
Abstract
Chlamydia trachomatis infection is one of the most common bacterial sexually transmitted infections (STIs) in the United States, with the highest prevalence in adolescents and young adults <25 years old. Incidence has been increasing in recent years. The majority of chlamydia infections are asymptomatic in both men and women. Chlamydia infection can lead to urethritis as well as serious health consequences, such as pelvic inflammatory disease, infertility, and increased risk of HIV transmission. Screening of high-risk individuals is critically important for controlling and preventing transmission of disease. Nucleic acid amplification testing (NAAT) of mucosal surfaces and urine is the diagnostic test of choice, with high sensitivity of detecting infection. Despite expansion of testing practices, many young people are still not being tested. Public health efforts to focus on prevention in adolescents and young adults will be extremely important to reduce the number and impact of STIs over the course of their lives.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Case StudyA 16-year-old male patient comes in to see his primary care doctor for an acute care visit. He has a chief complaint of a penile discharge and burning with urination. He also complains of mild fatigue but otherwise feels well. On further questioning, he is sexually active with multiple male partners and states he uses condoms approximately 10% of the time. His last anonymous sexual encounter was 3 weeks ago with a partner whom he met on a website. He also had sex with his regular partner last week, but his regular partner doesn’t have any symptoms. He has never been tested for HIV or other sexually transmitted infections.
On physical examination, he is afebrile. His genitourinary exam is notable for a purulent penile discharge. He is also noted to have very mild diffuse lymphadenopathy in the inguinal areas.
His physician prescribes treatment and orders testing for a range of sexually transmitted infections, including HIV. He is counseled to abstain from sex for 7 days after treatment. A urine NAAT for chlamydia comes back positive. With treatment, the patient feels well and is no longer having symptoms. His partners in the last 60 days are tested and treated for exposure to chlamydia despite not having symptoms. His HIV test is negative, and given his risk factors, he is counseled on PrEP (pre-exposure prophylaxis) for HIV.
Questions for Consideration
-
What are the clinical features of chlamydia infection?
-
What treatment is indicated at this time?
-
How should the patient be counseled to avoid further transmission?
Microbiology and Pathophysiology
Chlamydia are gram-negative obligate intracellular bacteria that rely on the host cell for all metabolic needs. They are exquisitely adapted to life inside cells and have specialized cell types for replication and cellular invasion. This developmental program alternates between two differentiated cell types, the elementary body (EB) and reticulate body (RB), and is critical to the completion of its life cycle [1]. The genus Chlamydia contains the causative agents of a number of important pathogens of humans. C. psittaci causes zoonotic infections resulting in pneumonia, while C. pneumoniae is a human pathogen that causes respiratory disease and is linked to atherosclerosis. Biovars of C. trachomatis are the causative agents of trachoma, the leading cause of preventable blindness worldwide, as well as the sexually transmitted disease Chlamydia. Irrespective of the resulting disease, all chlamydial species share the same obligate intracellular life cycle and biphasic developmental cycle.
The cell-type-specific division of labor (replication = RB, cell invasion = EB) in these pathogens generates a life cycle that results in a viral-like one-step growth curve with a defined eclipse period when no infectious progeny is present. Chlamydial pathogenesis is dependent on balancing the need to replicate with the need to create infectious progeny. The infectious cycle starts with the elementary body (EB) cell type binding to target cells and inducing uptake through engagement of a specialized secretion system called the type III secretion system (T3SS) and delivery of effector proteins directly into the target cell cytoplasm [2,3,4]. This pathogen-directed endocytosis results in the EB residing in a membrane-bound vesicle derived from the plasma membrane of the host cell and is termed the chlamydial inclusion. Chlamydia alters the properties of this vacuole shortly after entry by insertion of proteins into the inclusion membrane [5,6,7,8]. These membrane modifications ensure that the inclusion is not acidified by fusion with the endocytic or lysosomal pathway [9,10,11]. The diverse array of inclusion membrane (Inc) proteins give the inclusion unique properties and make the inclusion significantly different from other membrane systems of the host cell. One of these Inc proteins, IncA, confers homotypic fusion properties to the inclusion promoting fusion of nascent inclusions in multiply infected cells [12]. Additionally, the inclusions are trafficked to the microtubule-organizing center (MTOC) of the cell through hijacking the dynein microtubule motor protein [13]. The inclusion remains associated with the MTOC throughout the rest of the developmental cycle through continued interaction with dynein and the minus ends of microtubules [13,14,15]. The mature inclusion has unusual biophysical properties; it has a characteristic spacious inflated morphology, is neutral in pH and has an ionic environment identical to the host cytosol, and is permeable to small ions [16]. To increase in size and acquire nutrients, the inclusion interacts closely with the exocytic compartment intercepting the lipids sphingomyelin and cholesterol from the Golgi [17,18,19]. In addition to intercepting lipids from the Golgi, the chlamydial inclusion closely associates with the host cell ER system to obtain other nutrients through this unique interaction [20].
Late in the developmental cycle, RBs undergo secondary differentiation asynchronously back to the infectious EB form as the inclusion becomes filled with RBs. This step is characterized by a condensation of the chromosome to form a densely packed nucleoid structure, leading to a reduction in the size of the cell from 1 to 0.3 μm in diameter. The outer membrane proteins of the EB undergo significant disulfide cross-linking to impart a structural rigidity to the outer membrane [21]. The replicative cycle inside the host cell ends when the chlamydia fills the cell and induces either lysis of the host cell releasing the EB cell type or extrusion of the inclusion again releasing the infectious EB cell type [22, 23].
The components of this unique developmental cycle impart two important pathogenic advantages to chlamydial infection. One, the inclusion membrane acts as a barrier between the bacteria and host cytosol and is thought to effectively hide the bacteria from host innate immune surveillance [24, 25]. Two, the infectious EB cell types small size and cross-linked outer membrane are likely key virulence adaptations that enhance the transmission and spread of the infection from person to person and from initial infection location to distal sites within the urogenital tract. The inclusion membranes’ barrier function is a two-way street providing an immune evasion advantage but at the same time inhibiting the bacteria’s access to the nutrients in the cell cytosol and restricting the delivery of effector proteins. The balance between these two opposing properties likely reflects important trade-offs in the biophysical characteristics of this unique replicative niche. The EB cell type is likely specialized to enhance infectivity in the differing niches it encounters. It’s not clear what role the physical features of the EB cell type play in virulence, but increasingly, it is recognized that the EB cell type, although incapable of replication, can respond to environmental nutrients [26]. These results are consistent with the chlamydial EB being a metabolically responsive cell form that depends on maintaining active interactions with its environment to maintain infectivity.
Epidemiology
Chlamydia trachomatis is one of the most common bacterial sexually transmitted infections (STI) in the United States (US) among sexually active adolescents and young adults [27,28,29]. C. trachomatis can cause a variety of clinical syndromes including urethritis, cervicitis, and oropharyngeal disease and has the potential to lead to long-term sequelae in women such as pelvic inflammatory disease (PID) and infertility. Adding to the public health implications of this infection, C. trachomatis increases the risk for acquiring HIV infection [30]. There are 15 serotypes of C. trachomatis with anogenital infection caused often by serotypes D-K and LGV (lymphogranuloma venereum) caused by L1, L2, and L3 [31].
In 2017, there were >1.7 million cases reported in the United States with the highest prevalence in adolescents and young adults under 25 years of age [29]. Most chlamydia infections are asymptomatic, so the number of infections identified and reported can increase as more people are screened even when incidence is flat or decreasing. The incidence of C. trachomatis has increased steadily in recent years, with a 6.9% overall increase in the number of cases from 2016 to 2017. During 2016–2017 alone, the rate among men increased 10.5%; however, during 2013–2017, rates of reported cases among men increased 39.3% compared with an 11.1% increase among women. There are twice as many chlamydia cases in women (687.4 cases per 100,000 females) as in men (363.1 cases per 100,000 males) in the United States; however, the number of cases increased by 3.8% in women and 10.5% in men from 2016 to 2017.
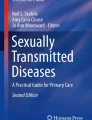
Rates of chlamydia vary by factors including age of patient, geographic region, race, and ethnicity (Fig. 13.1). Rates have been increasing in both young men and women since 2014 [32]. Among men, the age-specific rates of chlamydia cases were highest in the age group of 20–24 years old at 1705.4 cases per 100,000 males. Among women, the age-specific rates were highest in age group of 15–19 and 20–24 years and increased over the last 3 and 4 years, respectively. The rate among 15–19-year-olds increased 6.5% during 2016–2017, with a total increase of 10.7% during 2014–2017 (2949.3 to 3265.7 cases per 100,000 females). Black men and women are disproportionately affected by the disease with 5.6 times higher rates of chlamydia cases among Blacks than that among Whites (1175.8 and 211.3 cases per 100,000 population, respectively). Rates of reported cases are also high among American Indians/Alaska Natives (3.4 times higher), Hispanics (1.9 times higher), and Native Hawaiians/Other Pacific Islanders (3.3 times higher) than the rates among Whites [29].

