
Abstract
The objective of this study is to investigate the effect of sensory conflict on the occurrence and severity of simulator sickness in a flight simulator. According to the sensory conflict theory, it is expected that providing motion cues that match the visual cues will reduce the discrepancy between the sensory inputs and thus reduce simulator sickness. We tested the effect of motion cues thorough a human subject experiment with a spherical type motion platform. After completing pre-experiment questionnaire including Motion Sickness Susceptibility Questionnaire (MSSQ) and Immersive Tendency Questionnaire (ITQ), two groups of participants conducted a flight simulation session with or without motion cues for 40 min. In the simulation session, participants were asked to fly through the gates sequentially arranged along the figure-eight shaped route. The Simulator Sickness Questionnaire (SSQ) was filled out after the exposure to compare groups between with and without motion cues. Physiological data, including electrodermal activity, heart rate, blood volume pressure, and wrist temperature were also collected to find the relationship with perceived simulator sickness. The results showed that simulator sickness and disorientation significantly lowered in motion-based group. Also, nausea and oculomotor were marginally lower when motion cue was given. This study supports sensory conflict theory. Providing proper motion cue corresponding to the visual flow could be considered to prevent simulator sickness.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Training through simulators keeps gaining more attention since it saves enormous costs and enables a positive transfer to the real task. Despite these advantages, the use of simulators has limitations due to the occurrence of simulator sickness. Simulator sickness is, as the name suggests, a special form of motion sickness. Whereas general motion sickness occurs through vestibular stimulation, simulator sickness can occur with only visual cue. There are a couple of theories to explain the cause of simulator sickness. According to sensory conflict theory, when only a visual stimulus is given, a collision with the sense from vestibular and visual cue may occur, causing motion sickness [1]. Meanwhile, the development of the motion platform, which started with the Stewart platform, enables the simulator to provide not only visual stimuli but also vestibular proprioceptive stimuli. However, it is not yet clear whether a simulator with a motion platform can reduce simulator sickness because if sensory conflict theory is the cause of motion sickness, it’s hard to explain how to adapt to motion sickness when conflict continues [2]. Another model is called as postural instability theory [3]. Postural stability theory suggests that motion sickness occurs as the body slips the ability to control the stability of the posture during swaying in real or virtual reality.
Most people do not feel motion sickness when they are in a common situation where motion and visual cues coincide. But, they could feel sick in certain situations, such as when riding a vehicle, playing games, or experiencing virtual reality through a head-mounted display. On the other hand, we do not have symptoms called motion sickness when we study or work in our daily lives. In this sense, sensory conflict theory suggests that visual-vestibular sensory coherence can decrease sickness in simulators. According to Kennedy et al. (1993), the following three factors cause illness: simulator factors, individual factors, and simulated task factors [4]. One reason why analyzing the sensory conflict theory is important is that it could be determined if we can control motion sickness factors at the simulator factors level. If the cause of motion sickness is sensory conflict, the engineer has to design the cues so that they do not collide. Investigation about the theory can give directions to design guidelines from an engineering perspective. Individual factors are dealt with by postural stability theory and adaptation [5]. However, these are difficult to manipulate into design elements in applications. Simulated task factors are related to flight scenarios or vehicles [5].
In this paper, experiments were conducted to determine the effect of motion cues on simulator sickness. This experiment assumes that each sensor can independently indicate the orientation or motion of the body. It can explain why the sickness is caused by inconsistencies in cues from each organ. It has been hypothesized that the visual and vestibular system will receive cues that are as similar as possible by spherical motion simulator, resulting in lower sensory conflict and reduced simulator sickness.
This study aims to investigate the effect of sensory conflict on the occurrence and severity of simulator sickness in a flight simulator. The spherical motion-based simulator and fixed-based simulator were set to provide sensory cues. Also, the relationship between simulator sickness and other indicators measured by the questionnaire, such as motion sickness susceptibility and individual immersion tendency, is analyzed.
