
Abstract
Currently, effective hamstring injury prevention is primarily based on exercise strategies. The FIFA 11+ is a general strength and conditioning programme that has been shown to reduce injuries in football, including hamstring injuries. Many hamstring injury prevention studies have shown that eccentric hamstring strength training can reduce the risk of sustaining a hamstring injury, with a particular emphasis in the literature on the Nordic hamstring exercise. However, exercise-based prevention can only be effective when adhered to. Meticulous planning, a gradual increase of eccentric training loads for each individual athlete and stimulating adherence through knowledge transfer are key components to make hamstring injury prevention work in a practical setting. So far, evidence from studies that have investigated stretching and plyometric interventions indicate that these interventions do not seem to be effective at reducing hamstring injuries. Research on other types of preventive strategies, such as running drills, core stability training and sports-specific training, is currently insufficient, and the value of these approaches in hamstring injury prevention remains unclear. This chapter aims to provide a detailed understanding of the available evidence for hamstring injury prevention and the practical considerations around implementing these prevention strategies.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


6.1 Introduction
‘An ounce of prevention is worth a pound of cure’, Benjamin Franklin (1706–1790) once stated. Nowadays, the definitive answer to the prevention of hamstring injuries would probably be worth gold, considering the consequences and cost for the individual and their associated team/organisation due to this most common injury type. Compounding the importance of hamstring injury prevention is the well-established knowledge that prior injury is the strongest predictor of future hamstring injury. As a result, the prevention of an initial hamstring injury can allow an individual to avoid the potential injury-reinjury cycle.
In the last few decades, worldwide initiatives have been undertaken to develop strategies for sports injury prevention. There has been an exponential increase in knowledge, research, technological developments, implementation efforts and even international conferences focusing on sports injury prevention. Consequently, an increasing amount of evidence is available for clinicians and practitioners to inform a hamstring injury prevention strategy for any individual athlete or team.
Injury prevention can be divided into primary, secondary and tertiary approaches [1]. Primary prevention relates to the prevention of the initial event. This is done by preventing exposures to hazards that cause injury, altering unhealthy behaviour and increasing resistance to injury when exposure occurs. Secondary prevention aims to reduce the impact of the injury that has already occurred. This is done through counselling about reinjury prevention and proper rehabilitation strategies. Examples of secondary hamstring injury prevention are prevention and treatment protocols that aim for optimal hamstring health and recovery with minimal risk of injury/reinjury. Tertiary prevention aims to soften the impact of an (ongoing) injury that has lasting effects. When discussing hamstring injury tertiary prevention, this relates to hamstring injury rehabilitation (Chap. 10) and if conservative rehabilitation and primary prevention fails (Chap. 13).
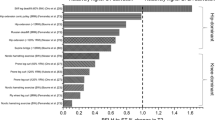
The purpose of this chapter is to inform the reader about strategies for primary prevention of hamstring injury, noting that secondary prevention and tertiary prevention will also be covered later in this book (Chaps. 9, 10, 11, 12 and 13, respectively). Given the increase in available knowledge, hamstring injury prevention strategies should be informed by the best available evidence [2]. For the sake of this chapter, the strongest available evidence, level 1a evidence, is deemed to come from systematic reviews with meta-analysis. Level 1b evidence, which is also considered high-level evidence, comes from randomised control trials (RCTs) that employ interventions aimed at reducing the rate/incidence/frequency of hamstring injury. Although of lower quality, findings from lower levels of evidence such as level 2 (cohort studies and low-quality RCTs), level 3 (case-control series), level 4 (case series and poor-quality cohort studies) and level 5 (expert opinion) will also be discussed in this chapter (see Fig. 6.1).

Levels of evidence based on [2]. Variables with a strike-through the text indicate that this variable has shown no preventative effect
Whilst many applications (i.e. massage, foam rolling, dry needling, acupuncture, taping techniques) have been popularised to varying extent in practice, there is little to no evidence of sufficient quality to support their efficacy, and these will not be discussed in this chapter.
6.2 Hamstring Injury Prevention
6.2.1 General Warm-Up
For general injury prevention, a proper warm-up is considered essential, as insufficient warm-up strategies could increase the risk of future (hamstring) injury [3]. Warm-up regimes can be applied in different formats, from running drills to targeted exercises, with or without additional weight and equipment. Ultimately, the aim of a good warm-up is to be prepared physically and mentally for an upcoming bout of activity. In a landmark study by Ekstrand et al. [4], warm-up was part of a multimodal approach, and this study was one of the first indications that a general warm-up may play an important part in reducing injuries in football. Despite this, no evidence exists on general warm-up approaches and their effects on (the prevention of) hamstring injuries. Other warm-up programmes have focused on additional strength and conditioning elements for the purpose of general injury prevention. These types of warm-up strategies have been investigated in different sports, such as balance training using a wobble board in basketball [5], and specific warm-up exercises in volleyball [6], handball [7] and basketball [8], each of which have been effective in reducing overall injury rates.
6.2.1.1 FIFA 11 and FIFA 11+ Programmes
One of the best known and widely adopted prevention programmes is the FIFA 11, a pretraining warm-up specifically designed to prevent lower limb injuries in football. In addition to fair play, the FIFA 11 programme is entirely exercise based. Initial research on the FIFA 11 showed no preventive effect for overall and hamstring injuries [9]. Subsequently, the FIFA 11 was amended to the FIFA 11+, which includes running, strength, plyometric and balance exercises, each with three levels of difficulty to allow for progression (see Fig. 6.2) [10]. The programme has traditionally been used as a warm-up in football, but recent data have shown superior efficacy when it is employed before and after training as opposed to being used as warm-up alone [11]. This is very interesting as it questions whether the effect of the FIFA 11+ is purely driven by warm-up and preactivation of certain muscle groups that lead to improvements in movement competencies or instead is driven by a dosage-specific adaptation response to strength and conditioning, resulting in reduced risk of injury.

