
Abstract
In addition to being a favored diagnostic tool for structure and function, echocardiography is the noninvasive alternative to cardiac catheterization for the assessment of various hemodynamic parameters, including intracardiac pressures, cardiac output, vascular resistance, shunt fraction, and valvular lesions. An understanding of Doppler physics, the Bernoulli equation, imaging technique, and limitations of echocardiography are critical for its successful application. This chapter begins with a review of the basic principles of physics relevant to echocardiography. Using these principles, we demonstrate how to estimate intracardiac pressures, following the traveled path of the Swan–Ganz catheter: right atrium, right ventricle, pulmonary artery, and pulmonary artery wedge. Thereafter, we will apply fundamental concepts including the Doppler equation, Bernoulli principle, continuity equation, PISA, and other principles to assess specific valve lesions. Cases will be presented to reinforce concepts discussed in the text.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Echocardiography is a powerful, noninvasive imaging tool that can provide useful hemodynamic information to guide patient management. Intracardiac pressures, cardiac output, vascular resistance, shunt fractions, and valve lesions can be assessed by using a combination of two-dimensional imaging, color Doppler, pulse and continuous wave Doppler, and tissue Doppler. While echocardiography can provide data complementary to catheter-derived measurements and in some situations has even supplanted invasive monitoring, its application requires meticulous technique, an understanding of basic principles of physics, and an appreciation of potential limitations of the method.
Basic Physics of Echocardiography
Doppler Principle
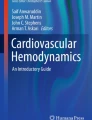
The Doppler principle explains that the frequency of a wave increases as the source of the wave moves toward an observer, while the frequency of a wave decreases as the source moves away from an observer [1]. The change in the frequency of the sound wave depends on the velocity of the moving object, the velocity of sound, and the angle at which the sound wave hits the object. Echocardiography extrapolates this principle of frequency shift to determine the velocity of blood flow in the heart. When a sound wave is transmitted from the transducer crystal at a given frequency, it is reflected by a red blood cell at a certain frequency back to the transducer (Fig. 11.1). If the red blood cell is moving toward the sound waves, the frequency will increase, but if the red blood cell is moving away from the sound wave, the frequency will decrease. The Doppler shift is the change in frequency between the transmitted sound and the reflected sound and is expressed in the following Doppler equation [2]:
where f 0 = transmitted frequency; f r = reflected frequency; θ = angle between the ultrasound beam and blood flow; v = velocity of red blood cells; and c = speed of ultrasound in blood (1540 m/s).

The Doppler principle and Bernoulli equation . Bottom right: The echo transducer sends ultrasound waves at a given frequency (f 0) to the heart, and the sound waves are reflected back to the transducer at a different frequency (f r). The difference between (f 0) and (f r) is the Doppler shift. As shown in the equation, the Doppler shift is directly proportional to the transmitted frequency (f 0), the cosine of the angle of incidence θ (angle between the ultrasound wave and vector of the red blood cell), and the velocity of the red blood cells, however, is inversely proportional to the speed of ultrasound in the medium (c). Rearrangement of the equation allows one to determine the velocity of the red blood cells. Top right: The Bernoulli equation enables one to determine the pressure gradient across a stenosis, in this case, a stenotic aortic valve. Flow accelerates just before and at the level of the stenosis. The velocity proximal to the stenosis is V 1, and the velocity distal to the stenosis is V 2. Based on certain assumptions (see text), the Bernoulli equation can be simplified to P1 − P2 = ΔP = 4(V 2)2. In this case, the peak gradient is 64 mmHg based on the peak velocity across the aortic valve (V 2) of 4 m/s. Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2011
Algebraic rearrangement of the equation allows one to solve for velocity:
Note that the number “2” in the equation results from the fact that there are actually two Doppler shifts: one when the sound wave sent from the transducer strikes the red blood cell, and the other when the wave reflected from the red blood cell is sent back to the transducer. Doppler echocardiography is highly angle-dependent. The angle should ideally be <20 ° which results in <10% underestimation of true flow velocity [2]. When the ultrasound beam is ideally oriented parallel to the direction of blood flow, that is, when the angle θ is 0 °, the equation is simplified since the cosine of 0 ° is 1. Using the simplified Bernoulli principle (Fig. 11.1), it follows that velocity can be used to estimate pressures.
Continuous Wave Versus Pulse Wave Doppler
Two forms of Doppler echocardiography are pulse wave (PW) Doppler and continuous wave (CW) Doppler. Pulse wave Doppler employs a single crystal that emits short bursts or pulses of ultrasound at a certain rate per second, known as the pulse repetition frequency (PRF), which is dependent on the depth of interrogation. These pulses are sent to a particular sampling location or depth, and the same crystal waits for the reflected frequency (Fig. 11.2a). Because the same crystal sends and receives the ultrasound wave, the maximum velocity that can be measured is limited by the time it takes to send and receive the wave. This is called the Nyquist limit, which is one-half the PRF. The PRF and the Nyquist limit are solely determined by the depth of the sample volume and not by the transducer frequency. The shallower the sample volume, the higher the PRF or number of pulses sent per second by the transducer. If the Doppler frequency shift is greater than the Nyquist limit, then the velocities above this limit are cut off the spectral Doppler profile and wrap around to the opposite direction, a phenomenon known as aliasing [1]. Anyone who has watched a wagon wheel in a Western movie appreciates this phenomenon. As the wagon starts to move away, the wheel appears to be moving clockwise. But as the wagon wheel picks up speed and exceeds the “Nyquist limit” of the movie camera, the wheel appears to be moving counterclockwise, which is the equivalent of aliasing. An example of aliasing in echocardiography can be found in Fig. 11.4c, in which PW is used to determine the right ventricular outflow tract (RVOT) velocity. Note that during diastole, the pulmonary regurgitation jet velocity exceeds the Nyquist limit of 1 m/s and wraps around (aliases) to the negative portion of the spectral Doppler profile. Therefore, PW is suited for measuring low velocity flow (<2 m/s) at specific locations in the heart, such as the left ventricular outflow tract (LVOT), right ventricular outflow tract (RVOT), mitral inflow, tricuspid inflow, and hepatic vein inflow. PW has the property of “range specificity” in that it provides information at a specific location. Figure 11.2a shows PW of the mitral inflow with sample volume at the leaflet tips, demonstrating the three phases of diastole: early filling (E wave), diastasis, and late filling (A wave).

Various forms of Doppler in echocardiography. (a) Pulse wave (PW) Doppler of the mitral inflow with the sample volume placed at the leaflet tips. In PW, the same transducer crystal sends and receives waves to determine the Doppler shift at a particular sample volume, marked by the white arrow. Because PW obtains information about a particular location, it is said to have “range specificity or range resolution,” but it is prone to aliasing. Note that in diastole there is early filling (E wave) and Late Filling (A wave). Diastasis is known as the period between the E and the A wave. The E velocity is 68 cm/s. (b) Continuous wave (CW) Doppler across the aortic valve. In CW, one crystal sends sound waves continuously and another crystal receives the sound waves. Because the CW profile represents all the velocities along the path of interrogation (represented by the dotted line), the peak velocity cannot be localized based on the CW signal alone. This phenomenon is known as “range ambiguity.” The y axis is velocity and the x axis is time, and therefore the area under the curve is the velocity time integral (VTI), or the aortic valve VTI, in units of distance (cm). In this example, the peak velocity is 1.3 m/s and the Aortic Valve VTI is 22 cm. (c) Tissue Doppler of the mitral annulus characterizes annular velocities, with the corresponding annular e′ and a′ waves. These waves correspond temporally with the E and A waves of the mitral inflow. Because E = 68 cm/s and e′ = 13 cm/s, the ratio E/e′ is roughly 5, suggesting normal PCWP pressures. (d) Color Doppler in which the color pixels represent the mean velocity vector at a particular location
Because continuous wave (CW) Doppler employs two crystals, one continuously emitting ultrasound waves and the other continuously receiving reflected waves, it does not fall under the Nyquist limitation (Fig. 11.2b). This allows for interrogation of higher velocities without aliasing. In CW, all the velocities along the ultrasound beam are recorded, rather than the velocities at one particular location. The peak velocity cannot be localized based on the CW signal alone, a phenomenon known as “range ambiguity.” CW is used to assess gradients in aortic stenosis and mitral stenosis, peak mitral regurgitation velocity, peak tricuspid regurgitation velocity, and intracardiac shunt velocity.
