
Abstract
The effects of alcohol consumption vary considerably and depend on the concentration and dose, together with various other factors, such as nutritional status, gender, and ethnicity. The present chapter analyzes the main medical consequences related to alcohol consumption on cardiovascular system. Low-to-moderate ethanol consumption has been linked to a reduced cardiovascular risk, with a J-shaped or U-shaped dose-response curve. However, alcohol intake has been associated with several cardiovascular diseases, such as hypertension, cardiomyopathy, coronary artery disease, and stroke. In particular, chronic alcohol consumption induces several alterations in the cardiovascular system, including low-grade systemic inflammation, hyperuricemia, dyslipidemia, hyperhomocysteinemia, increased oxidative stress with enhanced lipid peroxidation, impaired glucose tolerance with insulin resistance, endothelial dysfunction, arterial hypertension, and alcoholic cardiomyopathy. From a clinical point of view, all the mentioned mechanisms are able to modify the pathophysiology of atherosclerosis. In sum, although several studies have described a J-shaped or U-shaped curve to describe the relationship between alcohol intake and total and cardiovascular mortality, these studies have been observational and epidemiological in nature. Promoting alcohol for those who do not drink and/or the use of alcohol as a cardioprotective strategy is not recommended.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Alcohol
- Ethanol
- Cardiovascular disease
- Atherosclerosis
- Alcoholic cardiomyopathy
- Coronary heart disease
- Peripheral artery disease
- Stroke
Introduction
Alcohol is contained in different beverages consumed since ancient times in most countries around the world. In the past, it has been reported that the consumption of low dose of alcohol (1–2 drinks/day in men and 1 drink/day in women) is associated with decreased cardiovascular risk with a J-shaped dose-response curve. In the 1990s, Renaud et al. showed that in France, wine consumption protected from coronary heart disease, despite a high intake of saturated fat, the so- called French paradox [1].
The moderate consumption of alcoholic beverages seems to have a protective effect on arterial stiffness due to different alcohol-related mechanisms, such as increase in high-density lipoprotein cholesterol (HDL-C), decrease in platelet adhesivity to the endothelium, and changes in fibrinogen and fibrinolytic system [2, 3]. However, despite these findings, the consumption of alcohol for therapeutic purposes on cardiovascular risk should not be encouraged due to the potential risk of damage on several organs and apparatus and development of alcohol use disorders (alcohol abuse and alcohol dependence).
Both acute and chronic alcohol consumption may induce toxic effects on different organs, in particular on liver, digestive, nervous, and cardiovascular systems [4]. Alcohol plays a pivotal role on several cardiovascular disorders , such as alcoholic cardiomyopathy, coronary heart disease (CHD), cardiac arrhythmias, peripheral artery disease (PAD), and ischemic and hemorrhagic stroke [1, 5]. Moreover, ethanol promotes the development of arterial hypertension, and it negatively affects lipid profile, glucose metabolism, and systemic inflammation (with a pro-inflammatory effect at high doses), promoting atherosclerosis [2].
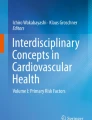
In the present chapter, the effects of alcohol on the cardiovascular system will be analyzed, and the most frequent diseases related to alcohol use and abuse will be discussed according to the most recent scientific data (Fig. 1).

Mechanisms involved in cardiovascular damage due to alcohol abuse. CV cardiovascular, NO nitric oxide
Alcohol, Atherosclerosis, and Cardiovascular Risk Factors
Several studies have shown that low-to-moderate alcohol consumption reduces the cardiovascular risk [6,7,8,9]. Renaud et al. in 1992 described the “French paradox,” which consisted in a reduced incidence of CHD among French population despite a high intake of saturated fat. The explanation of this phenomenon was ascribed to the consumption of wine, as well as to the consumption of similar amount of ethanol consumed in the form of beer and spirits [1]. Despite evidences of the role of alcohol in reducing HDL-C (responsible for transporting cholesterol from arteries to the liver, decreasing accumulation of cholesterol in arterial wall and thus the formation of atherosclerotic plaque), Renaud et al. proposed that a moderate intake of alcohol could inhibit platelet aggregation, thus preventing myocardial infarction.
