
Abstract
In the USA, the Latinx population has been identified as a minority group subject to disproportionate exposure to unhealthy environments. Given that a vast majority of Latinx persons live in highly segregated neighborhoods in metropolitan areas, an understanding of how urban environments affect Latinx persons’ health opportunities is vital for reducing health disparities. In this chapter, we explore some dimensions of the urban environment and explain its relevance to Latinx communities’ health. We provide an overview of the social composition and spatial distribution of the Latinx population. Then, we present a conceptual model describing a general pathway of how the social, built, and natural ecologies of the urban environment influence Latinx communities’ health. We illustrate empirically how these ecologies interact at the neighborhood level to affect Latinx persons’ physical activity. We conclude with a list of actionable policy alternatives that can address urban health problems in Latinx neighborhoods.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Latinx populations
- Residential segregation
- Environment–health nexus
- Urban environments
- Physical activity
The burgeoning body of research on the social determinants of health has increased the attention to the significant disparities in morbidity and mortality across multiple subpopulations and their association with complex contextual variables. Although hardly a novel perspective, this approach emphasizes the need to restore the broken link between epidemiology and social urban analysis amidst the growing evidence that health outcomes are influenced by the interaction and intersection of biologic, societal, and environmental factors (Angotti & Sze, 2009; Corburn, 2007; Lawrence, 2004). At first, studies embracing a socio-ecological view of health examined primarily income, education, support networks, and other factors that are related to the social life of a person and can be ascribed to individual subjects. Later, researchers gradually started to focus their attention more on factors that are not specific to individuals and affect large groups because they share common living and working spaces (Evans, Whitehead, & Diderichsen, 2001; Woolf & Aron, 2013). Ultimately, this shift in focus led to the recognition that morbidity and mortality foreshadow patterns that are directly correlated with observable variations in the density of community-level factors and therefore predicate a gradient of exposure of groups and individuals to their effects (Galea, & Vlahov, Freudenberg, 2005; Galea & Vlahov, 2005).
In urban settings, this gradient exists because the distribution of social and physical environments that are conducive to good health is not evenly dispersed across social groups and spaces, resulting in clustering of disease and other situations that affect the ability of people to reach their potential in life. Because certain social groups, particularly racial and ethnic minorities, are consistently more exposed than others to the detrimental or beneficial effects of certain environments, it has become increasingly clear that health disparities have an inequity component that can be addressed only through interventions at the community level (Angotti & Sze, 2009; Woolf & Aron, 2013).
In the context of the USA, the Latinx population has been identified as a minority group subject to a disproportionate exposure to unhealthy environments. For instance, in a statewide study using pollutant concentration estimates for California, researchers found that cancer risk from exposure to ambient air toxins was higher among Latinx persons compared with members in other racial/ethnic groups. This association persisted even after controlling for other variables that predict localized ambient pollution burdens, such as land use, household income, population density, and home ownership (Pastor, Morello-Frosch, & Sadd, 2005). These findings were independently validated by survey results indicating that the Latinx population is the most likely racial/ethnic group in this state to consider regional air pollution a serious problem (45%), followed by the [non-Hispanic] black (black) (36%), [non-Hispanic] white (white) (29%), and Asian (24%) populations (Public Polity Institute of California, 2007).
The Latinx population is also disproportionately affected by overweight and obesity. According to data from the National Health and Nutrition Examination Survey (NHANES) 2011–2014, 42.5% of Latinx adults are obese. Obesity especially targets poor Latinx women and children. Approximately 45.7% of adult Latinx women are obese, as well as 21.9% of Latinx youth (Ogden, Carroll, Fryar, & Flegal, 2015). The effect of overweight and obesity is significant, as 18% of Mexican-origin Latinx adults have diabetes compared with 9.6% of non-Latinx white adults (National Center for Health Statistics, 2017). The findings of a number of studies agree that, aside from biological factors, obesity in Latinx communities reflects the limited availability of affordable, healthy food in racial/ethnic minority neighborhoods, along with urban conditions that discourage physical activity (Abercrombie et al., 2008; Lopez & Hynes, 2009; Sister, Wolch, & Wilson, 2010; Wolch, Wilson, & Fehrenbach, 2005; Zenk, Schulz, Odoms-Young, & Lockett, 2009). Thus, in addition to income and education, inadequate access to a healthy living environment is the feature of the urban places that are key to explain the prevalence of chronic diseases in Latinx communities.
Given that a vast majority of Latinx persons live in metropolitan areas, with most of them living in highly segregated neighborhoods, an understanding of whether and how urban environments affect Latinx persons’ health opportunities is vital for reducing disparities in health (Logan, 2011). In this chapter, we explore some dimensions of the urban environment and explain its relevance to the health of Latinx communities. We first provide an outlook of the Latinx population, with an emphasis on its social composition and spatial distribution. We then present a conceptual model describing a general pathway of how the social, built, and natural ecologies of the urban environment influence the health of Latinx communities. Then, drawing on research we conducted in the Phoenix Metropolitan Area, we illustrate how these ecologies intersect and interact at the neighborhood level, affecting the active lifestyle opportunities of Latinx persons. We conclude with a list of actionable policy alternatives that potentially can address urban health problems in Latinx neighborhoods.
The Latinx Population and the City
“Latinx” is a generic term used to designate a diverse and changing segment of the US population that shares a strong connection with the cultures and societies of Latin America and the Spanish-speaking Caribbean. In 2015, with a population of 54.2 million, Latinx persons constituted 17.1% of the total US population and were the largest racial/ethnic minority in the nation (U.S. Census, 2015). The Mexican-origin population makes up the largest Latino subgroup (63.8%), followed by Puerto Rican (9.5%) and Cuban (3.7%) populations. Starting in the early 1980s, a surge in the number of migrants from Central and South America increased the contribution of persons from Salvador, Guatemala, Colombia, and other countries in the total Latinx population. Concurrently, the US Latinx population, while still highly concentrated in a few states, has diversified its geographic footprint, with individuals in recent years finding new places to settle beyond traditional Latinx gateways such as Los Angeles, Houston, or Chicago. The dispersal of Latinx in the USA has coincided with the rise of immigration from Mexico and Central America since the 1980s, with a significant number of newly arrived immigrants settling increasingly in smaller metropolitan and non-metropolitan areas in the South and the Midwest (Carr, Lichter, & Kafala, 2013; Stepler & Lopez, 2016; Tienda & Fuentes, 2014). Combined with the higher fertility of immigrant families already settled in the USA, changes in migration patterns during the latter quarter of the twentieth century contributed to an even a greater diversity of the Latinx population in terms of national origin, birthplace, legal status, and settlement patterns (Tienda & Fuentes, 2014).
Despite these changes, one thing that has remained unaffected is the fact that the Latinx population is basically an urban one. In 2015, 93.5% of Latinx resided in a metropolitan area, compared with 85.4% of the US general population. In 2018, 10 metropolitan areas alone housed almost one in two Latinx persons, with Los Angeles, New York, Miami, Houston, and Chicago at the top of the list of Latinx metro areas. The primary reason Latinx persons concentrate in cities is the work opportunities urban places provide, but also the accessibility to affordable housing, education, health services, and other resources that can be afforded only by high population density (Tienda & Fuentes, 2014). In fact, three specific trends indicate that the spatial distribution of the Latinx population is pointing toward a sustained growth of the Latinx urban imprint.
