
Abstract
Tumor vascularization refers to the formation of new blood vessels within a tumor and is considered one of the hallmarks of cancer. Tumor vessels supply the tumor with oxygen and nutrients, required to sustain tumor growth and progression, and provide a gateway for tumor metastasis through the blood or lymphatic vasculature. Blood vessels display an angiocrine capacity of supporting the survival and proliferation of tumor cells through the production of growth factors and cytokines. Although tumor vasculature plays an essential role in sustaining tumor growth, it represents at the same time an essential way to deliver drugs and immune cells to the tumor. However, tumor vasculature exhibits many morphological and functional abnormalities, thus resulting in the formation of hypoxic areas within tumors, believed to represent a mechanism to maintain tumor cells in an invasive state.
Tumors are vascularized through a variety of modalities, mainly represented by angiogenesis, where VEGF and other members of the VEGF family play a key role. This has represented the basis for the development of anti-VEGF blocking agents and their use in cancer therapy: however, these agents failed to induce significant therapeutic effects.
Much less is known about the cellular origin of vessel network in tumors. Various cell types may contribute to tumor vasculature in different tumors or in the same tumor, such as mature endothelial cells, endothelial progenitor cells (EPCs), or the same tumor cells through a process of transdifferentiation. Early studies have suggested a role for bone marrow-derived EPCs; these cells do not are true EPCs but myeloid progenitors differentiating into monocytic cells, exerting a proangiogenic effect through a paracrine mechanism. More recent studies have shown the existence of tissue-resident endothelial vascular progenitors (EVPs) present at the level of vessel endothelium and their possible involvement as cells of origin of tumor vasculature.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Cancer
- Tumor microenvironment
- Tumor progression
- Metastasis
- Tumor vasculature
- Angiogenesis
- Vasculogenesis
- Vascular mimicry
- Hypoxia
- Vascular endothelial growth factor
- Cancer therapy
- Angiogenic agents
- Antiangiogenic agents
- Endothelial progenitors
- Endothelium
- Vessel wall
7.1 Endothelial Progenitors and Tumor Angiogenesis
The blood vasculature is a closed circulatory system that is formed by arteries, veins, and capillaries; the inner layer of these vessels is formed by a single layer of endothelial cells. The physiological role of endothelial cells is not limited to the creation of a barrier between blood and tissues but is related also to the control of organ growth, regeneration, and stem cell niche. Furthermore, growing evidences indicate that endothelial cells are specialized according to the specific needs of the tissues that they supply, showing distinct barrier properties, angiogenic potential, and metabolic rate, all necessary to support specific organ functions [107].
The vascular system derives from the differentiation of mesodermal stem cells into angioblasts, embryonic endothelial progenitors. The vascular system first appears in the embryo as a highly branched network formed by primitive vessels composed by endothelial cells [25]. Embryonic endothelial cells acquire then an identity as arterial, venous, lymphatic, or hemogenic and then further specialize in an organotypic-dependent manner. The hemogenic endothelium is essential for the generation of the primitive and definitive hematopoietic system [17, 124].
Endothelial progenitor cells (EPCs) are present in adult life. Two types of EPCs have been reported: one of non-hematopoietic origin, called endothelial colony-forming cell (ECFC) able to generate true endothelial cells, resident in vessel wall but present also at very low levels in the peripheral blood and directly participating to the regeneration of endothelium following injury or ischemic damage [73], and another of hematopoietic origin, called myeloid angiogenic cells (MACs), resident in the bone marrow, generating monocytic cells supporting angiogenesis through paracrine mechanisms [10]. Growing evidences suggest that ECFCs may play a key role in reparative processes. ECFCs display a hierarchy of clonal proliferative potential and in experimental models display a pronounced postnatal vascularization ability in vivo (Table 7.1). Because of these properties, ECFCs represent a promising cell source for revascularization of damaged tissue. ECFCs are detectable in peripheral blood and were enriched in the cell fraction CD34+/CD133−/CD146+; however, these cells are not generated by the bone marrow.Therefore, ECFCs are not detected in the bone marrow, and CD34+/CD133−/CD146+ cells present in this tissue fail to generate ECFCs [171] (Table 7.1).
Emerging evidence supports the existence of specific endothelial cells with stem cell properties within blood vessels in the postnatal period. These cells exhibit the properties described for ECFCs and are present in the endothelium of vessels in a quiescent state: in response to injury, these quiescent endothelial stem/progenitor cells are activated and undergo a vasculogenic process [111, 180]. There are some remarkable differences between ECFCs and mature endothelial cells. Interestingly, a recent study showed that ECFCs possess a high sprouting activity, a property related to angiogenesis [164]. In fact, Sturtzel and coworkers showed that the forkhead box transcription factor (FOXF1) is selectively expressed in ECFCs compared to mature endothelial cells; FOXF1 expression had a strong impact on the sprouting capabilities of endothelial progenitor cells, as supported by the observation that FOXF1 overexpression in endothelial cells induces the expression of NOTCH2 receptors and induces sprouting [164]. Thus, this study supports a key role for endothelial progenitors as the mediators of both vasculogenic and angiogenic processes. A second recent study further supports the capacity of ECFCs to promote angiogenic sprouting, related to the synthesis and release of Cytokine-Like 1 (CYTL1): this proangiogenic factor is induced by hypoxia and promotes in both ECFCs and mature endothelial cells angiogenic sprouting [151]. Furthermore, CYTL1 promotes vessel formation in animal models comparable to VEGF-A [151]. Thus, these recent studies support a possible role of endothelial progenitor cells not only as promoters of vasculogenesis but also as mediators of angiogenic processes.
Endothelial cells are heterogeneous, and significant differences have been detected between arteries and veins, large and small vessels, and different microvascular beds in various organs. However, at the moment, it is largely unknown how each organ determines the specialization and functional properties of its endothelium. Intrinsic and microenvironmental mechanisms contribute to human endothelial cell heterogeneity. A better understanding of the cellular and molecular mechanisms underlying endothelial heterogeneity is of fundamental importance.
The discovery of EPCs, their purification and expansion in vitro opened the way to potential clinical applications for the use of these cells in clinical applications for the regeneration of damaged or injured endothelium and for the understanding of angiogenic mechanisms underlying various pathological conditions, such as tumors.
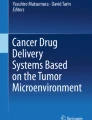
The mechanisms involved in tumor vessel generation are heterogeneous and imply different biological processes occurring in different tumors or in the same tumor (Fig. 7.1 and Table 7.1). The basic mechanisms of tumor vessel generation involve vasculogenesis and sprouting angiogenesis (Fig. 7.1 and Table 7.2). Vasculogenesis is a process that implies the de novo formation of blood vessel as a consequence of endothelial progenitor cell differentiation and represents the process of vessel generation during initial stages of embryonic and fetal development; sprouting angiogenesis implies the generation of new vessels from preexisting blood vessels. Vasculogenesis revquires the recruitment of EPCs in the tumor microenvironment, orchestrating their differentiation into mature endothelial cells and the generation of new vessels. Angiogenesis by vessel sprouting includes the specification of endothelial cells into tip and stalk cells, orchestrated by a variety of physical, chemical, and biological mechanisms [33], with a key role played by VEGF [9] and NOTCH signaling pathways; endothelial cells present at the vascular front are induced to become tip cells and may be activated by microenvironmental stimulations promoting vascular sprouting. In addition to these more commonly adopted mechanisms for new blood vessel generation by tumor cells, two additional mechanisms were observed in tumors: vascular mimicry and intussusception (Fig. 7.1 and Table 7.2). Vasculogenic mimicry implies the biological process adopted by some cancer cells with an aggressive phenotype to generate vascular-like structures without the presence of endothelial cells: in this process, tumor cells line tumor vessels and thus contribute to the formation of vessel-like structures (Fig. 7.1 and Table 7.2) [56]. Vascular intussusception or intussusceptive microvascular growth was defined as a process of intravascular growth consisting in the splitting of a preexisting vessel into two new vascular structures. Intussusceptive microvascular growth was reported in some tumors, including mammary, colorectal, and melanoma tumors [201].

Schematic representation of different patterns of tumor vasculature
Vascular co-option does not imply new vessel formation and is the process of taking over or incorporating the existing vasculature by developing tumor cells
Angiogenesis: new blood vessels branch out of preexisting ones via a process called angiogenesis. The formation of new vascular wall is a multistep process involving the migration of tip endothelial that with their extension creeps into the connective tissue and then the proliferation and subsequent migration of cells at the base (stalk endothelial cells)
Vasculogenesis : new blood vessel formation due to the proliferation and differentiation of vessel wall-resident endothelial progenitor cells (endothelial vascular progenitors)
Vascular mimicry is a process in which tumor cells create their own vessels without or in cooperation with endothelial cells, assuming the role and the properties of endothelial-like cells
In addition to the abovementioned mechanisms, there is now growing evidence that tumors can grow also through a mechanisms by which tumor cells infiltrate normal tissue, exploiting existing vessels to sustain their growth: this mechanism is known as vascular co-option and implies that in these nonangiogenic tumors, no new vessels are seen [42]. Only a minority of tumors grow in a purely nonangiogenic manner, while many tumors contain a mixture of angiogenic and nonangiogenic areas [42]. Both angiogenic and nonangiogenic areas have been commonly seen in primary and secondary lung tumors [20] and in breast cancer liver metastases [54]. Experimental and computational analyses of the dynamics of vessel co-option during tumor progression and in response to antiangiogenic treatment in gliomas and brain metastases provided evidence that vessel co-option is a mechanism of antiangiogenic resistance and that tumor progression can be efficiently blocked only by therapies inhibiting both angiogenesis and co-option [179].
Tumor progression from a benign to a malignant condition is usually associated with an angiogenic switch, characterized by the development of a vascular network actively growing and displaying infiltrative properties [39]. The pattern of vascularization is highly variable in various tumors, depending on the tumor type, grade and stage, the anatomical location, and the microenvironment composition and distribution of proangiogenic and antiangiogenic growth factors [39].
Tumor vessel formation involves the formation of highly disorganized vessel networks, morphologically and functionally abnormal [26]. Tumor vasculature displays numerous abnormalities, being tortuous, irregular, and nonhomogeneous and characterized by weak junctions between endothelial cells, resulting in augmented leakiness facilitating extravasation of cancer cells [76]. Tumor neovascularization plays an essential role in tumor biology by promoting tumor growth, metastasis, and resistance to chemotherapy. The proximity of cancer cells to blood vessels within a tumor is a major determinant of tumor phenotypic and metabolic diversification [90]. Furthermore, endothelial cells adapt to the tumor microenvironment and display a hyper-glycolytic metabolism, shunting glycolytic intermediates to nucleotide synthesis [27].
Tumor-associated endothelial cells not only provide oxygen and nutrient supply to tumors but regulate also tumor aggressiveness, converting naïve tumor cells to chemoresistant tumor cells with stemlike properties [22]. The blocking of the interactions between tumor cells and endothelial cells at the level of perivascular tumor niches may represent a strategy to bypass chemoresistance of these “protected” tumor cells [24].
The mechanisms driving tumor angiogenesis are heterogeneous and involve different molecular and cellular processes. The common initial driving force of tumor angiogenesis is represented by the tumor microenvironment, composed by a variety of cell types that under the influence of growth factors and cytokines activate their metabolic and functional activities and promote various types of angiogenic mechanisms, triggering an “angiogenic switch” to allow the tumor to progress [184]. Mechanical (stress relaxation) and chemical (hypoxia) properties are critical factors in tumor microenvironment driving tumor angiogenesis and tumor progression promoting tumor cell invasion and migration [93, 94]. Some of the mechanisms of tumor angiogenesis, involving the generation of new vessels by vasculogenesis, imply endothelial progenitor cells. These vasculogenic mechanisms are poorly defined, and some additional confusion is related also to the unprecise definition of endothelial progenitor cells, englobing both true endothelial progenitor cells (ECFC) generating in their differentiation an endothelial cell progeny and myeloid cell progenitor cells (myeloid angiogenic cells, MACs) generating a monocytic angiogenic cell progeny exerting an indirect proangiogenic activity through paracrine mechanisms. Thus, the tumor angiogenic mechanisms may involve the recruitment in the tumor microenvironment of either tissue-resident ECFCs or of circulating ECFCs or of bone-marrow-derived MACs. Initial studies in experimental mouse models have suggested that tumor angiogenesis requires the migration of endothelial progenitor cells from the bone marrow initially in the blood and then in the tumor microenvironment, promoting in this site tumor vascularization (reviewed in [38]). It is now evident that these studies describe the contribution of some bone marrow-derived myeloid cells to tumor angiogenesis. Subsequent studies have defined in various mouse models the specific proangiogenic role exerted by Tie-2+ monocytes/macrophages; Tie-2 inhibitors block the recruitment in the tumors of Tie-2+ monocytes and reduce tumor angiogenesis [39]. However, other studies have shown that mouse embryonic endothelial progenitor cells are able to home at the level of tumor, trapped by hypoxia-originated signals, promoting a process of active vasculogenesis [177]. This mechanism of vasculogenesis in adults was also supported by recent studies showing that tissue hypoxia through HIF-1-dependent and HIF-1-independent mechanisms promotes postnatal vasculogenesis through the recruitment of EPCs, their clusterization and integration in existing microvasculature [18].
The study of the involvement of EPCs in tumor angiogenesis is further complicated by the presence of numerous altered phenotypes of tumor endothelial cells. An example is given by the observation that tumor endothelial cells exhibit an increased aldehyde dehydrogenase (ALDH) expression: these ALDHhigh tumor endothelial cells have proangiogenic properties, express stem/progenitor cell genes (CD90, Oct-4, MDR-1), and show drug resistance [67]. High ALDH expression in some endothelial cells is induced by tumor-conditioned medium [67]. Furthermore, the heterogeneity of tumor endothelial cells between low- and high-metastatic tumors suggests in the latter ones the involvement of EPCs in the mechanisms sustaining tumor angiogenesis [122].
The study of endothelial progenitor cells in adult life remained closed within these last years within a scientific dilemma, with some studies supporting the presence and the functional contribution to reparative vascular processes of bone-marrow-derived EPCs and other studies showing that true EPCs are present in the vessel wall, do not derive from the bone marrow, and are capable of regenerating damaged vessels. A recent study was of fundamental importance to offer a reasonable explanation for this intriguing dilemma. Thus, Singhal et al. have used irradiation-based myeloablative and non-myeloablative mouse models to explore the cells responsible for vascular regeneration. The results of this study unequivocally showed that the preexisting endothelium is the source of cells capable of promoting vascular regeneration [156]. However, if endothelial cell proliferation is impaired by irradiation, myeloid cells were recruited from the bone marrow by the damaged endothelium and actively contribute to vessel wall reconstitution [156]. These findings support a model of vascularization in adults implying the cooperation between endothelial-derived and bone marrow-derived progenitors. This model must be carefully considered for its important implications for our understanding of tumor neovascularization processes.
The present paper reviews the study of tumors in which some evidences support a role for EPCs in the mechanisms underlying tumor vascularization.
7.2 Endothelial Progenitors in Melanoma
In melanoma, angiogenesis is implicated in tumor progression and metastasis, and microvessel density is an adverse prognostic factor [80]. A recent meta-analysis of all current studies on this topic shows that increased MVD in melanoma is associated with reduced DFS, but not with reduced OS [132]. More recent studies suggest that vascular proliferation index (VPI) could represent a more sensitive prognostic index to capture and to measure the expanding vasculature than the standard microvessel density evaluation [68]. The rate of intratumoral blood vessel proliferation at the level of metastatic sentinel lymph nodes was inversely associated with overall survival of melanoma patients [129]. In a recent study, Hugdahl and coworkers analyzed a large set of melanomas for MVD and VPI at the level of primary tumor sites and at the level of locoregional metastatic sites [62]. A significant impact of VPI on melanoma survival was observed; furthermore, VPI strongly correlated with high-grade characteristics of the primary tumor in terms of tumor thickness, tumor ulceration, mitotic count, and presence of necrotic areas. Interestingly, VPI was lower in locoregional metastases than in corresponding primary tumors, suggesting that activated angiogenesis is more critical for primary tumors than for metastatic tumors; in contrast, MVD was higher in metastatic sites than in primary ones [62]. A tentative explanation at least for lymph node metastases could be related to the presence in these tissues of a highly vascularized network, not requiring active neoangiogenesis to sustain tumor growth but predominantly co-option mechanisms [62]. The ensemble of these observations supports neoangiogenesis as an aggressive component of melanoma microenvironment, required to sustain tumor development and progression.
