
Abstract
Understanding burn injury and its complex wound healing cascade requires recognition of the anatomy and physiology of the skin. The skin is a bilayer organ with many protective functions essential for survival.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Understanding burn injury and its complex wound healing cascade requires recognition of the anatomy and physiology of the skin. The skin is a bilayer organ with many protective functions essential for survival.
The outer epidermal layer functions as a critical barrier composed of dead cells and keratin, which protects against bacterial and environmental toxins. The basal epidermal layer is the innermost layer of the epidermis that proliferate and divide to give rise to new cells for other epidermal layers. The undulating surface of the epidermis, called rete pegs, increases adherence of the epidermis to the dermis via the basement membrane.
The inner dermal layer has a number of essential functions, including continued restoration of the epidermis. The dermis is divided into the papillary and reticular dermis. The papillary dermis is extremely bioactive in comparison to the reticular dermis.
Superficial partial burns generally heal faster than deeper partial-thickness burns due to difference in bioactivity within the dermis; the papillary component is lost in deeper burns.
The damage or loss to the normal skin barrier functions cause the following common sequelae after burn injury:
-
infection,
-
loss of body heat,
-
increased evaporative water loss,
-
change in key interactive functions such as touch and appearance,
-
excessive scarring leading to contractures.
Scars form as a result of physiologic wound healing process and may arise following any insult to the deep dermis. Genetic susceptibility, specific anatomic location, prolonged inflammation and delayed epithelialization significantly increases risk of developing excessive scarring. Hypertrophic scarring forms frequently after burn injury with incidence rates varying from 40% to 91%, depending on the depth of the wound [1, 2].
2 Physiological Versus Pathophysiologic Wound Healing
The physiologic response to an injury to the skin in adult tissue is the formation of a scar which can be temporally grouped into three distinct overlapping phases.
Each phase is critical to the success of wound closure. Deviations from the norm may be associated with delayed or abnormal wound healing [6].
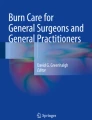
Immediately following wounding, platelet degranulation, and activation of the complement and clotting cascades form a fibrin clot for hemostasis, which acts as a scaffold for wound repair [3].
Platelet degranulation is responsible for the release and activation of an array of potent cytokines, such as epidermal growth factor (EGF), insulin-like growth factor (IGF-I), platelet-derived growth factor (PDGF), and transforming growth factor-beta (TGF-β), which serve as chemotactic agents for the recruitment of neutrophils, macrophages, epithelial cells, mast cells, endothelial cells, and fibroblasts [3, 7].
48–72 h after the initial event the healing process transitions into the proliferation phase which may last for up to 3–6 weeks [8]. Recruited fibroblasts synthesize a scaffold of reparative tissue, the so-called extracellular matrix (ECM). This granulation tissue is made of procollagen, elastin, proteoglycans, and hyaluronic acid and forms a structural repair framework to bridge the wound and allow vascular ingrowth [8]. Modified fibroblasts, the so-called myofibroblasts, containing actin filaments help initiating wound contraction.
Once the wound is closed, the immature scar can transition into the final maturation phase, which may last several months. The abundant ECM is then degraded and the immature type III collagen of the early wound can be modified into mature type I collagen [8] (Fig. 1).

Phases of wound healing
-
The transformation of a wound clot into granulation tissue thus requires a delicate balance between ECM protein deposition and degradation, and when disrupted, abnormalities in scarring appear, resulting in excessive scar formation [5].
Recent evidence suggests that it is not simply the severity of inflammation that predisposes to excessive scarring but also the type of the immune response [9]. T-helper cells (CD41) cells have been implicated as major immunoregulators in wound healing.
The characteristic cytokine expression profile of the CD41 T cells represents the basis for describing either a predominantly Th1 or Th2 response to a specific or unspecific stimulus [5, 10].
While the development of a Th2 response (with production of interleukin (IL) -4, IL-5, IL-10, and IL-13) has been strongly linked to fibrogenesis, a predominance of Th1 CD41 cells has been shown to almost completely attenuate the formation of tissue fibrosis via production of interferon-gamma (IFN-γ) and IL-12 [11, 12].
2.1 Growth Factors
2.1.1 Transforming Growth Factor-Beta
Many of the biologic actions of TGF-β contribute to the normal wound healing process and have been implicated in a wide variety of fibrotic disorders [5]. Early after injury, high levels of TGF-β are being released from degranulating platelets at the site of injury, where they act as chemoattractants for lymphocytes, fibroblasts, monocytes, and neutrophils [13].
-
The TGF-β family consists of at least five highly conserved polypeptides, with TGF-β1, −2, and −3 being the principal mammalian forms.