Exercises included in the FIFA 11 and FIFA 11+ prevention programmes [10]
The impact of four large-scale (sample sizes ranging from 383 to 2540 participants) RCTs [12,13,14,15] across male and female youth football and male senior and veteran football was summarised in a systematic review and meta-analysis [10]. This meta-analysis (level 1a evidence) showed that the FIFA 11+ is an effective injury prevention tool when compared to a control group, and this effect extended to a 60% reduction in hamstring injuries across two of these cohorts (incidence rate ratio, 0.40; 95%CI, 0.19–0.84) [10]. Given the breadth of exercises included in the FIFA 11+, it is impossible to determine if the preventative effect should be attributed to a single hamstring-specific exercise such as the Nordic hamstring exercise (NHE), which is part of the FIFA 11+ (and discussed later on in this chapter), or to the programme as a whole.
In summary, level 1 evidence suggests that the FIFA 11+ warm-up programme prevents hamstring injuries in football, although more studies across different athletic cohorts are needed to support broader generalisations of these findings.
6.2.2 Eccentric Strength Training
Numerous studies, primarily conducted in different football codes and baseball, have reported that hamstring strength training [1, 16,17,18,19,20,21], especially when training with an element of eccentric overload, reduces hamstring injury risk, as long as compliance with the intervention is high [22].
6.2.2.1 Flywheel Training
The first study to indicate a preventative effect from eccentric training for hamstring injury was from Askling and colleagues and included flywheel training [17]. Such devices, introduced in the literature by Berg and Tesch in 1994 [23], involve concentric contraction to accelerate the flywheel. Eccentric actions are then required for flywheel deceleration. Actively decelerating throughout a lesser range of motion (ROM) (compared to the concentric phase), allows for a period of eccentric overload.
The Askling study was performed in two Premier League teams in Sweden and was the first, and currently the only RCT to evaluate the preventive effect of preseason hamstring flywheel strength training [17]. Players in the intervention group performed both concentric and eccentric knee flexor actions in a prone position on a Yo-Yo flywheel ergometer, with the eccentric contraction performed over approximately the final two-thirds of the ROM compared to the concentric contraction [17]. This intervention (n = 15) was performed for a total of 16 sessions across a 10-week preseason period in addition to normal team training, whilst the control group (n = 15) completed normal team training only. During a 10-month follow-up, the intervention group had significantly fewer hamstring injuries (three injuries in 15 players) than the control group (ten injuries in 15 players) [17]. Whilst the sample size in the investigation is small (compared to other RCTs in this area) and the rate of hamstring injury in the control group is exceptionally high, this study was the first to indicate that eccentric training may impact hamstring injury incidence.
6.2.2.2 Nordic, Russian or Hamstring Lowers
The earliest published mention of the NHE (Fig. 6.3) can be traced back to 1880, when George Herbert Taylor described the movement in his book Health by Exercise [24] referring to it as ‘wing-kneeling’. Despite some contention around its name, this chapter will refer to the exercise as the NHE, as this currently seems to be the most commonly adopted term globally. The exercise has alternatively been called Nordic curls, Russians, Russian leans and hamstring lowers.

The Nordic hamstring exercise
The NHE is typically performed in pairs as a body weight exercise [1, 25]. Individuals are instructed to start in a kneeling position, with the torso from the knees upwards held rigid and straight. The training partner ensures that the exercising individual’s feet are in contact with the ground by applying pressure to the heels/lower legs. The exercising individual then lowers their upper body to the ground, as slowly as possible, to maximise loading during the descent, requiring an increasingly forceful eccentric contraction of the knee flexors. The hands and arms are used to catch the forward fall and to push the individual back up to the start position after the chest has touched the ground, to minimise loading in the concentric phase.
The first study to examine the protective effects of the NHE was conducted in community-level Australian football (n = 220) [19]. This RCT exposed the intervention group to five sessions of the NHE across a 12-week period. The NHE protocol, which was delivered identically across all five sessions (see Table 6.1 for a summary of all NHE intervention prescriptions), was devised from laboratory-based studies that had shown a shift in the knee flexor torque-joint angle relationship towards longer muscle lengths after the performance of 72 repetitions of the exercise (12 sets of six reps). The intervention group (n = 114) was encouraged to complete the NHE protocol at the completion of the main team training session but prior to the cool-down, whilst the control group (n = 106) completed a number of flexibility and mobility exercises without exposure to the NHE. The intervention group did not show a reduction in hamstring injury risk compared to the control group (relative risk (RR), 1.2; 95% CI, 0.5–2.8) [19]; however, the intervention group suffered from very poor compliance (30% failed to complete a single NHE session, 53% failed to complete at least two sessions), and the primary reason reported by players was delayed-onset muscle soreness which often limited their involvement in subsequent training sessions. When comparing the rates of hamstring injury in the intervention group who completed at least two sessions to the control group, still, no effect was found (RR, 0.3; 95% CI, 0.1–1.4).
A subsequent RCT by Engebretsen and colleagues employed a more graduated 10-week NHE protocol (Table 6.1) in Norwegian soccer players who were considered at high risk of hamstring injury (based on injury history and a subjective questionnaire) [18]. Those identified as being at high risk of hamstring injury (n = 161) were randomised either into the intervention group (n = 82) or control group (n = 76), with the control group completing normal team training, but no additional intervention. The incidence of hamstring injury did not differ between these two groups (intervention group, 1.5 hamstrings injuries per 1000 h of exposure; control group 0.9 hamstring injuries per 1000 h of exposure); however, this study again suffered from low compliance, with only 21% (n = 12) of players completing more than 20 sessions of the 24 total NHE sessions. Whilst a per-protocol analysis also found no difference in hamstring injury incidence between those in the intervention group who were compliant and the control group, this analysis was limited by the small sample size.