Subsequently, different studies have shown that the consumption of moderate amount of alcoholic beverages, wine in particular, was associated with cardiovascular benefits. The attention was particularly focused on the role of polyphenols, especially resveratrol (a polyphenol contained in red wine), and their antioxidant and anti-inflammatory effects [10]. However, a prospective cohort study by Semba et al. showed that resveratrol does not associate with inflammatory markers of cardiovascular disease and it does not seem to significantly influence health status and mortality risk [11]. Further studies are needed to verify the impact of resveratrol on cardiovascular risk.
Despite these weak evidences, it should be underlined that chronic alcohol consumption has a negative impact on cardiovascular risk factors (progression of atherosclerosis, arterial damage, and increased cardiovascular mortality) [2]. A prospective cohort study by O’Neill et al. showed that heavy alcohol consumption in men increased arterial stiffness, with consequent reduced responsiveness to pressure variations, thus indicative of both functional and structural vascular adverse changes [12]. Moreover, regular ethanol consumption influences blood pressure in a dose-dependent manner. At low doses (less than 10 gram/day), alcohol has a vasorelaxant effect [2], but at higher doses, alcohol increases blood pressure [11]. Chronic heavy drinking represents one of the most common reversible causes of hypertension [13], and its effect on the development of arterial hypertension is independent of age, smoking, obesity, salt intake, education level, and type of alcoholic beverage [14].
Pathophysiological mechanisms of arterial hypertension due to alcohol abuse are different. The pivotal role seems to be played by oxidative stress and endothelial injury, in addition to vascular responsiveness. It seems that alcohol sensitizes vascular reactivity to α-adrenoceptor agonists in aorta and in segments of superior mesenteric artery. Furthermore, ethanol reduces endothelial nitric oxide (NO) formation. A further mechanism involved is the activation of the renin-angiotensin-aldosterone (RAA) system and the increased central adrenergic activity. Moreover, long-term exposure to alcohol affects baroreflex activity through the control of heart rate [15]. Recently, genetic polymorphisms of aldehyde dehydrogenase 2 (ALDH2) have been related to alcoholic hypertension. ALDH2 is an enzyme involved in ethanol metabolism, turning acetaldehyde into acetate; the presence of a mutant or inactive ALDH2*2 gene increased the risk of hypertension through accumulation of acetaldehyde [16]. Finally, it should be underlined that blood pressure control usually improves with abstinence from alcoholic beverages [2].
Ethanol is also involved in glucose metabolism. Low-to-moderate drinking inhibits gluconeogenesis and glycogenolysis, and it improves insulin sensitivity, while heavy drinking eliminates these effects. With this regard, ethanol consumption induces β-cell dysfunction mediated by oxidative stress, and it is responsible of increased insulin resistance [17, 18]. Furthermore, ethanol acts by regulating appetite peptides such as ghrelin and leptin [18]. Ghrelin is an orexigenic peptide that has a proliferative and protective role on β-cells; it stimulates insulin secretion in response of high circulating glucose levels. This peptide is also able to reduce endogenous glucose production [18]. Leptin is an anorexigenic peptide able to suppress the production of ghrelin increasing insulin secretion and glucose utilization; leptin has a role in diabetogenic imbalance, leading to beta-cell dysfunction, insulin resistance, obesity, and impairment of liver function in glucose metabolism [18, 19]. Chronic alcohol abuse deregulates ghrelin and leptin systems, in favor this latter, and it leads to impaired insulin secretion, increased endogenous glucose production, and increased insulin resistance.
An additional mechanism involved in impaired glucose metabolism is the effect of alcohol on brain-derived neurotrophic factor (BDNF). BDNF is a neurotrophin expressed especially in the nervous system. It has a role in regulating neuronal survival, differentiation, synaptic plasticity, cognitive function, and memory [18]. People with type 2 diabetes have low levels of BDNF that seems to correlate with severity of insulin resistance [18]. Nakagawa et al. demonstrated that BDNF plays a role in regulating glucose metabolism, reducing food intake, and lowering blood glucose in the obese diabetic mice [20]. They also studied the effect of BDNF on normoglycemic mice with impaired glucose tolerance, demonstrating that BDNF administration improves insulin resistance [20]. Chronic alcohol exposure decreases BDNF levels leading to impaired glucose metabolism. However, the exact mechanism of BDNF in the pathophysiology of type 2 diabetes after ethanol intake needs to be further investigated.