2 Background
2.1 Theoretical Models of Simulator Sickness
Simulator sickness is a well-known unintended adverse reaction when trained in a simulated environment, such as a flight simulator. Reason and Brand (1975) have suggested sensory conflict theory, which claims that simulator sickness is caused by mismatches among different sensory inputs [1]. The theory has been reviewed in various aspects and is generally accepted [6,7,8,9]. According to the theory, it is expected that providing motion cues that match the visual cues will reduce the discrepancy between the sensory inputs and thus reduce simulator sickness.
Another reason which causes the sickness is vection. Vection does not contradict against sensory conflict theory. According to Hettinger et al. (1990), the interpretation of the sensory conflict theory of motion sickness suggested that in fixed simulators, vection could be a necessary prerequisite for simulator sickness [10]. Illusory self-motion, called vection, commonly induces in the fixed simulator because the motion of the pilot is fixed and the visual cue is flowing. The pilot’s perception of himself and real feeling isn’t consistent. Previous studies have shown that participants who experienced visually induced motion sickness reported vection, and that vection could precede visually induced motion sickness [11, 12]. In other words, users who experienced illusory self-motion are more likely to have symptoms of simulator sickness [12]. The motion simulator that can generate inertial cues reduces the occurrence of vection because the visual flow and real motion match over a certain level. However, it is not experimentally supported yet due to the Stewart platform simulator with a limited rotation angle. The conventional motion platform has difficulties in providing appropriate motion cues that match the visual flow.
2.2 Effect of the Motion Cues on Simulator Sickness
McCauley and Sharkey (1992) noted that a teleoperating system with virtual reality can cause inconsistency due to the lack of vestibular stimulus corresponding to the visual cue [13]. Kennedy et al. (1987) explained that the head movements of the pilot during simulation is the reason for reducing simulator sickness in motion-based simulators than fixed ones [14]. They explained based on Sinacori’s (1970) observation that head movements in motion-based simulators are similar to head movements in real helicopter maneuvers, whereas head movements in static simulators were dissimilar [15]. Aykent et al. (2013) conducted an experimental study using a driving simulator, which showed nausea, dizziness, eyestrain, and tiredness were significantly decreased in the dynamic simulator than the static one [16]. However, most of the studies in flight simulators did not reduce simulator sickness even when motion cues were provided [13, 17, 18]. Sharkey and McCauley (1992) noted that the motion-based cab’s movement can be reduced before visually described acceleration stops, resulting in false cues [17]. In other words, it can be accelerated in the opposite direction to the aircraft in the simulation. False cues could induce the inconsistency between visual and motion cue. Providing appropriate motion cues with the motion-based simulator is important to prove sensory conflict theory empirically.
2.3 Impact of Individual Immersive Tendency on Simulator Sickness
Previous studies have shown that the relation of sense of presence and simulator sickness [19, 20]. Witmer and Singer (1993) reported that there is a positive correlation between Simulator Sickness Questionnaire (SSQ) scores and Presence Questionnaire (PQ) scores (r = 0.426, p = .001) [19]. They noted that participants reporting more simulator sickness symptoms in virtual reality responded to less sense of presence than those who report fewer illnesses [19]. However, the relationship between immersive tendency and simulator sickness was not reported on their paper.
Witmer and Singer (1993) developed an immersive tendency questionnaire (ITQ) consisting of three subscales through cluster analysis [19]. The three subscales are Involvement (7 items), Focus (7 items) and Games (2 items). ITQ consists of a total of 18 items, including 2 items not included in three subscales. Afterward, Jerome and Witmer (2002) revealed that the effect of immersive tendency on simulator sickness was found to be positive through structural equation modeling using questionnaires (.15, p < .05) [20]. However, it is not yet known that each subscale of the immersive tendency is associated with which symptoms of simulator sickness.
