
Abstract
Long-term medication treatment has been demonstrated to be the most effective treatment for opioid use disorder. This chapter covers the treatment of opioid withdrawal and the use of methadone, buprenorphine, and extended-release naltrexone, the three medications approved by the Food and Drug Administration (FDA) for long-term treatment of this condition. It includes an overview of the pharmacology of each medication, specific criteria for patient selection, and guidelines for clinical use of the medications. Other topics covered include federal methadone regulations, procedures for obtaining the Drug Enforcement Administration (DEA) waiver to prescribe buprenorphine, criteria for an appropriate medication diversion control plan, care for pregnant women, patients with co-occurring psychiatric disorders, and the management of acute pain in patients on addiction pharmacotherapy. Guidance is provided for integrating medication into a comprehensive addiction recovery program that includes medical and psychiatric care, addiction counseling, and participation in mutual support programs. Addiction pharmacotherapy is presented as the most critical element in the successful management of an opioid use disorder.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Methadone
- Buprenorphine
- Buprenorphine/naloxone
- Extended-release naltrexone
- Naloxone
- Precipitated withdrawal
- Opioid overdose
- Naloxone
- Maintenance treatment
- Opioid use disorder
- Mu-opioid receptor
Introduction
Following the American Civil War, physicians often prescribed long-term opioid pharmacotherapy for the treatment of opioid use disorder (OUD) [1]. Support for this practice declined at the end of the nineteenth century and was outlawed with the passage of the Harrison Act in 1914. This reflected the general mindset of the prohibition era that categorized alcohol and opioid use disorder as moral failings rather than medical problems. This shift in paradigm dominated medical thinking until the period following WWII when the medical community began to reclaim a role in the treatment of alcohol use disorder. The epidemics of heroin use disorder that followed WWII and the Vietnam War led to recognition of the failure of the criminal justice paradigm and to the search for a more effective public health and medical model for the management of OUD. The modern era of medication treatment for OUD began in 1972 with Food and Drug Administration (FDA) approval of methadone for withdrawal and maintenance treatment [2]. The restriction of access to the medication to heavily regulated “methadone clinics” reflected pervasive stigma, fear of contact with individuals with OUD, and the ambivalence of both the legal and the medical communities to the restoration of a medical model for managing OUD. In the ensuing 50 years, there has been a heightened need for treatment driven by new epidemics of addiction to prescription medications and more recently illicit fentanyl and growing awareness that OUD has become a signature public health crisis of our era. This has been matched by appreciation for the strong evidence base that supports long-term medication treatment as the most effective treatment for OUD. This chapter will review medication options for treating OUD and explain how medications fit into a comprehensive, multidisciplinary treatment approach to this ongoing public health crisis.
Treatment of Withdrawal
Medication withdrawal treatment for OUD involves treatment with a long-acting opioid medication and gradually tapering the dose at a rate that minimizes severe withdrawal and avoids excessive sedation or intoxication. The standard withdrawal medications are oral methadone or sublingual buprenorphine/naloxone (BUP/NX) [3, 4]. If patients refuse opioids, or if opioid medications are not available, the alpha-2-adrenergic agonist clonidine may be used. Clonidine moderates autonomic nervous system withdrawal symptoms but does not adequately control dysphoria, craving, insomnia, or restlessness. It is sometimes used in combination with methadone, to permit more rapid withdrawal treatment with lower doses of opioids. For most patients clonidine alone is not a satisfactory treatment for the full range of withdrawal symptoms; higher rates of relapse have been reported than those seen with other medications [5]. However, in patients being tapered in anticipation of induction on to extended-release naltrexone (XR-NTX) , clonidine may permit more rapid induction and avoid the risk of precipitated opioid withdrawal [6]. An alternative alpha-2-adrenergic agonist, lofexidine, was approved by the FDA in 2018 for the treatment of opioid withdrawal. It is thought to have some safety advantages over clonidine since it produces less sedation and hypotension.
