL, Loy CT et al (2007) VBM signatures of abnormal eating behaviours in frontotemporal lobar degeneration. NeuroImage 35(1):207–213
Yi DS, Bertoux M, Mioshi E et al (2013) Fronto-striatal atrophy correlates of neuropsychiatric dysfunction in frontotemporal dementia (FTD) and Alzheimer’s disease (AD). Dement Neuropsychol 7(1):75–82
Piguet O, Petersén Å, Yin Ka Lam B et al (2011) Eating and hypothalamus changes in behavioral-variant frontotemporal dementia. Ann Neurol 69(2):312–319
Ikeda M, Shigenobu K, Fukuhara R et al (2004) Efficacy of fluvoxamine as a treatment for behavioral symptoms in frontotemporal lobar degeneration patients. Dement Geriatr Cogn Disord 17(3):117–121
Lebert F, Stekke W, Hasenbroekx C et al (2004) Frontotemporal dementia: a randomised, controlled trial with trazodone. Dement Geriatr Cogn Disord 17(4):355–359
Block NR, Sha SJ, Karydas AM et al (2016) Frontotemporal dementia and psychiatric illness: emerging clinical and biological links in gene carriers. Am J Geriatr Psychiatry 24(2):107–116
Banks SJ, Weintraub S (2008) Neuropsychiatric symptoms in behavioral variant frontotemporal dementia and primary progressive aphasia. J Geriatr Psychiatry Neurol 21(2):133–141
Gossink F, Vijverberg E, Pijnenburg Y et al (2018) Neuropsychiatry in clinical practice: the challenge of diagnosing behavioral variant frontotemporal dementia. J Neuropsychiatry 02(01)
Gossink FT, Dols A, Kerssens CJ et al (2016) Psychiatric diagnoses underlying the phenocopy syndrome of behavioural variant frontotemporal dementia. J Neurol Neurosurg Psychiatry 87(1):64–68
Hasin DS, Sarvet AL, Meyers JL et al (2018) Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiat 75(4):336–346
Knopman DS, Roberts RO (2011) Estimating the number of persons with frontotemporal lobar degeneration in the US population. J Mol Neurosci 45(3):330–335
Charney DS, Sklar PB, Buxbaum JD et al (2018) Charney & Nestler’s neurobiology of mental illness. Oxford University Press, New York
Lu X, Zhong Y, Ma Z et al (2019) Structural imaging biomarkers for bipolar disorder: meta-analyses of whole-brain voxel-based morphometry studies. Depress Anxiety 36(4):353–364
Redlich R, Almeida JJR, Grotegerd D et al (2014) Brain morphometric biomarkers distinguishing unipolar and bipolar depression. A voxel-based morphometry-pattern classification approach. JAMA Psychiat 71(11):1222–1230
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Peet, B.T., Castro-Suarez, S., Miller, B.L. (2021). The Neuropsychiatric Features of Behavioral Variant Frontotemporal Dementia. In: Ghetti, B., Buratti, E., Boeve, B., Rademakers, R. (eds) Frontotemporal Dementias . Advances in Experimental Medicine and Biology, vol 1281. Springer, Cham. https://doi.org/10.1007/978-3-030-51140-1_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-51140-1_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-51139-5
Online ISBN: 978-3-030-51140-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)