
Abstract
Recent guidelines on cardiopulmonary resuscitation (CPR) have stressed the necessity to improve the quality of CPR. Our previous studies demonstrated the usefulness of monitoring cerebral blood oxygenation (CBO) during CPR by near-infrared spectroscopy (NIRS). The present study evaluates whether the NIRO-CCR1, a new NIRS device, is as useful in the clinical setting as the NIRO-200NX. We monitored CBO in 20 patients with cardiac arrest by NIRS. On the arrival of patients at the emergency department, the attending physician immediately assessed whether the patient was eligible for this study after conventional advanced life support and, if eligible, measured CBO in the frontal lobe by NIRS. We found that in all patients, the cerebral blood flow waveform was in synchrony with the chest compressions. Moreover, the tissue oxygenation index increased following cardiopulmonary bypass (CPB) in patients undergoing CPB, including one patient in whom CBO was monitored using the NIRO-CCR1. In addition, although the NIRO-CCR1 could display the pulse rate (Tempo) in real time, Tempo was not always detected, despite detection of the cerebral blood flow waveform. This suggested that chest compressions may not have been effective, indicating that the NIRO-CCR1 also seems useful to assess the quality of CPR. This study suggests that the NIRO-CCR1 can measure CBO during CPR in patients with cardiac arrest as effectively as the NIRO-200NX; in addition, the new NIRO-CCR1 may be even more useful, especially in prehospital fields (e.g. in an ambulance), since it is easy to carry.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Cardiopulmonary resuscitation
- Near-infrared spectroscopy
- Extracorporeal cardiopulmonary resuscitation
- Quality of cardiopulmonary resuscitation
- Veno-arterial extracorporeal membrane oxygenation
1 Introduction
Cardiac arrest is a major public health issue worldwide. Despite significant advances in the care of cardiac arrest victims, the survival rate of patients suffering from cardiac arrest remains low [1]. Recent guidelines on cardiopulmonary resuscitation (CPR) have stressed that high-quality CPR remains the key to improving the outcomes [2]. Chest compression with as few interruptions as possible is important for high-quality CPR. These guidelines indicated it may be reasonable to use physiologic parameters when feasible to monitor and optimize CPR quality, guide vasopressor therapy, and detect return of spontaneous circulation (ROSC) (Class IIb) [3]. However, these guidelines have not mentioned monitoring cerebral blood oxygenation (CBO) during CPR by near-infrared spectroscopy (NIRS) in order to improve the quality of CPR. In addition, studies have shown that extracorporeal CPR (ECPR ) using emergency cardiopulmonary bypass (CPB) could improve neurologic outcome in cases of out-of-hospital cardiac arrest [4,5,6]. According to the guidelines, in settings where it can be immediately implemented, ECPR may be considered for selected patients in whom the suspected etiology of the cardiac arrest is potentially reversible during the limited period of CPB (Class IIb) [2].
We previously reported the usefulness of monitoring CBO during CPR and ECPR by NIRS (NIRO-200NX, Hamamatsu Photonics, Japan) [7, 8]. Moreover, Koyama et al. developed the NIRO-Pulse (Hamamatsu Photonics, Japan), a mode capable of depicting changes in hemoglobin concentrations as an indicator of cerebral blood flow, and simultaneously displaying the cerebral tissue oxygenation index (TOI) [9,10,11]. However, because the NIRO-200NX is heavy and big, it is difficult to use the NIRO-200NX in prehospital setting, such as inside an ambulance. Thus, the NIRO-CCR1 (Hamamatsu Photonics, Japan) which is smaller and lighter than the NIRO-200NX was developed. The NIRO-pulse can be used not only on the NIRO-200NX, but also on the NIRO-CCR1. However, it is unclear whether the NIRO-CCR1 can measure CBO during CPR and ECPR in patients with cardiac arrest as effectively as the NIRO-200NX in clinical setting. Therefore, this study evaluates whether the NIRO-CCR1 could be as useful in the clinical setting as the NIRO-200NX.
2 Methods
2.1 Patients
In this prospective observational study, NIRS (NIRO-200NX or NIRO-CCR1) was used to measure CBO in the frontal lobe in patients with cardiac arrest transported to the emergency department (ED) at Kawaguchi Municipal Medical Center or Surugadai Nihon University Hospital. The study was approved by the Kawaguchi Municipal Medical Center Ethics Committee. The informed consent was obtained from patients or their family for this study. Patients meeting the following criteria were enrolled in this study: persistent cardiac arrest on arrival at the ED, and successful ROSC after arrival at the ED with conventional advanced life support (ALS) and/or ECPR [4, 7, 8].
