
Abstract
Introduction: Although central venous catheters (CVCs) provide reliable vascular access, there are several risks linked with their use, with the rates of central-line-associated bloodstream infections (CLABSIs) being the most important ones. CLABSIs have a big impact on mortality rates and health care costs. The aim of this study was to investigate the incidence of obesity in the development of central venous catheter infections.
Material and Method: This is a prospective, observational study. The data were collected in the ICUs of three major hospitals in Greece, over a period of 18 months. Totally, 744 patients were included in the study.
Results: The study included 744 ICU patients aged 63.6 ± 16.6 years. The Apache II score and MODS score of patients were 23.3 ± 6.9 and 7.5 ± 3.8, respectively. Totally, 5.426 catheter-days were included in the study. Among the 722 CVCs, 178 (24.7%) were CLABSIs. The incidence rate of CVC-associated CLABSI was 22.48 infections per 1000 catheter-days. CLABSI was significantly predicted by the BMI (p = 0.001), by the diabetes mellitus as comorbidity (p = 0.013), by the doctors’ experience (p = 0.001), by the type of CVC (p = 0.001) and CVC site (p = 0.001), by the number of efforts for CVC insertion (p = 0.009), by the catheterization’s duration (p = 0.001) and by the MODS score (p = 0.001).
Conclusions: Better staff training focused on care bundles preventing infections, better medical training focused on less efforts for CVC insertion, and the use of Ultrasounds during the CVC insertion may be the main factors that can lead to lower CLABSI rates in obese patients. Further research relating CLABSI rates in ICU patients and obesity is needed.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
The central venous catheters (CVCs) are an integral part of the care of adult patients in Intensive Care Units (ICU) , providing vascular access for the administration of fluids, drugs, nutrition, blood products as well as hemodynamic monitoring and blood sampling (Kim et al. 2011). Approximately 48% of all ICU patients have central venous catheters or about 15 million catheterization days per year (Center for Disease Control and Prevention 2011). Although central venous catheters provide reliable vascular access, there are several risks linked with their use. The most common risk associated with the existence of central venous catheters is the CLABSI, caused by microorganisms that colonize the external surface of the device or the lumen through which the fluid passes when the device is inserted or during its use (Institute for Healthcare Improvement 2012).
CLABSIs are defined as laboratory-confirmed blood-borne infections associated with the presence of central venous catheters, provided that the central venous catheter has been placed at least 48 h prior to the onset of the infection with no apparent source other than the CVC (O’Grady et al. 2011). The estimated CLABSI rate in ICU in the United States is 0.8 per 1000 center line days (Hallam et al. 2018). According to the Institute for Health Care Improvement, in 2012, about 90% of all CLABSIs occurred due to the use of central venous catheters, resulting in increased hospitalization duration, increased costs, and increased mortality rates. CLABSIs are among the most important hospital infections in the ICU, accounting for 10–20% of all hospital-acquired infections (Bianco et al. 2013). These infections are the leading cause of death with reported mortality rates in adult ICU patients from 12% to 25% (Marra et al. 2010). CLABSIs are an important source of morbidity and mortality that in the United States account for about 28,000 annual deaths (Lissauer et al. 2012). In addition, CLABSIs contribute to a significant financial burden on health care institutions by extending the duration of hospitalization for about seven days at an additional cost of approximately $ 45,000 (Lissauer et al. 2012).
CLABSIs can usually be prevented by applying the indicated guidelines (Kusek 2012). Therefore, many Health Organizations have made efforts to reduce the incidence of CLABSIs. Such changes include the use of cessation-based insertion links (Lissauer et al. 2012) and in particular (1) hand hygiene before the use of chlorhexidine for skin antisepsis, (2) avoidance of the femoral vein for insertion of the catheter, and (3) direct removal of the catheters, when it is no longer advisable to use them (Agency for Healthcare Research and Quality 2013).
The purpose of this study was to investigate the incidence of obesity in the development of central venous catheter infections.