Finally, tissue Doppler is a specialized form of PW that allows the interrogation of myocardial and annular velocities by focusing on lower velocities of higher amplitude with a high frame rate (Fig. 11.2c). Tissue Doppler imaging is employed in the estimation of intracardiac pressures, quantification of wall motion in stress echo, detection of diastolic dysfunction, and intraventricular dyssynchrony, among other applications.
Color Doppler
Color Doppler provides a visual representation of intracardiac flow by translating the velocity vector into color: red and yellow represent flow moving toward the transducer while blue hues represent flow moving away from the transducer (Fig. 11.2d). Note that in the color scale which appears to the right of Fig. 11.2d, the darker the color shade, the closer to zero the velocity becomes, with black representing 0 m/s. The color image is constructed by the summation of multiple scanning lines which translates Doppler shifts into mean velocity, and then the mean velocity into a color based on the color scale. To determine real-time, accurate blood velocities along the path of multiple scanning lines, the transducer must rapidly send multiple groups of pulses or “packets” with pulse wave Doppler. While having more pulses per “packet” increases the accuracy of velocity measurements, this occurs at the expense of temporal resolution because more time is needed to acquire the information from the pulses. Because color Doppler relies on PW, if the velocity of flow is greater than the Nyquist limit, color aliasing occurs, in which color may reverse from blue to yellow, for example.
Bernoulli Equation
The Bernoulli equation has applications for echocardiography-based hemodynamic assessment. It is used to calculate the gradient across a stenosis, a regurgitant valve, or a septal defect between two cardiac chambers, and it consists of three components: convective acceleration, flow acceleration, and viscous friction (Fig. 11.1) [3].
where P1 = pressure proximal to stenosis; P2 = pressure distal to the stenosis, ρ = mass density of blood (1.06 × 103 kg/m3); V 1 = velocity at proximal location; V 2 = velocity at distal location; ds = acceleration distance; and R = viscous resistance.
Convective acceleration is the increase in kinetic energy that corresponds to the pressure drop across the orifice, and is analogous to the conversion of potential energy to kinetic energy that occurs when an object falls by gravity [3]. The flow acceleration component describes the pressure drop required to accelerate the blood by overcoming the blood’s inertial forces. Finally, the viscous friction component describes the frictional, viscous force that results from neighboring blood cells moving at different velocities.
There are some features of blood flow in the human heart that allow for simplification of the Bernoulli equation. First, the viscous friction term is negligible because the velocity profile of blood through a stenotic valve is relatively flat (little variation in blood velocity and therefore little friction), as well as because orifice diameters in the heart are relatively large, minimizing the effect of friction at the center of the orifice. In addition, previous studies have indicated that in most clinical situations the flow acceleration component is negligible [3]. In single, stenotic lesions, the proximal velocity term V 1 is typically small (<1 m/s) and can be ignored. Therefore, because in most clinical scenarios the viscous friction, flow acceleration, and V 1 components are negligible, the Bernoulli equation is simplified to P1 − P2 = ΔP = 4(V 2)2 (Fig. 11.1).
Intracardiac Pressures
The guide through echocardiographic assessment of various cardiac chamber pressures will follow the same sequence as during a diagnostic right heart catheterization, beginning with the right atrium. A summary of the equations discussed is presented at the end of the chapter (Fig. 11.10).
Right Atrium
Right atrial pressure is reflected in the size of the inferior vena cava (IVC), its response to changes in intrathoracic pressure, and the hepatic vein Doppler profile. Interrogation of the IVC by transthoracic echocardiography can be performed with the subcostal view (Fig. 11.3a, c). An IVC diameter ≤2.1 cm that collapses >50% with sniffing (which causes an acute drop in intrathoracic pressure resulting in decreased venous return) suggests a normal RA pressure of 3 mmHg (range 0–5 mmHg) [4]. An IVC diameter >2.1 cm that collapses <50% with a sniff suggests a high RA pressure around 15 mmHg (range 10–20 mmHg). IVC profiles that do not fit into these two categories (i.e., IVC ≤ 2.1 cm but <50% collapse or IVC > 2.1 cm but >50% collapse) can be designated as an intermediate RA pressure of 8 mmHg. Other additional parameters such as hepatic vein profile can be used to further refine this estimated pressure. Young healthy adults may have dilated IVCs but normal RA pressure, and estimation of RA pressure using the IVC index may not be reliable in patients who are intubated [4]. An additional estimate of right atrial pressure is derived from the ratio of the tricuspid inflow diastolic E wave velocity and the right ventricular annular e′ velocity, which is the right-sided correlate of estimating left atrial pressure by tissue Doppler. A ratio of E/e′ > 6 is suggestive of high right atrial pressures. This method can be used in situations where IVC measurements are unobtainable or inaccurate [5].

Right-sided pressures. (a) M-mode through the IVC from the subcostal view. Note that the IVC size is <2.1 cm and collapses greater than 50%, suggesting normal right atrial pressure (0–5 mmHg). (b) Pulse wave (PW) Doppler of the hepatic vein showing normal hepatic vein flow. Note that there are two antegrade waves (S and D) and one retrograde wave (a reversal). The representative portions on the JVP waveform are shown (S corresponds to the x descent, and D corresponds to the y descent). The onset of the S wave corresponds to the onset of the QRS (isovolumic contraction), although the peak occurs in mid to late systole. In this example, the velocity of the S wave is larger than the D wave, indicating normal right atrial pressures. (c) A plethoric IVC greater than 2.1 cm in width which does not collapse, suggesting a right atrial pressure between 10 and 20 mmHg. (d) Systolic flow reversal in the hepatic veins in severe tricuspid regurgitation. Notice that the S wave is above the baseline, indicating flow reversal. This corresponds to the blunted x descent and tall v wave in the JVP waveform
Because the hepatic vein drains into the IVC, which then drains into the RA, the hepatic vein Doppler profile can provide complementary information regarding right atrial and ventricular hemodynamics. The hepatic vein profile consists of two main antegrade flow waves (systolic (S) and diastolic (D) waveforms) and a retrograde atrial wave (a) (Fig. 11.3b). The S, D, and a waves correspond to the x, y, and a waves of the jugular venous pressure waveform, respectively. Flow in the hepatic vein is sensitive to respiration, with increasing antegrade flow during inspiration and decreasing flow during expiration. With normal RA pressure, there is a predominance of the s wave in the antegrade waveform, whereas with elevated RA pressure, because the pressure gradient between the RA and the hepatic vein is lower, the s wave is blunted and the d wave predominates. More quantitatively, a ratio of the s wave velocity divided by the sum of the s and d wave velocity [V s /(V s + V d )] less than 55% is highly correlated with an elevated RA pressure [6]. In addition, in severe tricuspid regurgitation, there may even be systolic wave reversal, which is the echocardiographic equivalent of the loss of the x descent in the jugular venous waveform (Fig. 11.3d). In pulmonary hypertension, there may be prominent flow reversal during atrial systole (prominent a wave) due to high pulmonary pressures transmitting back to the atrium during diastole. Utilizing the ECG to accurately differentiate systolic flow reversal in the hepatic vein (which should occur coincident with isovolumic contraction) from a prominent (a) wave can be key to avoiding misinterpretation of quite different hemodynamic conditions.
Right Ventricle
In the absence of tricuspid stenosis, the right ventricular end-diastolic pressure should equal the RA pressure as estimated from the IVC measurement. If tricuspid regurgitation (TR) is present, the peak velocity (v TR) measured at end-expiration can be used to estimate the pressure gradient between the right ventricle and right atrium during systole (ΔP = 4V TR 2) (Fig. 11.4a). This pressure gradient can be added to the RA pressure to estimate the right ventricular systolic pressure (RVSP = RA + 4V TR 2). A TR velocity greater than 2.8–2.9 cm/s, in the setting of a normal RA pressure (0–5 mmHg), corresponds roughly to an RVSP of 36 mmHg, which indicates the presence of mild pulmonary hypertension [4].