-
TGF-β1 and −2 are one of the most important stimulators of collagen and proteoglycan synthesis and affects the ECM not only by stimulating collagen synthesis but also by preventing its breakdown [14, 15].
-
TGF-β3, which is predominantly induced in the later stages of wound healing, has been found to reduce connective tissue deposition [16].
-
Specifically, beyond 1 week, differential expression of TGF-β isoforms, receptors and activity modulators, rather than the mere presence or absence of TGF-β, may have a major role in the development of both, keloids and hypertrophic scarring [17].
-
Interactions between keratinocytes and fibroblasts. Keratinocytes have been shown to mediate the behavior of fibroblasts during wound healing through their secretion, activation, or inhibition of growth factors such as TGF-β [9]. Particularly, release of IL-1 from keratinocytes at the wound site seems to represent the initial trigger for the inflammatory reaction and serves as an autocrine signal to fibroblasts and endothelial cells, resulting in a pleiotropic effect on them [18, 19].
2.1.2 Matrix Metalloproteinases (MMP)
The major effectors of ECM degradation and remodeling belong to a family of structurally related enzymes called MMP [5]. The MMP family consists of about 25 zinc-dependent and calcium-dependent proteinases in the mammalian system [20].
An imbalance in expression of MMPs has been implicated in a number of pathological conditions such as dermal fibrosis [21], tumor invasion and metastasis [22].
Several MMPs have been shown to mediate the breakdown of type I and III collagen, the most abundant types of collagen in the skin ECM [20]. Specifically, MMP-2 and MMP-9 activity persists after wound closure and seems to play a potent role in the remodeling process [23].
3 Wound Care Post-Burn
Treatment of burns depend on the characteristic, size, and depth of the wound. Treatments aim to expedite healing, prevent infection while minimizing patient discomfort. Burn wound therapies can be divided into three stages: assessment, management, and rehabilitation.
Management phase begins after the extent and depth of the wounds have been assessed and wounds have been thoroughly cleaned and debrided.
Each wound should be dressed with appropriate covering that serves several purposes.
-
First, it should protect the damaged epithelium, minimize bacterial and fungal colonization, and provide splinting action to maintain the desired position of function.
-
Second, the dressing should be occlusive to reduce evaporative heat loss and minimize cold stress.
-
Third, the dressing should provide comfort over the painful wound [24, 25].
The choice of dressing is based on the characteristics of the wound:
-
First-degree wounds are minor and superficial with minimal loss of barrier function. These wounds require no dressing and are treated with topical salves to decrease pain and keep the skin moist.
-
Superficial second-degree wounds will heal spontaneously, with minimal hypertrophic scarring, within 2–3 weeks if the wound remains free of infection. The capacity to heal is also dependent on the health and age of the individual. Older people and those with concomitant medical conditions are prone to delayed healing [26, 27]. These wounds need to be assessed daily and managed with dressings developed to aid in re-epithelialization, preventing wound infection, skin desiccation, and further skin damage.
-
Deep second-degree and third-degree wounds will not heal and these wounds require excision and grafting.
Wound dressings can be categorized into four groups as seen in Table 1.
3.1 Burn Wound Excision
Methods in treating burn wounds have changed in recent decades. Most studies have shown that skin excision within 72 h after injury leads to better results such as decrease in blood loss, lower incidence of infection, shorter length of hospital stay, higher probability of graft take, and drop in mortality [34].
Early wound closure has been found to decrease severity of hypertrophic scarring, joint contractures and stiffness and promotes quicker rehabilitation [35].
In general, most areas are excised with a hand skin graft knife or powered dermatome.
In partial-thickness wounds, attempts need to be made to preserve viable dermis, whereas in full-thickness injury, all necrotic and infected tissue must be removed leaving viable wound bed of either fascia, fat, or muscle [36].
3.2 Burn Wound Coverage
Following burn wound excision, it is vital to obtain wound closure. Autografting which is the transfer of the patient’s healthy skin to cover the excised burned tissue is the gold standard for burn wound coverage.
3.2.1 Skin Substitutes
With advances in burn resuscitation and critical care management, patients with large TBSA burns are surviving, leading to problems with wound coverage. This has led to the development of various biological and synthetic substrates to replace the injured skin post-burn. With the advantages of availability in large quantities, bioengineered skin substitutes, both biosynthetic and cultured autologous engineered skin, are available to provide temporary or permanent coverage [37,38,39].
There are different classifications of skin substitutes. The Kumar classification is the most common type. The Davison-Kotler classification is a newer type that categorizes skin substitutes based upon the following factors [39].
-
1.
Type of biomaterials.
-
(a)
synthetic,
-
(b)
biosynthetic,
-
(c)
biologic,
-
(a)
-
2.
