
Abstract
The history of the urbanization process can determine the social identity of specific places and neighbourhoods. Understanding historical processes behind the physical environment of a city is the first step in an action-research in an urban setting. The characterisation of a neighbourhood, especially in a deprived and segregated urban context, requires a multidisciplinary approach that cannot be separated from a dedicated quantitative analysis, integrating various tools and approaches. In this study’s setting, defined by a high level of informality due to a history of exclusion from the surrounding area and a structural segregation from the city’s fabric, the integration of tools and point of views had to be used to detect and assess the presence of any inequalities in health. We used administrative health data, census information, and a customised version of a national health survey, integrating different baseline populations in order to develop a global vision of the state of health. This research also includes an evaluation of social determinants of health, hospitalisation rates and access to the emergency room, as well as the general self-perception of the population’s health compared to the surrounding neighbourhoods.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Background, Defining the “Informal” Rome
Cities go through overlapping stages of development, leaving legible traces in the social and urban fabric. The understanding of these dynamics and the elements that fuel them is crucial for the analysis of urban exclusion. Moreover, this understanding is essential in order to tackle social inequalities, which have direct consequences on the health of populations and communities.
Within most cities, there are veritable islands of segregation. While in some contexts, such as U.S. cities with marked ethnic segregation [1], in European cities, with some exceptions especially due to the colonial heritage, they are particularly characterized by economic deprivation and social exclusion, as in the case of the city of Rome [2] and of the “ex-Bastogi” residential complex [3].
1.1 A Historic Overview
Italy shows some peculiarities in terms of urban development [4]. In addition to historical urbanization, mainly concerning the Roman era and the Renaissance (XVI and XVII century), the proper development of Italian urban areas in modern and contemporary terms took place in the immediate post-unification period. This led to the industrialization of the “Padania” Plain and the renovation and expansion of the main cities of the Kingdom, following by growth in the second half of the nineteenth century as well as the reconstruction phase following WWII [4, 5].
Urban expansion, with a mass move of the population from agricultural areas at the expense of a large internal migration, took place during the so-called “economic boom” or what was also called the “Italian miracle” [6]. This period was followed by a long wave of unbridled and disorganized urbanization, despite the fact that planning had been carried out. This growth lasted about two decades between the ’60s and the ’80s, with serious environmental, urban and social consequences [7].
Along with this “formal” urbanization, driven by speculation, throughout the entire history of modern Italy, the phenomenon of the informal settlements has been a constant factor. Since the turn of the twentieth century, around these rapidly growing cities, various “informal” areas developed, often with housing facilities defined by extremely poor quality, when not directly in the form of shacks and slums. Entire population groups resided in these areas, drawn by the employment opportunities and wellbeing that cities were beginning to offer. However, these areas were unable to fully become part of the “civitas”, part of the urban social community. This phenomenon affected in particular the city of Rome [8, 9], that became the new Capital of the Kingdom of Italy in 1871.
At the time of the Savoy troops entry, on September 20th, 1870, the city of Rome had a population of little more than 200,000 inhabitants, enclosed within the Aurelian Walls, the late-imperial historical walls of the city. [8] Rome’s entrance into modernity coincides with rapid, vast urban development, as well as changes to the city’s infrastructure. This period also saw the construction of public and administration buildings, and entire neighbourhoods intended both for the ministerial ruling class as well as the administrative middle-class [8]. Nevertheless, the mass influx of people, especially from central and southern Italy, employed for the construction of the Capital, was not accompanied by adequate housing allocation and programming. Consequently, a large part of such population was simply obliged to make the best of their situation [8]. On the one hand, the “borgate” (hamlets) arose, from scheduled subdivisions of the Roman countryside, run and developed by cooperatives and workers’ associations. On the other hand, the “baraccamenti” (barracks) were built, makeshift buildings that were not proper homes, close to the Roman construction sites and along the main consular roads [8]. While the borgate immediately took their own neighbourhood identity, the baraccamenti became slums. The next urbanization stage, during the Fascist period, was simply a confirmation of this division between the “formal” and the “informal” city. In fact, this era actually worsened the phenomenon with the deportation of population from the areas of the centre that were “gutted” into the so-called “Borgate Ufficiali”, “official hamlets”. These areas were defined by a noteworthy spatial isolation, far away from the consolidated city and proper infrastructure, in facilities built with dubious building quality [8].