Pulmonary pressures and signs of pulmonary hypertension. (a) The right ventricular systolic pressure can be estimated from the peak tricuspid regurgitation velocity obtained in the right ventricular inflow view (see Question 1). (b) The continuous wave (CW) Doppler profile of the pulmonary regurgitation jet. The early peak velocity can be used to determine the mean pulmonary artery (PA) pressure by the following formula: Mean PA Pressure = 4v EarlyDPR 2. In this case, early pulmonary regurgitation (PR) jet velocity is 3.9 m/s and the end-diastolic PR velocity is 1.9 m/s. Therefore, the mean PA pressure is roughly 39 mmHg. Also, the pulmonary artery end-diastolic pressure (PAEDP) can be determined from the end-diastolic velocity and estimated right atrial (RA) pressure: PAEDP = RA + 4v EDPR 2 (see Question 2). Note that in pulmonary hypertension, there is absence of the typical end-diastolic dip in the pulmonary regurgitation CW profile that normally corresponds to atrial systole. (c) The sample volume is in the RVOT, just below the pulmonic valve. In pulmonary hypertension, there is a steep slope in early systole (acceleration phase becomes shorter, upper left corner) and there can be a mid-systolic dip in the RVOT profile (yellow stars), due to high afterload. A simplified formula to calculate the mean pulmonary artery pressure (MPAP) is MPAP = 80 − 0.5 (acceleration time (ms)). Acceleration time is roughly 90 ms, yielding a MPAP of 35 mmHg. (d) Note the D-shaped septum during systole, suggestive of RV pressure overload
In cases of severe TR, in which the tricuspid valve is essentially “wide-open” during systole and there is no longer a fixed orifice with a significant pressure drop across the orifice, the RVSP may be underestimated. This is due to the fact that the flow acceleration (inertance) component of the Bernoulli equation is no longer negligible (a pressure drop must occur to overcome the inertance of the large volume of blood), while the convective flow component is less important (large orifice). Therefore, the simplified Bernoulli equation, which includes only the convective component, typically underestimates the RVSP in this scenario [4, 7].
If there is no RVOT obstruction or pulmonary stenosis, then the RVSP should be equal to the pulmonary artery systolic pressure (PASP). In the presence of pulmonary stenosis, because the peak gradient across the pulmonary valve during systole represents the pressure drop from the RV to the pulmonary artery (PA), the PASP can be derived from subtracting the peak gradient across the pulmonary valve during systole (obtained by CW) from the RVSP obtained from the TR jet [8].
Pulmonary Artery
As stated above, the PASP is equal to the right ventricular systolic pressure in the absence of RVOT obstruction. The end-diastolic pressure gradient between the pulmonary artery and the right ventricle is extrapolated from the end-diastolic velocity of the pulmonary regurgitation jet (ΔP = 4V PRed 2) (Fig. 11.4b). Because this jet represents the difference between pulmonary artery end-diastolic pressure (PAEDP) and RVEDP (i.e., ΔP = 4V PRed 2 = PAEDP − RVEDP), and RVEDP equals RA pressure in the absence of tricuspid stenosis, it follows by algebraic manipulation that PAEDP = RA + 4V EDPR 2 [9]. Also, the mean PA pressure can be estimated from the peak pulmonary regurgitation jet velocity (Mean PA Pressure = 4V EarlyDPR 2) or the RVOT flow measured by PW Doppler using the formula 80 − 0.5 ∗ (pulmonic acceleration time(ms)) (Fig. 11.4c) [10]. These formulae can be useful when TR velocity signal is weak and unreliable. Estimation of pulmonary vascular resistance can be made by determining the ratio of the Peak TR velocity and the RVOT VTI (right ventricular outflow tract velocity time integral) in the following formula [11]:
Echocardiographic signs of pulmonary hypertension include a D-shaped left ventricle, loss of the atrial systolic dip in the pulmonary regurgitation jet, and a mid-systolic decrease in the pulmonary outflow velocity (Fig. 11.4).
Pulmonary Capillary Wedge/Left Atrial Pressure
One method of estimating the left atrial (LA) pressure is to determine the peak mitral regurgitation velocity (V MR), from which one can derive the pressure gradient between the left ventricle (LV) and LA (LV systolic pressure − LA pressure = 4V MR 2) [12]. Because the LV systolic pressure equals the systolic blood pressure (SBP) in the absence of LVOT obstruction, the LA pressure = SBP − 4V MR 2. A more common method of estimating the left atrial pressure is to determine the ratio of the mitral inflow E velocity to septal mitral annular velocity (e′), or E/e′ [13]. An E/e′ ratio of >15 is highly correlated with a pulmonary capillary wedge pressure (PCWP) >20, while an E/e′ ratio less than 8 corresponds to a normal PCWP [13]. This method is valid for patients with normal and abnormal systolic function. Tissue Doppler-derived estimates of PCWP can be used in patients with atrial fibrillation as well. However, in patients with constriction the exaggerated e′ velocity, which corresponds to the rapid y descent on JVP waveform, yields a low E/e′ ratio in spite of the fact that the left atrial pressures are elevated. This is the so-called annulus paradoxus [14].
Finally, in patients with aortic insufficiency, because the end-diastolic velocity of the aortic regurgitation jet (\( 4{V}_{\mathrm{AI}}^2 \)) represents the pressure gradient between the aorta (diastolic blood pressure or DBP) and the LV end-diastolic blood pressure (LVEDP), one can estimate the LVEDP using the following formula: LVEDP = DBP − \( 4{V}_{\mathrm{EDAI}}^2 \). Measurement error inherent with sphygmomanometric readings provides the primary limitation of this method. In the case of severe acute AI, where the end-diastolic velocity of the aortic insufficiency jet approaches zero, the LVEDP approaches the DBP.
Cardiac Output and System Vascular Resistance
The flow rate through a vessel is the product of the cross-sectional area of the vessel and the velocity of blood. However, because velocity varies over time throughout the cardiac cycle due to pulsatility, one cannot take an instantaneous velocity to measure overall flow rate. Rather, an integral of the velocities over time, called the VTI from the Doppler profile, is used to characterize integrated velocity in a given time period to determine flow (volume), rather than flow rate (volume/time) (Fig. 11.5a, b). VTI is essentially a measure of stroke distance. When the VTI (distance) is multiplied by the cross-sectional area (distance squared), the product is a volume (distance cubed). Therefore, stroke volume of the left ventricle can be estimated by multiplying the cross-sectional area of the LVOT (πr 2 = π(D/2)2 = πD 2/4 = D 2 ∗ 0.785, where r is radius and D is diameter) obtained in the parasternal long axis view and multiplying it by the VTI of the PW Doppler profile obtained in the apical long axis view (Fig. 11.5a). The PW cursor is typically placed about 0.5–1 cm below the valve to obtain a laminar flow curve. It is important to measure the PW Doppler profile at the same location as the measured cross-sectional area to maintain accuracy. This stroke volume can be multiplied by the heart rate to give an estimated cardiac output (in the absence of significant aortic regurgitation). If there is no regurgitation or intracardiac shunts, then the stroke volume through the tricuspid, pulmonary, mitral, and aortic valves should be equivalent, and therefore, the principle of multiplying the cross-sectional area of these valves by the VTI of flow across the valves can be applied throughout the heart. Practically speaking, however, stroke volume is typically measured in the LVOT.

Stroke volume and aortic valve area (AVA) calculation using the continuity equation. (a) Based on the continuity equation, the flow through the left ventricular outflow tract (LVOT), or the volume of the blue cylinder, must equal the flow through the aortic valve, or the volume of the red cylinder. The stroke volume (represented by the blue cylinder) is estimated by multiplying the LVOT area by the LVOT VTI. The LVOT area is obtained using the equation Area = πr 2 = (Diameter)2∗0.785, with the diameter measured in the parasternal long axis view. Because the LVOT diameter in this case is 1.9 cm, the LVOT area is 2.84 cm2. From the apical 5 chamber or apical long axis view, the LVOT VTI is obtained, which in this case is 28.1 cm (bottom right and (b)). Therefore, the stroke volume = 28.1 cm∗2.84 cm2 = 79.8 cm3. The product of the stroke volume and the heart rate (SV∗HR) can give an estimate of cardiac output. The volume of the red cylinder is the product of the AVA and the AV VTI (c, d). Because the volume of the blue cylinder (LVOT Area∗LVOT VTI) must equal the volume of the red cylinder (AVA∗AV VTI) to satisfy the continuity equation, it follows that AVA = [LVOT VTI ∗ (LVOT diameter)2 ∗ 0.785]/[AV VTI] = Stroke volume/AV VTI (see Question 3). (b) Pulse wave Doppler Sample volume is placed just below the aortic valve in the 5 chamber view, and the LVOT VTI is traced. (c) Continuous wave Doppler measures the highest velocity along its path to estimate the peak and mean gradient across the aortic valve. The peak and mean gradients are 95/55 mmHg from the 5 chamber view, which is an underestimation of peak flow in this particular patient. Multiple views are necessary to obtain the highest, most representative jet velocity, as seen in (d). Right sternal border view obtains peak and mean gradients of 119/74 mmHg, higher than the peak gradient of 95 mmHg from the apical 5 chamber view
If a left to right shunt is present (i.e., ASD or VSD), then it is clinically relevant to estimate the severity of the shunt by determining the ratio of pulmonary blood flow (Q p) to systemic blood flow (Q s). Figure 11.6 shows an example of a secundum ASD with left to right flow. Systemic stroke volume is measured by multiplying the LVOT area (D 2∗0.785) by the LVOT VTI from the parasternal long axis views and the apical long axis views, respectively. The pulmonary stroke volume is measured by multiplying the RVOT Area by the RVOT VTI, measured in the basal short axis view across the pulmonary valve. The ratio of Q p/Q s, which equals [(RVOT VTI) (RVOT D 2∗0.785)]/[(LVOT VTI) (LVOT D 2∗0.785)], gives an estimate of the shunt fraction (Fig. 11.6). The term 0.785 cancels, and the ratio simplifies to (RVOT VTI) (RVOT D 2)/(LVOT VTI) (LVOT D 2). A ratio greater than 1.5 is considered a significant left to right shunt.