Alcohol plays also a role in visceral obesity. A review by Bendsen et al. shows an association between beer consumption and abdominal adiposity in men [21].
Moreover, ethanol affects systemic inflammation. At low doses, alcohol has an anti-inflammatory effect. At high doses, it has a pro-inflammatory role, affecting levels of inflammasomes, interleukins, cytokines, tumor necrosis factor, C-reactive protein, NADPH activation, and lipid peroxidation, with increased oxidative stress, glutathione and superoxide dismutase (SOD) depletion, endothelial dysfunction, increase of endothelial nitric oxide synthase expression, and monocyte adhesion to the endothelium [2, 22, 23]. As known, inflammation has a fundamental role in the pathogenesis of atherosclerosis, mediating all stages of this disease from initiation through progression and thrombotic complications [21].
All these factors contribute to increase cardiovascular risk in chronic alcohol abuse.
Alcohol and Coronary Heart Disease
Several studies have shown that moderate alcohol intake reduces the risk of new-onset coronary heart disease (CHD) , angina, myocardial infarction, and cardiovascular mortality [5, 24,25,26,27]. The role of different alcoholic beverages on CHD risk has been examined, but the benefits of components other than ethanol, such as antioxidants, have not been proved [2, 10, 11].
A meta-analysis by Costanzo et al. described a J-shaped association between wine consumption and vascular risk and between beer consumption and vascular risk [28]. Moreover Rebecca et al. recently showed that the type of alcoholic beverages (beer, wine, or liquor) did not influence CHD risk. Therefore, the benefits of alcoholic beverages on vascular risk may derive from ethanol and not from other components, such as polyphenols found in red wine [29].
As previously mentioned, the mechanisms involved in the decrease of CHD risk by low-to- moderate ethanol consumption are multiple, in particular increase in HDL-C and apolipoprotein A-I, decrease in LDL cholesterol, increased adiponectin, reduced gluconeogenesis, decrease in platelet agreeability, changes in fibrinogen and fibrinolysis system, and a decrease in inflammatory system responses [30,31,32].
Recently, Xu et al. showed that Chinese stable CHD patients with ALDH 2 mutated genotype were vulnerable to coronary artery lesions and had lower levels of HDL-C with respect to ALDH 2 wild genotype [3]. Moreover, low-to-moderate alcohol intake was protective for multi-vessel coronary artery lesion in ALDH2 wild genotype group [3].
The beneficial effect of alcohol on coronary risk disappears at higher doses [28, 33, 34]. Besides quantity of ethanol consumed (low to moderate vs. high), also drinking patterns seem to impact on CHD . Rehm et al. showed that irregular heavy drinking increases the risk of coronary artery disease via unfavorable impacts on blood lipids and effects on clotting, increasing the risk of thrombosis [35].
Alcohol and Peripheral Artery Disease
Peripheral artery disease (PAD) is the manifestation of atherosclerosis on lower extremities, mainly caused by the interaction of cited cardiovascular risk factors (aging, smoking, diabetes mellitus, dyslipidemia, hypertension, obesity, etc.) on arteries. PAD typically produces intermittent claudication with pain while walking or at rest.
The “PREDIMED Study” [36] demonstrated that a healthy lifestyle is associated with a substantially reduced risk of PAD. Thus, adherence to a Mediterranean diet (MedDiet), including moderate alcohol intake other than to a regular physical activity, normal weight (BMI < 25), and non-smoking must be encouraged. However, although some studies showed that low-to-moderate alcohol consumption is associated to a reduced risk of PAD [37], data on the effects of chronic intake of large amount of alcohol on PAD are lacking. A retrospective population-based cohort study comparing patients with alcohol intoxication, age, and gender matched with patients without alcohol intoxication investigated the relation between high level of alcohol and atherosclerosis in lower extremities. Patients with alcohol intoxication had a significantly higher cumulative incidence rate of PAD than those without alcohol intoxication. Increased risk has been shown in both men and women [37]. Thus, alcohol intoxication, besides complications of alcohol abuse, should be also considered a major risk factor of PAD . Further studies are needed to evaluate the quantitative effect of alcohol use on PAD.
Alcohol and Stroke
A recent meta-analysis by Zhan and co-workers summarized evidences regarding alcohol consumption and risk of stroke [38]. According to these results, a low alcohol intake is associated with a reduced risk of stroke morbidity and mortality, while heavy alcohol intake is associated with an increased risk of total stroke [38].