After WWII, the city of Rome saw a bitter struggle for the right to housing, especially in the new neighbourhoods of public residential housing (ERP, Edilizia Residenziale Pubblica). These areas served as urbanization centres and often arose next to the historical and official borgate, as well as the baraccamenti. As described above, next to an organized and public urban planning, the ’70s–’80s were defined by unbridled urbanization also in Rome, driven by building contractors (in Rome also called “palazzinari”, from the palazzina, the most common type of housing, with reduced volumes and isolation from the street front), often unscrupulous businessmen connected to the political power of parties from the First Republic [8]. The combination of these two phenomena, with the ERP areas once again as urbanization centres and the private sector expanding at the expenses of the Roman countryside, was flanked by another type of urbanization driven by the growing economic well-being in Italy. Consequently, new building aggregates arose even more distant from the historical centre of the City, starting from a mixture of subdivisions and authorized and unauthorized buildings. This resulted in entire neighbourhoods that were partly illegal and partly legal, often lacking the most basic urban services, and completely disassociated with the established and planned city. The original baraccamenti began to empty, but the practical and political practice of fighting for housing, combined with an overall superficial management of the enormous number of homes and apartment buildings, generated widespread cases of more or less politicised squatting of public and private buildings. Within this social and political context, the occupation and squatting of the Bastogi apartment complex took place [3].
In the 1990s immigration took hold of Italy, and the country’s major cities saw a sharp population increase as a result. In this case, social stratification also entailed different levels of access to the real estate market in its various forms. Consequently, the “barracks” arose once again, in an official or informal form, this time assuming also a strong ethnic connotation, yet maintaining always its economic and social causes [10, 11].
Answers to this rapid growth in housing demand can essentially be summarized along three lines:
-
(1)
The growth of informal and self-produced settlements, on one hand with the baraccamenti, and on the other hand with the construction of further informal borgate, in the outskirts of the Roman countryside, as discussed above;
-
(2)
The unbridled urbanization driven by private profit, investing especially in the eastern area of the city;
-
(3)
The public residential housing (ERP, Edilizia Residenziale Pubblica).
Each of these three answers further stratified the social classes of the capital city. The baraccamenti and self-produced settlements concerned the last and penultimate ones; the second were mainly addressed to the families of the wealthier classes who could access housing at market price; the last was addressed mainly to the working class that had fed the city’s economic growth.
1.2 Root Causes of Informal Settlements in Rome
The existence and persistence of urban social marginalization, particularly in Rome, are due to a series of causes with deep historical roots, albeit of different natures:
-
Normative and programming, especially related to the implementation of public housing policies, which are rarely accompanied by social inclusion policies;
-
Architectural, with striking examples of mistakes, especially in the implementation phase;
-
Urban planning, due to a fragmentation of the urban fabric as well as the substantial isolation of entire nuclei of urbanisation;
-
Social and economic, specifically due to an extensive deregulation of the real estate market, with consequent speculation, leading to an economic selection of the social composition of the neighbourhoods based on the price of the properties.
The city of Rome, or, more correctly, “Roma Capitale” [12], occupies an area of 1287.36 km2, with a population of 2,855,397 (February 2019), with an average population density of 2218.03 inhabitants/km2. The municipal territory is as large as the sum of the larger Italian cities (Milan, Naples, Genoa, Catania, Palermo, Florence and Bologna, all together), and larger than the municipal area of New York (1214 km2, including the waters of the Hudson bay).