First, regardless of their size, most metropolitan areas in the USA have experienced an expansion in the Latinx population in the last 20 years, with so-called new-destination metropolitan areas such as Atlanta and New Orleans registering the highest growth pace and traditional Latinx metropolitan areas such as Los Angeles and New York with the largest absolute increase (Suro & Singer, 2002; Tienda & Fuentes, 2014). This trend is likely to continue even after the slowdown of immigration from Latin America, as most of the Latinx persons in these places are US-born citizens (Stepler & Lopez, 2016). Second, Latinx persons have increased their presence in suburban areas, joining a national trend in which black and Asian persons are also participating. Since 1980, the growth of the suburban Latinx population outpaced the growth of Latinx persons residing in central cities, and now, more than 54% of Latinx individuals reside in the suburbs (Onésimo Sandoval & Jennings, 2012; Suro & Singer, 2002). Third, the escalation of anti-immigrant policies and sentiments in recent years has been associated with a reduction of mobility and rising levels of residential segregation affecting Latinx communities (Amuedo-Dorantes, Puttitanun, & Martinez-Donate, 2013; Tienda & Fuentes, 2014; Varsanyi, 2010). These trends are likely to reinforce the persisting concentration of Latinx persons in cities and further the salience of hypersegregated barrios in many metropolitan areas.
Nexus Between the Urban Environment and Community Health
Within the past two decades, there has been a rapid proliferation of research on the nexus between the urban environment and health within the social epidemiologic literature (Northridge, Sclar, & Biswas, 2003). Fitzpatrick and LaGory (2011) suggest that the interest in understanding the role of environmental factors on health outcomes arises from the recognition that individual and household-level factors have limited explanatory power in isolation from the environmental context that shapes and supports human living (Fitzpatrick & LaGory, 2011). Additional impetus for this interest comes from the repeated observation that many health outcomes correlate with differences across geographic areas in the density and dispersal of influential environmental factors. In fact, the findings of some reviews suggest that both individual and environmental factors seem to be part of a reinforcing cycle that creates and reproduces health disparities across social, racial, and ethnic groups (D’Amato et al., 2015; Woolf & Aron, 2013).
Although offering critical information for new insights regarding the impact of environmental factors on health, this research has also drawn some criticism for being too narrowly focused on isolating singular environmental influences on health. For example, while determining the role of the number and dispersion of grocery stores in urban neighborhoods could be important for understanding the food choices of inner-city residents, it is clearly incorrect to assume that simply bringing new supermarkets to a neighborhood will change unhealthy eating habits or solve food insecurity of residents (Angotti & Sze, 2009). Stuck in tenacious and pervasive poverty, quotidian food practices among a majority of Latinx families are under constant siege. Feeding family members is an act in which food choices are shaped primarily by severe budgetary constraints, work-schedule pressures, precarious employment, scant household savings, and an increasingly restricted safety net. In addition, the spatial distribution of grocery stores in cities and its limiting effect on the food choices available to residents of inner-city neighborhoods is an expression of the combined effect of three interrelated forces that operate at different temporal and spatial scales: residential segregation, economic restructuring, and reorganization in the retail food industry (Zenk et al., 2009). Therefore, although the food landscape plays an important role in the reproduction of unhealthy nutrition practices, any attempt to explain them will be incomplete if the structural factors that concentrate poverty in Latinx neighborhoods and regulate availability and accessibility to food in a market-driven economy are not taken into account.
Hence, understanding the influence of urban environments on health, but particularly explaining disparities in health among different subpopulations and neighborhoods requires a conceptual framework that can explicate cities as social systems embedded in larger milieus (Northridge et al., 2003). Comprehensive conceptions of the influence of the urban environment in producing health disparities must encompass the social fabric and institutions that generate and reproduce the spatial isolation and marginalization of racial/ethnic minority groups and maintain the privilege of the majority, and the physical systems—built and natural—that provide material support to the functionality of dominant social structures (Fitzpatrick & LaGory, 2011; Galea et al., 2005; Galea & Vlahov, 2005).
Following from this perspective, the health of urban populations is a function of multiple factors, spawn from the social, built, and natural urban environments (see Fig. 13.1). This framework assumes that these three ecologies of the urban environment are embedded in an all-encompassing and evolving milieu that is driven by shifting societal values, population dynamics, global climate change, technologic innovation, and politics and governance. These larger forces are not deterministic, but their influence over cities is apparent on the impact of national policies and climate change or migration, to mention some of the structural forces that condition the ability of cities to secure prosperity and sustainability in an increasingly interconnected and competitive society.

The framework also borrows from social epidemiology the notion that the urban environment operates its influence over health outcomes through a pathway that includes distal and proximate factors (Klitzman, Matte, & Kass, 2006; Markevych et al., 2017). For example, urban sprawl and strict zoning, two distal factors linked to the built environment, result in high car dependency and substantial vehicular emissions, which in turn, lead to poor air quality, a proximal factor for respiratory diseases such as asthma. Clearly, the concentration of airborne pollutants in a particular area is influenced by topography and atmospheric conditions, so built environmental factors often interact with natural factors in influencing the respiratory health of populations exposed to poor air quality. The point here is that this framework also admits that the elements of the urban environment are not independent of each other and their influence on health outcomes does not necessarily follow a linear pathway. The three ecologies of the urban environment and their influence on health are described briefly.
Social Environment
The social urban environment refers to the group of values, norms, and institutions that shape individual and collective behaviors, with implications for public health. Many cities, for example, have passed laws that tax the sale of sugary drinks with the intention of discouraging their consumption and reducing the incidence of obesity and associated health problems (Colchero, Popkin, Rivera, & Ng, 2016; Levell, O’Connell, & Smith, 2016). Another example is the investment that a community makes to support after-school programs providing recreational and educational opportunities to children in racial/ethnic minority neighborhoods. These two examples illustrate elements in the social environment that reflect a deliberate, proactive community action seeking to steer human behavior in a certain and desirable direction. Some other elements of the social environment with influence on health are less explicit in their intentionality, but they are equally tangible. This is the case of social values and norms that sort individuals into societal categories and expose them to a variety of contexts on the basis of race, ethnicity, gender, income, and other traits.
Residential segregation is perhaps the most concrete expression of how social norms that categorize people on a variety of scales results in fragmented communities and creates spaces that isolate individuals within socially and physically homogenous spaces (Acevedo-Garcia, Lochner, Osypuk, & Subramanian, 2003; Logan, 2011; Schulz, Williams, Israel, & Lempert, 2002). Both concentration and isolation patterns seem to facilitate the reproduction of unhealthy behaviors associated with cardiovascular diseases and communicable diseases, such as tuberculosis, as well as limiting the access to primary health care, two conditions that contribute to the Latinx-white health gap (Anderson & Fullerton, 2014; Kramer & Hogue, 2009; Li, Wen, & Henry, 2017). These patterns also expose Latinx persons to disproportionate levels of urban violence, which is positively correlated with sedentarism and higher obesity rates (Forsyth et al., 2015; Lin et al., 2016). It is important to acknowledge that the social environment can be experienced at multiple scales, often simultaneously, including household, neighborhood, city, region, and even global scales. Embedded within an increasingly interconnected network of spaces, contemporary social environments are open structures subject to the influence of people, ideas, information, and values that are multisourced and in constant flux (Galea et al., 2005).
