
Abstract
The anterior segment of the eye describes the space bordered by the cornea anteriorly and the iris and lens posteriorly. This chapter reviews manifestations of trauma to the anterior segment, with a focus on diagnostic and management strategies for the pediatric patient. The chapter highlights subconjunctival hemorrhage, hyphema, traumatic iritis, iris sphincter tear, iridodialysis, cyclodialysis, traumatic cataract, and lens subluxation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Subconjunctival hemorrhage
- Hyphema
- Traumatic iritis
- Iris sphincter tear
- Iridodialysis
- Cyclodialysis
- Traumatic cataract
- Ectopia lentis
- Lens subluxation
1 Introduction
The anterior chamber of the eye is the aqueous humor-filled space bordered by the cornea anteriorly and the iris and lens posteriorly. The iridocorneal angle created by the intersection of the iris root and the peripheral cornea is an important anatomical landmark which houses the ciliary body, scleral spur, Schlemm’s canal, and the trabecular meshwork. These structures are responsible for the production and drainage of aqueous humor and for controlling the size of the pupillary aperture.
The crystalline lens lies directly posterior to the pupillary diaphragm. It is held in place by suspensory ligaments called zonules of Zinn , which extend from the ciliary body to the lens. The normal lens is a transparent structure responsible for maintaining its own clarity, refracting light, and providing accommodation.
Slit lamp biomicroscopy is used to directly visualize the anterior chamber, while a mirrored lens called a gonioscope must be placed directly on the cornea to view the internal angle structures. Gonioscopy may be difficult to perform on a child, as the examination can be uncomfortable and requires stable positioning at the slit lamp. Other imaging modalities such as ultrasound biomicroscopy (UBM) and anterior segment ocular coherence tomography (AS-OCT) are non-contact methods of visualizing the anterior chamber and angle and may be better tolerated in children.
While trauma to the anterior chamber can occur in isolation after blunt trauma to the eye, it often occurs in conjunction with injury to adjacent ocular tissues such as the cornea or retina. A complete ophthalmologic examination of the anterior and posterior segment is essential for all children presenting with eye trauma. B-scan ultrasonography is often necessary as the view to the fundus may be obscured by blood, inflammation, or another anterior segment pathology. MRI or CT should be obtained if there is a concern for open globe or orbital injury. Examination under anesthesia may be required if a complete ophthalmologic exam is unable to be performed in an uncooperative child.
1.1 Subconjunctival Hemorrhage
Introduction
Subconjunctival hemorrhage (SCH) is an accumulation of blood in the subconjunctival space due to bleeding from a conjunctival or episcleral blood vessel. In young patients, trauma followed by contact lens wear is the most common causes of SCH [1]. The differential diagnosis for SCH in a child without a history of trauma is extensive and is outlined in ◘ Table 8.1. Non-accidental trauma is a rare but important cause of SCH that should be considered in the absence of other etiologies.
Clinical Presentation and Diagnosis
Children with SCH typically present to the emergency room after trauma to the eye or, in cases of spontaneous subconjunctival hemorrhage, are brought in by their parents who notice the striking red spot of blood. Because SCH often accompanies trauma to other ocular structures, presenting symptoms can be variable; however, when SCH occurs in isolation, it is asymptomatic.
The diagnosis of SCH is made on physical examination alone, which reveals a flat, sharply circumscribed, localized collection of blood in the subconjunctival space (◘ Fig. 8.1). It is typically described as involving a certain number of degrees of the conjunctiva (0–360). A complete anterior and posterior segment examination is important to rule out any coexisting injury. Three hundred sixty degrees of SCH is suspicious for globe rupture and may warrant surgical exploration.

Clinical photograph of nasal subconjunctival hemorrhage
Management
Though the appearance of SCH may be alarming, patients must be reassured that SCH alone will resolve spontaneously and does not require treatment. Blood degradation and absorption will cause the red color of SCH to evolve into orange or yellow before complete absorption usually occurring between 1 and 2 weeks from onset [2].
1.2 Hyphema
Introduction
A hyphema is the presence of blood within the anterior chamber of the eye. It most commonly occurs after blunt or penetrating trauma, with the presumed source of bleeding from tears in the anterior ciliary body and iris blood vessels [3]. Traumatic hyphema occurs at a rate of 17 per 100,000 per year with 70–75% of patients being children [4]. The majority of cases occur during sports, but other important causes include airbag, paintball, and nerf gun injuries [5,6,7].
Non-traumatic causes of hyphema are uncommon in children but include intraocular surgery, iris neovascularization, anterior chamber tumors, myotonic dystrophy, keratouveitis, leukemia, and bleeding disorders [8, 9]. A spontaneous hyphema from vascularized iris nodules is the most common presenting symptom of juvenile xanthogranuloma (JXG), a benign dermatologic disorder affecting infants and young children. Patients also present with a single (or rarely multiple) asymptomatic yellow and brown skin nodule. The nodules in JXG are benign and are the result of histiocyte proliferation [10].
