
Abstract
In this work, the development of a continuous monitoring system of a human’s respiratory rate (RR) is presented. The system is based on the impedance pneumography method and it is divided into two main blocks: the electronic circuit and the electrodes. For the electrodes, two technologies are considered: the first one is Ag/AgCl disposable electrodes frequently used in clinical applications. The second one, known as textile electrode, is built on electrically conductive fabric. The performance of both types of electrodes is compared. Therefore, the experimental tests are carried out in two stages. In both stages, 5 records of 10 min were acquired in 5 healthy subjects. The first stage is recorded with disposable electrodes and the second one with textile electrodes. In order to compare the results obtained in each case, reference values were simultaneously recorded in each subject with a commercial polysomnography system. This system records respiratory activity using a method based on piezoelectric respiratory effort bands placed in the abdomen and thorax. Finally, the absolute (eA) and relative (eR) errors are computed taking into account RR values obtained from the designed and reference system for each stage. The results show similar performance among textile and disposable electrodes.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
The respiratory rate (RR) is a vital sign extremely important not only in the diagnosis but also in the control of serious respiratory diseases. Through regular RR monitoring, it is possible an early detection of exacerbation in patients with Chronic Obstructive Pulmonary Disease (COPD) [1], as well as, acute respiratory dysfunction [2]. Furthermore, this also allows to assess the evolution of patients’ rehabilitation and athletes’ performance [3].
Patients’ lung volume and capacities can be usually assessed in the doctor’s office through the use of a spirometry test [4]. However, this type of test is not suitable for continuous monitoring [5]. For this reason, in other contexts, such as sleep studies, wereables and telehealth systems, etc., other techniques must be used. Among these techniques, plethysmography and impedance pneumography (IP) are widely used. They allow to register respiratory signals and, by means of digital processing techniques, respiratory rate can be estimated.
Plethysmography consists of respiratory bands adjusted around the thorax and abdomen. At the same time, these respiratory bands are connected to force sensors that measure thoracic and/or abdominal movements due to variations of the air present in the lungs. Force sensors are built from different and specific transducers such as strain gauges or piezoelectric materials [6].
On the other hand, IP is a technique that allows to instantly measure the variations of volume in the air that is present in the lungs by means of electrical impedance changes in the human thorax using electrodes placed on the skin’s surface [7].
Different electrode technologies can be used to achieve both a low cost system and a more comfortable system for continuous monitoring (CM) [8]. Among them, disposable electrodes Ag/AgCl are widely used [9]. They allow to acquire records with very low noise level and they are stable and inexpensive. On the other hand, when it is necessary to obtain long time records (>24 h), the electrode properties decrease considerably causing a lower quality in the signal’s recording. Therefore, they are not suitable for continuous monitoring systems.
One alternative to these electrodes can be textile electrodes that consist of conductive fabric and wire which, according to some studies, allow to obtain a good quality of register even during long periods [9].
One additional advantage of such electrodes is that they provide patients with the necessary comfort since they can be built in the clothes that the person normally wears and, in this way, acceptance by patients is facilitated [9].
In this research, the register of the respiratory rate (RR) is evaluated using the IP method with textile electrodes. For this reason, an electronic circuit in which such technique could be applied was designed. Moreover, a model of a textile electrode was built using conductive fabric in order to compare their performance with the performance of disposable electrodes Ag/AgCl. A commercial polysomnography system is used together with plestimographic bands in order to obtain a respiratory rate reference and statistical parameters.
2 Materials and Methods
2.1 Electronic Circuit
The IP method consists in injecting an electric current to a person’s chest and recording the changes in the resulting potential due to the variations of its impedance. The impedance varies for two reasons: the first is due to air entering the lungs causing changes in the electrical characteristics of the thorax. The second, it is produced by changes in the separation of the electrodes due to volume variation [10].
There are two electrodes configuration, tetrapolar and bipolar. The first uses four electrodes, two to inject the current and two to record potential’s variations. On the other hand, the bipolar method uses the same pair of electrodes to inject current and register the potential’s variations. Although the sensitivity is lower than in the previous case, the system is simpler and more comfortable for the patient [7].
Figure 1 shows a general scheme of the circuit which is implemented based on the Analog Front-End ADS1292R of Texas Instruments. It is important to highlight its internal current source called carrier signal which has a frequency of 100 kHz and 500 uA of intensity. According to these values, tissues are not stimulated and, therefore, no damage is caused [11].