Skin substitute composition regarding cellular component:
-
(a)
Cellular.
-
(b)
Acellular.
-
These skin substitutes are designed to prevent fluid loss and wound bed infection. They are mainly composed of a wide range of biomaterials such as silicone, nylon mesh, acellular cadaveric dermis, and collagen [42].
-
-
(a)
-
3.
Duration of the cover depending on its design and composition [43].
-
(a)
Permanent.
-
(b)
Semi-permanent.
-
(c)
Temporary.
-
(a)
-
4.
Layering.
-
(a)
Single.
-
(b)
Bilayer.
-
(a)
-
5.
Anatomical structure.
-
(a)
Epidermal.
-
(b)
Dermal.
-
(c)
Composite both epidermal and dermal components used to mimic the histological structure of normal skin [31].
-
(a)
Here, we will classify the skin substitutes according to anatomic structure.
3.3 Epidermal Substitutes
Act as the epidermis.
Most commonly used epidermal substitutes are cultured epithelial autografts (CEAs). These are autologous epithelial cells grown from a single full-thickness skin biopsy. These have been shown to decrease mortality in massively burned patients in a prospective, controlled trial [30]. However, widespread use of CEAs has been primarily hampered by poor long-term clinical results and exorbitant costs. They have also been consistently reported to be fragile and difficult to handle even when applied on properly prepared wound beds [32, 44, 45].
There have been studies using noncultured autologous skin cell spray grafts for burns. Following application, the skin cells induce rapid epidermal regeneration achieving re-epithelialization to heal burns, donor sites, and chronic wounds. This is useful for patients having limited donor tissue availability, as well as for patients in whom the creation of donor sites may lead to significant morbidity.
Currently, commercially available autologous epidermal substitutes for clinical use include ReCell (Avita Medical Woburn, Massachusetts), Myskin (Regenerys, Cambridge, UK), (RenovaCare, Inc., NY), CellSpray (Clinical Cell Culture (C3), Perth, Australia), Epicel (Genzyme Biosurgery, Cambridge, MA, USA), EpiDex (Modex Therapeutiques, Lausanne, Switzerland), Bioseed-S (BioTissue Technologies GmbH, Freiburg, Germany), etc.
3.4 Dermal Substitutes
In contrast to cultured epidermal sheets, engineered dermal constructs can prevent wound contraction and they provide a greater mechanical stability.
To date, a wide variety of marketed dermal constructs is available. These skin substitutes can promote the healing of acute and chronic wounds by secreting extracellular matrix (ECM) proteins, a variety of growth factors and cytokines into the wound until they undergo normal apoptosis a few weeks post-implantation [46, 47].
Allografts (cadaver skin) frequently serve as skin substitute in severely burned patients. Some are chemically treated (e.g., Alloderm®), lacking the cellular elements that are responsible for the immunogenic rejection [48]. While this approach is still commonly used in burn centers throughout the world, they only provide temporary coverage. It also bears considerable risks, including antigenicity, cross-infection as well as limited availability [49].
Xenografts have been used for hundreds of years as temporary replacement for skin loss. Even though these grafts provide a biologically active dermal matrix, the immunologic disparities prevent engraftment and predetermine rejection over time [32].
Dermagraft® (Advanced Biohealing; La Jolla, CA) consists of human foreskin fibroblasts, cultured in a biodegradable polyglactin mesh [50, 51]. It stimulates ingrowth of fibrovascular tissue and epithelialization. The frozen product offers an advantage but unfortunately requires storage at −75 °C. It is thawed in sterile saline and then applied to a clean, well-debrided wound. It has a 6-month shelf life and was approved by the FDA in 2001 for full-thickness diabetic foot ulcers of more than 6 weeks’ duration, extending through the dermis, but without exposed underlying structures. It has found value in healing complex surgical wounds with secondary closure.
3.5 Composite (Epidermal/Dermal) Substitutes
To date, the most advanced and sophisticated constructs that are available for clinical use. Composite skin substitutes mimic both epidermal and dermal layers of the skin. They have been shown to provide growth factors, cytokines, and ECM for host cells, thus initiating and regulating wound healing. Nevertheless, these skin substitutes are accompanied by long production time, high manufacturing cost and repeatedly fail to close the wound permanently due to tissue rejection [47].
Currently available epidermal/dermal substitutes that are in clinical use include StrataGraft (Stratatech, a Mallinckrodt Company), Epifix (MiMedx Group, Marietta, GA), MatriStem (ACell, Inc), Permaderm (Regenicis, New York, N.Y), Apligraf (Organogenesis Inc., Canton, Massachusetts, CA, USA), OrCel® (Ortec International, Inc., New York, NY, USA), PolyActive® (HC Implants BV, Leiden, The Netherlands), and TissueTech® Autograft System (Laser skin and Hyalograft 3D; Fidia Advanced Biopolymers, Abano Terme, Italy), Self-Assembled Skin Substitute (SASS) (Loex, Quebec).