Shunt calculation in a patient with a secundum atrial septal defect (ASD). (a) Color flow Doppler demonstrates left to right flow across the ASD in this subcostal view. (b) Pulse wave Doppler at the level of the ASD confirms that there is left to right continuous flow. During peak systole, based on the velocity of 1.2 m/s, the pressure gradient between the right atrium (RA) and the left atrium (LA) is 4v 2 = 4(1.2)2 = 5.8 mmHg. The RA pressure was estimated at 10 mmHg, so the LA pressure during systole is estimated at 15.8 mmHg (LA = RA + 4v 2). (c) Measurement of systemic flow (Q s) based on the LVOT area and LVOT VTI (pulse wave Doppler from the apical 5 chamber view, right upper corner). (d) Measurement of pulmonary flow (Q p) based on the RVOT area and the RVOT VTI (pulse wave Doppler from the basal short axis view, right upper corner). The Q p/Q s or shunt fraction is 1.3:1 (see Question 4 for calculation of Q p , Q s , and shunt fraction)
Just as pulmonary vascular resistance correlates with the TR velocity/RVOT VTI, systemic vascular resistance (SVR) correlates relatively well with MR velocity/LVOT VTI. A ratio of MR velocity/LVOT VTI > 0.27 has a relatively high sensitivity and specificity for SVR > 14 Woods units [15].
Valve Disease
It is important to recognize that an integrated approach using multiple echocardiographic methods of analysis and clinical context to determine severity of valve lesions is crucial, rather than relying on one specific measurement.
Aortic Stenosis
Echocardiography is currently the standard method to evaluate aortic valve stenosis. Application of the continuity equation is central to the calculation of aortic valve area (AVA) . Based on the conservation of mass, the flow in the left ventricular outflow tract (LVOT) should be equal to the flow through the aortic valve orifice. First, one must determine the flow in the LVOT, or the stroke volume, by multiplying the cross-sectional area of the LVOT by the LVOT VTI determined by PW Doppler in the apical long axis or 5 chamber view (Fig. 11.5a, b). The PW sample volume should be located in the LVOT beneath the valve, and a crisp laminar Doppler signal with no contamination from the pre-stenotic flow acceleration should be sought. This is typically 0.5–1.0 cm from the aortic valve. The LVOT diameter should be measured from the septum to the anterior mitral leaflet in mid-systole, roughly 0.5–1.0 cm from the aortic valve in the parasternal long axis view to approximate the location where the PW was measured in the other echocardiographic view [16]. This flow should equal the product of the cross-sectional area of the aortic valve (AVA) and the AV VTI as determined by CW Doppler, typically the highest VTI obtained from a given view (suprasternal, apical, right parasternal) (Fig. 11.5c, d). The volume of blood in the cylinder in the LVOT (blue cylinder) must equal the volume of blood in the cylinder at the aortic valve (red cylinder) to not violate the law of mass conservation. The AV VTI obtained by CW Doppler is highly dependent on technique and the ability to obtain a good signal that is parallel to flow. Occasionally the right parasternal approach is used to obtain the highest gradient (Fig. 11.5d).
Based on the continuity equation:
Rearrangement yields [17] (Fig. 11.5):
This equation gives a reliable estimate of the AVA; less than 1.0 cm2 is considered severe aortic stenosis [16, 18]. Because the LVOT diameter is squared and measurements can vary, this is the greatest source of error in the formula.
The AVA is just one method among many to assess severity of aortic stenosis. Other methods include identifying the peak and mean gradient across the aortic valve, peak velocity across the aortic valve, and dimensionless index [17]. The peak velocity across the aortic valve is obtained from the CW Doppler profile, from which the peak gradient is calculated (from the peak velocity using ΔP = 4V 2), and the mean gradient is calculated by averaging the instantaneous gradients during the ejection period [17]. A mean gradient >40 mmHg is considered severe. Echocardiographic assessment of peak gradient provides the instantaneous gradient between the LV and the aorta, which is different from cardiac catheterization in which often a peak to peak gradient is reported, a less physiologic value. Importantly, the mean gradient on cardiac catheterization correlates well with the Doppler-derived mean gradient. Table 11.1 shows the stages of severity of aortic stenosis based on the AHA/ACC 2014 Valve Guideline Update [16].
Although the peak velocity and estimated AVA are usually concordant (i.e., either velocity >4 m/s and AVA <1.0 cm2 or velocity <4 m/s and AVA >1.0 cm2), there may be scenarios in which the jet velocity and AVA may be discordant. In the case of velocity >4 m/s and AVA >1.0 cm2, possibilities include a high stroke volume, concomitant moderate-to-severe aortic regurgitation, and a large body size. In the case of velocity <4 m/s and AVA <1.0 cm2, possibilities include low stroke volume, severe concomitant mitral regurgitation, and small body size [16]. In either situation, the peak velocity is the better predictor of clinical outcome, and it is suggested that it be used to determine valve stenosis severity [16].
In patients who have left ventricular dysfunction (LVEF <40%) with concomitant aortic stenosis, the calculated AVA may be severe (<1.0 cm2), but the mean gradient may not be severe (<30–40 mmHg). It is important to then determine if the aortic stenosis is truly severe and causing left ventricular dysfunction, which would imply improved left ventricular function with valve replacement, or if the aortic stenosis is only moderate in the presence of LV dysfunction from another cause (i.e., coronary disease, non-valvular cardiomyopathy, etc.), in which the perceived small AVA is related to the inability of the left ventricle to generate the necessary valve opening forces (pseudostenosis). In the latter scenario, valve replacement would not be expected to improve left ventricular dysfunction. Low-dose dobutamine stress protocols (described in detail elsewhere [16]) can distinguish the two clinical scenarios. Recall from the continuity equation that the AVA is proportional to the LVOT VTI/AV VTI. If the patient truly has severe aortic stenosis, with the administration of dobutamine, the LVOT VTI and AV VTI should increase proportionally due to increased flow across a fixed, stenotic orifice, so the AVA should remain relatively unchanged. However, if the aortic stenosis only appears severe because of concomitant left ventricular dysfunction, dobutamine infusion will increase the LVOT VTI without a concomitant increase in AV VTI because of improved valve opening, thereby resulting in an increased calculated AVA. It follows that if the AVA increases above 1.0 cm2 with dobutamine infusion, it is not likely to be severe aortic stenosis. Severe AS is suggested by a peak jet velocity >4.0 m/s provided that the valve area does not increase to >1.0 cm2 [16]. In addition, the presence of contractile reserve (increase in EF or SV ≥ 20%) during dobutamine stress predicts a lower mortality rate (<10%) with AVR than if contractile reserve is absent (>30%) [19].
The velocity ratio, also known as the dimensionless index, which is flow independent, is the ratio of the LVOT peak velocity and the AV peak velocity (can also use VTI ratio). A velocity index <0.25 is considered severe. This is used to compare aortic stenosis severity over time in patients who may have different loading conditions.
