
Abstract
The radial artery is located in the lateral intermuscular septum which separates the flexor and extensor compartments of the forearm. Its superior half runs deep between the brachioradialis muscle and rotundum pronator muscle and its lower half between the tendons of brachioradialis and flexor radial carpalis. Along its course, the radial artery gives rise to 9–17 septocutaneous branches to supply the overlying fascia and skin. All these ramifications, with an average diameter of 0.5 mm, form a rich network of vascularization in subcutaneous layers, along with the fasciocutaneous ramifications of the ulnar, brachial, and interosseous arteries. Radial forearm free flap (RFFF) is one of the most common flaps used in head and neck reconstruction. In this chapter, neurovascular anatomy and harvesting surgical technique of the RFFF are described. Moreover, analitycal factors and technical considerations about RFFF are deeply discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

1 Anatomy
1.1 Artery
After passing underneath the biceps aponeurosis, the brachial artery divides into radial and ulnar arteries, at about one cm below the elbow ligament. The radial artery is located in the lateral intermuscular septum which separates the flexor and the extensor compartments of the forearm. Its superior half runs deep between the brachioradialis muscle and the rotundum pronator muscle, while its lower half runs between the tendons of the brachioradialis and the flexor radial carpalis. The radial pulse is palpable in the wrist, medial to the tip of the styloid process of the radius, and the artery is covered only by band and skin. The deep palmar arch is formed by the radial artery joining with the deep branch of the ulnar artery between the first and second metacarpal bone. Along its course, the radial artery rises up to 9–17 septocutaneous branches to supply the overlying fascia and skin. All of these ramifications, with an average diameter of 0.5 mm, form a rich network of vascularization in the subcutaneous layers, along with the fasciocutaneous ramifications of the ulnar, brachial, and interosseous arteries. Distal fasciocutaneous branches of radial artery can adequately perfuse all the skin of the forearm [1].
The periosteal blood supply to the distal radius relies on branches of the radial artery to the deep flexor pollicis longus and pronator quadratus muscles; perforators pass also through the lateral intermuscular septum from the radial artery to the periosteum. These perforators permit to harvest an osteocutaneous radial forearm flap including the distal anterolateral face of the radius.
1.2 Venous System
The radial forearm free flap (RFFF) has two venous drainage systems: a deep one, composed of two venae comitantes that accompany the radial artery and a superficial system, mainly composed of the cephalic vein laterally and the basilic vein medially.
The cephalic vein rises from the dorsal venous network, around the lateral margin of the distal forearm. It is a large, thick-walled vein that runs in a constant location deep to the subcutaneous fat plane. At the level of the elbow, the cephalic vein runs up to the anterolateral side of the arm, superficially at the groove between the brachioradialis muscle and biceps muscle.
The basilic vein runs deep into the fat plane along the medial side of the forearm.
A wide variety of venous connections can be encountered in the volar face of the forearm. The median cubital vein of the elbow joins the basilic and the cephalic vein in the proximal forearm. A short vein, the perforating cubitalis vein, connects the deep and superficial systems at the level of the antecubital fossa. These connections permit, in selected cases, to drain both superficial and deep venous system with a single anostomosis.
Moreover, a series of smaller veins form a sort of subcutaneous network.
Both superficial and deep systems are similarly able to drain the blood from the skin of the forearm. The multiple connections between the venae comitantes and the superficial veins form the basis for the use of either of these two systems to drain the flap.
1.3 Nerves
The cutaneous innervation of the forearm originates from the lateral and medial antebrachial cutaneous nerves. The lateral cutaneous antebrachial nerve (LCAN) is an extension of the muscle-cutaneous nerve that supplies the flexors muscle of the upper arm. After piercing the deep fascia of the cubital fossa, it runs deep under the cephalic vein to descend along the radial forearm face down to the wrist. With its anterior branch, it innervates the skin of the lateral half of the anterior surface of the forearm. The posterior branch supplies the sensation to the posterolateral forearm.
The medial antebrachial cutaneous nerve crosses the deep fascia in the medial part of the mid-upper arm. It divides into an anterior and a posterior branch. The anterior branch descends anteriorly to the basilic vein and innervates the skin of the anteromedial aspect of the forearm. The posterior branch lies anteriorly to the epitroclea of the humerus and innervates the skin of the posteromedial surface of the forearm.
The radial nerve has both motor and sensory components. In the forearm, it divides into a deep motor branch and a superficial sensory branch.
The deep branch of the radial nerve winds around the radius and comes to lie on the posterior interosseous membrane.
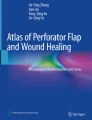
The superficial branch of the radial nerve, in its first tract, courses in the forearm, deep to the brachioradialis, and then passes laterally to the brachioradialis tendon where it becomes superficial, supplying sensation trough the dorsal digital nerves to the dorsum of the hand, thumb, index and middle fingers (Fig. 5.1).

