
Abstract
Rotator cuff tears are common injuries that occur in athletes as well as the general population. An overall understanding of the biomechanics, aetiology, treatment options, and outcomes can greatly assist the healthcare provider in optimising treatment for patients.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Shoulder injury
- Internal impingement
- Posterosuperior impingement
- Overhead activity
- Overhead athlete
- Throwing athlete
- Rotator cuff tear
- Rotator cuff repair
-
Rotator cuff muscles stabilise the glenohumeral joint and initiate glenohumeral motion in a way that allows deltoid and pectoralis muscles to be most effective.
-
Rotator cuff injuries occur in athletes and must be appreciated to help these individuals return to optimum function.
-
Glenohumeral internal rotation deficit is a common finding in throwers and results from tightness of the posterior IGHL complex and posteroinferior capsule that leads to a posterosuperior shift of the point of glenohumeral articulation and centre of rotation.
-
Most partial thickness rotator cuff tears can and should be managed nonoperatively. When surgical treatment is needed, debridement is often the preferred treatment, particularly in throwing athletes. Full-thickness rotator cuff tears usually require surgical repair.
5.1 Biomechanics of the Rotator Cuff
The muscles of the rotator cuff play a crucial role in shoulder motion. Coordinated activities of the four muscles serve to maintain position of the humeral head in the glenoid cavity when the deltoid contracts. With the initiation of voluntary movement, electromyographic activity of the deltoid and pectoralis major muscle occurs after the activation of the rotator cuff muscles, supporting the notion that the rotator cuff muscles actively prepare the glenohumeral joint for movement [1]. Deltoid contraction leading to abduction generates shear forces that the rotator cuff muscles counteract. Resting tension of the rotator cuff is also an important component of glenohumeral stability.
In order for the rotator cuff to stabilise the glenohumeral joint, there must be a balance of forces between the coronal and axial plane as described by Burkhart et al. [2]. The native anatomic position of the four rotator cuff tendons allows for these two force planes to compress the humeral head within the glenoid fossa. The coronal force plane is between the deltoid and the inferior rotator cuff whereas the axial plane exists between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. Rotator cuff tears can disrupt these force couples, resulting in the inability to maintain the fulcrum for motion at the glenohumeral joint leading to severe limitations in active range of motion.
Tears of the rotator cuff require greater forces to be exerted by both the deltoid as well as the muscles of the rotator cuff itself to achieve stable abduction [1]. Forces required increase with tear size and can contribute to the anterior or posterior extension of a tear. The part of the tendon that is torn cannot participate in load sharing of the exerted forces, therefore, increasing the tensile load on the remaining fibres. This can readily lead to tear propagation. Large retracted tears have been implicated to cause suprascapular nerve compression and may contribute to the progression of atrophy and fatty infiltration of the supraspinatus. Repair of these tears may release tension on the suprascapular nerve allowing for recovery of the nerve and improvement in function [3, 4].
5.2 Aetiology and Relevant Pathology
A common cause of rotator cuff tears as well as other shoulder pathology in athletes is impingement. Impingement of the shoulder can be classified into two categories, external and internal impingement. External impingement is a relatively uncommon condition in young athletes. It is synonymous with subacromial impingement and is a result of narrowing of the subacromial space. Internal impingement often occurs in young athletes with overhead activity, especially in the dominant arm of throwing athletes (Javelin, Tennis, Volleyball, Baseball, American Football, Rugby) [5, 6]. However, internal impingement can also occur and be symptomatic in patients who do not participate in sports.
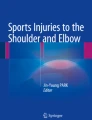
Often referred to as Thrower’s shoulder, internal impingement occurs during the cocking phase of throwing (Fig. 5.1). Cocking consists of a combination of abduction, external rotation, and extension, leading to compression and impingement of the articular side of the rotator cuff between the humeral head and the posterior superior labrum [6]. These biomechanics are believed to serve as a physiologic restraint to prevent excessive external rotation, however, with repetitive overhead activity it may result in the development of pathology.