Electronic circuit: general diagram block based on ADS1292R analog Front-End.
According to Ohm’s law, the current that is injected to the thorax and its impedance generates a potential drop. The latter is the carrier regulated by the variations in the impedance of the thorax due to breathing. The electrical potential is increased by an amplifier with high input impedance and common mode rejection ratio (CMRR).
Then a coherent demodulation process is applied in order to obtain the respiratory signal (SR). Finally, the SR is digitalized by means of an analog-digital converter (ADC) integrated in ADS1292R and which has a high resolution (24 bits). This characteristic allows the gain of the amplifier to be low (G = 6) thus reducing the noise levels [12]. The sampling frequency of the signal was selected at 128 Hz.
The ADS1292R sends via SPI communication the digitalized signal to ARM Cortex M4 processor; specifically the MSP432 microcontroller is used. The latter is responsible for retransmitting the data to a computer through USB connection.
2.2 Electrodes
In this research, two types of electrodes were examined to inject the current into the skin surface of the thorax. The first ones are disposable electrodes Ag/AgCl. The second ones are textile electrodes constructed using conductive fabric shown in Fig. 2. The fabric used is MedTexTM P-180 model which is built on a base of 94% nylon and 6% of elastic material. It also has a silver coating (Ag) of 99% purity [13].

Textile electrode built based on conductive fabric MedTexTM P-180.
2.3 Evaluation
In order to evaluate the performance of the electronic circuit and the textile electrodes, five records were acquired in 5 healthy persons. Each of these records is di-vided into two different stages: in the first stage disposable electrodes were used whereas in the second one textile electrodes were used. Both cases were simultaneously acquired with a respiratory signals reference (RSR).
The RSR signals correspond to the plethysmographic signals of the thorax, abdomen and the sum of both of these (RIPT, RIPA and RIPsum, respectively) and the sum of these (RIPSum). The third signal was included due to the fact that it is similar to the one obtained by the IP signal, based on the researcher carried out by other authors [14].
The recordings of these signals were performed with respiratory bands based on piezoelectric sensors connected to a commercial polysomnography, model Mini PC from Akonic®. This system samples the signals in 128 Hz and it sends all the digitalized signal to PC via USB communication. Figure 3 shows the placement of the respiratory effort belts and IP method’s superficial skin’s electrodes.

Piezoelectric respiratory band and IP methods electrodes placement.
Figure 4 shows the photography of the experimental tests. In this figure, the Akonic system, respiratory effort belts and the development electronic circuit board can be visualized.

Experimental tests photography
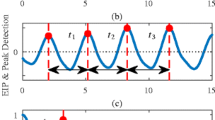
Once the respiratory signals have been acquired, the respiratory frequency is calculated for each record. This last is carried out using a method proposed and used by other authors [15]. First, each respiratory signal is divided into 32-second segments. Next, for each segment, their frequency spectrum is analyzed and the frequency respiratory rate corresponding to each interval is determined based on the component with the highest magnitude.
The RR values computed from the IP method with both types of electrodes were compared with the ones obtained from RSR signals. Two statistical parameters proposed by other authors were used in order to compare RR values [2]. The first one is the Absolute Error (eA) (1) and the other one is the Relative Error (eR) (2).
3 Results
The Tables 1 and 2, summarizes the results for disposable and textile electrodes, respectively. The mean and standard deviation were computed for both errors (eA and eR) and taking into account separately the group of records performed with the disposable and textile electrode.
Figure 5a and b show the first volunteer’s respiratory signals acquired from the disposable and textile electrode, respectively. Also, these include the corresponding RIPT, RIPA and RIPSum signals simultaneously acquired from Akonic system.