Accurate estimation of aortic stenosis severity depends on meticulous technique to obtain both an accurate LVOT diameter assessment, as well as the highest velocity jet which may require multiple echocardiographic views. In general, inaccuracies in measuring gradients by echocardiography typically err on the side of underestimation. However, there are two situations in which echocardiography may overestimate severity of stenosis. First, as stated earlier, the peak gradient estimated by the simplified Bernoulli equation ignores the velocity in the LVOT (V 1) as it is usually very small (<1 m/s). Scenarios in which the proximal velocity is >1.5 m/s or the peak velocity is <3 m/s, the flow velocity and gradient may be overestimated since the V 1 is ignored. Therefore, a more accurate estimate of peak gradient across the valve is \( \varDelta P=4\left({V}_2^2-{V}_1^2\right) \) [16]. Another scenario in which the stenosis severity may be overestimated is the pressure recovery phenomenon. This occurs when some of the potential energy which was converted to kinetic energy at the level of the aortic stenosis is converted back to potential energy as flow decelerates (i.e., increasing pressure distal to the valve in the aorta). This pressure recovery is typically negligible, except in the case of small aortas with gradual widening after the stenosis (typically less than 3 cm in diameter). With larger aortas, much of the kinetic energy is converted to heat due to turbulence and viscous friction, so pressure recovery is not an issue [16]. Pressure recovery can be quantitatively calculated as ΔP = 4V 2 ∗ 2(AVA/aorta area) ∗ (1 − AVA/Aorta area). As can be seen by the equation, if the AVA is small, and the aorta area is large, the AVA/aorta area ratio is small, and pressure recovery is minimal [16].
One collateral method to confirm the pressure gradient across the LVOT or aortic valve is to assess the peak mitral regurgitation velocity. As described previously, LV systolic pressure − LA pressure = 4V MR 2. If the LA pressure is estimated to be between 10 and 20 mmHg, then the LV systolic pressure can be estimated by 10–20 mmHg + 4V MR 2. If the SBP is known, then the difference between the estimated LV systolic pressure and SBP approximates the peak pressure gradient across the LVOT or aortic valve.
Mitral Stenosis
The most common cause of mitral stenosis (MS) is commissural fusion as a result of rheumatic fever. Several echocardiographically derived measurements can be used to assess mitral stenosis, including pressure gradient, pressure half-time, continuity equation, proximal isovelocity surface area (PISA) method, and planimetry. Although planimetry may well provide the most accurate measurement of the mitral valve area (MVA) provided that the images are acquired at leaflet tip level and are a true on-axis view, this section will focus on the pressure gradient, pressure half-time, and continuity equation to assess the valve area. PISA method and planimetry are discussed in detail in another reference [16]. Peak and mean pressure gradients across the mitral valve in diastole are measured by CW from the apical 4 chamber view (Fig. 11.7). It is essential to interrogate the mitral valve during a regular rhythm and normal heart rate (60–80 bpm). If the patient is in atrial fibrillation, then several cardiac cycles (6–8) should be averaged. Mean gradient is preferred to the peak gradient, since the peak gradient may be influenced by mitral regurgitation, atrial compliance, and left ventricular diastology. One cause of a very high peak gradient out of proportion to the mean gradient, for example, is severe mitral regurgitation. While pressure gradients are important parameters in the assessment of mitral stenosis severity, they are highly influenced by heart rate, cardiac output, and mitral regurgitation [16]. Mean pressure gradients supportive of mild, moderate, and severe MS are <5 mmHg, 5–10 mmHg, and >10 mmHg, respectively [20].

Assessment of mitral stenosis. (a) Continuous wave Doppler across the mitral valve yields the peak and mean gradient (14/7 mmHg). Given the irregular heart rhythm, 6–8 beats are measured and averaged to obtain the peak and mean gradient. (b) The pressure half-time (PHT) is the time for the pressure gradient to decrease by 50%, and is equal to 0.29∗Deceleration time. Again, multiple beats are averaged (6–8) to obtain the PHT of 214 ms. The mitral valve area (MVA) is estimated by the following empiric equation: MVA = 220/PHT, giving a MVA of 220/214, or 1.0 cm2, by the PHT method. (c) Calculation of MVA using the continuity equation. The flow across the mitral valve must equal the flow across the aortic valve, and therefore, MVA ∗ MV VTI = LVOT area ∗ LVOT VTI. In this case, the LVOT diameter is 1.9 cm, the LVOT VTI is 20 cm, and the MV VTI is 56.4 cm. Therefore, the calculated MV area is 1.0 cm2. Note that the MV VTI is measured using CW and the LVOT VTI is measured using PW in this situation. (d) Planimetry is another method of estimating the MVA. Note the commissural fusion and “fish-mouth” appearance of the mitral opening, characteristic of rheumatic mitral valve disease. In this example, planimetry yields a MVA of 1.0 cm2, concordant with the PHT and continuity methods
Pressure half-time (PHT) is the time (in ms) it takes for the peak pressure gradient across the mitral valve in diastole to decrease by 50%. Based on the relationship between pressure and velocity, it is also the time in ms it takes for the peak velocity to decrease by 29%. This measurement is obtained by tracing the slope of the E wave during early diastole (Fig. 11.7b). It has been found that there is an inverse relationship between PHT and MVA by the following equation: MVA (cm2) = 220/PHT [21]. In addition, the MVA (cm2) = 759/Deceleration Time (ms). See Table 11.2 for measurements and valve stenosis severity.
Pressure half-time may be low even in severe MS if atrial compliance is low. In severe aortic insufficiency, due to the increase in the LVEDP during diastole as a result of regurgitation, the pressure between the LV and LA will equilibrate sooner, so the PHT will be reduced and the MVA estimate using the PHT will be inaccurate.
The continuity equation estimates the MVA if there is no aortic insufficiency or mitral regurgitation. The flow through the mitral valve should equal the flow through the LVOT by conservation of mass. The formula for flow through the LVOT (i.e., stroke volume), as described previously, is LVOT VTI ∗ (LVOT diameter)2 ∗ 0.785. Again, this can be thought of as a cylinder, in which the base of the cylinder is the area of the LVOT and the height is the LVOT VTI. The flow through the mitral valve equals the product of the cross-sectional area of the mitral orifice (base of the cylinder) multiplied by the MV VTI (height of the cylinder). The MV VTI is determined by the computer package from the tracing of the CW mitral inflow from the 4 chamber view (Fig. 11.7c).
Because MS elevates LA pressures, pulmonary hypertension may result. In general, the more severe the MS is, the more severe the pulmonary hypertension becomes. Pulmonary artery (PA) pressures can be assessed using the estimated RVSP, assuming there is no RVOT obstruction or pulmonic stenosis. A resting PASP > 50 mmHg or exercise-induced pulmonary hypertension (PASP > 60 mmHg) in the absence of other causes implies hemodynamically significant mitral stenosis [22].
Mitral Regurgitation
Echocardiographic assessment of mitral regurgitation severity relies on a “weighted average” of the information obtained from multiple modalities (Table 11.3). Color Doppler is the most readily apparent and visualized method of assessing mitral regurgitation. The jet area in the atrium on color Doppler is highly dependent on PRF and color scale. Typically, a large jet area spanning more than 40% of the atrium is considered severe MR. However, there are many caveats to using jet area. The appearance of the color is highly technique-dependent, and can be affected by hemodynamic changes and atrial size. In addition, a very eccentric jet may “hug” the wall and appear to be smaller than a more central jet, giving the false impression that the eccentric MR is not severe. In addition, in the case of acute, severe mitral regurgitation, the jet duration may be very short given the acute rise in LA pressure, and technical factors such as insufficient color resolution may lead to underestimation [23]. Given its many limitations, jet area should not be the sole method used for quantification of mitral regurgitation.
Another method of MR assessment is the flow convergence or PISA method, which is an extension of the continuity principle and has been shown to correlate well with angiographically determined severity [24]. As flow converges toward a regurgitant orifice, the flow organizes into several concentric hemispheres, each with a specific velocity (Fig. 11.8a). As blood approaches the regurgitant orifice, the radius of the hemisphere decreases, while the velocity of blood at the surface of the hemisphere increases. Since the surface area (cm2) of the hemisphere can be derived from the radius (surface area of hemisphere = 2πr 2), and the velocity of the blood cells (cm/s) at the surface of the hemisphere (aliasing velocity, V a) can be obtained from the color scale, the product of these two values (in units of cm3/s) gives the flow rate proximal to the orifice (Fig. 11.8a). The flow rate distal to the orifice, which must equal the flow rate proximal to the orifice, can be calculated from the effective regurgitant orifice area (EROA) multiplied by the peak mitral regurgitant velocity, obtained from the CW Doppler in the 4 chamber view (Fig. 11.8c). To determine the velocity of the hemisphere of the proximal flow convergence, the color baseline or Nyquist limit are shifted downward toward the direction of flow (Fig. 11.8a). As shown in the figure, this maneuver increases the radius of the hemisphere, allowing easy visualization of color transition from blue to yellow, which is the location where the velocity is equal to the aliasing velocity. By having a larger radius and a lower aliasing velocity, propagation of error in radius measurement is reduced.