These constructs are composed of autologous and allogeneic skin cells (keratinocytes and fibroblasts), which are incorporated into scaffolds.
Apligraf® was the first commercially available composite tissue analog on the market. This medical device containing living allogeneic cells was approved by the US Food and Drug Administration (FDA) in 1998 for the treatment of venous ulcers of 1 month duration that have not responded to conventional therapy. It was approved in 2000 for neuropathic diabetic ulcers of more than 3-week duration [52]. The epidermal component of this bilayer skin construct consists of neonatal foreskin keratinocytes seeded on a dermal component comprised of neonatal foreskin fibroblasts within a matrix of bovine type I collagen.
Orocel®, the first biologic cellular matrix, was initially developed in 1971 as a treatment for dystrophic epidermolysis bullosa [53].
Self-Assembled Skin Substitute (SASS) is a reconstruction of a fully autologous bilayered skin substitute without using any exogenous scaffold or biomaterial. SASS requires a 31-day production period [54, 55].
Integra® was developed in 1981 and approved by the FDA in 2002. It is a bilaminar skin equivalent composed of porous matrix of cross-linked bovine collagen and shark-derived glycosaminoglycan, attached to a semipermeable silicone layer that serves as an epidermis. The membrane helps prevent water loss and provides a flexible wound covering, while the scaffolding promotes neovascularization and new dermal growth. Cells migrate into the matrix while the bovine collagen is absorbed and replaced by the patient’s dermal elements. Rebuilding of the scaffolding occurs within 2–3 weeks, at which time the silicone layer is removed, allowing re-epithelialization from the wound edge. Complete wound closure takes approximately 30 days. Indications for Integra include pressure, diabetic, chronic vascular and venous ulcers, as well as surgical wounds and has been successfully utilized in immediate and delayed closure of full-thickness burns, leading to reduction in length of hospital stay, favorable cosmetics, and improved functional outcome in a prospective and controlled clinical study [56,57,58,59,60]. Our group previously conducted a randomized clinical trial utilizing Integra® in the management of severe full-thickness burns of ≥50% TBSA in a pediatric patient population comparing it to standard autograft-allograft technique, and found Integra to be associated with improved resting energy expenditure and improved aesthetic outcome post-burn [61]. It has also been found to inhibit scar formation and wound contraction [62].
There are also newer skin substitutes available in the market (Table 2)
4 Adjuncts
To further stimulate healing, several adjuvant treatment methods have been developed.
4.1 Negative Pressure Wound Therapy (NPWT)
NPWT is a wound dressing system than continuously or intermittently applies subatmospheric pressure to the surface of the wound. NPWT has been commonly used in various acute and chronic wounds [63, 64]. Majority of published literature on the use of NPWT for burns is on the use of NPWT used in skin grafting to bolster the grafts which helps promote the growth of granulation tissue → increasing the success rate of graft take. There are a few studies on the use of NPWT on acute burn and there is promising evidence to suggest NPWT may reduce edema and wound progression [65,66,67].
NPWT promotes healing through exudate removal, increase in tissue perfusion, and by exerting tensile forces on the local tissue environment; they create cellular deformation that results in mitotic activity and cell proliferation [68, 69]. NPWT is contraindicated on wounds with exposed vessels, malignancy, necrotic tissue, and untreated osteomyelitis [70, 71].
4.2 Hyperbaric Oxygen (HBOT)
HBOT is a treatment modality that has been used as an adjunct in wound healing for over 40 years. The patient undergoes multiple treatments lasting for 60–120 min inside a sealed chamber with 100% pressurized oxygen at 1.5–3 atmospheres absolute (ATA) [72].
Recent studies have shown that HBOT is safe and effective for improving burn wound healing by improving tissue oxygen and phagocytosis, preventing dermal ischemia, reducing edema, modulating the zone of stasis, preventing partial- to full-thickness conversion, and preserving cellular metabolism [73,74,75]. HBOT has been demonstrated to be safe and effective. However, more data are needed before broad conclusions can be made about the overall utility of hyperbaric oxygen for treating burns [76, 77].
5 What’s Next?
There are multiple ongoing clinical trials on the use of new skin substitutes in the treatment of burn injuries. One of the interesting focus of bioengineering and regenerative science is on the use of stem cells and the development of the 3D skin printer.