Withdrawal treatment begins with a complete drug and medical history, a complete physical examination, and urine toxicology. Even for patients on long-term BUP/NX or methadone treatment, it is difficult to accurately predict the patient’s level of physical dependence. It can also be highly risky to estimate the quantity and quality of street drugs. Very potent analogues of fentanyl may be present, often in drugs purchased by unsuspecting patients. The only way to avoid an inadvertent overdose or precipitated withdrawal is to evaluate the patient for signs of moderate opioid withdrawal before initiating withdrawal treatment. This should be done using a standard withdrawal scale such as the Clinical Opiate Withdrawal Scale (COWS) or the Objective Opioid Withdrawal Scale (OOWS) [7, 8] and documenting the results in the patient’s record. An initial dose of methadone 20 mg orally or BUP/NX 4/1 mg sublingually should not be administered until the patient scores in the mild to moderate range on the COWS or OOWS in an effort to mitigate the risk of overdose with administration of methadone and the risk of precipitated withdrawal with administration of BUP/NX (please see Fig. 5.2 and the associated description for further information). Lower initial doses of 10 mg methadone or 2/0.5 mg BUP/NX are recommended for younger patients or for individuals who have been using smaller amounts. For patients being transferred from maintenance programs, the clinician must always verify the dose and time of the last dose, before initiating any new medication.
Further dosing should be guided by the patient’s response as indicated on the COWS /OOWS . An additional dose can be administered in 2–4 hours if withdrawal symptoms increase or do not subside. If the initial dose was effective in controlling withdrawal, it should be repeated in 12 hours if needed. Ordinarily the total dose in the first 24 hours of methadone should not exceed 40 mg or 16/4 mg BUP/NX except for clinically indicated exceptions. Once withdrawal symptoms are adequately controlled, the dose can be tapered at a rate that prevents further withdrawal and minimizes distress. Methadone can be reduced at a rate of 5 mg/day (or a maximum 20% dose reduction/day). An inpatient methadone taper can usually be completed in 5–7 days [9]. BUP/NX can be tapered at the rate of 50%/day. A more gradual taper extending over 13 days had a better outcome and was significantly more effective than clonidine [10, 11]. One study compared withdrawal treatment utilizing clonidine, methadone, and BUP/NX [5]. Compared with clonidine, BUP/NX patients were more likely to complete treatment, stayed in treatment longer (particular in outpatient withdrawal treatment), and had fewer withdrawal symptoms [11]. The outcomes showed no significant difference comparing methadone to BUP/NX in completion of treatment or severity of withdrawal, but withdrawal symptoms resolved more quickly in BUP/NX-treated patients.
The long-term outcome of withdrawal treatment is rarely good [12, 13]. There is a relapse rate of 80–93% within 1 year following a brief inpatient taper. The best results have been seen with very prolonged outpatient tapers or 1–2 week inpatient tapers followed by long-term residential treatment. Better results are seen with multiyear maintenance treatment followed by a very gradual outpatient taper. Nonetheless, even very stable patients have shown a relapse rate of 80% within 1 year following a taper [13]. Patients must be warned about these risks if withdrawal treatment is not followed by long-term residential care or treatment with XR-NTX. Large data sets have shown an elevated risk for fatal overdose immediately following inpatient withdrawal treatment or following termination of long-term treatment with methadone or BUP/NX [14]. All patients must be made aware of these risks.
New protocols are under study utilizing rapid inpatient clonidine taper combined with an escalating dose of naltrexone leading to induction on to XR-NTX . In some protocols, naltrexone is used to precipitate withdrawal, and then increasing doses of clonidine are used to suppress withdrawal symptoms as naltrexone is quickly increased to antagonist maintenance levels [15, 16]. These protocols often require initiation with very low doses of naltrexone that are not available formulations. Clinicians continue to seek out effective models for inducing physically dependent patients on to XR-NTX . Recent research has showed comparable efficacy between BUP/NX and XR-NX, once the patient has been stabilized on either medication (see below) [17]. However, long-term retention in treatment remains an issue in standard clinical practice [18].