2.4 Hypothesis
What is not revealed in previous studies is whether simulator sickness occurs less by providing the appropriate motion cues that matches the visual cues. Also, it is not yet clear which subscales of immersive tendency (Involvement, Focus, Games) are associated with symptoms of simulator sickness. Therefore, the hypothesis of the study is compared to fixed-based simulator (without motion), motion-based simulator (with motion) will reduce simulator sickness due to the sensory conflict theory. In this study, the experiment was carried out using a spherical motion platform to minimize false cues. An empirical experiment was conducted to reveal the effect of proper motion cues in flight simulator. On the other hand, the correlations between the individual’s immersive tendency and their subscales (Involvement, Focus, and Games) and simulator sickness symptoms (nausea, oculomotor, disorientation, and total severity) were analyzed to investigate the relation between them.
3 Method
3.1 Participants
Fifteen (10 men, 5 women) university students participated in the study with a mean age of 26.1 years (SD; Standard Deviation = 2.19). They were divided into two groups and assigned to different types of simulators. One group (7 men) named ‘Motion-based’ experienced the motion-based simulator with the mean age of 27.6 years (SD = 2.15). The other group (3 men, 5 women) named ‘Fixed-based’ experienced a fixed-based simulator with the mean age of 24.88 years (SD = 1.36). Before the experiment, participants were informed that the simulation with the head-mounted display could occur nausea or simulator sickness and they could stop the experiment anytime they want.
3.2 Apparatus
Flight simulator software used in the study was Lockheed Martin’s Prepar3D. It could simulate various flight environments with different conditions. The virtual environment implemented for this experiment used a head-mounted display VIVE Pro Eye form HTC, which provides a resolution of 1440 × 1600 pixels per eye (2880 × 1600 pixels combined) and 110° of field of view. Biosignals were recorded by an Empatica E4 Wristband. It can collect electrodermal activity (galvanic skin response), heart rate, blood volume pressure and the temperature of the wrist. Heart rate was measured once per second. Blood volume pressure was measured at 64 Hz. Electrodermal activity and temperature were measured at 4 Hz. The experiment was conducted in an immersive virtual reality environment equipped with a spherical type motion simulator using the multi-degree of freedom platform at UNIST (Ulsan National Institute of Science and Technology, Korea). The motion simulator independently controls rotation and translation motion, and provide unlimited yawing rotations [21]. For the safety of the participants, the angle of roll and pitch was limited up to 20°. The spherical type motion simulator generates closely matching body motions with the actual flight motion. In the fixed condition, motion cues were not provided to the participants.
3.3 Manipulation and Measurements
Independent Variable.
An independent variable in this study was whether there is the motion cues. With motion and without motion were the levels of the independent variable. A fixed-based simulator used to give only visual cue, whereas a motion-based simulator could give both visual and motion cue.
Dependent Variable and Measurement.
Simulator sickness was the main interest of the study. It was measured by the Simulator Sickness Questionnaire (SSQ). By SSQ, nausea, oculomotor, disorientation, and total severity were collected. Also, the biosignal was determined as a quantitative and objective data that can determine whether the simulator sickness occurred. Biosignal records were measured by Empatica E4 wristband. The SSQ was used as a subjective indicator of simulator sickness, and biosignals were used as an objective one.
Questionnaires.
Participants were asked to complete two surveys before the simulation which include motion sickness susceptibility questionnaire (MSSQ) and immersive tendency questionnaire [22]. A short form of motion sickness susceptibility questionnaire asks about their experience of motion sickness when riding various vehicles or park attractions in the past. The questionnaire divide into two sections. First section A is about the experience before age 12, whereas section B is about the past 10 years. The MSSQ percentile scores in this experiment ranged from 0 to 92.37. The average percentile score of the ‘Motion-based’ group was 42.11 (SD = 30.29) and the ‘Fixed-based’ group was 43.65 (SD = 33.12).
In the related paper, 18 items with verified scale reliability were used as ITQ [19]. In ITQ, 3 subscales were labeled as involvement, focus, and games. The questionnaire consists of questions asked about immersive tendencies based on the participant’s experience. The average total ITQ score of the ‘Motion-based’ group was 72.29 (SD = 5.09) and the ‘Fixed-based’ group was 72.50 (SD = 13.38).