As in the case of subconjunctival hemorrhage, a hyphema in the absence of known trauma or predisposing ocular or systemic disease should raise suspicion for non-accidental injury.
Clinical Presentation and Diagnosis
Children with hyphema typically present after eye trauma with pain, photophobia, and decreased vision. The hyphema may be visualized via penlight or slit lamp examination as a layering of blood within the anterior chamber (◘ Fig. 8.2) and can be graded as the percent of space it occupies (◘ Table 8.2). A microhyphema refers to the presence of red blood cells suspended in the anterior chamber, and an 8-ball hyphema describes an anterior chamber that is completely filled with dark-clotted blood.

Clinical photograph showing hyphema
A complete ophthalmologic examination must be performed, as hyphema can signify severe ocular injury and damage to adjacent tissues. Dilated fundus exam should be attempted to evaluate concomitant posterior segment trauma, but B-scan ultrasound may be necessary as blood may obscure the view to the fundus. CT scan or MRI of the orbits may also be indicated if there is suspicion for globe rupture. Sickle cell prep and, if indicated, hemoglobin electrophoresis should be ordered, as the presence of sickle cell hemoglobinopathy will change management and prognosis. Laboratory workup including complete blood count, prothrombin time, partial thromboplastin time, liver function tests, and bleeding time should be considered in patients with bleeding disorders.
Complications of Hyphema
Because of the complications that can be associated with hyphema, close follow-up is recommended until resolution of the layered clot. A secondary hemorrhage, or rebleed, can occur between 2 and 5 days of the initial trauma, and so daily follow-up is often recommended during this time. A rebleed carries a poor prognosis as it has been associated with increased intraocular pressure, corneal bloodstaining, and amblyopia. Rebleeds are more common in African American patients and patients with sickle cell disease [11].
Elevated Intraocular Pressure and Optic Atrophy
Elevations in intraocular pressure (IOP) can occur from hyphemas of any size, and so IOP should be checked and closely monitored. The iCare tonometer (Tiolat Oy, Helsinki, Finland) is a newer, non-contact method of measuring intraocular pressure which is useful in the pediatric population. Elevated intraocular pressure (>22 mm hg) can lead to glaucoma or optic atrophy resulting in permanent vision loss. Particular attention must be given to the sickle cell patient with hyphema as sickled red blood cells can clog the trabecular meshwork leading to persistently elevated intraocular pressure in eyes that are more prone to optic atrophy. Lower thresholds for surgical intervention exist for these patients.
Corneal Bloodstaining
Corneal bloodstaining occurs when hemoglobin and hemosiderin deposit into the corneal stroma typically due to severe and prolonged hyphema. The incidence is 5% of patients with hyphema, with risk factors including compromised corneal endothelium, large hyphemas, elevated intraocular pressure, and rebleed [4]. The pigment deposition results in a straw-yellow opacification of the cornea and subsequent vision loss. Corneal bloodstaining may take several months to 2 years to clear, which in children is problematic due to the risk of amblyopia. A corneal transplant may be indicated depending on the severity and duration of vision loss and the age of the child.
Posterior Synechiae and Peripheral Anterior Synechiae
Prolonged inflammation and clot organization may produce both posterior synechiae (adhesions between the iris and lens) and peripheral anterior synechiae (adhesions between the iris and the trabecular meshwork). Both conditions can result in angle-closure glaucoma and vision loss if left untreated.
Amblyopia
Visual deprivation due to the hyphema itself or from corneal bloodstaining obstructing the visual axis may lead to amblyopia. Though eye shields in adults with hyphema are often utilized to prevent additional trauma leading to rebleed, eye shields are avoided in children in order to reduce the risk of amblyopia [8]. The risk of traumatic hyphema-induced amblyopia may be overstated, however. In a study of 316 children with traumatic hyphema, only two patients developed amblyopia, and those two patients had concurrent traumatic cataracts [12].
Management
All patients with hyphema are instructed to refrain from physical activity to prevent secondary hemorrhage and to elevate the head to promote gravitational layering and clot formation. Admission to the hospital should be considered if it seems unlikely that the child and/or caregivers will be able to follow the recommendations.
Most cases of traumatic hyphema respond well to medical management. Topical cycloplegics are prescribed for symptom relief and for the prevention of posterior synechiae. Topical steroids are routinely used to decrease inflammation and prevent subsequent peripheral anterior synechiae formation. Topical steroids carry their own risks however, namely, glaucoma and cataract formation, and so should be used cautiously in children. In a Cochrane meta-analysis comparing topical steroid use to controls, no significant difference was seen in time to resolution of primary hemorrhage, risk of secondary hemorrhage, or risk of elevated intraocular pressure; however they are used routinely in cases of hyphema to control inflammation and prevent synechiae [13]. Antifibrinolytics have been shown to decrease the rate of secondary rebleed, but they may delay clot resorption [8].