In this regard, Rome represents a true anomaly on the international level. The capital has with a quite low population (not even three million residents), characterizing itself as a conurbation, with neighbourhoods that are far from the centre, yet belonging to the municipal administrative area, such as Ostia, more than 14 km from the GRA (great ring road, major highway around Rome) and almost 25 km from the city centre (in comparison, Milan and Pavia are 30 km away, just as Padua and Venice).
There is a direct consequence on the average population density, which is quite low. However, there is also an alternation of almost completely uninhabited areas and highly dense urban areas, with some neighbourhoods with over 15,000 people per square km, mostly in the belt of the so-called “historical periphery”. This leads to a vastly dispersed urban fabric, with substantial urban sprawl phenomena, and to a fragmentation in numerous settlements even quite populous, but extremely far from the centre, left disconnected [13].
The low population density and the dispersion of specific housing areas make the organization of public services such as transport (for which, according to current legislation, the municipal authority pays to the provider based on the number of km travelled) and waste collection (with means of transport has to cover enormous distances) extremely complicated and structurally expensive. This applies also to the organization of social and health services [14], especially in a context where the predominant model is hospital care. Only in recent years has there been a spread of the so-called “Case della Salute” (literally, “health houses”) [15], an organizational form that allows to take care in particular of fragile patients suffering from chronic pathologies, for whom, unless complications—often avoidable—occur, hospitalisation is certainly oversized, in particular in terms of cost compared to a territorial management. To date, in the face of a regional regulation providing one of these structures for each socio-medical district, only seven Case della Salute are active in the territory of “Roma Capitale” [16].
Another direct consequence certainly concerns the amount of traffic that crosses the city every day, also considering the enormous number of cars circulating in the capital [17]. The problem particularly concerns the city centre, where institutional and administrative activities are concentrated, and therefore a large part of the workforce, since the public employment sector is by far the most representative of the working population [18]. Traffic is primarily caused by the weakness of public transportation, which is clearly insufficient in order to guarantee effective connections among the different parts of the city. Moreover, due to the aforementioned fragmentation of the urban fabric, lack of efficient public transportation is one the main causes found in current studies on increasing volumes of private traffic [19], in a city with still a quite high number of road accidents [20].
This issue of population density is also connected to other problems of the city, with certainly more nuances, albeit also with perhaps more interesting roots. Different density patterns are correlated to the political orientation and to the economic sustainability of local commercial and business activities. These are contexts often characterized by a “segregated” population, due to their social background [21]. The groups also live in stigma and shame with respect to their belonging. Moreover, these elements also emerged several times during research and action activities in Bastogi [3].
Therefore, the study and analysis of data based on a single area of study would not allow—given the complexity of the phenomena in question—for an in-depth understanding of these contexts. Above all, a singular approach would lead only to a limited ability to act, in particular on the part of social and health institutions. The very existence of these areas involves problems relating to accessibility to services, varying from schools to hospitals. However, there are also problems related to crime, which has its roots in the economic deprivation, as well as social and economic problems, as in the case of Bastogi [3].
2 Social Determinants of Urban Health Inequalities
In order to try to reconstruct the multiplicity of factors that can affect health in urban areas, a classic instrument of epidemiology is quite useful: the directed acyclic graphs (DAGs) [22–24]. In DAGs each graphic sign acquires a precise meaning in regulating the causal relationship between the parties. The diagram in Fig. 1 is a DAGs. The development of DAGs may precede a research hypothesis, guiding the development of the consequent statistical analysis, or it may follow it, once significant associations have been highlighted by tests (obviously they are not necessarily random connections, however they can be a prerequisite).

A proposal of DAG of principal interaction between social determinants of health in urban contexts
There are examples in literature of proposed DAGs regarding urban health, some of which also consider the effect of the urban social ecosystem, or that of the constructed environment as well as macroeconomic dynamics.
The DAG proposed here (Fig. 1) is an attempt to synthesise a conceptual framework within which to move.