PISA (proximal isovelocity surface area) method for mitral regurgitation and vena contracta. (a) Artistic rendition of the PISA concept. As flow converges during systole toward the regurgitant orifice, it accelerates and forms concentric hemispheres of increasing velocity and decreasing radius. For example, the velocity at the edge of the yellow hemisphere is higher than the velocity at the edge of the blue hemisphere. First the image should be optimized and zoomed. Next, the color baseline is shifted downward toward the direction of flow, from −65 to −40 cm/s, creating the larger yellow hemisphere with a lower velocity on the right. The velocity at the boundary between the yellow and blue hemisphere is the aliasing velocity (V a = −40 cm/s). The flow proximal to the orifice equals the product of the hemisphere surface area (2πr 2) and the aliasing velocity (V a). This proximal flow should equal the flow distal to the orifice, which is the product of the regurgitant orifice area (EROA) and peak MR velocity (V MR). Therefore, EROA = (2πr 2∗V a)/V MR. (b) Similar to panel A, after creating a zoomed-in image, the color baseline is shifted toward the direction of flow, and a larger hemisphere with a known radius (0.8 cm) and aliasing velocity (V a = 38.5 cm/s) is created. Based on the above equation, the proximal flow rate is 154.7 cm3/s. (c) Continuous wave Doppler across the mitral valve to obtain the peak mitral regurgitant velocity (V MR) = 416 cm/s and MV VTI. The distal flow rate is V MR∗EROA. The EROA, which is equal to (2πr 2∗V a)/V MR, is 0.37 cm2, consistent with moderately-severe MR. Regurgitant volume can be calculated with the information in this figure (see Question 5). Using the simplified PISA formula, r 2/2, estimated EROA is 0.32 cm2, likely slightly underestimated because the aliasing velocity is 38.5 cm/s, not the 40 cm/s assumed in the simplified formula. (d) The vena contracta, the narrowest jet width at the orifice, measured in the parasternal long axis view, is 0.6 cm, consistent with moderately-severe MR
It follows that:
This, of course, assumes that the hemisphere radius is measured at the time that the peak MR velocity occurs, so attempts must be made and standardizing the timing of measurement (i.e., mid-systole). As seen in Table 11.2, ERO > 0.4 is severe MR, and <0.2 is mild MR. The PISA method is not very accurate in situations of very eccentric MR jets (may overestimate severity) and noncircular orifices. A geometric correction factor for eccentric jets that create a wedge of a hemisphere instead of a full hemisphere has been described [25]. The angle created by the wedge (α) is divided by 180° and multiplied by the EROA to obtain the geometrically corrected EROA. Therefore, Geometrically corrected EROA = (α/180) ∗ (6.28r 2 ∗ V a)/V MR. Furthermore, flow velocity calculated by the PISA method represents an instantaneous flow rate. For instance, in mitral valve prolapse, the instantaneous EROA may be large but if the regurgitation only occurs in mid to late systole, the total regurgitant volume may not be very large. So perhaps a more accurate measurement of MR severity in this situation would be regurgitant volume.
To determine the regurgitant volume (RV), the EROA is multiplied by the MV VTI.
EROA calculation using the PISA may be cumbersome, which can discourage its routine use. A simplified formula can be used if certain assumptions are made [26]. First, one assumes a pressure gradient between the LV and LA of 100 mmHg, which yields a mitral velocity (V MR) of 5 m/s or 500 cm/s (from the Bernoulli equation, LV systolic pressure − LA pressure = 4V MR 2). If aliasing velocity (V a) is set to 40 cm/s, then plugging these into the equation:
The vena contracta is the narrowest color flow at or upstream of the valve orifice [16]. For mitral regurgitation, it is typically assessed in the parasternal long axis view, and is considered to be independent of flow and pressure for a fixed orifice, even for eccentric jets (Fig. 11.8d). A vena contracta width of <0.3 cm is considered mild MR, and >0.7 cm is considered severe [16]. This parameter, when measurable, should always be considered a key component to the integrated approach to determining mitral regurgitation severity.
Other signs of severe MR are a triangular shape in the CW profile of the mitral regurgitant (early peaking) rather than a smooth parabolic profile, which implies rapid equilibration of LV and LA pressure from severe MR [16]. In addition, in the mitral inflow PW profile, severe MR is typically associated with a tall E wave >120 cm/s. Stage 1 diastolic dysfunction pattern on mitral inflow virtually excludes severe MR. In severe MR, the elevated LA pressures during systole decrease the gradient between the LA and the pulmonary veins, so the pulmonary vein s wave may be blunted or even reversed.
Aortic Insufficiency
In the parasternal long axis view, the percentage of the LVOT width that the regurgitant jet occupies has been correlated with aortic insufficiency (AI) severity [16]. If the jet width in diastole occupies more than 65% of the LVOT diameter, then it is considered severe. However, just as with jet area in MR, jet width in AI is not valid for eccentric jets in which severity may be underestimated (Fig. 11.9a) [27]. The vena contracta is the narrowest neck of the jet at the level of the valve. The width of the vena contracta correlates with regurgitant orifice area and is unaffected by jet eccentricity [28]. To accurately measure the vena contracta width, a zoomed-in parasternal long axis view should be obtained that shows the flow convergence zone, the vena contracta, as well as the regurgitant jet in the LVOT. A vena contracta width ≥6 mm suggests severe AI (Table 11.4). The utility of this method is limited if there are multiple jets [16]. The PISA method has been applied for the calculation of the aortic regurgitant EROA. This measurement should be made in the apical 5 chamber or apical long axis view in early diastole but is technically more difficult to obtain than the PISA for MR. The same principle applies as with MR, in that the flow rate proximal to the orifice (aorta) which is the product of the hemisphere area and the aliasing velocity (2πr 2∗V a) equals the flow rate distal to the orifice in the LVOT (EROA∗peak aortic regurgitant velocity). However, the color baseline is shifted up rather than down, as this is toward the direction of flow. EROA ≥0.3 cm2 correlates with severe AI (Table 11.4). The simplified PISA method used for MR (r 2/2) does not apply to AI.

Severe aortic insufficiency (AI). (a) Parasternal long axis view color Doppler demonstrates a very severe, eccentric, and posterior directed jet. Note that the M-Mode across the mitral leaflet shows fluttering of the anterior leaflet due to the aortic insufficiency jet (lower left corner inset). Given the eccentricity, one cannot use the LVOT jet area to assess severity. (b) Pulse wave Doppler with sample volume in the upper descending thoracic aorta, demonstrating holodiastolic flow reversal, a sign of severe AI. (c) Continuous wave Doppler across the aortic valve in the apical 5 chamber view. The PHT is 253 ms, consistent with severe AI. The aortic insufficiency VTI is 232 cm based on the CW profile. (d) Application of the continuity equation allows for the calculation of the regurgitant AI volume. Flow across the mitral valve plus the regurgitant volume should equal the flow across the aortic valve (Stroke volume). The MVA is determined by measuring the mitral valve diameter, and this area (5.3 cm2) is multiplied by the MV VTI at the annulus (19 cm) to yield a flow of 101 cm3. Flow across the aortic valve is determined by the product of the LVOT VTI and LVOT area, which yields a volume of 169 cm3, calculation not shown. Therefore, the aortic insufficiency regurgitant volume is 169 cm3 − 101 cm3 = 68 cm3, consistent with severe AI. The regurgitant orifice area (EROA) of the aortic valve is calculated by dividing the regurgitant volume (68 cm3) by the AI VTI (232 cm), which equals 0.3 cm2, also consistent with severe AI
Pulse wave Doppler in the upper descending thoracic aorta from the suprasternal view can both qualitatively and quantitatively assess aortic regurgitation severity [27]. Holodiastolic flow reversal in the proximal descending aorta is specific for at least moderately-severe aortic insufficiency, and is considered to be the echocardiographic equivalent of the Duroziez’s sign [16] (Fig. 11.9b). This is a much more specific finding if there is flow reversal is present when sampling in the abdominal aorta. The ratio of the reverse flow (diastolic VTI∗cross-sectional area of the aorta in diastole) to the forward flow (systolic VTI∗cross-sectional area of the aorta in systole) is proportional to the regurgitant fraction [29].