5.1 Stem Cells
The influence of stem cells on wound healing is very promising. Mesenchymal stem cells (MSCs) enhance wound healing through differentiation and angiogenesis. They also regulate the immune response and inflammation [78]. Preclinical and clinical trials show that MSC therapy accelerates wound closure [79].
5.2 3D Skin Printing
A solid 3D structure is made through a 3D printer by sequentially delivering thin layers of materials and bonding them together [80]. For 3D skin printing, this involves delivery of cells layer by layer, along with scaffolding materials using a microfluidic cartridge over the burned area. The use of 3D bioprinting is quite promising. However, there are still a lot of technological and regulatory challenges that need to be overcome [81, 82].
6 Summary
Loss of the normal skin barrier function causes the common complications of burn injury. These include infection, loss of body heat, increased evaporative water loss, and change in key interactive functions such as touch and appearance. Excessive scar formation in the areas of a deep dermal burn represents an additional well-known side effect that significantly affect the patient’s quality of life, both physically and psychologically.
Early excision and early closure of the burn wound has been probably the single greatest advancement in the treating patients with severe thermal injuries during the last 20 years. Despite all efforts, an off-the-shelf, full-thickness skin replacement is not yet available. A future prospective is to incorporate cellular growth-enhancing substances or additional cell types, besides keratinocytes and fibroblasts, in the bioengineered skin substitutes to obtain constructs with improved function and higher resemblance to native skin. The development of gene transfer technology and the use of stem cells appear to be a promising means in this context.
References
Deitch EA, Wheelahan TM, Rose MP, Clothier J, Cotter J (1983) Hypertrophic burn scars: analysis of variables. J Trauma 23(10):895–898
Lewis WH, Sun KK (1990) Hypertrophic scar: a genetic hypothesis. Burns 16(3):176–178
Tredget EE, Nedelec B, Scott PG, Ghahary A (1997) Hypertrophic scars, keloids, and contractures. The cellular and molecular basis for therapy. Surg Clin North Am 77(3):701–730
Gauglitz GG, Pavicic T (2012) Emerging strategies for the prevention and therapy of excessive scars. MMW Fortschr Med 154(15):55–58
Gauglitz GG, Korting HC, Pavicic T, Ruzicka T, Jeschke MG (2011) Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies. Mol Med 17(1–2):113–125
Janis H et al (2016) Wound healing: part I. Basic science. Plast Reconstr Surg 138(3):9S
Niessen FB, Spauwen PH, Schalkwijk J, Kon M (1999) On the nature of hypertrophic scars and keloids: a review. Plast Reconstr Surg 104(5):1435–1458
Slemp AE, Kirschner RE (2006) Keloids and scars: a review of keloids and scars, their pathogenesis, risk factors, and management. Curr Opin Pediatr 18(4):396–402
Brown JJ, Bayat A (2009) Genetic susceptibility to raised dermal scarring. Br J Dermatol 161(1):8–18
Armour A, Scott PG, Tredget EE (2007) Cellular and molecular pathology of HTS: basis for treatment. Wound Repair Regen 15(Suppl 1):S6–S17
Wynn TA (2004) Fibrotic disease and the T(H)1/T(H)2 paradigm. Nat Rev Immunol 4(8):583–594
Doucet C, Brouty-Boye D, Pottin-Clemenceau C, Canonica GW, Jasmin C, Azzarone B (1998) Interleukin (IL) 4 and IL-13 act on human lung fibroblasts. Implication in asthma. J Clin Invest 101(10):2129–2139
Bullard KM, Longaker MT, Lorenz HP (2003) Fetal wound healing: current biology. World J Surg 27(1):54–61
Szulgit G, Rudolph R, Wandel A, Tenenhaus M, Panos R, Gardner H (2002) Alterations in fibroblast alpha1beta1 integrin collagen receptor expression in keloids and hypertrophic scars. J Invest Dermatol 118(3):409–415
Kose O, Waseem A (2008) Keloids and hypertrophic scars: are they two different sides of the same coin? Dermatol Surg 34(3):336–346
Bock O, Yu H, Zitron S, Bayat A, Ferguson MW, Mrowietz U (2005) Studies of transforming growth factors beta 1-3 and their receptors I and II in fibroblast of keloids and hypertrophic scars. Acta Derm Venereol 85(3):216–220
