
Abstract
The chapter focuses on the established treatment options to preserve fertility using ovarian stimulation with its well-known rates of conception using cryopreserved oocytes/embryos. Due to the special character of ovarian stimulation in the context of fertility preservation, where endometrial characteristics can be ignored, new options of ovarian stimulation need to be considered. Besides the fact that ovarian hyperstimulation syndrome needs to be avoided, time is limited, and the number of oocytes retrieved for cryopreservation should be optimized. Therefore, this chapter describes unique stimulation protocols including random start of stimulation, adequate amounts of gonadotropins used, double stimulation, ovulation inhibition using progestins, as well as using an aromatase inhibitor to reduce the amount of estrogen production in cases of a hormone receptor-positive tumour. Finally, the optimal combination of fertility preservation techniques is described.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The aim of ovarian stimulation is to obtain mature oocytes in order to preserve them in an unfertilised or fertilised state as a fertility reserve. In the FertiPROTEKT network, stimulation for the collection and cryopreservation of unfertilised or fertilised oocytes was carried out in approximately 40% of all fertility-preserving therapies performed [1].
The distinctive features of this form of fertility preservation are, on the one hand, that the treatment should be carried out as quickly as possible, so that necessary treatment for the underlying disease is not unnecessarily delayed. On the other hand, only one attempt is usually possible, which must be as efficient as possible. The maximum possible number of mature oocytes should be obtained without the risk of overstimulation.
It is also important to note that fertilised eggs can only be transferred to the woman with the consent of both partners. Since the cells can be stored for several years before a transfer, a possible separation of the couple must be considered during this time, which means that the woman would no longer have the option of retransferring of the fertilized cells. To avoid this risk, even in a stable partnership, it is recommended that all oocytes are frozen unfertilised or that splitting is carried out (50% fertilised, 50% unfertilised cryopreserved) to guarantee the woman’s independence.
Ovarian stimulation which begins at the time of menstruation is a routine procedure. Measures to minimize the risk of ovarian hyperstimulation syndrome are also clinically established (Table 1).
Stimulation started after menstruation, e.g. in the luteal phase to limit the duration of stimulation to 2 weeks, has already been tested in several clinical studies [2,3,4]. Double stimulation [5,6,7] and stimulation immediately after removal of ovarian tissue have also been the subject of several studies [8, 9].
Effectiveness
The number of oocytes collected depends on the age of the patient and the underlying individual ovarian reserve. However, the underlying disease has very little effect on the number of oocytes obtained [10, 11]. According to the FertiPROTEKT register, the average number of oocytes obtained from 809 women was [1] (Table 2):
Exceptions [1] are women who have undergone a surgical intervention on the ovaries before stimulation (see chapter “Ovarian Tumors and Ovarian Cancer”) or with Hodgkin’s lymphoma (see chapter “Hodgkin’s Lymphoma”). Fewer oocytes may be obtained after ovarian stimulation in women with a BRCA mutation, presumably due to a lower ovarian reserve (see chapter “Breast Cancer”).
If vitrification is adequately performed as a freezing technique, the survival and fertilisation rates of cryopreserved oocytes are very good. Numerous studies comparing unfertilised and fertilised cryopreserved oocytes with eggs without cryopreservation showed no relevant differences in pregnancy rates [12,13,14].
The effectiveness of oocyte vitrification has also been confirmed in oncological patients. In 11 women whose oocytes were collected at an average age of 35.6 years (30–41) and thawed and fertilized after the disease, an oocyte survival rate of 92%, a fertilization rate of 77% and an implantation rate of 64% were found. Pregnancy occurred in 7 of the 11 women and 4 (36%) gave birth [15].
Based on the number of oocytes that were removed and successfully fertilized before cytotoxic therapy, a FertiPROTEKT [15] study calculated the theoretical birth rate depending on the age of the woman using 125 follicular aspirations (Table 3):
Therefore, after ovarian stimulation with cryopreservation of unfertilized or fertilized oocytes, the theoretical birth rates mentioned in Table 2 can be assumed if the specified number of oocytes is obtained.