PHT of the aortic regurgitation jet reflects the rate of equalization between the aortic and LV pressures (Fig. 11.9c). Therefore, this PHT is not only influenced by the severity of aortic insufficiency but also by LV pressure, LV compliance, and afterload conditions. Hence, it may be the least reliable method for assessing regurgitation severity [16]. A PHT <200 ms is supportive of severe aortic insufficiency, and a pressure half-time greater than 400 ms is unlikely to represent more than moderate AR. However, even in severe AI, if the LV has dilated as a chronic adaptation to the increased preload and afterload, then the pressure half-time could be normal since the LV and aorta pressures would not rapidly equilibrate. If vasodilators are given or LV pressures increase for a given degree of AI, the PHT would decrease.
The continuity equation can also be applied to aortic insufficiency if there is no more than mild mitral insufficiency. Think of the flow across the aortic valve as gross income, the regurgitant volume as the tax, and the flow across the mitral valve as the net income. The difference between the flow across the aortic valve (“gross” systolic stroke volume) and the flow across the mitral valve (“net” forward stroke volume) is equal to the “tax” or regurgitant volume per beat. The “gross” stroke volume can be obtained either from the LVOT VTI method or from the difference between the LV volumes in systole and diastole. To calculate “net” forward flow across the mitral valve, it is important to use PW and place the sample volume at the annulus of the mitral valve to measure and accurate flow across the mitral valve during diastole (Fig. 11.9d).
Once the regurgitant stroke volume is obtained, it can be divided by the regurgitant jet VTI obtained from CW in diastole to calculate the EROA [16]. If the EROA is in the severe range but the RV is not, it may be because in acute AI, the rapid increase in the LVEDP shortens the time for regurgitation, so the regurgitant volume may not be as large as expected from the EROA (Fig. 11.10).

Summary of intracardiac pressure calculations. RA right atrial pressure, IVC inferior vena cava, RVSP right ventricular systolic pressure, VTR peak tricuspid regurgitation velocity, PASP pulmonary artery systolic pressure, RVOT right ventricular outflow tract, PS pulmonic stenosis; PAEDP pulmonary artery end-diastolic pressure, VEDPR end-diastolic pulmonary regurgitation velocity, PAP pulmonary artery pressure, VEarlyDPR early diastolic pulmonary regurgitation velocity, PVR pulmonary vascular resistance, VTI velocity time integral, LVOT left ventricular outflow tract, D diameter, LA left atrial pressure, SBP systolic blood pressure, VMR peak mitral regurgitation velocity, PCWP pulmonary capillary wedge pressure, LVEDP left ventricular end-diastolic pressure, DBP diastolic blood pressure, VEDAI end-diastolic aortic insufficiency velocity, SVR systemic vascular resistance, Qp pulmonary flow, Qs systemic flow. (Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2011)
3D Echocardiography
The advent of 3D echocardiography has provided clinicians with more anatomic detail regarding valve structure and function. One arena in particular in which 3D echo provided value is the assessment of valves during valve interventions, either surgical or in the catheterization lab. For instance, 3D echo assists the operator in the transcatheter placement of the Mitra-clip for the treatment of mitral regurgitation. Beyond informing the clinical regarding anatomic structure and function, 3D echo has some limited clinical applications in the assessment of valve hemodynamics. In mitral stenosis, 3D echo can be used for measuring valve area. In addition, in the same way that a PISA is calculated using 2D echo, 3D Doppler can be used to assess the radius of the proximal isovelocity surface area. The 2D PISA assumes a hemispheric shape of the PISA, which may not be true in all regurgitant lesions, and, for example, in functional mitral regurgitation, the geometry may be more ellipsoid. By applying the hemi-ellipsoid formula for instance, the mitral regurgitation severity can be more accurately measured [30, 31]. Although its current clinical application in valve hemodynamics is somewhat limited, with time this method will likely receive wider adoption.
Review Questions
-
1.
What is the estimated right ventricular systolic pressure (RVSP) in the patient in Fig. 11.4a if the inferior vena cava (IVC) measures 2.5 cm and there is no collapse with sniff?
-
A.
60 mmHg
-
B.
70 mmHg
-
C.
30 mmHg
-
D.
85 mmHg
-
A.
-
2.
What is the estimated end-diastolic pulmonary artery pressure in Fig. 11.4b?
-
A.
14.4 mmHg
-
B.
14.4 mmHg + RA pressure
-
C.
38.5 mmHg
-
D.
38.5 mmHg + RA pressure
-
A.
-
3.
Based on the continuity equation, what is the estimated aortic valve area (AVA) in Fig. 11.5? Is this severe AS or moderate AS?
-
A.
1.2 cm2, moderate AS
-
B.
1.2 cm2, severe AS
-
C.
0.6 cm2, severe AS
-
D.
0.6 cm2, moderate AS
-
A.
-
4.
The patient in Fig. 11.6 has a known secundum atrial septal defect , and as shown in panel (a), there is left to right flow across the atrial septal defect. The echocardiogram was performed to estimate the shunt fraction. Based on the information provided in Fig. 11.6, what is the estimated Q p/Q s ratio?
-
A.
1:1
-
B.
1.3:1
-
C.
0.5:1
-
D.
2:1
-
A.
-
5.
In Fig. 11.8, the regurgitant orifice area is 0.37 cm2. Based on the information in panel (c), what is the estimated regurgitant volume per beat ?
-
A.
143 mL/beat
-
B.
416 mL/beat
-
C.
53 mL/beat
-
D.
100 cc/beat
-
A.
Answers
-
1.
The peak TR velocity is 420 cm/s, or 4.2 m/s. Based on the simplified Bernoulli equation, the difference between the RV and RA pressure is 4V TR 2, or 4∗(4.2)2 = 70.56 mmHg, roughly 70 mmHg. The RA pressure is estimated at 15 mmHg based on the dilated IVC that does not collapse greater than 50% with the sniff. Therefore, because the RVSP is equal to RA pressure plus the 4V TR 2, RVSP = 70 mmHg + 15 mmHg = 85 mmHg, compatible with severe pulmonary hypertension.
-
2.
In Fig. 11.4b, the spectral Doppler shows the CW across the RVOT and pulmonic valve. From the pulmonary regurgitation jet, the late diastolic pulmonary regurgitation velocity represents the pressure difference between the pulmonary artery and the right ventricle at end diastole (note the timing just at the onset of the QRS). Therefore, the 4v PRed 2 = RVEDP − PAEDP. It follows that PAEDP = RVEDP + 4v PRed 2. Because the RVEDP is equal to RA pressure, PAEDP = RA + 4v PRed 2. Here the end-diastolic velocity is 1.9 m/s. Therefore, PAEDP = RA + 4(1.9)2 = 14.4 mmHg + RA pressure.
-
3.
Based on the continuity equation, AVA = [LVOT VTI ∗ (LVOT diameter)2 ∗ 0.785]/[AV VTI]. The LVOT VTI from Fig. 11.5b is 28.1 cm, and the LVOT diameter from Fig. 11.5a is 1.9 cm. The highest AV VTI was obtained from the right sternal border view, which is 124 cm. Note that this corresponded to a peak and mean gradient of 119/74 mmHg, severe aortic stenosis (AS) by gradients. Using the continuity equation, AVA = [28.1 ∗ (1.9)2 ∗ 0.785]/[124] = 0.6 cm2, also compatible with severe AS.
-
4.
The ratio of pulmonary blood flow to systemic blood flow is the Q p/Q s, or shunt fraction. The systemic blood flow (Q s) is estimated by multiplying the LVOT area, (LVOT D)2∗0.785, by the LVOT VTI. As shown in Fig. 11.6c, the LVOT diameter is 2.1 cm and the LVOT VTI is 13.2 cm. Therefore, the systemic flow is (2.1)2 ∗ 0.785 ∗ 13.2 = 45.7 cm3. The pulmonary blood flow (Q p) is estimated by multiplying the RVOT area, (RVOT D)2∗0.785, by the RVOT VTI. As shown in Fig. 11.6d, the RVOT diameter is 2.47 cm and the RVOT VTI is 12.3 cm. Therefore, the pulmonary blood flow is (2.47)2 ∗ 0.785 ∗ 12.3 = 58.9 cm3. The Q p/Q s ratio is 45.7/58.9 = 1.3:1. Note that because the 0.785 constant is present in both the numerator and denominator, the Q p/Q s calculation can be simplified to [(RVOT D)2 ∗ (RVOT VTI)]/[(LVOT D)2 ∗ (LVOT VTI)].