The proposed scheme is generally divided into two sectors, which correspond to the principal aspects related to the state of health in an urban environment [25–27]. In detail, we find the personal characteristics of social stratification, namely the social determinants of health (income, education, social-health services). These contribute to the definition of the state of health of a population, also in relation to the socio-economic and political general context, also according to the first scheme defined by Dahlgreen and Withehead in 1991 [28]. Specifically, the arrow connecting the “who you are” section with health outcomes is bidirectional. This is due to the fact the health outcomes themselves, starting from the concept of “health-poverty trap” [29], can in turn socially stratify the population, especially in contexts where social welfare policies do not protect the most fragile groups of the population.
The second section concerns “where you live”. These last two groups of factors are strictly interdependent. Dialectically, the urban economy contributes to defining the constructed environment, however the constructed (or “built”) environment influences the possibilities of urban economy development. Together, they create a dialogue with those factors most closely linked to sociality and to the ways of living the city, such as relational goods (squares, green spaces, gathering places), social cohesion and social capital (described above and defined as effect mediators from the scheme produced by CSDH) [30]. Finally, relational assets, cohesion and social capital, are obviously linked to one another, and mutually dependent: the availability of relational goods in fact conditions the capacity to develop social cohesion and social capital, which in turn can lead to forms of self-organization capable of autonomously developing physical spaces for aggregation and socialization.
Therefore, according to the proposed scheme, “who you are” moderates the effects of the population on the built environment. Consequently, starting from features such as work, education, possibility of accessing services, and ultimately possibility of action in the context in which it is immersed [31], the environment can have greater or lesser influence on the characteristics of its urban context, modifying its physical structure and socio-economic relationships (and therefore also the health characteristics of the resident population).
Albeit far from creating a thorough study on the vast discussion on the relationship between personal characteristics and context in the definition of the state of health, the proposed scheme is useful in highlighting the research’s approach, within a perspective of urban health [32].
3 Analysing Spatial and Social Segregation
There is an extensive body of literature on social inequalities in health in the urban context. In Italy, extremely interesting assessments and results have been obtained from the network of the SLM (Metropolitan Longitudinal Studies) [33–37], epidemiological tools able to integrate heterogeneous but fundamental data sources for the study of social and health dynamics of the urban contexts.
These systems have developed around the evaluation of the impact of social determinants of health, i.e. those social and material dimensions that determine, through direct or indirect casual pathways, the health of people and communities.
The SLM surveys [33] integrate different administrative sources:
-
General Population Census. This is the main administrative tool, managed by the National Institute of Statistics (ISTAT), which, every ten years, surveyed the Italian population resident and not (since October 2019 the census survey is on an annual basis and on a sample basis), defining its main dimensions and aspects, such as socio-demographic characteristics, education, employment and, starting from the 15th General Census of 2011, as well as the state and upkeep of buildings and housing. The ISTAT Census also allows for an effective geolocation of the data, taking advantage of the Census Sections, areas that in the urban contexts have the indicative size of a block. These Census Sections can be aggregated into further levels, such as the administrative levels of the larger Municipalities and of the Metropolitan Areas. In particular, in Rome, these are called Municipi (15 urban areas administered independently on particular management areas) [38] and Zone Urbanistiche (Urbanistic zones, 155 areas divided on topographical, toponymic or urban planning criteria, corresponding in general line to the districts, in the city centre).
-
Flow of health information and mortality registers. These are generated starting from the data coming from people’s contacts with the National Health Service in its various forms. The Health Information System flows are regulated at national level. They were created for administrative purposes, but have become particularly useful for defining the state of health of the population through the definition of incidence and prevalence of pathologies, evaluation of outcomes and performance of health organizations, as well as for study purposes. The main limitation of this tool is related to a certain territorial variability of the quality of the data, as well as problems linked to the privacy of the patients, even if this last aspect is now managed in the terms established by the European General Data Protection Regulation.