Few studies support a direct role of endothelial progenitors in tumor vascularization.
In this context, particularly relevant was a recent study by Donovan and coworkers in a model of orthoptic melanoma. Fate-mapping analysis of endothelial cell populations showed a consistent heterogeneity of endothelial cells present in the growing melanomas, characterized by the very early infiltration of endovascular progenitors in growing tumors [43]. Importantly, delivery of melanoma cells with EVP resulted in the formation of larger tumors, whereas tumor cells delivered with D (mature) endothelial cells resulted in smaller tumors [43]. In the tumoral microenvironment, EVPs reactivated the expression of SOX18 transcription factor and initiated a vasculogenic process, progressing through various stages of endothelial differentiation, including TA cells and D cells, generating mature endothelial cells with arterial, venous, and lymphatic subtypes [43]. Molecular profiling by RNA sequencing of purified endothelial cell populations supported that EVPs are quiescent progenitors: EVPs present in the tumors or in the wall of the aorta share common molecular signature [43]. Importantly, anti-VEGF-A therapy was unable to target EVP cells; in contrast, conditional ablation of NOTCH signaling alters EVP. Endothelial-specific ablation of Rbpj, a direct protein interactor of SOX18B, depleted the EVP population and strongly inhibited metastasis. These important observations support the view that EVPs are major drivers of tumor vascularization and cannot be significantly inhibited by commonly used anti-VEGF antiangiogenic agents.
This interesting study was in part based on a previous study showing that, on the basis of flow cytometry detection of common endothelial markers, three subpopulations of endothelial cells can be identified among cells characterized by expression of an endothelial marker (VE-Cadherin) and absence of a pan-hematopoietic marker (CD45) [53, 130, 131]. Lineage tracing experiments have shown that the CD31−/VEGF-R2low cell population is heterogeneous and composed by three different subpopulations: Endothelial Vascular Progenitors (EVPs), displaying a self-renewing capacity, present in a quiescent state and capable of endothelial colony forming capacity in vitro and endothelial-regenerating capacity in vivo; Transit-Amplifying (TA) and Mature (D) endothelial cells not possessing self-renewal capacity [130, 131]. Gene expression studies show a remarkable difference between EVP and TA/D cells; SOX18 is essential for differentiation of EVP cells [130, 131]. Single-cell transcriptomic studies showed the existence of crucial regulatory gene expression networks specific for EVPs, including significant metabolic gene networks, and higher mitochondrial content and activity [104].
Studies in experimental models further support a role for SOX18 in promoting tumor angiogenesis in murine melanoma models. In fact, in these murine models, SOX18 induction represents a key step in mediating melanoma lymphangiogenesis and metastasis, as supported through experiments of genetic ablation of SOX18 in these tumors [46, 47].
These observations have strongly supported the development of small molecules acting as SOX18 inhibitors and exerting a potent antiangiogenic activity on tumor vasculature [52, 125]. These observations support the clinical study of SOX18 inhibitors, although the still limited understanding of the biological effects of SOX transcription factors on endothelial cell biology suggests a great prudency in the clinical translation of SOX18 inhibition [84]. A small mechanistic trial in which SOX18 inhibition will be initiated following diagnosis of melanoma and sentinel lymph nodes collected few weeks later the start of therapy will be performed with the aim of studying changes in vascularization [69].
Other studies have shown that elevated numbers of tumor-associated macrophages (TAM) in the tumor microenvironment are often associated with poor prognosis in melanoma and these cells activated by amoeboid melanoma cells play an essential role in tumor progression through a secretory cross talk with tumor microenvironment, promoting abnormal vascularization [57]. Adrenomedullin, clearly expressed by infiltrating TAMs in human melanomas, is a key mediator of angiogenesis in these tumors [32]. Previous studies have shown that (i) adrenomedullin/cyclic AMP pathways induce NOTCH activation and differentiation of arterial endothelial cells from vascular progenitor cells [193]; (ii) adrenomedullin augments the angiogenic potential of ECFCs [66]; and (iii) adrenomedullin augments proliferation and migration of endothelial progenitor cells [186].
7.3 Endothelial Progenitors in Lung Cancer
The lung is unique for having two different sources of blood: the systemic bronchial vasculature from the aorta and the pulmonary circulation of deoxygenated blood from pulmonary artery. The pulmonary circulation has a limited angiogenic capacity and is not able alone to sustain lung tumor growth, while the bronchial circulation possesses angiogenic properties and is exploited by lung tumors. In fact, studies in murine lung cancer models have shown that although the existing pulmonary circulation can supply the nutritional and metabolic needs for initial tumor development, further growth of the tumor requires angiogenesis from the highly proliferative bronchial circulation [48]. The circulation of human lung tumors was explored by contrast-enhanced computed tomography scanning. Yuan and coworkers reached the conclusion that the bronchial circulation is dominant, and the tumor circulation was related to the tumor size [192]. Nguyen-Kim and colleagues, using a comparable methodology, confirmed that tumor perfusion was related to tumor size and to the histological subtype [119].
The essential role of angiogenesis for lung cancer growth is supported by observations in naturally occurring tumors and in experimental models of lung cancerogenesis. A recent experimental model of lung cancer tumorigenesis is initiated by lung cancer stem cell (LCSC) expansion [96]. In this model, the expansion of LCSC pool promotes angiogenesis through secretion on angiogenic growth factors, such as placental growth factor (PlGF) by LCSCs [96]. This observation supports the view that the tumor cells responsible for tumor development trigger the angiogenic switch required to sustain tumor growth.
The analysis of the pattern of vascularization of a large set of primary non-small cell lung cancers through immunostaining of endothelial cells showed four distinct patterns of tumor vascularization – basal, papillary, and diffuse – implying destruction of normal lung tissue and generation of new vessels; a fourth pattern, called alveolar, was observed in 16% of cases and is characterized by the lack of parenchymal destruction and the absence of new vessel formation and, therefore, can be considered as a nonangiogenic subtype [134]. There is consistent variation in the differentiation of tumor vasculature in lung carcinoma, as evidenced through labeling of endothelial cells for CD31 and LH39 antigens. Highly angiogenic lung carcinoma exhibits an immature endothelial phenotype, while low angiogenic lung cancers have a mature endothelial phenotype [79]. These findings were confirmed and extended by Passalidou and coworkers showing that in non-oncogenic lung cancer, endothelial cells were characterized by positivity for the late endothelial marker LH39, while in the more frequent angiogenic tumors, only a minority of vessels express LH39 [128]. The angiogenic or nonangiogenic phenotype of primary lung cancers is in large part dictated by the properties of tumor cells. Thus, nonangiogenic tumors have higher levels of genes involved in mitochondrial metabolism, mRNA transcription, protein synthesis, and the cell cycle; angiogenic tumors have higher levels of genes coding for membrane vesicles, integrins, remodeling, angiogenesis, and apoptosis [71]. A recent study on a large set of lung cancer specimens confirmed these initial observations and led to conclude that both angiogenic and nonangiogenic lung cancers are characterized by a comparable hypoxia/HIF and VEGF expression, but angiogenesis does not ensue in nonangiogenic tumors in which hypoxia triggers a metabolic mitochondrial response which allows tumor growth without triggering angiogenesis; in angiogenic tumor in which the expression of genes involved in mitochondrial metabolism is more limited, hypoxia together with tissue remodeling and inflammation triggers an angiogenic response [1].
The functional integrity and homeostasis of lung tissue is maintained by lineage-restricted stem cells [70]. Alvarez and coworkers were among the first investigators to provide evidence about the existence of vascular resident progenitor cells, able to differentiate into ECs and capable of extensive proliferative activity [6]. These endothelial progenitor cells are involved in tissue endothelial repair mechanisms: in fact, in models of lung injury induced by chronic hypoxia [120] or LPS administration [82], tissue-resident endothelial progenitors increase, became highly proliferative, and substantially contribute to pulmonary vascular repair in vivo. The analysis of LPS-treated mice showed a transient decrease of the number of pulmonary vascular endothelial cells, associated with an increase of pulmonary vascular endothelial cells undergoing a process of endothelial-to-mesenchymal transition (EndMT) [166]. Interestingly, EndMT endothelial cells expressed c-kit and CD133 and had increased vasculogenic capacity, aldehyde dehydrogenase (ALDH) activity, and expression of drug-resistant genes, all properties typically observed in progenitor cells [166].
Sekine and coworkers identified CD31+CD45−CD133+ as a rare population of vascular-resident endothelial cells exhibiting properties of endothelial progenitor cells, with consistent in vitro and in vivo angiogenic capacities; these cells are locally resident endothelial progenitor cells expressing other progenitor cell markers, such as ALDH positivity, and do not derive from the bone marrow [155]. Immunofluorescence studies indicate that this population of CD133+ endothelial progenitors is preferentially resident in the arterial vasculature at the level of large vessels [155]. CD133+ endothelial progenitors have been reported also in human pulmonary arteries [50].
C-kit+ lung endothelial cells act as endothelial progenitors under homeostatic or repair conditions, but do not contribute to lung epithelium [100]. Xu and coworkers described two types of vascular endothelial progenitors in the adult mouse lung: CD45−/CD31+/VEGFR2−/LSP (lung side population) cells corresponding to bipotent progenitors of endothelial and smooth muscle and CD45−/CD31+/VEGFR2+/LSP acting as late endothelial progenitors [188]. Lineage tracking experiments have shown that maintenance and repair of the lung endothelium does not involve contributions from bone-marrow-derived endothelial progenitor/precursor cells [123].
Alphonse and coworkers have reported that human fetal and neonatal rat lung contain ECFCs with robust proliferative capacity, secondary colony formation on replating, and de novo blood vessel formation in vivo when transplanted into immunodeficient mice [4]. These lung-resident EPCs can be isolated by enzymatic dispersion of human lung samples by enzymatic tissue digestion and selection of CD31-positive cells by magnetic-activated cell sorting and plating in vitro in endothelial-specific conditions [5].
Vessel wall endothelial progenitor cells were identified on the basis of their capacity to efflux Hoechst 33342 dye, a property displayed by many stem cell populations [116]. Because of this property, these cells have been termed side population (SP) cells for their typical appearance in flow cytometry, being identified as a cell subpopulation at the side of main population (MP) cells [116]. These cells, called EC-SP, have the capacity to form in vitro colonies of endothelial cells and display in vivo potent angiogenic activity when assayed by transplantation in an ischemic limb [116]. These EC-SP cells were clearly detected in the lung vasculature and give a major contribution to new blood vessels in lung tumors [117]. These cells, whose origin is not at the level of the hematopoietic system, proliferate in lung tumors, and the frequency of this population clearly increases in the tumoral tissue, compared to normal lung tissue [117], survived to angiogenic drugs, and remained in the tumor tissue [117]. Other evidences in favor of a possible role of endothelial progenitor cells in mediating angiogenic mechanisms derive from the study of a KRAS-driven mouse model of lung cancer in which endothelial expression of the microRNAs (miRNAs) miR-143/145 promoted angiogenesis-induced tumor growth [41]. miR-143/145 were expressed at the level of a minor subpopulation of lung endothelial cells, seemingly endothelial progenitors [41]. miR-143/145-deficient mice displayed a reduced endothelial proliferation and reduced endothelial tip cells [41]. Lung tumor development was more limited in miR-143/145-deficient mice, where the tumors exploit co-option mechanisms of the normal lung vasculature, compared to WT mice exploiting neoangiogenic mechanisms to sustain lung tumor growth [41]. Another study showed that the NAD-dependent protein deacetylase Sirtuin 1, a master regulator of angiogenesis, increases vessel density and stimulates the growth of Lewis lung carcinoma xenografts through a mechanism involving downregulation of delta ligand 4 (DLL4)-NOTCH signaling and deacetylation of the NOTCH1 intracellular domain in lung cancer-derived endothelial cells [187]. These effects of SIRT1 on lung tumor angiogenesis are seemingly mediated by a stimulatory effect on the angiogenic properties of endothelial progenitor cells [182].
Although these experimental models supported a key role of neoangiogenic mechanisms operating in lung cancer, studies on primary human lung cancers have provided evidence that angiogenic mechanisms are heterogeneous in these patients and a subset of patients with non-small cell lung cancer exhibit nonangiogenic growth patterns [105].
Targeting angiogenesis was a therapeutic strategy intensively explored in NSCLC, but the utility of this approach remains limited. The addition of bevacizumab (mAb anti-VEGF) to platinum-based chemotherapy in first-line setting induces a modest benefit. Some antiangiogenic therapies have been approved in the second line by the FDA (bevacizumab or ramucirumab (anti-VEGF-R2)) or by the European Union (nintedanib anti-VEGF-R1, anti-VEGF-R2, anti-VEGF-R3, PDGFRA, FGF-R1), but the extent of the improvements at the level of PFS and OS were modest and must be balanced against the expected toxicities and the cost associated with these agents. These limited clinical benefits are related to therapy-induced blood vessel alterations, with consequent increased hypoxia which can worsen the tumor microenvironment and induce treatment resistance. However, in spite of all these limitations and the existence of intrinsic mechanisms of resistance to current antiangiogenesis inhibitors of NSCLCs, combination therapies targeting multiple mechanisms fueling neovascularization could bypass resistance to standard antiangiogenic therapy. In this context, a recent study provided evidence that targeting of the proangiogenic peptide Apelin (APLN), an endogenous ligand of the G-protein-coupled cell surface receptor APLN receptor, together with a standard antiangiogenic drug, such as sunitinib, in lung adenocarcinoma models, diminished tumor growth, blood vessel density, and vessel abnormality within the tumor microenvironment and consequently hypoxia and tumor resistance [173]. Apelin levels are elevated in lung adenocarcinomas and were associated with elevated microvessel densities [16]; apelin elevation in these tumors seems to be related to the downmodulation of miR-195, directly targeting Apelin [200]. Apelin levels are heterogeneous in lung adenocarcinomas, and Apelin-high tumors have a poorer prognosis than Apelin-low tumors [200].
7.4 Endothelial Progenitor Cells in Multiple Myeloma (MM)
MM is the second most common hematologic cancer after non-Hodgkin’s lymphoma, with a higher incidence over 60 years. Bone marrow angiogenesis is a constant hallmark of MM progression and has prognostic potential. Microvessel density in the bone marrow clearly increases with disease progression from monoclonal gammopathy to smoldering gammopathy and to primary and relapsing MM [139]. The pathophysiology of MM-induced angiogenesis implies production of angiogenic cytokines both by cells of the marrow microenvironment and by tumor plasma cells [89, 174].
Several studies suggest that an increased angiogenic activity mediated by EPCs could contribute in a relevant way to the increased angiogenesis observed in MM. Thus, Vacca and coworkers provided evidence that EPCs isolated from MM patients exhibit increased angiogenic activity in vitro showing rapid capacity to form capillary networks and in vivo inducing the generation of numerous new vessels [175]. Zhang et al. reported an increased number of EPCs among peripheral endothelial cells isolated from MM patients; their number was significantly decreased following thalidomide treatments [196].
The increased number/activity of EPCs in multiple myeloma suggests that vasculogenesis may contribute to new vessel formation in this disease. A study by Moschetta and coworkers investigated the role of vasculogenesis in a mouse model of MM [115]. This study showed an early mobilization of EPCs from BM to PB, followed by recruitment at the level of MM-colonized niches; the use of EPC-defective ID1+/−, ID3−/− mice showed that MM progression is strictly dependent upon EPC trafficking, due to the supportive role of endothelial cells for the growth of MM cells [115]. Importantly, angiogenic dependency of MM occurs at early and not at late stages of MM development; in line with this finding, early targeting of EPCs with anti-VEGF-R2 antibody at early stages, but not at all late stages of disease progression, inhibited MM development [115]. This study supports the idea of inhibiting vasculogenesis at an early stage of disease (smoldering MM) in future clinical trials. Vasculogenic activity in myeloma may be supported by some growth factors present in the tumor microenvironment: (a) pleiotrophin, a developmental cytokine highly expressed in MM [30, 191], promotes transdifferentiation of monocytes into vascular endothelial-like cells and through this mechanism promotes tumor-induced vasculogenesis [31]; (b) ephrin receptor A3 (EphA3) is markedly overexpressed in MM endothelial cells and acts as a proangiogenic factor [21]; (c) NOTCH signaling, a crucial pathway for embryonic vasculogenesis [2], is increased in MM microenvironment and sustains the increased vasculogenic/angiogenic activities observed in this tumor, and its targeting resulted in a marked inhibitory effect on tumor angiogenesis [148]. Importantly, recent studies have shown that NOTCH signaling in the bone marrow microenvironment promotes EPC expansion and in vivo vasculogenic activity of EPCs [74, 85].