A recent study by Costa and co-workers analyzed the relationship between alcohol intake and the risk of intracerebral hemorrhage (ICH). Participants were stratified into excessive drinkers (>45 g of alcohol), light-to-moderate drinkers, or nondrinkers: among white people aged 55 years and older, high alcohol intake was found to exert a causal effect on this cerebrovascular event, with a prominent role in the vascular pathologies underlying deep ICH [39].
Alcohol and Heart: Cardiac Arrhythmias
The toxic effect of alcohol on the heart is influenced by genetic, ethnic, and behavioral factors. Toxicity mostly targets myocytes, highly sensitive to ethanol. The damage is dose dependent, and it can be reversible with abstinence. In some cases, irreversible structural damage develops with cell death by apoptosis and development of fibrosis [2].
The most frequent acute toxic effect of ethanol on the heart is represented by arrhythmias. A positive association between episodic binge drinking (consumption >5 drinks per occasion) and onset of atrial fibrillation has been described in literature [12]. On this connection, heavy alcohol consumption is associated with atrial extrasystoles and atrial fibrillation, common manifestations of the so-called holiday heart syndrome. Even ventricular extrasystoles and ventricular tachycardia (that may result in sudden death) can be associated with alcohol abuse [40].
The arrhythmogenic effect of ethanol seems to be due to alterations in calcium homeostasis, in mitochondrial functions, and in contractile proteins leading to impaired myocardial function. Other mechanisms involved are prolongation of conduction times, of QT interval, and of myocyte refractory periods in the setting of increased sympathetic activity during alcohol withdrawal syndrome and of electrolytic imbalance (such as hypokalemia and hypomagnesaemia) that often accompanies heavy drinking. These conditions act altering transmembrane potentials [41].
Moreover, alcohol use disorder (AUD) is often associated with other substance use disorders or psychiatric comorbidities; these conditions expose patients to QT-prolonging therapies such as tricyclic antidepressants, selective serotonin reuptake inhibitors (SSRIs), and antipsychotic drugs, leading to a major risk of sudden cardiac death [40].
However, it should be underlined that acute arrhythmogenic effect of ethanol is infrequent in individuals with normal heart function and it is often associated with a structural myocardial damage , representing a clinical manifestation of alcoholic dilated cardiomyopathy [2, 40].
Alcohol and Heart: Alcoholic Cardiomyopathy
Chronic exposure of the heart to high doses of alcohol can result in alcoholic cardiomyopathy (AC), a disease characterized by dilation and impaired contraction of one or both myocardial ventricles in the presence of normal or reduced ventricular wall thickness [4].
According to epidemiological data, alcoholic cardiomyopathy is one of the main causes of non-ischemic dilated cardiomyopathy in Western countries [41]; an excessive alcohol intake is evidenced in almost half of cases of this cardiac disease [42]. Although several studies have tried to estimate the exact prevalence of AC, available data are not conclusive [2]. The reported prevalence of alcoholic cardiomyopathy in patients treated in alcohol addiction unit is between 21% and 32% [43, 44]. The diagnosis of AC can be performed in the presence of a history of chronic alcohol abuse after the exclusion of other causes of dilated non-ischemic cardiomyopathies [4, 12].
The effect of ethanol on ventricular function is dose dependent, even if the exact quantity and duration of alcohol consumption to induce cardiac damage are still unknown. There is no agreement on the quantity and duration of alcohol abuse to produce AC. However, according to the majority of the literature, 80 grams/day for at least 5 years represents a reliable cut-off [1].
However, because of different genetic, ethnic, and behavioral factors, not all the heavy drinkers will develop AC. HLA-B8, alleles of the alcohol dehydrogenase, and nongenetic factors, such as thiamine deficiency and exposure to other cardiotoxic substances (e.g., cocaine, previously utilized beer additives like cobalt and arsenic), are involved [45]. There is no difference in the prevalence of AC in males and females [46].