Rates of reported cases by age group and sex, United States, 2017 [29]
The National Health and Nutrition Examination Survey (NHANES) is a nationally representative survey of the US civilian, noninstitutionalized population that provides an important measure of chlamydia disease burden in respondents aged 14–39 years [4]. One NHANES study from 2013 to 2016 demonstrated that the overall prevalence of chlamydia among persons aged 14–39 years was 1.7% (95% confidence interval [CI]: 1.3–2.1). Among sexually active females aged 14–24 years, the population targeted for screening, prevalence was 4.3% (95% CI: 2.7–5.8), with the highest prevalence among Mexican American females (10.0%, 95% CI: 4.0–15.9) [29] (Fig. 13.2). A substantial number of infections are seen even among sexually active participants reporting only one partner in the last year [34]. With regard to certain high-risk populations, a cross-sectional analysis of chlamydia prevalence from incarcerated persons entering selected juvenile facilities was high at 14.3% for women and 6% for men. Incarcerated persons are more likely to report multiple partners, unprotected sex, history of substance abuse, and commercial sex work or difficulty accessing care and therefore at high risk for STIs including chlamydia [35,36,37].

While C. trachomatis often infects the urogenital tract, extragenital sites such as the oropharynx and rectum are emerging as important anatomic reservoirs of chlamydial disease burden in both men and women. Infections at these extragenital sites are often asymptomatic. A review of 80 studies from 5 international sites published between 1981 and 2015 focusing on extragenital infection reported a range of prevalence for rectal chlamydia of 2.0–77.3% and pharyngeal chlamydia of 0.2–3.2% in women, rectal chlamydia of 2.1–23% and pharyngeal chlamydia of 0–3.6% in MSM, and rectal chlamydia of 0–11.8% and pharyngeal chlamydia of 0–22% in limited data in MSW [38]. Specifically in the United States, one study at an STD clinic in Seattle, Washington, demonstrated pharyngeal chlamydia infection at 2.3% and rectal chlamydia infection at 11.9% [39]. Differences in prevalence of C. trachomatis infections at these extragenital sites were often seen due to different clinical settings and methods of diagnosis.
Despite expansion of testing, many young people who are at risk are still not being tested, with fewer than half of sexually active young women screened annually despite high prevalence and incidence of disease in this group. There is also data to support screening programs for chlamydia infection in women, in order to help prevent adverse sequelae such as PID [40]. However, studies have demonstrated suboptimal chlamydia screening and rescreening rates in both men and women, ranging from 22.3% to 44%, in a variety of clinical settings [41,42,43,44].
The high prevalence of chlamydial infection in the United States among adolescents and young adults is attributable to a variety of reasons including asymptomatic infection, lack of adequate screening, lack of familiarity with this infection among treating clinicians, and a paucity of available facilities for easy detection and treatment. Furthermore, there is a need for programs focused on screening high-risk patients, contact tracing, and rapid treatment of infected individuals. Most of cases of chlamydia (over 75%) have been reported outside of STD clinics, mostly from private physicians and health maintenance organizations, emphasizing the need for testing and treatment in a variety of settings (Fig. 13.3) [29]. There is therefore a clear need for training of a wide range of primary care providers, in order to enhance awareness of national recommendations for STI screening and improve rates of routine STI screening and health education among at-risk populations such as adolescents and young adults.

Chlamydia — Proportion of STD Clinic Patients Testing Positive∗ by Age Group, Sex, and Sexual Behavior, STD Surveillance Network (SSuN), 2017 [29]. ∗ Proportions represent the overall average of the mean value by jurisdiction. † Results are based on unique patients with known sexual behavior (n = 95,167) attending SSuN STD clinics who were tested ≥1 times for chlamydia in 2017. Acronyms: MSM = Gay, bisexual, and other men who have sex with men (collectively referred to as MSM); MSW = Men who have sex with women only
Screening
The majority of chlamydia infections are asymptomatic, making routine screening of high-risk individuals critically important for controlling and preventing disease transmission to protect both individuals and the public health. Detection and treatment of infection can prevent serious sequela in women, and screening programs have contributed to declines in rates of PID [40, 45, 46]. The 2015 CDC STD treatment guidelines outline screening recommendations for men and women, including adolescents [47]. Adolescents and young adults who initiate sex early in adolescence, those who are incarcerated or in detention facilities, those who use injection drugs, those evaluated in STD clinics, young men who have sex with men (MSM), and those with multiple sex partners are considered high risk and should be screened routinely for infection [29].
No state in the United States requires parental consent for STI care, but health-care providers should check with local and state recommendations regarding the details of STI services and parental notification. They should also be aware of insurance claims and notification to beneficiary of services performed when treating the adolescent and young adult community in the geographic area. However, these confidentiality concerns must be balanced against the benefits to the individual and society. If patients do not have access to care or clinicians do not screen, many infections go undiagnosed, unreported, and untreated leading to the spread of disease.
Heterosexual Individuals
The USPSTF and the CDC recommend screening for chlamydia in sexually active females ≤24 years and in older women at increased risk for infection, such as a new sex partner, multiple sex partners, or sex partners with an STI [47, 48]. While data to assess screening for chlamydia in heterosexual men is lacking, in areas with high prevalence of chlamydia, screening of young heterosexual men can also be considered. This can include screening in adolescent clinics, correctional facilities, STD clinics, or geographic areas with a high prevalence of chlamydia infection rates [48,49,50]. Despite the recommendations made by USPSTF and CDC regarding screening heterosexual individuals, rates of testing for C. trachomatis infection are still unfortunately low [51,52,53,54]. There are no recommendations regarding screening of extragenital sites in heterosexual individuals, such as rectal or oropharyngeal chlamydia infection, but these infections do occur and are often asymptomatic. Providers should therefore inquire about oral and anal sexual practices and test at extragenital sites as indicated by the individual patient’s sexual practices.
Pregnant Women
Mother-to-child transmission of chlamydia can cause severe complications in the neonate, including conjunctivitis and pneumonia. Screening for C. trachomatis infection in pregnant women is therefore extremely important [48]. It is recommended that all pregnant women <25 years be tested for chlamydial infection and gonorrhea during the first prenatal visit and retested during the third trimester [55]. If a pregnant woman is found to have evidence of chlamydia infection, repeat NAAT testing for eradication of the disease should be done 3–4 weeks after completion of therapy to document cure of infection and again 3 months after treatment. Repeat testing and documentation of cure is recommended in pregnant women as persistent or a new infection with C. trachomatis can be transmitted to the neonate during parturition. In addition to the risk of neonatal pneumonia and conjunctivitis, studies have shown that treatment of chlamydial infection is associated with significantly lower rates of preterm delivery, early rupture of membranes, and infants with low birth weight compared with no treatment or treatment failure [56].
MSM (Men Who Have Sex with Men)
In this population, there is increased risk for HIV and STDs, and screening is recommended at least yearly for urethral infection in men who have insertive intercourse and/or rectal infection in those who have receptive anal intercourse [47]. In those persons with multiple or anonymous partners, sexual partners with multiple partners, or other high-risk factors, 3–6 month screening for C. trachomatis is recommended [57]. Gay-focused community-based organizations can serve as valuable partners in helping to reach young MSM who may not be tested elsewhere. Other than urethral chlamydia infection, rectal and oropharyngeal chlamydial infection can be important anatomic areas of infection and routes of transmission to uninfected partners. Although testing for C. trachomatis pharyngeal infection is not specifically recommended by the CDC [47], extragenital infections are common in the MSM population. There have been reported cases of oropharyngeal to genital transmission of infection, and therefore screening can be considered, especially in highly prevalent populations [38, 39, 58,59,60,61,62,63,64,65]. Furthermore, rectal chlamydia infection has been associated with increased risk of HIV acquisition among MSM. While NAAT is not currently cleared by FDA for pharyngeal testing, many public health departments and other providers utilize NAAT-based pharyngeal, rectal, and urethral screening for chlamydia among the MSM population. Health-care providers should be aware of the significant public health implications associated with chlamydia: (1) multiple infections with gonorrhea or chlamydia are associated with increased risk of HIV infection among MSM [66, 67], and (2) incidence of STDs has been shown to decline with frequent, routine STD testing and risk reduction counseling in high-risk populations [68].
