
Abstract
Accurate manual execution of a pre- or intraoperatively generated plan is an essential ability of surgeons and can be related to a successful outcome of a surgery. Therefore, surgeons regularly need to control multiple parameters simultaneously which increases control complexity, particularly if the information has to be derived and fused from multiple reference frames (e.g. displays). In master-slave or cooperative robotic settings haptic assistances can be provided to facilitate manual control of e.g. milling tasks. Haptic assistances present the information in the human hand reference frame and therefore can make mental transformation obsolete. Additionally, in contrast to autonomous robotic milling, the surgeon remains in the control loop and is able to customize the plan according to his expertise and intraoperative requirements. This paper experimentally investigates effects on usability of different haptic assistances in separate degrees of freedom during a multiple parameter control task. Subjects had to apply a force and follow a path with a constant velocity, while different levels of haptic assistance were provided. Results indicate that each assistance provides a statistically significant improvement with respect to the associated measure (i.e. force, position, velocity) and the task-associated perceived workload is reduced. Consequently, haptically assisted milling allows for an efficient control of milling parameters during surgery whose performance lies in between completely manual and autonomous robotic execution while keeping the surgeon in the control loop.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Manual guidance of surgical instruments is a multidimensional sensomotoric control task, which varies in complexity and often involves the control of multiple parameters simultaneously. Dynamic control parameters include forces, to avoid damage of sensitive tissues, position and orientation along trajectories of motion, which vary in their geometric complexity, as well as velocity (e.g. to comply with optimal milling parameters of bone) [1, 2].
However, complexity of control increases with every additional parameter that needs to be controlled. Therefore, while tasks with two degrees of freedom (DOF) are still relatively easy to perform, tasks with three DOFs are already challenging (e.g. riding a bike) and five DOFs tasks (e.g. riding a unicycle) already need a comparably high amount of practice and induce higher workloads [3]. Workload associated with sensomotoric tasks also depends on the complexity of mental transformations necessary to process the perceived input information (e.g. from different reference frames) to generate an appropriate manual response, e.g. in case of eye-hand-coordination of visually controlled surgical navigation tasks [2, 4]. One way to reduce task complexity is to provide haptic guidance or virtual fixtures respectively. Haptic devices (in contrast to visual guidance) present guidance information in the human hand reference frame and therefore can make mental transformation obsolete. A study [5] showed that usability (efficiency, effectiveness, user satisfaction) in typical surgical instrument motion control tasks can be affected by incorporation of different haptic assistance modes. Thereby, improvements also depend on the number of tasks that are superimposed. If there is solely one task, tracking a trajectory, improvements can be seen with respect to efficiency (mean velocity of movement) or the task associated perceived workload. If participants have to control two parameters simultaneously, tracking a trajectory and applying a constant force, improvements with respect to efficiency cannot be seen, however, effectiveness improvements (mean deviation from trajectory) are observed.
For accurate and efficient milling of bone e.g. in orthopedics or craniofacial surgery [6] apart from tool pose, velocity control of the movement is crucial. Milling velocity influences the efficiency of the milling process as well as (in combination with the tool revolution speed and geometry) milling forces or temperature rise respectively which can lead to bone damage [7]. Reported feed rates in literature vary between 2–82.5 mm/s [7, 8]. Whereas dynamic control of all relevant milling parameters (e.g. position, force, feed rate, …) for efficient bone milling can be a major benefit of autonomous robotic milling, manual motion control requires additional guidance cues.
There have already been efforts to give haptic guidance information on movement velocities without a specific trajectory that needs to be followed [9, 10]. Another work investigates tracking of a trajectory with a specific velocity profile [11] which showed promising results, however, lacked a comprehensive user study. So far no user study including multiple subjects has been performed to statistically evaluate benefits of haptic assistance to track a trajectory with a defined velocity. With regard to robotic surgery sometimes not only position and velocity along a trajectory is important but also the applied force. One example is the control of the milling depth along the inner cortical layer of skull bone on basis of force sensor information in a master-slave robot setting to preserve underlying sensitive structures in craniofacial surgery [6]. Therefore, we investigated if haptic assistance can improve usability of a control task with three parameters position, velocity and force, in the context of robotic surgery.
2 Materials and Methods
A Phantom OMNI (SensAble Technologies Inc., Wilmington, MA, USA) haptic device was used in association with Matlab Simulink (The MathWorks Inc., Natick, MA, USA) and the real-time control software QUARC (Quanser, Markham, ON, Canada).
