
Abstract
Tracheotomies are common procedures in ventilated intensive care patients. They can be associated with severe complications, including fatal outcome. The complications bleeding, pneumothorax, tracheal posterior wall injuries, intraoperative loss of the respiratory tract, loss of the respiratory tract during tracheostomy tube changes, tracheal ring fractures, tracheal stenoses and stoma infections are clearly presented for the various procedures and methods in numerous illustrations, tables and text descriptions, and strategies for their avoidance are discussed in detail. The complications are defined for the first time in the literature by comparing concrete data. The performance of PDT with rigid endoscopic control is described in detail under interdisciplinary aspects. A separate section is dedicated to tracheotomy-related deaths. The chapter is compulsory reading for the practicing physician in his central concern to avoid complications and a helpful orientation for the expert.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
10.1 Introduction
Complications in tracheotomies are defined very differently in literature according to type and severity, which makes comparability difficult and prompted Fantoni [1] to recommend internationally comparable criteria and the assignment of events and complications in PDT to the three phases of puncture, dilatation or insertion of the tracheostomy tube. This requirement is still valid today. In the present chapter, only studies that show a minimum of comparable operations and defined study criteria have been included.
Percutaneous dilatational tracheotomy is repeatedly evaluated as a simple, quick and cost-effective intervention in literature. It should be emphasized that both surgical tracheotomy and percutaneous dilatational tracheotomy require a learning curve under the supervision of trained personnel. The problem was described by Páez et al. [2] when PDT was introduced in 38 patients: The procedure was described in 60% as easy, in 30% as moderate and in 10% as difficult, accompanied by 26% bleeding requiring therapy, 29% tube punctures and two deaths due to bleeding and pneumothorax. A new analysis of tracheotomy-associated deaths also warns of misjudgments [3].
The complication density of the various tracheotomy methods is shown in the following overviews.
10.2 Intraoperative and Perioperative Hemorrhage
The professional definitions of bleeding are very inconsistent worldwide, both with regard to the quantities and the frequently used classifications of minor and major complications, which leads to a complication bias. Table 10.1 shows the complication density regarding hemorrhages requiring therapy under definition of the individual authors.
Under the clarification that there is bleeding during every operation, there is no uniform definition for the “complication of hemorrhage”, which must be observed when comparing the data.
According to Shlugman et al. [20], bleeding hazards occur when the midline is missed, which can be observed with every fifth intervention. The risk of fatal bleeding complications increases especially with punctures below the fourth tracheal ring [21]. Unknown variants in vascular courses, a thyroid ima artery and a high standing brachiocephalic trunk are of predisposing importance for severe and fatal incidents [3]. Due to possible vascular variations (Chap. 3), ultrasound examinations and endoscopies of the trachea are recommended prior to PDT. Deitmer and Delank [22], Klemm et al. [23] and Nowak et al. [18] agree that a rigid endoscopy with powerful suction must always be at hand for every method of tracheotomy (Fig. 10.1).

Massive hemorrhage after injury of a thyroid ima artery with impending asphyxia during PDT with flexible endoscopy: A large coagulum in the trachea and main bronchi could only be removed in a 20-year-old patient by rigid endoscopy and powerful suction in a life-saving manner
It is not the amount of bleeding that is decisive for the respiratory tract, but the risk of acute impairment of gas exchange.
Preoperative clinical examination, neck sonography and endoscopy with light-intense diaphanoscopy contribute to the early detection of atypical vascular routes.
10.3 Pneumothorax
A detailed description for the causes of intraoperative pneumothorax in PDT is provided by Fikkers et al. [24] and, after literature searches, mention posterior tracheal wall injuries nine times, via falsa in punctures and dilatations eight times, a barotrauma twice and tracheostomy tube dislocations four times as well as unexplained causes seven times. Norwood et al. [25] describe the case of a pneumothorax with fatal lung over-inflation as a result of a valve mechanism using a flexible endoscope in a 7.5 mm inner diameter ventilator tube Fig. 10.2 (Table 10.2). In literature searches, Oeken et al. [32] found 40 severe posterior tracheal wall injuries with 28 cases of pneumothorax. Koitschev et al. [33] determined eight pneumothorax cases in surveys. Ten tracheotomy-related deaths from pneumothorax were reported by Klemm and Nowak [3].

High risk of pneumothorax risk due to pulmonary over-inflation as a result of hindered expiration when using flexible endoscopes in small ventilator tubes
Beiderlinden et al. [34] see dangers of posterior tracheal wall injuries with the consequences of pneumothorax, pneumomediastinum or pneumopericardium especially in young patients with a yet soft trachea and its impressions due to bougienage processes during PDT.
An intraoperative pneumothorax in PDT is not so rare and potentially fatal. Early detection through auscultation, percussion, sonography, thorax X-ray and immediate therapy are lifesaving.
10.4 Posterior Tracheal Wall Injuries
Posterior tracheal wall injuries occur in both percutaneous dilatational tracheotomies and surgical tracheotomies (Table 10.3) and may occur harmlessly as superficial mucous membrane injuries and severely in the form of ruptures resulting in tracheoesophageal fistulas Fig. 10.3.

(a, b) Posterior tracheal wall injuries levels I and II, as a result of PDT despite flexible endoscopic control
Therefore, Ciaglia warned in [37] against the use of rigid single dilators for PDT remarking that “The day of the rigid dilator... is over”.
In Table 10.3 Six authors did not report any severity levels Chap. 11.