2 Materials and Methods
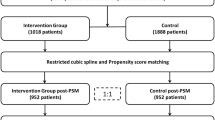
This is a prospective, observational study. The data were collected in the ICUs of three major hospitals in Greece during a period of 18 months. Totally, 744 patients were included in the study.
2.1 Exclusion Criteria
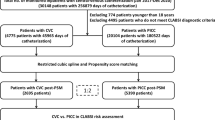
During the study, 224 patients were excluded. The exclusions criteria were:
-
Catheterizations performed in patients who died within 48 h of their admission to ICU (n = 211)
-
Patients whose BMI could not be calculated (n = 8)
-
Patients who did not have a disease severity score (APACHE II, MODS) (n = 5)
Patient demographics, body mass index (BMI), APACHE II, and MODS score were recorded. The patient’s height was measured from his/her bed with a specific measuring scale, while his/her weight was measured by a special crane scale that existed as equipment in the ICU. In order to ensure the validity and reliability of the measurements, the cranes in all three hospitals were calibrated daily.
An attempt to introduce the central venous catheter was considered when the catheter’s needle punctured the patient’s skin. As soon as the doctor pierced the patient’s skin, time recording began. In order to ensure the validity of the measurements and to ensure the reliability of the time measurement, the same timer was used in the three ICUs.
2.2 Statistical Analysis
The statistical analysis was carried out using IBM SPSS 21.0 statistical package. Categorical data are presented in absolute and relative frequencies. Numerical data are described by median and standard deviation (SD). Kolmogorov–Smirnov test was used for the normality of the distribution of numerical variables. Differences in categorical variables were determined by a chi square test and by Fisher’s exact test, while Student’s t-test was used to test the differences in numerical variables. Also, the differences in variables that deviate from normal distribution were tested by the Mann–Whitney U test. All P values were two-sided, and the level of significance was set at p = 0.05. Multivariate regression binary logistic analysis was used for the predictors of CLABSIs .
3 Results
The study included 744 ICU patients aged 63.6 ± 16.6 years. The Apache II score and MODS score of patients were 23.3 ± 6.9 and 7.5 ± 3.8, respectively. Totally, 512 (68.8%) patients were admitted to ICU from a clinic, 188 (25.3%) patients from the Emergency Department and 44 (5.9%) patients from another ICU. The demographics and clinical characteristics of the patients are presented in Table 1.
The number of doctors’ attempts to place the central venous catheter was 3.4 ± 2.8, while the catheterization duration was 11.8 ± 11.3 min. The days of hospitalization on catheterization were 9.6 ± 9.6 days.
Totally, 5.426 catheter-days were included in the study. Among the 722 CVCs, 178 (24.7%) were CLABSIs. The incidence rate of CVC-associated CLABSI was 22.48 infections per 1000 catheter-days.
The main cause of CLABSI was pseudomonas (29.4%), followed by Acinetobacter (22.2%), Klebsiella (10.3%), Candida (9.3%), enterococcus (7.2%), E. Coli (6.7%), Staphilococcus (5.2%), Proteus (4.6%), MRSA (2.1%), Pneumoniococcus (1.5%), and Hemophilus (1.5%).
The duration of hospitalization of patients in the ICU was 19.4 ± 12.8 days and the total hospitalization was 24.8 ± 12.8 days. Of all the patients, 316 (43.8%) survived and 406 (56.2%) died. At 28 days, 204 (28.3%) patients were discharged, 256 (35.5%) patients have died, and 262 (36.3%) remained in the hospital.
Among the CLABSI and no CLABSI groups, we found statistically significant difference concerning the diagnosis, BMI, comorbidity, CVC site, CVC type, N attempts for catheterization, doctors’ experience, catheterization duration, MODS score, LOS ICU, total LOS, as well as the outcome and 28 days’ outcomes. The results of the univariate analysis are shown in Table 2.