Evidences of alcohol-induced toxicity to myocardial cell have been reported [47] both in binge drinkers and in chronic alcohol abuse. In acute consumption, alcohol has been shown to promote myocardial inflammation, detectable by the raising in serum troponin concentration [48]. In chronic consumption, alcohol seems to produce alterations in myocytes as hypertrophy, apoptosis and necrosis, and intracellular structure dysfunction, modification of contractile proteins and calcium homeostasis, mitochondrial degeneration, and fibrosis [49]. Moreover, alcohol metabolites (acetaldehyde and ethyl esters) promote oxidative damage and lipid peroxidation causing the alteration of excitation-contraction sequence [29, 47, 50]. Thus, alcohol leads to the reduction of myofibrillar proteins and the expression of different isoforms of myosin that results in depressed cardiac contraction [51]. As a consequence, the decrease in cardiac output and the dilatation of the left ventricle ensue from the long-term activation of compensatory mechanisms (hyperactivation of sympathetic nervous system, RAA system, cytokines, and natriuretic peptide), resulting in increased preload and the hypertrophy of normal myocytes [52].
The natural history of AC is not completely understood for the scarcity of evidences and because of the few studies available [4, 42]. There are also uncertainties regarding the clinical progression of the disease and the prognosis. It is known that end-stage AC is characterized by left ventricle dilatation and systolic dysfunction but, if ventricular dilatation and ejection fraction impairment are preceded or not by hypertrophy and diastolic dysfunction, has not been completely clarified [4]. Diastolic dysfunction has been proposed as an early manifestation of AC [2]. Even systolic dysfunction (reduction in left ventricular ejection) can be found in a subclinical stage, and it seems to involve about 13% of heavy alcohol drinkers [2]. Clinical manifestations of AC appear at end stage when the damage is advanced. Signs and symptoms are those of congestive heart failure, and they are correlated to reduced cardiac output: dyspnea, orthopnea, bilateral peripheral edema, fatigue, oliguria, and nycturia. At physical examination, jugular vein distension, tachyarrhythmia, and third and/or fourth tone can be present. Moreover, it should be underlined that AC can be accompanied by alcoholic liver disease (ALD) and neurological disorders typical of AUD patients.
Regarding the diagnosis of AC, no specific clinical, instrumental, or histological features have been identified. AC remains a diagnosis of exclusion in the presence of a positive patient history of alcohol intake/abuse. Heavy drinking should be accurately evaluated and confirmed by biomarkers of alcohol abuse (gamma-glutamyltranspeptidase, mean corpuscular volume, carbohydrate-deficient transferrin, and ethyl glucuronide) and by the consultation of an alcohol addiction specialist [53]. ECG is not specific; it can show ST segment and/or T-wave alterations and any arrhythmias secondary to cardiac dilatation. Chest X-ray can document cardiomegaly, pulmonary congestion, and pleural effusion. Echocardiography can help to identify hypertrophy, dilatation, and systolic and diastolic dysfunction at early stage, and it can exclude other causes of heart failure, such as other diagnostic tools like magnetic resonance (MR) and biopsy.
The cornerstone of the treatment of AC is total alcohol abstinence or, at least, a significant reduction of alcohol consumption [2, 54]. Thus, the correct identification and treatment of AUD in the context of an alcohol addiction unit are of primary importance, even for the possibility to manage pharmacotherapies (i.e., anti-craving drugs) [55, 56]. Moreover, as recommended by the ESC Guidelines, patients have to receive a specific treatment for heart failure (i.e., beta-blockers, ace inhibitors, angiotensin receptor antagonists, diuretics, angiotensin receptor-neprilysin inhibitor (ARNI)) [57]. In case of persistent severe ventricular dysfunction, even with a maximally optimized therapy, an ICD implant and heart transplantation could be considered [57].
Currently, new strategies are being evaluated for the treatment of AC. In course of study, there are inhibitors of pathways involved in myocyte hypertrophy and cell loss (myostatin, sirtuins, caspase, etc.), drugs for the control of cardiac fibrosis (miRNAs, TGF-β, relaxin, etc.), drugs for the control of oxidative damage (cardiomyokines, leptin, ghrelin, etc.), and treatments direct to myocyte regeneration and repair (telocytes and stem cells [4, 58]).