In a Rapitrac PDT, Kedjanyi and Gupta [38] describe a rupture of the trachea in 75% of the circumference and Gomez-Caro et al. [39] defects of the trachea of 2–4 cm in length in the cervical and thoracic trachea by PDT, also with fatal outcome. In the result of a survey, Dost and Koeser [40] reported six posterior tracheal wall injuries and seven tracheoesophageal fistulas, Delank et al. [41] reported five severe tracheal lesions requiring surgery after PDT. For diagnostic and therapeutic options, please refer to Chap. 11.
Only an endoscopy with a clear overview and the control of the surgeon by the endoscopist, the use of suitable PDT sets as well as endoscopic control of the upper and lower trachea can prevent posterior tracheal wall injuries or detect them early.
10.5 Intraoperative Loss of the Airway
In all methods of percutaneous dilatational tracheotomy, the ventilation tube must be retracted into the laryngeal plane for the purpose of PDT. Regarding this situation, Rieger [42] formulated as follows, “It is recommended that the cuff of the endotracheal tube is unblocked, and the tube is withdrawn under direct laryngoscopic control until the cuff lies above the vocal cords. The cuff shall now be blocked again above the vocal folds. Here at the latest, the safe control of the airway with the endotracheal tube is abandoned. In this position, there is a danger of dislocation with the risk of loss of the airway and the danger of aspiration. The endotracheal tube must be held in this position by an assistant while the transtracheal puncture is performed.” (Fig. 10.4a, b, Table. 10.4).

(a, b) Danger of loss of the airway during flexible endoscopic controlled PDT
The intraoperative loss of the airway is methodically possible when PDT is performed with flexible endoscopes, regardless of the type of PDT performed. A ready-to-use and fast possibility for reintubation is required.
10.6 Perioperative and Postoperative Loss of Airway
Further latent dangers consist in the loss of the airway during tracheostomy tube change due to a “shifting-closure-phenomenon”, through accidental decannulation or closure of tracheostomy tube by blood clots and mucus plugs. The term “shifting-closure-phenomenon” refers to the displacement of pretracheal tissue layers, in which parts of fat, thyroid gland, muscles and fascia can immediately lay over the stoma after decannulation, making recannulation more difficult or impossible. The risk is greatest in the early postoperative period (Table 10.5).
No tracheostomy tube change after PDT without a light source (headlamp), guide catheter, speculum (Killian Nasal-Struycken Speculum ® with long blades or Tracheal Dilator Trousseau ® ) as well as the possibility of re-intubation in stand-by. The same requirements also apply to stomata according to OST.
10.7 Tracheal Ring Fractures
There are different views on the significance of tracheal ring fractures between the fields of intensive care medicine and laryngology. This is due to the fact that the incidence of tracheal ring fractures after surgical tracheotomy plays a minor role in a retrospective literature analysis by Straetmans et al. [11] and Fiorini et al. [15] at 0.9% and 0.6%, respectively, while tracheal ring fractures are a frequent event in both autopsy findings and endoscopic findings after PDT if they are systematically searched for by Nowak et al. [18] and Byhahn et al. [49]. The current type of flexible endoscopically controlled PDT does not reveal an obligatory search, as numerous clinical studies show. Dislocated tracheal rings do not usually lead to tracheal stenosis until 5–12 weeks after epithelization and scar formation [50]. These are periods of time after which patients have long disappeared from the intensive care medicine, and when diagnostics and therapy of tracheal stenoses are assigned to the specialties of laryngology, thoracic surgery or pneumology (Chap. 12). The tracheal braces with their different anatomical variants and histological tissue formations (Chap. 4) tend to fracture during powerful compression during bouginage in PDT, independent of the method described. Van Heurn et al. [51] described necrosis and ossification processes on injured tracheal braces, especially from the 3rd week after PDT.
Walz and Schmidt [52] describe a particular tendency to vertical tracheal ring fractures of 1 to 2 adjacent braces in autopsy findings. There are currently no systematic studies available on when and under what circumstances tracheal fractures lead to tracheal stenoses requiring treatment [53] (Fig. 10.5a, b, Table 10.6).

(a, b) Tracheal ring fracture during PDT. Immediate endoscopic therapy by TED for the necessary prophylaxis of tracheal stenosis
The high number of fractures detected by Nowak et al. [18] is the result of a targeted search by study protocol in a multi-center interdisciplinary study.
Dislocated tracheal ring fractures must be expected with every percutaneous dilatational tracheotomy. Cartilage and bone splinters must be subjected to immediate endoscopic therapy to prevent later tracheal stenosis. If this is not successful, early surgical intervention is indicated.
10.8 Tracheal Stenoses
The late complication of the development of tracheal stenosis requiring therapy, usually lumen constriction from 60 to 70% up to total occlusion (grade III and IV according to Myer and Cotton), is a feared event. This circumstance is very unfortunate for the patient, as all the effort of the original rehabilitation is lost and the patient is again hospitalized with surgical and rehabilitative measures, including conditions of shortness of breath and anxiety (Table 10.7).
The widely differing definitions make comparability of the follow-up examinations difficult. The classification of degrees of severity of tracheal stenosis [70] was ignored.
The causes of tracheal stenoses are complex and usually based on a combination of tracheal trauma, inflammation and foreign body irritation with tissue formation (granulation) at predisposed sites above, next to and below the stoma with loss of the original tracheal tissue layer by fibrosis.