-
Register of Municipalities. These are the main sources of administrative information, and allow to obtain constantly updated information on the resident population within the municipal area, identifying its main demographic characteristics and the place of residence.
3.1 Bastogi as a Case-Study of Urban Segregation
The context of Bastogi (also known as ex-Bastogi, or former-Bastogi Building Complex) is a valid example of spatial and social segregation within the area of the Municipality of Rome. Built as a corporate motel [3, 38], occupied to address the necessity for housing for the most disadvantaged popular classes, then taken over by the Municipality and used to deal with the so-called “housing emergency”, today the area finds itself in a sort of limbo where formal assignees of public housing, long-standing occupants, new squatters and more or less organized crime all coexist together [3, 39].
In order to study this context, an approach integrating different information sources was used:
-
General Census of Population and Housing;
-
Health information flows;
-
Tailored questionnaires developed by institutional bodies.
Each of these sources ensured that the research offered a different point of view on the context. Moreover, multiple sources led to an understanding of some specific aspects. The integration and harmonization of the sources has also guaranteed the definition and quantification of certain problems, their outcome in terms of access to services, and the identification of possible solutions.
ISTAT, in particular, through the use of the bt.viewer online software [40], identified, from satellite images, areas of interest, and defined the administrative boundaries related to the Census Sections, the basic units of census detection. These images allowed researchers to geolocate not only the data related to the census survey, therefore guaranteeing a rather high level of detail that more or less corresponded to a city block, but also a communication between the health and personal information systems, linking to the code of the section the totally anonymized residents’ codes. As already specified, the Census Sections in the Municipality of Rome can in turn be aggregated in the form of Zone Urbanistiche (Urban Zones) and Municipi (Municipalities).
However, the aspect that needs to be emphasized is the heterogeneity of the denominators of each source. In fact, with approximately 2000 inhabitants estimated by the volunteers of the associations operating there [3], only 1033 were registered in 2011, while on the other hand an average of 1222 inhabitants per year were registered in the municipal registry between 2011 and 2017. This difference is essentially linked to the methodology behind the various sources, as described below.
3.2 General Census
The 15th General Census of Population and Housing of 2011 [41] is the basis used to quantify some aspects related to the socio-demographic characteristics of the population of Bastogi. This is the main institutional instrument in Italy for population assessments, managed by ISTAT and carried out every ten years. It allows for a fairly in-depth evaluation of some aspects relevant to health, previously exposed, such as education, employment, distribution by age classes, quality of buildings. The limitations of this source are mainly related to the way data are collected, for example as regards the aspects connected to the identification of the census population and the acquisition of census information of citizens through a self-compiled questionnaire [41].
The data relating to Bastogi were then compared with those relating to the Zone Urbanistiche (Urban Zones) of the XIII Municipio (Municipality), the administrative district in which Bastogi falls.
3.3 Institutional Health Data
Evaluation and assessment of health information flows, carried out by the Department of Epidemiology of the Health Service of the Lazio Region, has in particular led to an understanding of the Bastogi population’s use of health services, in terms of accesses to the Emergency Room and hospitalisation by using the data relating to the SIO (Hospital Information System) and SIES (Health Emergencies Information System) database.
This was possible through record linkage procedures between the Municipal Registry, with a survey carried out up to December 31st, 2014, which allowed the research team to define the demographic characteristics of the population, as well as the Healthcare Registry of the Lazio Region, by extracting the 2015 data using anonymous unique identification codes, to which the health information was linked.
Once again, in this case the survey unit was the Census Section, and the data were compared with the aggregate of some neighbouring areas (urban zones) of the XIII Municipio of “Roma Capitale”. The data extracted have been age-standardized with the method of direct standardization with reference to the population under study, allowing in such way the comparison between the different areas.