Risks
Ovarian stimulation can lead to side effects from the medication, as well as complications during follicular puncture (www.deutsches-ivf-register.de). Women may experience temporary weight gain, mood swings and a feeling of abdominal pressure due to the increase in size of the ovaries. Clinically relevant bleeding from follicular puncture or inflammation is rare. During stimulation of patients in the FertiPROTEKT network, severe ovarian hyperstimulation syndrome occurred only once in 708 stimulations [4]. Chemotherapy has so far only had to be postponed once by one day.
In addition, Del Pup & Peccatori [16] were unable to demonstrate a worsening of prognosis in hormone receptor-positive breast cancer patients stimulated with letrozole compared to non-stimulated controls.
Practical Approach
General
The standard protocol for stimulation is the antagonist protocol with ovulation induction using a GnRH agonist (GnRHa) (triptorelin 0.2 mg s.c.) to minimize the risk of the ovarian overstimulation syndrome [17]. In practice, a daily gonadotropin dose which is approximately 50 IU higher than that of stimulation with an intended fresh transfer is often administered to increase the number of oocytes.
Random Start Stimulation
Ovarian stimulation can be started at any time during the menstrual cycle with the exclusive aim of collecting oocytes (without fresh embryo transfer) with the same number of oocytes and the same fertilisation rates [1,2,3] (“random start stimulation”). Pregnancy rates are equally high compared to standard stimulation protocolls, when stimulation is started in the luteal phase [18] and the malformation rates are unaffected [19]. Identical results have also been demonstrated for egg donors and there is currently no disadvantage from “random start” stimulation [20]. According to previous studies, stimulation takes 1–2 days longer when stimulation is started in the luteal phase than when stimulation begins in the early follicular phase.
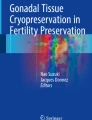
Stimulation can be performed as follows, depending on the cycle phase (Fig. 1):

Ovarian stimulation in different cycle phases
-
Start of stimulation in the early and middle follicular phase: conventional antagonist protocol with FSH or FSH/LH, addition of an GnRH antagonist (GnRHant) if dominant follicle >13 mm and GnRH agonist triggering with triptorelin 0.2 mg s.c. if 3 follicles ≥17 mm. Stimulation dose approx. 50 IU higher than with an intended fresh transfer.
-
Stimulation start in the late follicular phase with a dominant follicle ≥ approx. 13 mm: ovulation induction with triptorelin 0.2 mg s.c., followed by luteal phase stimulation directly after ovulation.
-
Stimulation start in the luteal phase: conventional antagonist protocol with FSH or FSH/LH, and GnRH agonist triggering with triptorelin 0.2 mg s.c. Stimulation dose approx. 75 IU higher than with an intended fresh transfer after a stimulation start in the early follicular phase. GnRH antagonist started when new dominant follicle > approx. 13 mm.
Progesterone Primed Ovarian Stimulation
Progesterone-primed ovarian stimulation (PPOS) was derived from luteal phase stimulation, which showed that no LH increase occurs under the influence of progesterone. Since the function of the endometrium does not play a role in fertility preservation (freeze-all strategy), the negative effect of progesterone on the endometrium does not come into effect [21]. Efficient ovulation inhibition, a low rate of side effects and predominantly comparable oocyte counts, fertilisation, implantation and pregnancy rates were demonstrated for 4 and 10 mg medroxyprogesterone acetate (MPA), 10 and 20 mg dydrogesterone and 100 and 200 mg oral micronized progesterone.