The ring cartilage reacts particularly sensitively to traumas and injuries with the development of recurrent tracheal stenoses, caused by excessive regeneration processes with osteoid expression of the osteoblasts and mineralization in an acidic environment. According to Nicolli et al. [71], independent of the tracheotomy method, overweight, diabetes and reflux with chronic inflammatory reactions are risk factors for the development of subglottic stenoses. Gadkaree et al. [72] extend the disposition to laryngotracheal stenoses by the co-morbidities COPD, nicotine abuse, OSAS as well as hypertension and microcirculation disorders after an analysis of 262 stenoses patients.
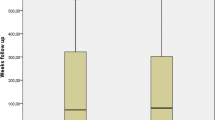
Between 1996 and 2016, a total of 102 patients with tracheal stenoses requiring therapy (aged 17–89, average age 60 years) were observed in the hospital's own patients of the University Teaching Hospital Dresden-Friedrichstadt. These were patients from 20 clinics who became conspicuous during rehabilitation several weeks after tracheotomies with shortness of breath. The occurrence of this stenosis was recurrent in 75 PDT but also in 27 OST with too high tracheostomata with injuries of the ring cartilage and/or associated with dislocated cartilage fractures left behind. One hundred and fourty-eight follow-up operations with therapy costs of Euro 1,174,850 were necessary (Fig. 10.6).

Total laryngeal atresia by via falsa in PDT: puncture, dilatation and insertion of the tracheostomy tube over the hyoid bone with subsequent total destruction and firm adhesions of the laryngeal internal structures, additionally upper tracheal stenosis Myer-Cotton IV. The patient did not survive the underlying brain tumor disease
For whatever reason, there is no indication for a tracheotomy that is supposedly “necessarily” too high, as is occasionally published in the literature. The safest prevention for later tracheal stenoses is a gentle atraumatic procedure at the right place between the 2nd and 4th tracheal braces in the midline, use of atraumatic ready sets for PDT and tissue-friendly, adapted tracheostomy tubes, therapy of infections and granulations, regular tracheostomy tube and skin care, therapy with existing reflux and continued controls with remaining tracheostoma.
10.9 Stoma Infections
There is a general opinion that surgical tracheotomies have a higher postoperative infection rate than PDT. There are no scientifically based studies on the causes. Wound infections in the stoma area are not defined in the literature (Table 10.8).
For the therapy of wound infections, please refer to Chap. 18.
10.10 Stoma Metastases
According to a study by Knipping et al. [73] using 58 PDT after Ciaglia and 17 PDT after Fantoni for malignant tumors in the mouth, larynx and throat, two cases of stomametastases with fatal outcome occurred according to the TLT Fantoni method, which is why this combination is strongly discouraged.
10.11 Tracheotomy-Related Deaths
While publications on tracheotomies have increased in recent years under various scientific aspects, communications on tracheotomy-related deaths have been published only sporadically, which is why Klemm and Nowak [3] conducted a systematic review for PDT and OST for the period 1990–2015.
In 109 publications from 21 countries with a total of 25,056 tracheotomies, including 16,827 PDT, 7,934 OST and 295 tracheotomies with no descriptions of the method, 352 tracheotomy-related deaths were found, corresponding to a total frequency of 1.4%, for PDT 0.67% (95-%-CI: 0.56; 0.81), for OST 0.62% (95-%-CI: 0.47; 0.82).
The main causes for death were bleeding (PDT 0.26%, OST 0.26%), loss of the airway (PDT 0.20%, OST 0.21%) and via falsa (PDT 0.20%, OST 0.11%). Disposing factors for deaths were variations of large blood vessels and variations of the anatomy, missing or insufficient overview in flexible endoscopy, loss of the respiratory tract, via falsa resulting in bleeding, pneumothorax and tracheoesophageal defects, sometimes in combination. Other causes for death were inadequate strategies to control complications, such as severe bleeding and pneumothorax. Too caudal tracheotomies are a high-risk factor for tracheoinominate fistula (TIF) or, synonymously, tracheaoarterial fistula (TAF). A review of the last 15 years showed a fatal outcome 77%, despite emergency intervention [74]. In addition, other risk factors are inexperience of the actors and insufficient knowledge of respiratory physiological peculiarities in tracheotomized patients and accessories in the clinic and outpatient area.
Caution! Danger of pneumothorax and death! The application of a speaking valve demands prior complete cuff-deflation whenever a cuffed tracheal tube is used [75].
Tracheotomy-related deaths are underreported worldwide [76].
Conclusions for practice
-
The frequency of tracheotomy-related deaths is similar for PDT and OST.
-
Deaths are caused by complications, the avoidance and control of which must be taken into account both during planning and aftercare, also from the point of view of medical law.
-
The use of a checklist makes sense.
-
The formation of a stoma lower than the fourth tracheal brace should be omitted; dangerous areas of the vascular anatomy can be reached.
-
Heavy bleeding to the outside must be treated surgically. For internal bleeding, securing the airways has absolute priority. Rigid endoscopy with powerful suction must be readily available.
-
Despite methodological weaknesses via falsa and flexible endoscopy are not mutually exclusive.
-
Early detection of pneumothorax can save lives.
-
Tracheotomies, regardless of the PDT or OST method, are not beginner operations and must be learned under the guidance of experienced physicians.
-
Tracheostomy tube management requires special knowledge and experience.
10.12 Avoidance and Reduction of Complications by the Rigid Tracheotomy Endoscope for Dilatational Tracheotomies (TED)
Whereas rigid tracheobronchoscopy was a common aid in the hands of the anesthetists and intensive care therapists decades ago, this management has almost been lost with the development of flexible endoscopes.