Built Environment
The built environment encompasses all the systems created by humans to shelter, connect, and support all forms of human activity in cities and their hinterland (Morello-Frosch & Jesdale, 2006; Northridge et al., 2003). By definition, cities are spaces that concentrate the highest density of such systems, as expressed in the concentration of housing, office buildings, parks, plazas, malls, streets, and other infrastructure networks that characterize urban places. As noted by Schulz and Northridge (2004), the built environment influences health through a range of pathways. Structures such as houses and office buildings, for example, are known to function as vessels of unhealthy indoor environments because their lack of maintenance, construction materials, technologies, and sanitary conditions promote the accumulation of mold, lead, or pests that increase the incidence of respiratory, neurologic, and infectious diseases. The spatial arrangement of workplaces, stores, housing, and other urban facilities resulting from strict zoning regulations can also have an impact on health by limiting the accessibility of jobs, consumption, and affordable housing, and by limiting the modes of transportation available to city residents (Sallis et al., 2016). The findings of some studies suggest that the atmosphere created by the form, accessibility, and aesthetic character of neighborhoods and other urban spaces influence children and adolescents’ level of engagement in physical activity (Christian et al., 2015; Timperio, Crawford, Ball, & Salmon, 2017; Timperio, Crawford, Telford, & Salmon, 2004).
Natural Environment
The natural environment refers to external tangible elements and processes that are produced by energy exchanges that occur continuously in nature and create ecologies in which the human body exists and which can influence its behavior and development. This environment includes landforms, soil types, vegetation, fauna, and climate. Although it was a reasonable assumption to think about the natural environment as a constant factor in models explaining urban health, the increasing unpredictability and variability of the global climate and the cauda of devastation and death caused by hurricanes and drought in cities across the world are making this supposition clearly untenable (Northridge et al., 2003). All of these factors are important to health because they can be both a resource and a hazard, depending on the ability of a society to maintain the delicate balance between human needs and nature’s needs. The natural environment can affect health through physical exposure, such as extreme variations in temperatures. Between 2006 and 2010, an average of 2,000 weather-related deaths occurred in the USA, of which most can be attributed to exposure to excessive natural cold or excessive natural heat (Berko, Ingram, Saha, & Parker, 2014). Extreme heat affects human health through heat stress and can exacerbate underlying medical conditions that lead to increased morbidity. Basu and Ostro (2008) estimated that, with each 10 °F increase in ambient temperature, there is a 2.6% increase in cardiovascular mortality, with the most significant risk associated with ischemic heart disease. Similarly, a growing body of the literature has documented that the rise in the prevalence of asthma and allergies is associated with increased air pollution in urbanized areas (Baldacci et al., 2015; D’Amato, Liccardi, D’Amato, & Cazzola, 2001). Research has identified specific physiological mechanisms by which air pollutants may promote airway sensitizing that may elevate the allergenicity of pollen and other airborne irritants present in urban areas (D’Amato, 2002; D’Amato et al., 2001, 2015). The impact of weather-related and ambience pollution on health also varies significantly across socioeconomic groups, racial/ethnic groups, regions, and neighborhoods (Morello-Frosch & Jesdale, 2006; Pastor et al., 2005).
Latinx Health and Urban Living
In this section, we use the framework described to explore the importance of the urban environment for the engagement of Latinx persons in active lifestyles. An active lifestyle, including regular leisure-time physical activity, can help individuals control weight, reduce the risk of cardiovascular disease, type 2 diabetes, metabolic syndrome, and some cancers; strengthen bones and muscles; and improve mental health and mood (Crespo, 2000; Powell & Blair, 1994; U.S. Surgeon General, 1999). As suggested by the results of a number of studies, Latinx persons do not engage in sufficient physical activity and may not be getting all the physiological and psychological health benefits associated with an active lifestyle, particularly leisure-time physical activity (Casper & Harrolle, 2013; Crespo, 2000; Cronan, Shinew, Schneider, Stanis, & Chavez, 2008; Lindsay, Sussner, Greaney, & Peterson, 2009). Research findings have indicated that the urban environment disproportionately affects the ability of Latinx persons to engage in an active lifestyle. First, Latinx persons are more likely to live in neighborhoods perceived as dangerous or unwelcoming, a circumstance that may discourage residents from engaging in outdoor activities, thus increasing the chance of sedentarism and isolation. Second, fragmented and homogenous spaces in metropolitan areas limit mobility and increase car dependency, reinforcing the propensity of Latinx persons toward sedentary lifestyles. Third, lack of greenery and expansive, hard surface buildup in Latinx neighborhoods upset natural processes, increasing air pollution and thermal discomfort, thus discouraging residents’ outdoor activity.
In particular, neighborhood parks have long been advocated as an essential ingredient for active urban living for all ethnic/racial groups (Loukaitou-Sideris, 1995; Jones, Brainard, Bateman, & Lovett, 2009; Wolch et al., 2005). Particularly, in increasingly multiethnic and socially fragmented urban contexts, public parks are potentially a key resource for leisure, solace, sense of community, and quality of life (Byrne & Wolch, 2009; Wolch, Byrne, & Newell, 2014). Accordingly, the results of a considerable number of studies suggest that urban parks contribute to healthier lifestyles by providing city residents with outdoor recreational opportunities, including green areas, open space, playgrounds, sport fields, and other amenities that encourage participation in different forms of physical activity. Proximity and density of parks have received great attention in these studies because people living closer to parks are more likely to exercise regularly—leading to weight loss, increased energy, and better health in general (Cohen, McKenzie, Sehgal, Williamson, Golinelli, & Lurie, 2007; Giles-Corti, Broomhall, Knuiman, Collins, Douglas, Ng, Lange, &Donovan, 2005; Kaczynski & Henderson, 2007; Nagel, Carlson, Bosworth, &Michael, 2008). Moreover, some researchers report that individuals living close to a park are more likely to report better self-perceived health than individuals who do not (Maas, Verheij, Groenewegen, De Vries, & Spreeuwenberg, 2006). The availability of parks has also been linked to mental and psychological well-being, as parks can create opportunities for social interaction, which in turn reduces isolation and increases life satisfaction, particularly among vulnerable populations (Kaźmierczak, 2013; Wood, Hooper, Foster, & Bull, 2017). Overall, research findings indicate a positive link between parks and people’s health and well-being (Maas, Verheij, Spreeuwenberg, & Groenewegen, 2008; Bedimo-Rung, Mowen, & Cohen, 2005; Chiesura, 2004).
Spatial equity research—the body of knowledge that systematically studies the geographic distribution of environmental burdens and amenities as a function of sociopolitical factors and processes (Jones et al., 2009; Sister et al., 2010; Talen, 1997)—has documented an unequal supply of public parks with regard to both race and ethnicity and socioeconomic status in many US cities. For example, in a study conducted in Los Angeles, white neighborhoods had 31.8 acres of park space for every 1,000 people, compared with 1.7 acres in black neighborhoods, and 0.6 acres in Latinx neighborhoods (Pincetl, Wolch, Wilson, & Longcore, 2003). Other studies also provide evidence that Latinx neighborhoods are likely to contain considerably fewer parks than non-Latinx neighborhoods, thereby reducing opportunities for an active lifestyle and recreation (Garcia, 2014; García, Gee, & Jones, 2016; Johnson Gaither, 2011; Kozlowski, 2008). Furthermore, the findings of other research indicate that parks in predominantly minority neighborhoods have fewer amenities and offer a less-than-pleasant experience for park goers than do parks located in predominantly non-minority neighborhoods in the suburbs (Bruton & Floyd, 2014; Jenkins et al., 2015; Sister et al., 2010; Suminski et al., 2012; Vaughan et al., 2013).
