
Abstract
Contact dermatitis is a common condition seen in primary care. It makes up 10–20% of dermatologic conditions. It can affect all professions, although some professionals are at higher risk. The condition develops secondary to an irritant or allergens. Irritants make up a larger portion of these two causes. Diagnosis is often clinical although some patients may require further testing to identify the offending agent. Treatment is usually topical steroids, and prevention by avoidance is a mainstay to prevent exacerbations.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Primary care physicians are often found on the front lines of diagnosing and treating dermatologic conditions. A common ailment that many family medicine physicians see is contact dermatitis. Although it may appear to have a simple etiology, the initial diagnosis and subsequent treatment can be difficult. With the chemical industry being on the rise, new allergens and irritants become the culprits of contact dermatitis.
Several sources cite the incidence of contact dermatitis as high as 10–20% of all dermatologic conditions [1]. Contact dermatitis affects people of various professions, age, and gender. Symptoms vary in severity; however, oftentimes, they can be lifelong and impact social and professional aspects of patients’ lives. Thus, the knowledge of how to recognize, diagnose, and treat contact dermatitis becomes essential.
Contact dermatitis is a skin condition which develops due to exposure to either an irritant or an allergen. Thus, it is classified into two categories: irritant contact dermatitis and allergic contact dermatitis. Irritant contact dermatitis is the more common of the two, being responsible for approximately 80% of cases, while allergens cause 20% of cases [2]. Although both types are caused by an insult to the epidermal barrier, the pathogenesis is very different.
Stratum corneum is an important part of the skin’s permeability barrier, which protects the dermis from chemicals, microbes, and mechanical assaults [3]. If the stratum corneum becomes disrupted, the skin becomes highly susceptible to outside insults. Skin lipids, corneocytes, and tight junctions such as occludin and claudin in the epidermis are the front lines of the skin permeability barrier [3]. Cytokine signaling plays a role in epidermal homeostasis and repair [3]. Chronic contact dermatitis can sometimes be attributed to an increase in cytokine production as a response to repair the epidermis [3].
Once skin barrier becomes damaged, allergens and irritants can penetrate easily.
Proksch and Brasch describe allergen-specific T cells being the most important differentiating factor between allergen and irritant contact dermatitis propagation. Irritant contact dermatitis is often a result of prolonged exposure to the irritant, such as water, soap, or detergents, whereas allergic contact dermatitis is a type IV delayed hypersensitivity reaction caused by re-exposure to an allergen after initial sensitization [4].
Prevalence and Etiology
Contact dermatitis can most commonly be attributed to occupational, cosmetic, or environmental exposure. Occupational exposure to a wide variety of chemicals is the typical setting in which contact dermatitis occurs. It accounts for over 70–80% of all occupational dermatologic conditions, and treatment costs exceed one billion dollars per year [5]. Recent data revealed that thiuram rubber chemical accelerators, epoxy resin, and antimicrobials such as formaldehyde, methyldibromo glutaronitrile, and methylchloroisothiazolinone are some of the common culprits in occupational contact dermatitis [5]. Cooks, butchers, beauticians, bakers, hairdressers, and painters are primarily affected, with estimates ranging from 23.3 to 96.8 cases per 10,000 workers per year [5]. A study done at a tertiary hospital in Spain noted that the incidence of occupational contact dermatitis almost doubled in the past 7 years [6]. Workers often suffer of hand contact dermatitis, and it has been suggested by several dermatologic associations to make hand eczema and contact dermatitis a separate subtype of this condition [5].
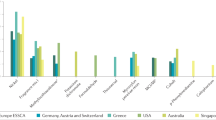
As cosmetic product consumption is on the rise, so are the adverse reactions to these products (Fig. 1). According to a study by Zaragoza-Ninet et al., which analyzed patch test results from 1996 to 2004 and compared them to data collected from 2005 to 2013, a 5% increase in allergic contact dermatitis attributed to cosmetics was noted. Preservatives and fragrances found in soap, moisturizing cream, and hair dye are the most prominent offending agents [6]. Formaldehyde, methylisothiazolinone, and iodopropynyl butylcarbamate are the preservatives responsible for contact dermatitis [6].

Local reaction to cosmetics – James Studdiford MD/Thomas Jefferson University
Interestingly, the growing trend to practice safe sun exposure has led to sunscreen being the seventh most widely used cosmetic agent to cause allergic contact dermatitis [6]. Its main ingredient, oxybenzone, has become the most frequent allergen [6]. In cosmetic-related contact dermatitis, the face, hands, and neck are the utmost affected sites [6].
Environmental allergens are very frequently the culprits of dermatitis. In particular, primary care physicians often see reactions caused by the Toxicodendron species: poison sumac, ivy, and oak [9]. Approximately 50–70% of population is sensitized to these species of plants [10] (Fig. 2). Urushiol found in the oleoresinous sap is the chief allergen responsible for dermatitis [10]. Direct or indirect contact can lead to manifestation of pruritus, skin desquamation, vesicles, and even bullae, typically within a 24–48-hour period [10]. Lesions appear in streak-like pattern on hands, legs, and trunk [9] (Fig. 3). This condition most commonly resolves within 1–2 weeks [10]. Typically, topical corticosteroids are usually sufficient to treat toxicodendron dermatitis. In severe cases, which may involve more than 20% of body surface area, severe itching, edema, or reaction involving the face, genitals, or hands, oral prednisone is often required [9].