The six phases of the throwing motion. Phase 1 is the wind-up phase. Phase 2 is the early cocking phase, ending with planting of the striding foot. Phase 3 is the late cocking phase, in which the arm reaches maximum external rotation. In Phase 4, the ball is accelerated until Phase 5 starts with release of the ball and deceleration of the arm. Phase 6, the follow-through, rebalances the body until the motion stops (from Braun et al. [7])
Posterior superior glenoid impingement by repetitive overhead activity can lead to rotator cuff injury in athletes as the posterosuperior labrum and rotator cuff can be compressed between the greater tuberosity and the glenoid rim (Fig. 5.2). Such glenoid impingement may injure the superior labrum and superior glenoid bone, rotator cuff tendons, the greater tuberosity, the inferior glenohumeral ligament (IGHL) [7, 9, 10] and inferior labrum, or any combination of these [11] “Kissing lesions” of both the rotator cuff and the labrum are not uncommon.

Illustration of the pathomechanism behind the development of symptomatic internal impingement. Jobe and Walch et al. postulated that the posterosuperior cuff and labrum can become entrapped between the greater tuberosity and the posterosuperior glenoid resulting in partial-thickness articular-sided rotator cuff tears and posterosuperior labral tearing. Arrows indicate the resulting pathologic lesions associated with symptomatic internal impingement (from Spiegl et al. [8])
5.3 Diagnosis
5.3.1 Physical Examination
Patients usually present with pain in overhead activities and throwing. It is common for throwing athletes to present with shoulder pain without a specific acute injury. Clinical examination can show localised posterior shoulder pain on full external rotation and 90° abduction, positive impingement signs and signs of rotator cuff tears [6]. In the case of rotator cuff tears, weakness especially during abduction and pain with resistance are very common findings. Physical examination may also reveal anterior glenohumeral laxity without true instability. The Jobe relocation test can also be used to determine if a patient has symptomatic internal impingement [11].
Several physical examination manoeuvres can be used to recreate shoulder pain by compacting the muscles of the rotator cuff between the bony structures of the humeral head and the acromion or coracoid. These include Neer’s impingement sign and Hawkins’ impingement sign. However, a positive sign of pain may be due to other causes such as acromioclavicular or biceps pathology. If the labrum has sustained relevant damage, glenohumeral instability may occur. Sometimes a painful clicking or clunking can be provoked on examination.
Posterior capsular tightness as detected by glenohumeral internal rotational deficit (GIRD) may also be present. GIRD has been suggested by Burkhart et al. in 2003 as a clinical symptom and starting point of pathological changes of the shoulder [9]. The posterior IGHL complex and posteroinferior capsule undergo scarring, provoking a posterosuperior shift of the point of glenohumeral articulation and centre of rotation [9] (Fig. 5.3). With chronic GIRD, it is not uncommon for overhead athletes to get articular sided rotator cuff pathology.

The arc of motion of the throwing shoulder is shifted posteriorly, with increased external rotation and decreased internal rotation of the abducted shoulder (from Braun et al. [7])
The active compression test, which is performed with the arm in 90° of forward flexion, starting in external rotation without pain and causing pain with internal rotation of the arm, is relatively specific in diagnosing labral tears [12]. Kibler’s test, as well as many other physical exam manoeuvres can also be used to help in establishing a diagnosis.
5.3.2 Imaging
Ultrasound can detect rotator cuff tears, but strongly depends on the skills of the investigator and may miss subtle partial thickness tears. Magnetic resonance imaging (MRI) or MR arthrograms with intraarticular injection of contrast agent are often used to establish a diagnosis. Partial thickness rotator cuff tears, full thickness rotator cuff tears, SLAP (superior labrum anterior to posterior) lesions and lesions of the posterosuperior labrum can be detected by MR-arthrogram [6].
Standard MRI with the conventional 3 sequences (coronal, sagittal, and axial) is performed with the arm in adduction. Full thickness rotator cuff tears can readily be detected. In this position, subtle labral tears as well as subtle partial thickness rotator cuff tears lying apposed to the intact tendon fibres may be missed [13].
To detect such partial thickness flap tears, the ABER view (Abduction External Rotation) for MRI of the shoulder has been introduced. This position tensions the anteroinferior glenohumeral ligament and labrum, while releasing tension on the cuff tendons compared with the normal coronal view with the arm in adduction.
Most conventional bore-style MRI scanners do not allow for the shoulder to be placed in the clinical position of apprehension, which is 90° of abduction and 90° of external rotation. This necessitates a modified position with the arm abducted and the hand tucked underneath the patient’s head. Both the execution and the interpretation of ABER views can be challenging for technicians and physicians unfamiliar with its use [13].