An experiment was designed such that subjects had to control three parameters in separate degrees of freedom simultaneously, which are:
-
Applying a constant force of 1.5 N in the depth direction orthogonal to the main visual plain,
-
tracking a 2D trajectory in the main visual plane, and
-
maintaining a constant velocity of 15 mm/s along the trajectory.
Furthermore, four haptic modes were designed for the experiments which consecutively introduce assistance in additional degrees of freedom to reduce the complexity of the task. The different haptic modes and their assisted DOFs are listed in Table 1.
Thereby, haptic feedback concerning the force application (Mode F) was implemented using a unidirectional PD controller. Haptic assistance based on the deviation from the path (Mode P) was implemented using a proxy method to avoid skipping of the reference point along the trajectory in association with a PD controller [12]. Velocity assistance (Mode V) was implemented using a PD controller on the current velocity whose force output was limited to 1 N to avoid an uncomfortable strong pull along the trajectory. All PD gains were tuned experimentally to suit the different assistances.
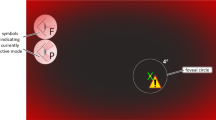
During experiments users received a graphical representation of the scene which can be seen in Fig. 1, which displayed the experimental path (inspired by a milling path) and the currently active assistance mode. Additionally, several visual elements (Table 2) were implemented such that all control parameters could also be perceived visually.

Graphical user interface (GUI) during the experiments (labeling of ∆v is not part of the GUI and only inserted here to support understanding). (Color figure online)
The experimental workflow consisted of a tutorial which all participants underwent first to accustom to the different assistance modes until they were confident. During experiments participants were first haptically guided to the start point of the trajectory. Afterwards, they were asked to apply the target force of 1.5 N supported by a randomly selected assistance mode. As soon as they were ready to start recording they pressed the space bar of the computer keyboard and started the task. Each participant performed the task with every haptic mode resulting in four test runs for each participant.
Dependent variables for the experiments were chosen based on usability evaluation criteria for medical electrical equipment defined in DIN EN 60601-1-6 and constituted of:
-
Effectiveness
-
Mean absolute deviation from path
-
Mean absolute force deviation
-
Mean absolute velocity deviation
-
-
User satisfaction
-
Perceived Workload obtained by the NASA-TLX questionnaire
-
Thereby, participants completed the NASA-TLX rating scales after each run and the NASA-TLX source of workload questionnaire after all runs were completed. Efficiency variables were not evaluated as a fixed tracking velocity was specified.
10 right-handed subjects took part in the experiments consisting of 6 males and 4 females. Subjects were aged between 22 and 43 and had a high technical affinity demonstrated by high ATI scores (Mean = 5.14, STD = 0.54) [13]. Furthermore, introductory questionnaires showed that on average subjects perfom tasks requiring high manual dexterity (e.g. playing computer games/an instrument, sewing) once a week.
3 Results
Statistical evaluation was done using analysis of variance (ANOVA) with a post-hoc test using the Tukey-Kramer method. In Figs. 2 and 3 statistically significant differences (α = 0.05) are marked with (*), while higher significance levels of p < 0.01 and p < 0.001 are marked with (**) and (***) respectively. Boxplots are used for representation of the results, thereby the central line indicates the median, bottom and top edges of the box represent the 25th and 75th percentiles, the whiskers display the most extreme data points and outliers are marked with the “+” symbol.

Mean absolute force deviation [N] applied in depth direction (left) and mean absolute deviation [mm] from the path (right) in directions of the graphical representation (*: p < 0.05; **: p < 0.01; ***: p < 0.001).

Mean absolute velocity deviation [N] in path direction (left) and TLX Index (right) obtained by questionnaire (*: p < 0.05; **: p < 0.01; ***: p < 0.001).
Figure 2 (left) illustrates the mean absolute force deviation depending on the different assistance modes. A statistically significant difference is observed (F(3, 36) = 24.62, p < 0.001). Furthermore, the post-hoc test reveals a difference between “No” and all other modes (p < 0.001).
The mean absolute path deviation can be seen in Fig. 2 (right) and statistically significant differences are observed (F(3, 36) = 6.53, p = 0.0012). Additionally, the post-hoc test indicates a difference between modes “No” and “F + P” (p = 0.0063) and modes “No” and “F + P + V” (p = 0.0032). The p-values for comparison of modes “F” and “F + P” or “F + P + V” are p = 0.1433 and p = 0.0861 respectively.