Poison ivy Public Domain

Plant dermatitis by BTDenyer at English Wikipedia – Transferred from en.wikipedia to Commons, Public Domain, https://commons.wikimedia.org/w/index.php?curid=3262811
Presentation
The identification of contact dermatitis can be a difficult task due to the fact that symptoms can vary based on the causative agent and the area of the body that is affected. The hands, head, neck, legs, and feet are the sites associated with manifestation of symptoms [2]. It has been documented that ~98% of contact dermatitis cases present on the hands of patients [11]. As detailed previously, it has been shown that members of the manufacturing and healthcare professions are at the highest risk [11].
Clinical presentation of symptoms is characteristically localized to the site of contact with an agent or irritant [2] (Figs. 4 and 5). The manifestation of symptoms can occur as rapidly as within minutes or upward of hours following exposure to an insult [11]. Patients usually complain of a localized erythema with itching. Based on the agent involved in the insult, symptoms can increase in intensity. With chronic contact dermatitis, the skin may present with dryness, scaling, and the development of fissures that can lead to the development of a secondary bacterial infection.

Contact dermatitis from necklace – James Studdiford MD/Thomas Jefferson University

Contact dermatitis metal – James Studdiford MD/ Thomas Jefferson University
Overall, the ways that contact dermatitis presents share a great deal of similarities with a variety of other conditions. This reason makes delineation of diagnosis difficult. Thus, it is important to obtain thorough history of a patient’s occupation, hobbies, cosmetic use, and family history/personal history of atopy.
Diagnosis
For many years, patch testing has been the gold standard for diagnosis of allergic contact dermatitis [12]. Irritant contact dermatitis is considered to be the diagnosis of exclusion, when patch testing is found to be negative [4]. Currently, standard panel testing consists of 35 allergens and 1 control [12]. Results of patch testing should be correlated carefully with clinical history. The process itself is very simple. Allergens are selected, based on a patient’s history, then placed on patient’s back, and left in place.
After 48 hours, they are removed, and the results are read immediately and then reread after 72 hours and 1 week later [12]. Reaction grading is based on its severity and is done on a scale 1+ to 3+ [4]. A certain degree of erythema should be present for a reaction to be considered positive [4]. Since anaphylactic reactions during testing have been reported, it is important to conduct this procedure in a facility with resuscitation capabilities.
Frequently standard panel testing is a good starting point, and sometimes expanded series testing is necessary, as 26% of allergens can be missed with standard allergen testing [12]. It is also possible to test with patient’s own products.
Several factors should be considered when patch testing patients (Fig. 6). Individuals with recent oral corticosteroid exposure or on chronic immunosuppressive therapy or those with recent sun exposure have a risk of having false-negative results. Patients with diffuse dermatitis can develop false-positive reactions [4]. It is also not recommended to patch test pregnant patients [4].