The design of the rigid tracheotomy endoscope has been adapted to the modern requirements of respiratory medicine and combines the advantages of rigid endoscopy with the aim of better controlling and reducing known and severe complications in percutaneous dilatational tracheotomies. Any current method of PDT can be performed with the endoscope in a controlled manner. The method is easy to learn.
This technique has been introduced into the endoscopy of ENT medicine by Klemm [77, 82] and adopted by Nowak et al. [78, 79] into the practice of anesthesia/intensive care.Footnote 1
10.12.1 Percutaneous Dilatational Tracheotomy with the Tracheotomy Endoscope, Practical Execution in Seven Steps
Step 1 Endoscope Insertion
Preoperative control on the basis of the “Surgical Safety Checklist” of the WHO and determination of the external landmarks, the disinfection of the neck and cleaning of the mouth and throat is carried out with the installation of a silicone dental protector in the upper jaw. The rigid endoscope is carefully inserted into the larynx entrance along the lying tube via the right corner of the mouth under sight (Fig. 10.7).

(a, b) Rigid endoscope insertion under sight. The endotracheal tube is the guidance!
The patient’s endotracheal tube is the guidance when the endoscope is inserted.
Step 2 Extubation/Intubation
With recognition of the laryngeal structures, the lying tube is unblocked by an anesthesia nurse. The endoscopist removes the endotracheal tube step by step with his left hand and simultaneously inserts the rigid endoscope into the larynx and trachea with his right hand under direct vision. Then the endoscope is connected to the ventilator (IPPV or JET). The connection of a monitor system with image transmission and respiratory gas monitoring is possible (Fig. 10.8).

The endotracheal tube is removed by the endoscopist simultaneously with the insertion of the rigid endoscope into the larynx under direct vision
With IPPV via a rigid endoscope, the leakage can be reduced using a tamponade around the endoscope with a narrow gauze bandage. However, in the case of jet ventilation, the leakage around the rigid endoscope must be maintained to exhaust respiratory gases. A tamponade around the endoscope is prohibited in jet ventilation due to the risk of air trapped with a subsequent pneumothorax.
The processes of extubation (endotracheal tube) and intubation (rigid tracheotomy endoscope) must not be separated in time.
Step 3 Clarification of the Internal Anatomy/Topography
If necessary, the trachea is cleaned by suction from secretion to the main bronchi. The trachea is then optically inspected with exact determination of the clearly visible tracheal braces 1 to 4 with deliberate identification of the ring cartilage not to be affected during tracheotomy, with possible displacement of the trachea (goiter) and possible pulsating protrusion of the brachiocephalic trunk (Arteria anonyma) (Fig. 10.9).

The correct place for tracheotomy is between the second and fourth tracheal braces
The internal anatomy is of equal obligatory importance as the external anatomy of the neck. The higher the body mass index, the more the topography of the inner trachea gains in importance.
Step 4 Diaphanoscopy and Puncture
A rigid diaphanoscopy rod, which is specially bent at the front and brightly shining, has been developed for the endoscope (Karl Storz GmbH Tuttlingen Germany), which enables brightly lit diaphanoscopy and, in individual cases, the detection of large vessels in the intended tracheotomy area. The puncture of the trachea takes place in the center of the light cone in harmonious consultation between endoscopist and surgeon between the second and fourth tracheal braces. The endoscopist always controls the surgeon. If the puncture needle is placed on a tracheal brace, it must be corrected by a few millimeters downwards or upwards with only a slight retraction of the needle to reach the space between two tracheal braces in the midline. The Seldinger wire is inserted through the puncture needle. There is a sufficiently large skin incision horizontally next to the needle, possible is also a blunt spreading (Figs. 10.10 and 10.11).

Bright diaphanoscopy provides security in orientation

(a, b) Puncture of the trachea. The extended rear tube lip of the TED protects the posterior tracheal wall from injury
Bright diaphanoscopy facilitates the view on prescribed ways. The surgeon must follow the instructions of the endoscopist.
Step 5 Bougienage
Bougienization takes place from the outside under continuous ventilation, whereby any commercially available ready set is suitable for PDT. The rigid endoscope stabilizes the trachea from the inside and protects the posterior tracheal wall (Fig. 10.12).

Bougienage of the trachea under sight with a conical single dilator
Bougienage must be carried out with “gentle force”" adapted to the vulnerable trachea under continuous visual control by the endoscopist.
Step 6 Insertion of the Tracheostomy Tube
Taking age, gender and body height into consideration, the appropriate—stepless, if possible—tracheostomy tube is inserted into the trachea and blocked under endoscopic vision. Ventilation is transferred from the endoscope to the fixed tracheostomy tube. Auscultation is used to check lateral equidistant ventilation and monitoring of the ETCO2 is used to verify the endotracheal position of the tracheostomy tube. In case of ambiguities, the position of the tracheostomy tube is checked flexibly endoscopically, also with regard to the distance to the bifurcation (Fig. 10.13).

Controlled insertion of the tracheostomy tube
Step 7 Check of Upper Trachea, Larynx and Dental Status
After determining optimal equidistant ventilation via the tracheostomy tube, the rigid endoscope is slowly withdrawn into the laryngeal plane with inspection regarding possible pathological changes of the trachea (dislocated fragments of tracheal braces) and regarding long-term intubation damage of the larynx. It is necessary to check the dental status. Tooth damage can be expected in 0.15% of cases with rigid tracheobronchoscopy [80]. Do not forget to remove foreign objects, e.g. tooth protection, tamponade.