The treatment of multiple myeloma is a complex medical problem, related to the difficulty to completely eradicate malignant plasmocytes and their precursors. Recent developments have provided significant improvements in the treatment of these patients based on autologous bone marrow transplantation when possible or drug combinations involving the association of corticosteroids with immunomodulating agents (thalidomide, lenalidomide, pomalidomide) and either proteasome inhibitors (bortezomib, carfilzomib, or ixazomib) or monoclonal antibodies (daratumumab, anti-CD38) or histone deacetylase inhibitors (panobinostat). Interestingly, immunomodulatory agents, such as lenalidomide or thalidomide, exert many biological effects, including an antiangiogenic effect on MM and, when administered with other drugs, contribute to a significant antitumor effect [141]. One example of the clinical utility of this triplet drug combination is given by a recent study: lenalidomide plus dexamethasone and daratumumab (anti-CD38 mAb) significantly improved both PFS and OS of newly diagnosed MM patients ineligible for autologous stem cell transplantation [49].
The value of inhibiting angiogenesis in MM as a therapeutic tool is supported also by two recent studies. A phase I/II study explored evofosfamide, a hypoxia-activated prodrug without or with bortezomib in patients with relapsed/refractory MM: although the number of patients exhibiting CR and PR was not high, disease stabilization was observed in >80% of patients, resulting in a prolonged overall survival of 11.2 months [91].
Recent studies have explored the antitumor effects of melphalan-flufenamide (mel-flufen), a dipeptide prodrug of melphalan: the intracellular conversion of mel-flufen to melphalan is mediated by the enzyme aminopeptidase N [29]. Mel-flufen was more active than melphalan in inducing apoptosis of myeloma cell and in vitro and in vivo exerted a potent inhibitory effect on angiogenesis [162]. A phase I/II study (OP-104 Anchor study) is evaluating safety and efficacy of mel-flufen and dexamethasone in combination with either bortezomib or daratumumab in patients with relapsed/refractory MM, and an early analysis showed preliminary encouraging data about the antitumor efficacy, particularly in patients treated with mel-flufen and daratumumab [138]. The phase I/II study OP-106 Horizon showed that mel-flufen has promising activity in heavily pretreated refractory-stage RRMM patients, in whom the majority of available therapies have failed [144].
7.5 Endothelial Progenitor Cells in Myeloproliferative Disorders
The study of EPCs and of angiogenesis in myeloproliferative disorders is particularly important because in these tumors, the endothelial lineage could be directly involved in the neoplastic transformation and pathological endothelial cells could be directly involved in the neoplastic transformation and could contribute to tumor development promoting the formation of a pathological marrow niche. Myeloproliferative neoplasms (MPNs) are clonal hematopoietic cancers characterized, in their chronic phase, by overproduction of differentiated hematopoietic cells pertaining to one or more lineages The Philadelphia chromosome-negative are the most frequent diseases among the myeloproliferative disorders and include three different main diseases: polycythemia vera (PV), essential thrombocytopenia (RT), and myelofibrosis (MF) [118, 176]. All MPNs arise from the malignant transformation of hematopoietic stem cells (HSCs) that acquire a growth advantage over normal HSCs, leading to their expansion and generation of all myeloid-related lineages [112]. These disorders have frequent disease-related complications, mainly represented by venous and arterial thromboses, hemorrhages, and transformation to acute myeloid leukemia [176]. In MPNs, in >95% of cases, mutations that affect and drive tumor development occur in a mutually exclusive manner in one of three different genes: JAK (Janus Activating Kinase 2), CALR (calreticulin), or MPL (myeloproliferative leukemia virus, corresponding to the thrombopoietin receptor); while the JAK2V617F mutation activates three different membrane receptors (erythropoietin receptor, granulocyte colony-stimulating factor receptor, and thrombopoietin receptor), CALR or MPL mutants affect only thrombopoietin receptor activation [176]. The different consequences of these three different mutations help to understand the reasons of their different disease association: JAK2V617F is associated with PV, ET, and PMF, while CALR and MPL mutations are exclusively associated with ET and PMF.
Studies performed in the last years have supported a possible direct implication of the endothelial lineage in the pathological processes involving the development of JAK2V617F-mutated MPNs [169].
Initial studies have provided conflicting results: thus, an initial study based on the in vitro assay of endothelial progenitor cells showed that JAK2V617F mutation was detected in CFU-ECs (colonies of monocytoid proangiogenic cells), but not in E-CFCs (colonies formed by true endothelial cells) [135]. However, Sozer and coworkers reached a different conclusion through the analysis of the liver endothelial cells of patients with Budd-Chiari syndrome and JAK2V617F-positive hematopoiesis showing a positivity of the endothelial lineage for JAK2V617F mutations [160, 161]. According to these findings, it was hypothesized that JAK2V617F neoplasia may derive from a common cell of origin for both hematopoietic and endothelial cells.
Teofili and coworkers have subsequently explored this issue and have analyzed the molecular features of EC-CFCs generated from 22 MPN JAK2V617F-positive patients and showed that in 45% of cases, endothelial cells present in these colonies are positive for this disease-specific marker [168]. These findings were corroborated by two additional important observations: all patients displaying molecular abnormalities at the level of the endothelial lineage experienced thrombotic complications; endothelial cells bearing JAK2V617F mutations showed a pronounced Stat3/Stat5 activation [168]. In line with these observations, CD34+ cells isolated from JAK2V617F-positive MPN patients generate in vivo in immunodeficient mice both mutation-positive and mutation-negative endothelial cells [160, 161]. Furthermore, endothelial cells displaying JAK2V617F mutation were observed in >60% of myelofibrosis patients at the level of splenic capillaries and splenic vein [147].
Other recent studies have developed animal models to directly assess the consequences of JAK2V617F expression at the level of endothelial cells. Thus, Guadall et al. have developed an induced pluripotent stem cell strategy to compare JAK2 mutant to JAK2 wild-type endothelial cells [60]. The results of this study showed that JAK2V617F-mutant endothelial cells exhibit a pro-inflammatory and pro-thrombotic phenotype and display pro-adherent features [60]. Guy et al. have explored the role of endothelial cells that express JAK2V617F mutant through an in vitro model of endothelial cells expressing JAK2V617F and in vivo model of mice with endothelial-specific JAK2V617F expression [61]. Endothelial cells expressing JAK2V617F have a pro-adhesive phenotype associated with increased P-selectin expression and increased propensity to thrombotic events [61].
Another set of studies provided evidence that the development of myeloproliferative syndromes requires JAK2V617F expression in both HSCs and endothelial cells. Two lines of evidence support this conclusion: (a) no difference was noted between WT and JAK2V617F Lin−/Kit+ progenitor cell proliferation when cocultured on WT endothelial cells while a relative growth advantage over the corresponding WT progenitor cells when cocultured on JAK2V617F-bearing endothelial cells [97]; and (b) competitive marrow transplantation experiments provided evidence that the JAK2V617F-bearing vascular niche promotes clonal expansion of JAK2V617F HSCs but not normal HSCs [195]. Another study showed that JAK2V617F expression in the niche leads to HSC radioresistance, which could be responsible for the high frequency of disease relapse in patients undergoing allogeneic stem cell transplantation for MPNs [98].
7.6 Tumor Angiogenesis in Lymphoma
Several studies have shown an association between increased angiogenesis and more aggressive tumor behavior in different lymphoid neoplasms, including large B-cell lymphoma [23], mantle cell lymphoma [178], and follicular lymphoma [172].
Intriguingly, a study by Streubel and coworkers suggested that 15 to 85% of the microvascular endothelial cells in the B-cell lymphomas bear lymphoma-specific chromosomal translocations [163]. This observation may be explained either assuming the existence of a common lymphoid-endothelial malignant progenitor cell or of a lymphoid progenitor with a peculiar differentiation plasticity or by cell fusion or gene transfer events [163].
Among the various lymphomas, particularly interesting is the SOX11-positive mantle cell lymphoma (MCL), characterized by increased angiogenesis that could be ascribed to neoangiogenic mechanisms. MCL is an aggressive B-cell lymphoma, genetically characterized by the presence of the translocation t(11;14)(q13;q32) inducing overexpression of cyclin D1. MCLs can be subdivided according to SOX11 expression into SOX11-negative characterized by more frequent leukemic non-nodal disease, classic morphology, more frequent CD23 expression, and lower Ki67 proliferation index and SOZ11-positive, characterized by conventional nodal disease and aggressive phenotype. SOX11 is not expressed in normal B-lymphocytes, and its expression characterizes a part of MCLs, where it acts as a key transcription factor interfering with B-cell differentiation program and promoting tumor cell-microenvironment interactions that favor tumor growth [15]. Experimental studies have shown that SOX11 expression is associated with the induction of an angiogenic switch, characterized by increased expression of angiogenic-related gene expression signatures and induction of tumor vasculature [127]. Petrakis and coworkers directly analyzed primary tumors and showed that MVD was much higher in SOX11-positive MCLs than in SOX11-negative MCLs [133]. Studies in zebrafish support a key role of SOX11 as a key regulator of vascular development, particularly involved in sprouting angiogenesis during development [150].
7.7 Angiogenesis in Malignant Gliomas
Glioblastomas are the most common and aggressive brain tumors. These tumors are characterized by their resistance to chemotherapy and radiotherapy and by the abundant and abnormal vasculature. High-grade gliomas have been classified as one of the solid tumors’ most vascular, and vessel proliferation is a typical feature of glioblastomas [19]. One pathological feature that distinguishes glioblastoma multiforme from lower-grade glial tumors is represented by the presence of microvascular proliferation.
Glioblastoma is characterized by abundant and abnormal neovascularization giving rise to functionally and structurally abnormal vessels, with the generation of hypoxic, necrotic tumor regions. The mechanisms generating the neovascularization of glioblastomas are complex and multiple and certainly heterogeneous in their individual contribution from one tumor to another: (i) vascular co-option which is a mechanism operating during the early phases of glioblastoma development and implies the migration of tumor cells, forming cuffs around preexisting normal vessels, and must be considered as a strategy to increase blood flow before the development of mechanisms of adaptation of the tumor vasculature [42]; (ii) sprouting angiogenesis, consisting in the generation of capillaries from preexisting blood vessels, through a mechanism implying endothelial cell proliferation triggered by tumor hypoxia, inducing VEGF production and resulting in the development of an abnormal vascular network with dilated blood vessels, abnormal branching, arteriovenous shunts, and vascular leakiness [95]; (iii) release of angiogenic growth factors from tumor cells, particularly from glioma stem cells, with consequent stimulation of new vessel formation [13]; (iv) vasculogenesis , induced by the migration (triggered by hypoxia and VEGF) and differentiation of bone marrow endothelial progenitors (MACs) acting at the tumor sites as catalyzers of vasculogenic processes, seemingly involving local endothelial progenitors cells (Du et al. [44, 51]); the vasculogenic mechanisms are particularly active in glioblastoma recurrence after radiotherapy, where the vasculogenic response is not promoted by VEGF but by the cytokine stromal-derived factor-1 (SDF-1) [87, 167]; (v) vasculogenic mimicry, a process in which the same tumor cells form functional vessel-like networks, providing an alternate mechanism to support tumor growth, a phenomenon correlated with tumor grade, poor outcome, and aggressive phenotype [99] and triggered by growth factors released in the tumor microenvironment [101, 102]; and (vi) transdifferentiation of glioma stem cells into endothelial cells or pericytes [63].
The mechanism of glioma stem cell transdifferentiation seems to represent a peculiar mechanism of tumor oncogenesis observed in glioblastomas. Using tumor biopsies, Wang and coworkers [181] and Ricci-Vitiani and coworkers [143] identified a subset of endothelial cells lining tumor vessels, carrying the same genetic alterations, as well as malignant glioma cells. Furthermore, the CD133+ tumor population includes a subset of vascular endothelial-cadherin (CD144)-positive population showing features of endothelial progenitor cells and capable of generating mature endothelial cells [143, 181]. These tumor-derived endothelial cells comprise from 20 to 90% of the tumor vasculature, have tumor-specific genetic abnormalities, and do not respond to inhibitors of VEGF or bFGF; furthermore, these cells are preferentially localized at the level of deep hypoxic tumoral areas, thus suggesting that hypoxia is a major driver in their genesis. Mei and coworkers have reported the occurrence of tumor-derived endothelial cells in 47% of a group of 64 glioblastoma patients [113]. In the cases displaying the endothelial transdifferentiation, tumor-derived endothelial cells accounted for 14–18% of total vessels [113].
Importantly, cancer stem cells isolated from primary glioblastomas are able to transdifferentiate to endothelial cells in vitro [143, 181]. Soda et al. identified a subpopulation of endothelial cells within glioblastomas, expressing both endothelial-specific and tumor-specific markers [157]. In a more recent study, De Pascalis and coworkers showed that the fraction tumor-derived endothelial cells increased in glioblastomas recurring after radiotherapy [40]. These findings were further extended by a study of Cheng and coworkers providing evidence that glioma stem cells are able to generate also the vascular pericytes, cells normally of mesenchymal origin, which surround blood vessels; however, these authors provided strong evidence that glioma cancer stem cells do not differentiate to form endothelial cells [34]. Thus, the data of these studies are contradictory, suggesting the origin from tumor cells of either endothelial cells or of pericytes.
Golebiewska et al. have confirmed the existence within glioblastomas of an endothelial subpopulation of side cells, CD133+/CD31+ cells [58]. However, at variance with the previous studies, this CD133+/CD31+ cell population is non-tumorigenic [58].
Subsequent studies have explored the cellular and molecular mechanisms responsible for the differentiation of glioma stem cells into endothelial progenitor cells. In this context, particularly relevant was a study by Hu et al. based on a model of glioma stem cells obtained through the transformation of neural stem cells with mutant TP53 and constitutively expressing active AKT: these transformed cells exhibited an increased EC cell signaling and the augmentation of a subpopulation of CD133+/CD144+ cells [72]. Particularly, using these cells, it was shown that AKT activation upregulates WNT 5A to drive glioma-like EC differentiation of GSCs [72], resulting in the development of tumor invasive growth properties. Interestingly, clinical data showed higher glioma-specific endothelial and WNT5A expression in peritumoral and recurrent glioblastomas than in matched intratumoral and primary glioblastomas, respectively [72].
Other studies have shown that the adenosine A3 receptor is a regulator of the differentiation of glioma stem cells to endothelial cells under hypoxic conditions [146]. β1,4-Galactosyltransferase (β1,4GalTV) is highly expressed in glioma cells and contributes to the increased expression of highly branched N-glycans observed in these tumor cells; β1,4GalTV stimulates transdifferentiation of glioma stemlike cells into endothelial cells by activation of NOTCH1 signaling [37]. Finally, ETSA-variant 2 (ETV2), a master regulator of endothelial cell development, induces in glioma stem cells, in a VEGFA-independent manner, the repression of proneural genes and the activation of vascular genes; in primary glioblastomas, high ETV2 expression was associated with a particularly negative prognosis [198]. Interestingly, bone morphogenetic protein 9 (BMP9) counteracts the process of glioblastoma cell transdifferentiation into tumor-derived endothelial cells, in both in vitro and in vivo xenotransplantation models [137].
Other experimental studies support a major role of glioma stem cells in monitoring and regulating the angiogenic response of glioblastoma. Oligodendrocyte precursors (OPCs) expressing OLIG2, present at the level of the subventricular zone, can serve as the tumor progenitors of high-grade gliomas, including glioblastoma [92]. Using an experimental model of EGFRvIII-driven, TP53-negative murine glioma that can grow as OLIG2+ or OLIG2−, Griveau et al. have shown that (i) OLIG2+ gliomas grow by invasion of the parenchyma by single-cell vessel co-option and (ii) OLIG2− gliomas grow as perivascular clusters, leading to disruption of the blood-brain barrier and innate immune cell activation [59]. Importantly, WNT7 expression in OLIG2+ cells is required for vessel co-option, and WNT inhibition enhances the response to temozolomide therapy [59].