Vascular and nervous anatomy of the flap
2 Analytical Factors and Technical Considerations
2.1 Venous Drainage: Superficial and Deep Vein System
Since the initial description of RFFF by Song R. in 1982, the superficial venous system was considered as the primary venous drainage of this flap [2]. The superficial venous systems are preferred by most of the surgeons for the larger diameter and thicker wall of the vessels, and a consequent easier anastomosis. Moreover, the independent and relative distant course of the cephalic vein and the radial artery, allows a simpler placement and maneuverability of both vein and artery, one to each other, in the receiving site.
It is argued which of the venous systems is the dominant one, whether the superficial or the deep one. The Ichinose et al. [3] hemodynamic study demonstrated that, at an early stage after flap elevation, the comitantes veins have twice the volume of drainage per unit time compared with the cephalic vein, and in 60% of cases, there is no obvious communication between the deep and superficial venous system.
Futran et al. [4] suggested that single venous anastomosis of the subcutaneous system provided adequate drainage of the flap reducing the operative time. The bigger concern of the supporters of the single superficial venous anastomosis is the inadequacy of the caliber of the deep veins. To overcome this limit Gottlieb et al. proposed the dissection of the pedicle up to the antecubital fossa near the confluence of the two venae comitantes [5]. In any case, the communication between the two system is absent in 40% of cases; moreover, the time of the dissection and morbidity to donor site increases, and a pedicle with an unnecessary length tends to be prone to kinking. On the other hand, the anastomosis of both drainage systems seem to reduce the venous pressure, creating a low-flow state, thus increasing the risk of venous thrombosis. Some authors suggested that the comitantes veins and the cephalic vein should be anastomosed independently on two distinct venous systems (internal and external jugular) assuring two separate and parallel drainage systems.
It is easy to note that still debate exists about which venous system prefer and whether one or two vein anastomosis give better results, probably because both the alternatives provide reliable and reproducible outcomes.
2.2 Sensate Flap
A sensate flap can be harvested using the LCAN. It can be anastomized in the neck with the proximal stump of the lingual nerve or more rarely with a branch of the cervical plexus. LCAN and its branches determine the most of the sensitive innervation of the RFFF, but also the medial cutaneous antebrachial nerve and the branches of the superficial radial nerve may innervate clinically relevant portions of the flap [6]. Reinnervation seems to favour sensory recovery providing larger, better arranged and more numerous nerve fibers compared to not-sensate flap [7]. Despite this, evidence about short and long term better functional outcomes with sensate flap is lacking, considering also the complexity and quantity of variables that affect recovery after reconstructive surgery [8]. On the other hand, section of the LCAN will invariably results in skin sensory deficits.
3 Flap Harvesting
3.1 Preoperative Management
At the admission, the patient and hospital personnel must be warned to avoid the violation of the nondominant forearm that must be shaved.
Although exceedingly rare, the occurrence of acute hand vascular insufficiency when harvesting a radial forearm free flap is always a possibility (two cases described in literature) and must be kept in mind.
The Allen test is the most important preoperative evaluation to assess the adequacy of the perfusion of the hand (especially the index and the thumb) through the residual ulnar artery, after forearm flap harvesting. Simultaneous digital compression of the ulnar and radial arteries is applied for few seconds by the examiner while the patient is invited to alternately open and close the hand. This pumping action causes mechanical exsanguination with the hand that becomes pale. The hand is then opened before releasing the compression on the ulnar artery. Reperfusion is evident trough a blush of the hand within 15–20 s. If a delay is noted, it can be concluded that there is not a good crossflow from the ulnar artery trough the palmar arch, representing, contraindication for proceeding with a radial forearm flap. Controlateral forearm vascular circulation should be explored.
There are no substantial differences in flaps harvested from the left or right side, so it is widespread practice to choose the donor site from the nondominant upper limb, although it is preferable to have the operating arm on the contralateral side to the resection to create more space for two surgical teams to work simultaneously. Previous intravenous lines positioning must be avoided on the side of the flap harvesting, but venepuncture itself is not an absolute contraindication. Previous surgery, scars, injury, fractures, and burns may contraindicate the use of a specific arm. Moreover, the patient’s preference is taken into account.
The patient must be counseled about the possibility of donor site sequelae and, in particular, poor cosmetic results, use of a skin graft for closure and temporary or permanent variable sensory loss of the posterolateral portion of the hand.
3.2 Flap Design
The radial artery (Fig. 5.2) runs under a virtual line that joins the central point of the antecubital fossa and the tubercle of the scaphoid and, in the most of cases, it can be identified by palpation at the wrist, between the brachioradialis and the flexor carpi radialis tendon and marked on the skin for about 10 cm length starting from the distal border of the flap. The lateral intermuscular septum incorporates the radial artery and the venae comitantes. After inflating the tourniquet, the cephalic vein system is identified and marked on the volar and lateral aspect of the arm (Fig. 5.2). In fat arms, the cephalic vein may be not visible; in this case the probable course is marked based on anatomical knowledge. The size and shape of the flap are determined and marked on the forearm, often with a template from the estimated surgical defect. The axis of the flap should be centered over the course of the radial artery. The ulnar margin of the flap is outlined over the flexor carpi ulnaris muscle while the lateral has to be drawn beyond the radial artery, comprehending the cephalic vein. The flap can be extended ulnarward to the less hair bearing part of the forearm, as desired, while the dorsal aspect of the arm should be spare for aesthetic reasons. Proximal margin depends on the flap size needed.