While MRI is very useful in evaluating shoulder pathology, it can be misleading in throwing athletes as several studies have demonstrated significant amounts of shoulder pathology in asymptomatic athletes [14,15,16,17,18]. The incidence of full thickness tears was 0% in these studies, however, the partial thickness tears were detected in 20–86% of patients. Therefore, when evaluating a throwing athlete for shoulder pain, the physician must perform a thorough history and exam as the pain the patient may be experiencing may not be a result of rotator cuff pathology [19]. Furthermore, SLAP tears are a common finding in throwing athletes, which may not require immediate intervention [19].
5.4 Management Principles
5.4.1 Non-surgical Treatment
The primary goal of intervention is to restore painless function to the affected shoulder. Conservative treatment should be employed for all patients prior to seeking surgical intervention, especially for throwing athletes. The first line of therapy consists of activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), and rehabilitation. This is an attempt to decrease inflammation and improve function.
Physical therapy with a stretching and strengthening programme, as well as sports and job specific training are performed. Physical therapy is sport- and/or job-specific and focuses on restoring normal glenohumeral kinematics. Exercises in the scapular plane with strengthening of the scapular stabilisers such as the serratus anterior and trapezius muscle, strengthening of the internal rotators of the shoulder, stretching of the posterior capsule, and isokinetic progressive endurance training should all be included (Fig. 5.4) [8].

For the sleeper stretch, the individual lies on the involved side with the shoulder in approximately 90° of forward elevation. The other arm is used to internally rotate the involved shoulder until a stretch is achieved on the posterior aspect of the shoulder (from Braun et al. [7])
Corticosteroid injections into the glenohumeral joint may provide both pain relief and serve as diagnostic tool by serial injections to differentiate glenohumeral joint pain from acromioclavicular joint pain and subacromial pain.
A recent randomised controlled study investigated the differences in outcomes at 5 years following physiotherapy only or operative treatment for rotator cuff tears not exceeding 3 cm [20]. The investigators found that primary repair of small- and medium-sized rotator cuff tears were associated with better outcomes than the tears treated with physiotherapy, however, they concluded they may be below clinical importance. Importantly, 37% of tears treated with physiotherapy only, progressed by greater than 5 mm over 5 years. Given that these tears are now larger, surgical treatment is more challenging and outcomes less predictable [21,22,23,24,25].
5.4.2 Surgical Treatment
In case of failed non-operative treatment or proven full thickness rotator cuff tearing, surgery is indicated. Rotator cuff tears and SLAP lesions usually do not heal spontaneously [26]. Historically, open repairs of the rotator cuff and labrum were effective. However, with the improvement in arthroscopic equipment as well as surgical skill most rotator cuff tears and lesions of the labrum can readily be repaired arthroscopically [25, 27,28,29].
Bilateral examination under anaesthesia is performed first to assess range of motion and stability of the joint. Diagnostic arthroscopy enables visualisation of intraarticular pathologies throughout dynamic positioning of the shoulder. These pathologies include SLAP lesions, partial thickness tears of the undersurface of the rotator cuff, as well as full thickness tears. If scuffing of the articular side of the rotator cuff is noted on diagnostic arthroscopy, the physician should be aware that this can be a normal physiologic phenomenon in baseball players. This should, therefore, only be addressed if the clinical symptoms are concordant [15]. Posterior labral repair is rarely indicated in overhead athletes unless there is evidence of posterior glenohumeral instability.
The surgical management of partial thickness tears varies depending on the overhead demands of the patient (Fig. 5.5). Many surgeons advocate for simple debridement when the tear involves less than 50% of the thickness of the tendon while tears involving greater than 50% of the thickness should undergo repair. However, in the throwing athlete, outcomes of repair are less favourable [19] and, therefore, the senior surgeon (PJM) prefers to manage tears involving up to 75% thickness with debridement.

(a) A high grade partial thickness articular sided tear of the supraspinatus tendon is visualized from the posterior portal. (b) View after repair of the bursal side of the rotator cuff from the lateral portal. (c) View after repair of the articular side of the rotator cuff from the posterior portal
Full-thickness rotator cuff tears are repaired in a stepwise manner that both reduces the torn rotator cuff tendon to its native footprint but also creates a favourable environment for healing. In progression, the rotator cuff footprint on the greater tuberosity is first decorticated to create a bleeding bony surface for healing [28,29,30]. Next, the tendon is mobilised to remove bursal adhesions and scarring that could prevent anatomic reduction. Third, suture anchors are placed into the humerus and sequentially passed through the rotator cuff tendon. These anchors can be placed in a variety of configurations (single-row or double-row) depending on the biomechanical stability desired. Lastly, the sutures are secured to the tendon in either a knotless or knotted fashion while confirming anatomic reduction of the tendon to its footprint.