The issues encountered by both Gabbe and colleagues [19] and Engebretsen and colleagues [18], that of poor compliance and relatively low sample sizes, were overcome by two separate studies completed in Danish and Dutch professional and amateur football cohorts [1, 20]. More than 1500 football players were included in these two RCTs (Petersen et al., [1], n = 942; van der Horst et al. [20], n = 579). Control group players performed regular team training, whereas intervention group players performed comparable NHE protocols (Table 6.1). The Danish [1] study involved a 10-week protocol followed by a weekly maintenance session across the remainder of the season, whereas the Dutch [20] study concluded NHE exposures after the 13-week intervention period. In the Danish study, coaches decided when the exercises were performed, being advised not to perform the NHE without a prior warm-up, and in the Dutch study, players were advised to perform the exercises after regular training but before the cool-down.
The Danish RCT showed that the NHE reduced the rate of new hamstring injuries by 70% (rate ratio, 0.29; 95% CI, 0.14–0.63) [1] and that the programme was even more effective for decreasing the rate of recurrent hamstring injuries, which were reduced by ~85% (rate ratio, 0.156; 95% CI, 0.05–0.53). The numbers needed to treat, defined as the number of players that need to complete the programme to prevent one injury, were 25 and 3 for new and recurrent injuries, respectively. Similarly, the Dutch RCT [20] reported a threefold reduction in the risk of hamstring injury for players who performed the NHE (rate ratio, 0.30; 95% CI, 0.12–0.73). Neither the Dutch nor Danish study reported any effect of the NHE on injury severity as the time lost to each injury was similar in experimental and control participants.
A level 2b study, which was the first to assess the effect of the NHE on hamstring injury rates specifically in soccer players, was performed in Premier League and First Division footballers from Iceland and Norway [16]. These footballers participated in a study designed as a non-RCT that investigated the preventive effect of flexibility training, with or without the addition of the NHE, on the incidence of hamstring injuries. The warm-up protocol that combined the NHE with flexibility training reduced the rate of hamstring injury risk by half (RR, 0.43; 95% CI, 0.19–0.98) compared to stretching and flexibility training of the hamstrings alone.
Some level 2b evidence is also available from other sports than football. This exemplifies the potential crossover effect to other sports. In a non-randomised cohort study in a single Major League Baseball organisation [21], there was no standardised prescription of the NHE. Instead, the strength and conditioning coaches for seven (out of a total of eight) teams (n = 243) were instructed to incorporate the NHE into daily workouts, and players were deemed compliant if they completed on average more than 3.5 repetitions of the NHE per week across the season. The control group (n = 40) was the Major League team who were not explicitly instructed to perform the NHE. Not a single hamstring injury was sustained by a compliant individual in the intervention group (31% of the intervention group were deemed compliant), whereas the control group had an injury rate of 8.8%. Across the organisation, the year-on-year days missed due to hamstring injury were reduced by 50% during the intervention season (273 days missed in the year prior to the intervention compared to 136 days missed during the intervention year) [21]. A descriptive study (level 4 evidence) in sprinters also highlighted how the injury incidence seemed to decline during consecutive seasons as agility, flexibility and NHE were added to a more traditional and concentrically based strength training programme [26].
One common criticism of the NHE is that it has not been compared to alternative exercise programmes. For example, it has been argued that the NHE may not protect athletes who already engage in conventional strength training. However, a cross-sectional cohort study (level 3 evidence) by Brooks and colleagues [27] has compared hamstring injury rates in English rugby clubs that did and did not use the NHE in addition to their strength training programmes. Teams that employed regular strength training with exercises including both concentric and eccentric phases and regular flexibility training (144 players) experienced injury rates of 7.5 (95% CI, 4.4–10.6) per 1000 h of training, while teams that employed the same methods with the addition of the NHE (200 players) experienced injury rates of 4.2 (95% CI, 2.3–6.0) per 1000 h [27]. Teams that employed the NHE did so, on average (±SD), in 65% of training weeks, with 1.3 ± 0.5 training sessions per week, 2.8 ± 0.7 sets per training session and 6.7 ± 1.5 repetitions per set. So, while there are limitations in the strength of this evidence due to study design, it does suggest the possibility that hamstring injury prevention requires a high-intensity eccentric component for it to be optimally effective.
6.2.3 Stretching
The first, and only, RCT (level 1b evidence) known to the authors focusing on the effect of stretching for hamstring injury prevention dates back to 1993, when the effectiveness of stretching exercises alongside warm-up/cool-down protocols was studied [28]. Following a 22% dropout after a 16-week intervention period, data of 326 athletes were analysed. There were no differences between intervention and control groups with regard to lower limb injuries (RR, 1.05; 95% CI, 0.22–5.13) or hamstring injuries (defined as ‘injuries on the posterior side of the upper leg’) with three hamstring injuries in both intervention and control group. However, a low compliance with the stretching exercises (47%) may have influenced the results.
Other studies into the effects of flexibility training on hamstring injury rates have been conducted, although these have a higher risk of bias due to methodological issues. For example, the preventive effect of stretching exercises was also investigated in the aforementioned study by Arnason and colleagues [16], who included one intervention arm with stretching exercises alone (without the addition of eccentric strength exercise). In addition to their standard warm-up stretching, these teams were required to use a partner-assisted contract-relax stretch for the hamstrings before sprinting or shooting exercises prior to training and matches. The teams were asked to perform this exercise three times per week during preseason and one or two times per week during the competitive season. No effect was detected from stretching alone, although a preventive effect was found in the other intervention arm that included the NHE alongside the warm-up and stretching. Hence, the results of this level 2b study suggested that the stretching component showed no preventive effect, and as such, the preventive effect was derived from the NHE alone.
A level 4 study that adopted stretching as an element of a prevention programme was performed in 2005 in Australian rules football [29]. Passive isometric hamstring stretches were performed during breaks in playing and training, particularly when players were considered to have muscle fatigue. Other elements of the intervention included more high-speed running, the removal of heavy strength training for the lower limbs and the use of ‘stooped’ running drills in which players ran while paddling a ball along the ground. Stretching was performed with the knee in varying degrees of flexion (0°, 10° and 90°) and subsequent flexion of the trunk to stretch the hamstrings. Athletes were encouraged to hold each stretch for at least 15 s. The team sustained 27 hamstring injuries in 2 years before the intervention and eight hamstring injuries in 2 years after its implementation. In addition, this led to significantly fewer matches being missed due to injury (69 in year 1–2 compared to 21 in year 3–4). Although this study provided promising results, the multifaceted nature of the intervention makes it impossible to assess the preventive effects of each of its components. Consequently, this study does not substantiate the effectiveness of stretching as a prevention strategy for hamstring injuries.