Right arm: identification and drawing of the radial artery, cephalic vein and flap design
3.3 Patient Positioning
The arm is placed 70° with respect to the patient’s body on a self-stained board. Care must be taken to minimize traction on nerves in the axilla and elbow region.
We advise the use of the tourniquet to obtain a surgical field without bleeding during the dissection. Orthopaedic cotton bandage proximally wraps the arm to avoid the prolonged contact with the inflated tourniquet. Without proper protection, the underlying soft tissue is prone to damage caused by wrinkling, pinching, or shearing.
The cuff is secured around the limb proximal to the operative site. Pressure is exerted on the circumference of the arm; when sufficient pressure is obtained, vessels and arteries beneath the cuff become temporarily occluded, preventing blood flow past the cuff. While the cuff is inflated, the tourniquet system automatically monitors and maintains the pressure chosen by the user (approximately 250 mmHg). Cuff pressure and inflation time are displayed, and an audiovisual alarm alert informs the user to alarm conditions, such as a cuff leak.
Pneumatic surgical tourniquet prevents blood flow to the arm and enables the surgeon to work in a bloodless operative field (Fig. 5.3).

Pneumatic surgical tourniquet prevents blood flow to the arm and enables the surgeon to work in a bloodless operative field
Before the tourniquet inflation, moderate exsanguination of the limb is also recommended using an Esmarch bandage (a narrow elastic bandage 5–10 cm wide) before inflating the tourniquet to stop the arterial flow (Fig. 5.4).

Esmarch bandage is used to expel venous blood from the arm (exsanguinate) elevating the limb as the elastic pressure is applied
The acceptable range of tolerance to ischemia of the arm remains controversial. Tolerance of composite tissue is dependent on the quantity of contained skeletal muscle. VanderWilde et al. reported a successful hand replantation after 54 hours of cold ischemia [9].
4 Surgical Steps
4.1 Step 1
The procedure starts with the elevation of the superior skin flap: after the flap has been marked, a median skin incision is prolonged from the upper border of the flap to the antecubital fossa. A superior (radial) skin and subcutaneous flap is harvested, exposing the course of the superficial vein system. Careful dissection of the cephalic vein that runs over the brachioradialis musle, ligating its collateral branches, permits to harvest a thicker skin flap, reducing the risk of necrosis (Fig. 5.5).

Harvesting of the superior skin flap with exposition of the course of the cephalic vein
4.2 Step 2
Elevation of the RFFF starts trough the incision of the skin at the radial border through the subcutaneous fatty tissue until the forearm fascia is reached. The fascia is incised and elevated from lateral to medial. A collateral branch of the cephalic vein is recognized: it is transected and the proximal stump of the vein is sutured to the subfascial plane of the flap in order to avoid a vein detachement due to traction (Fig. 5.6).