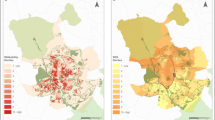
With the aim of illustrating in direct ways the nexus between the urban environment and health, we studied how residents of Latinx neighborhoods interact with their immediate living space for leisure-time physical activity. Using the greater Phoenix Metropolitan Area as a case study (Fig. 13.2), we explored the meaning and significance of neighborhood urban environments from Latinx women seeking an active lifestyle for themselves and their families. We evaluated three aspects.

Source Lara-Valencia, & Garcia-Perez, (2018)
Concentration of Latinx populations in the Phoenix Metropolitan Area in 2010.
-
What the women say about the importance of maintaining an active lifestyle.
-
The women’s perceptions of what makes public open space, especially parks, a resource for active living.
-
Strategies the women use to overcome barriers resulting from the concrete social, built, and natural ecologies of Latinx neighborhoods in the Phoenix Metropolitan Area.
Exploring the way residents of Latinx neighborhoods relate to public parks from these three angles allows us to examine how the various aspects of urban environment discussed above interact and intersect in the context of a metropolitan area in rapid demographic and cultural transformation.
Before we present some findings, we noted that the analysis presented here is part of a comparative multicity project on women’s perceptions of neighborhood resources and hazards for leisure-time physical activity. Here, we report the interviews with 12 Latinx women living in the Phoenix Metropolitan Area in 2017. The participants’ ages ranged from 27 to 48 years old, with a median of 35.7 years (Table 13.1). The length of residence in the area ranged from 1 to 34 years (median, 18.6 years). The majority of the participants were married or living as married (83%), had at least 1 year of high school education (83%), and were primarily immigrants from Mexico (83%). Most of the interviews were conducted in Spanish (92%) in a park during the spring months.
Challenges of Being Active
Generally speaking, Latinx women understand and value the benefits of being physically active. Almost all mentioned that they try to exercise regularly and also try to facilitate the participation of their children in sports and other forms of physical activity. Women cited benefits like keeping their weight in check, complying with medical recommendations, feeling well, or simply relaxing after a long day of work. Regardless of the source of their motivation, most of the women mentioned their home or neighborhood as a primary place for physical exercise.
On the very enthusiastic end of the spectrum was Patricia,Footnote 1 a Mexican immigrant in her forties who is a mother of three. Patricia moved to the Phoenix suburb of Glendale 24 years ago and, like most of the participants, has had to balance work and family demands, while finding some personal time to exercise, which frequently ends up being a location in the neighborhood. As she told us during the interview:
[I exercise] with the objective of feeling well, because lately I have been depressed, exhausted, and with exercise I feel more motivated. I have been to the gym, and nothing! Lately, I have been going to the neighborhood park early in the morning.
Through the interview, Patricia explained that exercise time for her is not only residual, but also has to complement her family’s needs in terms of recreation and exercise. In Patricia’s case, complementarity means that exercise time and place for her and her family have to overlap in order for her to stay physically active. As she explained:
Since my children do sports, I take advantage of their practice periods to do some exercise like jogging or running, or simply walking.
Similarly, Marina, an American woman of Central American decedent who is in her early thirties and runs a home-base daycare to support her four children, explained that despite doing a lot of physical work in her job, such as bending, lifting, and cleaning, she still exercises in the neighborhood.
Yes, sometimes I go for a walk to the neighborhood park and sometimes I go to the homes of my friends to exercise in [a] group.
For all women, motherhood and entry to the workforce are of the utmost significance in terms of their ability to be physically active. Bertha, an immigrant from Mexico and mother of two daughters, explains her level of activity before and after she becomes a mother.
…before, when I was 18 or 19… I had a job and I was able to go to the mountain to hike and all those things. But now I can’t do that, I have my daughters… I am a mom and also have a job. It is quite difficult…I have less time.
Overall, the circumstances of these Latinx women highlight the unquestionable relevance of the neighborhood environment for active living in the Phoenix Metropolitan Area. As suggested by the interviewees, being physically active could be challenging even for women who are knowledgeable and inclined to engage in physical exercise. For the women in these interviews, close-to-home facilities like neighborhood parks provide physical activity opportunities that are not only affordable but also essential, given the unyielding time constrains many of them face in their double role as mothers and employees. Other elements of the neighborhood’s built environment, such as sidewalks and tree canopies along streets, if properly maintained and planned, may also help women to navigate the pressures of daily life that act as barrier for active living. In fact, given prevailing theories on the positive impacts of walkable neighborhoods with access to parks for promoting physical activity, it would be easy to assume that improving walkability and accessibility to parks will be an appropriate intervention to pursue in Latinx neighborhoods of the Phoenix Metropolitan Area. However, even though such actions are steps in the right direction, transforming neighborhoods in spaces that encourage and sustain an active living requires more than simple physical interventions.
Neighborhood Parks as Assets for Active Living
A look at Latinx women’s experiences and perceptions regarding neighborhood parks reveals much about the significance of the urban environment for physical activity of Latinx women in the Phoenix Metropolitan Area. Through their own activity and that of their families, women are able to interact with the various elements of their neighborhood’s urban environment that affect their ability to use parks, streets, and other local open spaces for exercise or play. As conveyed by the interviews, the study participants have a significantly nuanced understanding of parks as a resource, and through their narratives they are able to unpack and weight each of the ecologies that shape the potential of Latinx neighborhoods for an active lifestyle.
All the women acknowledged the existence of a park in their neighborhood. However, many of them told us that the parks and their surroundings are not safe, and as a result, were not a good place for them or their families to exercise or play. Consider, for example, the following observation by Zaida, a Yaqui indigenous woman in her thirties—an observation that was similar to that in a number of other interviews.
I wouldn’t go to walk [especially at night]. Some of the streets in my neighborhood are dark, there is too much traffic, and drivers don’t pay attention to speed limits….
Male-dominated environments were commonly mentioned as ongoing problems in some of the neighborhoods. Women described how this situation affected their ability to use nearby parks or simply going out for a walk.
You don’t feel safe on the street or the park; I live near a trailer park and sometimes they (adult males) are out there simply sitting outside their homes… Some of them seem to be fixing their cars or their homes, but sometimes they just look at you and you don’t feel comfortable. I prefer to go to another park or a gym, so I can feel comfortable. (Patricia)
Crime and substance abuse in the neighborhood were often described as factors that inhibited the women from visiting local parks. They considered the presence of homeless individuals, discarded drug paraphernalia, and broken bottles as indications of risk of violence they chose to avoid. Mothers did not want their children exposed to people using drugs or being victims of violence, so they preferred to stay indoors or go to other places in the metropolitan area. Another common concern among the women was the presence of unleashed dogs in the street and parks of their neighborhood. Two women described their experience with this kind of incivility in the following manner:
Sometimes people come [to the park] with their dogs and they are unleashed… The last time I was here, about two weeks ago, they had a Pitbull here and did not have a leash…It was unleashed! (Marina)
No, I don’t like to walk on the street…I always see unleashed dogs and I am afraid of them. I don’t like my neighborhood for walking! (Bertha)
The women were asked about what amenities and features of the parks in their neighborhood they liked the most or were a concern. Their responses indicated that a variety of facilities, size, and design are important factors influencing the value of neighborhoods for physical activity and recreation. Most of the women agreed that the Phoenix Metropolitan Area has an adequate number of parks, but said that parks in Latinx neighborhoods need to adapt to the needs of the residents. For instance, most parks in Latinx neighborhoods have the same layout and amenities, including soccer fields and basketball courts, but lack walking paths or large free-play areas where young children can play safely. Diana, a 31-year-old Mexican immigrant, criticized the uniformity of parks in the area and highlighted the qualities of an ideal park.