WSW (Women Who Have Sex with Women)
While historically WSW were considered to be low risk for STIs [69, 70], recent data suggests that assessment and screening of STIs among WSW is an important part of their sexual health [71,72,73,74]. There is data to suggest this population is still at risk for STIs, particularly adolescent and young adult WSW and those who also have male partners [75,76,77,78]. A study evaluating young women ages 18–24 years reported that bisexual students were most likely to have an STI in the past year; of note, even among those who reported only female partners, 6% had evidence of an STI [78]. In another study, a high rate of C. trachomatis infection was seen in African American WSW who participated in exclusive sexual activity with women (13.5%), and an even higher rate (35%) was demonstrated if these women had sex with men as well [79]. Another study among WSW ages 15–24 years old showed positive chlamydia cases among WSW and WSMW (women who have sex with men and women) at 7.1% compared to WSM (women who have sex with men) at 5.3%. This provides evidence to suggest that C. trachomatis is common among women reporting same-sex sexual behavior, especially in the adolescent and young adult age group. Health-care providers should implement STI screening according to the general guideline for young women and cannot assume that WSW are at low risk for STIs [80].
Transgender Patients
While there are few studies of C. trachomatis infection specifically in transgender men and women, providers should discuss patient anatomy and sexual behavior with these patients and provide screening according to risk behavior and guidelines [81]. It is recommended that transgender patients should be assessed closely for STD- and HIV-related risks and screened accordingly based on behavioral history and sexual practices.
HIV
For those with HIV -positive status, all men and women should be screened for chlamydia, in addition to other STIs, initially upon entering into care and at least annually, with more frequent follow-up testing (3–6 months) depending on risk behavior [81,82,83]. Given high reinfection rates in this population, retesting for chlamydia infection is indicated at 3 months after treatment, not to document cure but to assess for new infection. Specifically, MSM with HIV infection are at increased risk for STDs [68]; therefore, screening for syphilis, gonorrhea, and chlamydia is an important part of primary care by health-care providers.
Persons in Correctional Facilities
There are high rates of chlamydia infection, as well as other STIs, in both men and women ≤35 in juvenile and adult detention facilities [84]. The rates are higher in women than in men which is concerning given the long-term complications of chlamydia infection that can occur in women. This patient population might have had limited access to medical care or engage in high-risk behaviors for STIs. Therefore, universal screening for chlamydia in women ≤35 entering correctional facilities is recommended. For men, it is recommended to screen for chlamydia among <30 years old at intake into jails and other correctional facilities [49, 81].
Coinfections
Persons infected with N. gonorrhoeae are frequently coinfected with C. trachomatis and other STDs; therefore, it is important to screen for these infections, including gonorrhea, syphilis, and HIV [85, 86]. Women with bacterial vaginosis have also been shown to be at increased risk for chlamydia infection [87].
Repeat Infections
Several studies have shown there are high rates of repeat infection several months after initial chlamydia infection, often due to unprotected sex with an untreated sex partner or a new sex partner. In men, 13% had evidence of repeat infection within 4 months of initial diagnosis, and among female adolescents, 26.3% had reinfection within one year [88,89,90]. Repeat infection with chlamydia is associated with elevated risk for PID and other complications in women. Therefore, rescreening for this STI is an underutilized but important intervention in those persons with a past history of chlamydia infection in many primary care settings. The CDC STD treatment guidelines recommend men and women who have been treated for C. trachomatis should be retested approximately 3 months after treatment (or whenever persons next present for medical care if retesting at 3 months is not possible) [47], regardless of whether patients believe sex partners were treated. Test-of-cure using NAAT at 3–4 weeks is not routinely recommended for patients except in cases of pregnant women, questionable medication adherence, persistence of symptoms, or suspected reinfection.
Clinical Features
Infections with C. trachomatis are often asymptomatic but can lead to both acute symptoms and long-term health consequences such as PID and infertility in women and increased risk of HIV transmission in both sexes [91]. In men, the urethra is the most common site of infection, while in women, infection is often in the urethra and cervix. Adolescent and young adult women often have undiagnosed chlamydial infection. The asymptomatic nature of disease facilitates transmission of the bacteria between partners given a large reservoir of untreated persons who do not know they are infected.
Infections in Women
While chlamydial infections in women are often asymptomatic, the disease can result in urethritis, cervicitis, pelvic inflammatory disease, ectopic pregnancy, and ultimately infertility [92, 93]. Some symptoms in women mimic that of a urinary tract infection (painful or burning urination), and abnormal vaginal discharge or bleeding can also be seen. On speculum examination, patients with cervicitis will have cervical erythema, endocervical discharge, and/or a friable cervix (easily induced bleeding) [94, 95]. Providers should suspect an STI in women with urethritis, especially those with a new sex partner. Symptoms of PID include fever, pelvic or abdominal pain, and adnexal/cervical motion tenderness [92, 94] with the potential to scar and produce adhesions and inflammation in the fallopian tubes, ovaries, and endometrial lining leading to infertility [96]. While the rate of progression to PID in the general, asymptomatic population appears to be low, in some high-risk settings, 2–5% of untreated women can develop PID [97,98,99]. If an infected mother passes the infection to infants in delivery, potential consequences of blindness and pneumonia in the infant can occur.
Infections in Men
In men, chlamydia infection is a cause of urethritis, epididymitis, oropharyngeal infection, and acute proctitis in MSM who practice receptive rectal intercourse. C. trachomatis accounts for approximately 20–50% of cases of NGU (nongonococcal urethritis) [100]. Often, men present with symptoms of dysuria, urethral discharge, and urethral discomfort. The discharge which can be sparse might be mucopurulent, cloudy, or clear. Patients might have erythema of the urethral meatus with localized lymphadenopathy. In younger men, C. trachomatis is a common cause of acute epididymitis, in which patients present with testicular or scrotal pain and tenderness on exam [101]. Epididymitis is usually associated with urethritis; the latter is often asymptomatic.
Anorectal Infection
Anorectal infection can occur in men or women who practice receptive rectal intercourse. Like urethral infection, it can be asymptomatic but also has the potential to lead to severe proctitis or inflammation of the rectum. Anorectal chlamydia infection often presents with anal pruritus, mucopurulent or bloody rectal discharge, anal pain, constipation, or tenesmus. If patients present with symptoms of proctitis, they should have anoscopy and evaluated for STIs. Treatment of anorectal C. trachomatis infection appears to have more efficacy with a doxycycline-based regimen rather than a single dose of azithromycin [102] (outlined further in Treatment section of chapter). Sigmoidoscopy, when performed (generally to rule out other causes of proctitis), might demonstrate friable rectal mucosa, and a rectal gram stain would be expected to show elevated polymorphonuclear leukocytes (PMNs).
Oropharyngeal Disease
The pharynx can be a site of chlamydial infection in either men or women, if oral-genital contact occurs [59]. While this presentation is also often asymptomatic and underdiagnosed due to inadequate screening, patients can present with symptoms of pharyngitis including sore throat, fever, and tender cervical adenopathy. If infected at this anatomic site, patients have the potential to transmit this infection to uninfected partners through oral-genital contact [103, 104].
LGV (Lymphogranuloma Venereum)
LGV is caused by chlamydial serotypes L1, L2, and L3 – like other strains of chlamydia, these serotypes are also transmitted through unprotected vaginal, anal, or oral sexual contact. The classic presentation of LGV includes typically painless genital ulcers with tender femoral and inguinal adenopathy. LGV can also manifest as proctitis in those practicing receptive anal intercourse – symptoms may include diarrhea, abdominal cramps, rectal pain, mucoid/bloody rectal discharge, and/or fever [105, 106]. LGV proctitis can lead to serious sequelae if left untreated, such as perirectal abscess, fistulas, and strictures [107, 108]. Coinfections of other STIs with LGV is common. Due to the increase of LGV in MSM populations in the last 10–15 years, health-care providers should consider LGV in the diagnosis when sexually active patients present with proctitis or inguinal/femoral lymphadenopathy, especially if they are HIV-seropositive MSM.
Diagnostic Testing
While empiric therapy is recommended in a patient with symptoms suggestive of chlamydia, diagnostic testing should always be performed to confirm C. trachomatis infection. This testing facilitates the evaluation and treatment of both patients and sexual contacts. Chlamydia trachomatis is a reportable disease in every state which helps with public health efforts including monitoring, treatment, and prevention. Clinicians should familiarize themselves with local reporting requirements by local STI programs, as well as national guidelines.