-
5.
The regurgitant volume is equal to the product of the regurgitant orifice area (EROA, cm2) and the MV VTI (cm). In this case, the product of the EROA (0.37 cm2) and the MV VTI (143 cm) gives a regurgitant volume of 53 mL/beat, which is consistent with moderately-severe MR.
References
Anavekar NS, Oh JK. Doppler echocardiography: a contemporary review. J Cardiol. 2009;54(3):347–58.
Quinones MA, Otto CM, Stoddard M, Waggoner A, Zoghbi WA, Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. Recommendations for quantification of Doppler echocardiography: a report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. J Am Soc Echocardiogr. 2002;15(2):167–84.
Hatle L, Angelsen B. Doppler ultrasound in cardiology: physical principles and clinical applications. 2nd ed. Philadelphia: Lea & Febiger; 1985. p. 331.
Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23(7):685–713; 786–8.
Nageh MF, Kopelen HA, Zoghbi WA, Quinones MA, Nagueh SF. Estimation of mean right atrial pressure using tissue Doppler imaging. Am J Cardiol. 1999;84(12):1448–51, A8.
Nagueh SF, Kopelen HA, Zoghbi WA. Relation of mean right atrial pressure to echocardiographic and Doppler parameters of right atrial and right ventricular function. Circulation. 1996;93(6):1160–9.
Firstenberg MS, Vandervoort PM, Greenberg NL, et al. Noninvasive estimation of transmitral pressure drop across the normal mitral valve in humans: importance of convective and inertial forces during left ventricular filling. J Am Coll Cardiol. 2000;36(6):1942–9.
Lima CO, Sahn DJ, Valdes-Cruz LM, et al. Noninvasive prediction of transvalvular pressure gradient in patients with pulmonary stenosis by quantitative two-dimensional echocardiographic Doppler studies. Circulation. 1983;67(4):866–71.
Masuyama T, Kodama K, Kitabatake A, Sato H, Nanto S, Inoue M. Continuous-wave Doppler echocardiographic detection of pulmonary regurgitation and its application to noninvasive estimation of pulmonary artery pressure. Circulation. 1986;74(3):484–92.
Beard JT II, Newman JH, Loyd JE, Byrd BF III. Doppler estimation of changes in pulmonary artery pressure during hypoxic breathing. J Am Soc Echocardiogr. 1991;4(2):121–30.
Scapellato F, Temporelli PL, Eleuteri E, Corra U, Imparato A, Giannuzzi P. Accurate noninvasive estimation of pulmonary vascular resistance by Doppler echocardiography in patients with chronic failure heart failure. J Am Coll Cardiol. 2001;37(7):1813–9.
Gorcsan J III, Snow FR, Paulsen W, Nixon JV. Noninvasive estimation of left atrial pressure in patients with congestive heart failure and mitral regurgitation by Doppler echocardiography. Am Heart J. 1991;121(3 pt 1):858–63.
Ommen SR, Nishimura RA, Appleton CP, et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: a comparative simultaneous Doppler-catheterization study. Circulation. 2000;102(15):1788–94.
Ha JW, Oh JK, Ling LH, Nishimura RA, Seward JB, Tajik AJ. Annulus paradoxus: transmitral flow velocity to mitral annular velocity ratio is inversely proportional to pulmonary capillary wedge pressure in patients with constrictive pericarditis. Circulation. 2001;104(9):976–8.
Abbas AE, Fortuin FD, Patel B, Moreno CA, Schiller NB, Lester SJ. Noninvasive measurement of systemic vascular resistance using Doppler echocardiography. J Am Soc Echocardiogr. 2004;17(8):834–8.
2014 AHA/ACC Guideline for Management of Patients with Valvular Heart Disease. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:2440–92.
Baumgartner H, Hung J, Bermejo J, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009;22(1):1–23; 101–2.
Oh JK, Taliercio CP, Holmes DR Jr, et al. Prediction of the severity of aortic stenosis by Doppler aortic valve area determination: prospective Doppler-catheterization correlation in 100 patients. J Am Coll Cardiol. 1988;11(6):1227–34.
Monin JL, Quere JP, Monchi M, et al. Low-gradient aortic stenosis: operative risk stratification and predictors for long-term outcome: a multicenter study using dobutamine stress hemodynamics. Circulation. 2003;108(3):319–24.
Rahimtoola SH, Durairaj A, Mehra A, Nuno I. Current evaluation and management of patients with mitral stenosis. Circulation. 2002;106(10):1183–8.
Thomas JD, Weyman AE. Doppler mitral pressure half-time: a clinical tool in search of theoretical justification. J Am Coll Cardiol. 1987;10(4):923–9.
Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52(13):e1–142.
Smith MD, Cassidy JM, Gurley JC, Smith AC, Booth DC. Echo Doppler evaluation of patients with acute mitral regurgitation: superiority of transesophageal echocardiography with color flow imaging. Am Heart J. 1995;129(5):967–74.
Bargiggia GS, Tronconi L, Sahn DJ, et al. A new method for quantitation of mitral regurgitation based on color flow Doppler imaging of flow convergence proximal to regurgitant orifice. Circulation. 1991;84(4):1481–9.
Pu M, Vandervoort PM, Griffin BP, et al. Quantification of mitral regurgitation by the proximal convergence method using transesophageal echocardiography. Clinical validation of a geometric correction for proximal flow constraint. Circulation. 1995;92(8):2169–77.
Pu M, Prior DL, Fan X, et al. Calculation of mitral regurgitant orifice area with use of a simplified proximal convergence method: initial clinical application. J Am Soc Echocardiogr. 2001;14(3):180–5.
Zoghbi WA, Enriquez-Sarano M, Foster E, et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16(7):777–802.
Tribouilloy CM, Enriquez-Sarano M, Bailey KR, Seward JB, Tajik AJ. Assessment of severity of aortic regurgitation using the width of the vena contracta: a clinical color Doppler imaging study. Circulation. 2000;102(5):558–64.
Touche T, Prasquier R, Nitenberg A, de Zuttere D, Gourgon R. Assessment and follow-up of patients with aortic regurgitation by an updated Doppler echocardiographic measurement of the regurgitant fraction in the aortic arch. Circulation. 1985;72(4):819–24.
Schmidt FP, Gniewosz T, Jabs A, Münzel T, Hink U, Lancellotti P, von Bardeleben RS. Usefulness of 3D-PISA as compared to guideline endorsed parameters for mitral regurgitation quantification. Int J Cardiovasc Imaging. 2014;30(8):1501–8.
Matsumura Y, Fukuda S, Tran H, et al. Geometry of the proximal isovelocity surface area in mitral regurgitation by 3-dimensional color Doppler echocardiography: difference between functional mitral regurgitation and prolapse regurgitation. Am Heart J. 2008;155:231–8.
Suggested Reading
Hatle L, Angelsen B. Doppler ultrasound in cardiology: physical principles and clinical applications. 2nd ed. Philadelphia: Lea & Febiger; 1985. p. 331.
Quinones MA, Otto CM, Stoddard M, Waggoner A, Zoghbi WA, Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. Recommendations for quantification of Doppler echocardiography: a report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. J Am Soc Echocardiogr. 2002;15(2):167–84.
Baumgartner H, Hung J, Bermejo J, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009;22(1):1–23; 101–2.
Zoghbi WA, Enriquez-Sarano M, Foster E, et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16(7):777–802.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Zardkoohi, O., Grimm, R.A. (2019). Echocardiography. In: Askari, A., Messerli, A. (eds) Cardiovascular Hemodynamics. Contemporary Cardiology. Humana, Cham. https://doi.org/10.1007/978-3-030-19131-3_11
Download citation
DOI: https://doi.org/10.1007/978-3-030-19131-3_11
Published:
Publisher Name: Humana, Cham
Print ISBN: 978-3-030-19130-6
Online ISBN: 978-3-030-19131-3
eBook Packages: MedicineMedicine (R0)