Aggressive treatment of elevated IOP is necessary to prevent corneal bloodstaining, optic atrophy, and glaucoma. Topical beta blockers are the first-line treatment of elevated IOP in children. An alternative or adjunctive option is a topical carbonic anhydrase inhibitor. Adrenergic agonists such as brimonidine are contraindicated in children due to the risk of central nervous system depression [14]. Systemic carbonic anhydrase inhibitors are used when topical medications fail to control the intraocular pressure.
Surgical evacuation of the hyphema or anterior chamber washout should be considered in the setting of non-resolving hyphema, persistently elevated IOP unresponsive to medical therapy, or visual deprivation in children who are at risk for amblyopia. In patients with sickle cell disease or trait, there should be a low threshold for surgical evacuation because of the increased risk of optic atrophy.
1.3 Traumatic Iritis
Introduction
Traumatic iritis, or traumatic acute anterior uveitis, refers to inflammation of the iris and/or ciliary body following ocular trauma. It is the most common cause of uveitis in children accounting for up to 25% of childhood uveitis diagnoses [15]. Traumatic iritis is thought to be caused by the inflammatory response to cell injury and necrosis following trauma. Inflammatory mediators are released after injury, resulting in vasodilation, increased vascular permeability, and chemotaxis of inflammatory cells.
Clinical Presentation and Diagnosis
Patients with traumatic iritis typically present 24–48 hours after traumatic eye injury complaining of photophobia, tearing, and blurry vision. Inflammatory cells and aqueous flare in the anterior chamber are visible on slit lamp examination. Irritation of the iris and ciliary body can cause spasm of accommodation and often results in a poorly dilating pupil. Intraocular pressure may initially be low due to transient shutdown of the ciliary body but may later rise secondary to trabecular meshwork swelling and obstruction by inflammatory debris [16].
Management
Traumatic iritis is a self-limited process and will resolve on its own in 7–14 days; however, most patients are treated with topical cycloplegics and topical steroids for patient comfort and to prevent the formation of posterior synechiae and peripheral anterior synechiae. With the resolution of iritis, cycloplegics can be discontinued and steroids tapered to prevent rebound inflammation.
1.4 Iris Trauma: Sphincter Tear
Introduction
Blunt trauma to the eye can cause tears in the iris sphincter muscle, resulting in pupillary abnormalities. Compressive forces generate horizontal stretching within the pupillary aperture in opposition to the resistance provided by the lens, resulting in disruption of the marginal sphincter fibers [17].
Clinical Presentation and Diagnosis
Patients with iris sphincter tears commonly present after blunt trauma to the eye. Symptoms are dependent on the extent and severity of associated injuries but can include pain, photophobia, and blurry vision. Iris sphincter tears can be seen on slit lamp examination as scalloped notches in the iris sphincter at the pupillary margin. Depending on the extent of tearing, the pupil may appear irregular or dilated and may be minimally reactive to light. Evaluation requires careful slit lamp examination as hyphema and traumatic iritis often occur in conjunction with iris sphincter tears. In cases where the pupil appears dilated, it is important to rule out a third nerve palsy, which can present with mydriasis, ptosis, and extraocular muscle abnormalities on the affected side. Neuroimaging is indicated if third nerve palsy is suspected.
Management
Topical corticosteroids and cycloplegics are used to treat accompanying iritis and/or hyphema. If pupillary function does not return after a period of observation, patients may report persistent debilitating glare, photophobia, and monocular diplopia. Prosthetic contact lenses employ the pinhole effect to alleviate these symptoms [18]. Surgical pupilloplasty may be considered in cases of multiple or large tears [19].
1.5 Iris Trauma: Iridodialysis
Introduction
Iridodialysis is the separation of the iris root from the ciliary body. The iris root is the thinnest portion of the iris stroma, leaving it particularly vulnerable to damage [20]. Blunt or penetrating trauma is the most common cause of iridodialysis in all age groups. Airsoft toy guns, bottle rockets, and water balloon slingshots are important causes of iridodialysis in the pediatric population [5, 21, 22].
Clinical Presentation and Diagnosis
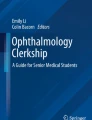
Symptoms of iridodialysis depend on its size and associated inflammatory response. Small dialyses may be asymptomatic, while larger dialyses may cause monocular diplopia, glare, and photophobia. The disinserted iris root appears on slit lamp examination as polycoria, or the presence of an additional “D-shaped” pupil (◘ Fig. 8.3). Accompanying hyphema and/or traumatic iritis are common findings.

Clinical photograph showing irregular D-shaped pupil, clinically significant for iridodialysis. (Reprinted with permission from the American Academy of Ophthalmology. © 2019 American Academy of Ophthalmology)
Management
Topical corticosteroids and cycloplegics may be given to treat the accompanying traumatic iritis and/or hyphema. Small asymptomatic iridodialyses require no further intervention, but a larger or symptomatic iridodialysis presents both functional and cosmetic concerns . Treatment is either a prosthetic contact lens or surgical repair of the iridodialysis [23, 24].