Lastly, the relationship between stretching protocols and hamstring injury incidence was investigated in a level 4 study that included the top four English professional divisions [30]. After collecting data through self-administered questionnaires, a relationship between a standard stretching protocol and hamstring injury risk was identified. It was stated that the more the stretching protocol was used, the lower the hamstring injury risk was. However, a high risk of bias due to the design of this study needs to be taken into consideration when interpreting these results.
In conclusion, the currently available scientific literature does not support the use of stretching as a means of preventing hamstring strain injury.
6.2.4 Core Stability
Core stability is specifically addressed in this chapter as it is often emphasised as important for preventing injuries in the lower limb generally and the hamstrings specifically. However, the term core stability is poorly defined in both scientific studies and clinical use. The ‘core’ can mean different things to different people, such as the ‘lumbopelvic region’, ‘lumbar spine’ and even the ‘trunk’. Furthermore, while the term ‘stability’ enjoys widespread use in the sports medicine literature, it has never been quantified in any hamstring studies [31]. Instead, researchers tend to measure strength, endurance or nothing at all and then too often assume that ‘stability’ has then been changed in the desired direction. There is, however, some preliminary level 3 evidence that certain aspects of lumbopelvic kinematics, such as exaggerated degrees of forward tilt of the pelvis and lateral trunk flexion, may be associated with an elevated hamstring injury risk [32].
6.2.5 Plyometric and Running Drill Interventions
High-speed running, accelerations and decelerations are critical for performance in many sports, but these variables are also closely linked to hamstring injury aetiology and mechanism [33]. Running drills are often included in training programmes with the belief that there is both a performance and injury prevention benefit [34].
As mentioned above, the effectiveness of the FIFA 11+ for hamstring injury prevention is possibly attributed to the NHE, but the FIFA 11+ also incorporates plyometrics and running drills. Unfortunately, there has been very little research specifically on plyometrics and running drills as an isolated means to prevent hamstring injury. To date, there is only a single RCT (level 1b evidence) in this area, conducted in 32 competitive amateur Dutch football teams (sixth division) (n = 400) [35]. The intervention consisted of 12 weeks of walking lunges, ‘tripplings’, drop lunges and bounding, after which a maintenance programme was conducted for the rest of the season. The intervention group performed these exercises after regular training, whereas the control group performed regular training without these additional exercises. Hamstring injury incidence, number and severity in the intervention group (1.12/1000 h; n = 31; lay off time, 33.0 ± 42.7 days) did not differ from the control group (1.39/1000 h; n = 26 injuries; lay-off time, 21.35 ± 12.7). Compliance with the bounding programme (metres performed/metres prescribed ×100) was 71%. These findings suggest that including walking lunges, ‘tripplings’, drop lunges and bounding to regular team training does not reduce the incidence of hamstring injury in amateur soccer, albeit with a modest level of programme compliance. It should be noted that there are a multitude of different plyometric and running drills that are utilised in practice, so further work is needed to explore the possible impact of these derivatives on hamstring injury incidence.
6.2.6 Sports-Specific Interventions
It can be argued that high levels of sports-specific fitness should enable athletes to better withstand the demands of their sport and thereby be less likely to sustain injury. The aforementioned study by Verrall and colleagues [29] is one example. Given the addition of knowledge since the publication of this study, it would seem reasonable that the intervention elements that focused on running exposures and drills that better replicated the demands of Australian football are the ‘active ingredients’ of this intervention. However, due to the lack of a control group, it is not possible to infer whether the benefits arose because of the intervention or just represented normal seasonal variations. In addition, the level 4 study design makes it impossible to determine which part or parts of the injury prevention programme were important for hamstring injury prevention and what the additional value of each element was with regard to the reduced number of hamstring injuries.
6.3 Hamstring Injury Prevention Conclusion
At present, there is level 1a evidence showing that eccentric hamstring strength training delivered via the NHE is an effective measure for hamstring injury prevention [36], so long as the exercise is implemented gradually, with appropriate volumes, and compliance is high [22]. It is important to acknowledge that most of these studies on the NHE were performed in semiprofessional and amateur football environments, so how these findings translate to other populations (e.g. elite level, woman or other sports) remains a topic for further research. However, there are some indications that including eccentric strength training in the hamstring injury prevention approach may reduce the risk of sustaining hamstring injuries in other sports such as baseball, track and field and rugby union. There is also level 1 evidence of a preventive effect from the FIFA 11+ warm-up programme, but it is unclear if the FIFA 11+ provides additional benefit to hamstring injury prevention from exercises other than the NHE. So far, the evidence from stretching studies indicates that these interventions do not seem to be effective at reducing hamstring injuries. The evidence on core stability, plyometrics, running drills and sports-specific training currently remains too limited to fully understand their effectiveness on hamstring injury prevention.
6.4 Hamstring Injury Implementation
Hamstring injury prevention programmes need to be implemented and adhered to by the targeted end users to show effectiveness [22]. Implementation of (hamstring) injury prevention in a sports environment is often a difficult task, even for athletes at increased risk of hamstring injury [18]. Multiple stakeholders can be involved such as sports associations (for rules and legislations), club boards, coaches, medical staff members, agents and so forth. In a sport setting the coach and medical staff are often the most important administrators of the prevention programme. Ultimately, however, the athlete is the end user, and his/her views with regard to the drivers and barriers for adoption of evidence-based hamstring prevention programmes need to be considered. Clearly, there are many reasons to excuse athletes from injury prevention: these include heavy game schedules, competing training priorities, poor staff communication, player and staff motivation and limited knowledge of preventive strategies [37, 38]. However, such barriers to hamstring injury prevention participation may play an important part in the lack of risk reduction seen in some sports over the last decade [39].