Recently, efforts have been made to incorporate non-pharmacological interventions in the treatment of acute withdrawal. One such example is a percutaneous electrical nerve field stimulation device which received FDA approval for the treatment of opioid withdrawal in late 2017 [19]. The device is placed on the external ear for 5 days to stimulate neurovascular bundles with the purpose of helping to alleviate symptoms of acute opioid withdrawal. The approval for this device was based on a small, uncontrolled, retrospective study which included 73 patients who saw a reduction in COWS scores from a baseline mean of 20.1 to 7.5 after 20 minutes, 4.0 after 30 minutes, and finally 3.1 after 60 minutes of wearing the device. It was also noted that of the 73 patient cohort, 64 patients transitioned to naltrexone after a 5-day course with the stimulation device [20]. There is limited evidence at this time for the role of non-pharmacological interventions in the treatment of acute opioid withdrawal; however, further study is needed.
In summary, it must be stressed that regardless of the medication or protocol used, medication withdrawal treatment for OUD has a poor outcome with more than 90% of patients relapsing within 1 year. All of these patients are at high risk for a fatal overdose. Unless withdrawal treatment is followed by long-term residential care (9 months or more), it should not be considered adequate treatment for OUD.
Maintenance Treatment
There is abundant evidence that long-term medication is the treatment of choice for most individuals with OUD [12, 17, 21, 22]. FDA-approved medications include the mu-opioid agonists methadone and buprenorphine or the antagonist, naltrexone. These treatment options have unique sets of advantages and disadvantages which need to be weighed for each patient individually.
Agonist Therapy
Any discussion of agonist therapy needs to first clarify what it is not; it is not a substitution of “one addiction for another.” Agonist therapy for OUD is the use of a long acting medication (either methadone or buprenorphine) as a daily medication to induce opioid tolerance and prevent opioid withdrawal and craving. This mode of therapy has been demonstrated to establish physiologic stability, improve general health and nutrition, decrease injection drug use, decrease criminal behavior, increase employment, and stabilize lifestyle [13]. Individuals who have responded well to these medications no longer present the behavioral symptoms associated with an OUD and no longer meet diagnostic criteria for opioid use disorder.
Buprenorphine
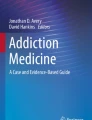
Buprenorphine, a partial agonist at the mu-opioid receptor , was approved by the FDA for the treatment of OUD in 2002. Safety and efficacy have been shown in a number of double-blind, placebo-controlled clinical trials [23,24,25,26]. It has a very high affinity for the mu-opioid receptor and it will displace other agonists (either natural opiates or synthetic or semisynthetic opioids) from the receptor. However, as a partial-agonist, it does not fully activate the receptor. This “ceiling effect ” prevents respiratory depression regardless of the amount ingested, making buprenorphine an unusually safe medication (Fig. 5.1). Because of its safety and its slow dissociation from the receptor, it provides long lasting receptor blockade, making it an ideal choice for the treatment of OUD.

Intrinsic activity of OUD medications. (Adapted from the Treatment Improvement Protocol 63 from the Substance Abuse and Mental Health Services Administration [62])
This Schedule III medication is available as either a single medication (mono-formulation ) or in combination with the antagonist naloxone (combo-formulation) in a ratio of approximately 4 mg buprenorphine to 1 mg naloxone. The combo-formulation was developed for sublingual use, to discourage diversion and misuse. Because naloxone has poor sublingual bioavailability, it has no clinical effect when taken as prescribed ensuring that the patient receives the full, intended buprenorphine effect. However, should the combo-formulation be crushed and injected, the naloxone is active, either blunting the effect of the buprenorphine or precipitating full opioid withdrawal in physically dependent individuals. Buprenorphine is now available in sublingual or buccal formulations , as a 6-month implantable rod, or as a monthly subcutaneous injection. Available branded or generic formulations (in some cases, tablets or film strips) include sublingual formulations, either alone (Subutex®) or in a combination formulation with naloxone (Bunavail®, Suboxone®, and Zubsolv®), a 6-month implant (Probuphine®), and a monthly injectable (Sublocade®).
