
Abstract
This chapter will review the management of stress fractures, particularly in acute settings. Stress fractures are common overuse injuries and clinicians should expect to manage these injuries both acutely and chronically. Although stress fractures are not typically acute injuries, stress fractures in high-risk locations often require acute and sometimes emergent medical management, especially if these are allowed to progress to complete fractures. This chapter will review the epidemiology, sideline evaluation, and management of stress fractures. Finally, this will briefly review management of associated risk factors for bony stress injuries including the spectrum of relative energy deficiency in sport (RED-S).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Key Points-
Stress fractures are common injuries in active athletes.
-
Distance running and sports associated with leanness are the highest risk for stress fracture.
-
Stress fractures associated with relative energy deficiency or the female athlete triad require additional evaluation.
-
High-risk stress fractures have increased risk of complication including nonunion, delayed union, fracture with displacement, avascular necrosis, and need for surgical management.
-
High-risk locations include the femoral neck, anterior mid-tibia, navicular, body of the talus, proximal second metatarsal, sesamoids, and pars interarticularis.
-
Upper extremity stress fractures are uncommon; however, athletes who participate in overhead sports can develop these injuries.
-
Imaging typically starts with plain radiographs; however, this method of imaging is not sensitive for stress fractures, especially early stress fractures.
-
Preferred follow-up imaging includes MRI and radionuclide bone scans. CT imaging is occasionally used in confirmation of fracture lines or follow-up to assess bony healing.
-
Treatment of stress fractures varies by the grade of stress fracture and location of injury, though recovery times can be prolonged compared to acute fractures.
-
Acute presentations of stress fractures can occur if stress injuries are allowed to progress to complete fractures (Grade IV injuries); however, it is uncommon for these fractures to cause comminuted or displaced fractures other than tension-sided stress fractures.
Introduction
Bone stress injuries are common overuse injuries in athletes and nonathletes alike. These injuries result from the failure of the skeleton to hold up against repetitive submaximal forces [1]. Stress fractures can occur in normal or metabolically weakened bones. Those that occur in the setting of weakened or osteoporotic bones are sometimes termed insufficiency fractures. Stress and insufficiency fractures should be differentiated from pathologic fractures that result from fractures of abnormal bone like those associated with bone tumors (malignant or nonmalignant) or Paget’s disease [2]. This chapter will focus on bone stress injuries, particularly in acute symptomatic settings and sideline management in athletes.
Epidemiology
Rates of stress fractures vary by sport, age, and level of competitiveness. Due to inconsistent standards for measuring stress injuries with previous studies, it can be challenging to compare rates of injuries across populations. High school students have a rate of 2.22/100,000 athletic exposures in girls’ sports and 1.27/100,000 athletic exposures in boys’ sports [3]. At the collegiate level, 15% of division 1 female athletes reported a history of stress fracture on a pre-participation evaluation [4]. In a cohort study of a similar population of division 1 female athletes, approximately 10% suffered a bone stress injury over a 6-year study period [5].
Stress fractures occur most commonly in female athletes, distance running, and sports associated with leanness [6,7,8,9,10,11]. Women have a relative risk of 1.5–3.5 for stress fractures compared to men [3, 7]. One prospective study described an incidence of 3.9% in female adolescent athletes and demonstrated that several sports were risk factors for stress fractures, including running, basketball, and cheerleading/gymnastics [11]. Other risk factors for bone stress injuries include prior bone stress injury, BMI <19 kg/m2, and late menarche (e.g., ≥15 years), all features of the female athlete triad [12]. Of note, several studies have demonstrated that prior fracture is the biggest risk factor for a bone stress injury [6, 13]. Clinicians should inquire about previous stress fracture history when evaluating athletes with a suspected bony stress injury.
In retrospective case studies, the most common locations for stress fractures are the tibia (24%), tarsal navicular (18%), metatarsal (16%), fibula (16%), femur (7%), pelvis (2%), and spine (1%) [14,15,16]; however, the location of stress injury varies by sport (Table 33.1). Stress fractures of the upper extremity are found nearly exclusively in overhead athletes and are much less common than lower extremity stress fractures [3, 17].