A level I meta-analysis conducted by Millett et al. [31] investigated the differences in clinical outcomes between rotator cuff tears that were repaired with a single row versus a double row technique. Although no statistically significant differences were found in clinical outcomes between the repair techniques, single row repairs were associated with higher re-tear rate.
In case of anterior subluxation and a distended anterior joint capsule, anterior or antero-inferior plication can be performed. The posterior capsule is usually released. Range of motion and stability are re-checked after the capsular procedures.
Derotational humeral osteotomy with a myorraphy of the subscapularis muscle is an option to be considered in athletes after failure of all other means of treatment, including arthroscopic management [32].
5.5 Rehabilitation Following Surgery
Rehabilitation after surgery is an important aspect of treatment. Physical therapy is divided into four phases. Phase I focuses on establishing passive range of motion to reduce the risk of postoperative stiffness while focusing on protecting the integrity of the rotator cuff repair. Once passive motion has been established, typically about 4 weeks following surgery, the patient progresses to phase II which focuses on active assisted range of motion and active range of motion. At approximately 8 weeks postoperatively, phase III is begun which focuses on strengthening the rotator cuff followed by phase IV at approximately 12–16 weeks postoperatively at which advanced strengthening is begun. When phase IV is completed a gradual progressive return to sport rehabilitation plan is initiated prior to allowing the patient to return to competitive sporting activities.
5.6 Clinical Outcomes
5.6.1 Partial Thickness Tears
The management of partial thickness rotator cuff tears remains controversial. Studies have reported excellent overall outcomes after arthroscopic treatment of partial thickness rotator cuff tears, however, the ideal management remains an area of debate [31, 33,34,35,36,37,38,39,40].
Millett et al. [31] investigated the outcomes of treatment of partial thickness tears and found improvements in ASES, and SANE scores—79% of athletes in the cohort were able to compete in sports at or near preinjury levels of intensity. In addition, patients who underwent a concomitant acromioplasty had a significantly better SANE score (p = 0.043). However, other investigators have advised to avoid anterior acromioplasty in patients with impingement due to unfavourable outcomes [41, 42]. Sonnery-Cottet et al. [43] investigated the outcomes of 28 tennis players with symptomatic posterosuperior glenoid impingement who underwent arthroscopic debridement for partial articular sided tendon avulsions. Despite a high level of satisfaction (82%) and high level of return to sport (79%), 82% of the players who returned to sport reported continued pain while competing.
In throwing athletes, the rate of return to sport at the same level following debridement of partial thickness rotator cuff tears has ranged from 16% to 76% [44,45,46,47]. Reynolds et al. [46] investigated outcomes of debridement for small partial thickness rotator cuff tears in elite pitchers. Sixty-seven out of eighty-two (82%) returned to sport, however, only 37/67 (55%) returned to sport at the same or higher level. Payne et al. investigated debridement of partial thickness tears in young athletes and found that for overhead athletes, they had significant pain relief from the surgery but only 45% returned to sport. Ide et al. [48] investigated outcomes or repair of partial thickness rotator cuff tears to the bone and found that 2/6 throwing athletes returned to the same level of sport. These studies highlighting return to sport levels are important and can be used in counselling patients and managing preoperative expectations.
5.6.2 Full Thickness Tears
Reported outcomes following surgical treatment of full thickness rotator cuff tears have been favourable across a wide spectrum of activity levels and age ranges [25, 30, 31, 40, 49,50,51]. In fact, a recent study conducted by Bhatia et al. [49] investigated the outcomes of arthroscopic repair of full thickness rotator cuff tears in recreational athletes aged 70 years or older. At a mean follow-up of 3.6 years, there were significant improvements in all subjective outcomes scores and no patients required revision rotator cuff repairs. The American Shoulder and Elbow Score (ASES) was comparable to age-matched individuals with normal shoulder function. In addition, 77% of patients were able to return to their recreational sport at a similar level of intensity to pre injury levels.