1.6 Iris Trauma: Cyclodialysis
Introduction
Cyclodialysis describes a separation of the longitudinal fibers of the ciliary muscle from the scleral spur. This separation, or cleft, provides a pathway for aqueous humor to drain into the suprachoroidal space and results in ocular hypotony (IOP lower than or equal to 5 mmHg). The primary cause of cyclodialysis in all age groups is blunt trauma [25]. Less frequently, cyclodialysis may be iatrogenic from surgical iris manipulation. Aminlari described a 4.5-month-old girl who had cyclodialysis following trabeculotomy for congenital glaucoma [26].
Clinical Presentation and Diagnosis
All patients with cyclodialysis will present with a very low IOP often less than 5 mmHg. In a case review of 32 eyes with cyclodialysis, mean presenting IOP was 3.2 mm Hg [27]. Clinical studies repeatedly demonstrate that the size of the cyclodialysis cleft does not correlate with the degree of hypotony [26, 27]. Patient’s history should correlate with clinical findings, for example, report of recent blunt injury or ocular surgery. Concurrent clinical evidence of severe ocular trauma, such as iris sphincter tears or hyphema, can also aid in the diagnosis. Complications of severe ocular hypotony may be observed on initial clinical presentation, including shallow anterior chamber, cataract, optic disc edema, macular edema, choroidal effusion, and retinal or choroidal folds [25, 26, 28].
Gonioscopy is the primary method to confirm the diagnosis of cyclodialysis, but it has several limitations. Gonioscopy is difficult to perform on a child, and it is especially difficult on a hypotonous eye with a shallow anterior chamber. Ultrasound biomicroscopy and anterior segment OCT are noninvasive imaging modalities that minimize patient discomfort because they do not require direct contact with the eye. Both AS-OCT and UBM are easy to repeat in order to monitor response to treatment [27, 29].
Management
The size of the cyclodialysis guides treatment. For small clefts (<4 clock hours), treatment should begin conservatively with medical management consisting of 1% atropine, one to two times daily for a period of 6 to 8 weeks. It is hypothesized that by relaxing the ciliary muscle with atropine, the detached muscle fibers are brought closer to the sclera to permit cleft closure [30]. Topical corticosteroids should be limited because they can delay healing of the cleft.
Noninvasive methods of closure such as laser photocoagulation [31], transscleral diathermy [32], or transconjunctival cryotherapy [33] can be considered for moderate sized clefts. Surgical approaches are reserved for larger clefts, or if noninvasive methods have failed [34, 35]. Overall, the prognosis of cyclodialysis is favorable. Good visual outcomes have been reported following cyclodialysis closure regardless of cleft size or time until receiving treatment [26, 36].
1.7 Traumatic Cataract
Introduction
Cataract , or opacification of the crystalline lens, is a major preventable cause of blindness in children worldwide. While a cataract in an adult can be successfully managed at any point after its development, delayed treatment of a cataract in a child can lead to deprivation amblyopia, in which improper development of the visual pathways leads to permanent vision loss. In developed countries, 0.1 to 0.4 per 10,000 children are blind from childhood cataracts, and the number increases tenfold in developing countries with limited access to healthcare [37]. Trauma to the globe can induce monocular cataract formation, which carries the highest risk of amblyopia in children. The percentage of childhood cataracts from a traumatic etiology has been reported from 11.6% to 57% [39,40,40]. Cataract in a child can also be congenital, which may be genetic (autosomal dominant), associated with a systemic disease, or idiopathic [41].
Traumatic cataract is precipitated by blunt injury to the eye or direct penetrating injury to the crystalline lens and can occur acutely or years after the inciting injury. Blunt trauma causes a “shock wave” to advance through the eye, which stimulates cataract formation. Penetrating injury leads to opacification at the site of penetrating trauma and can rapidly progress to complete lens opacification. The mechanism of traumatic cataract in children varies based on geographic location. The majority of injuries are accidental while children are playing or involved in sports [42, 43]. In a review of patients in Colorado, United States, the most common cause of monocular cataract was from metallic objects including knives or BB guns, while bilateral cataracts were often associated with chronic self-injurious hitting or firework injuries [44].
Clinical Presentation and Diagnosis
The clinical presentation of cataract is variable in a child. Patients typically have a recent, or sometimes remote, history of ocular trauma and may or may not complain of decreased visual acuity. Other presenting signs and symptoms include photophobia, strabismus, or the parents noting an abnormal opacification or discoloration of the child’s eye. Leukocoria or “white pupil” is the loss of the pupillary red reflex and may be present. Small cataracts may not cause any symptoms and may be found incidentally during a routine eye exam. The diagnosis of cataract is made by slit lamp examination which demonstrates focal or complete opacification of the crystalline lens. Contusion-related traumatic cataracts classically form a rosette or stellate opacification (◘ Fig. 8.4). Total white lens opacification may also be seen.