Identification (left) and ligation (right) of a collateral branch of the cephalic vein
4.3 Step 3
The distal margin of the flap is incised. The fascial plane is identified above the cephalic vein and its branches. At the distal aspect of the flap the vein is completely isolated and transected (Figs. 5.6 and 5.7). Radial dissection is carried out in a subfascial plane, elevating the flap off from the tendons of the muscle in the flexor compartment. The superficial branch of the radial nerve is (Fig. 5.7) usually identified over the tendon of brachioradialis muscle. There are usually two main distal branches: although the distal branching pattern is highly variable, the major branches are always encountered in the wrist while elevating the radial forearm flap. This nerve and all its branches can be routinely preserved to maintain sensation to the hand. By careful dissection, a lateral cutaneous antebrachial nerve becomes visible. The LCAN is identified usually in the central to slightly radial aspect of the flap. This sensory nerve usually runs in close proximity to the cephalic vein in the upper forearm before ramifying in the distal forearm and continuing onto the hand in the region of the thenar eminence.

Identification, section and ligation of the cephalic vein. Subfascial dissection of the flap, preserving the superficial branch of the radial nerve
4.4 Step 4
The intermuscular septum containing the radial artery and venae comitantes is identified and separated from the brachioradialis muscle. Vessels are sectioned, ligated, and carefully elevated together with the flap. The radial artery is isolated distally, where it is only covered by fascia and skin and lies between the tendon of the brachioradialis and the flexor carpi radialis muscles (Fig. 5.8).

Identification, section and ligation of the radial artery
4.5 Step 5
The radial artery is dissected distally to proximally by transecting and cauterizing the deeper branches that supply the muscles of the forearm and the radius. It’s important to maintain the integrity of the paratenon when performing this dissection. Vessels, fascia and skin must be sutured, usually with few stitches with Vicryl 3–0, to avoid superficial devascularization. The tendon of the flexor muscles and palmaris longus (not present in our dissection and reported to be absent in 20% of patients) are exposed (Fig. 5.9).

Subfascial dissection of the flap. Intermuscular septum with radial artery and concomitantes veins and tendon of brachiradial (lateral) and radial flexor palmaris (medial) are exposed
4.6 Step 6
In the distal third of the forearm, where the radial artery is not covered by muscle bellies, the septum contains the highest number of cutaneous perforators. In this area numerous small branches directed to the deep muscle and to the radial bone have to be identified and cauterized or clipped (Fig. 5.10).

Elevation of the flap and identification of numerous deep perforating vessels
Exposure of the proximal radial artery and the venae comitantes is achieved by separating the brachioradialis from the flexor carpi radialis (Fig. 5.11).

Exposure of the radial artery up to the antecubital fossa
4.7 Step 7
The dissection of the medial border of the brachiradialis muscle and its lateral retraction allows the exposure of the pedicle in its entire length (Fig. 5.12).

Retraction of the brachioradialis muscle to expose the vascular pedicle
Some perforator branches from the radial artery are identified in the middle and proximal third of the forearm and clipped (Fig. 5.13). It is advisable to cauterize or tight the vessels as far as possible from the pedicle to avoid its damage.

Identification of the proximal perforating vessels of the radial artery
4.8 Step 8
The vascular pedicled is traced proximally until the desired length is reached, depending on the subsequent kind of reconstruction. It is possible to harvest the pedicle up to the confluence with the brachial artery. The length of the pedicle has to be long enough to reach the donor vessels, but an excessive long pedicle could generate a kneeling or a kinking, thus increasing the risk of thrombosis (Fig. 5.14).

Vascular pedicles are freed for their whole length
4.9 Step 9
At the same way, the cephalic vein is exposed up to the level of the antecubital fossa, where a venous anastomosis between superficial and deep circulation can be usually identified. Harvesting the vein proximal to this point allows the surgeon to maintain both superficial and deep venous drainage. Otherwise, it is possible to harvest separately the cephalic vein and venae comitantes (Fig. 5.15). At this point, the tourniquet is deflated, and accurate hemostasis is obtained with bipolar forceps or hemoclips if necessary. Accurate hemostasis is of paramount importance to prevent bleeding after flap inset and hematoma formation. Section of the pedicle is not performed until the recipient vessels are ready for anastomosis (Fig. 5.15).