Because of its combination of clinical efficacy, safety, and lesser diversion potential, the FDA and the Drug Enforcement Administration (DEA) approved buprenorphine for the treatment of OUD in the office-based setting without the regulatory constraints placed on methadone treatment. The introduction of office-based treatment for OUD has been a major public health success [27]. Patients have been attracted to the greater flexibility of office-based treatment and the faster induction on to buprenorphine, as compared to methadone. Methadone, however, has higher retention rates and may be a better option for patients who require closer monitoring and a broader range of ancillary services. It is recommended that all maintenance patients be engaged in individualized psychosocial supports, which can be delivered by patients’ healthcare providers in the form of medication management and supportive counseling and/or through adjunctive addiction counseling, recovery coaching, mental health services, and ancillary supports that may be necessary (TIP 63 from SAMHSA).
The DATA 2000 legislation indicated that to qualify for buprenorphine treatment, an individual must be 16 years of age and meet the DSM-IV criteria for opioid dependence. This is currently interpreted as meeting Diagnostic and Statistical Manual of Mental Disorders, 5th edition criteria for OUD, moderate or severe. As compared to methadone regulations, this permits the treatment of younger people with shorter addiction histories. Initial data from buprenorphine treatment found that patients who were younger, white, primarily used prescription opioids, and had greater stability were more likely to utilize buprenorphine treatment. More recently, evidence has demonstrated the effectiveness of buprenorphine in more marginalized and complex patient populations, including people recently incarcerated, people experiencing homelessness, people who inject opioids, and patients engaging in lower threshold settings (see, e.g., [28,29,30,31]).
Obtaining the DEA Buprenorphine Waiver
DATA 2000 legislation specified a number of ways for a physician to obtain the waiver to prescribe buprenorphine. Individuals could apply if they were certified in addiction psychiatry by the American Board of Psychiatry and Neurology, or certified in addiction medicine by the American Board of Addiction Medicine, or if they completed an 8-hour training course. The clinician’s patient load is capped to 30 for the first year. After holding a waiver for 1 year, clinicians can apply for an increase to treat up to 100 patients. The Comprehensive Addiction and Recovery Act of 2016 (CARA) legislation and Substance Abuse and Mental Health Services Administration (SAMHSA) regulations of 2016 now permit certain clinicians to apply for an increased waiver limit of 275 patients after 1 year at the 100 patient limit [32, 33]. These regulations also permit nurse practitioners and physician assistants to apply for the waiver, but they are required to complete 24 hours of training. By 2017, more than 35,000 physicians had obtained the DEA waiver to prescribe buprenorphine. Of those physicians with the waiver, 23,982 can prescribe for up to 30 patients, 9285 for up to 100 patients, and 2525 for up to 275 patients. It is estimated that there are now over 600,000 patients being treated in the office-based setting, and an additional 12,500 receiving buprenorphine in opioid treatment programs, compared with 350,000 patients on methadone maintenance.
Clinical Use of Buprenorphine
Initiating buprenorphine treatment requires a clear understanding of the drug’s pharmacology. As a partial opioid agonist, it has a very high affinity for the mu-opioid receptor, and it will displace most other opioid agonists. Because it does not fully activate the receptor, any individual physically dependent on a full opioid agonist will experience this displacement as the acute onset or severe worsening of opioid withdrawal symptoms, a syndrome called “precipitated withdrawal .” This severe but brief syndrome is comparable to the effects of treatment with an opioid antagonist. The important clinical task of buprenorphine induction is to introduce the medication while not causing precipitated withdrawal. This problem can be avoided by waiting until the patient is opioid free or already in mild to moderate opioid withdrawal before administering the first dose of buprenorphine. This is best accomplished by instructing the patient to avoid any opioids for 12–24 hours for short acting opioids and at least 24 hours for long acting opioids prior to induction and by documenting the presence of withdrawal using a standard scale such at the COWS. The COWS scores patients on observable measures including pulse, sweating, restlessness, pupil size, tremor, yawning, runny nose/tearing, and goose flesh and more subjective measures such as bone or joint aches and abdominal cramps, permitting a reliable measure of the severity of withdrawal (Fig. 5.2) [8].