Immediate therapy of possible pathological changes (granuloma formation, tracheal fractures) is possible and recommended without delay through the rigid endoscope.
Every elective tracheotomy requires preoperative clarification and postoperative documentation (surgical report).
10.12.2 What Are the Advantages for Avoiding and Reducing Complications in Percutaneous Dilatational Tracheotomies Using the Rigid Tracheotomy Endoscope (TED)?
-
Optimum ventilation of the intensive care patient is possible during the entire tracheotomy process. Superimposed High-frequency Jet Ventilation SHFJV® has proven to be particularly effective, Chap. 16.
-
No loss of airway during PDT. The rigid tracheotomy endoscope secures the airway during all individual steps. Loss of the airway is practically impossible.
-
Optimum protection of the posterior tracheal wall. The tracheotomy endoscope is designed in such a way that an extended rear tube lip deliberately protects the posterior tracheal wall from injury right from the start during puncture, dilatation and tracheostomy tube insertion. Severe tracheal posterior wall injury with tracheoesophageal fistula is avoided.
-
The rigid tracheotomy endoscope forms an abutment when bougienage and tracheostomy tube insertion into the trachea are necessary and prevents tracheal lumen loss and lateral compression.
-
The excellent overview through a rigid endoscope with bright illumination of the entire trachea up to the bifurcation allows optimal execution of the tracheotomy with early detection of malfunctions and via falsa with the danger of a pneumothorax or a tracheoesophageal fistula.
-
In the event of unforeseen significant bleeding, blood suction via a rigid endoscope with metal suction cups is much more effective than suction via flexible endoscopes, which can save lives. According to own experimental studies, the better capacities of blood suction with a correspondingly long metal suction cup differ from those of flexible endoscopes by 70%. Light bleeding can be stopped endotracheally with a curved special coagulation suction device.
-
In the case of massive bleeding, immediate reintubation through the endoscope is possible with a cuff that can be placed under sight at or under the bleeding source to secure the airway.
-
Dislocated tracheal braces and fragments as well as granulomas in the larynx can be treated endoscopically immediately to prevent later stenosis.
-
The possibility of stent implantation exists.
-
The entire tracheotomy process can be demonstrated via image monitoring for teaching purposes and documented by images for the patient file.
-
All parts of the endoscope are easily accessible for cleaning and can be sterilized.
-
The use of the rigid endoscope complies with the 2015 German guidelines for tracheobronchoscopy [83].
Note: From 2006 to 2010, the rigid Tracheotomy Endoscope (TED) was used in a multicenter study under the positive vote of the Ethics Committee of the Saxon Medical Association (EK-MPG-09/06-1) in 180 patients of intensive care medicine and ENT medicine on the basis of a study protocol based on Fantoni [1], published by Nowak et al. [18].
Notes
- 1.
Tracheotomy endoscope for dilatational tracheotomies (TED acc. to KLEMM): Manufactured by Karl Storz GmbH Tuttlingen, Germany, patented Nov 30, 2006, USA Pub. No. US2006/0270907A1 by Karl Storz GmbH Tuttlingen.
EC Declaration of Conformity: Karl Storz GmbH Tuttlingen, Oct 16, 2008, Endoscopes E, F, G.
Tracheoscope acc. to ALOY-KLEMM: Manufactured by Carl Reiner GmbH Wien, Austria, adapted to TwinStream™ Multi Mode Respirator made by Carl Reiner GmbH, Declaration of Product Compatibility, Vienna, Jan 28, 2008.
References
Fantoni A. The need to compare different techniques of tracheostomy in a more reliable way. Journal fur Anasthesie und Intensivbehandlung. 2006;13:61–4.
Páez M, Buisán F, Almaraz A, Martínez-Martínez A, Munoz F. Percutaneous tracheotomy with the Ciaglia Blue Rhino technique: a critical analysis after 1 year. Rev Esp Anestesiol Reanim. 2005;52(8):466–73.
Klemm E, Nowak A. Tracheotomy-related death- a systematic review. Deutsch Arztebl Int. 2017;114:273–9.
Fantoni A, Ripamonti D. A non-derivative, non-surgical tracheostomy: the translaryngeal method. Intensive Care Med. 1997;23:386–92.
Muhammad JK, Major E, Wood A, Patton D. Percutaneous dilatational tracheostomy: haemorrhagic complication and the vascular anatomy of the anterior neck. A review on 497 cases. Int J Oral Maxillofac Surg. 2000;29:217–22.
Klemm E, Henker M, Mürbe B. Percutaneous and surgical tracheotomy: discussion of risks in various procedures. Laryngo Rhino Otol. 2000;79(Suppl 1):148.
Dongelmans DA, Van Der Lely AJ, Tepaske R, Schultz M. Complications of percutaneous dilating tracheostomy. Crit Care. 2004;8:397–8.
Kost KM. Endoscopic percutaneous dilatational tracheotomy: a prospective evaluation of 500 consecutive cases. Laryngoscope. 2005;115(Suppl):1–30.
Delaney A, Bagshaw SM, Nalos M. Percutaneous dilatational tracheostomy versus surgical tracheostomy in critically ill patients: a systematic review and meta-analysis. Crit Care. 2006;10(2):R55.