Slit lamp photograph showing stellate traumatic cataract following blunt trauma
Management
Visually significant traumatic cataracts should be removed surgically within weeks of the injury, especially for children less than 6 years of age who are at greatest risk of developing deprivation amblyopia [45]. Surgical planning can be complex for these patients and varies depending on the age of the child and the extent of ocular injury. Postoperatively, pediatric patients have a higher tendency for inflammation, intraocular pressure increases, hyphema, posterior capsular opacification, lens-iris capture with intraocular lens decentration, and long-term increased risk of glaucoma [47,48,48]. However the prognosis is overall favorable. Patients with traumatic cataract often have good visual outcomes [49, 50].
1.8 Ectopia Lentis and Lens Subluxation
Introduction
Ectopia lentis describes displacement or malposition of the crystalline lens. The lens may be subluxed, partially displaced while remaining in the pupillary space, or it may be luxed, completely dislocated and found free floating in the vitreous, anterior chamber or laying directly on the retina. Ectopia lentis is most commonly the result of blunt trauma to the globe, in which shearing forces stretch and break the lens zonules resulting in zonular dehiscence and subsequent dislocation. Other causes of ectopia lentis include congenital conditions that predispose to zonular weakness such as Marfan syndrome, homocystinuria, or Ehlers-Danlos syndrome. These conditions should be considered in non-traumatic cases, or when lens dislocation occurs after a minor injury.
Clinical Presentation and Diagnosis
Symptoms of ectopia lentis depend on the degree of lens dislocation. In cases of mild subluxation, vision may be minimally affected due to refractive changes or not affected at all. Complete dislocation will cause severe vision loss. Slit lamp examination is necessary to evaluate the position of the lens, and the edge of a subluxed lens may be visible through a dilated pupil (◘ Fig. 8.5). Iridodonesis (quivering of the iris) or phacodonesis (quivering of the lens) may be present. A posteriorly luxed lens may be visualized on dilated funduscopic exam, B-scan ultrasonography, UBM, or CT scan. An anteriorly luxed lens will be visualized in the anterior chamber and can cause pain and a rise in intraocular pressure due to pupillary block.

Clinical photograph showing lens subluxation (ectopia lentis) inferiorly
Management
Management of ectopia lentis in children initially involves optimization of optical refraction in order to prevent amblyopia. Cataract extraction with intraocular lens implantation may be considered when functional visual acuity cannot be achieved with refraction, the refraction is unstable due to lens mobility, or when displacement of the lens causes secondary ocular hypertension [51]. Following surgical correction, patients should be monitored for late intraocular lens (IOL) decentration or subluxation, especially if there is a sutured IOL which has long-term risks of suture breakage 5 or more years following insertion [53,54,54]. Overall, prognosis is good for these patients with the majority experiencing an improvement in visual acuity after surgery [55]. Despite the risks of long-term suture breakage, overall good outcomes have been reported with both iris-fixated [56] and scleral-fixated [57, 58] intraocular lenses in children. Long-term follow-up shows stability of corrected vision [59].
1.9 Case Study
A 7-year-old boy presented to the emergency department after being hit in the left eye with a soccer ball. He complained of ocular pain and blurry vision. Visual acuity was 20/20 in the right eye and 20/100 in the left eye. A 3 mm layered hyphema was visible inferiorly in the anterior chamber (◘ Fig. 8.6). Initial intraocular pressure (IOP) measurements were within normal limits. A B-scan was performed because of the poor view to the fundus and was within normal limits. A sickle cell screen was negative. The patient was started on prednisolone acetate 1% eye drops four times a day to the left eye and cyclopentolate hydrochloride eye drops three times a day to his left eye. The patient was advised to maintain strict bed rest and was given daily follow-up. On day 1, intraocular pressure was found to be elevated to 35 mm hg. The patient was started on timolol eye drops twice a day with improvement in intraocular pressure. After 10 days, the clot resorbed and intraocular pressure remained stable after cessation of timolol. His visual acuity returned to 20/20.

Clinical photograph showing layered hyphema. (Reprinted with permission from the American Academy of Ophthalmology. © 2019 American Academy of Ophthalmology)
Key Points
-
For all childhood ocular trauma, early intervention is critical to decrease the risk of amblyopia, in which improper development of the visual pathways leads to permanent vision loss.
-
Subconjunctival hemorrhage resolves spontaneously and does not require treatment.
-
Patients with hyphema must be closely monitored for complications, which include rebleed, elevations in intraocular pressure, optic atrophy, corneal bloodstaining, synechiae formation, and amblyopia.
-
Traumatic hyphemas are typically managed with topical cycloplegics, steroids, and, if necessary, intraocular pressure lowering medications.
