
Abstract
When sphincter preservation is feasible, a low anterior resection can be performed. It is important to be able to perform a tension – free anastomosis to avoid breakdown and leak. This procedure is oftentimes combined with a loop ileostomy to allow healing of the anastomosis, particularly in low rectal cancers and rectal cancers that have been treated with neoadjuvant therapy. The present chapter describes a laparoscopic anterior resection.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Overview
-
Inferior mesenteric vessels identified, and dissection extended caudally and cranially
-
Ureter and gonadal vessels identified and protected
-
IMA isolated and divided (at its origin if high ligation needed)
-
IMV isolated at inferior border of pancreas and divided
-
Splenic flexure mobilization
-
Rectal dissection carried out, including the mesorectum posteriorly
-
Distal margin chosen and colon stapled
-
Specimen exteriorized, and proximal margin then stapled across
-
Colorectal anastomosis performed
Clinical Pearls
-
During preop workup, ensure either DRE, rigid proctoscope, or flex sig has identified distal extent of tumor
-
Sacral promontory is a reliable anatomic marker for identifying the IMA to begin dissection
-
When in “Holy Plane” during posterior dissection, pneumoperitoneum will help assist with dissection in this avascular plane
-
Low Anterior Syndrome
-
Patients can have fecal urgency, frequency, clustered stool, and sensation of incomplete evacuation
-
Treatment varies, typically start with dietary fiber supplementation
-
-
ERAS protocol
-
preop HSQ
-
preop entereg if opioid naive
-
TAP block
-
foley remains until POD 3 for pelvic dissection
-
start patient on clear liquid diet and advance with return of bowel function
-
early, aggressive ambulation
-
preop NSAID
-
high carb drink 2 h before surgery
-
-
Ureters cross medially at level of common iliac arteries
-
Stents do not decrease rate of ureteral injury
-
Only help in identifying injury intraop
-
Patient Positioning
The procedure is performed with the patient in modified lithotomy, with both arms tucked.
The patient should be secured to the bed; depending on institutional practice and/or surgeon preference, techniques to accomplish this include bean bags, nonskid pads, shoulder braces, and silk tape.
A standard skin prep from the xiphoid superiorly to the pubis inferiorly and laterally to the anterior superior iliac spine.
Once the procedure is underway, the patient will be placed with the left side up and in steep Trendelenburg position; extremes of patient positioning are required to maximize visualization.
Anesthesia/Preparation
General endotracheal anesthesia.
Appropriately timed (within 60 min of incision) intravenous antibiotics covering enteric organisms (e.g., cefoxitin, ciprofloxacin/metronidazole).
Depending on patient’s physiologic status and comorbidity burden, more invasive monitoring (e.g., arterial catheter) may be required.
Consider adjunctive pain strategies (preoperative administration of acetaminophen, gabapentin, NSAIDs, TAPP blocks, and epidural catheter placement).
In the preoperative period, consider placement of ureteral catheter/stents.
A foley catheter is placed using sterile precautions.
A rectal preparation can be used using saline and a tumoricidal solution such as povidone iodine.
Access and Port Placement
The abdominal access can be achieved based on the surgeon’s preference (open/Hassan technique, closed technique/Veress needle, direct visualizing trocar).
The camera port location should be at the apex of the pneumoperitoneum; most commonly, a 10–12 mm camera port is placed in the supraumbilical position, which will also function as the site of exteriorization.
Three additional 5 mm working ports are placed.
Two are generally placed in the right upper and lower quadrants about a handbreadth apart. The lower port should be placed roughly two centimeters medial to and above the anterior superior iliac spine. The lower port should be a 12 mm port if the distal division will be performed intracorporeally.
The third can be placed in a variable (suprapubic or left lower quadrant) position, depending on patient anatomy and pathology.
The specimen can be removed via a suprapubic extraction site.
Operative Steps
-
1.
