
Abstract
Fluoroscopy allows for the diagnosis of both functional and anatomic pathology. This chapter focuses on the fluoroscopic evaluation of the upper gastrointestinal tract and small bowel.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Objectives:-
1.
Identify normal anatomy on a “barium swallow” and “upper GI” series.
-
2.
Be able to differentiate mucosal versus extramucosal lesions based on radiographic findings.
-
3.
Describe the radiographic features of malignant esophageal lesions.
-
4.
Know the common locations for esophageal diverticula and their radiographic appearance.
-
5.
Understand the main advantages and disadvantages of the various means of small bowel examination.
Fluoroscopy
GI studies are observed fluoroscopically in real-time imaging to evaluate peristalsis and the rate of flow of contrast. Exposures and limited video captures of key anatomic regions or focal abnormalities are also obtained. Static images covering a large region of the GI tract are acquired at the end of the study for the purpose of giving a geographic perspective of the contrast distribution throughout the GI tract.
Normal Esophageal Motility
Swallowed contrast is propelled by peristaltic waves, which are visible as smooth, segmental, and progressive narrowings of the esophagus. The normal peristaltic wave with swallowing is called the primary peristaltic wave. A secondary wave may occur if the patient swallows quickly after the primary swallow. Figure 30.1 demonstrates a single image from a normal fluoroscopic exam of the esophagus.

- Normal contrast esophagramContrast upper gastrointestinal (UGI) study performed with barium demonstrating a normal esophageal appearance
Abnormal Esophageal Motility
Sometimes abnormalities of esophageal motility may manifest as tertiary contractions which are seen as multiple small disorganized and transient indentations of the contrast column within the esophagus. These are generally related to abnormalities of the neurologic plexus responsible for propagation of the peristaltic wave. They are commonly seen in older individuals as the plexus and motor function degenerates with age, but may also be observed in those with underlying gastrointestinal dysmotility or neurological disorders. Fluoroscopic evaluations should be correlated with any available manometric examinations.
When the neurologic plexus in the distal esophagus degenerates, spasm without relaxation of the lower esophageal sphincter may occur, producing a condition termed achalasia (Fig. 30.2). This results in distension of the proximal esophagus with collections of ingested food and secretions leading to an increased risk of aspiration pneumonia. An increasing number of fluoroscopic exams are now being performed on patients who have undergone peroral endoscopic myotomy (POEM) in which the circular muscles of the esophagus are divided endoscopically for the treatment of achalasia.

- AchalasiaMalfunction of the neurologic plexus leads to spasm of the lower esophageal sphincter, resulting in a markedly distended esophagus and the classic “birds beak” (arrow) narrowing at the level of the lower esophageal sphincter
Esophageal Carcinoma
Esophageal carcinomata create areas of fixed narrowing, often with mucosal ulceration and overhanging edges that result in “shouldering” of the barium column at the edges of the fixed narrowing. Shouldering of contrast around a narrowing suggests malignancy as compared to smooth margins that occur more frequently about benign lesions as depicted in Fig. 30.3.

- Contrast esophagramOn contrast swallow studies, benign (left) and malignant (right) lesions have a different appearance. Note the gradual narrowing with smooth margins of the benign lesion versus the overhanging edges and abrupt appearance of the malignant lesion
Esophageal carcinoma occurs most commonly in the mid to lower esophagus (Fig. 30.4). As it is difficult to definitively distinguish a benign esophageal stricture (i.e., caused by gastric reflux) from a carcinoma on fluoroscopy, endoscopic evaluation with biopsy is often necessary.

- Esophageal carcinomaNote the irregularity and overhanging edges (arrows) resulting in abrupt shouldering of the contrast column above and below the narrowing
Esophageal Diverticula
Diverticula of the esophagus take two forms: traction diverticula and pulsion diverticula. Traction diverticula most commonly arise in the region of the carina. They result from retraction of the inflamed subcarinal lymph nodes as they pull on the esophageal mucosa via fibrous adhesions. Pulsion diverticula occur when peristaltic waves exert a positive pressure within the esophageal lumen. Any weakness in the esophageal wall may lead to a “ballooning out” of the mucosa. A common location for esophageal wall weakness is in the upper esophagus posteriorly where the constrictor muscles fail to completely cover the esophageal wall. This region is known as Killian’s dehiscence. The pulsion diverticulum formed in this area is termed a Zenker’s diverticulum and may be present as a mass in the upper neck. Another common location for pulsion diverticula is just above the lower esophageal sphincter. These diverticula are called epiphrenic diverticula and can be associated with achalasia.
Double- and Single-Contrast Upper GI Studies
Standard upper GI studies utilize either a single- or double-contrast evaluation of the esophagus, stomach, and duodenal bulb. In a double-contrast study, barium and air are the two contrast agents. Within the stomach, the barium coats the gastric mucosa, and the air distension allows the mucosal folds of the stomach to be clearly evident (Fig. 30.5).