Precipitated withdrawal if buprenorphine displaces full agonist conceptual representation only, not to be used for dosing purposes. (Adapted from the Treatment Improvement Protocol 63 from the Substance Abuse and Mental Health Services Administration [62])
To avoid precipitated withdrawal, the patient should demonstrate mild to moderate opioid withdrawal (>12) on the COWS before he or she takes the first buprenorphine dose. If the patient has been using a more potent opioid such as fentanyl, we recommended that induction not begin until they have demonstrated a higher level of withdrawal in the range of 13–15 on the COWS. In observed induction, an initial dose of BUP/NX 2/0.5 mg or BUP/NX 4/1 mg sublingually is given under observation and the patient is observed for an additional 1+ hours to ensure that there is no precipitated withdrawal. Supplemental doses can be given if withdrawal symptoms persist, with a maximum recommended first-day dose of BUP/NX of 16/4 mg.
Home induction, or unobserved induction , is an alternative option which has been demonstrated to be non-inferior to observed induction [34]. A home induction involves giving a patient an initial prescription for BUP/NX to take up to 16/4 mg on day one with careful instructions on the induction process. These patients can be monitored daily by telephone to ensure a safe and effective induction and seen for close follow-up in the office. The dose can be increased in 2–4 mg increments over the next 2–3 days to a dose that eliminates any further craving or withdrawal symptoms. The target maintenance dose was initially thought to be between 12 and 16 mg BUP/NX sublingually daily; however increasing evidence has demonstrated that higher doses (16–32 mg) are associated with improved treatment retention [35, 36]. Additional dose increases may be considered if craving and opioid use does not cease or diminish within 1–3 weeks.
In some circumstances it may be appropriate to initiate buprenorphine treatment in individuals not currently physically dependent (individuals recently released from residential care or from the justice system). Toxicology testing should be obtained to document their opioid negative status. Dosing should begin with BUP/NX 2/0.5 mg sublingually the first day and increase by 2/0.5 mg daily until a stabilization dose is achieved. If the patient experiences any level of sedation or intoxication, the dose should be reduced or further increases held until there is no further evidence of intoxication.
Buprenorphine has a long half-life, and clinicians should wait 5–7 days after initial stabilization or after any further dose increases to assess the full clinical response. The FDA-approved dosing range is 4–24 mg. Studies on receptor occupancy suggest that there is little pharmacological justification for doses over 32 mg [37]. The implant formulation was approved in 2016 and is only recommended for stable patients currently on a sublingual BUP/NX dose of 8/2 mg [38]. Additionally, the monthly injectable buprenorphine depot formulation was approved in 2017 which provides greater flexibility in dosage when compared to the implant formulation . As with the implant formulation, before transitioning to the depot formulation the patient must have been on a stable dose of transmucosal buprenorphine. The depot requirements differ in that the transmucosal dose could be between 8 and 24 mg as long as the dose has been stable for at least 7 days before initiating the depot formulation. Furthermore, after the first 2 months of 300 mg depot injections, the dose of the injection decreases to 100 mg, but the dose can be titrated back up to 300 mg if clinically indicated [39].
Weekly office visits are generally recommended for the first 3–4 weeks, with a gradual increase in duration between appointments as clinically indicated. Frequent monitoring visits and regular toxicology testing are associated with the best outcomes. As such, even very stable patients should generally be seen once every 1–2 months.