Figure 3 (left) shows the mean absolute velocity deviation for different assistance modes for which a statistically significant difference is also proven (F(3, 36) = 5.66, p = 0.0028). Moreover, the post-hoc test reveals a difference between modes “No” and “F + P + V” (p = 0.0013). The p-values for comparison of modes “F + P + V” and “F” or “F + P” are p = 0.077 and p = 0.093 respectively.
Results of the TLX ratings are illustrated in Fig. 3 (right) and a statistically significant difference is proven (F(3, 36) = 4.91, p = 0.0058). The post-hoc test reveals additionally that there is a difference between modes “No” and “F + P” (p = 0.042) and modes “No” and “F + P + V” (p = 0.004). The P-value for comparison of modes “No” and “F” is p = 0.1662.
4 Discussion and Conclusion
In this paper, issues pertaining to human motor control of multiple parameters (force, position, velocity) during robotic surgery have been outlined. A potential solution to the associated problems is to utilize haptic assistance to reduce the complexity of the task and consequently improve human-machine system performance. Several haptic assistances have already proven effective [14]; however, so far no comprehensive user study regarding a haptic velocity assistance has been performed. An experiment has been described to evaluate the influence of different haptic assistance modes on human-machine-system performance during a multiple parameter control task.
Results show that each assistance, force, position and velocity, significantly improves human-machine-system performance of the respective measure compared to the reference mode. Furthermore, significant decreases in perceived workload can be achieved as soon as force and position are assisted.
Considering the results of the force application in detail it can be seen that the absolute force deviation improves from between 0.3 N and 0.4 N (No) to around 0.2 N (F). Thereby, the latter force is only slightly higher than the just noticeable difference found by Allin et al. [15] of approximately 10% of the base force which would be 0.15 N for our experiments. The slight difference of 0.05 N could be due to inherent delays in the perception-cognition-action chain, which are prevalent in human manual control [16].
Absolute positional deviations of the reference mode (No) between 0.5 mm and 0.6 mm are only slightly lower than literature average values for manual bone milling of eleven neurosurgeons (mean deviation 0.7 mm) [17]. As soon as haptic assistance is provided the positional deviation reduces to about 0.3 mm. Compared to an automatic robotic milling process (mean deviation 0.2 mm [8]) deviations are still slightly increased. However, keeping surgeons in the control loop reduces negative side effects such as low situational awareness, overreliance, dependency on the system and retention of skills [18]. Additionally, interactive robotic systems enable surgeons to adapt surgical plans based on their expert appraisal of the intraoperative situation, thereby increasing the versatility and robustness of robot assisted surgery. Tendencies also indicate a slight positional improvement as soon as the feedback on the force application is activated, but sample sizes were too small for statistical approval.
Average deviations with respect to velocity are around 6 mm/s in the reference mode (No) and are reduced to 4 mm/s with haptic assistance (F+P+V). This finding is in coherence with literature, however, the performed study has a low level of evidence as trials were only performed with one user [11]. Tendencies also indicate a slight improvement as soon as haptic feedback concerning the force application (F) is activated, however, sample sizes were too small for statistical approval.
For the NASA TLX perceived workload there seems to be an improvement with each additional assistance which could also be observed in [5]. Statistical approval is observed for all assistance modes that provide haptic assistance for both force and position (F+P, F+P+V). Tendencies indicate an improvement if feedback on the force application (F) is provided, but sample sizes were too small for statistical approval.
Limitations of the study include that the investigated user group did not consist of surgeons. The study was based on a computer simulation scenario, whereas the real surgical context of use could potentially induce additional constraints or boundary conditions. Knowledge of the subjects concerning the active haptic mode could have influenced their subjective workload ratings. Learning effects could have influenced results, however, due to randomization they constitute a random and not a systematic error.
All things considered, results of the presented experiment indicate that for multiparameter control tasks the execution accuracy with haptic assistance lies between the completely manual and the completely automated execution. In case of telerobotic surgery, accuracy could be further improved by motion scaling. Thereby, accuracy would largely depend on the executing slave robot. The task associated perceived workload is decreased with haptic assistance enabling the surgeon to shift his attention to higher level decisions. Consequently, haptic assistance seems to be a potential solution to improve accuracy as well as decrease complexity for the human operator while keeping him in the control loop in robotic surgery.