Diagnostic testing for C. trachomatis rely primarily on molecular testing by PCR. Serologic tests are not widely used, other than to help support the diagnosis of LGV since baseline prevalence of antibody to C. trachomatis is high in certain populations and IgM Ab often cannot be demonstrated within the time frame of disease. In men with urethritis, a gram stain showing gram-negative intracellular diplococci (suggesting N. gonorrhoeae) is a rapid way to distinguish NGU from gonorrheal infection; however, microscopy alone cannot diagnose chlamydia infection. There is not enough data to support the use of gram stain on endocervical specimens from women or pharyngeal or rectal specimens from men or women.
The recommended test to diagnose chlamydia infection in both men and women is NAAT (nucleic acid amplification testing) [65, 109]. The FDA has approved NAAT testing for the diagnosis of C. trachomatis testing in genitourinary tract specimens [110]. In women, this can be done by testing first-catch urine or collecting swab specimens from the endocervix or vagina. In men, urethral swabs or first-catch urine specimens can be tested. Extragenital sites, such as oropharyngeal and rectal specimens, have not been cleared by the FDA for detection of chlamydia, but most laboratories have performed Clinical Laboratory Improvement Amendment (CLIA)-compliant validation studies and may offer NAAT for extragenital specimens [58, 65, 110]. All cases of urethritis in men should be screened for C. trachomatis by NAAT on first-catch urine, and MSM should be tested for C. trachomatis from any potentially exposed site (e.g., rectum, throat) [103].
Point-of-care tests can help facilitate early treatment, but they have reduced sensitivity and specificity compared with NAAT testing [111]. However, rapid NAAT tests for chlamydia are available, can provide testing with same-day results, and might be of benefit to use in the adolescent and young adult population. The Cepheid GeneXPert CT/NG assay is a chlamydia rapid NAAT with high sensitivity and specificity of >97% for C. trachomatis and is approved for urine and endocervical/vaginal swabs [112]. Self-collection of swabs as an alternative to clinician-collected swabs is reliable and one way to help expedite or simplify screening in both men and women that is acceptable to patients [113,114,115,116].
Women with cervicitis should be tested for chlamydial infection and assessed for signs of PID. The finding of >10 WBC per high power (400X) field is consistent with endocervical inflammation caused by C. trachomatis or N. gonorrhoeae, but this is not diagnostic [117]. NAAT testing on vaginal swab fluid collected by clinician or the patient has higher sensitivity than urine, and for women being evaluated with a speculum exam, NAAT testing can be done on endocervical swabs [118].
Genital lesions and rectal specimens can be tested for C. trachomatis in the setting of LGV or other anorectal disease by NAAT if CLIA validation studies have been done in the laboratory and are the preferred method of detection. Diagnosis of LGV is based on clinical suspicion and rates seen in the community while excluding other causes of symptoms. Based on clinical presentation (e.g., symptoms of proctitis) with or without a positive NAAT, patients with findings of LGV should be treated empirically.
Recurrence of infection occurs frequently in adolescents and young adults of both sexes [90, 119]. Therefore, if a patient tests positive for chlamydia, recommendations are to rescreen that person 3 months after treatment to evaluate for new STIs [47]. One study demonstrated that 13% of men with C. trachomatis infection in urban centers ages 15–35 years of age were reinfected [88]. Among female adolescents in school-based health centers, the incidence of reinfection was also high, supporting the recommendation to rescreen adolescents frequently (both men and women) [89]. Early repeated chlamydial infections (<3 months) in adolescent women were often by the same genotype than later repeated infections [90], suggesting that most repeated infections may result from failure of sex partners to receive treatment. Despite these findings, studies have shown that the repeat testing recommendations are infrequently followed. In an analysis of chlamydia testing data from a large US laboratory from 2008 to 2010, positivity rates were highest among female adolescents, and retesting rates of persons with a history of infection were suboptimal, with only 22.3% of men and 38.0% of nonpregnant women retested. Of pregnant women, although 60.1% with a positive test were retested, only 22.0% received a test-of-cure within the time frame recommended in the CDC STD treatment guidelines [43].
If follow-up cannot be insured in patients presenting with symptoms consistent with chlamydia infection, they should be treated presumptively until results of testing are available. Cases should be reported to the health department per state requirements. Test-of-cure or repeat testing 3–4 weeks after completing therapy is no longer routinely recommended except in specific situations such as pregnant women, suspected nonadherence to treatment, persistent symptoms in a patient or partner, and concern for reinfection. Of note, however, positive NAAT testing within 3 weeks might reflect the presence of nonviable organisms; therefore, repeat testing less than 3 weeks after a positive result is generally not recommended [110].
Treatment
Antibiotics with good intracellular penetration must be used for C. trachomatis infections, which also necessitate either a long half-life or a prolonged course of therapy. Treatment is critical to prevent health complications in the individual, reinfection of sex partners, and transmission to uninfected individuals and infants in pregnant women [98]. The most active agents against C. trachomatis include rifampin, tetracyclines, macrolides, sulfonamides, some fluoroquinolones, and clindamycin [120] (Table 13.2).
Recommended Regimens
Oral doxycycline 100 mg twice daily for 7 days and azithromycin as a single-dose therapy (1 gram taken orally) in directly observed therapy are both first-line recommendations for treatment of chlamydia infection of the urogenital tract. Alternative regimens are listed in Table 13.3a and include erythromycin, levofloxacin, and ofloxacin. Erythromycin might have a higher rate of GI side effects and lower efficacy [121]. Azithromycin (but not doxycycline) can be administered in pregnant women, who – as noted above – should have repeat NAAT for test-of-cure in 3–4 weeks. Persons with chlamydia should be instructed to abstain from sexual intercourse for 7 days after treatment completion or until resolution of symptoms, whichever occurs last [47].
There is some evidence of heterotypic in vitro resistance to doxycycline [122]. However, doxycycline has been shown to be quite effective in clearing C. trachomatis infections, and recent studies have shown better efficacy with doxycycline compared to azithromycin for treatment of NGU and chlamydia rectal disease [102, 122,123,124,125,126]. A meta-analysis evaluating treatment for rectal chlamydia demonstrated pooled efficacy for doxycycline at 99.6% compared to azithromycin at 82.9% [102]. A summary of 23 studies found there might be small increased efficacy for doxycycline compared with azithromycin for the treatment of urogenital chlamydia as well, but more data are needed in this area [124, 125]. However, suboptimal adherence to the multiday dosing of doxycycline might contribute to poor treatment outcomes for C. trachomatis infection in men with NGU, although nonadherence was not significantly associated with clinical failure overall [127]. Compliance with a 7-day antibiotic regimen might be especially challenging in the adolescent and young adult population; therefore, health-care providers should assess their patient’s ability to comply with therapy and weigh the risks and benefits of 7 days of doxycycline versus one-time azithromycin therapy. A randomized control trial to evaluate treatment efficacy of azithromycin versus doxycycline for the treatment of rectal chlamydia among MSM is pending [128].
LGV infection with serotypes L1, L2, and L3 can lead to serious consequences if left untreated. These include colorectal fistulas, strictures, and even elephantiasis. Relative to other chlamydial infections, LGV requires a prolonged course of therapy [121]. For LGV, the treatment of choice is doxycycline 100 mg orally twice daily for 21 days. Erythromycin 500 mg orally four times daily for 21 days is an alternative regimen that can be used in pregnancy (Table 13.3b) [47].
Sexual partners should also be referred for evaluation, testing, and treatment if they have had sexual contact with the patient within 60 days of symptom onset or diagnosis. Expedited partner therapy (EPT) also known as patient-delivered partner therapy (PDPT) is legal in most states and refers to the process of giving prescriptions or medications to the patient for delivery to their partner(s), without direct evaluation of the partner by the treating clinician. The impact of prescriptions on sex partner treatment using expedited partner therapy for C. trachomatis was recently evaluated in young women ages 15–25 years, and prescription-EPT and medication-EPT chlamydia showed comparable rates of partner treatment [129]. These methods of partner treatment are recommended by the CDC STD guidelines to be offered to heterosexual patients with chlamydia infection when the provider cannot ensure that all sex partners from the prior 60 days will be otherwise treated, only if this practice is legal in their state (www.cdc.gov/std/ept) [47]. Patients assigned to expedited treatment of sexual partners are significantly more likely than those assigned to standard referral of partners to report that all of their partners are treated. They are also significantly less likely to report having sex with an untreated partner and are shown to have high levels of acceptability in the adolescent population [130, 131]. Studies have shown that EPT/PDPT can increase partner treatment rates, thereby decreasing the rate of reinfection, with potential to decrease C. trachomatis incidence at the population level [131,132,133,134]. The main limitation of EPT is that it misses an opportunity to test partners for coexisting infections that may require treatment – including gonorrhea, syphilis, or HIV. For this reason, the recommendation is for EPT to be used in low HIV prevalence settings, for heterosexual populations. EPT chlamydia is not currently recommended for MSM with chlamydia given the high risk of undiagnosed concomitant HIV infection and other STDs in this patient population. For all patients, full evaluation and testing of a partner of an infected patient is ideal, and all persons with chlamydia should be encouraged to notify sex partners and to seek treatment.