Full thickness tears in elite overhead athletes are uncommon, however they can be a career-threatening injury [52, 53]. Mazoue and Andrews [52] investigated outcomes in 12 professional baseball pitchers who underwent a mini-open repair on their dominant arm. Only 1 player (8%) was able to return to a high level of competition. Van Kleunen et al. [53] investigated outcomes following repair of combined SLAP and infraspinatus tears and found that 17% of patients with full thickness tears returned to the same sporting level. Given the low rates of return to sport following full thickness rotator cuff tears, it is extremely important to exhaust all conservative treatment options prior to engaging in surgical intervention.
5.7 Conclusion
Rotator cuff tears are a common cause of shoulder pain and discomfort in the general population and athletes. An understanding of the biomechanics, aetiology, diagnostic testing, and outcomes can help the healthcare provider optimally treat patients and return them to a high level of function and activity. Athletes often suffer from partial thickness rotator cuff tears, however, outcomes are favourable following treatment. Full thickness tears are uncommon but career threatening in elite overhead athletes.
References
Hansen ML, Otis JC, Johnson JS, Cordasco FA, Craig EV, Warren RF. Biomechanics of massive rotator cuff tears: implications for treatment. J Bone Joint Surg Am. 2008;90:316–25.
Burkhart SS, Nottage WM, Ogilvie-Harris DJ, Kohn HS, Pachelli A. Partial repair of irreparable rotator cuff tears. Arthroscopy. 1994;10:363–70.
Costouros JG, Porramatikul M, Lie DT, Warner JJ. Reversal of suprascapular neuropathy following repair of massive supraspinatus and infraspinatus rotator cuff tears. Arthroscopy. 2007;23(11):1152–61.
Mallon WJ, Wilson RJ, Basamania CJ. The association of suprascapular neuropathy with massive rotator cuff tears: a preliminary report. J Shoulder Elb Surg. 2006;15(4):395–8.
Paley KJ, Jobe FW, Pink MM, Kvitne RS, ElAttrache NS. Arthroscopic findings in the overhand throwing athlete: evidence for posterior internal impingement of the rotator cuff. Arthroscopy. 2000;16(1):35–40.
Walch G, Boileau P, Noel E, Donell ST. Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elb Surg. 1992;1(5):238–45.
Braun S, Kokmeyer D, Millett PJ. Shoulder injuries in the throwing athlete. J Bone Joint Surg Am. 2009;91:966–78.
Spiegl UJ, Warth RJ, Millett PJ. Symptomatic internal impingement of the shoulder in overhead athletes. Sports Med Arthrosc. 2014;22(2):120–9.
Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology part I: pathoanatomy and biomechanics. Arthroscopy. 2003;19(4):404–20.
Tétreault P, Krueger A, Zurakowski D, Gerber C. Glenoid version and rotator cuff tears. J Orthop Res. 2004;22(1):202–7.
Jobe CM. Posterior superior glenoid impingement: expanded spectrum. Arthroscopy. 1995;11(5):530–6.
O’Brien SJ, Pagnani MJ, Fealy S, McGlynn SR, Wilson JB. The active compression test: a new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med. 1998;25(6):610–3.
Iyengar JJ, Burnett KR, Nottage WM, Harwin SF. The abduction external rotation (ABER) view for MRI of the shoulder. Orthopedics. 2010;33(8):562–5.
Connor PM, Banks DM, Tyson AB, Coumas JS, D’Alessandro DF. Magnetic resonance imaging of the asymptomatic shoulder of overhead athletes: a 5-year follow-up study. Am J Sports Med. 2003;31(5):724–7.
Halbrecht JL, Tirman P, Atkin D. Internal impingement of the shoulder: comparison of findings between the throwing and nonthrowing shoulders of college baseball players. Arthroscopy. 1999;15(3):253–8.
Jerosch J, Castro WH, Drescher H, Assheuer J. Magnetic resonance morphologic changes in shoulder joints of world class water polo players. Sportverletz Sportschaden. 1992;7(3):109–14.
Jost B, Zumstein M, Pfirrmann CW, Zanetti M, Gerber C. MRI findings in throwing shoulders: abnormalities in professional handball players. Clin Orthop Relat Res. 2005;434:130–7.
Miniaci A, Mascia AT, Salonen DC, Becker EJ. Magnetic resonance imaging of the shoulder in asymptomatic professional baseball pitchers. Am J Sports Med. 2002;30(1):66–73.