-
Traumatic iritis presents 24–48 hours after traumatic eye injury, and patients present with photophobia, tearing, and blurry vision.
-
Iris sphincter tears appear as scalloped notches in the iris sphincter at the pupillary margin and may coincide with the presence of hyphema and traumatic iritis.
-
Cyclodialysis is a separation of the longitudinal fibers of the ciliary muscle from the scleral spur. Patients will have low intraocular pressure, and early management is medical with topical cycloplegics.
-
Traumatic cataract may form after blunt or penetrating injury to the eye, and patients will have decreased visual acuity in the affected eye. Early surgical management is indicated in children.
-
Ectopia lentis describes displacement or malposition of the crystalline lens, and usually occurs following blunt ocular trauma.
Review Questions
-
1.
Subconjunctival hemorrhages are best managed by
-
(a)
Observation
-
(b)
Topical cycloplegics
-
(c)
Topical steroids
-
(d)
Stopping use of blood thinners
-
(a)
-
2.
An 8-year-old boy presents to the emergency room after being hit in the right eye with a basketball. He reports blurry vision, eye pain, headache, and sensitivity to light. The intraocular pressure of the right eye is 34 mm Hg, and a 2 mm layered hyphema is found in the anterior chamber. Sickle cell prep is negative. The best next step is
-
(a)
Surgical evacuation of the anterior chamber
-
(b)
Placement of an eye shield, bed rest, and observation
-
(c)
Topical cycloplegics, steroids, and intraocular pressure lowering drops
-
(d)
Topical and oral NSAIDs
-
(a)
-
3.
Traumatic iritis typically presents __ after a traumatic eye injury
-
(a)
Immediately
-
(b)
Several hours
-
(c)
24–48 hours
-
(d)
1 week
-
(a)
-
4.
Iridodialysis is
-
(a)
The separation of the longitudinal fibers of the ciliary muscle from the scleral spur
-
(b)
The separation of the iris root from the ciliary body
-
(c)
The separation of the anterior layer of iris stroma is separated from the posterior iris stroma
-
(d)
The disruption of the marginal sphincter fibers of the iris
-
(a)
-
5.
What is the typical clinical presentation of traumatic cyclodialysis?
-
(a)
Elevated intraocular pressure > 35 mmHg
-
(b)
Very low intraocular pressure < 5 mmHg
-
(c)
Irregularly shaped pupillary margins
-
(d)
Blood in the anterior chamber (hyphema)
-
(a)
-
6.
A 2-year-old girl with no past medical history and normal development to date was a passenger in a motor vehicle accident and on examination is noted to have a “white pupil” with loss of the pupillary light reflex. What is the likely diagnosis?
-
(a)
Traumatic cataract
-
(b)
Hyphema
-
(c)
Ptosis
-
(d)
Strabismus
-
(a)
Answer
-
1.
(a)
-
2.
(c)
-
3.
(c)
-
4.
(b)
-
5.
(b)
-
6.
(a)
References
Subconjunctival Hemorrhage
Mimura T, Usui T, Yamagami S, Funatsu H, Noma H, Honda N, Amano S. Recent causes of subconjunctival hemorrhage. Ophthalmologica. 2010;224(3):133–7.
Hu DN, Mou CH, Chao SC, Lin CY, NIen CW, Kuan PT, Jonas JB, Sung FC. Incidence of Non-Traumatic Subconjunctival Hemorrhage in a Nationwide Study in Taiwan from 2000 to 2011. PLoS One. 2015;10(6):e0132762.
Hyphema
Turkcu FM, Yuksei H, Sahin A, Cingu K, Ari S, Cinar Y, Sahin M, Yildirim A, Caca I. Demographic and etiologic characteristics of children with traumatic serious hyphema. Ulus Travma Acil Cerrahi Derg. 2013;19(4):357–62.
Trief D, Adebona OT, Turaiba AV, Shah AS. The pediatric traumatic hyphema. Int Ophthalmol Clin. 2013;53(4):43–57.
Shazly TA, Al Hussaini AK. Pediatric ocular injuries from airsoft toy guns. J Pediatr Ophthalmol Strabismus. 2012;49(1):54–7.
Motley WW 3rd, Kaufman AH, West CE. Pediatric airbag-associated ocular trauma and endothelial cell loss. J AAPOS. 2003;7(6):380–3.
Leuder GT. Air bag-associated ocular trauma in children. Ophthalmology. 2000;107(8):1472–5.
Bansal S, Gunasekeran DV, Ang B, Lee J, Khandelwal R, Sullivan P, Agrawal R. Controversies in the pathophysiology and management of hyphema. Surv Ophthalmol. 2016;61(3):297–308.
Shields JA, Shields CL, Materin M. Diffuse infiltrating retinoblastoma presenting as a spontaneous hyphema. J Pediatr Ophthalmol Strabismus. 2000;37(5):311–2.
Karcioglu ZA, Mullaney PB. Diagnosis and management of iris juvenile xanthogranuloma. J Pediatr Ophthalmol Strabismus. 1997;34(1):44–51.