Prevention
There is no vaccine that prevents chlamydia infections. Abstinence from oral, vaginal, and anal sex and a monogamous relationship with a partner known to be uninfected are the most effective ways to prevent disease. Male and female condoms, when used consistently and correctly, can significantly decrease the rate of STIs, including chlamydia [135].
As a high proportion of chlamydia infections impact adolescents and young adults, public health efforts focused on prevention in this age group are extremely important to reduce the number and impact of STIs over the course of their lives. Health-care providers play an important role in these efforts, including obtaining detailed sexual histories from patients and providing risk reduction and prevention counseling in a nonjudgmental way to all sexually active adolescents [136,137,138]. Programs to institute strategies for chlamydia screening, especially in asymptomatic individuals, as well as effective diagnosis, treatment, and follow-up of patients and their partners can help with prevention and control of this disease. In adolescents and young adults, patients might be marginalized and may not have access to care or psychosocial barriers that make access to care difficult.
An analysis of 31 trials suggested that high-intensity counseling (>2 hours) reduced STI incidence in adolescence in primary care and related settings [137]. While data are sparse, less intensive interventions also have the potential to reduce STIs in adolescents and young adults [139,140,141]. Both enhanced (quarterly, high intensity, interactive) and brief counseling groups lowered STD incidence at 3 and 6 months, and 30% fewer participants had new STDs in the enhanced counseling group at 6 months [142]. Sexual risk reduction interventions should provide information on all STIs, including HIV, as well as prevention strategies such as condoms, regular screening, and pre-exposure prophylaxis for HIV if indicated.
Early sexual education and STD testing of all sexually active adolescents is an important part of prevention. For this particular population, barriers to screening that have been identified include lack of health insurance coverage or coverage under a parent, lack of regular access to health care, as well as the difficulties of identifying adolescents who have been sexually active [143,144,145,146,147]. The majority of women initiate sexual activity during adolescence, and even those youth who have little sexual experience (e.g., less than one year) or those with few lifetime partners, the prevalence of any STI is quite high. However, despite recommendations and high prevalence of STIs in this sexually active young female population, only 42% of eligible young women received annual chlamydia screening in 2007 in US commercial and Medicaid health plans [51], recognizing there is a great need for chlamydia screening to protect young women from sequelae of this infection [148]. Health-care providers should educate young patients about prevention strategies to lower STI risk by using condoms consistently and correctly, safer sex, and how to obtain medical care for STIs without parental consent in their geographic area [142].
As chlamydia is common and infections are usually asymptomatic, health-care providers should routinely screen sexually active young men and women according to guidelines, provide prompt treatment for infected persons, and ensure that infected patients’ sex partners receive timely treatment to prevent reinfection.
Case Conclusion
The patient’s presentation is consistent with acute Chlamydia trachomatis urethritis given his penile discharge, burning with urination, and mild inguinal lymphadenopathy. While these symptoms are classic for urethritis, the majority of patients with chlamydia infection are asymptomatic. Therefore, it is a major public health problem as persons might not realize they have the disease and are likely to unknowingly spread C. trachomatis to previously uninfected individuals. In men, symptomatic chlamydia infection causes urethritis; in women, it can cause urethritis or vaginitis. C. trachomatis can also colonize the oropharynx or rectum, as it can be transmitted through oral, vaginal, or anal sex. Complications in women can lead to pelvic inflammatory disease and infertility. Treatment involves therapy as soon as possible. Both this patient and his partners should be treated, even if they don’t have evidence of symptomatic disease. Given this patient’s risk factors of multiple sex partners as well as positive chlamydia testing, he should be screened at least every 3–6 months for sexually transmitted infections, including HIV. Barrier methods should be advised to protect the patient and his partners against other sexually transmitted infections.
References
Hafner L, Beagley K, Timms P. Chlamydia trachomatis infection: host immune responses and potential vaccines. Mucosal Immunol. 2008;1:116–30.
Jewett TJ, Miller NJ, Dooley CA, Hackstadt T. The conserved Tarp actin binding domain is important for chlamydial invasion. PLoS Pathog. 2010;6:e1000997.
Clifton DR, Fields KA, Grieshaber SS, et al. A chlamydial type III translocated protein is tyrosine-phosphorylated at the site of entry and associated with recruitment of actin. Proc Natl Acad Sci U S A. 2004;101:10166–71.
Engel J. Tarp and Arp: how Chlamydia induces its own entry. Proc Natl Acad Sci U S A. 2004;101:9947–8.
Suchland RJ, Rockey DD, Bannantine JP, Stamm WE. Isolates of Chlamydia trachomatis that occupy nonfusogenic inclusions lack IncA, a protein localized to the inclusion membrane. Infect Immun. 2000;68:360–7.
Bannantine JP, Griffiths RS, Viratyosin W, Brown WJ, Rockey DD. A secondary structure motif predictive of protein localization to the chlamydial inclusion membrane. Cell Microbiol. 2000;2:35–47.
Rockey DD, Viratyosin W, Bannantine JP, Suchland RJ, Stamm WE. Diversity within inc genes of clinical Chlamydia trachomatis variant isolates that occupy non-fusogenic inclusions. Microbiology. 2002;148:2497–505.
Betts HJ, Wolf K, Fields KA. Effector protein modulation of host cells: examples in the Chlamydia spp. arsenal. Curr Opin Microbiol. 2009;12:81–7.
Scidmore MA, Rockey DD, Fischer ER, Heinzen RA, Hackstadt T. Vesicular interactions of the Chlamydia trachomatis inclusion are determined by chlamydial early protein synthesis rather than route of entry. Infect Immun. 1996;64:5366–72.
Hackstadt T, Fischer ER, Scidmore MA, Rockey DD, Heinzen RA. Origins and functions of the chlamydial inclusion. Trends Microbiol. 1997;5:288–93.
Fields KA, Hackstadt T. The chlamydial inclusion: escape from the endocytic pathway. Annu Rev Cell Dev Biol. 2002;18:221–45.
Hackstadt T, Scidmore-Carlson MA, Shaw EI, Fischer ER. The Chlamydia trachomatis IncA protein is required for homotypic vesicle fusion. Cell Microbiol. 1999;1:119–30.
Grieshaber SS, Grieshaber NA, Hackstadt T. Chlamydia trachomatis uses host cell dynein to traffic to the microtubule-organizing center in a p50 dynamitin-independent process. J Cell Sci. 2003;116:3793–802.
Grieshaber SS, Grieshaber NA, Miller N, Hackstadt T. Chlamydia trachomatis causes centrosomal defects resulting in chromosomal segregation abnormalities. Traffic. 2006;7:940–9.
Richards TS, Knowlton AE, Grieshaber SS. Chlamydia trachomatis homotypic inclusion fusion is promoted by host microtubule trafficking. BMC Microbiol. 2013;13:185.
Grieshaber S, Swanson JA, Hackstadt T. Determination of the physical environment within the Chlamydia trachomatis inclusion using ion-selective ratiometric probes. Cell Microbiol. 2002;4:273–83.
Hackstadt T, Scidmore MA, Rockey DD. Lipid metabolism in Chlamydia trachomatis-infected cells: directed trafficking of Golgi-derived sphingolipids to the chlamydial inclusion. Proc Natl Acad Sci U S A. 1995;92:4877–81.
Saka HA, Valdivia RH. Acquisition of nutrients by Chlamydiae: unique challenges of living in an intracellular compartment. Curr Opin Microbiol. 2010;13:4–10.
Carabeo RA, Mead DJ, Hackstadt T. Golgi-dependent transport of cholesterol to the Chlamydia trachomatis inclusion. Proc Natl Acad Sci U S A. 2003;100:6771–6.
Derre I. Chlamydiae interaction with the endoplasmic reticulum: contact, function and consequences. Cell Microbiol. 2015;17:959–66.
Betts-Hampikian HJ, Fields KA. Disulfide bonding within components of the Chlamydia type III secretion apparatus correlates with development. J Bacteriol. 2011;193:6950–9.
Hybiske K, Stephens RS. Mechanisms of host cell exit by the intracellular bacterium Chlamydia. Proc Natl Acad Sci U S A. 2007;104:11430–5.
Todd WJ, Caldwell HD. The interaction of Chlamydia trachomatis with host cells: ultrastructural studies of the mechanism of release of a biovar II strain from HeLa 229 cells. J Infect Dis. 1985;151:1037–44.