Lu L, Saulis AS, Liu WR, Roy NK, Chao JD, Ledbetter S, Mustoe TA (2005) The temporal effects of anti-TGF-beta1, 2, and 3 monoclonal antibody on wound healing and hypertrophic scar formation. J Am Coll Surg 201(3):391–397
Niessen FB, Schalkwijk J, Vos H, Timens W (2004) Hypertrophic scar formation is associated with an increased number of epidermal Langerhans cells. J Pathol 202(1):121–129
Andriessen MP, Niessen FB, Van de Kerkhof PC, Schalkwijk J (1998) Hypertrophic scarring is associated with epidermal abnormalities: an immunohistochemical study. J Pathol 186(2):192–200
Ghahary A, Ghaffari A (2007) Role of keratinocyte-fibroblast cross-talk in development of hypertrophic scar. Wound Repair Regen 15(Suppl 1):S46–S53
Ghahary A, Shen YJ, Nedelec B, Wang R, Scott PG, Tredget EE (1996) Collagenase production is lower in post-burn hypertrophic scar fibroblasts than in normal fibroblasts and is reduced by insulin-like growth factor-1. J Invest Dermatol 106(3):476–481
Birkedal-Hansen H, Moore WG, Bodden MK, Windsor LJ, Birkedal-Hansen B, DeCarlo A, Engler JA (1993) Matrix metalloproteinases: a review. Crit Rev Oral Biol Med 4(2):197–250
Fujiwara M, Muragaki Y, Ooshima A (2005) Keloid-derived fibroblasts show increased secretion of factors involved in collagen turnover and depend on matrix metalloproteinase for migration. Br J Dermatol 153(2):295–300
Carta T, Gawaziuk JP et al (2009) Properties of an ideal burn dressing: a survey of burn survivors and front-line burn healthcare providers. Burns 45(2):364–368
Selig H, Lumenta D et al (2012) The properties of an “ideal” burn wound dressing: what do we need in daily clinical practice? Results of a worldwide online survey among burn care specialists. Burns 38:960–966
Deitch EA, Wheelahan TM, Rose MP (1983) Hypertrophic burns scars: analysis of variables. J Trauma 3:895–898
Wasaik C (2015) Burns: dressings. BMJ Clin Evid 07:1903
Liu Z et al (2017) History and advancement of burn treatments. Ann Plast Surg 78(2):S2–S8
Boateng J, Catanzano O (2015) Advanced therapeutic dressings for effective wound healing—a review. J Pharm Sci 104(11):3653–3680
Halim Y et al (2010) Biologic and synthetic skin substitutes: an overview. Indian J Plast Surg 43:S23–S28
Mohan G et al (2017) Human amnion membrane: potential applications in Oral and periodontal field. J Int Soc Prev Community Dent 7(1):15–21
Garfein ES, Orgill DP, Pribaz JJ (2003) Clinical applications of tissue engineered constructs. Clin Plast Surg 30(4):485–498
Junkins-Hopkins JM (2011) Biologic dressings. J Am Acad Dermatol 64(1):e5–e7
Desai MH, Herndon DN, Broemeling et al (1990) Early burn wound excision significantly reduces blood loss. Ann Surg 211:753–759. discussion 759–62
Saaiq M, Zaib S, Ahmad S (2012) Early excision and grafting versus delayed excision and grafting of deep thermal burns up to 40% total body surface area: a comparison of outcome. Ann Burns Fire Disasters 25:143–147
Atiyeh BS, Dham R, Kadry M, Abdallah AF, Al-Oteify M, Fathi O, Samir A (2002) Benefit-cost analysis of moist exposed burn ointment. Burns 28(7):659–663
Dziewulski P, Barret JP (1999) Assessment, operative planning and surgery for burn wound closure. In: Wolf SE, Herndon DN (eds) Burn care. Landes Bioscience, Austin, TX, pp 19–52
Murphy, Evans (2012) Review article advances in wound healing: a review of current wound healing products. Plast Surg Int:190436 – 8
Peran M et al (2019) Therapeutic strategies for skin regeneration based on biomedical substitutes. J Eur Acad Dermatol Venereol 33(3):484–496
Davison-Kotler E et al (2018) A universal classification system of skin substitutes inspired by factorial design. Tissue Eng Part B Rev 24(4):279–288
Nicholas Y (2017) Current status and future of skin substitutes for chronic wound healing. J Cutan Med Surg 21(1):23–30
Zuijlen J et al (2015) Tissue engineering in burn scar reconstruction. Burns Trauma 3:18–22
Climov E et al (2016) Bioengineered self-assembled skin as an alternative to skin grafts. Plast Reconstr Surg Glob 4:731–773
Munster AM (1996) Cultured skin for massive burns. A prospective, controlled trial. Ann Surg 224(3):372–375; discussion 375-377
Bannasch H, Fohn M, Unterberg T, Bach AD, Weyand B, Stark GB (2003) Skin tissue engineering. Clin Plast Surg 30(4):573–579