3.4 Official Health Survey: PASSI
The last source of data is the questionnaire called PASSI (an acronym that can be loosely translated as an assessment of “Progress of Healthcare Services in Italy”) [42], a tool used since 2005 by the Italian Local Health Authorities to verify the state of health perceived by the resident population recorded in the healthcare registries. Alongside this instrument, two further brief questionnaires were developed, concerning housing quality and Health Literacy. This survey was managed by the Prevention Department of ASL RM1 (Roma 1 Local Health Authority). In this case, the results were partially compared with the territory of the entire ASL RM1.
4 Results and Discussion
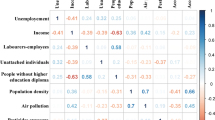
The Census data give us a fairly complete picture of Bastogi (Table 1). This area, compared with the XIII Municipio urbanistic zones, has significantly higher percentages of population with low educational qualifications, a higher number of foreigners, as well as a higher unemployment rate. All of the buildings appear in a poor state of maintenance and upkeep. Furthermore, all values are significantly higher than the comparison areas [3].
Regarding the data from the health information flows (Fig. 2), the Bastogi population has higher hospitalisation and Emergency Room accesses compared to the neighbouring areas of the XIII Municipio. In particular, rather high rates are found in the younger age groups (20–39) and among the elderly, both with regard to hospitalisations and access to the ER. Regarding access to the Emergency Room, we observed rates more than double for all age groups and both sexes.

Results from Regional Informative Health Data, Department of Epidemiology of Regional Health Service, Rome
From the data relating to the PASSI monitoring system, an overall picture of the health perceived by the population of Bastogi emerges (Table 2), with obvious criticalities. Specifically, the Bastogi population has a greater number of days with poor health, both physical and psychological, and a greater number of days in which, due to health problems, the population has not been possible to carry out their usual activities. Overall, 40% of respondents assess their health in negative terms (Table 2). Furthermore, although the majority of residents declare that they have their own general practitioner in the vicinity of their place of residence, two-thirds of the interviews state that their health problems are managed in particular by second level services, such as emergency rooms, outpatient clinics and hospitals.
5 Conclusions
The reported results suggest that are fundamental differences between the population living in the Bastogi area and the population of the neighbouring areas. These differences regard not only the social determinants of health distribution, such as low level of education and unemployment, but also self-perception of health and the use of health services, a pattern defined by a greater use of emergency health services in Bastogi when compared to their neighbours.
Moreover, the Bastogi population, although younger than the population of the surrounding areas, have alarming hospitalisation rates, indeed higher in the younger age groups.
Despite the different information sources used, the territory-based assessment of the Bastogi area shows a coherent picture, characterized by a concentration of social and health problems, with which the population copes by using hospital services rather than relying on prevention and primary care. On the one hand, the latter underlines issues in the offer of healthcare service and appropriateness of use, while on the other this aspect suggests that local health services have extensive room for improvement in health promotion and health services orientation, according to urban health principles [43, 44]. The interpretation of Census data—based on the Social Determinant of Health theory—may represent an effective starting point in the definition of possible issue related to the socio-health dimension. The implementation of additional integrated tools capable of communicating different data bases, such as the Permanent Census [45], or the Metropolitan Longitudinal Studies described above, certainly represents a step in the right direction.