After exposure to the virtual reality simulation, each participant was completed SSQ [4]. The questionnaire contains 16 specific symptoms. Participants were asked to rate symptoms from 0 to 3 (None = 0; Slight = 1; Moderate = 2; Severe = 3). 16 specific symptoms are classified on 3 subscales: Nausea, Oculomotor, and Disorientation. The total severity representing the overall simulator sickness can be calculated by multiplying the sum of these three subscales with the weight 3.74. The results for this SSQ score are discussed in Sect. 4.
3.4 Procedures
Participants were fully informed about the experiment that the simulation could cause simulator sickness and they have a right to stop anytime. They were given brief information about the biosignal recording device and the experimental procedures. All participants filled the pre-exposure questionnaires which include MSSQ and ITQ. After wearing the biosignal recording device, Empatica E4 wristband, each participant had a 10 min electrode stabilization period and a 5 min baseline measuring period. Participants received a training period of about 5 min to practice controlling aircraft, and they conducted the main experiment for about 40 min. Experiment scenario designed in Prepar3D guided the participant to fly through a figure-eight route in the sky where the gates are arranged to pass through sequentially. Through the experiment, participants were asked about their current simulator sickness symptoms in 4-point scale (0 to 3; None = 0; Slight = 1; Moderate = 2; Severe = 3) every two minutes. Before the experiment, participants were informed about the symptoms of simulator sickness such as nausea, oculomotor and disorientation. After performing the simulation, participants completed simulator sickness questionnaire.
4 Results
4.1 Subjective Indicator: Simulator Sickness Questionnaire
In this experiment, two different groups of virtual reality flight simulations were compared using ‘Motion-based’ and ‘Fixed-based’. A total of 15 data were collected from each group. By the Kolmogorov-Smirnov test and Shapiro-Wilk test, it was confirmed that the normality assumptions were met. Levene’s test was also performed to confirm that the two groups were following the equality of variances. Levene’s test indicated equal variances of Nausea (F = 0.274, p = .609), Oculomotor (F = 0.242, p = .631), Disorientation (F = .041, p = .842), Total Severity (F = 0.031, p = .864).
The results showed that total severity, which means simulator sickness (F(1, 13) = 4.8, p = .047), and disorientation (F(1, 13) = 6.665, p = .023) were significantly lower for the motion-based group than for the fixed-based group. The nausea (F(1, 13) = 2.614, p = .130) and oculomotor (F(1, 13) = 3.431, p = .087) which is the symptoms of simulator sickness were marginally lower for the motion-based group than another (Table 1) and (Fig. 1).

Box plot of SSQ results for each symptom for two conditions
4.2 Objective Indicators: Biosignal Records
Biosignals were compared to simulator sickness severity on the 0 to 3 scale which was asked every two minutes in the simulation period. For the analysis of the physiological response, the baseline was measured for each signal through a baseline period of 5 min. The baseline was subtracted from the biosignals recorded every two minutes after exposure to the simulator. Analysis of the experimental data proceeded with the difference from baseline.
Blood volume pressure (BVP) data from two groups met equal variances assumption by Levene’s test. However, heart rate (HR), electrodermal activity (EDA) and temperature (TEMP) do not satisfy the equality of variance. Therefore, an analysis of variance (ANOVA) was conducted with only BVP records. Other biosignals such as HR, EDA and TEMP were analyzed by Welch’s ANOVA. It is because the analysis method can be used even if equality of variances are not assumed [23].
Results of Objective Indicators.
The difference in BVP from baseline was significantly higher in the group with motion cues than another group without motion, F(1, 280) = 19.370, p < .001. Also, the difference from the baseline of HR was significantly higher in the motion simulation group than the fixed simulation group, F(1, 233.796) = 60.669, p < .001. The differences from the baseline of EDA (F(1, 252.684) = 16.098, p < .001) and TEMP (F(1, 255.430) = 11.828, p = .001) were significantly higher in the fixed-based simulator group than motion-based simulator group.
4.3 Expected Correlation Between Simulator Sickness and Others
Relation to Immersive Tendency.