Glioblastoma tumor cells, including the stemlike cell population, invade into the brain parenchyma, engaging a migration along blood vessels. The interaction between glioma cancer stem cells and endothelial cells at the level of tumor perivascular niches is of fundamental importance for the promotion of tumor invasion and for new vessel formation, two properties that strictly intertwined [77, 194].
Therapy with currently used antiangiogenic agents blocking VEGF-A is used in the treatment of high-grade gliomas but is of limited benefit. A meta-analysis of randomized controlled trials showed that bevacizumab when combined with chemotherapy improved PFS, but not OS; furthermore, patients treated with bevacizumab-containing therapy reported increased objective response rate, but more treatment-related adverse events [190]. The same conclusions were reached by a recent Cochrane Database of Systematic Review showing that the use of antiangiogenic therapy does not significantly improve overall survival in newly diagnosed people with glioblastoma [7]. Similarly, there is lack of evidence of a survival advantage for antiangiogenic therapy over chemotherapy in recurrent glioma [7]. The limited benefits of antiangiogenic therapy in glioblastomas are related to two different tumor-related mechanisms: resistance and indifference. The resistance mechanism implies that the tumor, after an initial response, rapidly relapses acquiring an enhanced tumor invasion capacity [28, 126] or producing alternative angiogenic growth factors [152].
Large-scale clinical trials have shown the incapacity of bevacizumab, an anti-VEGFA monoclonal antibody, to significantly improve overall survival of high-grade glioma patients. However, in spite of the absence of benefit related to anti-VEGFA blocking therapy, glioma patients can be subdivided into a nonresponder and a responder group, the responders being characterized by a transient clinical benefit. This differential response to anti-VEGFA blocking therapy implies the existence of a heterogeneity of the mechanisms underlying tumor angiogenesis in glioblastomas. A recent study suggested that this heterogeneity could be related to the heterogeneity of the expression of SOX17 at the level of high-grade glioma tumor vessels: high Sox17 expression correlated with poor survival, early recurrence, and abnormal tumor vessels (Kim et al. [86]).
Currently, there are only two drugs approved for systemic treatment of glioblastoma: temozolomide, approved for the treatment of newly diagnosed glioblastoma, and bevacizumab, approved for the treatment of recurrent glioblastoma. Few studies have explored the effect of these two drugs on the aberrant neovascularization pattern of glioblastoma. In this context, particularly interesting was a study carried out by Xue et al. showing in an orthoptic mouse model transplanted with human glioblastoma cells that an increase in vascular mimicry was observed after bevacizumab administration, while an increased microvessel density was observed after temozolomide administration [189]. Similar conclusions were reached by Obad and coworkers exploring the morphology and the function of tumor vessels in two human glioblastoma xenografts treated with bevacizumab, as investigated by emission tomography; the results of this study provided evidence that bevacizumab normalized vascular morphology in the period time investigated but failed to improve vascular function [121].
These studies clearly indicate the limitations of drugs, such as bevacizumab, as therapeutically efficacious agents for glioblastoma treatment. Even the exploration of new antiangiogenic treatments was at the moment unsuccessful. Thus, angiopoietin 1 and angiopoietin 2 inhibition with blocking peptidobody Trebananib was ineffective as monotherapy and failed to enhance the ability of VEGF blockade to improve the outcomes of patients with recurrent glioblastoma [140]. Recent data from a phase II trial involving patients with relapsed glioblastoma following chemoradiotherapy showed a slight but significant superiority of the antiangiogenic tyrosine-multikinase inhibitor regorafenib over lomustine chemotherapy, with an improvement of median overall survival from 5.6 months with lomustine to 7.6 months with regorafenib (Lombardi et al. [103]). These findings, if confirmed in future clinical trials, support the identification of a new antiangiogenic drug active in relapsing glioblastoma patients.
Apelin (APLN) is an endogenous peptide ligand for the G protein-coupled receptor APJ/AGTRL1/APLNR and is widely expressed throughout the human body. ELABELA was identified as a second endogenous APLNR ligand. APLN and ELABELA represent a double spatiotemporal system to control APLNR signaling. APLN acts as a proangiogenic peptide during embryonic development playing an essential role in promoting the migration of embryonic angioblasts, expressing APLNR, to midline under the stimulation of ELABELA and, through this mechanism, exerts an essential role in the control of vasculogenesis [65]. APLN was identified by mass spectrometry as one molecule present in endothelial secretome and found expressed in glioblastoma specimens in close proximity to blood vessels [64]. APLN was shown to be essential for the survival and expansion of glioma stem cells, as supported by experiments with specific inhibitors of APLNR signaling [64]. Mastrella and coworkers showed that APLN is selectively expressed in glioblastoma, compared to normal brain tissue; furthermore, APLN expression was decreased by anti-VEGF therapy, but tumor invasion was increased [109]. In glioblastoma xenotransplantation models, APLN and APLNR upregulation occurred in association with angiogenic switch [109]. Using a mutant form of the natural APLN peptide (APELIN-F13A), a reduction in both angiogenesis and tumor invasiveness and a potentiation of the efficacy on anti-VEGF therapy were shown [109]. These observations support a potential role of targeting of APLNR as a strategy to overcome resistance to VEGF blockade in glioblastoma. Finally, a recent study showed the abundant expression in high-grade gliomas of the poorly characterized APELIN early ligand A (APELA): high APELA expression was associated with poor patient survival and correlates with glioma grade [55]. APLN targeting could represent, used alone or in combination with anti-VEGF therapy, as a potentially new interesting approach in glioblastoma treatment. However, many questions remain to be carefully explored, as pointed out by Amoozgar et al. [8]. First, it remains to be explored the efficacy of APLN targeting on vascular function and vasogenic edema in glioblastoma patients. Second, it remains completely to be explored the possible effect of APLN targeting on the immunosuppressive microenvironment of glioblastoma. This point is justified by previous studies showing that in experimental tumor models the normalization of tumor vasculature induced by APLN targeting improves the efficiency of antitumor immune therapy [83]. On the other hand, studies on the mechanisms of resistance of cancer patients to anti-PD-1 immune check inhibitors showed the presence of APLNR mutations with consequent loss of function: restoration of APLNR function through JAK/STAT1 signaling is essential for IFNγ-mediated antitumor responses, including T-cell trafficking through tumor vasculature [130, 131].
The possible improvements of response of glioblastoma tumors to immunotherapy with immune check inhibitors are particularly important because the clinical efficacy of PD-1/PD-L1 blockers in glioblastoma is not significant and the combination of anti-PD-1 agents with bevacizumab did not show better efficacy over bevacizumab alone [183]. The recent demonstration in recurrent glioblastoma patients that neoadjuvant anti-PD-L1 treatment with continued therapy after surgery improved patient survival compared to patients receiving adjuvant, postsurgical PD-1 blockade alone [35], supports future studies aiming to improve immunotherapy response through a vascular normalization and a consequent better trafficking of immune effectors.
The large majority of studies on glioblastomas, as well as in other tumors, were based on the idea to target endothelial cells as a tool to inhibit or normalize tumor-associated vasculature; an alternative cell target could be represented by pericytes. Pericytes are multipotent perivascular cells playing a key role within the glioblastoma microenvironment to support tumors during all their stages of development [149]. The biological role of pericytes in the regulation of blood-brain barrier permeability and in promoting angiogenesis and tumor growth represents a strong support for their therapeutic targeting. Furthermore, a recent study showed that a glioblastoma subtype, characterized by the presence of isocitrate dehydrogenase 1 mutations, is associated with a reduced pericyte coverage, seemingly related to the downmodulation of several angiogenic growth factors [165]. The blood-tumor barrier is major obstacle for drug delivery to malignant brain tumors; eliminating the blood-tumor barrier by targeting of glioma stem cell-derived pericytes though inhibition of the BMX kinase with Ibrutinib consistently enhanced the chemotherapeutic efficacy of drugs with poor blood-tumor barrier penetration [199].
7.8 CD276: A Target of Both Tumor Cells and Tumor Vasculature
In 2007, Seaman and coworkers have made a fundamental observation in the context of a study aiming to identify genes whose pattern of expression allows to distinguish physiological and pathological angiogenesis: CD276 (also known as B7-H3) was the most differentially expressed cell surface tumor-specific endothelial marker identified in this study [153]. CD276 is a member of the B7 family of immunoregulatory molecules whose expression can be induced on T, B, and dendritic cells activated by different types of inflammatory cytokines. This first study showed CD276 expression on the tumor vasculature in colon, lung, breast, esophageal, and bladder cancers; CD276 expression was observed also on tumor cells [153].
Various clinical studies have shown the impact of CD276 expression on tumor vasculature for many cancers. Thus, tumor cell and tumor vasculature expression of CD276, observed in 46% of tumor specimens, predicts survival in clear cell renal cell carcinoma [36]. These findings were confirmed by a study on metastatic clear cell renal cell carcinoma patients undergoing cytoreductive nephrectomy and interferon (IFN) treatment, showing that patients with B7-H3 expression levels ≤16% were associated with an improved OS, while those with high B7-H3 expression had a poor survival [114]. The large majority of ovarian cancers express CD276 at the level of tumor cells; CD276 was also expressed in the endothelium of tumor vasculature in 44% of patients, largely pertaining to late-stage high-grade serous tumors (Zhang et al. [197]). Tumors with CD276-positive tumor vasculature display a reduced OS and a higher incidence of recurrence (Zhang et al. [197]). In Merkel cell carcinoma, an aggressive cutaneous malignancy whose pathogenesis and prognosis are related to the integrity of the host immune system, CD276 expression is colocalized with CD31, indicating a localization at the level of tumor vasculature: positivity for CD276 correlates with aggressive clinicopathological parameters and predicts a poor prognosis [11].
Given the pattern of expression of CD276 in many tumors, CD276 is also a promising ultrasound molecular imaging target. In this context, studies carried out in breast tumors showed that antibodies anti-CD276 conjugated with indocyanine green (ICG) allowed the imaging of prostate cancers, with labeling of both tumor neovasculature and tumor tissue, sparing the normal mammary tissue or benign neoplastic lesions [12, 185].
The expression of CD276 at the level of both tumor cells and tumor vasculature offers the unique opportunity through the targeting of this molecule to destroy both tumor cells and their associated vasculature. Thus, Seaman and coworkers have shown that a monoclonal antibody reacting with both human and mouse CD276 conjugated with pyrrolobenzodiazepine injected in mouse transplanted with human tumors destroys both tumor cells and tumor vasculature, resulting in tumor eradication [154]. The type of drug conjugated with anti-CD276 is important because some drugs are unable to kill tumor-associated endothelial cells because these cells express high levels of the drug transporter P-glycoprotein (MDR-1). In fact, tumor endothelial cells resulted to be resistant to drugs such as monomethyl auristatin E [154]. Interestingly and importantly, CD276 was found to be expressed at the level of ECFCs, but not of MACs [158]. siRNA expression silencing experiments indicated a role for CD276 in ECFCs, showing that this protein promotes cell proliferation and migration (by targeting the extracellular matrix) but inhibits tube formation and exerts antiapoptotic, antioxidant, and antisenescence function in endothelial progenitor cells [158]. Additional experiments supported the view that CD276 stimulates endothelial progenitor cell proliferation and inhibits their angiogenic activity.
CD276 is a potentially interesting target for human cancer immunotherapy. Monoclonal antibodies anti-CD276, conjugated or not with cytotoxic drugs, are under clinical evaluation [136]. In preclinical models, CD276-specific monoclonal antibodies and antibody-drug conjugates displayed antitumor activity against CD276+ tumor cells in xenograft mouse models. Phase I clinical studies showed a good safety profile (NCT01099644, NCT02381314 and NCT02982941). A recent dose I study showed an interesting application of radiolabeled anti-CD276 mAb by convection-enhanced delivery in diffuse intrinsic pontine glioma [159].
Recent preclinical studies have shown the consistent antitumor potential of chimeric antigen receptor T cells (CAR-Ts) for targeting CD276 in solid tumors. Thus, Du and coworkers developed CAR-Ts for targeting CD276, which effectively controlled tumor cell growth in vitro and in orthoptic, metastatic, and patient-derived xenograft models of pancreatic cancer, ovarian cancer, and neuroblastoma [45]. Appropriate 4-1BB co-stimulation promotes lower PD-1 expression in B7-H3.CAR-Ts and superior antitumor activity when targeting tumor cells, such as pancreatic cancer, which constitutively express PD-L1 [45]. Importantly, using mAbs that cross-react with murine CD276, it was shown that B7-H3.CAR-Ts control tumor growth in syngeneic tumor model without any evident toxicity; this lack of toxicity could be related to the observation that CD276 is expressed also in many normal tissues, but at a level significantly lower than that observed in tumor cells and in tumor vasculature [45]. Another recent study provided evidence that B7-H3.CAR-Ts mediate significant antitumor activity in vivo against various pediatric tumors, including osteosarcoma, medulloblastoma, and Ewing sarcoma; the strong efficacy of CAR-Ts in these tumor models is largely related to the high surface target antigen density on tumor tissues, including tumor vasculature, with an activity diminished against target cells that express low levels of CD276 [106].
CD276 targeting offers also the opportunity to overcome the immunosuppressive effects of tumor microenvironment and to enhance anti-PD-1/PD-L1 immune checkpoint inhibitors in cancer therapy in a model of metastatic lung cancer [14].
7.9 Conclusion
An increased understanding of the mechanisms of vessel formation and their regulation in tumors is strictly necessary to the development of novel agents targeting tumor vasculature. The investigation of neovascular processes observed in various tumors indicates that the pathways to neovascularization are complex and imply various cellular and molecular mechanisms. It is still unclear which cells are at the source of newly formed vessels in tumors. Growing evidences indicate that the adult endothelium is heterogeneous and is composed by mature, transition, and progenitor endothelial cells. Evidences limited to few tumors support the view that these vascular-resident endothelial progenitors could represent the cells of origin of tumor vasculature. However, the understanding of the heterogeneity of endothelial cells is of recent acquisition, and its application to the study of tumor vasculature is very limited. Future studies are strictly required to define the implications of endothelial cell heterogeneity to the understanding of the cellular origin of vessel network in tumors.
Tumor neovascularization is a complex process involving five different, in part interlinked, pathways: vascular co-option, angiogenesis, vasculogenesis, vascular mimicry, and endothelial cell transdifferentiation. This heterogeneity is further amplified by phenomena of spatiotemporal heterogeneity, implying that tumors may utilize different mechanisms of vasculature formation in a spatially variable and temporally dynamic fashion. Angiogenesis was considered the predominant pathway and is triggered by hypoxia and by the release of hypoxia-regulated growth factors pertaining to the VEGF family. Thus, various agents targeting VEGF signaling entered clinical use, such as antibodies targeting VEGF (bevacizumab) or VEGF-R2 (ramucirumab), a VEGF trap (aflibercept), and various VEGF receptor tyrosine-kinase inhibitors (nintedanib, pazopanib, regorafenib, sorafenib, sunitinib, and vatalanib). The big hopes for the therapeutic antitumor efficacy of antiangiogenic drugs have been not fully met; these agents have shown to improve the progression-free survival and overall survival only in certain cancers, including renal cell carcinoma, colorectal carcinoma, and hepatocarcinoma; however, no improvements in overall survival have been documented in patients with brain tumors, pancreatic adenocarcinoma, prostate cancer, breast cancer, and melanoma. Furthermore, biomarkers linked to the evaluation of antiangiogenic effects, such as MVD and VEGF levels, did not adequately predict a response to antiangiogenic agents [81, 88, 142]. The reasons of tumor resistance to antiangiogenic growth factors are multiple and involve stroma-driven mechanisms of drug resistance and the production of angiogenic growth factors different from VEGF [81, 88, 142]. However, growing evidences indicate that some tumors are resistant because their tumor vasculature is not dependent upon angiogenesis, but upon nonangiogenic mechanisms such as vasculogenesis, vascular mimicry, or vascular co-option [81, 88, 142].
No clinically validated predictive biomarkers allow the identification of cancer patients who have elevated probability to respond to antiangiogenic therapies. Histopathology is probably the best approach to distinguish between the various pathways of tumor neovascularization and may represent a precious tool in future studies for stratification of patients for different types of antiangiogenic therapy.