[Parks] are so square! They only have basketball courts, tennis courts, soccer fields… we need a little bit more of variety, not only basketball and soccer. Yes, almost everywhere is the same! I like a park with trees and walking paths that are not straight, where you can go up and down.
Later in the interview, Diana described how much she enjoys being in a park where trees are abundant to shade the path while she walks, and where the design of the path would allow her to reach her daily fitness goals easier. She mentioned that these features are not present in the park near her home. That park is small, it has few trees, and after ten turns around its perimeter, exercising becomes monotonous and boring.
Some of the interviewed women noted that parks in their neighborhood are so small that visitors of different age groups compete for space and equipment. High visitation of small park areas produces saturation, which in turn, reduces the attractiveness of Latinx neighborhoods parks, especially for mothers with small children. As explained during the interviews, overpopulated playgrounds, particularly by teenagers who do not have dedicated spaces, are ground for tension, unwanted physical contact, and accidents affecting mostly young children. The following account by Bertha, a Mexican woman in her thirties, was repeated by many women in the study.
[The park] near to my house, I don’t like it, I don’t like it! It is hard, the environment… too much people! Too much people saying obscenities and kids fighting… and my two daughters see things….
The women were attracted to parks with open space, greenery, and tree canopy. Some expressed their dissatisfaction with the lack of replacement of trees fallen during the monsoon season, which makes parks less green and, in consequence, less appealing. They also showed preference for parks with large open spaces where their children could play freely and safely. Consider for example, the following observation by Cecilia, a Mexican woman in her late twenties with three children.
This park has a lot of open views. Right now, for example, I am here seated with my toddler and I can see where my two-year old boy is playing. I can see him! …there is a high visibility and there is a lot of grass. I like it because the playground’s equipment is not too high or dangerous.
The hot summers of the Arizona desert constrain outdoor activities to a narrow window of time encompassing early mornings and early evenings. As noted earlier, even though the women see parks as an important recreational asset, many are not able to use them because the parks frequently lack proper lighting during the so-called good hours for exercise. These good hours of exercise also often coincide with homeless and young people loitering or engaging in activities deemed unacceptable by some of the women. As described by Vilma, a 32-year-old Mexican immigrant who moved to Phoenix one year ago:
I don’t know if I should go [to the park], it does not look safe …there are many [homeless] men that are doing other things… they are not going to exercise or play.
In general, the women’s descriptions of their interactions with neighborhood parks are influenced by a variety of factors, including prominently perceived safety in and around the site, but also by the opportunities for physical activity resulting from its design, equipment, and greenery. One highlight of the descriptions is that individual women are most likely to relate to parks as bundles of amenities and services embedded in the neighborhood and linked to the three ecologies of the urban environment: social, built, and natural. This so-called bundling is a reflection of how close these three ecologies are intertwined. For example, the perceived safety of a park is directly affected by its design, which includes physical characteristics such as poor visibility of play areas, limited lighting, isolation, poor maintenance, and surrounding land uses, among others. Through appropriate design, parks planners could balance the negative impacts of a social environment that is perceived as threatening by women in Latinx neighborhoods. Another example of the interaction between ecologies is how good lighting could augment the night time usability of parks during the hot summer days of Arizona, which can also be mitigated by tree canopies and water bodies that are known to reduce ambient temperatures through shading and evapotranspiration.
Not All Parks Are Created Equal
The findings of a significant proportion of the research examining the nexus between the urban environment and health suggest profound disparities across racial/ethnic groups in the distribution of environmental factors, such as access to green space or walkable neighborhoods (García et al., 2016; Stodolska, 2015). Most of these studies tend to focus on quantitative dimensions of accessibility to those factors, such as distance to the nearest neighborhood park or the number of street intersections within the neighborhood. Although these types of studies contribute to essential analyses to understand the impact of environmental factors on active-living opportunities across social groups, they often overlook the subjective and perceived quality of those factors. Interestingly, studies in this field have also failed to produce conclusive findings on the magnitude and pervasiveness of these disparities and their cause.
In contrast, the Latinx women in this study are unequivocally convinced that urban environments, but especially parks, are not equal across neighborhoods. Among other things, we learned that women are very sensitive to conditions and features of parks. The women made it clear that parks’ social, physical, and natural characteristics are as important as proximity to their homes. In fact, many of the interviewed women traveled to different neighborhoods to use a park that offered the amenities and conditions they considered desirable: choice of recreational activity, large park space, safety, and cleanliness.
For example, Bertha traveled 20 min three times a week to gain access to an open space that provides the recreational opportunities that she and her family need. One of the most frequent referred motivations for this type of recreational commuting is that the destination park is “prettier,” it has “a little bit more light” at sunset, “has better mountain views,” and people in the park are simply “exercising or playing.” Clearly, the inequitable distribution of active-living environmental factors like safety, cleanliness, greenness, and well-designed neighborhood parks has not been overlooked by these Latinx women in this area.
We already mentioned many of the conditions of urban environments in Latinx neighborhoods that forced these women to avoid engagement with the outdoors or push them to other recreational destinations in the metro area. One factor that deserves special mention is the rigidity of open-space design that homogenizes use and produces parks that seem predisposed against diversity and change. Women in Latinx neighborhoods in the Metropolitan Phoenix Area perceived parks as male-oriented spaces that failed to accommodate the needs of diverse user groups and especially exclude women with caregiving responsibilities. Exclusion is particularly severe for women who face economic, social, or physical constraints that prevent them from traveling to other neighborhoods where urban environments offer more and better recreational opportunities and amenities.
Unpacking the Urban Environment–Health Nexus
Most city residents get their leisure-time physical activity in their neighborhood, and close-to-home open public spaces are frequently the most likely places to engage in physical activity (Casper & Harrolle, 2013). Therefore, urban environments in Latinx neighborhoods play a crucial role in facilitating or preventing active living and their associated health benefits. The environments do this by providing opportunities for children, adolescents, adults, and older adults to engage with the place they live during their leisure time and utilitarian physical activities.
Although proximity to open space, such as neighborhood parks, is important in determining whether residents in Latinx neighborhoods will engage in active living, we have argued and provided evidence that focusing on only one of the ecologies of the urban environment is not enough. As indicated earlier, a host of socio-environmental factors act as constraints that impede the translation of the availability of open space into active lifestyles among Latinx persons. To start with, demanding occupations and family responsibilities limit the availability for Latinx individuals to engage in leisure-time physical activity. Indeed, for some of the women interviewed in the study in the Phoenix Metropolitan Area, freeing time for exercise was a challenging proposition, considering the amount of physical effort that they and other income earners in their family exerted during a regular workday. Nonetheless, the perceived health benefits of an active lifestyle motivate many of these Latinx women to pursue leisure-time physical activity, which forces them to negotiate a variety of obstacles in their neighborhoods. These obstacles include streets that are unsafe for pedestrians, isolated parks where residents feel threatened by crime and incivilities, play areas that fail to accommodate the activity needs of different groups, or poorly designed spaces that are unlikely to bring pleasure or result in frequent visits. As we learned from the women interviewed, the parks in the area vary in quality, and existing differences in their recreational and amenity value justify traveling to get to parks where the desirable mix of social, built, and natural environmental elements is available.