In the ITQ questionnaire, labeled as involvement, focus, and games, higher scores indicate that the individuals are more immersive. A correlation analysis between SSQ symptoms and GAMES label revealed that participants’ experience with the more frequent (Q21) and deeply involved (Q10) in the game, the less simulator sickness (total severity) occurred (r(13) = −.755, p = .001). Also, symptoms of simulator sickness and the GAMES subscale showed negative correlation, and the Pearson correlation coefficients are as follows: Nausea (r(13) = −.611, p = .016), Oculomotor (r(13) = −.747, p = .001), disorientation (r(13) = −.731, p = .002) (Fig. 2). Other labels and total ITQ score weren’t significantly correlated to SSQ scores.

Relationship between the label GAMES and simulator sickness (and its symptoms)
Relation to Motion Sickness Susceptibility.
Motion sickness susceptibility questionnaire is well known as a predictor of the simulator sickness. However, in this experiment, there was no significant correlation between MSSQ and SSQ.
The Relation Between Immersive Tendency and Motion Sickness Susceptibility.
There was a positive Pearson correlation between the MSSQ raw (MSA + MSB) score and total ITQ score (r(13) = .607, p = .016). There was also a positive correlation with the MSSQ raw score and the FOCUS scale of ITQ (r(13) = .684, p = .005). Participants with high susceptibility scores who frequently experienced motion sickness, both when childhood (MSA) and adults (MSB), tended to maintain focus on their activities more than others who scored lower in MSSQ (Table 2).
4.4 Temporal Aspects of the Simulator Sickness
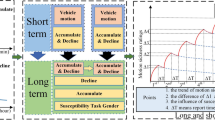
As the simulation time passed, the severity of simulator sickness (0 to 3) gradually increased. A linear regression was calculated to predict simulator sickness severity based on exposure time. A significant regression equation was found (F(1, 280) = 37.615, p < .001), with an R2 of .118. Participants’ predicted simulator sickness severity is equal to .277 + .026 * (Simulation time) when the simulation time is measured in minutes. Simulator sickness increased .026 for each minute of simulation time. Results of the Pearson correlation also indicated that there was a significant positive association between simulation time and simulator sickness severity, r(280) = .344, p < .001 (Fig. 3).

Severity of simulator sickness over time (with 95% confidence interval bars)
5 Discussion
The experimental result showed significant differences in simulator sickness and disorientation depending upon the existence of motion cues. Also, there are marginally significant differences in nausea and oculomotor between the motion-based group and the fixed-based group. The results of the subjective index (SSQ) support the evidence for the sensory conflict theory. The spherical motion-based simulator provided proper motion cues, which reduced the mismatch between visual and vestibule-proprioceptive signal. In terms of flight posture, it can be explained based on a discussion by Kennedy et al. (1987), which states that the pilot’s head movements are more similar to the head movements of a real helicopter in a motion-based simulator [14]. This study was conducted using fixed-wing aircraft, not helicopters, but a spherical motion platform was used to provide a motion similar to the angle at which the actual plane would tilt. Providing proper motion cues that correspond to visual cues can reduce simulator sickness by reducing the magnitude of sensory conflict and providing realistic head movements in flight.
5.1 Discussions on the Physiological Response
The change in biosignal was analyzed by the difference between the signal measured at the interval of 2 min and the signal measured at the baseline (5 min). The results showed that BVP and HR were higher in the motion-based group and EDA and TEMP were higher in the fixed-based group. BVP and EDA support the results of the subjective questionnaire SSQ, but HR and TEMP are not. The BVP and EDA results indicate that simulator sickness is less severe with motion cues, which supports the SSQ results. However, HR and TEMP results suggest that simulator sickness is more severe when there are motion cues, contrary to the subjective questionnaire results.
Blood Volume Pulse.