Andrews JR, Wilcox JR. Decision making in the throwing athlete. Sports Med Arthrosc Rev. 2014;22(2):130–6.
Moosmayer S, Lund G, Seljom US, Haldorsen B, Svege IC, Henning T, Pripp AH, Smith HJ. Tendon repair compared with physiotherapy in the treatment of rotator cuff tears: a randomized controlled study in 103 cases with a five year follow-up. J Bone Joint Surg Am. 2014;96(18):1504–14.
Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K. The outcome and repair integrity of complete arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86A:219–24.
Gerber C, Fuchs B, Hodler J. The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am. 2000;82:505–15.
Holtby R, Razmjou H. Relationship between clinical and surgical findings and reparability of large and massive rotator cuff tears: a longitudinal study. BMC Musculoskelet Disord. 2014;15:180.
Iagulli ND, Field LD, Hobgood R, Ramsey JR, Savoie FH III. Comparison of partial versus complete arthroscopic repair of massive rotator cuff tears. Am J Sports Med. 2012;40:1022–6.
Millett PJ, Warth RJ. Posterosuperior rotator cuff tears: classification, pattern recognition, and treatment. J Am Acad Orthop Surg. 2014;30:778–80.
Conway JE. Arthroscopic repair of partial-thickness rotator cuff tears and SLAP lesions in professional baseball players. Orthop Clin North Am. 2001;32(3):443–56.
Gaskill TR, Braun S, Millett PJ. Multimedia article. The rotator interval: pathology and management. Arthroscopy. 2011;27(4):556–67.
Vaishnav S, Millett PJ. Arthroscopic rotator cuff repair: scientific rationale, surgical technique, and early clinical and functional results of a knotless self-reinforcing double-row rotator cuff repair system. J Shoulder Elb Surg. 2010;19(2 Suppl):83–90.
Warth RJ, Greenspoon JA, Bhatia S, Millett PJ. Arthroscopic double-row rotator cuff repair using a knotless, interconnected technique. Oper Tech Orthop. 2015;25(1):1–6.
Ames JB, Horan MP, Van der Meijden OA, Leake MJ, Millett PJ. Association between acromial index and outcomes following arthroscopic repair of full-thickness rotator cuff tears. J Bone Joint Surg Am. 2012;94(20):1862–9.
Millett PJ, Warth RJ, Dornan GJ, Lee JT, Speigl UJ. Clinical and structural outcomes after arthroscopic single-row versus double-row rotator cuff repair: a systematic review and meta-analysis of level I randomized clinical trials. J Shoulder Elb Surg. 2014;23(4):586–97.
Riand N, Levigne C, Renaud E, Walch G. Results of derotational humeral osteotomy in posterosuperior glenoid impingement. Am J Sports Med. 1998;26(3):453–9.
Chung SW, Kim JY, Yoon JP, Lyu SH, Rhee SM, Oh SB. Arthroscopic repair of partial-thickness and small full-thickness rotator cuff tears: tendon quality as a prognostic factor for repair integrity. Am J Sports Med. 2014;43(3):588–96.
Duralde XA, McClelland WB Jr. The clinical results of arthroscopic transtendinous repair of grade III partial articular-sided supraspinatus tendon tears. Arthroscopy. 2012;28(2):160–8.
Eid AS, Dwyer AJ, Chambler AF. Mid-term results of arthroscopic subacromial decompression in patients with or without partial thickness rotator cuff tears. Int J Shoulder Surg. 2012;6(3):86–9.
Franceschi F, Papalia R, Del Buono A, Vasta S, Costa V, Maffulli N, Denaro V. Articular-sided rotator cuff tears: which is the best repair? A three-year prospective randomised controlled trial. Int Orthop. 2013;37(8):1487–93.
Kim KC, Shin HD, Cha SM, Park JY. Clinical outcomes after arthroscopic trans-tendon suture-bridge technique in partial-thickness articular-side rotator cuff tear. Knee Surg Sports Traumatol Arthrosc. 2013;21(5):1183–8.
Kim KC, Shin HD, Cha SM, Park JY. Repair integrity and functional outcome after arthroscopic conversion to a full-thickness rotator cuff tear: articular- versus bursal-side partial tears. Am J Sports Med. 2014;42(2):451–6.