The fact that engagement in active living is a multifactorial and multiscalar outcome is widely recognized, but research using this approach in the study of the Latinx urban environments is hard to find. There are several reasons for this. First, it is difficult to avoid the tendency in this type of research to fragment urban realities into pieces that are both appealing to academic audiences and can be easily processed by a well-established disciplinary apparatus. As explained by Corburn (2007), professionalization, technocratization, and bureaucratization are factors underlying the difficulty of bringing together the realms of public health and urban planning. Second, urban and public health researchers have hesitated to abandon the safety of established methodologic approaches based on mere quantification and need to embrace new methodologic approaches mixing quantitative tools (e.g., surveys, geospatial mapping) with visual ethnographies, focus groups, and other qualitative methodologies. Therefore, approaches that unbundle the multifactorial and multiscalar processes that link neighborhood urban environments and residents’ active lifestyles still need to be adopted. Third, prevailing conceptions of the influence of the urban environment on health are not only narrow and restrictive but also fail to accept the larger sociospatial processes, such as segregation and racial discrimination, that produce environmental inequities affecting Latinx persons and persons in other urban minority groups.
Conclusions and Recommendations for Future Research
This chapter represents an initial effort to map the complex relationship between neighborhood urban environments and the health of Latinx communities. The intention has been to highlight the point that the conditions that influence the level of physical activity of Latinx persons are complex and suggest a need for comprehensive approaches, recognizing that lifestyles leading to better health are the net effect of interacting and overlapping social, built, and natural neighborhood ecologies. Besides the obvious conceptual and analytic implications of this, there is also a need for all-inclusive strategies, including policies and programs to bring about changes in each of these ecologies if the goal is to actively pursue a healthier Latinx population. Overall, such changes should have as a priority the removal of barriers to physical activity and the conversion of neighborhoods into safe, accessible, and attractive places for all Latinx individuals. The transformation of Latinx neighborhoods into active-living spaces requires the application of old and new ideas, many of which were suggested in the accounts of the Latinx women we talked to in the Phoenix Metropolitan Area.
First, a good place to start is to see Latinx neighborhoods as disarticulated spatial systems that need to be reconnected by linking streets, school yards, parks, and other public facilities in a network for active human mobility. Many cities in the USA, and around the world, are using this approach to promote walking, cycling, running, and mobility because of their beneficial effect on public health and sense of community (Sallis et al., 2016). The creation of these types of networks is an intervention that is likely to contribute to the reduction of obesity and the incidence of non-communicable diseases among residents of Latinx neighborhoods. Furthermore, such networks provide a way to expand the amount of available public open space while augmenting near-to-home opportunities for recreation and exercise by improving the accessibility of parks and creating trails connecting parks and other public spaces within the neighborhood. Having additional walking venues closer to residences may encourage individuals to increase their level of physical activity, particularly for residents with demanding work schedules or transportation constraints.
Second, perceived safety is as a factor that will affect the beneficial impact of the creation of such network. It is imperative then, that signs of disorder in the neighborhood, such as vandalism, trash, unleashed dogs, uncontrolled traffic, and loitering be eliminated. Many of these things require effective actions to control crime, improve street and park lighting, and eliminate so-called hideouts for engaging in undesirable behaviors. As Stodolska (2015) suggested, it is also important to obtain current information about perceived safety issues, not only from residents using neighborhood parks, but also from nonusers, as they may be affected the most by existing safety issues.
Third, equally important are efforts to redesign public open space, including local streets and parks, in order to accommodate a diverse demand for active-living opportunities from women, men, children, and older adults living in Latinx neighborhoods. It is obvious that if residents of Latinx neighborhoods are to derive the greatest health benefit of public parks, diverse types of park amenities and services must be provided. The creation of active environments supportive of a diverse demand should focus on designing neighborhood parks that are safe and attractive especially to Latinx women, as they tend to be less physically active than women who identify with other US ethnic/racial groups and who (as are other women) are particularly sensitive to conditions that affect their perception of parks as a hazard or a resource and have significant influence in the level of activity of other family members.
Fourth, cities should organize regular events to encourage neighborhood residents to engage in physical activity. Examples include walking, yoga, dance groups, and other organized activities that appeal to Latinx residents and meet the needs of a diverse group of users. Indeed, opportunities for both moderate and vigorous activities are needed, particularly for women and older adults—two groups clearly excluded by park facilities that are often biased toward men and youth (Cohen et al., 2016). In particular, many Latinx women will be encouraged to participate if such efforts, as suggested by Stodolska (2015), include such things as childcare services and activities for the entire family.
Lastly, in agreement with many other scholars, we want to emphasize that the creation of active, supportive urban environments should be a regular function not only for urban planning departments but also for public health departments in cities and towns in metropolitan areas (Christian et al., 2015; Corburn, 2007; Northridge et al., 2003; Sallis et al., 2016). Urban planners and public health professionals should set a priority to reconnect their practices and priorities with the needs of minority populations who are particularly affected by inadequate and outdated planning, designs, and maintenance of streets, parks, public transportation, and other environmental elements that could trigger the activation of residents in Latinx neighborhoods.
Notes
- 1.
All individuals’ names in this chapter are pseudonyms.
References
Abercrombie, L. C., Sallis, J. F., Conway, T. L., Frank, L. D., Saelens, B. E., & Chapman, J. E. (2008). Income and racial disparities in access to public parks and private recreation facilities. American Journal of Preventive Medicine, 34, 9–15.
Acevedo-Garcia, D., Lochner, K. A., Osypuk, T. L., & Subramanian, S. V. (2003). Future directions in residential segregation and health research: A multilevel approach. American Journal of Public Health, 93, 215–221.
Amuedo-Dorantes, C., Puttitanun, T., & Martinez-Donate, A. P. (2013). How do tougher immigration measures affect unauthorized immigrants? Demography, 50, 1067–1091.
Anderson, K., & Fullerton, A. (2014). Residential segregation, health, and health care: Answering the Latino question. Race and Social Problems, 6, 262–279.
Angotti, T., & Sze, J. (2009). Environmental justice practice: implications for interdisciplinary urban public health. In N. Freudenberg, S. Klitzman, & S. Saegert (Eds.), Urban health and society: Interdisciplinary approaches to research and practice (pp. 19–42). San Francisco: Jossey-Bass.
Baldacci, S., Maio, S., Cerrai, S., Sarno, G., Baiz, N., Simoni, M., et al. (2015). Allergy and asthma: Effects of the exposure to particulate matter and biological allergens. Respiratory Medicine, 109, 1089–1104.
Basu, R., & Ostro, B. D. (2008). A multicounty analysis identifying the populations vulnerable to mortality associated with high ambient temperature in California. American Journal of Epidemiology, 168, 632–637.
Bedimo-Rung, A. L., Mowen, A. J., & Cohen, D. A. (2005). The Significance of Parks to Physical Activity and Public Health: A Conceptual Model. American Journal of Preventive Medicine ,28(2):159–168.
Berko, J., Ingram, D. D., Saha, S., & Parker, J. D. (2014). Deaths attributed to heat, cold, and other weather events in the United States, 2006–2010. In National health statistical reports (p. 15). Hyattsville, MD: National Center for Health Statistics.
Bruton, C. M., & Floyd, M. F. (2014). Disparities in built and natural features of urban parks: Comparisons by neighborhood level race/ethnicity and income. Journal of Urban Health, 91, 894–907.
Byrne, J., & Wolch, J. (2009). Nature, race, and parks: past research and future directions for geographic research. Progress in Human Geography , 33 (6), 743–765.
Carr, P., Lichter, D., & Kafala, M. (2013). Can immigration save small-town America? In Research and policy brief series, issue 53. Ithaca, NY: Community and Regional Development Institute. https://cardi.cals.cornell.edu/sites/cardi.cals.cornell.edu/files/shared/documents/ResearchPolicyBriefs/Policy-Brief-April13.pdf.