According to reviewed by Dahlman (2009), BVP falls as a result of sympathetic domination as motion sickness progresses [24, 25]. Besides, the BVP response was highly variable between individuals and varied depending on the context [24, 26]. In the study of Cowings et al. (1986), the volume pulse decreased sharply at the onset of motion sickness stimulation and then gradually increased as motion stimulation continued [26]. The 0 to 3 verbally asked simulator sickness scale and the BVP response difference from baseline responded every two minutes were negatively correlated with r(280) = −.197 and p = .001. The correlation results support previous studies that BVP decreased with motion sickness progresses.
Heart Rate.
R. Liu et al. (2017) discussed that HR declined at the beginning of exposure and then increased in the last few minutes [27]. Similar patterns were founded in this experiment. After the onset of the simulation, HR gradually decreased for about 28 min in both groups, then slowly increased at the end. The 0 to 3 verbally asked simulator sickness scale and the HR response difference from baseline responded every two minutes were negatively correlated with r(280) = −.290 and p < .001. In this experiment, the motion-based simulator participants who responded that they felt relatively less simulator sickness increased HR than baseline when exposed. On the other hand, there are contrast results in other studies [28, 29]. In their studies, HR was decreased when sickness induced. Further research on the relationship between HR and motion sickness is needed.
Electrodermal Activity.
EDA and TEMP rose with inducing simulator sickness compared to other signals. EDA is generally known as a physiological response that increases with motion sickness [30, 31] or nausea [32]. The 0 to 3 verbally asked simulator sickness scale and the EDA response difference from baseline responded every two minutes were positively correlated with r(280) = .227 and p < .001. The correlation between simulator sickness and EDA matched with the results of previous studies.
Temperature.
TEMP is known to decrease as motion sickness occurs [30]. The 0 to 3 verbally asked simulator sickness scale and the TEMP response difference from baseline responded every two minutes were negatively correlated with r(280) = −.176 and p = .003. The correlation between simulator sickness and TEMP was found to support the results of the previous study. However, SSQ results are not supported by TEMP. In this experiment, TEMP was higher in the fixed-base group with more simulator sickness than motion-base group. Motion simulator experiments were conducted in a relatively well ventilated large laboratory, while fixed simulator experiments were conducted in a closed, narrow laboratory. The laboratory environment may have affected the subject’s temperature.
5.2 Positive Correlation Between Immersive Tendency in Game and Simulator Sickness
These were two questions that correspond to the GAMES subscale in ITQ [19].
-
1)
Do you ever become so involved in a video game that it is as if you are inside the game rather than moving a joystick and watching the screen?
-
2)
How often do you play arcade or video games? (OFTEN should be taken to mean every day or every two days, on average.)
It was a question of how often and how involved to play the game. Subjects who were more involved and more likely to play games felt less symptoms of simulator sickness. This can be interpreted as a game experience that help people feel less sick. For non-pilots, the flight simulator may feel like a game. When experiencing a simulator that feels like a game, people who have been more involved and frequently played games in the past may have become resistant to game sickness.
5.3 Simulator Sickness over Simulation Time
In this experiment, simulator sickness gradually increased in both groups as simulation time elapsed. The results of regression analysis using only fixed simulator results, a regression equation was found (F(1, 140) = 16.653, p < .001), with an R2 of .106. Fixed-based simulator participants’ predicted severity is equal to .448 + .025 * (Simulation Time) score when the simulation time is measured in minutes. Fixed-based participants’ severity of simulator sickness increased .025 for each minute of simulation time. In comparison, the results of regression using only motion simulator results, an equation was found (F(1, 138) = 26.061, p < .001), with an R2 of .399. Motion-based simulator participants’ predicted severity is equal to .064 + .028 * (Simulation Time) score. Motion-based participants’ severity of simulator sickness increased .028 for each minute of simulation time. The coefficient of the equation is similar in both conditions, whereas the y-intercept is higher in the fixed simulator, so the onset of symptoms is faster when there was no motion cues.