Cephalic vein is followed up to the antecubital fossa. Note the interindependent cours of the arterial pedicle and the superficial vein pedicle
5 Final Aspect of the Flap
Once the demolitive procedure has been completed, vascular pedicles are carefully sectioned and the flap is detached (Fig. 5.16). The vessels of the flap may be divided at any point along their course to reach the recipient vessels, avoiding kinking.

The radial forearm flap with the radial artery, the comitantes veins, and the cephalic vein
6 Donor Site Closure
The radial forearm flap is a highly reliable method of reconstruction, but there are some donor site problems that may be encountered (total or partial loss of skin, necrosis, seroma, infection, wound dehiscence). Many skin closure method has been proposed, but as of today, the topic is somewhat controversial.
Many surgeons prefer to harvest a split-thickness skin graft from distant sites (thigh, groin), but adjuntive morbidities including pain, infection, or hypertrophic scar formation have to be considered. Other authors report the use of a suprafascial dissection technique with primary closure of the forearm and split-thickness skin graft.
Some recent studies demonstrate that suprafascial harvest of the radial free flap decreases the incidence of postoperative tendon exposure at the donor site, resulting in a reduced burden of postoperative wound management [10, 11].
A few authors have suggested alternative closure including tissue expanders, full-thickness skin grafts, and transposition flaps to improve outcomes. An other alternative the ulnar-based transposition flap as an alternative closure method for small donor defects.
The authors generally perform the skin closure after flap harvesting with a full-thickness skin graft previously harvested. In this case, at the beginning of the procedure, a full-thickness skin graft can be elevated on the volar face of the forearm. The skin graft is isosceles triangle shaped, with the height twice the radial forearm flap length, in the direction of the forearm axis. The base of the triangle is the same as the width of the proximal side of the forearm flap. The skin graft is then preserved in physiological solution until the flap has been detached. The cutaneous margins of the defect must be dissected to favor the subsequent suture of the proximal portion of the donor site. The suction drainage should be placed in the most cranial portion of the surgical field to avoid the skin graft failure (Fig. 5.17).

Final aspect of the the forearm with the residual surgical defect
The skin graft is positioned with the base on the distal side of the residual defect, and both sides are progressively sutured to the residual skin graft. The proximal portion of the forearm is close with V-Y advancement technique. Multiple slits in the graft are made to prevent fluid collection and to allow the graft to be stretched to cover a large area. After the suture is completed, wet gauzes (with paraffin) and compressive dressing (tie-over) are made and take in place for 7–10 days (Fig. 5.18).