2.2 Procedures
The procedures used in the present study are described in detail elsewhere [7, 8]. Briefly, on arrival at the ED, the attending physicians rapidly assessed whether the patient was eligible for this study after conventional ALS, and employed NIRS to measure CBO in the frontal lobe. ECPR was initiated when ROSC could not be achieved within 10 min of arrival of the patient at the ED.
2.3 Statistical Analysis
Data are expressed as means ± standard deviation for continuous variables. Levels of the TOI and saturation of the waveform (SnO2) were compared using the Mann-Whitney U test for continuous variables. P-values ≤0.05 were considered to be statistically significant. All analyses were performed using the SPSS software (version 25.0, J SPSS).
3 Results
Table 1 lists the characteristics of the NIRO-200NX and the NIRO-CCR1. Although the NIRO-CCR1 device is smaller and lighter than the NIRO-200NX, the internal data storage time of the NIRO-CCR1 is only 1 h. The blue, red and white waveforms obtained using the NIRO-Pulse mode on the NIRO-200NX and on the NIRO-CCR1 are displayed in real time. The blue, red and white waveforms show the delta-deoxyhemoglobin (Δ-Deoxy Hb), delta-oxyhemoglobin (Δ-Oxy Hb) and delta-total hemoglobin (Δ-total Hb) concentrations, respectively. Moreover, the TOI, SnO2 and Tempo are also displayed on the NIRO-Pulse. The SnO2 represents the ratio of Δ-Oxy Hb to Δ-total Hb (= Δ-Oxy Hb + Δ-Deoxy Hb), and Tempo represents the pulse rate.
We monitored CBO in 20 patients with cardiac arrest by NIRS (using the NIRO-200NX in 19 patients and the NIRO-CCR1 in one patient). Of these patients, after arrival at the ED, ROSC was achieved with conventional ALS in two patients and after ECPR in the remaining 18 patients. The mean age of the study population was 60.7 ± 14.2 years, and 95.0% was male.
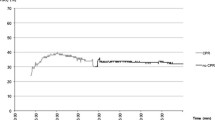
Figure 1 shows typical profiles of patients in whom we employed the NIRO-200NX (Fig. 1a) or the NIRO-CCR1 (Fig. 1b) to measure CBO in the frontal lobe. In all patients, the cerebral blood flow waveform was in synchrony with the chest compressions. Moreover, the TOI increased following implementation of CPB in patients in whom CPB was performed, including the patient in whom CBO was monitored using the NIRO-CCR1. Figure 1b shows that the pulse rate (Tempo) was not always detected, despite detection of the cerebral blood flow waveform, and that the TOI and SnO2 were significantly higher after implementation of CPB than before (TOI before implementation of CPB versus (vs.) after: 36.2 ± 1.61% vs. 52.9 ± 3.84%, P < 0.001; SnO2 before implementation of CPB vs. after: 27.4 ± 8.29% vs. 54.6 ± 23.4%, P < 0.001).

(a) NIRO-200NX and (b) NIRO-CCR1 to measure cerebral blood oxygenation during cardiopulmonary resuscitation (CPR) and extracorporeal CPR. (b) The upper figure shows the total hemoglobin concentration, the oxidized hemoglobin and the deoxidized hemoglobin of the cerebral blood flow. Hb, hemoglobin; TOI, tissue oxygenation index; SnO2, saturation of the waveform; Tempo, pulse/compression rate; ALS, advanced life support; CPB, cardiopulmonary bypass
4 Discussion
This study suggests that CBO during CPR and ECPR in patients with cardiac ar-rest might be measured as effectively with the NIRO-CCR1 as with the NIRO-200NX. That is, synchrony of the cerebral blood flow waveform with the chest compressions and a significant increase in the TOI after implementation of CPB were observed with both the NIRO-200NX and the NIRO-CCR1. When establishing CPB, emergency cannulation of a femoral vein and artery is usually performed under ultra-sonographic or fluoroscopic guidance. However, in EDs and prehospital setting [12], cannulation often has to be performed without ultrasonographic or fluoroscopic guidance. In these situations, it is often difficult to perform cannulation safely. Cannulation can be deemed as successful by confirming a significant increase in the TOI using NIRS after the establishment of CPB. In fact, in our patient in whom CBO was monitored using the NIRO-CCR1, CPB was established without ultrasonographic or fluoroscopic guidance (Fig. 1b).
In addition, the NIRO-Pulse could display the pulse rate (Tempo) in real time; however, we found that Tempo was not always detected, despite detection of the cerebral blood flow waveform. This suggests that some of the chest compressions may not have been effective; this implies that that the NIRO-Pulse may also be useful to assess the quality of CPR. Because recent guidelines recommend that, in adult victims of cardiac arrest, rescuers perform chest compressions at the rate of 100 to 120/min [2], it is important for rescuers to know the number of useful chest compressions per minute. Thus, it is important and necessary for rescuers to measure Tempo using the NIRO-Pulse during CPR in order to perform high-quality CPR. The NIRO-CCR1 can only be used together with the NIRO-Pulse.