Research on hamstring injury prevention adherence in both professional and amateur football has shown that despite its effectiveness, the full evidence-based NHE programme (as employed by Petersen et al. [1]) is almost never adhered to by Champions League, Norwegian Premier League and Dutch amateur teams [37, 40]. Although the majority of the coaches of Champions League and Norwegian Premier League football were positive about the NHE, some reported unsatisfactory outcomes including muscle soreness and difficulty getting the players to comply with the programme. In addition, only 4% of physiotherapists, sports scientists and strength and conditioning coaches from the academies of elite soccer clubs in the United Kingdom reported using the FIFA 11+, with 9% stating the use of a modified version of the FIFA 11+ [41].
Different factors can stimulate injury prevention behaviour at the level of the athlete. Studies have shown that adoption of preventive measures can be stimulated by player motivation [37, 42], staff support [43, 44] and knowledge about injuries and injury prevention [37, 45,46,47]. For example, football players that had personally experienced an evidence-based hamstring injury prevention programme reported higher compliance at 2-year follow-up than those who had not [37]. While community football players acknowledged their effectiveness, they also believed that the injury prevention programmes need to be short in length and that some variety in drills/exercises is preferable [48]. In addition to this, athletes stated that their personal knowledge of the effectiveness of the injury prevention programme and their personal motivation are key factors for future adoption. Coaches and medical staff members reported these factors as important as well but also stated that consensus among the team staff was important for successful implementation [37].
6.4.1 Practicalities of Implementation
6.4.1.1 How Can the Attitude Towards Hamstring Injury Prevention Be Positively Stimulated?
Stimulating injury prevention adherence should be a mutual effort from all stakeholders involved. The individual athlete, the coaching staff and the medical team are often responsible for planning of sports-specific technical and medical routines for each training and match activity. From a practical perspective for the athlete, it is suggested that the NHE programme should be supervised to improve adherence [37]. Athletes need to be made aware of, or educated about, the importance of hamstring injury prevention considering the increased risk for hamstring injuries as well as the high recurrence rates after the initial injury [46, 47].
With regard to the coaches, it should be recognised that injuries have a significant influence on team performance [49]. Lower injury burden and thus higher training and match availability are associated with more points in league matches, as well as more success in Champions League and Europa League football. Further awareness of the performance benefits of injury prevention is also an important part of implementing preventive strategies and involving coaches in hamstring injury prevention. Both the FIFA 11+ programme and the NHE protocol have been shown to improve jumping and balance performance and short sprinting ability [3, 50, 51] suggesting that there is also a physical capacity benefit, which might resonate more readily with coaching staff.
For the medical staff, there is an important role to play in facilitating knowledge transfer from evidence-based medicine to end users (e.g. the athlete) and the administrators (e.g. the coaches or other members of team staff) because knowledge of the effectiveness of an intervention plays a major role in hamstring injury prevention adherence for all of these stakeholders.
6.4.1.2 When Should Prevention Exercises Be Scheduled in Footballers?
Careful planning of prevention exercises is important to optimise effectiveness, facilitate performance and stimulate adherence [52,53,54,55]. However, the timing of prevention exercises entails many considerations such as when to perform prevention exercises in a competitive season (pre-, in- or off-season), when in a weekly schedule and before, during or after training.
6.4.1.3 Scheduling Prevention During a Competitive Season
All studies derived from level 1 evidence that showed a preventive effect for hamstring injuries in football through eccentric strength training implemented their intervention protocol during the preseason [1, 17, 20]. The Danish and Dutch RCTs both involved a progressive increase in volume of the exercise during preseason and a maintenance phase in-season. In contrast, the FIFA 11+ programme has been investigated as a weekly intervention programme, with 2–3 scheduled pretraining/warm-up sessions a week, during football training.
6.4.1.4 Scheduling Prevention in a Weekly Schedule
Strong scientific evidence is lacking in regards to the optimal scheduling of eccentric exercise within the training week. In addition, a ‘one size fits all’ approach is not feasible as different sports, leagues and competitions have varying fixture structures that heavily influence such a decision. As mentioned previously, there is evidence for the effectiveness of the FIFA 11+ warm-up (which includes the NHE) to reduce hamstring injury risk in youth and amateur players. Therefore, one strategy at these levels could be to simply introduce the 11+ (or components of it) into the pre-football training warm-up, particularly in these populations. However, specific injury prevention sessions that are separate from the main football training session are popular methods in practice [54], particularly for higher-level players (e.g. professional and semiprofessional).
Level 5 findings from a recent Delphi study found that, in general, when players play only one match per week (i.e. ≥5 days recovery between matches), the main eccentric exercise session is recommended to be performed at 72 h (otherwise referred to as match day plus 3 days or MD + 3) following the match ([56], in review) and 2–3 days before the next match. However, caution should be taken that there are no residual fatigue or soreness effects prior to the next match. A study in semiprofessional players [52] showed that when an eccentric exercise session was performed on MD + 3, some residual fatigue and muscle damage markers were still present on the day before the match (otherwise referred to as match day minus 1 day or MD - 1). In particular, creatine kinase (a blood marker of muscle damage) and perceived muscle soreness remained elevated in players. However, isometric strength was unaffected by scheduling the eccentric exercise on MD + 3 [52, 57]. In the Delphi survey of professional teams, familiarising players with eccentric exercise was reported to be important as a means of minimising the damage response ([56], in review). The experts agreed that during periods with ≤4 days recovery between matches (which may be more applicable to professional senior and youth football teams), low-intensity eccentric exercises can be used (i.e. low load, low volume) ([56], in review). The experts’ view was that players should be accustomed to performing eccentric exercise to allow low intensity eccentric training during short recovery periods between matches. Interestingly, the study by Lovell and colleagues [52] showed that performing eccentric exercises on the day after a match (MD + 1) was not only tolerated by players but meant that there was also no residual fatigue or muscle damage markers evident on the MD - 1. This could be particularly important during these periods where there are ≤4 days recovery.