Peters KS, McCallum S, Briggs L, Murrell GA. A comparison of outcomes after arthroscopic repair of partial versus small or medium-sized full-thickness rotator cuff tears. J Bone Joint Surg Am. 2012;94(12):1078–85.
Sonnery-Cottet B, Edwards TB, Noel E, Walch G. Rotator cuff tears in middle-aged tennis players: results of surgical treatment. Am J Sports Med. 2002;30(4):558–64.
Mithofer K, Fealey S, Altchek DW. Arthroscopic treatment of internal impingement of the shoulder. Tech Should Elbow Surg. 2004;5:66–75.
Tibone JE, Jobe FW, Kerlan RK, Carter VS, Shields CL, Lombardo SJ, Yocum LA. Shoulder impingement syndrome in athletes treated by an anterior acromioplasty. Clin Orthop Relat Res. 1985;198:134–40.
Sonnery-Cottet B, Edwards TB, Noel E, Walch G. Results of arthroscopic treatment of posterosuperior glenoid impingement in tennis players. Am J Sports Med. 2002;30(2):227–32.
Andrews JR, Broussard TS, Carson WG. Arthroscopy of the shoulder in the management of partial tears of the rotator cuff: a preliminary report. Arthroscopy. 1985;1(2):117–22.
Payne LZ, Altchek DW, Craig EV, Warren RF. Arthroscopic treatment of partial rotator cuff tears in young athletes. A preliminary report. Am J Sports Med. 1997;25(3):299–305.
Reynolds SB, Dugas JR, Cain EL, McMichael CS, Andrews JR. Debridement of small partial-thickness rotatorcuff tears in elite overhead throwers. Clin Orthop Relat Res. 2008;466(3):614–21.
Riand N, Boulahia A, Walch G. Posterosuperior impingement of the shoulder in the athlete: results of arthroscopic debridement in 75 patients. Rev Chir Orthop Reparatrice Appar Mot. 2002;88(1):19–27.
Ide J, Maeda S, Takagi K. Arthroscopic transtendon repair of partial-thickness articular-sided tears of the rotator cuff: anatomical and clinical study. Am J Sports Med. 2005;33(11):1672–9.
Bhatia S, Greenspoon JA, Horan MP, Warth RJ, Millett PJ. Two-year outcomes following arthroscopic rotator cuff repair in recreational athletes over 70 years of age. Am J Sports Med. 2015;43(7):1737–42.
MacKenchia MA, Chahal J, Wasserstein D, Thoeoropoulos JS, Henry P, Dwyer T. Repair of full-thickness rotator cuff tears in patients aged younger than 55 years. Arthroscopy. 2014;30(10):1366–71.
Warth RJ, Dornan GJ, James EW, Horan MP, Millett PJ. Clinical and structural outcomes after arthroscopic repair of full-thickness rotator cuff tears with and without platelet-rich product supplementation: a meta-analysis and meta-regression. Arthroscopy. 2015;31(2):306–20.
Mazoue CG, Andrews JR. Repair of full-thickness tears in professional baseball players. Am J Sports Med. 2006;34(2):182–9.
Van Kleunen JP, Tucker SA, Field LD, Savoie FH. Return to high level throwing after combination infraspinatus, SLAP repair, and release of glenohumeral internal rotation deficit. Am J Sports Med. 2012;40(11):2536–41.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Q&A
Q&A
-
(1)
What is Glenohumeral Internal Rotation Deficit?
Tightness of the posterior IGHL complex and posteroinferior capsule that is commonly seen in throwers
-
(2)
Which type of impingement is relatively uncommon in young athletes?
External impingement
-
(3)
In rehabilitation of rotator cuff repairs, what type of motion is typically done first during rehab?
Passive range of motion
-
(4)
The Abduction and External Rotation view (ABER view) is especially helpful during MRI to look for the presence of what kind of pathology?
Partial thickness flap tears of the rotator cuff
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Greenspoon, J.A., Petri, M., Bhatia, S., Millett, P.J. (2020). Rotator Cuff Disorders in Athletes. In: Funk, L., Walton, M., Watts, A., Hayton, M., Ng, C. (eds) Sports Injuries of the Shoulder. Springer, Cham. https://doi.org/10.1007/978-3-030-23029-6_5
Download citation
DOI: https://doi.org/10.1007/978-3-030-23029-6_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-23028-9
Online ISBN: 978-3-030-23029-6
eBook Packages: MedicineMedicine (R0)