Diaz-Reganon G, Minambres E, Ruiz A, Gonzales-Herrera S, Holanda Pena M, Lopez-Espadas F. Safety and complications of percutaneous tracheostomy in a cohort of 800 mixed ICU patients. Anaesthesia. 2008;63:1198–203.
Straetmans J, Schlöndorff G, Herzhoff G, et al. Complications of midline-open tracheotomy in adults. Laryngoscope. 2010;120:84–92.
Fattahi T, Vega L, Fernandes R, Golman N, Steinberg B, Schare H. Our experience with 171 open tracheotomies. J Oral Maxillofac Surg. 2012;70:1699–702.
Halum SL, Ting JY, Plowman EK, Belafsky PC, Harbarger CF, Postma GN, Pitman MJ, et al. A multi-institutional analysis of tracheotomy complications. Laryngoscope. 2011;122:38–45.
Hashemian SM, Digaleh H. A prospective randomized study comparing mini-surgical percutaneous dilatational tracheostomy with surgical and classical percutaneous tracheostomy. Medicine. 2015;94(47):e2015.
Fiorini F, Santoro R, Deganello A, Mannelli G, Meccarariello G, Gallo O. Is open tracheotomy performed by residents in otolaryngology a safe procedure? A retrospective cohort study. Eur Arch Otolaryngol. 2015;272:1483–9.
Decker S, Gottlieb J, Cruz D, Müller CW, Wilhelmi M, Krettek C, Wilhelmi M. Percutaneous dilatational tracheostomy (PDT) in trauma patients: a safe procedure. Eur J Trauma Emerg Surg. 2016;42(5):605–10.
Pilarczyk K, Haake N, Dudasova M, Huschens B, Wendt D, Demircioglu E, Jakob H, Dusse F. Risk factors for bleeding complications after percutaneous dilatational tracheostomy: a ten-year institutional analysis. Anaesth Intensive Care. 2016;44:227–36.
Nowak A, Kern P, Koscielny S, Usichenko TI, Hahnenkamp A, Jungehülsing M, Tittel M, Oeken J, Klemm E. Feasibility and safety of dilatational tracheotomy using the rigid endoscope: a multicenter study. BMC Anesthesiol. 2017;17(1):7.
Janik S, Kliman J, Hacker P, Erovic BM. Preserving the thyroidal isthmus during low tracheostomy with creation of a Björk flap. Laryngoscope. 2018;128(12):2783–9.
Shlugman D, Satya-Krishna R, Loh R. Acute fatal haemorrhage during percutaneous dilatational tracheostomy. Br J Anaesth. 2003;90:517–20.
Ayoub O, Griffiths MV. Aortic arch laceration: a lethal complication after percutaneous tracheostomy. Laryngoscope. 2006;117:1–3.
Deitmer T, Delank K. Critical comments from the ENT physician viewpoint on Ciaglia percutaneous dilatative tracheostomy. Anaesthesiol Intensivmed Notfallmed Schmerzther. 1995;30:501–3. German.
Klemm E, Künstle TH, Graf A, Henker M. Tracheostomy, critical comments and conclusions. Intensivmedizin und Notfallmedizin. 1999;36:309–13. German.
Fikkers BG, Van Veen JA, Kooloos JG, Fickkers P, Van Den Hoogen F, et al. Emphysema and pneumothorax after percutaneous tracheostomy: case reports and anatomic study. Chest. 2004;125:1805–14.
Norwood S, Vallina V, Short K, Saigusa M, Fernandez L, Mc Larty J. Incidence of tracheal stenosis and other late complications after percutaneous tracheostomy. Ann Surg. 2000;232:233–41.
Escarment J, Suppini A, Sallaberry M, Kaiser E, et al. Percutaneous tracheostomy by forceps dilation: report of 162 cases. Anaesthesia. 2000;55:125–30.
Trouillet J, Luyt CE, Guiguet M, et al. Early percutaneous tracheotomy versus prolonged intubation of mechanically ventilated patients after cardiac surgery. Ann Intern Med. 2011;154:373–83.
Oreadi D, Carlson ER. Morbidity and mortality associated with tracheotomy procedure in a university medical centre. Int J Oral Maxillofac Surg. 2012;41:974–7.
Ulkumen B, Eskiizmir G, Celik O. The safety of open surgical tracheotomy performed by otorhinolaryngology residents. Pak J Med Sci. 2018;34(3):600–5.
Cohen O, Shnipper R, Yosef L, et al. Bedside percutaneous dilatational tracheostomy in patients outside the ICU: a single center experience. J Crit Care. 2018;47:127–32.
Tamir SO, Khaleily N, Einav S, et al. 30-day morbidity and mortality rates in elderly subjects following surgical tracheostomy. Respir Care. 2018;63(8):1009–15.
Oeken J, Adam H, Bootz F. Experiences with translaryngeal tracheotomy (TLT) by Fantoni with rigid endoscopic control. HNO. 2002;50:638–43. German.
Koitschev A, Graumüller S, Dommerich S, Koitschev CH, Simon C. Tracheostomy in intensive care medicine. Is the ENT specialist still needed? HNO. 2003;51:616–21. German.
Beiderlinden M, Adamzik M, Peters J. Conservative treatment of tracheal injuries. Anesth Analg. 2005;100:210–4.
Remacle M, Lawson G, Jamart J, Trussart C, Bulpa P. Comparison between the Percutwist® and the Ciaglia® percutaneous tracheotomy techniques. Eur Arch Otorhinolaryngol. 2008;265:1515–9.