6.4.1.5 Scheduling Prevention Before, During or After Training
Another important question about prevention exercise scheduling is whether or not to perform an eccentric exercise session before or after the main training session. Unfortunately, again, there is no strong scientific evidence to recommend one over the other, and each approach has advantages and disadvantages. While the Delphi survey of practitioners from professional football ([56], in review) agreed that the eccentric session can be performed either before or after, it appears that the timing of the session may have different effects on the muscle. For example, Lovell and colleagues [53] found that estimated BFLH fascicle lengths were increased and pennation angles decreased when NHE training was performed before football training sessions. The performance of NHE training after football training was, by contrast, associated with increases in pennation angle and muscle thickness without change in estimated fascicle lengths. Given the preliminary evidence that BFLH fascicle length may influence hamstring injury risk, these findings suggest the possibility that the scheduling of eccentric training may impact on its injury protective effects. However, it seems unlikely that any single adaptation would mediate the benefits of an injury prevention programme. Regardless of the timing of the delivery of eccentric exercise, both approaches have been found to lead to similar chronic increases in hamstring strength [53]. Performing eccentric exercise after a training session has also been shown to enhance the ability of players to maintain eccentric knee flexor strength at half-time and at the end of simulated matches [55].
While it appears appropriate to perform eccentric exercise before or after the main football training session, there are some considerations to take into account as either approach could increase the risk of injury [53]. The acute effect of performing eccentric exercise may result in muscle fatigue and could increase the risk of injury [58] (although such risk is yet to be substantiated), particularly if the planned session is to be performed at high intensity and/or with high amounts of high-speed running and sprinting. Therefore, the subsequent exposure should also be considered when deciding whether or not to perform eccentric exercise before or after a training session.
It is worth raising the point that the larger hamstring injury prevention RCTs [1, 20] have employed the NHE either before or after training, and both approaches have resulted in reductions in injury rates. The Al Attar study provides an interesting perspective on this topic as well, since performing the FIFA 11+ pre- and post-training was more effective in reducing hamstring injury rates compared to performing the FIFA 11+ programme only before training [11]. From this, it is hypothesised that there could be a dosage-specific adaptation response to injury prevention exercises, resulting in a reduced risk of injury. Translating this to practice, the decision around the timing of delivery of an eccentric strength training stimulus may be dictated by other contextual factors such as coach, practitioner and athlete preference and consideration of the nature of the upcoming training session.
6.4.1.6 Should Hamstring Injury Prevention Strategies Be Tailored to the Individual?
Practitioners are often encouraged to provide tailored injury prevention strategies. Programmes may be tailored based on sport- or position-specific requirements or on the injury risk profile of the individual (noting that this risk profile will have some degree of subjectivity). This approach is predicated on the notion that screening for risk factors can assist risk profiling, hence providing guidance for tailored injury prevention programmes. Yet, the evidence for providing interventions based on a risk assessment [18, 59] is limited, and results have been mixed. With this in mind, it is critical that all individuals are provided with interventions that have been proven to reduce the incidence of hamstring injury, regardless of the perceived risk profile [60].
Beyond the blanket application of proven primary prevention strategies, an individualised approach to support the overarching hamstring injury prevention strategy may very well include the individualised interpretation of serial monitoring data, via secondary and tertiary prevention strategies, and this will be discussed in more detail in Chap. 11.
6.5 Hamstring Injury Implementation Conclusion
This chapter has presented an evidence-based framework to guide the development and implementation of hamstring injury prevention strategies (Fig. 6.1). Level 1 evidence strongly indicates that primary hamstring injury prevention should utilise exercise programmes for hamstring strength with eccentric overload. Ultimately, stimulating adherence to preventive measures is the final step to make evidence-based hamstring injury prevention work in a real-world setting.
It is imperative to consider injury prevention from a performance perspective as well, especially when faced with a congested schedule that can make planning of injury prevention exercises difficult. Therefore, it seems important to carefully plan and gradually increase eccentric training load for each athlete.
In conclusion, the evidence suggests building up a hamstring injury prevention programme during preseason and maintaining it in the in-season. When playing one match per week, the recommended day to perform the main eccentric exercise session seems to be on MD + 3. Players should, however, be accustomed to the eccentric stimulus by maintaining at least weekly sessions to minimise the damage response prior to the next match. Based on expert opinion, it may also be appropriate to perform low-load/low-volume eccentric exercise on the MD + 1, but again, players must be accustomed to this. Finally, eccentric conditioning sessions have proven effective whether they were conducted before or after the main football session, so the context of the planned football session and other factors that may improve coach or athlete buy-in are important considerations before planning an implementation strategy.
References
Petersen J, Thorborg K, Nielsen MB, Budtz-Jørgensen E, Hölmich P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39:2296–303.
Howick J. Levels of evidence. Oxford: Oxford Centre for Evidence-Based Medicine; 2009.
Junge A, Lamprecht M, Stamm H, Hasler H, Bizzini M, Tschopp M, Reuter H, Wyss H, Chilvers C, Dvorak J. Country-wide campaign to prevent soccer injuries in Swiss amateur players. Am J Sports Med. 2011;39:57–63.
Ekstrand J, Gillquist J, Liljedahl SO. Prevention of soccer injuries. Supervision by doctor and physiotherapist. Am J Sports Med. 1983;11:116–20.
Emery CA, Rose MS, McAllister JR, Meeuwisse WH. A prevention strategy to reduce the incidence of injury in high school basketball: a cluster randomized controlled trial. Clin J Sport Med. 2007;17:17–24.
Gouttebarge V, Zwerver J, Verhagen E. Preventing musculoskeletal injuries among recreational adult volleyball players: design of a randomised prospective controlled trial. BMC Musculoskelet Disord. 2017;18:333.
Andersson SH, Bahr R, Clarsen B, Myklebust G. Preventing overuse shoulder injuries among throwing athletes: a cluster-randomised controlled trial in 660 elite handball players. Br J Sports Med. 2017;51:1073–80.