6 Conclusions
This study investigates how simulator sickness changes with the presence of motion cue. Participants in the group with motion cues felt significantly less simulator sickness and disorientation, and marginally less nausea and oculomotor. This supports the study of sensory conflict theory and subjective vertical conflict called vection which often leads to motion sickness. This result suggests that it may be helpful to provide a suitable motion cue that matches the visual flow to reduce simulator sickness. In the case of biosignals, BVP, HR, EDA, and TEMP were measured. Simulator sickness severity scale which were participants reported positively correlated with EDA, whereas negatively correlated with BVP, HR, and TEMP.
There are a couple of limitations to generalize the findings of this study. Since this experiment was conducted with adult college students, not actual pilots, it is prudent to apply experimental results directly to pilots who have experienced real motion. Also, the number of subjects was small as 15 in total, and the experiment was conducted with the between-subject design. Although we can avoid carry-over or order effects there are potential worries that the two groups may have different inclinations or individual differences. The motion-based group consisted of 7 men only, and the fixed-based group consisted of 3 men and 5 women. Motion sickness susceptibility due to these gender differences may vary. In this experiment, the average MSSQ percentile of the motion-based group was 42.11 (SD = 30.29) and the average of the fixed-based group was 43.65 (SD = 33.12). Motion sickness susceptibility acquired from MSSQ between the two groups was quite similar, but the effects of gender differences may have been confounded in the results.
References
Reason, J.T., Brand, J.J.: Motion Sickness. Academic Press, London (1975)
Stoffregen, T.A., Riccio, G.E.: An ecological critique of the sensory conflict theory of motion sickness. Ecol. Psychol. 3(3), 159–194 (1991)
Riccio, G.E., Stoffregen, T.A.: An ecological theory of motion sickness and postural instability. Ecol. Psychol. 3(3), 195–240 (1991)
Kennedy, R.S., Lane, N.E., Berbaum, K.S., Lilienthal, M.G.: Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 3(3), 203–220 (1993)
Aykent, B., Merienne, F., Guillet, C., Paillot, D., Kemeny, A.: Motion sickness evaluation and comparison for a static driving simulator and a dynamic driving simulator. Proc. Inst. Mech. Eng. Part D: J. Automob. Eng. 228(7), 818–829 (2014)
Kennedy, R.S., Hettinger, L.J., Lilienthal, M.G.: Simulator sickness. In: Motion and Space Sickness, pp. 317–341 (1988)
Kolasinski, E.M.: Simulator sickness in virtual environments, vol. 1027. US Army Research Institute for the Behavioral and Social Sciences (1995)
Schmäl, F.: Neuronal mechanisms and the treatment of motion sickness. Pharmacology 91(3–4), 229–241 (2013)
Shupak, A., Gordon, C.R.: Motion sickness: advances in pathogenesis, prediction, prevention, and treatment. Aviat. Space Environ. Med. 77(12), 1213–1223 (2006)
Hettinger, L.J., Berbaum, K.S., Kennedy, R.S., Dunlap, W.P., Nolan, M.D.: Vection and simulator sickness. Mil. Psychol. 2(3), 171–181 (1990)
Ji, J.T., So, R.H., Cheung, R.T.: Isolating the effects of vection and optokinetic nystagmus on optokinetic rotation-induced motion sickness. Hum. Factors 51(5), 739–751 (2009)
Koohestani, A., et al.: A knowledge discovery in motion sickness: a comprehensive literature review. IEEE access 7, 85755–85770 (2019)
McCauley, M.E., Sharkey, T.J.: Cybersickness: perception of self-motion in virtual environments. Presence: Teleoper. Virtual Environ. 1(3), 311–318 (1992)
Kennedy, R.S., Berbaum, K.S., Lilienthal, M.G., Dunlap, W.P., Mulligan, B.E.: Guidelines for alleviation of simulator sickness symptomatology (No. NAVTRASYSCEN-TR-87-007). Naval Training Systems Center Orlando FL (1987)