References
Massey DS, Denton NA (1988) Suburbanization and Segregation in U.S. Metropolitan Areas. Am J Soc 94(3):592–626
Mudu P (2006) Patterns of segregation in contemporary Rome. Urban Geogr 27(5):422–440. https://doi.org/10.2747/0272-3638.27.5.422
Iorio S, Salvatori LM, Barnocchi A et al (2019) Social inequalities in the metropolitan area of Rome. A multidisciplinary analysis of the urban segregation of the “formerly-Bastogi” compound. Ann Ig 31(3):211–229
Benevolo L (1993) La città nella Storia d’Europa. Gius Laterza & Figli, Roma-Bari
Capanna A (2005) La casa per tutti. Il primo concorso INA-Casa e la ricostruzione civile del Paese. Rassegna di Architettura e Urbanistica 117:78–85
Nardozzi G (2003) The Italian “Economic Miracle”. Rivista di storia economica, Rivista fondata da Luigi Einaudi. 2(2003):139–180. https://doi.org/10.1410/9557
Secchi B (2005) La città del ventesimo secolo. Editori Laterza, Bari
Insolera I (2011) Roma Moderna, da Napoleone I al XXI Secolo. [(1° ed. 1962), Edizione ampliata con la collaborazione di Paolo Berdini, 2011]. Einaudi, Torino
Berlinguer G, Della Seta P (1960) Borgate di Roma. Editori Riuniti, Roma
Mudu P, Rossini L (2018) Occupations of housing and social centers in Rome: A durable resistance to neoliberalism and institutionalization. In: Lopez M, Angel M (eds) The urban politics of squatters’ movements. Palgrave MacMillan, pp 99–120
Associazione 21 Luglio. I margini del margine, comunità rom negli insediamenti formali e informali in Italia, rapporto 2018
Legge 42/2009, modifica dell’art114 comma 3 della Costituzione, introdotto con la L. Cost.3/2001 di revisione del titolo V parte II. G.U. n.103 del 6 maggio 2009
Lelo K (2017) Suburbs and fragmentation patterns: the case of Rome. Eurodiv Paper 44
Capolongo S, Rebecchi A, Dettori M et al (2018) Healthy design and urban planning strategies, actions, and policy to achieve salutogenic cities. Int J Environ Res Public Health 15:2698
Brambilla A, Maciocco G (2014) Le Case della salute. Recenti Prog Med 105:147–150
On Local Health Institution in Rome [Case della Salute nel territorio di Roma Capitale]: http://www.retesalutelazio.it/rete-salute-lazio/it/
Vehicles circulating in Rome [Veicoli circolanti a Roma Capitale], Ragioneria Generale—I Direzione “Sistemi informativi di pianificazione e controllo finanziario”—U.O. Statistica, anno 2016
Ufficio Statistico Roma (2016) Le Caratteristiche dell’Occupazione a Roma, anni 2008–2015. Ragioneria Generale—I Direzione “Sistemi informativi di pianificazione e controllo finanziario” U.O. Statistica, Dicembre 2016
Batty M, Besussi E, Chin N (2003) Traffic, Urban growth and suburban sprawl. Centre for Advanced Spatial Analysis, UCL, Working Paper Series, paper 70
Gariazzo C, Stafoggia M, Bruzzone S et al (2018) Association between mobile phone traffic volume and road crash fatalities: a population-based case-crossover study. Accid Anal Prev 115:25–33
Tomassi F (2013) Disuguaglianze, beni relazionali ed elezioni nelle periferie di Roma, Rivista di Politica Economica, n. 1–3, pp 403–450
Pearce N (1996) Traditional epidemiology, modern epidemiology, and public health. Am J Public Health 86(5):678–683
Greenland S, Pearl J, Robins JM (1999) Causal diagrams for epidemiologic research. Epidemiology 10(1):37–48
Lederer DJ, Bell SC, Branson RD, Chalmers JD, Marshall R, Maslove DM et al (2019) Control of confounding and reporting of results in causal inference studies. Guidance for authors from editors of respiratory, sleep, and critical care journals. Annals ATS 16(1):22–8
Vlahov D, Galea S, Gibble E, Freudenberg N (2005) Perspectives on urban conditions and population health. Cad Saúde Pública 21(3):949–957
Fleischer NL, Roux AVD (2008) Using directed acyclic graphs to guide analyses of neighbourhood health effects: an introduction. J Epidemiol Commun Health 62(9):842–846