Bonato M, Benis R, La Torre A. Neuromuscular training reduces lower limb injuries in elite female basketball players. A cluster randomized controlled trial. Scand J Sports Med. 2018;28:1451–60.
van Beijsterveldt AM, van de Port IG, Krist MR, Schmikli SL, Stubbe JH, Frederiks JE, Backx FJ. Effectiveness of an injury prevention programme for adult male soccer players: a cluster-randomised controlled trial. Br J Sports Med. 2012;46:1114–8.
Thorborg K, Krommes KK, Esteve E, Clausen MB, Bartels EM, Rathleff MS. Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: a systematic review and meta-analysis of the FIFA 11 and 11+ programmes. Br J Sports Med. 2017;51:562–71.
Al Attar WSA, Soomro N, Pappas E, Sinclair PJ, Sanders RH. Adding a post-training FIFA11+ exercise program to the pre-training FIFA11+ injury prevention program reduces injury rates among male amateur soccer players: a cluster-randomised trial. J Physiother. 2017b;63:235–42.
Hammes D, Der Fünten A, Kaiser S, Frisen E, Bizzini M, Meyer T. Injury prevention in male veteran football players – a randomised controlled trial using “FIFA11+”. J Sports Sci. 2015;33:873–81.
Owoeye OB, Akinbo SR, Tella BA, Olawale OA. Efficacy of the FIFA 11+ warm-up programme in male youth football: a cluster randomised controlled trial. J Sports Sci Med. 2014;13:321–8.
Silvers-Granelli H, Mandelbaum B, Adeniji O, Insler S, Bizzini M, Pohlig R, Junge A, Snyder-Mackler L, Dvorak J. Efficacy of the FIFA 11+ injury prevention program in the collegiate male soccer player. Am J Sports Med. 2015;43:2628–37.
Soligard T, Myklebust G, Steffen K, Holme I, Silvers H, Bizzini M, Junge A, Dvorak J, Bahr R, Andersen TE. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ. 2008;337:a2469.
Arnason A, Andersen TE, Holme I, Engebretsen L, Bahr R. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports. 2008;18:40–8.
Askling C, Karlsson J, Thorstensson A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand J Med Sci Sports. 2003;13:244–50.
Engebretsen AH, Myklebust G, Holme I, Engebretsen L, Bahr R. Prevention of injuries among male soccer players: a prospective, randomized intervention study targeting players with previous injuries or reduced function. Am J Sports Med. 2008;36:1052–60.
Gabbe BJ, Branson R, Bennell KL. A pilot randomised controlled trial of eccentric exercise to prevent hamstring injuries in community-level Australian football. J Sci Med Sport. 2006;9:103–9.
Van der Horst N, Smits DW, Petersen J, Goedhart EA, Backx FJ. The preventive effect of the Nordic hamstring exercise on hamstring injuries in amateur soccer players: a randomized controlled trial. Am J Sports Med. 2015;43:1316–23.
Seagrave RA III, Perez L, McQueeney S, Toby EB, Key V, Nelson JD. Preventive effects of eccentric training on acute hamstring muscle injury in professional baseball. Orthop J Sports Med. 2014;2:2325967114535351.
Goode AP, Reiman MP, Harris L, DeLisa L, Kauffman A, Beltramo D, Poole C, Ledbetter L, Taylor AB. Eccentric training for prevention of hamstring injuries may depend on intervention compliance: a systematic review and meta-analysis. Br J Sports Med. 2015;49:349–56.
Berg HE, Tesch A. A gravity-independent ergometer to be used for resistance training in space. Aviat Space Environ Med. 1994;65:752–6.
Taylor GH. Health by exercise. New York, NY: Am Book Exc; 1880.
Mjølsnes R, Arnason A, Østhagen T, Raastad T, Bahr R. A 10-week randomized trial comparing eccentric vs. concentric strength training in well-trained soccer players. Scand J Med Sci Sports. 2004;14:311–7.
Sugiura Y, Sakuma K, Sakuraba K, Sato Y. Prevention of hamstring injuries in collegiate sprinters. Orthop J Sports Med. 2017;5:2325967116681524.
Brooks JH, Fuller CW, Kemp SP, Reddin DB. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am J Sports Med. 2006;34:1297–306.
Van Mechelen W, Hlobil H, Kemper HC, Voorn WJ, de Jongh HR. Prevention of running injuries by warm-up, cool-down, and stretching exercises. Am J Sports Med. 1993;21:711–9.
Verrall GM, Slavotinek JP, Barnes PG. The effect of sports specific training on reducing the incidence of hamstring injuries in professional Australian Rules football players. Br J Sports Med. 2005;39:363–8.
Dadebo B, White J, George KP. A survey of flexibility training protocols and hamstring strains in professional football clubs in England. Br J Sports Med. 2004;38:388–94.
Shield AJ, Bourne MN. Hamstring injury prevention practices in elite sport: evidence for eccentric strength vs. lumbopelvic training. Sports Med. 2018;48:513–24.
Schuermans J, Danneels L, van Tiggelen D, Palmans T, Witvrouw E. Proximal neuromuscular control protects against hamstring injuries in male soccer players: a prospective study with electromyography time-series analysis during maximal sprinting. Am J Sports Med. 2017;45:1315–25.
Duhig S, Shield AJ, Opar D, Gabbett TJ, Ferguson C, Williams M. Effect of high-speed running on hamstring strain injury risk. Br J Sports Med. 2016;50:1536–40.
Oakley AJ, Jennings J, Bishop CJ. Holistic hamstring health: not just the Nordic hamstring exercise. Br J Sports Med. 2018;52:816–7.
Van de Hoef PAS, Brink MSM, Huisstede BMAB, van Smeden MM, de Vries NN, Goedhart EAE, Gouttebarge VV, Backx FJGF. Does a bounding exercise program prevent hamstring injuries in adult male soccer players? A cluster RCT. Scand J Med Sci Sports. 2018;29(4):515–23.