The NIRO-CCR1 allows noninvasive, continuous monitoring of changes of CBO with high time resolution and is easy to carry. Therefore, the NIRO-CCR1 may be even more useful, especially in prehospital setting, such as inside an ambulance. On the other hand, the internal data storage time of the NIRO-CCR1 is only 1 h. Some studies suggest that it is important to observe TOI changes over several hours after the establishment of CPB [7, 10, 13]. Future improvements of the NIRO-CCR1 may help to resolve this issue.
There are several limitations to our study. First, this study was not a randomized controlled trial. Second, our findings should be considered preliminary because of the small sample size: there were only 20 patients in the present study and only one patient used NIRO-CCR1. Therefore, from now on, it is necessary to monitor CBO using the NIRO-CCR1 by more physicians and emergency medical responders in more cardiac arrest patients, especially in the prehospital setting.
5 Conclusions
On the basis of these findings, we conclude that the NIRO-CCR1 can measure CBO during CPR and ECPR in patients with cardiac arrest. Furthermore, the NIRO-CCR1 may be even more useful than the NIRO-200NX, especially in prehospital setting, as the device is easy to carry.
References
Meaney PA, Bobrow BJ, Mancini ME et al (2013) Cardiopulmonary resuscitation quality: [corrected] improving cardiac resuscitation outcomes both inside and outside the hospital: a consensus statement from the American Heart Association. Circulation 128:417–435
Neumar RW, Shuster M, Callaway CW et al (2015) Part 1: executive summary: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 132:S315–S367
Link MS, Berkow LC, Kudenchuk PJ et al (2015) Part 7: adult advanced cardiovascular life support: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 132:S444–S464
Nagao K, Kikushima K, Watanabe K et al (2010) Early induction of hypothermia during cardiac arrest improves neurological outcomes in patients with out-of-hospital cardiac arrest who undergo emergency cardiopulmonary bypass and percutaneous coronary intervention. Circ J 74:77–85
Maekawa K, Tanno K, Hase M et al (2013) Extracorporeal cardiopulmonary resuscitation for patients with out-of-hospital cardiac arrest of cardiac origin: a propensity-matched study and predictor analysis. Crit Care Med 41:1186–1196
Sakamoto T, Morimura N, Nagao K et al (2014) Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out-of-hospital cardiac arrest: a prospective observational study. Resuscitation 85:762–768
Yagi T, Nagao K, Sakatani K et al (2013) Changes of cerebral oxygen metabolism and hemodynamics during ECPR with hypothermia measured by near-infrared spectroscopy: a pilot study. Adv Exp Med Biol 789:121–128
Yagi T, Nagao K, Kawamorita T et al (2016) Detection of ROSC in patients with cardiac arrest during chest compression using NIRS: a pilot study. Adv Exp Med Biol 876:151–157
Koyama Y, Wada T, Lohman BD et al (2013) A new method to detect cerebral blood flow waveform in synchrony with chest compression by near-infrared spectroscopy during CPR. Am J Emerg Med 31:1504–1508
Koyama Y, Mizutani T, Marushima A et al (2017) Cerebral tissue oxygenation index using near-infrared spectroscopy during extracorporeal cardio-pulmonary resuscitation predicted good neurological recovery in a patient with acute severe anemia. Intern Med 56:2451–2453
Koyama Y, Inoue Y, Hisago S et al (2018) Improving the neurological prognosis following OHCA using real-time evaluation of cerebral tissue oxygenation. Am J Emerg Med 36:344 e345–344 e347
Lamhaut L, Hutin A, Deutsch J et al (2017) Extracorporeal cardiopulmonary resuscitation (ECPR) in the prehospital setting: an illustrative case of ECPR performed in the louvre museum. Prehosp Emerg Care 21:386–389
Ehara N, Hirose T, Shiozaki T et al (2017) The relationship between cerebral regional oxygen saturation during extracorporeal cardiopulmonary resuscitation and the neurological outcome in a retrospective analysis of 16 cases. J Intensive Care 5:20
Disclosure
The authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Yagi, T. et al. (2020). Usefulness of a New Device to Monitor Cerebral Blood Oxygenation Using NIRS During Cardiopulmonary Resuscitation in Patients with Cardiac Arrest: A Pilot Study. In: Ryu, PD., LaManna, J., Harrison, D., Lee, SS. (eds) Oxygen Transport to Tissue XLI. Advances in Experimental Medicine and Biology, vol 1232. Springer, Cham. https://doi.org/10.1007/978-3-030-34461-0_41
Download citation
DOI: https://doi.org/10.1007/978-3-030-34461-0_41
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-34459-7
Online ISBN: 978-3-030-34461-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)