Placement of the skin graft. A compressive-dressing is used to cover and facilitate healing
Most authors have concluded that, without subjective complaints and patient’s noticing interference with activities of daily living, the morbidities associated with RFFF are acceptable and well tolerated, even after long-term follow-up.
7 Composite Flaps
7.1 Tendon-Fasciocoutaneous Radial Forearm Flap
The palmaris longus muscle and tendon can be seen by flexing the wrist and touching the pads of the first and fifth finger. If present, it will be visible in the midline of the anterior wrist. It is absent in up to 15% of individuals. It is a weak flexor and provides no substantial flexing force, so tendon removing does not cause significant loss of hand function.
In the head and neck, the tendon is mainly used in lower lip reconstruction or static facial suspension.
After preoperative identification, the flap is draped over the tendon. The flap is elevated in a standard fashion, and the palmaris longus tendon is incorporated in the flap by incising the deep fascia medial to the tendon, down to the deeper muscle. The proximal and the distal ends of the tendon are transected 2 cm from the flap.
When the palmaris longus tendon is absent, the flexor carpi radialis tendon can be used as alternative, with limited functional impairment.
7.2 Osteo-Fasciocutaneous Radial Forearm Flap
It is possible to harvest a forearm flap with a portion of the radius with the advantage to have a composite flap with a long pedicle and thin and pliable skin. Unfortunately, the bone is inadequate for bone-integrated implants and reconstruction of areas subject to great force and torque, as in case of mandible reconstruction after segmental resection. Moreover, the limited bone length (about 12 cm) that can be harvested, the risk of forearm fracture, and the long period of postoperative forearm rehabilitation, entail the use of the flap only for selected cases of midface and periorbital reconstruction.
Up to 40% of the circumference of a mid-lateral portion of the radius can be harvested. The available bone lies between the insertion of the pronator teres muscle and the insertion of the brachioradialis muscle laterally at the base of the radial styloid. During the flap harvesting, the lateral dissection has to be conduit deep to the brachioradialis tendon and muscle that have to be widely retracted, to make the dissection quite lateral to the radial artery avoiding the injury to the perforator that supplies the bone. On the opposite medial side, the dissection requires the incision of the deep fascia over the pronator quadratus, flexor pollicis longus, and flexor digitorum superficialis muscles that are exposed after medial retraction of the flexor carpi radialis muscle and lateral gentle retraction of the flap with the vascular pedicle not yet distally divided. The partial release and retraction of the flexor digitorum superficialis muscle permit the exposure of the flexor pollicis longus that is longitudinally cut exposing the periosteum of the medial surface of the radius. After the exposure of the bone, the radial artery and the comitantes vein can be distally legated and resected, anchoring the proximal stump to the fascial portion of the flap. With a high-speed oscillating saw in the medial-lateral direction, the radius is cut along its length, taking care to leave intact about 60% of the circumference of the bone and to perform the proximal and distal osteotomies with an angle of about 45° to avoid the creation of stress point. After the bone resection is done, the osteo-fasciocutaneous flap is completely elevated, and prophylactically plate fixation of the remaining radius is done with appropriate thickness plate fixed out of the bone gap with 2/3 bicortical screw proximally and distally. The fixed plate must be completely covered by muscles and skin mobilized over the lateral forearm, and a skin graft covers the soft tissue. For three weeks after surgery, the forearm is immobilized by a volar splint.
References
Henker DD, et al. Perforator anatomy of the radial forearm free flaps versus the ulnar forearm free flap for head and neck reconstruction. Int J Oral Maxillofac Surg. 2016;45(8):955–9.
Song R, Gao Y, Song Y, Yu Y, Song Y. The forearm flap. Clin Plast Surg. 1982;9(1):21–6.
Ichinose A, Tahara S, Terashi H, Yokoo S, Nakahara M, Hashikawa K, Kenmoku K. Importance of the deep vein in the drainage of a radial forearm flap: a haemodynamic study. Scand J Plast Reconstr Surg Hand Surg. 2003;37(3):145–9.
Futran ND, Stack BC Jr. Single versus dual venous drainage of the radial forearm free flap. Am J Otolaryngol. 1996;17(2):112–7.
Gottlieb LJ, Tachmes L, Pielet RW. Improved venous drainage of the radial artery forearm free flap: use of the profundus cubitalis vein. J Reconstr Microsurg. 1993;9(4):281–4; discussion 284–5.
Boutros S, et al. Neural anatomy of the radial forearm flap. Ann Plast Surg. 2000;44(4):375–80.
Kim JH, Rho YS, Ahn HY, Chung CH. Comparison of sensory recovery and morphologic change between sensate and nonsensate flaps in oral cavity and oropharyngeal reconstruction. Head Neck. 2008;30(8):1099–104.
Namin AW, Varvares MA. Functional outcomes of sensate versus insensate free flap reconstruction in oral and oropharyngeal reconstruction: a systematic review. Head Neck. 2016;38(11):1717–21.
VanderWilde RS, Wood MB, Zu ZG. Hand replantation after 54 hours of cold ischemia: a case report. J Hand Surg Am. 1992;17(2):217–20.
Shonka DC, et al. Suprafascial harvest of the radial forearm flap decreases the risk of postoperative tendon exposure. Ann Otol Rhinol Laryngol. 2017;126(3):224–8.
Schwarzer C, et al. Donor site morbidity and flap perfusion of subfascial and suprafascial radial forearm flaps: a randomized prospective clinical comparison trial. J Craniomaxillofac Surg. 2016;44(9):1299–304.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Pellini, R., Ghirelli, M., Ferreli, F., Pichi, B., Mercante, G., Molteni, G. (2020). Radial Forearm Flap. In: Pellini, R., Molteni, G. (eds) Free Flaps in Head and Neck Reconstruction. Springer, Cham. https://doi.org/10.1007/978-3-030-29582-0_5
Download citation
DOI: https://doi.org/10.1007/978-3-030-29582-0_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-29581-3
Online ISBN: 978-3-030-29582-0
eBook Packages: MedicineMedicine (R0)