Recent studies suggest the existence of a possible therapeutic interaction between antiangiogenic agents and cancer immunotherapy. This approach was based on the observation that the functionally aberrant tumor vasculature contributes to the immunosuppressive tumor microenvironment generating a physical barrier to T cells’ infiltration. This conclusion is supported by experimental studies showing that anti-PD-1 therapy sensitized and prolonged the efficacy of antiangiogenesis inhibitors and increased vessel normalization [3, 78, 170]. The clinical rationale of this approach is supported by recent results obtained in clear cell renal cell carcinoma (RCC). RCC is characterized by a hyperangiogenic state related to the overproduction of VEGF, as a consequence of the von Hippel-Lindau gene inactivation. VEGF signaling targeting with bevacizumab or sunitinib was effective in the majority of RCC patients; however, the development of resistance limits the impact of this therapy. A phase II and a phase III trials showed improved progression-free survival for metastatic RCC patients treated with atezolizumab (anti-PD-L1) plus bevacizumab compared to those treated with subutinib (11.2 months versus 7.7 months) [110, 145].
Although at the moment the clinical impact of antiangiogenic agents for cancer therapy is limited, there is a reasonable hope that a better understanding of the mechanisms leading to tumor vascularization; the development of drugs targeting vasculogenesis, vascular mimicry, and vascular co-option; and a better stratification of patients could consistently improve the antitumor efficacy of this therapeutic approach in the future. The development of these new antiangiogenic treatments will meet the general philosophy proposed by Jain in 2001 [75] that alleviating hypoxia at the level of the tumor through a normalization of tumor microenvironment may represent a general paradigm for improving cancer treatment using conventional (chemotherapy or radiotherapy) and novel therapy (targeted therapy or immunotherapy) [108].
References
Adighibe O, Leek RD, Fernandez-Mercado M, Hu J, Snell C, Gatter KC, Harris AL, Pezzella F (2016) Why some tumours trigger neovascularisation and others don’t: the story thus far. Chin J Cancer 35:18
Alabi RO, Farber G, Blobel CP (2018) Intriguing roles for endothelial ADAM10/Notch signaling in the development of organ-specific vascular beds. Physiol Rev 98:2025–2061
Allen E, Jabouille A, Rivera LB, Lodewijckx I, Missiaen R, Steri V, Feyen K, Trawney J, Hanahan D, Michael IP, Bergers G (2017) Combined antiangiogenic and anti-PD-L1 therapy stimulates tumor immunity through HEV formation. Sci Transl Med 9:eaak9679
Alphonse RS, Vadivel A, Fung M, Shelley WC, Critser PJ, Ionescu L, O’Reilly M, Ohls RK, McConaghy S, Eaton F, Zhong S, Yoder M, Thébaud B (2014) Existence, functional impairment, and lung repair potential of endothelial colony-forming cells in oxygen-induced arrested alveolar growth. Circulation 129:2144–2157
Alphonse RS, Vadivel A, Zhong S, McConaghy S, Ohis R, Yoder MC, Thébaud B (2015) The isolation and culture of endothelial colony-forming cells from human and rat lungs. Nat Protoc 10:16971708
Alvarez DF, Huang I, King JA, El Zarrad MK, Yoder MC, Stevens T (2008) Lung microvascular endothelium is enriched with progenitor cells that exhibit vasculogenic capacity. Am J Physiol Lung Cell Mol Physiol 294:L419–L430
Ameratunga M, Pavlakis N, Wheeler N, Grant R, Simes J, Karasaw M (2018) Anti-angiogenic therapy for high-grade glioma. Cochrane Database Syst Rev 11:CD008218
Amoozgar Z, Jain RK, Duda DG (2019) Role of apelin in glioblastoma vascularization and invasion after anti-VEGF therapy: what is the impact on the immune system? Cancer Res 79:2104–2106
Apte RS, Chen DS, Ferrara N (2019) VEGF in signaling and disease: beyond discovery and development. Cell 176:1248–1264
Asahara T, Murdrara T, Sullivan A, Silbver M, van der Zee R, Li T, Witzenbichler B, Schatteman G, Isner GM (1997) Isolation of putative progenitor endothelial cells for angiogenesis. Science 275:964–967
Aung PP, Parra ER, Barua S, Sui D, Ning J, Mino B, Ledesma DA, Curry JL, Nagarajan P, Torras-Cabala CA, Efstathion E, Hoang AG, Wong MK, Wargo JA, Lazar AJ, Rao A, Prieto VG, Wistuba I, Tetzlaff MT (2019) B7-H3 expression in Merkel cell carcinoma-associated endothelial cells correlates with locally aggressive primary tumor features and increased vascular density. Clin Cancer Res 25:3455–3467
Bachawal SV, Jensen KC, Wilson KE, Tian L, Lutz AM, Willmann JK (2015) Breast cancer detection by B7-H3-targeted ultrasound molecular imaging. Cancer res 75: 2501-2509
Bao S, Wu Q, Sathorsnusumetee S, Hao Y, Li Z, Hjelmeland AB, Shi Q, McLendon RE, Bigner DD, Rich JN (2006) Stem cell-like glioma cells promote tumor angiogenesis through vascular endothelial growth factor. Cancer Res 66:7843–7848
Bao R, Wang Y, Lai J, Zhu H, Zhao Y, Li S, Li N, Huang J, Yang Z, Wang F, Liu Z (2019) Enhancing anti-PD-1/PD-L1 immune checkpoint inhibitory cancer therapy by CD276-targeted photodynamic ablation of tumor cells and tumor vasculature. Mol Pharmacol 16:339–348
Beekman R, Amador V, Campo E (2018) SOX11, a key oncogenic factor in mantle cell lymphoma. Curr Opin Hematol 25:299–306
Berta J, Kenessey I, Dobos J, Tovari J, Klepetko W, Jan Ankersmit H, Hegedus B, Renyi-Vamos F, Varga J, Lorincz Z, Paku S, Ostoros G, Rozsas A, Timar J, Dome B (2010) Apelin expression in human non-small cell lung cancer: role in angiogenesis and prognosis. J Trorac Oncol 5:1120–1129
Blaser BW, Zon LI (2018) Making HSCs in vitro: don’t forget the hemogenic endothelium. Blood 132:1372–1378
Blatchley MR, Hall F, Wang S, Pruitt HC, Gerecht S (2019) Hypoxia and matrix viscoelasticity sequentially regulate endothelial progenitor cluster-based vasculogenesis. Sci Adv 5:eaau7518
Brem S, Cotran R, Folkman J (1972) Tumor angiogenesis: a quantitative method of histologic grading. J Natl Cancer Inst 48:347–356
Bridgeman VL, Vermeulen PB, Foo S, Bilecz A, Daley F, Kostaras E, Nathan MR, Wan E, Frentzas S, Schweiger T, Hegedus B, Hoetzenecker K, Renyi-Vamos F, Kuczynski EA (2017) Vessel co-option is common in human lung metastases and mediates resistance to anti-angiogenic therapy in preclinical lung metastasis model. J Pathol 241:362–374
Caivano A, La Rocca F, Laurenzana I, Annese T, Tamma R, Famigliari U, Simeon V, Trino S, De Luca L, Villani O, Berardi S, Basile A, Vacca A, Saglio G, Del Vecchio L, Musto P, Cilloni D (2017) Epha3 acts as proangiogenic factor in multiple myeloma. Oncotarget 8:34298–34309
Cao Z, Scandura JM, Inghirami GG, Shido K, Ding BS, Rafii S (2017) Molecular checkpoint decisions made by subverted vascular niche transform indolent tumor cells into chemoresistant cancer stem cells. Cancer Cell 31:110–126
Cardesa-Salzmann TM, Colomo L, Gutierrez G, Chan WC, Weisenburger D, Climent F, Gonzalez-Barca E, Mercadal S, Arenillas L, Serrano S, Tubbs R, Delabie J, Gascoyne RD, Connors JM, Mate JL, Rimsza L, Braziel R, Rosenwald A, Lenz G, Wright G, Jaffe ES, Staudt L, Jares P, Lopez-Guillermo A, Campo E (2011) High microvessel density determines a poor outcome in patients with diffuse large B-cell lymphoma treated with rituximab plus chemotherapy. Haematologica 96:996–1001
Carlson P, Dasgupta A, Grzelak CA, Kim J, Barrett A, Coleman IM, Shor RE, Goddard ET, Dai J, Schweitzer EM, Lim AR, Crist SB, Cherech DA, Nelson PS, Hansen KC, Ghajar CM (2019) Targeting the perivascular niche sensitizes disseminated tumour cells to chemotherapy. Nat Cell Biol 21:238–250
Carmeliet P (2005) Angiogenesis in life, disease and medicine. Nature 438:932–936
Carmeliet P, Jain RK (2011) Molecular mechanisms and clinical applications of angiogenesis. Nature 473:298–306
Centelmo AR, Conradi LC, Brajic A, Goveia J, Kalucka J, Picher A, Chaturvedi P, Hol J, Thienpont B, Teuwen LA, Schoors S, Boeckx B, Vriens J, Kuchnio A, Veys K, Cruys B, Finotto L, Trepsa L (2016) Inhibition of the glycolytic activator PFKFB3 in endothelium induces tumor vessel normalization, impairs metastasis, and improves chemotherapy. Cancer Cell 30:968–985
Chang JP, Parachoniak CA, Pandika MM, Aghi MK, Meyronet D, Isachenko N, Fouse SD, Phillips JJ, Cheresh DA (2012) VEGF inhibits tumor cell invasion and mesenchymal transition through a MET/VEGFR2 complex. Cancer Cell 22:21–35
Chauhan D, Ray A, Viktorsson K, Spira J, Paba-Prada C, Munshi N, Richardson P, Lowensohn R, Anderson KC (2013) In vitro and in vivo antitumor activity of a novel alkylating agent, melphalan-flufenamnide, against multiple myeloma cells. Clin Cancer Res 19:3019–3031
Chen H, Gordon MS, Campbell RA, Li M, Wang CS, Lee HJ, Sanchez E, Manvak SJ, Gui D, Shalitin D, Said J, Chang Y, Deuel TF, Baritaki S, Bonavida B, Berenson JR (2007) Pleiotroiphin is highly expressed by myeloma cells and promotes myeloma tumor growth. Blood 110:287–295
Chen H, Campbell RA, Chang Y, Li M, Wang CS, Li J, Sanchez E, Share M, Steinberg J, Berenson A, Shalitin D, Zeng Z, Gui D, Perez-Pinera P, Berenson RJ, Said J, Bonavida B, Deuel TF, Berenson JR (2009) Pleiotrophin produced by multiple myeloma induces transdifferentiation of monocytes into vascular endothelial cells: a novel mechanism of tumor-induced vasculogenesis. Blood 113:1992–2002
Chen P, Huang Y, Bong R, Ding Y, Song N, Wang X, Song X, Luo Y (2011) Tumor-associated macrophages promote angiogenesis and melanoma growth via adrenomedullin in a paracrine and autocrine manner. Clin Cancer Res 17:7230–7239
Chen W, Xia P, Wang H, Tu J, Liang X, Zhang X, Li L (2019) The endothelial tip-stalk cell selection and shuffling during angiogenesis. J Cell Commun Signal in Press 13(3):291–301
Cheng L, Huang Z, Zhou W, Wu Q, Donnola S, Liu JK, Fang X, Sloan AE, Mao Y, Lathia JD, Min W, McLendon RE, Rich JN, Bao S (2013) Glioblastoma stem cells generate vascular pericytes to support vessel function and tumor growth. Cell 153:139–152
Cloughesy TF, Mochizuki AY, Orpilla JR, Hugo W, Lee AH, Davidson TB, Wang AC, Ellingson BM, Ritlewski JA, Sanders CM, Kawaguchi ES, Du L, Li G, Yong WHJ, Gaffey SC, Cohen AL, Mellinghoff IK, Lee EQ, Reardon DA, O’Brien BJ, Butowski NA, Nghiemphu PL, Clarke JL, Arrillaga-Romany IC, Colmasn H, Kaleyt TJ, de Groiot JF, Liau LM, Wen PY, Prins RM (2019) Neoadjuvant anti-PD-1 immunotherapy promotes a survival benefit with intratumoral and systemic immune responses in recurrent glioblastoma. Nat Med 25:477–486
Crispen PL, Sheinin Y, Roth TJ, Lohse CM, Kuntz SM, Frigola X, Thopson RH, Boorjian SA, Dong H, Leibovich BC, Blute ML, Kwon ED (2008) Tumor cell and tumor vasculature expression of B7-H3 predict survival in clear cell renal cell carcinoma. Clin Cancer Res 14:5150–5157
Cui C, Chen X, Liu Y, Cao B, Xing Y, Liu C, Yang F, Li Y, Yang T, Hua L, Tian M, Wei Y, Gong Y, Jiang J (2018) β1,4-Galactosyltransferase V activates Notch 1 signaling in glioma stem-like cells and promotes their transdifferentiation into endothelial cells. J Biol Chem 293:2219–2230
De la Puente P, Muz B, Azab F, Azab AK (2013) Cell trafficking of endothelial progenitor cells in tumor progression. Clin Cancer Res 19:3360–3368
De Palma M, Biziato D, Petrova TV (2017) Microenvironmental regulation of tumor angiogenesis. Nat Rev Cancer 17:457–474
De Pascalis I, Morgante L, Pacioni S, D’Alessandris QG, Giannetti S, Martini M, Ricci-Vitiani L, Malinverno M, Dejana E, Larocca LM, Pallini R (2018) Endothelial trans-differentiation in glioblastoma recurring after radiotherapy. Mod Pathol 31:1361–1366
Dimitrova N, Gocheva V, Bhutkar A, Resnick R, Jong RM, Miller KM, Bendor J, Jacks T (2016) Stromal expression of miR-143/145 promotes neoangiogenesis in lung cancer development. Cancer Discov 6:188–201
Donnem T, Reynolds AR, Kuczynski EA, Gatter K, Vermeulen PB, Kerbel RS, Harris AL, Pezzella F (2018) Non-angiogenic tumours and their influence on cancer biology. Nat Rev Cancer 18:323–336
Donovan P, Patel J, Dight J, Wong HY, Sim SL, Murigneux V, Francois M, Khosrotehrani K (2019) Endovascular progenitors infiltrate melanomas and differentiate towards a variety of vascular beds promoting tumor metastasis. Nat Commun 10:18
Du R, Lu KV, Petritsch C, Liu P, Ganss R, Passegué E, Song H, Vandenberg S, Johnson RS, Werb Z, Bergers G (2002) HIF1alpha induces the recruitment of bone marrow-derived vascular modulatory cells to regulate tumor angiogenesis and invasion. Cancer Cell 13:206–220
Du H, Hirabayashi K, Ahn S, Kren NP, Montgomery SA, Wang X, Tiruthani K, Mirlekar B, Michaud D, Greene K, Herrera SG, Xu Y, Sun C, Chen Y, Ma X, Ferrone CR, Pylayeva-Gupta Y, Yeh JJ, Liu R, Savoldo B, Ferrone S, Dotti G (2019) Antitumor responses in the absence of toxicity in solid tumors by targeting B7-H3 via chimeric antigen receptor T cells. Cancer Cell 35:221–237
Duong T, Proulx ST, Luciani P, Leroux JC, Detmar M, Koopman P, Francois M (2012) Genetic ablation of SOX18 function suppresses tumor lymphangiogenesis and metastasis of melanoma in mice. Cancer Res 72:3105–3114
Duong T, Koltowska K, Pichol-Thievend C, Le Guen L, Fontaine F, Smith KA, Truong V, Skoczylas R, Stacker SA, Achen MG, Koopman P, Hogan BM, Francois M (2014) VEGFD regulates blood vascular development by modulating SOX18 activity. Blood 123:1102–1112