Acquired signals test. Reference RIP signal and IP method with: (a) disposable and (b) textile electrodes.
4 Conclusions
In this research, an electronic circuit, which allows the RR registration by the IP method, has been designed and evaluated. It works together with a textile electrode model that was also built. Furthermore, its performance is compared with the one by standard disposable Ag/AgCl electrodes based on RR values.
The comparative test was carried out based on RR values and respiratory reference signal. These are the signals acquired from plethysmography bands (thorax, abdomen and its arithmetic addition), connected to a commercial polysomnogram.
The statistical parameters of the eA and eR errors were computed for each type of electrode technology respect to the respiratory reference signal. In order to simplify the analysis, the mean and the standard deviation were computed for both electrodes technologies.
The results show that eA is similar in both electrodes types but the eR is better in disposable electrodes. This difference could be by the electrode motion because tex-tile electrodes are most sensible.
In the future, the new smaller dimension prototype and its case will be built. The latter will be designed with a material that improves the system’s electromagnetic compatibility features. Based on the new design a study will be carried out comparing the respiratory signal’ waveform acquired from textile electrodes and other standards methods.
References
Aburto, M., Esteban, C., Moraza, F.J., Aguirre, U., Egurrola, M., Capelastegui, A.: COPD exacerbation: mortality prognosis factors in a respiratory care unit. Arch. Bronconeumol. 47, 79–84 (2011). https://doi.org/10.1016/S1579-2129(11)70018-0
Lázaro, J., Gil, E., Bailón, R., Mincholé, A., Laguna, P.: Deriving respiration from photoplethysmographic pulse width. Med. Biol. Eng. Comput. 51, 233–242 (2013). https://doi.org/10.1007/s11517-012-0954-0
Lázaro, J., Alcaine, A., Romero, D., Gil, E., Laguna, P., Pueyo, E., Bailón, R.: Electrocardiogram derived respiratory rate from QRS slopes and R-wave angle. Ann. Biomed. Eng. 42, 2072–2083 (2014). https://doi.org/10.1007/s10439-014-1073-x
Sokol, K.C., Sharma, G., Lin, Y.L., Goldblum, R.M.: Choosing wisely: adherence by physicians to recommended use of spirometry in the diagnosis and management of adult asthma. Am. J. Med. 128, 502–508 (2015). https://doi.org/10.1016/j.amjmed.2014.12.006
Wang, H., Yen, C., Liang, J., Wang, Q., Liu, G., Song, R.: A robust electrode configuration for bioimpedance measurement of respiration. J. Healthc. Eng. 5, 313–328 (2014). https://doi.org/10.1260/2040-2295.5.3.313
Frank, P.: Primiano: measurements of the respiratory system. In: Webster, J.G. (ed.) Medical Instrumentation: Application and Design. Wiley, Hoboken (2009)
Seppä, V.P., Pelkonen, A.S., Kotaniemi-Syrjänen, A., Viik, J., Mäkelä, M.J., Malmberg, L.P.: Tidal flow variability measured by impedance pneumography relates to childhood asthma risk. Eur. Respir. J. 47, 1687–1696 (2016). https://doi.org/10.1183/13993003.00989-2015
Klum, M., Schenck, T., Pielmus, A., Tigges, T., Orglmeister, R.: Short distance impedance pneumography. Curr. Dir. Biomed. Eng. 4, 109–113 (2018). https://doi.org/10.1515/cdbme-2018-0028
Fiedler, P., Biller, S., Haueisen, J.: Impedance pneumography using textile electrodes, pp. 1606–1609 (2012)
Grimnes, S., Martinsen, Ø.G.: Chapter 10 - Selected applications. In: Grimnes, S., Martinsen, Ø.G. (eds.) Bioimpedance and Bioelectricity Basics, 3rd edn, pp. 405–494. Academic Press, Oxford (2015)
Młyńczak, M., Cybulski, G.: Impedance pneumography: is it possible? Proc. SPIE 8454, 84541T (2012). https://doi.org/10.1117/12.2000223
Soundarapandian, K., Berarducci, M.: Analog front-end design for ECG systems using delta-sigma ADCs (2010)
Shieldex(R): Technical Data Sheet: Shieldex (R) Med-tex P180. https://www.statex.de/wp-content/uploads/2017/05/ShieldexMedtexP180_02-07-13.pdf
Leder, R.S., Cohen, K.P., Peterson, N., Palreddy, S., Green, C., Tompkins, W.J., Webster, J.G.: Performance of impedance and inductance ventilation sensors on premature infants during natural breathing, motion, and airway obstruction. In: Proceedings of the 25th Annual International Conference IEEE Engineering Medicine Biology Society, vol. 1–4 (New Begin. Hum. Heal. 25), pp. 3094–3097 (2003). https://doi.org/10.1109/iembs.2003.1280796
Charlton, P.H., Villarroel, M., Salguiero, F.: An assessment of algorithms to estimate respiratory rate from the electrocardiogram and photoplethysmogram. Second. Anal. Electron. Heal. Rec., 1–427 (2016). https://doi.org/10.1007/978-3-319-43742-2
Acknowledgment
All authors are supported by UniversidadNacional de San Juan (UNSJ) and Consejo Nacional de InvestigacionesCientíficas y Técnicas (CONICET). The research project is supported by grants of Secretaría de Ciencia, Tecnología e Innovación – Universidad Nacional de San Juan (SECITI-UNSJ – Res 1054-18-R) and CONICET (PIP 11220150100059 CO), Argentina.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Ethics declarations
The authors declare that they have no conflict of interest.
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this paper

Cite this paper
Dell’Aquila, C.R., Cañadas, G.E., Laciar, E. (2020). Evaluation of Respiratory Signal Record Based on Impedance Pneumography and Textile Electrodes. In: González Díaz, C., et al. VIII Latin American Conference on Biomedical Engineering and XLII National Conference on Biomedical Engineering. CLAIB 2019. IFMBE Proceedings, vol 75. Springer, Cham. https://doi.org/10.1007/978-3-030-30648-9_193
Download citation
DOI: https://doi.org/10.1007/978-3-030-30648-9_193
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-30647-2
Online ISBN: 978-3-030-30648-9
eBook Packages: EngineeringEngineering (R0)