Scidmore MA, Fischer ER, Hackstadt T. Restricted fusion of Chlamydia trachomatis vesicles with endocytic compartments during the initial stages of infection. Infect Immun. 2003;71:973–84.
Starnbach MN, Loomis WP, Ovendale P, et al. An inclusion membrane protein from Chlamydia trachomatis enters the MHC class I pathway and stimulates a CD8+ T cell response. J Immunol. 2003;171:4742–9.
Omsland A, Sager J, Nair V, Sturdevant DE, Hackstadt T. Developmental stage-specific metabolic and transcriptional activity of Chlamydia trachomatis in an axenic medium. Proc Natl Acad Sci U S A. 2012;109:19781–5.
Forhan SE, Gottlieb SL, Sternberg MR, et al. Prevalence of sexually transmitted infections among female adolescents aged 14 to 19 in the United States. Pediatrics. 2009;124:1505–12.
Sexually transmitted disease surveillance 2000. Atlanta: Centers for Disease Control and Prevention, 2001.
Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2017.2018.
Weinstock H, Berman S, Cates W Jr. Sexually transmitted diseases among American youth: incidence and prevalence estimates, 2000. Perspect Sex Reprod Health. 2004;36:6–10.
Bebear C, de Barbeyrac B. Genital Chlamydia trachomatis infections. Clin Microbiol Infect. 2009;15:4–10.
Garofalo R, Hotton AL, Kuhns LM, Gratzer B, Mustanski B. Incidence of HIV infection and sexually transmitted infections and related risk factors among very young men who have sex with men. J Acquir Immune Defic Syndr. 2016;72:79–86.
Torrone E, Papp J, Weinstock H. Prevalence of Chlamydia trachomatis genital infection among persons aged 14-39 years – United States, 2007-2012. MMWR Morb Mortal Wkly Rep. 2014;63:834–8.
Torrone E, Papp J, Weinstock H, Centers for Disease C, Prevention. Prevalence of Chlamydia trachomatis genital infection among persons aged 14–39 years--United States, 2007–2012. MMWR Morb Mortal Wkly Rep. 2014;63:834–8.
Harwell TS, Trino R, Rudy B, Yorkman S, Gollub EL. Sexual activity, substance use, and HIV/STD knowledge among detained male adolescents with multiple versus first admissions. Sex Transm Dis. 1999;26:265–71.
Oh MK, Smith KR, O'Cain M, Kilmer D, Johnson J, Hook EW 3rd. Urine-based screening of adolescents in detention to guide treatment for gonococcal and chlamydial infections. Translating research into intervention. Arch Pediatr Adolesc Med. 1998;152:52–6.
Oh MK, Cloud GA, Wallace LS, Reynolds J, Sturdevant M, Feinstein RA. Sexual behavior and sexually transmitted diseases among male adolescents in detention. Sex Transm Dis. 1994;21:127–32.
Chan PA, Robinette A, Montgomery M, et al. Extragenital infections caused by Chlamydia trachomatis and Neisseria gonorrhoeae: a review of the literature. Infect Dis Obstet Gynecol. 2016;2016:5758387.
Barbee LA, Dombrowski JC, Kerani R, Golden MR. Effect of nucleic acid amplification testing on detection of extragenital gonorrhea and chlamydial infections in men who have sex with men sexually transmitted disease clinic patients. Sex Transm Dis. 2014;41:168–72.
Gottlieb SL, Xu F, Brunham RC. Screening and treating Chlamydia trachomatis genital infection to prevent pelvic inflammatory disease: interpretation of findings from randomized controlled trials. Sex Transm Dis. 2013;40:97–102.
Tao G, Hoover KW, Kent CK. Chlamydia testing patterns for commercially insured women, 2008. Am J Prev Med. 2012;42:337–41.
Christiansen-Lindquist L, Tao G, Hoover K, Frank R, Kent C. Chlamydia screening of young sexually active, Medicaid-insured women by race and ethnicity, 2002-2005. Sex Transm Dis. 2009;36:642–6.
Hoover KW, Tao G, Nye MB, Body BA. Suboptimal adherence to repeat testing recommendations for men and women with positive Chlamydia tests in the United States, 2008-2010. Clin Infect Dis. 2013;56:51–7.
Hoover KW, Butler M, Workowski K, et al. STD screening of HIV-infected MSM in HIV clinics. Sex Transm Dis. 2010;37:771–6.
Scholes D, Stergachis A, Heidrich FE, Andrilla H, Holmes KK, Stamm WE. Prevention of pelvic inflammatory disease by screening for cervical chlamydial infection. N Engl J Med. 1996;334:1362–6.
Oakeshott P, Kerry S, Aghaizu A, et al. Randomised controlled trial of screening for Chlamydia trachomatis to prevent pelvic inflammatory disease: the POPI (prevention of pelvic infection) trial. BMJ. 2010;340:c1642.
Workowski KA, Bolan GA, Centers for Disease C, Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1–137.
LeFevre ML, Force USPST. Screening for Chlamydia and gonorrhea: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161:902–10.
Prevention CfDCa. Male Chlamydia consultation, March 28–29, 2006. Atlanta. 2007.
Force USPST. Screening for chlamydial infection: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2007;147:128–34.
Centers for Disease C, Prevention. Chlamydia screening among sexually active young female enrollees of health plans – United States, 2000–2007. MMWR Morb Mortal Wkly Rep. 2009;58:362–5.
Hoover K, Tao G, Kent C. Low rates of both asymptomatic chlamydia screening and diagnostic testing of women in US outpatient clinics. Obstet Gynecol. 2008;112:891–8.
Hoover K, Tao G. Missed opportunities for chlamydia screening of young women in the United States. Obstet Gynecol. 2008;111:1097–102.
Eugene JM, Hoover KW, Tao G, Kent CK. Higher yet suboptimal chlamydia testing rates at community health centers and outpatient clinics compared with physician offices. Am J Public Health. 2012;102:e26–9.
Meyers DS, Halvorson H, Luckhaupt S, Force USPST. Screening for chlamydial infection: an evidence update for the U.S. Preventive Services Task Force. Ann Intern Med. 2007;147:135–42.
Ryan GM Jr, Abdella TN, McNeeley SG, Baselski VS, Drummond DE. Chlamydia trachomatis infection in pregnancy and effect of treatment on outcome. Am J Obstet Gynecol. 1990;162:34–9.
Centers for Disease C, Prevention. Clinic-based testing for rectal and pharyngeal Neisseria gonorrhoeae and Chlamydia trachomatis infections by community-based organizations--five cities, United States, 2007. MMWR Morb Mortal Wkly Rep. 2009;58:716–9.
Kent CK, Chaw JK, Wong W, et al. Prevalence of rectal, urethral, and pharyngeal chlamydia and gonorrhea detected in 2 clinical settings among men who have sex with men: San Francisco, California, 2003. Clin Infect Dis. 2005;41:67–74.
Bernstein KT, Stephens SC, Barry PM, et al. Chlamydia trachomatis and Neisseria gonorrhoeae transmission from the oropharynx to the urethra among men who have sex with men. Clin Infect Dis. 2009;49:1793–7.
Marcus JL, Kohn RP, Barry PM, Philip SS, Bernstein KT. Chlamydia trachomatis and Neisseria gonorrhoeae transmission from the female oropharynx to the male urethra. Sex Transm Dis. 2011;38:372–3.
Marcus JL, Bernstein KT, Kohn RP, Liska S, Philip SS. Infections missed by urethral-only screening for chlamydia or gonorrhea detection among men who have sex with men. Sex Transm Dis. 2011;38:922–4.
Koedijk FD, van Bergen JE, Dukers-Muijrers NH, et al. The value of testing multiple anatomic sites for gonorrhoea and chlamydia in sexually transmitted infection centres in the Netherlands, 2006-2010. Int J STD AIDS. 2012;23:626–31.
Danby CS, Cosentino LA, Rabe LK, et al. Patterns of extragenital chlamydia and gonorrhea in women and men who have sex with men reporting a history of receptive anal intercourse. Sex Transm Dis. 2016;43:105–9.
Trebach JD, Chaulk CP, Page KR, Tuddenham S, Ghanem KG. Neisseria gonorrhoeae and Chlamydia trachomatis among women reporting extragenital exposures. Sex Transm Dis. 2015;42:233–9.
Schachter J, Moncada J, Liska S, Shayevich C, Klausner JD. Nucleic acid amplification tests in the diagnosis of chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sex Transm Dis. 2008;35:637–42.
Bernstein KT, Marcus JL, Nieri G, Philip SS, Klausner JD. Rectal gonorrhea and chlamydia reinfection is associated with increased risk of HIV seroconversion. J Acquir Immune Defic Syndr. 2010;53:537–43.