The variables that were related to the CLABSIs were entered into the multivariate binary regression model . CLABSI was significantly predicted by the BMI (p = 0.001), by the diabetes mellitus as comorbidity (p = 0.013), by the doctors’ experience (p = 0.001), by the type of CVC (p = 0.001) and the CVC site (p = 0.001), by the number of efforts for CVC insertion (p = 0.009), by the catheterizations’ duration (p = 0.001) and by the MODS score (p = 0.001). The findings of binary regression are shown in Table 3.
4 Discussion
The findings of this study showed high incidence rate of CLABSI (22.48 infections per 1000 catheter-days) among ICU patients in Greece, while the CLABSI rate in intensive care units (ICUs) in the United States is estimated to be 0.96 per 1000 central line days (Furuya et al. 2016). The main reason for the higher rates in our study may be due to doctors’ low experience inducting the CVC and the nonuse of Ultrasound during the procedure.
Furthermore, this study showed that among the CLABSI and no CLABSI groups there is statistically significant difference concerning the diagnosis, BMI, comorbidity, CVC site, CVC type, N attempts for catheterization, doctors’ experience, catheterization duration, MODS score, LOS ICU, total LOS as well as the outcome and 28 days’ outcomes. According to the multivariate binary regression model, CLABSI was significantly predicted by the BMI (p = 0.001), by the diabetes mellitus as comorbidity (p = 0.013), by the doctors’ experience (p = 0.001), by the type of CVC (p = 0.001), CVC site (p = 0.001), by the number of efforts for CVC insertion (p = 0.009), by the catheterization’s duration (p = 0.001) and by the MODS score (p = 0.001). In literature, there is a lack of studies relating obesity and the development of central venous catheter infections.
Pepin et al. (2015) conducted a retrospective longitudinal study of ICU patients, aged 18 years and older, who had central venous catheters. They found that the number of central line days was a predictor of CLABSI, consistent with the findings of our study. Lissauer et al. (2012), over a period of 2 years, studied critically ill surgical patients admitted to the intensive care unit (ICU) for ≥4 days. According to their findings, patients who developed CLABSI were (i) more likely to be male, (ii) more critically ill on ICU admission, (iii) more likely admitted to the emergency surgery service, and (iv) they had an association with reopening of recent laparotomy. The sample of said study consisted of surgical patients only, while the sample of our study consists of general patients in the ICU.
Tao et al. (2015) evaluated the efficacy of the topical administration, among others, of mupirocin in CVC care to prevent CLABSI in patients with major burns. They found that administering mupirocin, increasing the frequency of insertion-site care and avoiding cannulation at the burn site, reduced skin colonization at the CVC insertion site. Topical administration of mupirocin significantly reduced both the bacterial colonization rate at CVC tips and the incidence of CLABSI. In our study, we did not examine the correlation of similar factors affecting the prevention of CLABSI.
Dahan et al. (2016) conducted a retrospective matched case–control study of infants admitted to the neonatal ICUs of two hospitals in Canada. They found that active intraabdominal pathology, abdominal surgery in the prior 7 days, male sex, and ≥3 heel punctures were related to CLABSI. According to a multivariate matched analysis, intraabdominal pathology, and ≥3 heel punctures remained independent risk factors for CLABSI. Their findings cannot be compared with the findings of our study because of the different population characteristics (infants vs. adults).
Kaye et al. (2014) tried to quantify the impact of nosocomial bloodstream infections (BSI) on older patients, including mortality, length of stay (LOS), and costs attributed to BSI. They found that Nosocomial BSI in older adults was significantly associated with increases in 90-day mortality, increased LOS, and increased costs of care. Although the general conclusions of their study were similar with ours, we must point out that their sample did not consist of ICU patients.
4.1 Limitations
The limitations of the present study are the small number of the patients’ sample and the fact that the study was conducted in the ICUs of only two hospitals.
5 Conclusions
CLABSI rates seem to be higher in Greece in comparison to other countries. Better staff training focused on care bundles preventing infections, better medical training focused on less efforts for CVC insertion, and use of Ultrasounds during the CVC insertion may be the main factors that can lead to lower CLABSI rates in obese patients. Finally, further research relating CLABSI rates in ICU patients and obesity is needed.