Eldridge L, Moldobaeva A, Zhong Q, Jenkins J, Snyder M, Brown RH, Mitzner W, Wagner EM (2016) Bronchial artery angiogenesis drives lung tumor growth. Cancer Res 76:5962–5969
Facon T, Kumar S, Plesner T, Orlowski RZ, Moreau P, Bahlis N, Basu S, Nahi H, Hulin C, Quach H, Goldschmidt H, O’Dwyver M, Perrot A, Venner CP, Weisel K, Mace JR, Raje N, Attal M, Tiab M, Macro M, Frenzel L, Leleu X, Ahmadi T, Chiu C, Wang J, Van Rampelbergh R, Uhlar CM, Kobos R, Qi M, Usmani SZ, MAIA trial investigators (2019) Duratumumab plus lenalidomide and dexamethasone for untreated myeloma. N Engl J Med 380:2104–2115
Farha S, Asossingh K, Xu W, Sharp J, George D, Comhair S, Park M, Tang WH, Loyd JE, Theil K, Tubbs R, His E, Lichtin A, Ezurum SC (2011) Hypoxia-inducible factors in human pulmonary arterial hypertension: a link to the intrinsic myeloid abnormalities. Blood 117:3485–3493
Folkins C, Shaked Y, Man S, Tang T, Lee CR, Zhu Z, Hoffman RM, Kerbel RS (2009) Glioma stem-like cells promote tumor angiogenesis and vasculogenesis via vascular endothelial growth factor and stromal-derived factor 1. Cancer Res 69:7243–7251
Fontaine F, Overman J, Moustaqil M, Mamidyala S, Salim A, Narasimhan K, Prokoph N, Robertson AAB, Lua L, Alexandrov K, Koopman P, Capon RJ, Sierecki E, Jauch R, Cooper MA, Zuegg J, Francois M (2017) Small-molecule inhibitors of the SOX18 transcription factor. Cell Chem Biol 24:346–359
Francois M, Caprini A, Hosking B, Orsenigo F, Wilhelm D, Browne C, Paavonen K, Karnezis T, Shavan R, Downer M, Davidson T, Tutt DF, Cheah KS, Stacker SA, Muscat GE, Achen MG, Dejana E, Koopmenm P (2008) SOX18 induces development of the lymphatic vasculature in mice. Nature 456:643–647
Frantzas S, Simoneau E, Bridgeman VL, Vermeulen PB, Foo S, Kostaras E, Natahan M, Wothrspoon A, Gao ZH, Shi Y, Van den Eynden G, Daley F, Peckitt C, Tan X, Salman A, Lazaris A (2016) Vessel co-option mediates resistance to anti-angiogenic therapy in liver metastases. Nat Med 22:1294–1302
Ganguly D, Cai C, Sims MM, Yang CH, Thomas M, Cheng J, Saad AG, Pfeffer LM (2019) APELA expression in glioma, and its association with patient survival and tumor grade. Pharmaceuticals 12:E45
Ge H, Luo H (2018) Overview of advances in vasculogenic mimicry-a potential target for tumor therapy. Cancer Managem Res 10:2429–2437
Georgouli M, Herraiz C, Crosas-Molist E, Fanshawe B, Maiques O, Perdrix A, Pandya P, Rodriguez-Hernandez I, Ilieva KM, Cantelli G, Karagiannis P, Mele S, Lam H, Josephs DH, Matias-Guiu X, Marti RM, Nestle FO, Orgaz JL, Malanchi I, Fruhwirth GO, Karagiannis SN, Sanz-Moreno V (2019) Regional activation of myosin II in cancer cells drives tumor progression via a secretory cross-talk with the immune microenvironment. Cell 176:757–774
Golebiewska A, Bougnaud S, Stieber D, Brons N, Vallar L, Hertel F, Klink B, Schrock E, Bjerkvig R, Nichou SP (2013) Side population in human glioblastoma is non-tumorigenic and characterizes brain endothelial cells. Brain 136:1462–1475
Griveau A, Seano G, Shelton SJ, Kupp R, Johangiri A, Obernier K, Krishnan S, Lindberg OR, Yuen TJ, Tien AC, Sabo JK, Wang N, Chen I, Kloepper J, Larrouquere L, Ghosh M, Tirosh I, Huillard E, Alvarez-Buylla A, Oldham MC, Persson AI, Weiss WA, Batchelor TT, Stemmer-Rachamimov A, Suvà ML, Phillips JJ, Aghi MK, Mehta S, Jain RK, Rowitch DH (2018) A glial signature and Wnt/7 signaling regulate glioma-vascular interactions and tumor microenvironment. Cancer Cell 33:874–889
Guadall A, Lesteven E, Letort G, Awan Toor S, Delord M, Pognant D, Brusson M, Verger E, Masiah N, Giraudier S, Larghero J, Vanneaux V, Chonmienne C, El Nemer W, Cassinat B, Kiladjian JJ (2018) Endothelial cells harbouring the JAK2V617F mutation display pro-adherent pro-thrombotic features. Thromb Hemost 118:1586–1599
Guy A, Gourdou-Latsyszenok V, Le Lay N, Peghaire C, Kilani B, Dias JV, Duplaa C, Renault MA, Denis C, Villel JL, Boulaftali Y, Jandrot-Perrus M, Couffinhal T, James C (2019) Vascular endothelial cell expression of JAK2V617F is sufficient to promote a pro-thrombotic state due to increased P-selectin expression. Haematologica 104:70–81
Hagdahl E, Bachmann IM, Schuster C, Ladstein RG, Akslen LA (2019) Prognostic value of uPAR expression and angiogenesis in primary and metastatic melanoma. PLoS One 14:e0210399
Hardee ME, Zagzagh D (2012) Mechanisms of glioma-associated neovascularization. Am J Pathol 181:1126–1141
Harford-Wright E, Andre-Gregoire G, Jacobs KA, Treps L, Le Gouidec S, Leclair HM, Gonzalez-Djest S, Roux Q, Guillonneau F, Lossouam D, Olivere L, Vallette FM, Foufelle F, Vallet P, Davenport AP, Glen RC, Bidere N, Gavard J (2017) Pharmacological targeting of apelin impairs glioblastoma growth. Brain 140:2939–2954
Helker CS, Schuemann A, Pollmann C, Chng SC, Kiefer F, Reversade B, Herzog W (2015) The hormonal peptide Elabela guides angioblast to the midline during vasculogenesis. Elife 4. https://doi.org/10.7554/seLife.06726.001
Hermansen SE, Lund T, Kaòlstad T, Ytrehus K, Myrmel T (2011) Adrenomeullin augments the angiogenic potential of late outgrowth endothelial progenitor cells. Am J Cell Physiol 300:C783–C791
Hida K, Maishi N, Akiyama K, Ohmura-Kakutani H, Torii C, Ohga N, Osawa T, Kikuchi H, Morimoto H, Shindoh M, Shinohara N, Hida Y (2017) Tumor endothelial cells with high aldehyde dehydrogenase activity show drug resistance. Cancer Sci 108:2195–2203
Hillen F, van de Winkel A, Creytens D, Vermeulen AH, Griffioen AW (2006) Proliferating endothelial cells, but not microvessel density, are a prognostic parameter in human cutaneous melanoma. Melanoma Res 16:453–457
Hindson J (2019) Targeting endovascular progenitors control cancer. Nat Rev Cancer 19:1298–1130
Hogan B, Barkauskas CE, Chapman HA, Epstein JA, Jain R, Hsia C, Niklason L, Calle E, Le A, Randell SH, Rock J, Snitow M, Krummel M, Stripp BR, Vu T, White ES, Whitsett JA, Morrisey EE (2014) Repair and regeneration of the respiratory system: complexity, plasticity, and mechanisms of lung stem cells function. Cell Stem Cell 15:123–138
Hu J, Bianchi F, Ferguson M, Cesario A, Margaritora S, Granone P, Goldstraw P, Tetlow M, Ratcliffe C, Nicholson AG, Harris A, Gatter K, Pezzella F (2005) Gene expression signature for angiogenic and nonangiogenic non-small-cell lung cancer. Oncogene 24:1212–1219
Hu B, Wang YA, Hua S, Sauvé CEG, Ong D, Lan ZD, Chang Q, Ho YW, Monasterio M, Lu X, Zhong Y, Zhang J, Deng P, Tan Z, Wang G, Liao WT, Cortey LJ, Yan H, Zhang J, You Y, Liu N, Cal L, Finocchiaro G, Phillipos JJ, Berger MS, Spring DJ, Hu J, Sulma EP, Fuller GN, Chin L, Verhaak R, DePinho RA (2016) Epigenetic activation of WNT5A drives glioblastoma stem cell differentiation and invasive growth. Cell 167:1281–1295
Ingram DA, Mead LE, Tanaka H, Meade V, Fenoglio A, Mortell K (2004) Identification of a novel hierarchy of endothelial progenitor cells using human peripheral and umbilical cord blood. Blood 104:2752–2760
Ishige-Wada M, Kwon SM, Eguchi M, Hozumi K, Iwaguro H, Matsumoto T, Fukuda N, Mugishima H, Masuda AT (2016) Jagged-1 signaling in the bone marrow microenvironment promotes endothelial progenitor cell expansion and commitment of CD133+ human cord blood cells for postnatal vasculogenesis. PLoS One 11:e0166660
Jain RK (2001) Normalizing tumor vasculature with anti-angiogenic therapy: a new paradigm for combination therapy. Nat Med 7:987–989
Jain RK (2005) Normalization of tumor vasculature: an emerging concept in antiangiogenic therapy. Science 307:58–62
Jeon HM, Kim SH, Jin X, Park JB, Kim SH, Joshi K, Nakano I, Kim H (2014) Crosstalk between glioma-initiating cells and endothelial cells drives tumor progression. Cancer Res 74:4482–4492
Johansson-Percival A, He B, Li ZJ, Kjellen A, Russell K, Li J, Larma I, Ganas R (2017) De novo induction of intratumoral lymphoid structures and vessel normalization enhances immunotherapy in resistant tumors. Nat Immunol 18:1207–1217
Kakolyris S, Gatromanoiaki A, Koukourakis M, Leigh IM, Georgoulias V, Kanavarios P, Sivridis E, Gatter KC, Harns AL (1999) Assessment of vascular maturation in non-small cell lung cancer using a novel basement membrane component, LH39: correlation with p53 and angiogenic factor expression. Cancer Res 59:5602–5607
Kashani-Sabet M, Sagebiel RW, Ferreira CM, Nosrati M, Miller JR 3d (2002) Tumor vascularity in the prognostic assessment of primary cutaneous melanoma. J Clin Oncol 20:1826–1183
Katayama Y, Uchino J, Chihara Y, Tamiya N, Kaneko Y, Yamada T, Takayama K (2019) Tumor neovascularization and developments in therapeutics. Cancers 11:316
Kawasaki T, Nishiwaki T, Sekine A, Nishimura R, Suda R, Urushibara T, Suzuki T, Takayanagi S, Terada J, Sakao S, Tatsumi K (2015) Vascular repair by tissue resident endothelial progenitor cells in endotoxin-induced lung injury. Am J Respir Cell Mol Biol 53:500–512
Kidoya H, Kunii N, Naito H, Marumatsu F, Okamoto Y, Nakayama T (2012) The apelin/APJ system induces maturation of the tumor vasculature and improves the efficiency of immune therapy. Oncogene 31:3254–3264
Kim I, Koh Y (2017) Taking aim at Sox18. Elife 6:e24238
Kim H, Huang L, Critser PJ, Yang Z, Chan RJ, Wang L, Carlesso N, Voytik-Harbin SL, Bernstein ID, Yoder MC (2015) Notch ligand delta-like 1 promotes in vivo vasculogenesis in human cord blood-derived endothelial colony forming cells. Cytotherapy 17:579–592
Kim IK, Kim K, Lee E, Oh DS, Park CS, Park S, Yang JM, Kim JH, Kim HS, Shima DT, Kim JH, Hong SH, Cho YH, Kim YH, Park JB, Koh GY, Ju YS, Lee HK, Lee S, Kim I (2018) Sox7 promotes high-grade glioma by increasing VEGFR2-mediated vascular abnormality. J Exp Med 215:963–983
Kioi M, Vogel H, Schultz G, Hoffman RM, Harsh GR, Brown JM (2010) Inhibition of vasculogenesis, but not angiogenesis, prevents the recurrence of glioblastoma after irradiation in mice. J Clin Invest 120:694–705
Kuczynski EA, Vermeulen PB, Pezzella F, Kerbel RS, Reynolds AR (2019) Vessel co-option in cancer. Nat Rev Clin Oncol in Press 16:469–493
Kumar S, Witzig TE, Timm M, Haug J, Wellik L, Kimlinger TK, Greipp PR, Rajikumar SV (2004) Bone marrow angiogenic ability and expression of angiogenic cytokines in myeloma: evidence favoring loss of marrow angiogenesis inhibitory activity with disease progression. Blood 104:1159–1165
Kumar S, Sharife H, Kreisel T, Mogilevsky M, Bar-Lev L, Grunewald M, Aizenshtein E, Karni R, Paldor I, Shlomi T, Keshet E (2019) Intra-tumoral metabolic zonation and resultant phenotypic diversification are dictated by blood vessel proximity. Cell Metab 30:1–11
Laubach JP, Liu CJ, Raje NS, Yee AJ, Armand P, Schlossman RL, Rosenblatt J, Hedlund J, Martin M, Reynolds C, Shain KH, Zackon I, Stampleman L, Henrick P, Rivotto B, Hornburg KTV, Dumke HJ, Chuma S, Savell A, Handisides DR, Kroll S, Anderson KC, Richardson PG, Ghobrial IM (2019) A phase I/II study of evofosfamide, a hypoxia-activated prodrug with or without bortezomib in subjects with relapsed/refractory multiple myeloma. Clin Cancer Res 25:478–486
Lee JH, Lee JE, Kahng JY, Kim SH, Park JS, Yoon SJ, Um JY, Kim WK, Lee JK, Park J, Kim EH, Lee JH, Ching WS, Ju YS, Park SH, Chang JH, Kang SG, Lee JH (2018) Human glioblastoma arises from subventricular zone cells with low-level driver mutations. Nature 560:243–247
Lewis DM, Park KM, Tang V, Yu Y, Pak K, Eisnger-Mathason TS, Simon MC, Gerecht S (2016) Intratumoral oxygen gradients mediate sarcoma cell invasion. Proc Natl Acad Sci USA 113:9292–9297
Lewis DM, Pruitt H, Jain N, Ciccaglione M, McCaffery JM, Xia Z, Weber K, Eisinger-Mathason TSK, Gerecht S (2019) A feedback loop between hypoxia and matrix stress relaxation increases oxygen-axis migration and metastasis. Cancer Res 79:1981–1995
Li Z, Bao S, Wu Q, Wang H, Eyler C, Sathornsumetee S, Shi Q, Cao Y, Lathia J, McLendon RE, Hjelmeland AB, Rich JN (2009) Hypoxia-inducible factors regulate tumorigenic capacity of glioma stem cells. Cancer Cell 15:501–513
Li L, Li JCV, Yang H, Zhang X, Liu LL, Li Y, Zeng TT, Zhu YH, Li XD, Li Y, Xie D, Fu L, Fuan XY (2019) Expansion of cancer stem cell pool initiates lung cancer recurrence before angiogenesis. Proc Natl Acad Sci USA 115:E8948–E8957
Lin CH, Kaushansky K, Zhan H (2016) JAK2V617F-mutant vascular niche contributes to JAK2V617F clonal expansion in myeloproliferative neoplasms. Blood Cells Mol Dis 62:42–48
Lin CH, Zhang Y, Kaushansky K, Zhan H (2018) JAK2V617F-bearing vascular niche enhances malignant hematopoietic regeneration following radiation injury. Haematologica 103:1160–1168
Liu XM, Zhang QP, Mu YG, Zhang XH, Sai K, Pang JC, Ng HK, Chen ZP (2011) Clinical significance of vasculogenic mimicry in human gliomas. J Neuro-Oncol 105:173–179
Liu Q, Huang X, Zhang H, Tian X, He L, Yang R, Yan Y, Wang QD, Gillich A, Zhou B (2015) c-kit+ cells adopt vascular endothelial but not epithelial cell fates during lung maintenance and repair. Nat Med 21:866–868
Liu M, Zhang L, Marsboom G, Jambusaria A, Xiong S, Toth PT, Benevolenskaya EV, Rehman J, Malik AB (2019a) Sox17 is required for endothelial regeneration following inflammation-induced vascular injury. Nat Commun 10:2126
Liu XM, LI F, Yang YT, Xu XD, Chen JS, Chen TL, Chen HJ, Zhu YB, Lin JY, Li Y, Xie XM, Sun XL, Ke YQ (2019b) IGFB2 promotes vasculogenic mimicry formation via regulating CD144 and MMP2 expression in glioma. Oncogene 38:1815–1831