Example of patch testing
Frequent patient follow-up is important in interpreting patch test results. Importantly, the second reading at 72 hours can help distinguish between irritant and allergic contact dermatitis [12]. In addition, allergens that cause delayed reactions can be detected at this reading. Some of those allergens are bacitracin, corticosteroids, and disperse blue dyes [12].
Inconsistent patient follow-up, constant emergence of new allergens, and variable interpretation of test results are some of the challenges of patch testing [12]. Patch testing for fragrances and botanicals poses another challenge, as new products marketed as “natural” come on the market every day and identifying responsible allergens can be very difficult [4]. Other diagnostic testing includes repeat open application tests and lymphocyte transformation tests [4]. Repeat open application tests are useful at determining whether certain identified allergens can cause a reaction at most frequently used concentrations [4]. Lymphocyte transformation tests are easier to perform in terms of patient convenience as it only requires a blood sample [4]. However, it is limited in its availability and the number of allergens that can be tested [4].
Management
According to Lee et al., recovery time for acute contact dermatitis after exposure to a single irritant is typically 4 weeks [7]. Healing time is even longer after prolonged exposure to more than one irritant with certain studies citing numbers as high as 10 weeks [8].
Once the culprit is identified, treatment can be streamlined. Avoidance of the irritant or allergen, reduction of skin inflammation, and restoration of the epidermal barrier are all key approaches to treatment of contact dermatitis. Patient education is essential for successful outcome. It is often difficult for patients to remember the long names of allergens; thus databases such as the Contact Allergen Management Program (CAMP) and Contact Allergen Replacement Database (CARD) list products devoid of particular allergens [10, 16].
As mentioned previously, insult to skin barrier is often the first step in the pathogenesis of contact dermatitis. Thus, of foremost importance is protection and restoration of the skin barrier. Barrier protection and repair creams are often utilized. These creams enhance hydration by reducing the transepidermal water loss, thus reducing the effect of irritants on the protective barrier [14]. Although it is very difficult to standardize.
studies, some researchers have found that barrier creams can be protective against four of the irritants such as sodium laureth sulfate (SLS), sodium hydroxide (NaOH), lactic acid, and toluene [15]. Barrier creams can contain a variety of combinations of ceramide.
and petrolatum, one of the oldest barriers known. Ceramide, hyaluronic acid, and palmitoylethanolamide have been found helpful in skin hydration maintenance [15].
In addition to cold compresses or calamine lotion, topical corticosteroids can often be effective in the acute phase of allergic contact dermatitis. Several factors such as location, expected duration of treatment, and previous corticosteroid use affect choice of topical treatment. Steroids are classified into five groups based on their structure: triamcinolone acetonide, hydrocortisone type, betamethasone type including betamethasone dipropionate type, and methylprednisolone acetonate [13]. Typically, low-potency corticosteroids should be used in areas where the skin is thinner, such as the face or genital area [13]. High-potency topical corticosteroid can be used for reactions that are localized. Moderate-potency preparations can be used for more widespread reactions [10]. Patients should be advised to apply the minimum amount of medication to the affected area as well as to not exceed the prescribed treatment duration.
Severe reactions can often require oral steroid treatment. Prednisone tapered over 2–3 weeks has been shown to be more effective in decreasing the risk of rebound reactions as well as use of other medications [9].
Prevention
In terms of prevention of contact dermatitis, discontinuation of the irritating agent is the best measure to alleviate reoccurrence. If avoidance of the agent is impossible, then the addition of a barrier can aid in preventing contact dermatitis. Masks, protective eyewear, and gloves are excellent sources for creating a barrier [16].
References
Martin S. Contact dermatitis: from pathomechanisms to immunotoxicology. Exp Dermatol. 2012;21(5):382–9.
Rashid RS, Shim TN. Contact dermatitis. BMJ. 2016;353:i3299.
Proksch E, Brasch J. Abnormal epidermal barrier in the pathogenesis of contact dermatitis. Clin Dermatol. 2012;30(3):335–44.
Mowad C, et al. Allergic contact dermatitis. J Am Acad Dermatol. 2016;74(6):1029–40.
Wiszniewska M, Walusiak-Skorupa J. Recent trends in occupational contact dermatitis. Curr Allergy Asthma Rep. 2015;15(7):43.
Laguna C, et al. Allergic contact dermatitis due to cosmetics: a clinical and epidemiological study in a tertiary hospital. Actas Dermosifiliogr. 2009;100(1):53–60.
Lee JY, Effendy I, Maibach HI. Acute irritant contact dermatitis: recovery time in man. Contact Dermatitis. 1997;36:285–90.
Choi JM, Lee JY, Cho BK. Chronic irritant contact dermatitis: recovery time in man. Contact Dermatitis. 2000;42(5):264–9.
Curtis G, Lewis AC. Treatment of severe poison ivy: a randomized, controlled trial of long versus short course oral prednisone. J Clin Med Res. 2014;6(6):429–34. PMC. Web. 1 Sept. 2016.
Lee NP, Arriola ER. Poison ivy, oak, and sumac dermatitis. West J Med. 1999;171.5-6:354–355. Print.
Kranke B, Schuster C. Contact dermatitis: relevant differential diagnoses, simulators and variants. J Dtsch Dermatol Ges. 2015;13:1073.
Mowad C. Contact dermatitis: practice gaps and challenges. Dermatol Clin. 2016;34:263–7.
Welsh E, Goldenberg A, Welsh O, Jacob SE. Contact dermatitis: therapeutics when avoidance fails. J Allergy Ther. 2014;5:185.
Draelos Z. New treatments for restoring impaired epidermal barrier permeability: skin barrier repair creams. Clin Dermatol. 2012;30:345–8.
Mostosi C, Simonart T. Effectiveness of barrier creams against irritant contact dermatitis. Dermatology. 2016;232:353–62.
American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology. Contact dermatitis: a practice parameter. Ann Allergy Asthma Immunol. 2006;97(3 suppl 2):S1–S38.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kiselova, K., Russell, J.J. (2019). Contact Dermatitis. In: Russell, J., Ryan Jr., E. (eds) Common Dermatologic Conditions in Primary Care. Current Clinical Practice. Humana, Cham. https://doi.org/10.1007/978-3-030-18065-2_5
Download citation
DOI: https://doi.org/10.1007/978-3-030-18065-2_5
Published:
Publisher Name: Humana, Cham
Print ISBN: 978-3-030-18064-5
Online ISBN: 978-3-030-18065-2
eBook Packages: MedicineMedicine (R0)