Casper, J. M., & Harrolle, M. G. (2013). Perceptions of constraints to leisure time physical activity among Latinos in Wake County, North Carolina. American Journal of Health Promotion, 27, 139–142.
Cohen, D., McKenzie, T., Sehgal, A., Williamson, S., Golinelli, D., & Lurie, N. (2007). Contribution of public parks to physical activity. American Journal of Public Health ,97.
Chiesura, A. (2004). The role of urban parks for the sustainable city. Landscape and Urban Planning, 68(1), 129–138.
Christian, H., Zubrick, S. R., Foster, S., Giles-Corti, B., Bull, F., Wood, L., et al. (2015). The influence of the neighborhood physical environment on early child health and development: A review and call for research. Health & Place, 33, 25–36.
Cohen, D. A., Han, B., Nagel, C. J., Harnik, P., McKenzie, T. L., Evenson, K. R., et al. (2016). The First National Study of Neighborhood Parks. American Journal of Preventive Medicine, 51, 419–426.
Colchero, M. A., Popkin, B. M., Rivera, J. A., & Ng, S. W. (2016). Beverage purchases from stores in Mexico under the excise tax on sugar sweetened beverages: Observational study. BMJ, 352.
Corburn, J. (2007). Reconnecting with our roots. Urban Affairs Review, 42, 688–713.
Crespo, C. J. (2000). Encouraging physical activity in minorities: Eliminating disparities by 2010. Physician & Sportsmedicine, 28, 36–51.
Cronan, M. K., Shinew, K. J., Schneider, I., Stanis, S. A. W., & Chavez, D. (2008). Physical activity patterns and preferences among Latinos in different types of public parks. Journal of Physical Activity and Health, 5, 894–908.
D’Amato, G. (2002). Environmental urban factors (air pollution and allergens) and the rising trends in allergic respiratory diseases. Allergy, 57(Suppl 72), 30–33.
D’Amato, G., Holgate, S. T., Pawankar, R., Ledford, D. K., Cecchi, L., Al-Ahmad, M. … Annesi-Maesano, I. (2015). Meteorological conditions, climate change, new emerging factors, and asthma and related allergic disorders. A statement of the World Allergy Organization. World Allergy Organization Journal, 8, 25.
D’Amato, G., Liccardi, G., D’Amato, M., & Cazzola, M. (2001). The role of outdoor air pollution and climatic changes on the rising trends in respiratory allergy. Respiratory Medicine, 95, 606–611.
Evans, T., Whitehead, M., & Diderichsen, F. (2001). The social basis of disparities in health. In T. Evans, M. Whitehead, F. Diderichsen, A. Bhuiya, & M. Wirth (Eds.), Challenging inequities in health: From ethics to action (pp. 13–23). New York: Oxford University Press.
Fitzpatrick, K., & LaGory, M. (2011). Unhealthy cities: Poverty, race, and place in America. London: Routledge.
Forsyth, A., Wall, M., Choo, T., Larson, N., Van Riper, D., & Neumark-Sztainer, D. (2015). Perceived and police-reported neighborhood crime: Linkages to adolescent activity behaviors and weight status. Journal of Adolescent Health, 57, 222–228.
Galea, S., Freudenberg, N., & Vlahov, D. (2005). Cities and population health. Social Science & Medicine, 60(5), 1017–1033.
Garcia, J. (2014). Does living in Latino neighborhoods affect risk for obesity? Findings from a study of social capital and parks availability in Los Angeles neighborhoods (Unpublished dissertation). Los Angeles, CA: University of California.
García, J. J., Gee, G. C., & Jones, M. (2016). A critical race theory analysis of public park features in Latino immigrant neighborhoods. Du Bois Review: Social Science Research on Race, 13, 397–411.
Giles-Corti, B., Broomhall, M. H., Knuiman, M., Collins, C., Douglas, K., Ng, K., Lange, A., & Donovan, R. J. (2005). Increasing walking: How important is distance to, atractivennes and size of public open space?. America Journal of Preventive Medicine, 28(2):169–176.
Jenkins, G., Yuen, H., Rose, E., Maher, A., Gregory, K., & Cotton, M. (2015). Disparities in quality of park play spaces between two cities with diverse income and race/ethnicity composition: A pilot study. International Journal of Environmental Research and Public Health, 12, 8009.
Johnson Gaither, C. (2011). Latino park access: Examining environmental equity in a “New Destination” county in the South. Journal of Park and Recreation Administration, 29(4), 37–52.
Jones, A. P., Brainard, J., Bateman, I. J., & Lovett, A. A. (2009). Equity of access to public parks in Birmingham, England. Environmental Research Journal, 3, 237–256.
Kaczynski, A. T., & Henderson, K. A. (2007). Environmental correlates of physical activity: A review of evidence about parks and recreation. Leisure Sciences, 29.
Kaźmierczak, A. (2013). The contribution of local parks to neighbourhood social ties. Landscape and Urban Planning, 109, 31–44.
Klitzman, S., Matte, T., & Kass, D. (2006). The urban physical environment and its effects on health. In N. Freudenberg, S. Galea, & D. Vlahov (Eds.), Cities and the health of the public (pp. 61–84). Nashville, TN: Vanderbilt University Press.
Kozlowski, J. C. (2008). Equity in Latino neighborhood parks. Parks and Recreation, 43, 26–28.
Kramer, M. R., & Hogue, C. R. (2009). Is segregation bad for your health? Epidemiologic Reviews, 31, 178–194.
Lara-Valencia, F., & Garcia-Perez, H. (2018). Disparities in the provision of public parks in neighbourhoods with varied Latino composition in the Phoenix Metropolitan Area. Local Environment, 23(12), 1107–1120.
Lawrence, R. J. (2004). Housing and health: From interdisciplinary principles to transdisciplinary research and practice. Futures, 36, 487–502.
Levell, P., O’Connell, M., & Smith, K. (2016). Sugary drinks tax: Response from the Institute for Fiscal Studies. The Lancet, 387, 1907–1908.
Li, K., Wen, M., & Henry, K. A. (2017). Ethnic density, immigrant enclaves, and Latino health risks: A propensity score matching approach. Social Science and Medicine, 189, 44–52.
Lin, A. R., Menjívar, C., Ettekal, A. V., Simpkins, S. D., Gaskin, E. R., & Pesch, A. (2016). “They will post a law about playing soccer” and other ethnic/racial microaggressions in organized activities experienced by Mexican-origin families. Journal of Adolescent Research, 31, 557–581.
Lindsay, A. C., Sussner, K. M., Greaney, M. L., & Peterson, K. E. (2009). Influence of social context on eating, physical activity, and sedentary behaviors of Latina mothers and their preschool-age children. Health Education & Behavior, 36, 81–96.
Logan, J. R. (2011). Separate and unequal: The neighborhood gap for blacks, Hispanics and Asians in metropolitan America. Project US2010. https://s4.ad.brown.edu/Projects/Diversity/Data/Report/report0727.pdf.
Lopez, R. P., & Hynes, H. P. (2009). Obesity, physical activity and the urban environment: Public health research needs. In H. P. Hynes & R. P. Lopez (Eds.), Urban health: Readings in social, built, and physical environments of U.S. cities (pp. 169–181). Sudbury, MA: Jones and Bartlett.
Loukaitou-Sideris, A. (1995). Urban Form and Social Context: Cultural Differentiation in the Uses of Urban Parks. Journal of Planning Education and Research 14(2), 89–102.