The only exception was the latest study by Begueria et al. [22], which showed a lower efficiency of 10 mg MPA compared to the GnRH antagonist protocol in an egg donation programme. Furthermore, in the studies published to date (now >2600 women), there were no increased malformations among the children. In the protocols, the progestins were started on the third day of the cycle at the same time as the gonadotrophins (Fig. 2). It should be noted that an approx. 25 IE higher gonadotrophin dose/dose must be administered to obtain the same number of oocytes and the stimulation takes about 1 day longer (corresponding to luteal phase stimulation). When using MPA and dydrogesterone, the physiological production of progesterone in serum can be demonstrated, whereas this is not the case for oral micronized progesterone. The use of gestagens for ovulation suppression is also conceivable in principle with “random-start” protocols, but their efficiency has yet to be proven.

Progesterone-primed ovarian stimulation (PPOS)
Double Stimulation
Double stimulation allows an increase in the number of oocytes obtained within approximately 4 weeks [5, 7, 23] (Fig. 3). Most double stimulations are “poor responders”, but they have also been described occasionally in the context of fertility preservation. The similar stimulation protocols all resulted in a higher number of mature oocytes the second stimulation with good developmental quality (summarised in [6, 18]).

Double stimulation
With this method, stimulation with a classical antagonist protocol and follicle aspiration is performed first after ovulation induction with a GnRHa. It can be assumed that the first stimulation can also be started in every cycle phase (random start stimulation). A second stimulation is started 2–5 days after follicular puncture according to the luteal phase stimulation described above [23]. A prerequisite is that the ovary does not have too many large follicles (whether the administration of GnRHant for 2 days after follicle puncture accelerates luteolysis has not yet been proven). To rule out premature ovulation, GnRHant are administered additionally as soon as the new dominant follicle exceeds a size of 13 mm [7] (Fig. 3). Double stimulation takes approximately 30 days.
Reduction of Estradiol Concentration in Hormone Receptor Positive Tumours
Hormone-receptor-positive tumours, in particular hormone receptor-positive breast cancer, represent a special case, since their growth could at least theoretically be increased by supraphysiological estrogen concentrations.
To reduce the increasing estrogen concentrations during ovarian stimulation, the addition of aromatase inhibitors, e.g. letrozole 5 mg (2.5 mg each morning and evening from the first day of stimulation), is recommended for ovarian stimulation in hormone receptor-positive patients [14]. Since letrozole is not approved for use in ovarian stimulation, treatment is off-label. Previous studies have not shown increased malformation rates in children after stimulation with letrozole [24, 25]. The number of oocytes [26] and the pregnancy rates described so far [14, 27] are also unaffected by the addition of letrozole. A more recent study of egg cell quality after letrozole stimulation and an ovulation trigger with GnRHa showed good egg cell quality based on an analysis of gene expression of granulosa cells and local estrogen concentration in the follicular fluid [28]. Oktay et al. [29] recommended that ovulation should only be triggered when the follicle size reaches 20 mm.
It should be noted that stimulation of a hormone receptor-positive patient should only take place after consultation with the responsible oncologists.
Combination of Ovarian Stimulation with the Removal of Ovarian Tissue
Ovarian stimulation can be combined with cryopreservation of ovarian tissue to increase the chance of success in treatments with high gonadotoxicity (Fig. 4) [7, 8]. Ovarian stimulation begins approximately 2 days after the laparoscopic removal of 50% of an ovary. In addition, a GnRHa depot injection could be given for fertility preservation on the day of follicular puncture. According to the studies carried out so far, there is no increased risk of complications. The number of oocytes obtained is not reduced after the removal of ovarian tissue. The time required for the combination of both therapies is approximately 2.5 weeks.

Combination of ovarian stimulation with the removal of ovarian tissue and the administration of a GnRHa
References
von Wolff M, Dittrich R, Liebenthron J, Nawroth F, Schüring AN, Bruckner T, Germeyer A. Fertility-preservation counselling and treatment for medical reasons: data from a multinational network of over 5.000 women. Reprod Biomed Online. 2015;31:605–12.
von Wolff M, Thaler CJ, Frambach T, Zeeb C, Lawrenz B, Popovici RM, Strowitzki T. Ovarian stimulation to cryopreserve fertilized oocytes in cancer patients can be started in the luteal phase. Fertil Steril. 2009;92:1360–5.