References
Troccaz, J., Peshkin, M., Davies, B.: Guiding systems for computer-assisted surgery: introducing synergistic devices and discussing the different approaches. Med. Image Anal. 2, 101–119 (1998)
Radermacher, K.: Computerunterstützte Operationsplanung und-ausführung mittels individueller Bearbeitungsschablonen in der Orthopädie. Shaker (1999)
Luczak, H.: Prinzipien menschlicher Informationsverarbeitung-Analytik und Gestaltung informatorisch-mentaler Arbeit. In: Luczak, H. (ed.) Arbeitswissenschaft, pp. 126–213. Springer, Heidelberg (1993). https://doi.org/10.1007/978-3-662-21634-7_7
Wickens, C.D., Hollands, J.G., Banbury, S., Parasuraman, R.: Engineering Psychology and Human Performance. Pearson, London (2013)
Schleer, P., Drobinsky, S., Radermacher, K.: Evaluation of different modes of haptic guidance for robotic surgery. IFAC-PapersOnLine 51, 97–103 (2019). https://doi.org/10.1016/j.ifacol.2019.01.035
Cunha-Cruz, V., et al.: Robot-and computer-assisted craniotomy (CRANIO): from active systems to synergistic man—machine interaction. Proc. Inst. Mech. Eng. Part H: J. Eng. Med. 224, 441–452 (2010)
Denis, K., et al.: Influence of bone milling parameters on the temperature rise, milling forces and surface flatness in view of robot-assisted total knee arthroplasty. In: International Congress Series, pp. 300–306. Elsevier (2001)
Engelhardt, M., Bast, P., Lauer, W., Rohde, V., Schmieder, K., Radermacher, K.: Manual vs. robotic milling parameters for development of a new robotic system in cranial surgery. In: International Congress Series, pp. 533–538. Elsevier (2004)
Fu, Y., Yin, H., Pan, B.: Fuzzy based velocity constraints of virtual fixtures in tele-robotic surgery. In: 2014 IEEE International Conference on Robotics and Biomimetics (ROBIO), pp. 2625–2630. IEEE (2014)
Kouskoulas, Y., Renshaw, D., Platzer, A., Kazanzides, P.: Certifying the safe design of a virtual fixture control algorithm for a surgical robot. In: Proceedings of the 16th International Conference on Hybrid Systems: Computation and Control, pp. 263–272. ACM (2013)
Pezzementi, Z.A., Okamura, A.M., Hager, G.D.: Dynamic guidance with pseudoadmittance virtual fixtures. In: ICRA, pp. 1761–1767 (2007)
Bowyer, S.A., Davies, B.L., Rodriguez, Y., Baena, F.: Active constraints/virtual fixtures: a survey. IEEE Trans. Robot. 30, 138–157 (2014). https://doi.org/10.1109/tro.2013.2283410
Franke, T., Attig, C., Wessel, D.: A personal resource for technology interaction: development and validation of the Affinity for Technology Interaction (ATI) scale. Int. J. Hum.–Comput. Interact. 35(6), 456–467 (2018)
Enayati, N., De Momi, E., Ferrigno, G.: Haptics in robot-assisted surgery: challenges and benefits. IEEE Rev. Biomed. Eng. 9, 49–65 (2016)
Allin, S., Matsuoka, Y., Klatzky, R.: Measuring just noticeable differences for haptic force feedback: implications for rehabilitation. In: Proceedings of the 10th Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems, HAPTICS 2002, pp. 299–302. IEEE (2002)
Peon, A.R., Prattichizzo, D.: Reaction times to constraint violation in haptics: comparing vibration, visual and audio stimuli. In: World Haptics Conference (WHC), pp. 657–661. IEEE (2013)
Bast, P., Engelhardt, M., Lauer, W., Schmieder, K., Rohde, V., Radermacher, K.: Identification of milling parameters for manual cutting of bicortical bone structures. Comput. Aided Surg. 8, 257–263 (2003)
Abbink, D.A., Mulder, M., Boer, E.R.: Haptic shared control: smoothly shifting control authority? Cogn. Technol. Work 14, 19–28 (2012)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this paper

Cite this paper
Schleer, P., Drobinsky, S., Hmaid, T., Radermacher, K. (2019). Haptic Modes for Multiparameter Control in Robotic Surgery. In: Shen, D., et al. Medical Image Computing and Computer Assisted Intervention – MICCAI 2019. MICCAI 2019. Lecture Notes in Computer Science(), vol 11768. Springer, Cham. https://doi.org/10.1007/978-3-030-32254-0_20
Download citation
DOI: https://doi.org/10.1007/978-3-030-32254-0_20
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-32253-3
Online ISBN: 978-3-030-32254-0
eBook Packages: Computer ScienceComputer Science (R0)