Pellegrini G, Ranno R, Stracuzzi G, Bondanza S, Guerra L, Zambruno G, Micali G, De Luca M (1999) The control of epidermal stem cells (holoclones) in the treatment of massive full-thickness burns with autologous keratinocytes cultured on fibrin. Transplantation 68(6):868–879
Ponec M (2002) Skin constructs for replacement of skin tissues for in vitro testing. Adv Drug Deliv Rev 54(Suppl 1):S19–S30
Groeber F, Holeiter M, Hampel M, Hinderer S, Schenke-Layland K (2011) Skin tissue engineering: in vivo and in vitro applications. Adv Drug Deliv Rev 63(4–5):352–366
Wainwright DJ (1995) Use of an acellular allograft dermal matrix (AlloDerm) in the management of full-thickness burns. Burns 21(4):243–248
Raff TM, Germann G, Pelzer M (2002) Clinical practice of glycerol preserved allograft skin coverage. Burns 28(Suppl 1):S10–S12
Supp DM, Boyce ST (2005) Engineered skin substitutes: practices and potentials. Clin Dermatol 23(4):403–412
Zaulyanov L, Kirsner RS (2007) A review of a bi-layered living cell treatment (Apligraf) in the treatment of venous leg ulcers and diabetic foot ulcers. Clin Interv Aging 2(1):93–98
Eisenberg M, Llewelyn D (1998) Surgical management of hands in children with recessive dystrophic epidermolysis bullosa: use of allogeneic composite cultured skin grafts. Br J Plast Surg 51(8):608–613
Boa, Genest et al (2013) Prospective study on the treatment of lower-extremity chronic venous and mixed ulcers using tissue-engineered skin substitute made by the self-assembly approach. Adv Skin Wound Care 26(9):400
Efanov D et al (2018) Use of bilaminar grafts as life-saving interventions for severe burns: a single-center experience. Burns 44:1336–1345
Tompkins RG, Burke JF (1990) Progress in burn treatment and the use of artificial skin. World J Surg 14(6):819–824
Burke JF, Yannas IV, Quinby WC Jr, Bondoc CC, Jung WK (1981) Successful use of a physiologically acceptable artificial skin in the treatment of extensive burn injury. Ann Surg 194(4):413–428
Yannas IV, Burke JF, Orgill DP, Skrabut EM (1982) Wound tissue can utilize a polymeric template to synthesize a functional extension of skin. Science 215(4529):174–176
Yannas IV, Burke JF, Warpehoski M, Stasikelis P, Skrabut EM, Orgill D, Giard DJ (1981) Prompt, long-term functional replacement of skin. Trans Am Soc Artif Intern Organs 27:19–23
Branski LK, Herndon DN, Pereira C, Mlcak RP, Celis MM, Lee JO, Sanford AP, Norbury WB, Zhang XJ, Jeschke MG (2007) Longitudinal assessment of Integra in primary burn management: a randomized pediatric clinical trial. Crit Care Med 35(11):2615–2623
Kolokol'chikova EG, Budkevich LI, Bobrovnikov AE, Badikova AK, Tumanov VP (2001) Morphological changes in burn wounds after transplantation of allogenic fibroblasts. Bull Exp Biol Med 131(1):89–93
Clayman MA, Clayman SM, Mozingo DW (2006) The use of collagen-glycosaminoglycan copolymer (Integra) for the repair of hypertrophic scars and keloids. J Burn Care Res 27(3):404–409
Morykwas D et al (1999) Use of subatmospheric pressure to prevent progression of partial thickness burns in a swine model. J Burn Care Rehabil 20(1):15–21
Molnar, Simpson et al (2006) Management of an acute thermal injury with subatmospheric pressure. J Burns Wounds 4:e5
Kamolz A et al (2004) Use of subatmospheric pressure therapy to prevent burn wound progression in human: first experiences. Burns 30(3):253–258
Teng et al (2016) Use of negative pressure wound therapy in burn patients. Int Wound J 13(S3):15–18
Kantak NA, Mistry R, Varon DE, Halvorson EG (2017) Negative pressure wound therapy for burns. Clin Plast Surg 44(3):671–677
Glass N (2012) The methodology of negative pressure wound therapy: separating fact from fiction. J Plast Reconstr Aesthet Surg 65:989–1001
Pietramaggiori, Liu et al (2007) Tensile forces stimulate vascular remodeling and epidermal cell proliferation in living skin. Ann Surg 246:896–902
Mendonca, Papini et al (2006) Negative-pressure wound therapy: a snapshot of the evidence. Int Wound J 3:261–271
Desai, Hahn et al (2012) Negative pressure wound therapy: an algorithm. Clin Plast Surg 39:311–324
Hunter L et al (2010) Hyperbaric oxygen therapy for chronic wounds. Adv Skin Wound Care 23(3):116–119
Selcuk, Ozalp et al (2013) The effect of hyperbaric oxygen treatment on the healing of burn wounds in nicotinized and nonnicotinized rats. J Burn Care Res 34:e237–e243