Cakmak H, Katz A, Cedars MI, Rosen MP. Effective method for emergency fertility preservation: random-start controlled ovarian stimulation. Fertil Steril. 2013;100:1673–80.
von Wolff M, Capp E, Jauckus J, Strowitzki T, Germeyer A. Timing of ovarian stimulation in patients prior to gonadotoxic therapy – an analysis of 684 stimulations. Eur J Obstet Gynecol Reprod Biol. 2016;199:146–9.
Moffat R, Pirtea P, Gayet V, Wolf JP, Chapron C, de Ziegler D. Dual ovarian stimulation is a new viable option for enhancing the oocyte yield when the time for assisted reproductive technology is limited. Reprod Biomed Online. 2014;29:659–61.
Zhang J. Luteal phase ovarian stimulation following oocyte retrieval: is it helpful for poor responders? Reprod Biol Endocrinol. 2015;13:76.
Turan V, Bedoschi G, Moy F, Oktay K. Safety and feasibility of performing two consecutive ovarian stimulation cycles with the use of letrozole-gonadotropin protocol for fertility preservation in breast cancer patients. Fertil Steril. 2013;100:1681–5.
Huober-Zeeb C, Lawrenz B, Popovici RM, Strowitzki T, Germeyer A, Stute P, von Wolff M. Improving fertility preservation in cancer: ovarian tissue cryobanking followed by ovarian stimulation can be efficiently combined. Fertil Steril. 2011;95:342–4.
Dolmans MM, Marotta ML, Pirard C, Donnez J, Donnez O. Ovarian tissue cryopreservation followed by controlled ovarian stimulation and pick-up of mature oocytes does not impair the number or quality of retrieved oocytes. J Ovarian Res. 2014;7:80.
Turan V, Quinn MM, Dayioglu N, Rosen MP, Oktay K. The impact of malignancy on response to ovarian stimulation for fertility preservation: a meta-analysis. Fertil Steril. 2018;110:1347–55.
von Wolff M, Bruckner T, Strowitzki T, Germeyer A. Fertility preservation: ovarian response to freeze oocytes is not affected by different malignant diseases - an analysis of 992 stimulations. J Assist Reprod Genet. 2018;35:1713–9.
Rienzi L, Romano S, Albricci L, Maggiulli R, Capalbo A, Baroni E, Colamaria S, Sapienza F, Ubaldi F. Embryo development of fresh 'versus' vitrified metaphase II oocytes after ICSI: a prospective randomized sibling-oocyte study. Hum Reprod. 2010;25:66–73.
Martinez M, Rabadan S, Domingo J, Cobo A, Pellicer A, Garcia-Velasco JA. Obstetric outcome after oocyte vitrification and warming for fertility preservation in women with cancer. Reprod Biomed Online. 2014;29:722–8.
Oktay K, Turan V, Bedoschi G, Pacheco FS, Moy F. Fertility preservation success subsequent to concurrent aromatase inhibitor treatment and ovarian stimu- lation in women with breast cancer. J Clin Oncol. 2015;33:2424–9.
Lawrenz B, Jauckus J, Kupka M, Strowitzki T, von Wolff M. Efficacy and safety of ovarian stimulation before chemotherapy in 205 cases. Fertil Steril. 2010;94:2871–3.
Del Pup L, Peccatori FA. Is ovulation induction with letrozole in breast cancer patients still safe even if it could increase progesterone levels? Eur Rev Med Pharmacol Sci. 2018;22:246–9.
Youssef MA, Abdelmoty HI, Ahmed MA, Elmohamady M. GnRH agonist for final oocyte maturation in GnRH antagonist co-treated IVF/ICSI treatment cycles: systematic review and meta-analysis. J Adv Res. 2015;6:341–9.