Prognosis of AC has not been completely defined because of lack of evidences. Generally, AC patients show a better prognosis and a longer transplantation-free survival than patients affected by idiopathic dilated cardiomyopathy [42]. The presence of atrial fibrillation, QRS duration >120 ms, and lack of beta-blocker therapy seem to represent independent predictors of mortality [42]. Moreover, the long-term prognosis seems to be influenced also by the course of AUD; in fact worsening of systolic function is directly related to the amount and to the duration of alcohol consumption [4]. However, although total alcohol abstinence represents the gold standard in the treatment of AC, data of a correlation between reduction of alcohol intake and cardiac improvement are still lacking [4].
Conclusion
Data on the potential benefits of low-to-moderate alcohol intake on cardiovascular risk are at present still debated and controversial. At present, promoting alcohol consumption for those not drinking or the use of alcohol as a cardioprotective strategy is not recommended for the risk of organ damage and of alcohol misuse.
Acknowledgment
We wish to thank Mariangela Antonelli, Tommaso Dionisi, Daniele Ferrarese, Carolina Mosoni, Claudia Tarli, Alberto Tosoni and Gabriele Vassallo for their cooperation in the literature review useful to finalize the present chapter.
References
Renaud S, de Lorgeril M. Wine, alcohol, platelets, and the French paradox for coronary heart disease. Lancet. 1992;339(8808):1523–6.
Fernández-Solà J. Cardiovascular risks and benefits of moderate and heavy alcohol consumption. Nat Rev Cardiol. 2015;12(10):576–87.
Xu L, Zhao G, Wang J, et al. Impact of genetic variation in aldehyde dehydrogenase 2 and alcohol consumption on coronary artery lesions in Chinese patients with stable coronary artery disease. Int Heart J. 2018;59:689–94.
Mirijello A, Tarli C, Vassallo GA, et al. Alcoholic cardiomyopathy: what is known and what is not known. Eur J Intern Med. 2017;43:1–5.
Ricci C, Wood A, Muller D, Gunter MJ, Agudo A, Boeing H, et al. Alcohol intake in relation to non-fatal and fatal coronary heart disease and stroke: EPIC-CVD case-cohort study. BMJ. 2018;361:k934.
Thun MJ, Peto R, Lopez AD, et al. Alcohol consumption and mortality among middle-aged and elderly U.S. adults. N Engl J Med. 1997;337:1705–14.
Renaud SC, Gueguen R, Schenker J, d’Houtaud A. Alcohol and mortality in middle-aged men from eastern France. Epidemiology. 1998;9:184–8.
Waskiewicz A, Sygnowska E, Drygas W. Relationship between alcohol consumption and cardiovascular mortality – the Warsaw Pol-MONICA project. Kardiol Pol. 2004;60:552–62. discussion 563
Ronksley P, Brien S, Turner B, Mukamal K, Ghali W. Association of alcohol consumption with selected cardiovascular disease outcomes: a systematic review and meta-analysis – with comments. BMJ. 2011;342:d671.
Biagi M, Bertelli AAE. Wine, alcohol and pills: what future for the French paradox? Life Sci. 2015;131:19–22.
Semba RD, Ferrucci L, Bartali B, et al. Resveratrol levels and all-cause mortality in older community-dwelling adults. JAMA Intern Med. 2014;174(7):1077–84.
O’Neill D, Britton A, Brunner EJ, Bell S. Twenty-five-year alcohol consumption trajectories and their association with arterial aging: a prospective cohort study. J Am Heart Assoc. 2017;6(2): pii: e005288.
O’Keefe EL, Di Nicolantonio JJ, O’Keefe JH, Lavie CJ. Alcohol and CV health: Jekyll and Hyde J-curves. Prog Cardiovasc Dis. 2018;61:68–75.
Katsiki N, Tziomalos K, Mikhailidis DP. Alcohol and the cardiovascular system: a double-edged sword. Curr Pharm Des. 2014;20:6276–88.
Crestani CC, Lopes da Silva A, Scopinho AA, Ruginsk SG, Uchoa ET, FMA C, et al. Cardiovascular alterations at different stages of hypertension development during ethanol consumption: time-course of vascular and autonomic changes. Toxicol Appl Pharmacol. 2014;280(2):245–55.
Hu N, Zhang Y, Nair S, Culver BW, Ren J. Contribution of ALDH2 polymorphism to alcoholism-associated hypertension. Recent Pat Endocr Metab Immune Drug Discov. 2014;8:180–5.
Pietraszek A, Gregersen S, Hermansen K. Alcohol and type 2 diabetes. A review. Nutr Metab Cardiovasc Dis. 2010;20:366–75.