If left untreated, bony stress injuries can progress to complete fractures. This sometimes occurs in an acute manner as the weakened bone suddenly gives out. Athletes who continue to compete or train despite known bony stress injuries are more likely to have severe injuries as are athletes who have delays in diagnosis. These acute injuries are less likely to occur if bony stress injuries are diagnosed early. Higher-grade bony stress injuries (Grades 3 and 4) represented approximately 40% of bony stress injuries in a prospective study of college runners [18].
What Is Unique About Acute Presentation of Stress Fractures?
Stress fractures are unique overuse injuries with a broad spectrum of risk factors for injury. Risk factors for stress fractures can be divided into biological and biomechanical risk factors [1, 24]. Biological factors include female sex, medications, genetics, female athlete triad, and other dietary contributors [1]. Biomechanical factors include training patterns (e.g., mileage, inadequate recovery, type of exercise (e.g., running, basketball, gymnastics), training surface, and footwear), bone characteristics, and anatomic considerations (e.g., leg length discrepancy, foot type, small calf cross-sectional area) [1, 24].
What Do the Practitioners Need to Know While Managing Acute Presentation of Stress Fractures?
Stress fractures should be suspected when athletes complain of pain with increasing activity or repeated excessive activity and limited rest. Pain with ambulation, focal tenderness, and edema are the most common history and exam findings [16]. Athletes with acute symptoms at the site of a previous stress fracture have a high risk of recurrent injury in this area; athletes should be questioned for previous stress injuries.
The differential diagnosis of stress fractures certainly depends on location of injury, but includes muscle strains, tendinopathies, periostitis, exertional compartment syndrome, nerve or artery entrapment, and pathologic fractures [7, 16]. Exam findings include the “hop” test for tibial stress fractures (and other lower extremity stress fractures), the “fulcrum” test for femoral stress fractures, and a spinal extension or “stork” test for pars interarticularis stress fractures (spondylolysis) [7, 16]. Direct palpation with reproduction of pain, where feasible, is probably the best diagnostic test maneuver [7].
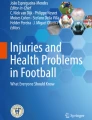
Plain radiographs are the recommended initial step in diagnosis of a suspected stress fracture [16]; however, plain radiographs may miss early stress injuries as they only have a sensitivity between 10% and 70% depending on the timing of imaging and onset of symptoms [7, 25]. Radionuclide bone scans are more sensitive than MRI, but limited by specificity and need for radiation. MRI is generally the preferred follow-up imaging for suspected stress fractures [7]. On MRI, a Grade 1 injury shows periosteal edema on fat-suppressed images. Grade 2 injury shows abnormal increased signal within the marrow cavity or along the endosteal surface on fat-suppressed images. Grade 3 injuries show abnormal signal also present on T1 images and T2 images. Finally, Grade 4 injuries show a fracture line on both T1 and T2 images [7]. Fracture lines visible on plain radiographs are consistent with Grade 4 injuries (Fig. 33.1).

Anterior tibia stress fracture. This 18-year-old female athlete developed bilateral anterior tibial stress fractures. This postoperative radiograph of the left leg demonstrated the “dreaded black line” consistent with cortical disruption of the anterior tibia (tension sided) due to a stress fracture (white arrows) and the surgically implemented intramedullary rods. (Photo Courtesy of Dr. Michelle Wolcott)
High-risk stress fractures are located in areas of poor vascular supply or are tension-sided stress injuries. High-risk stress fractures therefore have an increased risk of complication including nonunion, delayed union, fracture with displacement, avascular necrosis, and need for surgical management [7]. High-risk locations include the femoral neck, anterior mid-tibia, navicular, body of the talus, proximal second metatarsal, sesamoids, and pars interarticularis [7, 18, 24, 26]. Stress fractures located in trabecular bone (e.g., femoral neck, sacrum, and pelvis) are more common in athletes with low bone mineral density and should prompt additional bone health evaluation [18]. Although most bony stress injuries do not require urgent or emergent management, approximately 1% may progress to needing surgical intervention [3].
Stress fracture management should take into consideration the location of injury, the grade of injury, and the individual’s competitive situation [27]. Clinicians should consider the location of injury and risk in determining the urgency for imaging when considering a possible stress fracture as high-risk locations should be imaged more urgently. Ultimately, early detection of stress fractures is important as delay in diagnosis and treatment can result in prolonged return to activity and progression of injury [16, 17].