References
Agency for Healthcare Research and Quality (AHRQ) (2013) Making health care safer II: an updated critical analysis of the evidence for patient safety practices – Executive report. Available at http://www.ahrq.gov/research/findings/evidence-based-reports/ptsafetysum.html
Bianco A, Coscarelli P, Nobile C, Pileggi C, Pavia M (2013) The reduction of risk in central line-associated bloodstream infections: knowledge, attitudes, and evidence-based practices in health care workers. Am J Infect Control 41(2):107–112
CDC (2011) Guidelines for the prevention of intravascular catheter-related infections. Available from: http://www.cdc.gov/hicpac/pdf/guidelines/bsi-guidelines-2011.pdf
Dahan M, O’Donnell S, Hebert J, Gonzales M, Lee B, Chandran A, Woolsey S, Escoredo S, Chinnery H, Quach C (2016) CLABSI risk factors in the NICU: potential for prevention: a PICNIC study. Infect Control Hosp Epidemiol 37(12):1446–1452
Furuya E, Dick A, Herzig C, Pogorzelska-Maziarz M, Larson E, Stone P (2016) Central line–associated bloodstream infection reduction and bundle compliance in intensive care units: a National Study. Infect Control Hosp Epidemiol 37(07):805–810
Hallam C, Jackson T, Rajgopal A, Russell B (2018) Establishing catheter-related bloodstream infection surveillance to drive improvement. J Infect Prev 19(4):160–166
Institute of Healthcare Improvement (IHI) (2012) How-to-guide: prevent central line associated bloodstream infections (CLABSI). Retrieved from http://www.ihi.org/knowledge/Pages/Tools/HowtoGuidePreventCentralLineAssociatedBloodstreamInfections.aspx
Kaye K, Marchaim D, Chen T, Baures T, Anderson D, Choi Y, Sloane R, Schmader K (2014) Effect of nosocomial bloodstream infections on mortality, length of stay, and hospital costs in older adults. J Am Geriatr Soc 62(2):306–311
Kim J, Holtom P, Vigen C (2011) Reduction of catheter-related bloodstream infections through the use of a central venous line bundle: epidemiologic and economic consequences. Am J Infect Control 39(8):640–646
Kusek L (2012) Preventing central line-associated bloodstream infections. J Nurs Care Qual 27(4):283–287
Lissauer M, Leekha S, Preas M, Thom K, Johnson S (2012) Risk factors for central line-associated bloodstream infections in the era of best practice. J Trauma Acute Care Surg 72(5):1174–1180
Marra A, Cal R, Durão M, Correa L, Guastelli L, Moura D, Edmond M, dos Santos O (2010) Impact of a program to prevent central line-associated bloodstream infection in the zero tolerance era. Am J Infect Control 38(6):434–439
O’Grady N, Alexander M, Burns L, Dellinger E, Garland J, Heard S, Lipsett P, Masur H, Mermel L, Pearson M, Raad I, Randolph A, Rupp M, Saint S (2011) Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis 52(9):e162–e193
Pepin C, Thom K, Sorkin J, Leekha S, Masnick M, Preas M, Pineles L, Harris A (2015) Risk factors for central-line–associated bloodstream infections: a focus on comorbid conditions. Infect Control Hosp Epidemiol 36(04):479–481
Tao L, Zhou J, Gong Y, Liu W, Long T, Huang X, Luo G, Peng Y, Wu J (2015) Risk factors for central line-associated bloodstream infection in patients with major burns and the efficacy of the topical application of mupirocin at the central venous catheter exit site. Burns 41(8):1831–1838
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this paper

Cite this paper
Tsolakoglou, I. et al. (2020). Central-Line-Associated Bloodstream Infections (CLABSIs) Incidence and the Role of Obesity: A Prospective, Observational Study in Greece. In: Vlamos, P. (eds) GeNeDis 2018. Advances in Experimental Medicine and Biology, vol 1196. Springer, Cham. https://doi.org/10.1007/978-3-030-32637-1_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-32637-1_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-32636-4
Online ISBN: 978-3-030-32637-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)