After positioning the patient left side up and in steep Trendelenburg, the small bowel is retracted out of the left lower quadrant, and the greater omentum is placed in the upper abdomen, exposing the transverse colon. Optimal exposure should allow visualization of the left colon mesentery.
-
2.
Atraumatic graspers and an energy device (electrocautery, bipolar energy, ultrasonic) will be required.
-
3.
The mobilization of the left and sigmoid colon, splenic flexure, and the division of the inferior mesenteric vessels is carried out as described in the laparoscopic left hemicolectomy section.
-
4.
The pelvic dissection may require a slight change in patient positioning, with less Trendelenburg. The dissection begins with elevation of the rectum and anterior retraction. The retrorectal space, characterized by filmy/areolar tissue is identified and developed sharply.
-
5.
A sharp dissection (using electrocautery or energy device) is carried out along this “holy plane,” which separates the presacral (below) and investing fascia of the mesorectum (above) (Fig. 17.1).
Figure 17.1 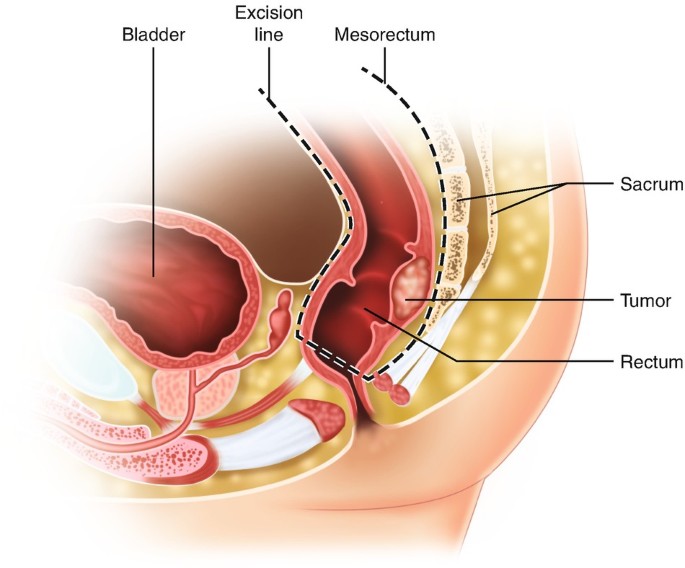
The ‘holy plane’ for total mesenteric excision during low anterior resection
-
6.
The hypogastric nerves, which descend into the pelvis and bifurcate into a wishbone configuration, should be identified, preserved, and swept laterally.
-
7.
Anteriorly, be aware of the bladder, vagina, and, in men, the seminal vesicles/prostate.
-
8.
Once the rectum has been mobilized circumferentially, ensure the level of transection and the tumor margin digitally and with an endoscopic examination, if necessary.
-
9.
The rectum can be divided with an endoscopic stapler intracorporeally or by using an open technique via the extraction site.
-
10.
The rectum and distal colon are then exteriorized via a suprapubic incision with a wound protector in place. The colon is divided proximally and the specimen removed from the field.
-
11.
An end-to-end stapled anastomosis is performed in the typical fashion, with the placement of the anvil into the proximal colotomy after placement of a purse-string suture and the introduction of the stapler transanally under direct vision. This can be done either via the suprapubic extraction site or laparoscopically after a temporary closure or use of an occlusive port (e.g., Gelport) of the extraction site. An air leak test and/or endoscopic assessment completed the anastomosis.
-
12.
A diverting ileostomy can be created selectively.
-
13.
The viscera are returned to their anatomic locations and the fascial closure is performed in the typical fashion.

Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Mohanty, S. (2020). Laparoscopic Low Anterior Resection. In: Karamanos, E. (eds) Common Surgeries Made Easy. Springer, Cham. https://doi.org/10.1007/978-3-030-41350-7_17
Download citation
DOI: https://doi.org/10.1007/978-3-030-41350-7_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-41349-1
Online ISBN: 978-3-030-41350-7
eBook Packages: MedicineMedicine (R0)