Sinacori, J.B.: Validation of ground based simulation. J. Am. Helicopter Soc. 15(3), 10–21 (1970)
Aykent, B., Merienne, F., Paillot, D., Kemeny, A.: Influence of inertial stimulus on visuo-vestibular cues conflict for lateral dynamics at driving simulators (2013)
Sharkey, T., McCauley, M.: Does a motion base prevent simulator sickness? In: Flight Simulation Technologies Conference, p. 4133, January 1992
Kaufeld, M., Alexander, T.: The impact of motion on individual simulator sickness in a moving Base VR simulator with head-mounted display (HMD). In: Chen, J., Fragomeni, G. (eds.) HCII 2019. LNCS, vol. 11574, pp. 461–472. Springer, Cham (2019). https://doi.org/10.1007/978-3-030-21607-8_36
Witmer, B.G., Singer, M.J.: Measuring presence in virtual environments: a presence questionnaire. Presence 7(3), 225–240 (1998)
Jerome, C.J., Witmer, B.: Immersive tendency, feeling of presence, and simulator sickness: formulation of a causal model. In: Proceedings of the Human Factors and Ergonomics Society Annual Meeting, vol. 46, no. 26, pp. 2197–2201. SAGE Publications, Los Angeles, September 2002
Lee, S., Park, S., Son, H.: Multi-DOFs motion platform based on spherical wheels for unmanned systems. In: 2016 13th International Conference on Ubiquitous Robots and Ambient Intelligence (URAI), pp. 35–37. IEEE, August 2016
Golding, J.F.: Predicting individual differences in motion sickness susceptibility by questionnaire. Pers. Individ. Differ. 41(2), 237–248 (2006)
Moder, K.: Alternatives to F-test in one way ANOVA in case of heterogeneity of variances (a simulation study). Psychol. Test Assess. Model. 52(4), 343–353 (2010)
Dahlman, J.: Psychophysiological and performance aspects on motion sickness. Doctoral dissertation, Linköping University Electronic Press (2009)
Brodal, P.: The Central Nervous System: Structure and Function. Oxford university Press, Oxford (2004)
Cowings, P.S., Suter, S., Toscano, W.B., Kamiya, J., Naifeh, K.: General autonomic components of motion sickness. Psychophysiology 23(5), 542–551 (1986)
Liu, R., Peli, E., Hwang, A.D.: Measuring visually induced motion sickness using wearable devices. Electron. Imaging 2017(14), 218–223 (2017)
Holmes, S.R., Griffin, M.J.: Correlation between heart rate and the severity of motion sickness caused by optokinetic stimulation. J. Psychophysiol. 15(1), 35 (2001)
Sugita, N., et al.: Quantitative evaluation of effects of visually-induced motion sickness based on causal coherence functions between blood pressure and heart rate. Displays 29(2), 167–175 (2008)
Kim, Y.Y., Kim, H.J., Kim, E.N., Ko, H.D., Kim, H.T.: Characteristic changes in the physiological components of cybersickness. Psychophysiology 42(5), 616–625 (2005)
Hu, S., Grant, W.F., Stern, R.M., Koch, K.L.: Motion sickness severity and physiological correlates during repeated exposures to a rotating optokinetic drum. Aviat. Space Environ. Med. 62, 308–314 (1991)
Crampton, G.H.: Studies of motion sickness: XVII. Physiological changes accompanying sickness in man. J. Appl. Physiol. 7(5), 501–507 (1955)
Acknowledgment
This work is financially supported by the Institute of Civil-Military Technology Cooperation funded by the Defense Acquisition Program Administration and Ministry of Trade, Industry, and Energy of Korea government under grant No. 17-CM-RB-27.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this paper

Cite this paper
Kim, J., Hwang, J., Park, T. (2020). Effect of Motion Cues on Simulator Sickness in a Flight Simulator. In: Chen, J.Y.C., Fragomeni, G. (eds) Virtual, Augmented and Mixed Reality. Design and Interaction. HCII 2020. Lecture Notes in Computer Science(), vol 12190. Springer, Cham. https://doi.org/10.1007/978-3-030-49695-1_33
Download citation
DOI: https://doi.org/10.1007/978-3-030-49695-1_33
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-49694-4
Online ISBN: 978-3-030-49695-1
eBook Packages: Computer ScienceComputer Science (R0)