Lai JC, Fekrat S, Barron Y, Golberg MF. Traumatic hyphema in children: risk factors for complications. Arch Ophthalmol. 2001;119(1):64–70.
Agapitos PJ, Noel LP, Clarke WN. Traumatic hyphema in children. Ophthalmology. 1987;94(10):1238–41.
Gharaibeh A, Savage HI, Scherer RW, Goldberg MF, Lindsley K. Medical interventions for traumatic hyphema. Cochrane Database Syst Rev. 2019;1:CD005431.
Oh DJ, Chen JL, Vajaranant TS, Dikopf MS. Brimonidine tartrate for the treatment of glaucoma. Expert Opin Pharmacother. 2018;8:1–8.
Traumatic Iritis
Engelhard SB, Bajwa A, Reddy AK. Causes of uveitis in children without juvenile idiopathic arthritis. Clin Ophthalmol. 2015;9:1121–8.
Kaur S, Kaushik S, Singh PS. Traumatic Glaucoma in children. J Curr Glaucoma Pract. 2014;8(2):58–62.
Iris Trauma: Sphincter Tear
Pujari A, Agarwal D, Kumar Behera A, Bhaskaran K, Sharma N. Pathomechanism of iris sphincter tear. Med Hypotheses. 2019;122:147–9.
Weissbart SB, Ayres BD. Management of aniridia and iris defects: an update on iris prosthesis options. Curr Opin Ophthalmol. 2016;27(3):244–9.
Yousif M. Single suture customized loop for large iridodialysis repair. Clin Ophthalmol. 2016;10:1883–90.
Iris Trauma: Iridodialysis
Kumar S, Miller D, Atebara N, Blance E. A quantitative animal model of traumatic iridodialysis. Acta Ophthalmol. 1990;68(5):591–6.
Khan M, Reichstein DM, Recchia F. Ocular consequences of bottle rocket injuries in children and adolescents. Arch Ophthalmol. 2011;129(5):639–42.
Bullock JD, Ballal DR, Johnson DA, Bullock RJ. Ocular and orbital traumat from water balloon slingshots. A clinical, epidemiological, and experimental study. Ophthalmology. 1997;104(5):878–87.
Pandav SS, Gupta PC, Singh RR, Das K, Kaushik S, Raj S, Ram J. Cobbler’s technique for iridodialysis repair. Middle East Afr J Ophthalmol. 2016;23(1):142–4.
Okamoto Y, Yamada S, Akimoto M. Suturing repair of subtotal iridodialysis. Int Ophthalmol. 2018;38(1):395–8.
Iris Trauma: Cyclodialysis
González-Martín-Moro J, Contreras-Martín I, Muñoz-Negrete FJ, Gómez-sanz F, Zarallo-Gallardo J. Cyclodialysis: an update. Int Ophthalmol. 2017;37(2):441–57.
Aminlari A, Callahan CE. Medical, laser, and surgical management of inadvertent cyclodialysis cleft with hypotony. Arch Ophthalmol. 2004;122(3):399–404.
Hwang JM, Ahn K, Kim C, Park KA, Kee C. Ultrasonic biomicroscopic evaluation of cyclodialysis before and after direct cyclopexy. Arch Ophthalmol. 2008;126(9):1222–5.
Ioannidis AS, Barton K. Cyclodialysis cleft: causes and repair. Curr Opin Ophthalmol. 2010;21(2):150–4.
Mateo-Montoya A, Dreifuss S. Anterior segment optical coherence tomography as a diagnostic tool for cyclodialysis clefts. Arch Ophthalmol. 2009;127(1):109–10.
Prata TS, Palmiero PM, De Moraes CG, et al. Imaging of a traumatic cyclodialysis cleft in a child using slit-lamp-adapted optical coherence tomography. Eye (Lond). 2009;23(7):1618–9.
Han JC, Kwun YK, Cho SH, Kee C. Long-term outcomes of argon laser photocoagulation in small size cyclodialysis cleft. BMC Ophthalmol. 2015;15:123.
Ormerod LD, Baerveldt G, Sunalp MA, Riekhof FT. Management of the hypotonous cyclodialysis cleft. Ophthalmology. 1991;98(9):1384–93.
Ceruti P, Tosi R, Marchini G. Gas tamponade and cyclocryotherapy of a chronic cyclodialysis cleft. Br J Ophthalmol. 2009;93(3):414–6.
Agrawal P, Shah P. Long-term outcomes following the surgical repair of traumatic cyclodialysis clefts. Eye (Lond). 2013;27(12):1347–52.
Ioannidis AS, Bunce C, Barton K. The evaluation and surgical management of cyclodialysis clefts that have failed to respond to conservative management. Br J Ophthalmol. 2014;98(4):544–9.