Pathela P, Braunstein SL, Blank S, Schillinger JA. HIV incidence among men with and those without sexually transmitted rectal infections: estimates from matching against an HIV case registry. Clin Infect Dis. 2013;57:1203–9.
Patel P, Bush T, Mayer K, et al. Routine brief risk-reduction counseling with biannual STD testing reduces STD incidence among HIV-infected men who have sex with men in care. Sex Transm Dis. 2012;39:470–4.
Austin EL, Irwin JA. Health behaviors and health care utilization of southern lesbians. Womens Health Issues. 2010;20:178–84.
Edwards A, Thin RN. Sexually transmitted diseases in lesbians. Int J STD AIDS. 1990;1:178–81.
Pinto VM, Tancredi MV, Tancredi Neto A, Buchalla CM. Sexually transmitted disease/HIV risk behaviour among women who have sex with women. AIDS. 2005;19(Suppl 4):S64–9.
Marrazzo JM, Koutsky LA, Handsfield HH. Characteristics of female sexually transmitted disease clinic clients who report same-sex behaviour. Int J STD AIDS. 2001;12:41–6.
Fethers K, Marks C, Mindel A, Estcourt CS. Sexually transmitted infections and risk behaviours in women who have sex with women. Sex Transm Infect. 2000;76:345–9.
Lindley LL, Kerby MB, Nicholson TJ, Lu N. Sexual behaviors and sexually transmitted infections among self-identified lesbian and bisexual college women. J LGBT Health Res. 2007;3:41–54.
Marrazzo JM. Barriers to infectious disease care among lesbians. Emerg Infect Dis. 2004;10:1974–8.
Eisenberg M. Differences in sexual risk behaviors between college students with same-sex and opposite-sex experience: results from a national survey. Arch Sex Behav. 2001;30:575–89.
Koh AS, Gomez CA, Shade S, Rowley E. Sexual risk factors among self-identified lesbians, bisexual women, and heterosexual women accessing primary care settings. Sex Transm Dis. 2005;32:563–9.
Lindley LL, Barnett CL, Brandt HM, Hardin JW, Burcin M. STDs among sexually active female college students: does sexual orientation make a difference? Perspect Sex Reprod Health. 2008;40:212–7.
Muzny CA, Sunesara IR, Martin DH, Mena LA. Sexually transmitted infections and risk behaviors among African American women who have sex with women: does sex with men make a difference? Sex Transm Dis. 2011;38:1118–25.
Singh D, Fine DN, Marrazzo JM. Chlamydia trachomatis infection among women reporting sexual activity with women screened in Family Planning Clinics in the Pacific Northwest, 1997 to 2005. Am J Public Health. 2011;101:1284–90.
Workowski KA. Centers for Disease Control and Prevention Sexually Transmitted Diseases Treatment Guidelines. Clin Infect Dis. 2015;61(Suppl 8):S759–62.
Aberg JA, Gallant JE, Ghanem KG, et al. Primary care guidelines for the management of persons infected with HIV: 2013 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2014;58:1–10.
Mayer KH, Bekker LG, Stall R, Grulich AE, Colfax G, Lama JR. Comprehensive clinical care for men who have sex with men: an integrated approach. Lancet. 2012;380:378–87.
Joesoef MR, Weinstock HS, Kent CK, et al. Sex and age correlates of Chlamydia prevalence in adolescents and adults entering correctional facilities, 2005: implications for screening policy. Sex Transm Dis. 2009;36:S67–71.
Lyss SB, Kamb ML, Peterman TA, et al. Chlamydia trachomatis among patients infected with and treated for Neisseria gonorrhoeae in sexually transmitted disease clinics in the United States. Ann Intern Med. 2003;139:178–85.
Stupiansky NW, Van Der Pol B, Williams JA, Weaver B, Taylor SE, Fortenberry JD. The natural history of incident gonococcal infection in adolescent women. Sex Transm Dis. 2011;38:750–4.
Brotman RM, Klebanoff MA, Nansel TR, et al. Bacterial vaginosis assessed by gram stain and diminished colonization resistance to incident gonococcal, chlamydial, and trichomonal genital infection. J Infect Dis. 2010;202:1907–15.
Dunne EF, Chapin JB, Rietmeijer CA, et al. Rate and predictors of repeat Chlamydia trachomatis infection among men. Sex Transm Dis. 2008;35:S40–4.
Gaydos CA, Wright C, Wood BJ, Waterfield G, Hobson S, Quinn TC. Chlamydia trachomatis reinfection rates among female adolescents seeking rescreening in school-based health centers. Sex Transm Dis. 2008;35:233–7.
Batteiger BE, Tu W, Ofner S, et al. Repeated Chlamydia trachomatis genital infections in adolescent women. J Infect Dis. 2010;201:42–51.
Fleming DT, Wasserheit JN. From epidemiological synergy to public health policy and practice: the contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex Transm Infect. 1999;75:3–17.
Workowski K. In the clinic. Chlamydia and gonorrhea. Ann Intern Med. 2013;158:ITC2–1.
Haggerty CL, Gottlieb SL, Taylor BD, Low N, Xu F, Ness RB. Risk of sequelae after Chlamydia trachomatis genital infection in women. J Infect Dis. 2010;201(Suppl 2):S134–55.
Marrazzo JM, Martin DH. Management of women with cervicitis. Clin Infect Dis. 2007;44(Suppl 3):S102–10.
Marrazzo JM, Handsfield HH, Whittington WLH. Predicting chlamydial and gonococcal cervical infection: implications for management of cervicitis. Obstet Gynecol. 2002;100:579–84.
Marrazzo J, Suchland R. Recent advances in understanding and managing Chlamydia trachomatis infections. F1000Prime Rep. 2014;6:s.
Bachmann LH, Richey CM, Waites K, Schwebke JR, Hook EW 3rd. Patterns of Chlamydia trachomatis testing and follow-up at a University Hospital Medical Center. Sex Transm Dis. 1999;26:496–9.
Geisler WM, Wang C, Morrison SG, Black CM, Bandea CI, Hook EW 3rd. The natural history of untreated Chlamydia trachomatis infection in the interval between screening and returning for treatment. Sex Transm Dis. 2008;35:119–23.
Hook EW 3rd, Spitters C, Reichart CA, Neumann TM, Quinn TC. Use of cell culture and a rapid diagnostic assay for Chlamydia trachomatis screening. JAMA. 1994;272:867–70.
Gaydos C, Maldeis NE, Hardick A, Hardick J, Quinn TC. Mycoplasma genitalium compared to chlamydia, gonorrhoea and trichomonas as an aetiological agent of urethritis in men attending STD clinics. Sex Transm Infect. 2009;85:438–40.
Taylor SN. Epididymitis. Clin Infect Dis. 2015;61(Suppl 8):S770–3.
Kong FY, Tabrizi SN, Fairley CK, et al. The efficacy of azithromycin and doxycycline for the treatment of rectal chlamydia infection: a systematic review and meta-analysis. J Antimicrob Chemother. 2015;70:1290–7.
Reinton N, Moi H, Olsen AO, et al. Anatomic distribution of Neisseria gonorrhoeae, Chlamydia trachomatis and Mycoplasma genitalium infections in men who have sex with men. Sex Health. 2013;10:199–203.
Barbee LA, Khosropour CM, Dombrowski JC, Manhart LE, Golden MR. An estimate of the proportion of symptomatic gonococcal, chlamydial and non-gonococcal non-chlamydial urethritis attributable to oral sex among men who have sex with men: a case-control study. Sex Transm Infect. 2016;92:155–60.
Mabey D, Peeling RW. Lymphogranuloma venereum. Sex Transm Infect. 2002;78:90–2.
White JA. Manifestations and management of lymphogranuloma venereum. Curr Opin Infect Dis. 2009;22:57–66.
Pallawela SN, Sullivan AK, Macdonald N, et al. Clinical predictors of rectal lymphogranuloma venereum infection: results from a multicentre case-control study in the U.K. Sex Transm Infect. 2014;90:269–74.
de Vrieze NH, de Vries HJ. Lymphogranuloma venereum among men who have sex with men. An epidemiological and clinical review. Expert Rev Anti Infect Ther. 2014;12:697–704.
Association of Public Health Laboratories. Laboratory diagnostic testing for Chlamydia trachomatis and Neisseria gonorrhoeae. January 13–15, 2009.
Centers for Disease C, Prevention. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae--2014. MMWR Recomm Rep. 2014;63:1–19.
Brook G. The performance of non-NAAT point-of-care (POC) tests and rapid NAAT tests for chlamydia and gonorrhoea infections. An assessment of currently available assays. Sex Transm Infect. 2015;91:539–44.