Borrell C, Pons-Vigués M, Morrison J, Díez È (2013) Factors and processes influencing health inequalities in urban areas. J Epidemiol Commun Health 67(5):389–391
Dahlgren G, Whitehead M (1991) Policies and strategies to promote social equity in health. Institute for Futures Studies, Stockholm, Sweden
Whitehead M, Dahlgren G, Evans T (2001) Equity and health sector reforms: can low-income countries escape the medical poverty trap? The Lancet 358(9284):833–836
CSDH (2008) Closing the gap in a generation: health equity through action on the social determinants of health. Final Report of the Commission on Social Determinants of Health. World Health Organization, Geneva
Marmot M (2005) Social determinants of health inequalities. Lancet 365:1099–1104. https://doi.org/10.1016/S0140-6736-(05)71146-6
D’Alessandro D, Apolloni L, Capasso L (2017) Public health and urban planning: a powerful alliance to be enhanced in Italy. Ann Ig 29(5):453–463. https://doi.org/10.7416/ai.2017.2177
Caranci N, Di Girolamo C, Giorgi Rossi P on behalf of the IN-LiMeS Group et al (2018) Cohort profile: the Italian Network of Longitudinal Metropolitan Studies (IN-LiMeS), a multicentre cohort for socioeconomic inequalities in health monitoring. BMJ Open 8:e020572. https://doi.org/10.1136/bmjopen-2017-020572
Cacciani L, Bargagli AM, Cesaroni G et al (2015) Education and mortality in the rome longitudinal study. PLOS ONE 10(9):e0137576
Cesaroni G, Badaloni C, Romano V et al (2010) Socioeconomic position and health status of people who live near busy roads: the Rome Longitudinal Study (RoLS). Environ Health 9(1):41
Agabiti N, Barbieri G, Bardin A et al (2019) Immigrants’ health and socioeconomic inequalities of overall population residing in Italy evaluated through the Italian network of longitudinal metropolitan studies. Epidemiol Prev 43(5–6 Suppl 1):1–80
Paglione L, Angelici L, Davoli M, Agabiti N, Cesaroni G (2020) Mortality inequalities by occupational status and type of job in men and women: results from the Rome Longitudinal Study. BMJ Open 10(6):e033776
Statuto Roma Capitale, Delibera n.8 del 7 marzo 2013, confini stabiliti con Delibera n.11 dell’11 marzo 2013
Battisti A, Barnocchi A, Iorio S (2019) Urban regeneration process: the case of a residential complex in a suburb of Rome, Italy. Sustainability 11(21):6122
Online software bt.viewer, ISTAT. http://gisportal.istat.it/bt.viewer/
15th General Census ISTAT. https://www.istat.it/it/archivio/189483
Progresses of Local Health Units for Health in Italy [Progressi delle Aziende Sanitarie per la Salute in Italia—PASSI], EpiCentro, National Health Institute. https://www.epicentro.iss.it/passi/
Corburn J, Cohen AK (2012) Why we need urban health equity indicators: integrating science, policy, and community. PLoS Med 9(8):e1001285. https://doi.org/10.1371/journal.pmed.1001285
D’Alessandro D, Arletti S, Azara A, Buffoli M, Capasso L, Cappuccitti A, Casuccio A et al (2017) Strategies for disease prevention and health promotion in urban areas: the Erice 50 Charter. Ann Ig 29:481–493
Permanent Census, National Statistic Institute (ISTAT). Available at: https://www.istat.it/it/censimenti-permanenti/popolazione-e-abitazioni
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 The Editor(s) (if applicable) and The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Paglione, L. et al. (2020). Characterising a Setting with a High Level of Informality, Integrating National and Specialised Surveys, Administrative and Census Data. In: Battisti, A., Marceca, M., Iorio, S. (eds) Urban Health. AIMETA 2019. Green Energy and Technology. Springer, Cham. https://doi.org/10.1007/978-3-030-49446-9_6
Download citation
DOI: https://doi.org/10.1007/978-3-030-49446-9_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-49445-2
Online ISBN: 978-3-030-49446-9
eBook Packages: EnergyEnergy (R0)