Delgado MF, Daniels S, Pascal S, Dickens CJ. Hypotony maculopathy: improvement of visual acuity after 7 years. Am J Ophthalmol. 2001;132(6):931–3.
Traumatic Cataract
Lim Z, Rubab S, Chan YH, Levin AV. Pediatric cataract: the Toronto experience-etiology. Am J Ophthalmol. 2010;149(6):887–92.
Khokhar S, Agarwal T, Kumar G, Kushmesh R, Tejwani LK. Lenticular abnormalities in children. J Pediatr Ophthalmol Strabismus. 2012;49(1):32–7.
Johar SR, Savalia NK, Vasavada AR, Gupta PD. Epidemiology based etiological study of pediatric cataract in western India. Indian J Med Sci. 2004;58(3):115–21.
Xu YN, Huang YS, Xie LX. Pediatric traumatic cataract and surgery outcomes in eastern China: a hospital-based study. Int J Ophthalmol. 2013;6(2):160–4.
Deng H, Yuan L. Molecular genetics of congenital nuclear cataract. Eur J Med Genet. 2014;57(2–3):113–22.
Pandey SK, Ram J, Werner L, et al. Visual results and postoperative complications of capsular bag and ciliary sulcus fixation of posterior chamber intraocular lenses in children with traumatic cataracts. J Cataract Refract Surg. 1999;25(12):1576–84.
Sen P, Shah C, Sen A, Jain E, Mohan A. Primary versus secondary intraocular lens implantation in traumatic cataract after open-globe injury in pediatric patients. J Cataract Refract Surg. 2018;44(12):1446–53.
Qiu H, Fischer NA, Patnaik JL, Jung JL, Singh JK, Mccourt EA. Frequency of pediatric traumatic cataract and simultaneous retinal detachment. J AAPOS. 2018;22(6):429–32.
Shah M, Shah S, Upadhyay P, Agrawal R. Controversies in traumatic cataract classification and management: a review. Can J Ophthalmol. 2013;48(4):251–8.
Lacmanović Loncar V, Petric I. Surgical treatment, clinical outcomes, and complications of traumatic cataract: retrospective study. Croat Med J. 2004;45(3):310–3.
Trivedi RH, Wilson ME. Posterior capsule opacification in pediatric eyes with and without traumatic cataract. J Cataract Refract Surg. 2015;41(7):1461–4.
Haargaard B, Ritz C, Oudin A, et al. Risk of glaucoma after pediatric cataract surgery. Invest Ophthalmol Vis Sci. 2008;49(5):1791–6.
Birch EE, Cheng C, Stager DR, Felius J. Visual acuity development after the implantation of unilateral intraocular lenses in infants and young children. J AAPOS. 2005;9(6):527–32.
Lambert SR, Lynn MJ, Hartmann EE, et al. Comparison of contact lens and intraocular lens correction of monocular aphakia during infancy: a randomized clinical trial of HOTV optotype acuity at age 4.5 years and clinical findings at age 5 years. JAMA Ophthalmol. 2014;132(6):676–82.
Ectopia Lentis and Lens Subluxation
Neely DE, Plager DA. Management of ectopia lentis in children. Ophthalmol Clin N Am. 2001;14(3):493–9.
Buckley EG. Pediatric sutured intraocular lenses: trouble waiting to happen. Am J Ophthalmol. 2009;147(1):3–4.
Price MO, Price FW, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg. 2005;31(7):1320–6.
Asadi R, Kheirkhah A. Long-term results of scleral fixation of posterior chamber intraocular lenses in children. Ophthalmology. 2008;115(1):67–72.
Bardorf CM, Epley KD, Lueder GT, Tychsen L. Pediatric transscleral sutured intraocular lenses: efficacy and safety in 43 eyes followed an average of 3 years. J AAPOS. 2004;8(4):318–24.
Yen KG, Reddy AK, Weikert MP, Song Y, Hamill MB. Iris-fixated posterior chamber intraocular lenses in children. Am J Ophthalmol. 2009;147(1):121–6.
Konradsen T, Kugelberg M, Zetterström C. Visual outcomes and complications in surgery for ectopia lentis in children. J Cataract Refract Surg. 2007;33(5):819–24.
Hyun DW, Lee TG, Cho SW. Unilateral scleral fixation of posterior chamber intraocular lenses in pediatric complicated traumatic cataracts. Korean J Ophthalmol. 2009;23(3):148–52.
Anteby I, Isaac M, Benezra D. Hereditary subluxated lenses: visual performances and long-term follow-up after surgery. Ophthalmology. 2003;110(7):1344–8.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Palazzolo, L., Lanza, N., Rizzuti, A.E. (2021). Anterior Chamber and Lens. In: Shinder, R. (eds) Pediatric Ophthalmology in the Emergency Room . Springer, Cham. https://doi.org/10.1007/978-3-030-49950-1_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-49950-1_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-49949-5
Online ISBN: 978-3-030-49950-1
eBook Packages: MedicineMedicine (R0)