Cianci S et al (2013) Adjunctive hyperbaric oxygen therapy in the treatment of thermal burns. Undersea Hyperb Med 40:89–108
Dauwe PB, Pulikkottil BJ, Lavery L, Stuzin JM, Rohrich RJ (2014) Does hyperbaric oxygen therapy work in facilitating acute wound healing: a systematic review. Plast Reconstr Surg 133:208e–215e
Chiang C (2017) Adjunctive hyperbaric oxygen therapy in severe burns: experience in Taiwan Formosa Water Park dust explosion disaster. Burns 43:852–857
Schreml S et al (2010) P. Oxygen in acute and chronic wound healing. Br J Dermatol 163:257–268
Wu T et al (2007) Mesenchymal stem cells enhance wound healing through differentiation and angiogenesis. Stem Cells 25:2648–2659
Maxon, Lopez et al (2012) Concise review: role of mesenchymal stem cells in wound repair. Stem Cells Transl Med 1:142–149
Varkey Y et al (2019) Skin bioprinting: the future of burn wound reconstruction? Burns Trauma 7:4
Chouhan M et al (2019) Emerging and innovative approaches for wound healing and skin regeneration: current status and advances. Biomaterials 216:119267
Chua K et al (2016) Skin tissue engineering advances in severe burns: review and therapeutic applications. Burns Trauma 4:3
Holmes M et al (2018) A comparative study of the ReCell® device and autologous split-thickness meshed skin graft in the treatment of acute burn injuries. J Burn Care Res 39:5
Gravante A et al (2007) A randomized trial comparing ReCell system of epidermal cells delivery versus classic skin grafts for the treatment of deep partial thickness burns. Burns 33:966–927
Moustafa C et al (2007) Randomized, controlled, single-blind study on use of autologous keratinocytes on a transfer dressing to treat nonhealing diabetic ulcers. Regen Med 2(6):887–902
Hernon D et al (2006) Clinical experience using cultured epithelial autografts leads to an alternative methodology for transferring skin cells from the laboratory to the patient. Regen Med 1(6):809–821
Corcos MC et al (2011) Autologous skin cell spray-transplantation for a deep dermal burn patient in an ambulant treatment room setting. Burns 37(4):e19–e23
Lee (2012) Outcomes of sprayed cultured epithelial autografts for full-thickness wounds: a single-Centre experience. Burns 38:931–936
Greenwood JE (2011) A randomized, prospective study of the treatment of superficial partial-thickness burns: AWBAT-S versus biobrane. Eplasty 11:e10
Romanelli B et al (2007) OASIS wound matrix versus Hyaloskin in the treatment of difficult-to-heal wounds of mixed arterial/venous aetiology. Int Wound J 4:3–7
Hodde E et al (2005) An investigation of the long-term bioactivity of endogenous growth factor in OASIS wound matrix. J Wound Care 14:23–25
Philandrianos M et al (2012) Comparison of five dermal substitutes in full thickness skin wound healing in a porcine model. Burns 38(6):820–829
Kogan H et al (2019) Biologics in acute burn injury. Ann Plast Surg 83(1):26
Kim S et al (2016) New innovations for deep partial thickness burn treatment with Acell MatriStem matrix. Adv Wound Care 5(12):546
Debels H et al (2015) Dermal matrices and bioengineered skin substitutes: a critical review of current options. Plast Reconstr Surg Glob Open 3(1):e284
Zelen G (2015) A prospective, randomised, controlled, multi-Centre comparative effectiveness study of healing using dehydrated human amnion/chorion membrane allograft, bioengineered skin substitute or standard of care for treatment of chronic lower extremity diabetic ulcers. Int Wound J 12(6):724–732
Baetz G et al (2019) In vivo expansion and regeneration of full thickness functional skin with an autologous homologous skin construct: clinical proof of concept for chronic wound healing. Int Wound J 16(3):841–846
Boyce et al (2002) Cultured skin substitutes reduce donor skin harvesting for closure of excised, full thickness burns. Ann Surg 235(2):269–279
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Elloso, M., Gauglitz, G.G. (2021). Wound Healing and Wound Care. In: Jeschke, M.G., Kamolz, LP., Shahrokhi, S. (eds) Burn Care and Treatment. Springer, Cham. https://doi.org/10.1007/978-3-030-39193-5_6
Download citation
DOI: https://doi.org/10.1007/978-3-030-39193-5_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-39192-8
Online ISBN: 978-3-030-39193-5
eBook Packages: MedicineMedicine (R0)