Kim S-J, Kim D-J. Alcoholism and diabetes mellitus. Diabetes Metab J. 2012;36(2):108–15.
Addolorato G, Capristo E, Greco AV, Stefanini GF, Gasbarrini G. Influence of chronic alcohol abuse on body weight and energy metabolism: is excess ethanol consumption a risk factor for obesity or malnutrition? J Intern Med. 1998;244(5):387–95.
Nakagawa T, Tsuchida A, Itakura Y, Nonomura T, Ono M, Hirota F, et al. Brain-derived neurotrophic factor regulates glucose metabolism by modulating energy balance in diabetic mice. Diabetes. 2000;49:436–44.
Bendsen NT, Christensen R, Bartels EM, Kok FJ, Sierksma A, Raben A, et al. Is beer consumption related to measures of abdominal and general obesity? A systematic review and meta-analysis. Nutr Rev. 2013;71:67–87.
Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. 2002;105:1135–43.
Obad A, Peeran A, Little JI, Haddad GE, Tarzami ST. Alcohol-mediated organ damages: heart and brain. Front Pharmacol. 2018;9:81.
Wells S, Broad J, Jackson R. Alcohol consumption and its contribution to the burden of coronary heart disease in middle-aged and older New Zealanders: a population-based case-control study. N Z Med J. 2004;117:U793.
Camargo CA, Stampfer MJ, Glynn RJ, Grodstein F, Gaziano JM, Manson JE, et al. Moderate alcohol consumption and risk for angina pectoris or myocardial infarction in U.S. male physicians. Ann Intern Med. 1997;126(5):372–5.
Mukamal KJ, Chiuve SE, Rimm EB. Alcohol consumption and risk for coronary heart disease in men with healthy lifestyles. Arch Intern Med. 2006;166(19):2145–50.
Song RJ, Nguyen X-MT, Quaden R, Ho Y-L, Justice AC, Gagnon DR, et al. Alcohol consumption and risk of coronary artery disease (from the Million Veteran Program). Am J Cardiol. 2018;121(10):1162–8.
Costanzo S, Di Castelnuovo A, Donati MB, Iacoviello L, de Gaetano G. Wine, beer or spirit drinking in relation to fatal and non-fatal cardiovascular events: a meta-analysis. Eur J Epidemiol. 2011;26(11):833–50.
Department of Agriculture Dietary Guidelines Recommendation. In: https://health.gov/dietaryguidelines/2015/resources/2015-2020_Dietary_Guidelines.pdf.
Demrow HS, Slane PR, Folts JD. Administration of wine and grape juice inhibits in vivo platelet activity and thrombosis in stenosed canine coronary arteries. Circulation. 1995;91(4):1182–8.
Miceli M, Alberti L, Bennardini F, Di Simplicio P, Seghieri G, Rao GHR, et al. Effect of low doses of ethanol on platelet function in long-life abstainers and moderate-wine drinkers. Life Sci. 2003;73(12):1557–66.
Brien SE, Ronksley PE, Turner BJ, Mukamal KJ, Ghali WA. Effect of alcohol consumption on biological markers associated with risk of coronary heart disease: systematic review and meta-analysis of interventional studies. BMJ. 2011;342:d636.
Kloner RA, Rezkalla SH. To drink or not to drink? That is the question. Circulation. 2007;116:1306–17.
Foerster M. Alcohol drinking and cardiovascular risk in a population with high mean alcohol consumption. Am J Cardiol. 2009;103:361–8.
Rehm J, Roerecke M. Cardiovascular effects of alcohol consumption. Trends Cardiovasc Med. 2017;27(8):534–8.
Ros E, Martínez-González MA, Estruch R, Salas-Salvadó J, Fitó M, Martínez JA, et al. Mediterranean diet and cardiovascular health: teachings of the PREDIMED study. Adv Nutr. 2014;5(3):330S–6S.
Huang JY, Chen WK, Lin CL, Lai CY, Kao CH, Yang TY. Increased risk of peripheral arterial disease in patients with alcohol intoxication: a population-based retrospective cohort study. Alcohol. 2017;65:25–30.
Zhang C, Qin YY, Chen Q, Jiang H, Chen XZ, Xu CL, et al. Alcohol intake and risk of stroke: a dose-response meta-analysis of prospective studies. Int J Cardiol. 2014;174(3):669–77.