- Double-contrast gastric studyNote the detail of the gastric and duodenal mucosa
In a single-contrast upper GI series, barium is the only contrast agent. The stomach is nearly filled with barium, and the mucosal detail is not as evident. Single-contrast studies are faster to perform and result in less radiation exposure; however, mucosal information is expectedly more limited.
Filling of ulcer craters with barium produces small collections of contrast within the gastric wall. Gastric folds may radiate toward the ulcer as a result of inflammation. Ulcers may be malignant or benign, and endoscopic evaluation is often required for differentiation. Adenocarcinoma is the most common gastric malignancy and can present as an irregular solitary filling defect or as a diffuse infiltrative lesion that rigidly narrows the gastric body and antrum in a pattern termed “linitis plastica.”
After evaluation of the stomach, static images are obtained of the duodenal bulb and proximal “C” loop of the duodenum as it curves around the head of the pancreas. The duodenal bulb and post-bulbar portion of the duodenum are common places for ulceration and diverticula formation. The duodenum ends anatomically at the ligament of Treitz which should be at the same craniocaudal level as the duodenal bulb and lies to the left of the midline.
Small Bowel Follow-Through
A single-contrast study of the contrast column may be followed through the small bowel as it passes distally through the GI tract, termed “a small bowel follow-through” (Fig. 30.6). This will reveal gross abnormalities such as mucosal masses, strictures, and mass effect displacing the small bowel loops, in addition to serving as a rough indicator of overall small bowel transit time and motility. The small bowel follow-through terminates when contrast is seen within the cecum of the colon, having passed through the terminal ileum and the ileocecal valve.

- Small bowel follow-throughDetail of the mucosal lining is visible as barium passes through the small bowel
Conventional Enteroclysis
A double-contrast study of the small bowel, termed an “enteroclysis,” may be performed for the purpose of further elucidating small bowel anatomy. By placing an enteric tube distal to the ligament of Treitz, occluding the jejunal lumen with a balloon and slowly injecting soluble barium and methylcellulose as a “solid column,” a double-contrast effect is achieved. Multiple single exposure images of the small bowel are obtained with fluoroscopy. The study is concluded once contrast reaches the cecum.
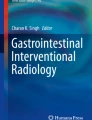
Small bowel malignancies may be either primary or metastatic and usually will appear as focal narrowing or strictures of the small bowel and/or nodular filling defects. Given the dynamic nature of the exam, this study can be useful for detecting low-grade small bowel obstruction secondary to Crohn’s disease and postoperative adhesions (Fig. 30.7). Active Crohn’s disease may also be detected with this type of examination, although the diagnostic modality of choice for evaluation of Crohn’s disease is CT or MR enterography.

- Conventional versus CT enteroclysis(a) Conventional enteroclysis demonstrates a focal area of narrowing in the distal ileum (arrow). (b) Coronal image from a CT enteroclysis of the same patient demonstrates the focal area of narrowing in the distal ileum in the same location as the narrowing seen on conventional enteroclysis (arrow). CT enteroclysis had the added advantage of being able to demonstrate multiple different areas of narrowing in this patient (not shown) as well as evaluating bowel wall thickness and extraluminal pathology
This study is more difficult for the radiologist to perform and for the patient to tolerate. Therefore, it is used only in select situations, as when cross-sectional and endoscopic evaluations have proven unrevealing.
CT Enteroclysis
This type of study evaluates the small bowel in a similar manner to conventional enteroclysis. However, barium and methylcellulose are not used as contrast agents. The patient receives either positive (radiopaque) contrast, such as barium or diluted water-soluble contrast, or negative (radiolucent) contrast, such as water, prior to being taken to the CT scanner. Typically, the scan is performed once contrast has reached the cecum. CT enteroclysis is more sensitive for the detection of small strictures and mucosal inflammation such as in Crohn’s disease.
Postoperative Imaging
Conventional fluoroscopic evaluation has become less frequently utilized in the day-to-day evaluation of gastrointestinal complaints owing to the expanding role of cross-sectional imaging and endoscopy. In the postoperative setting, however, fluoroscopy has gained a larger role as a low-risk (as compared to a return to surgery) evaluation of anatomy, leaks, or fistulae in patients post gastric bypass, esophagectomy, and stent placement. Of note, barium is contraindicated when a leak is suspected as it can stimulate an inflammatory response and peritonitis. Therefore, fluoroscopy with a water-soluble contrast agent is commonly performed to identify anastomotic leakage or stenosis.
-
S: Contrast fluoroscopy exams provide readily accessible anatomic and physiologic data. However, care should be taken to minimize the risks of ionizing radiation both to examiners and patients alike. Consultation with health physics personnel should be considered particularly in children. In addition, barium should not be used in the setting of suspected obstruction or perforation. Care should be taken to avoid the use of water-soluble contrast in the setting of possible aspiration.
-
A: While radiographs and CT play roles in evaluation of the upper gastrointestinal tract and small bowel, contrast fluoroscopy examination allows for real-time evaluation of physiology, anatomic delineation, and localization of focal abnormalities, such as leaks. This modality is of particular use in the postoperative setting, in which complications and variant anatomy are frequently of clinical concern.
-
F: An understanding of upper gastrointestinal and small bowel physiology, normal and postoperative anatomy is essential in the interpretation of fluoroscopic GI exams. As an example, it is key to recognize the presence of a gastro-gastric fistula in the patient who is status post Roux-en-Y gastric bypass or to localize an esophageal leak status post intervention.
-
E: Fluoroscopic examination of the upper GI tract and small bowel can be used in elective and emergent settings and allow for the relatively rapid detection of potentially acute but correctable findings. Actionable findings require immediate communication to the appropriate providers.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kissane, J., Neutze, J.A., Singh, H. (2020). Fluoroscopic Evaluation of the Upper GI Tract and Small Bowel. In: Kissane, J., Neutze, J., Singh, H. (eds) Radiology Fundamentals. Springer, Cham. https://doi.org/10.1007/978-3-030-22173-7_30
Download citation
DOI: https://doi.org/10.1007/978-3-030-22173-7_30
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-22172-0
Online ISBN: 978-3-030-22173-7
eBook Packages: MedicineMedicine (R0)