Managing suspected acute stress fractures on the sideline is relatively straightforward. Athletes should be removed from competition or training. Lower extremity injuries should be made non-weight bearing until the injury is better characterized with imaging. Urgent or emergent imaging should be considered if there is concern for a complete stress fracture, a displaced stress fracture, or especially if there is a concern for a stress fracture in a high-risk location. Overall, however, the risk of displaced fractures and comminuted fractures is small.
Return to Play
Return to play for stress fractures can vary between 4 and 12 weeks or longer once activity is restricted [14, 17]. The degree of severity found on MRI correlates to return to play in athletes [18]. On average, those with triad risks have higher-grade bone stress injuries on MRI and longer return to play [18].
Low-risk injuries respond well to nonoperative management and treatment is guided by the patient’s symptoms. High-risk injuries (by location and/or grade of injury) should be treated more aggressively with absolute rest, immobilization, or surgical fixation. The goal of management is to allow the stress injuries to heal with avoiding excessive deconditioning to the athlete [27].
Finally, for athletes with stress fractures, clinicians need to evaluate for relative energy deficiency in sport [28]. As stress fractures are the result of complex interactions between bone health, energy availability, hormonal states, and activity levels [28], failure to identify these athletes can lead to long-term health consequences outside of re-injury including osteoporosis, menstrual dysfunction, and abnormalities in immunity, and cardiovascular and psychological health [28]. For example, peak bone mineral density, a major determinant of long-term risk of osteoporosis risk, is attained by early adulthood [11, 29]. Ongoing bone loss or failure to obtain adequate bone stores in young athletes is a major risk factor for osteoporosis. Identifying those at risk for stress injuries can help clinicians implement strategies to prevent stress fractures and sequelae of low energy availability states [12].
References
Tenforde AS, Kraus E, Fredericson M. Bone stress injuries in runners. Phys Med Rehabil Clin N Am. 2016;27:139–49. https://doi.org/10.1016/j.pmr.2015.08.008.
Fayad LM, Kamel IR, Kawamoto S, et al. Distinguishing stress fractures from pathologic fractures: a multimodality approach. Skelet Radiol. 2005;34:245–59. https://doi.org/10.1007/s00256-004-0872-9.
Changstrom BG, Brou L, Khodaee M, et al. Epidemiology of stress fracture injuries among US high school athletes, 2005–2006 through 2012–2013. Am J Sports Med 2005–2006. 2014; https://doi.org/10.1177/0363546514562739.
Matheson GO, Anderson S, Robell K. Injuries and illnesses in the preparticipation evaluation data of 1693 college student-athletes. Am J Sports Med. 2015;43:1518–25. https://doi.org/10.1177/0363546515572144.
Tenforde AS, Carlson JL, Chang A, et al. Association of the female athlete triad risk assessment stratification to the development of bone stress injuries in collegiate athletes. Am J Sports Med. 2017;45:302–10. https://doi.org/10.1177/0363546516676262.
Tenforde AS, Sayres LC, McCurdy ML, et al. Identifying sex-specific risk factors for stress fractures in adolescent runners. Med Sci Sports Exerc. 2013;45:1843–51. https://doi.org/10.1249/MSS.0b013e3182963d75.
Fredericson M, Jennings F, Beaulieu C, Matheson GO. Stress fractures in athletes. Top Magn Reson Imaging. 2006;17:309–25. https://doi.org/10.1097/RMR.0b013e3180421c8c.
Brunet ME, Cook SD, Brinker MR, Dickinson JA. A survey of running injuries in 1505 competitive and recreational runners. J Sports Med Phys Fitness. 1990;30:307–15.
O’Toole ML. Prevention and treatment of injuries to runners. Med Sci Sports Exerc. 1992;24:S360–3.
Johnson AW, Weiss CB, Wheeler DL. Stress fractures of the femoral shaft in athletes – more common than expected. a new clinical test. Am J Sports Med. 1994;22:248–56.
Field AE, Gordon CM, Pierce LM, et al. Prospective study of physical activity and risk of developing a stress fracture among preadolescent and adolescent girls. Arch Pediatr Adolesc Med. 2011;165:723–8. https://doi.org/10.1001/archpediatrics.2011.34.