Al Attar WSA, Soomro N, Sinclair PJ, Pappas E, Sanders RH. Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players: a systematic review and meta-analysis. Sports Med. 2017a;47:907–16.
Van der Horst N, Hoef SV, Otterloo PV, Klein M, Brink M, Backx F. Effective but not adhered to: how can we improve adherence to evidence-based hamstring injury prevention in amateur football? Clin J Sports Med. 2018; https://doi.org/10.1097/JSM0000000000000710.
O’Brien. Enhancing the implementation of injury prevention exercise programmes in professional football. Br J Sports Med. 2017;51:1507–8.
Ekstrand J, Waldén M, Hägglund M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: a 13-year longitudinal analysis of the UEFA Elite Club injury study. Br J Sports Med. 2016;50:731–7.
Bahr R, Thorborg K, Ekstrand J. Evidence-based hamstring injury prevention is not adopted by the majority of Champions League or Norwegian Premier League football teams: the Nordic hamstring survey. Br J Sports Med. 2015;49:1466–71.
Read PJ, Jimenez P, Oliver JL, Lloyd RS. Injury prevention in male youth soccer: current practices and perceptions of practitioners working at elite English academies. J Sports Sci. 2018;36:1423–31.
Emery CA, Roy TO, Whittaker JL, Nettel-Aguirre A, van Mechelen W. Neuromuscular training injury prevention strategies in youth sport: a systematic review and meta-analysis. Br J Sport Med. 2015;49:865–70.
Niven A. Rehabilitation adherence in sport injury: sport physiotherapists’ perceptions. J Sport Rehabil. 2007;16:93–110.
Soligard T, Nilstad A, Steffen K, Myklebust G, Holme I, Dvorak J, Bahr R, Andersen TE. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br J Sports Med. 2010;44:787–93.
Orr B, Brown C, Hemsing J, McCormick T, Pound S, Otto D, Emery CA, Beaupre LA. Female soccer knee injury: observed knowledge gaps in injury prevention among players/parents/coaches & current evidence (the KNOW study). Scand J Med Sci Sports. 2013;23:271–80.
Steffen K, Meeuwisse WH, Romiti M, Kang J, McKay C, Bizzini M, Dvorak J, Finch C, Myklebust G, Emery CA. Evaluation of how different implementation strategies of an injury prevention programme (FIFA 11+) impact team adherence and injury risk in Canadian female youth football players: a cluster-randomised trial. Br J Sports Med. 2013;47:480–7.
Twomey D, Finch CF, Roediger E, Lloyd DG. Preventing lower limb injuries: is the latest evidence being translated into the football field? J Sci Med Sport. 2009;12:452–6.
Finch CF, Doyle TL, Dempsey AR, Elliott BC, Twomey DM, White PE, Diamantopoulou K, Young W, Lloyd DG. What do community football players think about different exercise-training programmes? Implications for the delivery of lower limb injury prevention programmes. Br J Sports Med. 2014;48:702–7.
Hägglund M, Waldén M, Magnusson H, Kristenson K, Bengtsson H, Ekstrand J. Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA Champions League injury study. Br J Sports Med. 2013;47:738–42.
Impellizzeri FM, Bizzini M, Dvorak J, Pellegrini B, Schena F, Junga A. Physiological and performance responses to the FIFA11+ (part 2): a randomised controlled trial on the training effects. J Sports Sci. 2013;31:1491–502.
Ishøi L, Hölmich P, Aagaard P, Thorborg K, Bandholm T, Serner A. Effects of the Nordic hamstring exercise on sprint capacity in male football players: a randomized controlled trial. J Sports Sci. 2018;36:1663–72.
Lovell R, Whalan M, Marshall PWM, Sampson JA, Siegler JC, Buchheit M. Scheduling of eccentric lower limb injury prevention exercises during the soccer micro-cycle: which day of the week? Scand J Med Sci Sports. 2018a;28:2216–25.
Lovell R, Knox M, Weston M, Siegler JC, Brennan S, Marshall PWM. Hamstring injury prevention in soccer: before or after training? Scand J Med Sci Sports. 2018b;28:658–66.
McCall A, Carling C, Nedelec M, Davison M, Le Gall F, Berthoin S, Dupont G. Risk factors, testing and preventative strategies for non-contact injuries in professional football: current perceptions and practices of 44 teams from various premier leagues. Br J Sports Med. 2014;48:1352–7.
Small K, McNaughton L, Greig M, Lovell R. Effect of timing of eccentric strengthening exercises during soccer training: implications for muscle fatigability. J Strength Cond Res. 2009;23:1077–83.
McCall A, Pruna R, van der Horst N, Dupont G, Buchheit M, Coutts A, Impellizzeri FM, Pons E, Fanchini M Exercise-based strategies to prevent muscle injury in professional footballers: part II – an expert-led Delphi survey of the Big-5 European football leagues. 2018. Submitted.
Warren GL, Lowe DA, Armstrong RB. Measurement tools used in the study of eccentric contraction-induced injury. Sports Med. 1999;27:43–59.
Lovell R, Siegler JC, Knox M, Brennan S, Marshall PW. Acute neuromuscular and performance responses to Nordic hamstring exercises completed before or after football training. J Sports Sci. 2016;34:2286–94.
Croisier JL, Ganteaume S, Binet J, Genty M, Ferret JM. Strength imbalances and prevention of hamstring injury in professional soccer players: a prospective study. Am J Sports Med. 2008;36:1469–75.
Bahr R. Why screening tests to predict injury do not work – and probably never will…: a critical review. Br J Sports Med. 2016;50:776–80.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
van der Horst, N., Thorborg, K., Opar, D. (2020). Hamstring Injury Prevention and Implementation. In: Thorborg, K., Opar, D., Shield, A. (eds) Prevention and Rehabilitation of Hamstring Injuries. Springer, Cham. https://doi.org/10.1007/978-3-030-31638-9_6
Download citation
DOI: https://doi.org/10.1007/978-3-030-31638-9_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-31637-2
Online ISBN: 978-3-030-31638-9
eBook Packages: MedicineMedicine (R0)