Lombardi G, De Salvo GL, Brandes AA, Eoli M, Rudà R, Faedi M, Lolli I, Pace A, Daniele B, Pasqualetti F, Rizzato S, Bellu L, Pambuku A, Farina M, Magui G, Indraccolo S, Gardiman MP, Soffietti R, Zanogel V (2019) Regorafenib compared with lomustine in patients with relapsed glioblastoma (REGOMA): a multicentre, open-label, randomised, controlled, phase 2 trial. Lancet Oncol 20:110–119
Lukowski SW, Patel J, Andersen SB, Sim SL, Wong HY, Tay J, Winkler I, Powell JE, Khosrotehrani K (2019) Single-cell transcriptional profiling of aortic endothelium identifies a hierarchy from endovascular progenitors to differentiated cells. Cell Rep 27:2748–2758
McClelland MR, Carkskadon SL, Zhao L, White ES, Beer DG, Orringer MB, Pickens A, Chang AC, Arenberg DA (2007) Diversity of the angiogenic phenotype in non-small cell lung cancer. Am J Respir Cell Mol Biol 36:343–350
Majzner RG, Theruvath JL, Nellan A, Heitzeneder S, Cui Y, Mount CW, Rietberg SP, Linde MH, Xu P, Rota C, Sotillo E, Labanieh L, Lee DW, Orentas RJ, Dimitrov DS, Zhu Z, Croix BS, Delaidelli A, Sekunova A, Bonvini E, Mitra SS, Quezado MM, Majeti R, Monje M, Sorensen PHB, Maris JM, Mackall CL (2019) CAR T cell targeting B7-H3, a pan-cancer antigen, demonstrate potent preclinical activity against pediatric solid tumors and brain tumors. Clin Cancer Res 25:2560–2574
Marcu R, Choi YJ, Xue J, Fortin CL, Wang Y, Nagao RJ, Xu J, MacDonald JW, Bammler TK, Murry CE, Muczynski K, Stevens KR, Himmelfarb J, Schwartz SM, Zheng Y (2018) Human organ-specific endothelial cell heterogeneity. iScience 4:20–235
Martin JD, Seano G, Jain RK (2019) Normalizing function of tumor vessels: progress, opportunities, and challenges. Annu Rev Physiol 81:505–531
Mastrella G, Hou M, Li M, Stoecklein VM, Volmain NNM, Mileteic H, Reinhard S, Herold-Mende CC, Kleber S, Eisoenhut K, Gargiulo G, Symowitz M, Vescovi AL, Horelr PN, Pennonga JM, Wagner E, Mittebron M, Bjervig R, Hambadzumyan D, Schuller U, Tonn JC, Modke J, Glon R, Kalin RE (2019) Targeting APLN/APLNR improves anti-angiogenic efficiency and blunts proinvasive side effects of VEGFA/VEGFR2-blockade in glioblastoma. Cancer Res 79:2298–2313
McDermott DF, Huseni MA, Atkins MB, Motzer RJ, Rini BI, Escudier B, Fong L, Joseph RW, Pal SK, Reeves JA, Sznol M, Hainswoth J, Rathmell WK, Stadler WM, Hutsion T, Gore ME, Ravaud A, Bracarda S, Suarez C, Danielli R, Gruenwald V, Chouiri TK, Nickles D, Jhunjhunwala S, Piault-Louis E, Thobhani A, Qiu J, Chen DS, Hedge PS, Schiff C, Fine GD, Powles T (2018) Clinical activity and molecular correlates of response to atezolizumab alone or in combination with bevacizumab versus sunitinib in renal cell carcinoma. Nat Med 24:749–757
McDonald AI, Shirali AS, Aragon R, Ma F, Hernandez G, Vaughn DA, Mack JJ, Lim TY, Sunshine H, Zhao P, Kalinichenko V, Hai T, Pellegrini M, Ardehali R, Iruela-Arispe ML (2018) Endothelial regeneration of large vessels is a biphasic process driven by local cells with distinct proliferative capacities. Cell Stem Cell 23:210–225
Mead AJ, Mullally A (2017) Myeloproliferative neoplasm stem cells. Blood 129:1607–1616
Mei X, Chen YS, Chen FR, Xi SY, Chen ZP (2017) Glioblastoma stem cell differentiation into endothelial cells evidenced through live-cell imaging. Neuro-Oncology 19:1109–1118
Mischinger J, Frohlich E, Mannweiter S, Meindl C, Absenger-Novak M, Hutterer JC, Seles M, Augustin H, Chromecki TF, Jesche-Chromercki J, Pummer K, Zigeuner R (2019) Prognostic value of B7-H3 and the stage, size, grade and necrosis (SSIGN) score in metastatic clear cell renal cell carcinoma. Cent European J Urol 72:23–31
Moschetta M, Mishima Y, Kawano Y, Manier S, Paiva B, Palomera L, Aliawai Y, Calcinotto A, Unitt C, Sahin I, Sacco A, Glavey S, Shi J, Reagan MR, Prosper F, Bellone M, Chesi M, Bergsagel LP, Vacca A, Roccaro AM, Ghobrial IM (2016) Targeting vasculogenesis to prevent progression in multiple myeloma. Leukemia 30:1103–1115
Naito H, Kidoya H, Sakimoto S, Wakabayashi T, Takakura N (2012) Identification and characterization of a resident vascular stem/progenitor cell population in preexisting blood vessels. EMBO J 31:842–855
Naito H, Wakabayashi T, Kidoya H, Muramatsu F, Fakara K, Eino D, Yamane K, Iba T, Takakura N (2016) Endothelial side population cells contribute to tumor angiogenesis and antiangiogenic drug resistance. Cancer Res 76:3200–3210
Ngalia J, Green AR (2017) Myeloproliferative neoplasms: from origins to outcomes. Blood 130:2475–2483
Nguyen-Kim TD, Frauenfelder T, Strobel K, Veit-Haibach P, Hueliner MW (2015) Assessment of bronchial and pulmonary blood supply in non-small cell lung cancer subtypes using computed tomography perfusion. Investig Radiol 50:179–186
Nishimura R, Nishiwaki T, Kawasaki T, Sekine A, Suda R, Urushibara T, Suzuki T, Takayanagi S, Terada J, Sakao S, Tatsumi K (2015) Hypoxia-induced proliferation of tissue-resident endothelial progenitor cells in the lung. Am J Physiol Lung Cell Mol Physiol 308: L746–L758
Obad N, Espedal H, Jirik R, Sakariassen PO, Brekke Rygh C, Lund-Johansen M, Taxt T, Niclou SAP, Bjervig R, Keunen O (2018) Lack of functional normalization of tumour vessels following anti-angiogenic therapy in glioblastoma. J Cerebr Blood Flow Metab 38:1741–1753
Ohga N, Ishikawa S, Maishi N, Akiyama K, Hida Y, Kawamoto T, Sadamoto Y, Osawa T, Yamamaoto K, Kondoh M (2012) Heterogeneity of tumor endothelial cells: comparison between tumor endothelial cells isolated from high- and low-metastatic tumors. Am J Pathol 180:1294–1307
Ohle SJ, Anandaiah A, Fabian AJ, Fine A, Kotton DN (2012) Maintenance and repair of the lung endothelium does not involve contributions from marrow-derived endothelial precursor cells. Am J Respir Cell Mol Biol 47:11–19
Ottesbach K (2019) Endothelial-to-haematopoietic transition: an update on the process of making blood. Biochem Soc Trans 47:2752–2760
Overman J, Fontaine F, Moustaqil M, Mittal D, Sierecki E, Sacilotto N, Zuegg J, Robertson AA, Holmes K, Salim AA, Mamidyala S, Butler MS, Robinson AS, Lesieur E, Johnston W, Alexandrov K, Black BL, Hogan BM, De Val S, Capon RJ, Carroll JS, Bailey TL, Koopman P, Jauch SMJ, Cooper MA, Gambin Y, Francois M (2017) Pharmacological targeting of the transcription factor SOX18 delays breast cancer in mice. elife 6:e21221
Pàez-Ribes M, Allen E, Hudock J, Takedaq T, Okuyama H, Vinals F, Inoue M, Bergers G, Hanahan D, Casanovas O (2009) Antiangiogenic therapy elicits malignant progression of tumors to increased local invasion and distant metastasis. Cancer Cell 15:220–231
Palomero J, Vegliante MC, Rodriguez ML, Equileor A, Castellano G, Planas-Rigol E, Jares P, Ribera-Cortada I, Cide MC, Campo E, Amador V (2014) SOX11 promotes tumor angiogenesis through transcriptional regulation of PDGFA in mantle cell lymphoma. Blood 124:2235–2247
Passalidou E, Trivella M, Singh N, Ferguson M, Hu J, Cesario A, Granone P, Nicholson AG, Goldstraw P, Ratcliffe C, Teflow M, Leigh I, Harris AL, Gatter KC, Pezzella F (2002) Vascular phenotype in angiogenic and non-angiogenic lung non-small cell carcinomas. Br J Cancer 88:244–249
Pastushenko I, Van den Eynden GG, Vicente-Arregui S, Prieto-Torres L, Alvarez-Alegret R, Querol I, Dirix LY, Carapeto FJ, Vermeulen PB, Van Laere SJ (2016) Increased angiogenesis and lymphangiogenesis in metastatic sentinel lymph nodes is associated with nonsentinel lymph node and distant metastasis in patients with melanoma. Am J Dermapathol 38:338–346
Patel J, Seppanen EJ, Rodero MP, Wong HY, Donovan P, Neufeld Z, Fisk NM, Francois M, Khosrotehrani (2017a) Functional definition of progenitors versus mature endothelial cells reveals key SoxF-dependent differentiation process. Circulation 135:786–805
Patel SI, Sanjana NE, Kishton RI, Eidizadeh A, Vodnala SK, Lee AH, Cam M, Gartner JJ, Jia L, Steinberg SM, Yamamoto TN, Merchant AS, Mehta GU, Chichura A, AShaslem O, Tran E, Eil R, Sukumar M, Guijarro EP, Day CP, Robbins P, Feldman S, Merlino G, Zhang F, Restifo NP (2017b) Identification of essential genes for cancer immunotherapy. Nature 548:537–542
Pervoliotis K, Ntellas P, Dadouli K, Koutoukoglou P, Ioannou M, Tepetes K (2017) Microvessel density in patients with cutaneous melanoma: an up-to-date systematic review and meta-analysis. J Skin Cancer 2017:2049140
Petrakis G, Veloza L, Clot G, Gine E, Gonzalez-Farre B, Navarro A, Bea S, Martinez A, Lopez-Guillermo A, Amador V, Ribera-Cortada I, Campo E (2019) Increased tumor angiogenesis in SOX11-positive mantle cell lymphoma. Histopathology in Press 75(5):704–714
Pezzella F, Pastorino U, Tagliabue E, Andreola S, Sozzi G, Gasparini G, Menard S, Gatter KC, Harris AL, Fox S, Buyse M, Pilotti S, Pierotti M, Rilke F (1997) Non-small-cell lung carcinoma tumor growth without morphological evidence of neo-angiogenesis. Am J Pathol 151:1417–1423
Piaggio G, Rosti V, Corselli M, Bertolotti F, Bergamaschi G, Pozzi S, Imperiale D, Chiavarina B, Bonetti E, Novara F, Sessarego M, Villani L, Garuti A, Massa M, Ghio R, Campanelli R, Bacigalupo A, Pecci A, Viarengo G, Zuffardi O, Frassoni F, Barosi G (2009) Endothelial colony-forming cells from patients with chronic myeloproliferative disorders lack the disease-specific molecular clonality marker. Blood 114:3127–3130
Picarda E, Ohaegbulam KC, Zang X (2016) Molecular pathways: targeting B7-H3 (CD276) for human cancer immunotherapy. Cancer Res 22:1–7
Porcù E, Maule F, Boso D, Rampazzo E, Barbieri V, Zuccolotto G, Rosato A, Frasson C, Viola G, Della Puppa A, Basso G, Persano L (2018) BMP9 counteracts the tumorigenic and pro-angiogenic potential of glioblastoma. Cell Death Differ 25:1808–1822
Pour L, Efebera Y, Granell M, Hajek R, Oriol A, Delaunay J, Le Du K, Eveillard JM, Karlin L; Maisnar V, Martinez-Lopez J, Mateos MV, Moreb J, Ribrag V, Richardson PG, Straub J, Byrne C, Jacques C, Zubair H, Oclo EM (2019) A phase 1 / 2 study of safety of safety and efficacy of melflufen and dexamethasone in combination with either bortezomib or daramutamamb in patients with RRMM; first report on phase 1 data. AACR annual meeting, Atlanta, 2019, abstract, CT080
Rajikumar SV, Mesa RA, Fonseca R, Schroeder G, Plevak MF, Diuspenzieri A, Lacy MQ, Lust JA, Witzig TE, Gertz MA, Kyle RA, Russell SJ, Greipp PR (2002) Bone marrow angiogenesis in 400 patients with monoclonal gammopathy of undetermined significance, multiple myeloma, and primary amyloidosis. Clin Cancer Res 8:2210–2216
Reardon DA, Lassman AB, Schiff D, Yunns SA, Gerstner ER, Choughesy TF, Lee EQ, Gaffey SC, Barns J, Bruno J, Murikansky A, Duda DG, Jain RK, When PY (2018) Phase 2 and biomarker study of trebanabib, an angiopoietin-blocking peptidobody, with and without bevacizumab for patients with recurrent glioblastoma. Cancer 124:1438–1448
Ribatti D, Vacca A (2018) New insights in anti-angiogenesis in multiple myeloma. Int J Mol Sci 19: 20131
Ribatti D, Annese T, Ruggieri S, Tamma R, Crivellato E (2019) Limitations of anti-angiogenic treatment of tumors. Trans Oncol 12:981–986
Ricci-Vitiani L, Pallini R, Biffoni M, Todaro M, Invernici G, Cenci T, Maira G, Parati EA, Stassi G, Larocca LM, De Maria R (2010) Tumour vascularization via endothelial differentiation of glioblastoma stem-like cells. Nature 468:824–828
Richardson P, Ocio E, Oriol A, Larocca A, Rodriguez Otero P, Moreb J, Bladé J, Hassoun H, Cavo M, Alegre A, Mazumder A, Maisel C, Paner A, Gabrail N, Zonder JA, Chauhan D, Harmenberg J, Thuresson S, Zut A, Mateos MV (2019) OP-106 Horizon – Melflufen therapy for RRMM patients refractory to Daratumumab and /or pomalidomide; updated results and first report on PFS. Blood 132:600
Rini RI, Powles T, Atkins MB, Escudier B, DE MD, Suarez C, Bracarda S, Stadier WM, Donskov E, Lee JL, Hawkins R, Ravaud A, Aleskeev B, Staehler M, uemura M, De Giorgi U, Mellado B, Porta C, Melichar B, Gurney H, Bedke J, Choueri TK, Parnis F, Khaznadar T, Thobhani A, LI S, Piault-Louis E, FrantzG HM, Schiff C, Green MC, Motzer RJ, IMmotion151 Study Group (2019) Atezolizumab plus bevacizumab versus sunitinib in patients with previously untreated metastatic renal cell carcinoma (IMmotion 151): a multicenter, open-label, phase 3, randomized controlled trial. Lancet 393:2404–2415
Rocha R, Torres A, Ojeda K, Uribe D, Rocha D, Erices J, Niechi I, Ehrenfeld P, San Martin R, Quezada C (2018) The adenosine A3 receptor regulates differentiation of glioblastoma stem-like cells to endothelial cells under hypoxia. Int J Mol Sci 19:1228
Rosti V, Villani L, Riboni R, Poletto V, Bonetti F, Tozzi L, Bergamaschi G, Catarsi P, Dallera E, Novara F (2013) Spleen endothelial cells from patients with myelofibrosis harbor the JAK2V617F mutation. Blood 121:360–368
Saltarella I, Frassanito MA, Lamanuzzi A, Brevi A, Leone P, Desantis V, Di Marzo L, Bellone M, Derudas D, Ribatti D, Chiaramonte R, Palano MT, Neri A, Mariggiò MA, Fumarulo R, Dammacco F, Recanelli V, Vacca A, Ria R (2019) Homotypic and heterotypic activation of the Notch pathway in multiple myeloma-enhanced angiogenesis: a novel therapeutic target? Neoplasia 21:93–105
Sattiraju A, Mintz A (2019) Pericytes in glioblastomas: multifaceted role within tumor microenvironments and potential for therapeutic interventions. Adv Exp Med Biol 1147: 65–91