Markevych, I., Schoierer, J., Hartig, T., Chudnovsky, A., Hystad, P., Dzhambov, A. M. … Fuertes, E. (2017). Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environmental Research, 158, 301–317.
Maas, J., Verheij, R., Groenewegen, P., De Vries, S., & Spreeuwenberg, P. (2006). Green space, urbanity, and health: How strong is the relation?. Journal of Epidemiol and Community Health, 60(7), 587–592.
Maas, J., Verheij, R., Spreeuwenberg, P., & Groenewegen, P. (2008). Physical activity as a possible mechanism behind the relationship between green space and health: A multilevel analysis. BMC Public Health, 8
Morello-Frosch, R., & Jesdale, B. M. (2006). Separate and unequal: Residential segregation and estimated cancer risks associated with ambient air toxics in U.S. metropolitan areas. Environmental Health Perspectives, 114, 386–393.
Nagel, C. L., Carlson N. E., Bosworth, M., & Michael, Y. L. (2008). The Relation between Neighborhood Built Environment and Walking Activity among Older Adults. American Journal of Epidemiology, 168(4), 461–468.
National Center for Health Statistics. (2017). Health, United States, 2016: With chartbook on long-term trends in health. Hyattsville, MD: National Center for Health Statistics.
Northridge, M. E., Sclar, E. D., & Biswas, P. (2003). Sorting out the connections between the built environment and health: A conceptual framework for navigating pathways and planning healthy cities. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 80, 556–568.
Ogden, C. L., Carroll, M. D., Fryar, C. D., & Flegal, K. M. (2015). Prevalence of obesity among adults and youth: United States, 2011–2014. In NCHS data brief (p. 8). Hyattsville, MD: National Center for Health Statistics.
Onésimo Sandoval, J. S., & Jennings, J. (2012). Barrios and hyper barrios: How Latino neighborhoods changed the urban built environment. Journal of Urbanism: International Research on Placemaking and Urban Sustainability, 5, 111–138.
Pastor, M., Morello-Frosch, R., & Sadd, J. L. (2005). The air is always cleaner on the other side: Race, space, and ambient air toxics exposures in California. Journal of Urban Affairs, 27, 127–148.
Pincetl, S., Wolch, J., Wilson, J., & Longcore, T. (2003). Toward a sustainable Los Angeles: A “nature’s services” approach. Los Angeles, CA: Center for Sustainable Cities, University of Southern California.
Powell, K. E., & Blair, S. N. (1994). The public health burdens of sedentary living habits: Theoretical but realistic estimates. Medicine and Science in Sports and Exercise, 26, 851–856.
Public Polity Institute of California. (2007). Latino attitudes and the environment. In Just the facts: San Francisco: Public Polity Institute of California. http://www.ppic.org/content/pubs/jtf/JTF_LatinoAttitudesEnvironmentJTF.pdf.
Sallis, J. F., Bull, F., Burdett, R., Frank, L. D., Griffiths, P., Giles-Corti, B., et al. (2016). Use of science to guide city planning policy and practice: How to achieve healthy and sustainable future cities. Lancet, 388, 2936–2947.
Schulz, A., & Northridge, M. E. (2004). Social determinants of health: Implications for environmental health promotion. Health Education & Behavior, 31, 455–471.
Schulz, A. J., Williams, D. R., Israel, B. A., & Lempert, L. B. (2002). Racial and spatial relations as fundamental determinants of health in Detroit. Milbank Quarterly, 80, 677–707.
Sister, C., Wolch, J., & Wilson, J. (2010). Got green? Addressing environmental justice in park provision. GeoJournal, 75, 229–248.
Stepler, R., & Lopez, M. H. (2016). U.S. Latino population growth and dispersion has slowed since onset of the Great Recession (p. 53). Washington, DC: Pew Research Center. http://www.pewhispanic.org/2016/09/08/latino-population-growth-and-dispersion-has-slowed-since-the-onset-of-the-great-recession/.
Stodolska, M. (2015). Recreation for all: Providing leisure and recreation services in multi-ethnic communities. World Leisure Journal, 57, 89–103.
Suminski, R. R., Connolly, E. K., May, L. E., Wasserman, J., Olvera, N., & Lee, R. E. (2012). Park quality in racial/ethnic minority neighborhoods. Environmental Justice, 5, 271–278.
Suro, R., & Singer, A. (2002). Latino growth in metropolitan America: Changing patterns, new locations. Washington, DC: The Brookings Institution, Center on Urban and Metropolitan Policy, and Pew Hispanic Center.
Talen, E. (1997). The social equity of urban service distribution an exploration of park access in Pueblo, Colorado, and Macon, Georgia. Urban Geography, 18, 521–541.
Tienda, M., & Fuentes, N. (2014). Hispanics in metropolitan America: New realities and old debates. Annual Review of Sociology, 40, 499.
Timperio, A., Crawford, D., Ball, K., & Salmon, J. (2017). Typologies of neighbourhood environments and children’s physical activity, sedentary time and television viewing. Health & Place, 43, 121–127.
Timperio, A., Crawford, D., Telford, A., & Salmon, J. (2004). Perceptions about the local neighborhood and walking and cycling among children. Preventive Medicine, 38, 39–47.
U.S. Census. (2015). 2011–2015 American Community Survey 5-year estimates. U.S. Census Bureau: Washington, DC.
U.S. Surgeon General. (1999). Physical activity and health: A report of the Surgeon General. Atlanta. GA: Centers for Disease Control and Prevention.
Varsanyi, M. (2010). Taking local control: Immigration policy activism in U.S. cities and states. Redwood City, CA: Stanford University Press.
Vaughan, K. B., Kaczynski, A. T., Wilhelm Stanis, S. A., Besenyi, G. M., Bergstrom, R., & Heinrich, K. M. (2013). Exploring the distribution of park availability, features, and quality across Kansas City, Missouri by income and race/ethnicity: An environmental justice investigation. Annals of Behavioral Medicine, 45(Suppl 1), S28–S38.
Wolch, J., Wilson, J. P., & Fehrenbach, J. (2005). Parks and park funding in Los Angeles: An equity-mapping analysis. Urban Geography, 26, 4–35.
Wolch, J., Byrne, J., & Newell, J. (2014). Urban green space, public health, and environmental justice: The challenge of making cities ‘just green enough’. Landscape and Urban Planning, 125, 234–244.
Wood, L., Hooper, P., Foster, S., & Bull, F. (2017). Public green spaces and positive mental health—Investigating the relationship between access, quantity and types of parks and mental wellbeing. Health & Place, 48, 63–71.
Woolf, S. H., & Aron, L. (2013). U.S. health in international perspective: Shorter lives, poorer health. Washington, DC: The National Academies Press.
Zenk, S. N., Schulz, A. J., Odoms-Young, A. M., & Lockett, M. (2009). Interdisciplinary, participatory research on urban food environments and dietary behavior. In N. Freudenberg, S. Klitzman, & S. Saegert (Eds.), Urban health and society: Interdisciplinary approaches to research and practice (pp. 45–61). San Francico: Jossey-Bass.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Lara-Valencia, F., García-Pérez, H. (2020). Three Ecologies of the Urban Environment and the Health of Latinx Communities. In: Martínez, A., Rhodes, S. (eds) New and Emerging Issues in Latinx Health. Springer, Cham. https://doi.org/10.1007/978-3-030-24043-1_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-24043-1_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-24042-4
Online ISBN: 978-3-030-24043-1
eBook Packages: MedicineMedicine (R0)