Costa P, Grassi M, Iacoviello L, Zedde M, Marcheselli S, Silvestrelli G, et al. Alcohol intake and the risk of intracerebral hemorrhage in the elderly: the MUCH-Italy. Multicenter Study on Cerebral Haemorrhage in Italy (MUCH-Italy) Investigators. Neurology. 2018;91(3):e227–35.
George A, Figueredo VM. Alcohol and arrhythmias: a comprehensive review. J Cardiovasc Med. 2010;11:221–8.
Guzzo-Merello G, Cobo-Marcos M, Gallego-Delgado M, Garcia-Pavia P. Alcoholic cardiomyopathy. World J Cardiol. 2014;6(8):771–81.
Guzzo-Merello G, Segovia J, Dominguez F, Cobo-Marcos M, Gomez-Bueno M, Avellana P, et al. Natural history and prognostic factors in alcoholic cardiomyopathy. JACC Heart Fail. 2015;3(1):78–86.
Regan TJ. Alcohol and the cardiovascular system. JAMA. 1990;264(3):377–81.
Urbano-Marquez A, Estruch R, Navarro-Lopez F, Grau JM, Mont L, Rubin E. The effects of alcoholism on skeletal and cardiac muscle. N Engl J Med. 1989;320:409–15.
Maisch B. Alcoholic cardiomyopathy: the result of dosage and individual predisposition. Herz. 2016;41(6):484–93.
Fernández-Solà J, Estruch R, Nicolás JM, Paré JC, Sacanella E, Antúnez E, et al. Comparison of alcoholic cardiomyopathy in women versus men. Am J Cardiol. 1997;80(4):481–5.
Klatsky AL. Alcohol and cardiovascular diseases: where do we stand today? J Intern Med. 2015;278(3):238–50.
Waszkiewicz N, Szulc A, Zwierz K. Binge drinking-induced subtle myocardial injury. Alcohol Clin Exp Res. 2013;37(8):1261–3.
Beckemeier ME, Bora PS. Fatty acid ethyl esters: potentially toxic products of myocardial ethanol metabolism. J Mol Cell Cardiol. 1998;30(11):2487–94.
Ren J, Wold LE. Mechanisms of alcoholic heart disease. Ther Adv Cardiovasc Dis. 2008;2(6):497–506.
Mahmoud S, Beauchesne LM, Davis DR, Glover C. Acute reversible left ventricular dysfunction secondary to alcohol. Can J Cardiol. 2007;23(6):475–7.
Laonigro I, Correale M, Di Biase M, Altomare E. Alcohol abuse and heart failure. Eur J Heart Fail. 2009;11(5):453–62.
Fernández-Solà J, Nicolás JM, Paré JC, Sacanella E, Fatjó F, Cofán M, et al. Diastolic function impairment in alcoholics. Alcohol Clin Exp Res. 2000;24(12):1830–5.
Voskoboinik A, Prabhu S, Ling LH, Kalman JM, Kistler PM. Alcohol and atrial fibrillation: a sobering review. J Am Coll Cardiol. 2016;68(23):2567–76.
Addolorato G, Mirijello A, Barrio P, Gual A. Treatment of alcohol use disorders in patients with alcoholic liver disease. J Hepatol. 2016;65(3):618–30.
Addolorato G, Abenavoli L, Leggio L, Gasbarrini G. How many cravings? Pharmacological aspects of craving treatment in alcohol addiction: a review. Neuropsychobiology. 2005;51(2):59–66.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–200.
Fernández-Solà J, Planavila PA. New treatment strategies for alcohol-induced heart damage. Int J Mol Sci. 2016;17(10):1651.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Section Editor information
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this entry

Cite this entry
Rando, M.M., Sestito, L., Mirijello, A., Addolorato, G. (2020). Alcohol and Cardiovascular Function. In: Govoni, S., Politi, P., Vanoli, E. (eds) Brain and Heart Dynamics. Springer, Cham. https://doi.org/10.1007/978-3-030-28008-6_51
Download citation
DOI: https://doi.org/10.1007/978-3-030-28008-6_51
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-28007-9
Online ISBN: 978-3-030-28008-6
eBook Packages: MedicineReference Module Medicine