Oggiano M, Ewig S, Hecker E. A comparison of percutaneous dilatational tracheostomy versus conventional surgical tracheostomy. retrospective study in 378 patients 2003–2008. Pneumologie. 2014;68:322–8.
Ciaglia P. Technique, complications and improvements in percutaneous dilatational tracheostomy. Chest. 1999;115:1229–30.
Kedjanyi WK, Gupta D. Near total transection of the trachea following percutaneous dilatational tracheostomy. J R Coll Surg Edinb. 2001;46:242–3.
Gomez-Caro A, Diez F, Herrero P, Gude V, Cabrero E, Porch E, Nicolas J. Successful Conservative Management in Iatrogenic Tracheobronchial Injury. Ann Thorax Surg. 2005;79:1872–8.
Dost P, Koeser K. Complications of dilatative percutaneous tracheostomy in German otorhinolaryngological departments. Laryngo Rhino Otol. 1999;78:81–5. German.
Delank KW, Schmäl F, Stoll W. Trauma of the membranous trachea managed by ENT-surgeon. Laryngo Rhino Otol. 2002;81:299–304. German.
Rieger A. Tracheotomie unter Einsatz der Intubationslarynxmaske. Journal fur Anasthesie und Intensivbehandlung. 2006;13:51–4.
Gambale G, Cancellieri F, Baldini U, Vacchi Suzzi M, Baroncini S, Ferrari F, Petrini F. Ciaglia percutaneous dilational tracheostomy: Early and late complications and follow-up. Minerva Anestesiologica. 2003;69:825–33.
Altmann E, Badaev R, Radinsky E, Croitoru M, Rosin I, Davidova N, Taitelman U. Clinical and experimental assessment of griggs percutaneous tracheostomy. Journal fur Anasthesie und Intensivbehandlung. 2006;13:82–3.
Terragni PP, Antonelli M, Fumagalli R, et al. Early vs late tracheotomy for prevention of pneumonia in mechanically ventilated adult ICU patients: a randomized controlled trial. JAMA. 2010;303(15):1483–9.
Hazelton JP, Orfe EC, Calcino AM, Hunter K, Capano-Wehrle LM, Lachant MT, et al. The impact of a multidisciplinary safety checklist on adverse procedural events during bedside bronchoscopy-guided percutaneous tracheostomy. J Trauma Acute Care Surg. 2015;79(1):111–6.
Massick D, Yao S, Powell D, et al. Bedside tracheostomy in the intensive care unit: a prospective randomized trial comparing surgical tracheostomy with endoscopically percutaneous dilational tracheotomy. Laryngoscope. 2001;111:494–500.
Liao DZ, Mehta V, Kinkhabwala CM, et al. The safety and efficiacy of open bedside tracheotomy: a retrosprective analysis of 1000 patients. Laryngoscope. 2019. https://doi.org/10.1002/lary.28234.
Byhahn CH, Westphal K, Meiniger D, Gürke B, Kessler P, Lischke V. Single dilator percutaneous tracheostomy: a comparison of Percu Twist and Ciaglia Blue Rhino techniques. Intensive Care Med. 2002;28:1262–6.
Raghuraman G, Rajan S, Marzouk JK, Mullhi D, Smith FG. Is tracheal stenosis caused by percutaneous tracheostomy different from that by surgical tracheostomy? Chest. 2005;127:879–85.
van Heurn LW, Goei R, De Ploeg I, Ramsay G, Brink PR. Late complications of percutaneous dilatational tracheotomy. Chest. 1996;110:1572–6.
Walz MK, Schmidt U. Tracheal lesion caused by percutaneous dilatational tracheostomy – a clinico-pathological study. Intensive Care Med. 1999;25:102–5.
Christenson TE, Artz GE, Goldammer JE, Spiegel JE, Boon ME. Tracheal stenosis after placement of percutaneous dilational tracheotomy. Laryngoscope. 2008;118:222–7.
Dollner R, Verch M, Schweiger P, Deluigi C, Graf B, Wallner F. Laryngotracheoscopic findings in longterm follow-up after Griggs tracheostomy. Chest. 2002;122:206–12.
Frova G, Quintel M. A new simple method for percutaneous tracheostomy: controlled rotating dilation. Intensive Care Med. 2002;28:299–303.
Higgins D, Bunker N, Kinnear J. Follow-up of patients with tracheal ring fractures secondary to antegrade percutaneous dilational tracheostomy. Eur J Anaesthesiol. 2009;26(2):147–9.
Dempsey GA, Grant CA, Jones TA. Percutaneous tracheostomy: a 6 year prospective evaluation of the single tapered dilator technique. Br J Anaesth. 2010;105(6):782–8.
McCague A, Aljanabi H, Wong DT. Safety analysis of percutaneous dilatational tracheostomies with bronchoscopy in the obese patient. Laryngoscope. 2012;122:1031–4.
Ferraro F, Marfella R, Esposito M, Petruzzi J, Torino A, Santini M, Fiorelli A. Tracheal ring fracture secondary to percutaneous tracheostomy: is tracheal flaccidity a risk factor? J Cardiothorac Vasc Anaesth. 2015;29(3):560–4.
Hill B, Zweng T, Maley R, Charash W, Toursarkassian B, Kearny PA. Percutaneous dilatational tracheostomy: report of 356 Cases. J Trauma. 1996;41(2):238–44.
Law RA, Carney AS, Manara AR. Long-term outcome after percutaneous dilatational tracheostomy. Anaesthesia. 1997;52:51–6.