De Souza MJ, Nattiv A, Joy E, et al. 2014 female athlete triad coalition consensus statement on treatment and return to play of the female athlete triad: 1st International Conference held in San Francisco, California, May 2012 and 2nd International Conference held in Indianapolis, Indiana, May 2013. Br J Sports Med. 2014;48:289. https://doi.org/10.1136/bjsports-2013-093218.
Tenforde AS, Carlson JL, Chang A, et al. Association of the female athlete triad risk assessment stratification to the development of bone stress injuries in collegiate athletes. Am J Sports Med. 2016;45:302–10. https://doi.org/10.1177/0363546516676262.
Matheson GO, Clement DB, McKenzie DC, et al. Stress fractures in athletes. A study of 320 cases. Am J Sports Med. 1987;15:46–58.
Brukner P, Bradshaw C, Khan KM, et al. Stress fractures: a review of 180 cases. Clin J Sport Med. 1996;6:85–9.
Patel DS, Roth M, Kapil N. Stress fractures: diagnosis, treatment, and prevention. Am Fam Physician. 2011;83:39–46.
Ohta-Fukushima M, Mutoh Y, Takasugi S, et al. Characteristics of stress fractures in young athletes under 20 years. J Sports Med Phys Fitness. 2002;42:198–206.
Nattiv A, Kennedy G, Barrack MT, et al. Correlation of MRI grading of bone stress injuries with clinical risk factors and return to play: a 5-year prospective study in collegiate track and field athletes. Am J Sports Med. 2013;41:1930–41. https://doi.org/10.1177/0363546513490645.
Snyder RA, Koester MC, Dunn WR. Epidemiology of stress fractures. Clin Sports Med. 2006;25:37–52. https://doi.org/10.1016/j.csm.2005.08.005.
Iwamoto J, Takeda T. Stress fractures in athletes: review of 196 cases. J Orthop Sci. 2003;8:273–8. https://doi.org/10.1007/s10776-002-0632-5.
Maquirriain J, Ghisi JP. The incidence and distribution of stress fractures in elite tennis players. Br J Sports Med. 2006;40:454–9. ; discussion 459. https://doi.org/10.1136/bjsm.2005.023465.
Ekstrand J, Torstveit MK. Stress fractures in elite male football players. Scand J Med Sci Sports. 2012;22:341–6. https://doi.org/10.1111/j.1600-0838.2010.01171.x.
Hosea TM, Hannafin JA. Rowing injuries. Sports Health. 2012;4:236–45. https://doi.org/10.1177/1941738112442484.
Pegrum J, Crisp T, Padhiar N. Diagnosis and management of bone stress injuries of the lower limb in athletes. BMJ. 2012;2511:1–8. https://doi.org/10.1136/bmj.e2511.
Kiuru MJ, Pihlajamäki HK, Ahovuo JA. Bone stress injuries. Acta Radiol. 2004;45:317–26.
Kaeding CC, Yu JR, Wright R, et al. Management and return to play of stress fractures. Clin J Sport Med. 2005;15:442–7.
Diehl JJ, Best TM, Kaeding CC. Classification and return-to-play considerations for stress fractures. Clin Sports Med. 2006;25:17–28. https://doi.org/10.1016/j.csm.2005.08.012.
Mountjoy M, Sundgot-Borgen J, Burke L, et al. The IOC consensus statement: beyond the female athlete triad--relative energy deficiency in sport (RED-S). Br J Sports Med. 2014;48:491–7. https://doi.org/10.1136/bjsports-2014-093502.
Hergenroeder AC. Bone mineralization, hypothalamic amenorrhea, and sex steroid therapy in female adolescents and young adults. J Pediatr. 1995;126:683–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Changstrom, B.G. (2020). Stress Fractures. In: Khodaee, M., Waterbrook, A., Gammons, M. (eds) Sports-related Fractures, Dislocations and Trauma. Springer, Cham. https://doi.org/10.1007/978-3-030-36790-9_33
Download citation
DOI: https://doi.org/10.1007/978-3-030-36790-9_33
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-36789-3
Online ISBN: 978-3-030-36790-9
eBook Packages: MedicineMedicine (R0)