Kuang Y, Hong Q, Chen Q, Lyu Q, Ai A, Fu Y, Shoham Z. Luteal-phase ovarian stimulation is feasible for producing competent oocytes in women undergoing in vitro fertilization/intracytoplasmic sperm injection treatment, with optimal pregnancy outcomes in frozen-thawed embryo transfer cycles. Fertil Steril. 2014;101:105–11.
Chen H, Wang Y, Lyu Q, Ai A, Fu Y, Tian H, Cai R, Hong Q, Chen Q, Shoham Z, Kuang Y. Comparison of live-birth defects after luteal-phase ovarian stimulation vs. conventional ovarian stimulation for in vitro fertilization and vitrified embryo transfer cycles. Fertil Steril. 2015;103:1194–201.
Martínez F, Clua E, Devesa M, Rodríguez I, Arroyo G, González C, Solé M, Tur R, Coroleu B, Barri PN. Comparison of starting ovarian stimulation on day 2 versus day 15 of the menstrual cycle in the same oocyte donor and pregnancy rates among the corresponding recipients of vitrified oocytes. Fertil Steril. 2014;102:1307–11.
La Marca A, Capuzzo M. Use of progestins to inhibit spontaneous ovulation during ovarian stimulation: the beginning of a new era? Reprod Biomed Online. 2019;39:321–31.
Begueria R, Garcia D, Vassena R, Rodriguez A. Medroxyprogesterone acetate versus ganirelix in oocyte donation: a randomized controlled trial. Hum Reprod. 2019;34:872–80.
Sighinolfi G, Sunkara SK, La Marca A. New strategies of ovarian stimulation based on the concept of ovarian follicular waves: from conventional to random and double stimulation. Reprod Biomed Online. 2018;37:489–97.
Sharma S, Ghosh S, Singh S, Chakravarty A, Ganesh A, Rajani S, Chakravarty BN. Congenital malformations among babies born following letrozole or clomiphene for infertility treatment. PLoS One. 2014;9:e108219.
Kim J, Turan V, Oktay K. Long-term safety of letrozole and gonadotropin stimulation for fertility preservation in women with breast cancer. J Clin Endocrinol Metab. 2016;101:1364–71.
Pereira N, Hancock K, Cordeiro CN, Lekovich JP, Schattman GL, Rosenwaks Z. Comparison of ovarian stimulation response in patients with breast cancer undergoing ovarian stimulation with letrozole and gonadotropins to patients undergoing ovarian stimulation with gonadotropins alone for elective cryopreservation of oocytes. Gynecol Endocrinol. 2016;32:823–6.
Haas J, Bassil R, Meriano J, Samara N, Barzilay E, Gonen N, Casper RF. Does daily co-administration of letrozole and gonadotropins during ovarian stimulation improve IVF outcome? Reprod Biol Endocrinol. 2017;15:70.
Goldrat O, Van Den Steen G, Gonzalez-Merino E, Dechène J, Gervy C, Delbaere A, Devreker F, De Maertelaer V, Demeestere I. Letrozole-associated controlled ovarian hyperstimulation in breast cancer patients versus conventional controlled ovarian hyperstimulation in infertile patients: assessment of oocyte quality related biomarkers. Reprod Biol Endocrinol. 2019;17:3.
Oktay K, Hourvitz A, Sahin G, Oktem O, Safro B, Cil A, Bang H. Letrozole reduces estrogen and gonadotropin exposure in women with breast cancer undergoing ovarian stimulation before chemotherapy. J Clin Endocrinol Metab. 2006;91:3885–90.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Germeyer, A., von Wolff, M. (2020). Ovarian Stimulation to Collect Oocytes. In: von Wolff, M., Nawroth, F. (eds) Fertility Preservation in Oncological and Non-Oncological Diseases. Springer, Cham. https://doi.org/10.1007/978-3-030-47568-0_19
Download citation
DOI: https://doi.org/10.1007/978-3-030-47568-0_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-47567-3
Online ISBN: 978-3-030-47568-0
eBook Packages: MedicineMedicine (R0)