Schmitt CE, Woolls MJ, Jin SW (2013) Mutant-specific gene expression profiling identifies SRY-related HMG box 11b (SOX11b) as a novel regulator of vascular development in zebrafish. Mol Cells 35:166–172
Schneller D, Hofer-Warbinek R, Sturtzel C, Lipnik K, Gencelli B, Seltenhammer M, Wen M, Testori J, Bilban M, Borowski A, Windwarder M, Kapel SS, Besemfelder E, Cejka P, Habertheuer A, Schlechta B, Majdic O, Altmann F, Kocher A, Augustin HG, Luttmann W, Hofer E (2019) Cytokine-like 1 is a novel proangiogenic factor secreted by and mediating functions of endothelial progenitor cells. Circ Res 124:243–255
Scholz A, Harter PN, Cremer S, Yalcin BH, Gurnik S, Yamaii M, Di Tacchio M, Sommer K, Baumgarten P, Bahr O, Steinbach JP, Trojan J, Glas M, Herlinger U, Krex D, Meinhardt M, Weyerbrock A, Timmer M, Goldbrunner R, Deckert M, Braun C, Schittenhelm J, Frueh JT, Ulrich E, Mittelbronn M, Plate KH, Reiss Y (2016) Endothelial cell-derived angiopoietin-2 is a therapeutic target in treatment-naïve and bevacizumab-resistant glioblastoma. EMBO Mol Med 8:39–57
Seaman S, Stevens J, Yang MY, Logsdon D, Graff-Cheny C, Croix B (2007) Genes that distinguish physiological and pathological angiogenesis. Cancer Cell 11:539–554
Seaman S, Zhu Z, Saha S, Zhang XM, Yang MY, Hilton MB, Morris K, Szot C, Morris H, Swing DA, Tessarollo L, Smith SW, Degrado S, Borkin D, Jain N, Scheiermann J, Feng Y, Wang Y, Li J, Welsch D, DeCrescenzo D, Chaudhary A, Zudaire E, Klarmann KD, Keller JR, Dimitrov DS, Croix B (2017) Eradication of tumors through simultaneous ablation of CD276/B7-H3-positive tumor cells and tumor vasculature. Cancer Cell 31:515.e8
Sekine A, Nishiwaki T, Nishimura R, Kawasaki T, Urushibara T, Suda R, Suzuki T, Takayanagi S, Terada J, Sakao S, Tada Y, Iwama A, Tatsumi K (2016) Prominin-1/CD133 expression as potential tissue-resident vascular endothelial progenitor cells in the pulmonary circulation. Am J Physiol Lung Cell Mol Biol Physiol 310:L1130–L1142
Singhal M, Liu X, Inverse D, Jiang K, Dai J, He H, Bartels S, Li W, Pari AAA, Gengenbacher N, Besemfelder E, Hui L, Augustin HG, Hu J (2018) Endothelial cell fitness dictates the source of regenerating liver vasculature. J Exp Med 215:2497–2508
Soda Y, Marumoto T, Friedmann-Morvinski D, Soda M, Liu F, Michiue H, Pastorino S, Yang M, Hoffman RM, Kesari S, Verma IM (2011) Transdifferentiation of glioblastoma into vascular endothelial cells. Proc Natl Acad Sci USA 108:4274–4280
Son YS, Kwon SM, Cho JY (2019) CD276 (B7-H3) maintains proliferation and regulates differentiation in angiogenic function in late endothelial progenitor cells. Stem Cells 37:382–394
Souweidane MM, Kramer K, Pendit-Taskar N, Zhou Z, Haque S, Zanzonico P, Carrasquillo JA, Lyashchenko SK, Takur SB, Donzelli M, Turner RS, Lewis JS, Cheung NV, Larson SM, Dunkel IJ (2018) Convection-enhanced delivery for diffuse intrinsic pontine glioma: a single-centre, dose-escalation, phase 1 trial. Lancet Oncol 19:1040–1050
Sozer S, Fiel MI, Schiano T, Xu M, Mascarenhas J, Hoffman R (2009a) The presence of JAK2V617F mutation in the liver endothelial cells of patients with Budd-Chiari syndrome. Blood 113:5246–5249
Sozer S, Ishii T, Fiel MI, Wang J, Wang X, Zhang W, Godbold J, Xu M, Hoffman R (2009b) Human CD34+ cells are capable of generating normal and JAK2V617F positive endothelial like cells in vivo. Blood Cells Mol Dis 43:304–312
Strese S, Wickstrom M, Fuchs PF, Fryknas M, Gerwins P, Dale T, Larsson R, Guilbo J (2013) The novel alkylating prodrug melflufen (J1) inhibits angiogenesis in vitro and in vivo. Biochem Pharmacol 86:888–895
Streubel B, Chott A, Huber D, Exner M, Jager U, Wagner O, Schwarzinger I (2004) Lymphoma-specific genetic aberrations in microvascular endothelial cells in B-cell lymphomas. N Engl J Med 351:250–259
Sturtzel C, Lipnik K, Hofer-Warbinek R, Tsetori J, Ebner B, Seigner J, Qiu P, Bilban M, Jandrositz A, Preisegger KH, Untergasser G, Gunsilius E, de Martin R, Kroll J, Hofer E (2018) FOXF1 mediates endothelila progenitor functions and regulates vascular sprouting. Front Bioeng Biotec 6:76
Su C, Zhao Y, Shi J, Zhang J, Yuan Y, Gu Y, Zhang F, Gao X, Wang C, Wang Y, Wang Z, Hu P, Qin J, Xiao L, Chang T, Wang L, Xi Y, Yin H, Chen H, Zhang L, Cheng G, Lin J, Zhang MM, Li Z, Ye J (2019) Isocitrate dehydrogenase 1 mutation reduces the pericyte coverage of microvessels in astrocytic tumors. J Neuroncol 143: 187–196
Suzuki T, Tada Y, Nishimura R, Kawasaki T, Sekine A, Urushibara T, Kato F, Kinoshita T, Ikari J, West J, Tatsumi K (2016) Endothelial-to-mesenchymal transition in lipopolysaccharide-induced acute lung injury drives a progenitor cell-like phenotype. Am J Physiol Lung Cell Mol Physiol 310:L1185–L1190
Tabouret E, Tchoghandjian A, Denicolai E, Delfino C, Metellus P, Graillon T, Boucard C, Nanni I, Padovani L, Ouafik L, Figarella-Branger D, Chinot O (2015) Recurrence of glioblastoma after radio-chemotherapy is associated with an angiogenic switch to the CXCL12-CXCR4 pathway. Oncotarget 6:11664–11675
Teofili L, Martini M, Iachininoto MG, Capodimonti S, Nuzzolo ER, Torti L, Cenci T, Larocca LM, Leone G (2011) Endothelial progenitor cells are clonal and exhibit the JAK2(V617F) mutation in a subset of thrombotic patients with Ph-negative myeloproliferative neoplasms. Blood 117:2700–2707
Testa U, Saulle E, Castelli G, Pelosi E (2016) Endothelial progenitor cells in hematologic malignancies. Stem Cell Invest 3:26
Tian L, Goldstein A, Wang H, Ching Lo H, Sun Kim I, Welte T, Sheng K, Dobroiecki LE, Zhang X, Putiuri N, Phung TL, Mani SA, Stossi F, Streekumar A, Mancini MA, Decker WK, Zong C, Lewis MT, Zhang KH (2017) Mutual regulation of tumor vessel normalization and immunostimulatory reprogramming. Nature 544:250–254
Tura O, Skinner EM, Barclay GR, Sannel K, Gallagheer RC, Brittan M (2013) Late outgrowth endothelial cells resemble mature endothelial cells and are not derived from bone marrow. Stem Cells 31:338–348
Tzankov A, Heiss S, Ebner S, Sterlacci W, Schaefer G, Augustin F, Fiegl M, Dirnhofer S (2007) Angiogenesis in nodal B cell lymphomas: a high throughput study. J Clin Pathol 60:476–482
Uribesalgo I, Hoffmann D, Zhang Y, Kavirayani A, Lazovic J, Berta J, Navatchkova M, Pai TP, Wimmer RA, Lazlo V, Schramek D, Karim R, Tortola L, Deswal S, Haas L, Zuber J, Szucs M, Kuba K, Dome B, Cao Y, Haubner BJ, Penninger JM (2019) Apelin inhibition prevents resistance and metastasis associated with anti-angiogenic therapy. EMBO Mol Med 11:e9266
Vacca A, Ribatti D (2006) Bone marrow angiogenesis in multiple myeloma. Leukemia 20:193–199
Vacca A, Ria R, Semeraro F, Merchionne F, Coluccia M, Boccarelli A, Scavelli C, Nico B, Gernone A, Battelli F, Tabilio A, Guidolin D, Petrucci MT, Ribatti D, Dammacco F (2003) Endothelial cells in the bone marrow of patients with multiple myeloma. Blood 102:3340–3348
Vainchenker W, Kralovics R (2017) Genetic basis and molecular pathophysiology of classical myeloproliferative neoplesms. Blood 130:2475–2483
Vajkoczy P, Blum S, Lamparter M, Mailhammer R, Erber R, Engelhardt B, Vestweber D, Hatzopoulos AK (2003) Multistep nature of microvascular recruitment of ex vivo-expanded embryonic endothelial progenitor cells during tumor angiogenesis. J Exp Med 197:1755–1765
Vessela P, Tonar Z, Salek D, Vokurka S, Trneny M, Kodet R, Moulis M, Kasparova P, Vermerova Z, Valenska Z, Strilesky J, Michal M, Boudova L (2014) Microvessel density of mantle cell lymphoma. A retrospective study of its prognostic role and the correlation with the Ki-67 and the mantle cell lymphoma international prognostic index in 177 cases. Virchows Arch 465:587–597
Voutouri C, Kirkpatrick ND, Chung E, Mpekris F, Baish JW, Munn LL, Fukumura D, Stylianopoulos T, Jain RK (2019) Experimental and computational analyses reveal dynamics of tumor vessel cooption and optimal treatment strategies. Proc Natl Acad Sci USA 116:2662–2671
Wakabayashi T, Naito H, Suehiro JI, Lin Y, Kawaji H, Iba T, Kouno T, Ishikawa-Kato S, Furuno M, Takara K, Maramatsu F, Weizhen J, Kidoya H, Ishihara K, Hayashizaki Y, Nishida K, Yoder MC, Takakura N (2018) CD157 marks tissue-resident endothelial stem cells with homeostatic and regenerative properties. Cell Stem Cell 22:384–397
Wang R, Chadalavada K, Wishire J, Kowalik U, Hovinga KEW, Geber A, Fligelman B, Leversha M, Brennan C, Tabar V (2010) Glioblastoma stem-like cells give rise to tumour endothelium. Nature 468:829–833
Wang P, Du H, Zhou CC, Song J, Liu X, Cao X, Mehta JL, Shi Y, Su DF, Miao CY (2014) Intracellular NAMPT-NAD+-SIRT1 cascade improves post-ischaemic vascular repair by modulating Notch signaling in endothelial progenitors. Cardiovasc Res 104:477–488
Wang X, Guo G, Guan H, Yu Y, Lu J, Yu T (2019) Challenges and potential of PD-1/PD-L1 checkpoint blockade immunotherapy for glioblastoma. J Expo Clin Cancer Res 38:87
Weis SM, Cheresh DA (2011) Tumor angiogenesis: molecular pathways and therapeutic targets. Nature Med 17:1359–1369
Wilson KE, Bachawal SV, Abou-Elkacem L, Jensen K, Machtaler S, Tian L, Willmann JK (2017) Spectroscopic photoacoustic molecular imaging of breast cancer using a B7-H3-targeted ICG contrast agent. Theranotics 7:1463–1476
Xian X, Sakurai T, Kamoyoshi A, Ichikawa-Shindo Y, Tanaka M, Koyama T, Kawate H, Yang L, Liu T, Imai A, Zhai L, Hirabayashi K, Dai K, Tanimura K, Liu T, Cui N, Igarashi K, Yamauchi A, Shindo T (2017) Vasoprotective activities of the adrenomedullin-RAMP2 system in endothelial cells. Endocrinology 158:1359–1372
Xie M, Liu M, He CS (2012) SIRT1 regulates endothelial Notch signaling in lung cancer. PLoS One 7:e45331
Xu Y, Sun P, Wang JY, Li ZZ, Gao RL, Wang XZ, Phillips WD, Liang SX (2019) Differentiation of CD45−/CD31+ lung side population cells into endothelial and smooth muscle cells in vitro. Int J Mol Med 43:1128–1138
Xue W, Du X, Wu H, Liu H, Xie T, Tong H, Chen X, Guo Y, Zhang W (2017) Aberrant glioblastoma neovascularization patterns and their correlation with DCE-MRI-derived parameters following temozolamide and bevacizumab treatment. Sci Rep 7:13894
Yang SB, Gao KD, Jiang T, Cheng SJ, Li WB (2017) Bevacizumab combined with chemotherapy for glioblastoma: a meta-analysis of randomized controlled trials. Oncotarget 8:57337–57344
Yeh HS, Chen H, Manvak SJ, Swift RA, Campbell RA, Wang C, Li M, Waterman G, Gordon MS, Ma J, Bonavida B, Berenson JR (2006) Serum pleiotrophin levels are elevated in multiple myeloma patients and correlate with disease status. Br J Haematol 133:5426–5529
Yuan X, Zhang J, Ao G, Quan C, Tian Y, Li H (2012) Lung cancer perfusion: can we measure pulmonary and bronchial circulation simultaneously? Eur Radiol 22:1665–1671
Yurugi-Kobayashi T, Itoh H, Scroeder T, Nakano A, Narazaki G, Kita F, Yanagi K, Hiraoka-Kanie M, Inoue E, Ara T, Nagasawa T, Just U, Nakao K, Nishikawa S, Yamashita JK (2006) Adrenomedullin/cyclic AMP pathway induces Notch activation and differentiation of arterial endothelial cells from vascular progenitors. Arterioscler Thromb Vasc Biol 26:1977–1984
Zeng Q, Li S, Chepeha DB, Giordano TJ, Li J, Zhang H, Polverini PJ, Nor J, Kitajewski J, Wang CY (2005) Crosstalk between tumor and endothelial cells promotes tumor angiogenesis by MAPK activation of Notch signaling. Cancer Cell 8:13–23
Zhan H, Lin CH, Segal Y, Kaushansky K (2018) The JAK2V617F-bearing vascular niche promotes clonal expansion in myeloproliferative neoplasms. Leukemia 32:462–469
Zhang H, Vakil V, Braunstein M, Smith EL, Maroney J, Chen L, Dai K, Berenson JR, Hussain MM, Klueppelberg U, Norin AJ, Akman HO, Oczelik T, Batuman OA (2005) Circulating endothelial progenitor cells in multiple myeloma: implications and significance. Blood 105:3266–3294
Zhang X, Sullivan PS, Soslow RA, Waitz R, Reuter VE, Wilton A, Thaler HT, Arul M, Slovin SF, Wei J, Spriggs DR, Dupont J, Allkison JP (2010) Tumor associated endothelial expression of B7-H3 predicts survival in ovarian carcinomas. Mod Pathol 23:1104–1112
Zhao O, Gomez GA, Zhao Y, Yang Y, Cao D, Lu J, Yang H, Lin S (2018) ETV2 mediates endothelial transdifferentiation of glioblastoma. Sign Trans Target Ther 3:4
Zhou W, Chen C, Shi Y, Wu Q, Gimple RC, Fang X, Huang Z, Zhai K, Ke SQ, Ping YF, Feng H, Rich JN, YU JS, Bao S, Bian XW (2017) Targeting glioma stem cell-derived pericytes disrupts the blood-tumor barrier and improves chemotherapeutic efficacy. Cell Stem Cell 21:591–603
Zhou Y, Zhao M, Du Y, Liu Y, Zhao G, Ye L, Li Q, Li H, Wang X, Liu X, Guo Y, Liu J, Huang Y (2019) MicroRNA-195 suppresses the progression of lung adenocarcinoma by directly targeting apelin. Torac Cancer 10:1419–1430
Zuazo-Gatzelu I, Casanovas O (2018) Unraveling the role of angiogenesis in cancer ecosystems. Front Oncol 8:248
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 The Editor(s) (if applicable) and The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Testa, U., Pelosi, E., Castelli, G. (2020). Endothelial Progenitors in the Tumor Microenvironment. In: Birbrair, A. (eds) Tumor Microenvironment. Advances in Experimental Medicine and Biology, vol 1263. Springer, Cham. https://doi.org/10.1007/978-3-030-44518-8_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-44518-8_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-44517-1
Online ISBN: 978-3-030-44518-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)