Rosenbower T, Morris J, Eddy V, Ries W. The long-term complications of percutaneous dilatational tracheostomy. Am Surg. 1998;64:82–6.
Walz MK, Peitken K, Thürauf N, et al. Percutaneous dilatational tracheostomy-early results and long-term outcome of 326 critically ill patients. Intensive Care Med. 1998;24:685–90.
Kearny PA, Griffen MM, Ochoa JB, Boulanger BR, Tseui BJ, Mentzner RM. A Sigle-center 8-year experience with percutaneous dilatational tracheostomy. Ann Surg. 2000;231(5):701–9.
Jung HP, Henker M, Klemm E. Langzeitergebnisse nach intercartilaginärer Visier-Tracheotomie. Mitteilungen Norddeutsche Gesellschaft für Otorhinolaryngologie and zervikofaziale Chirurgie. Demeter Thieme Verlag Stuttgart; 2004. p. 43–6.
Young E, Pugh R, Hanlon R, et al. Tracheal stenosis following percutaneos dilatational tracheostomy using the single tapered dilator: an MRI study. Anaesth Intensive Care. 2014;42(6):745–51.
Lopez-Pastorini A, Kraja O, Ludwig C, Plönes T, Storre JH, Rommel T, Riecker A, Stoelben E. Reduction of tracheotomy associated tracheal stenosis by surgical closure of the tracheotomy. A retrospective analysis of 410 tracheotomies. Pneumologie. 2015;69:335–40. German.
Dempsey GA, Morton B, Hammell C, Williams L, Smith C, Jones T. Longterm outcome following tracheostomy in critical care: A systematic review. Crit Care Med. 2016;44(3):617–28.
Araujo JB, Anon JM, Garcia de Lorenzo A, et al. Late complications of percutaneous tracheostomy using the balloon dilation technique. Med Intensiva. 2018;42(3):151–8.
Myer CM 3rd, O’Conner DM, Cotton RT. Proposed grading system for subglottic stenoses based on endotracheal tube sizes. Ann Otol Rhinol Laryngol. 1994;103:319–23.
Nicolli EA, Carey RM, Farquhar D, Haft S, Alfonso KP, Mirza N. Risk factors for adult acquired subglottic stenosis. J Laryngol Otol. 2017;131:264–7.
Gadkaree SK, Pandian V, Best S, Motz KM, Allen C, Kim Y, Akst L, Hillel AT. Laryngotracheal Stenosis: Risk Factors for Tracheostomy Dependence and Dilation Interval. Otolaryngol Head Neck Surg. 2017;156(2):321–28.
Knipping S, Schmidt A, Bartel-Friedrich S. Dilatational tracheotomy in head and neck surgery. Laryngo Rhino Otol. 2016;95(1):29–36. German.
Ried M, Reger B, Hofmann HS. Surgical treatment of tracheoarterial fistulas. Chirurg. 2019;90(9):731–5. German.
Heimer J, Eggert S, Fliss B, Meixner E. Fatal bilateral pneumothorax and generalized emphysema following contraindicated speaking-valve application. Forensic Sci Med Pathol. 2019;15:239–42.
Klemm E, Nowak A. Regarding “mortality associated with tracheostomy complications in the United States: 2007–2016”. Laryngoscope. 2019;129(6):E198.
Klemm E. Tracheotomy-endoscope for dilatational percutaneous tracheotomy. Laryngorhinootologie. 2006;85(9):628–32. German.
Nowak A, Klemm E, Rothe KF. Dilatational tracheostomy using the KLEMM tracheotomy endoscope, a new procedure for percutaneous dilatational tracheostomy in intensive care medicine. Anesth Analg. 2007a;105(6):109–10.
Nowak A, Klemm E, Rothe KF. Use of a tracheotomy-endoscope for percutaneous dilatational tracheostomy, results of a pilot study. Anesthesiology. 2007b;107:A961.
Klemm E, Petz R, Freigang B. Der Gebissschaden, ein endoskopischer Unfall? HNO-Praxis (Leipzig). 1983;8:295–300.
Nowak A, Klemm E. Percutaneous diltational tracheotomy using the tracheotomy endoscope. Laryngoscope. 2011;121:1490–4.
Klemm E, Nowak A. Das Tracheotomie-Endoskop für Dilatationstracheotomien (TED), erste Vorstellung eines neuen Verfahrens der HNO-Heilkunde und Intensivmedizin. J An Ints. 2006;13:58.
Leitlinie Tracheo-Bronchoskopie. AWMF online Register Nr. 017/061, Stand 07/2015. http://www.awmf.org/uploads/tx_szleitlinien/017-061l_S1_Tracheo_Bronchoskopie_2015-07.pdf. Latest access 9 Nov 2019.
Trottier SJ, Hazard PB, Sakabu SA, et al. Posterior tracheal wall perforation during percutaneous dilational tracheostomy: an investigation into its mechanism and prevention. Chest. 1999;115:1383–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Klemm, E., Nowak, A. (2020). Complications of Tracheotomy and Strategies to Avoid Them. In: Klemm, E., Nowak, A. (eds) Tracheotomy and Airway. Springer, Cham. https://doi.org/10.1007/978-3-030-44314-6_10
Download citation
DOI: https://doi.org/10.1007/978-3-030-44314-6_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-44313-9
Online ISBN: 978-3-030-44314-6
eBook Packages: MedicineMedicine (R0)