Gaydos CA, Van Der Pol B, Jett-Goheen M, et al. Performance of the cepheid CT/NG Xpert rapid PCR test for detection of Chlamydia trachomatis and Neisseria gonorrhoeae. J Clin Microbiol. 2013;51:1666–72.
Barbee LA, Tat S, Dhanireddy S, Marrazzo JM. Implementation and operational research: effectiveness and patient acceptability of a sexually transmitted infection self-testing program in an HIV care setting. J Acquir Immune Defic Syndr. 2016;72:e26–31.
Schachter J, Chernesky MA, Willis DE, et al. Vaginal swabs are the specimens of choice when screening for Chlamydia trachomatis and Neisseria gonorrhoeae: results from a multicenter evaluation of the APTIMA assays for both infections. Sex Transm Dis. 2005;32:725–8.
Doshi JS, Power J, Allen E. Acceptability of chlamydia screening using self-taken vaginal swabs. Int J STD AIDS. 2008;19:507–9.
van der Helm JJ, Hoebe CJ, van Rooijen MS, et al. High performance and acceptability of self-collected rectal swabs for diagnosis of Chlamydia trachomatis and Neisseria gonorrhoeae in men who have sex with men and women. Sex Transm Dis. 2009;36:493–7.
Steinhandler L, Peipert JF, Heber W, Montagno A, Cruickshank C. Combination of bacterial vaginosis and leukorrhea as a predictor of cervical chlamydial or gonococcal infection. Obstet Gynecol. 2002;99:603–7.
Hobbs MM, van der Pol B, Totten P, et al. From the NIH: proceedings of a workshop on the importance of self-obtained vaginal specimens for detection of sexually transmitted infections. Sex Transm Dis. 2008;35:8–13.
Hosenfeld CB, Workowski KA, Berman S, et al. Repeat infection with Chlamydia and gonorrhea among females: a systematic review of the literature. Sex Transm Dis. 2009;36:478–89.
Morrissey I, Salman H, Bakker S, Farrell D, Bebear CM, Ridgway G. Serial passage of Chlamydia spp. in sub-inhibitory fluoroquinolone concentrations. J Antimicrob Chemother. 2002;49:757–61.
Kohlhoff SA, Hammerschlag MR. Treatment of Chlamydial infections: 2014 update. Expert Opin Pharmacother. 2015;16:205–12.
Wang SA, Papp JR, Stamm WE, Peeling RW, Martin DH, Holmes KK. Evaluation of antimicrobial resistance and treatment failures for Chlamydia trachomatis: a meeting report. J Infect Dis. 2005;191:917–23.
Hocking JS, Kong FY, Timms P, Huston WM, Tabrizi SN. Treatment of rectal chlamydia infection may be more complicated than we originally thought. J Antimicrob Chemother. 2015;70:961–4.
Schwebke JR, Rompalo A, Taylor S, et al. Re-evaluating the treatment of nongonococcal urethritis: emphasizing emerging pathogens – a randomized clinical trial. Clin Infect Dis. 2011;52:163–70.
Kong FY, Tabrizi SN, Law M, et al. Azithromycin versus doxycycline for the treatment of genital chlamydia infection: a meta-analysis of randomized controlled trials. Clin Infect Dis. 2014;59:193–205.
Khosropour CM, Dombrowski JC, Barbee LA, Manhart LE, Golden MR. Comparing azithromycin and doxycycline for the treatment of rectal chlamydial infection: a retrospective cohort study. Sex Transm Dis. 2014;41:79–85.
Khosropour CM, Manhart LE, Colombara DV, et al. Suboptimal adherence to doxycycline and treatment outcomes among men with non-gonococcal urethritis: a prospective cohort study. Sex Transm Infect. 2014;90:3–7.
Lau A, Kong F, Fairley CK, et al. Treatment efficacy of azithromycin 1 g single dose versus doxycycline 100 mg twice daily for 7 days for the treatment of rectal chlamydia among men who have sex with men – a double-blind randomised controlled trial protocol. BMC Infect Dis. 2017;17:35.
Oliver A, Rogers M, Schillinger JA. The impact of prescriptions on sex partner treatment using expedited partner therapy for Chlamydia trachomatis Infection, New York City, 2014-2015. Sex Transm Dis. 2016;43:673–8.
Radovic A, Burstein GR, Marshal MP, Murray PJ, Miller E, Sucato GS. Adolescents’ attitudes toward expedited partner therapy for sexually transmitted infections. Sex Transm Dis. 2013;40:894–7.
Golden MR, Whittington WL, Handsfield HH, et al. Effect of expedited treatment of sex partners on recurrent or persistent gonorrhea or chlamydial infection. N Engl J Med. 2005;352:676–85.
Golden MR, Kerani RP, Stenger M, et al. Uptake and population-level impact of expedited partner therapy (EPT) on Chlamydia trachomatis and Neisseria gonorrhoeae: the Washington State community-level randomized trial of EPT. PLoS Med. 2015;12:e1001777.
Schillinger JA, Kissinger P, Calvet H, et al. Patient-delivered partner treatment with azithromycin to prevent repeated Chlamydia trachomatis infection among women: a randomized, controlled trial. Sex Transm Dis. 2003;30:49–56.
Kissinger P, Mohammed H, Richardson-Alston G, et al. Patient-delivered partner treatment for male urethritis: a randomized, controlled trial. Clin Infect Dis. 2005;41:623–9.
Gallo MF, Steiner MJ, Warner L, et al. Self-reported condom use is associated with reduced risk of chlamydia, gonorrhea, and trichomoniasis. Sex Transm Dis. 2007;34:829–33.
In-Iw S, Braverman PK, Bates JR, Biro FM. The impact of health education counseling on rate of recurrent sexually transmitted infections in adolescents. J Pediatr Adolesc Gynecol. 2015;28:481–5.
O'Connor EA, Lin JS, Burda BU, Henderson JT, Walsh ES, Whitlock EP. Behavioral sexual risk-reduction counseling in primary care to prevent sexually transmitted infections: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2014;161:874–83.
LeFevre ML, Force USPST. Behavioral counseling interventions to prevent sexually transmitted infections: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161:894–901.
Boekeloo BO, Schamus LA, Simmens SJ, Cheng TL, O’Connor K, D'Angelo LJ. A STD/HIV prevention trial among adolescents in managed care. Pediatrics. 1999;103:107–15.
Guilamo-Ramos V, Bouris A, Jaccard J, Gonzalez B, McCoy W, Aranda D. A parent-based intervention to reduce sexual risk behavior in early adolescence: building alliances between physicians, social workers, and parents. J Adolesc Health. 2011;48:159–63.
Jemmott JB 3rd, Jemmott LS, Braverman PK, Fong GT. HIV/STD risk reduction interventions for African American and Latino adolescent girls at an adolescent medicine clinic: a randomized controlled trial. Arch Pediatr Adolesc Med. 2005;159:440–9.
Kamb ML, Fishbein M, Douglas JM Jr, et al. Efficacy of risk-reduction counseling to prevent human immunodeficiency virus and sexually transmitted diseases: a randomized controlled trial. Project RESPECT Study Group. JAMA. 1998;280:1161–7.
Lafferty WE, Downey L, Shields AW, Holan CM, Lind A. Adolescent enrollees in Medicaid managed care: the provision of well care and sexual health assessment. J Adolesc Health. 2001;28:497–508.
Wimberly YH, Hogben M, Moore-Ruffin J, Moore SE, Fry-Johnson Y. Sexual history-taking among primary care physicians. J Natl Med Assoc. 2006;98:1924–9.
Goyal MK, Witt R, Hayes KL, Zaoutis TE, Gerber JS. Clinician adherence to recommendations for screening of adolescents for sexual activity and sexually transmitted infection/human immunodeficiency virus. J Pediatr. 2014;165:343–7.
DiClemente RJ, Sales JM, Danner F, Crosby RA. Association between sexually transmitted diseases and young adults’ self-reported abstinence. Pediatrics. 2011;127:208–13.
Datta SD, Sternberg M, Johnson RE, et al. Gonorrhea and chlamydia in the United States among persons 14 to 39 years of age, 1999 to 2002. Ann Intern Med. 2007;147:89–96.
Chiaradonna C. The Chlamydia cascade: enhanced STD prevention strategies for adolescents. J Pediatr Adolesc Gynecol. 2008;21:233–41.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kandiah, S., Ramchandani, M., Grieshaber, S. (2020). Chlamydia. In: Hussen, S. (eds) Sexually Transmitted Infections in Adolescence and Young Adulthood. Springer, Cham. https://doi.org/10.1007/978-3-030-20491-4_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-20491-4_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-20490-7
Online ISBN: 978-3-030-20491-4
eBook Packages: MedicineMedicine (R0)