Patients treated with buprenorphine can benefit from individualized psychosocial supports. These can range from medication management and supportive counseling offered by the patients’ provider to more intensive adjunctive group or individual counseling, ancillary services, and mutual support (TIP 63 SAMHSA). Patients with significant co-occurring psychiatric problems may do best with adjunctive counseling. There have been four studies in both primary care and mental health settings that have shown that more stable patients may do just as well with less intensive ancillary services. Medication management with supportive counseling in the setting of a prescriber visit has been demonstrated to be an effective management tool for selected patients with no serious co-occurring medical or psychiatric disorders. The patients were seen either weekly or monthly for 15–25-minute individual visits. The clinician would monitor adherence, response to treatment, and any adverse effects. They would also provide education about alcohol use disorder/OUD, health consequences, and treatments, encourage abstinence from illicit opioids and other addictive substances and participation in community supports for recovery, and encourage other lifestyle changes that support recovery [12, 40,41,42]. The World Health Organization recommends that all patients with OUD be offered psychosocial interventions with buprenorphine but that people who decline additional counseling should not be denied medication treatment [43].
Buprenorphine has also shown promise as a treatment for pregnant women with OUD. The “MOTHER” study was a double-blind, double-dummy randomized control trial of buprenorphine versus methadone for pregnant women. The results showed comparable safety and equivalent reductions of illicit opioids and other substance use with both medications. There were higher dropouts in the buprenorphine condition but higher rates of medical complications at delivery in the methadone condition. Of particular note were the milder withdrawal symptoms seen in infants born to the mothers on buprenorphine [44, 45]. It is anticipated that buprenorphine will soon become accepted as standard care for pregnant women with opioid use disorder. For women who become pregnant while being treated with buprenorphine, it is recommended that they be transferred from the BUP/NX combo-formulation to the mono-formulation and that they be referred for prenatal care while being continued on buprenorphine [46].
There is little information available on the interaction of buprenorphine and other medications. Like methadone it is a substrate of cytochrome P450(CYP)3A4 , but unlike methadone, it has an active metabolite, norbuprenorphine, which appears to moderate the effect of other drugs that may induce buprenorphine metabolism. Drugs that inhibit CYP3A4, such as nefazodone or fluoxetine, could theoretically cause problems, but little difficulty has been reported. Of greater concern is the pharmacodynamic interaction between buprenorphine and sedating drugs such as benzodiazepines and antihistamines. Buprenorphine should be used with caution in patients with active, severe benzodiazepine use disorder, although the risks are less than among people treated with methadone and misusing benzodiazepines [47]. Overall, buprenorphine has fewer drug-drug interactions than methadone and can be prescribed more easily to a broader range of patients.
Methadone
Methadone was the first medication approved by the FDA for maintenance treatment of OUD. It acts as a full agonist at the mu-opioid receptors as well as an N-methyl-D-aspartate receptor antagonist. Treatment with methadone along with supportive services is highly effective as a maintenance treatment, with those in treatment for 6 months showing a substantial decrease in illicit opioid use. Treatment retention is higher with methadone maintenance compared to prolonged and psychosocially enriched withdrawal management [48], and opioid use is lower among those treated with methadone compared to other types of addiction treatment [49]. Ball and Ross noted that there was a nearly 80% decrease in crimes committed by patients after successful treatment in the methadone clinic [13]. Additionally, when comparing individuals engaged in illicit opioid use to those on long-term methadone maintenance, there remains some endocrine dysfunction such as hypogonadism in both groups, but there also appears to be an allostasis that occurs with long-term methadone use which stabilizes some endocrine physiology. This stabilization is most notable in the hypothalamic-pituitary-adrenal axis [10].
The use of methadone is strictly regulated in the United States and only available to patients for the treatment of OUD in designated treatment programs. Specific guidelines that were established in Title 42 of the Code of Federal Regulations (42 CFR) require that patients must be 18 years of age and older and have a documented 1-year history of addiction to opioids prior to treatment. According to 42 CFR patients less than 18 years of age can be treated with methadone with parental or guardian consent, if they have had two documented previous treatment attempts in the previous 12-month period. Additionally, it is possible to waive the 1-year history of OUD for patients previously treated with methadone, patients who are pregnant, or for patients within 6 months of incarceration. There are two exceptions when methadone can be prescribed for the treatment of OUD outside of a designated treatment program . These exceptions are (1) during emergent care (such as in the emergency department, for no longer than a period of 3 days) and (2) while receiving care as an inpatient for a medical or psychiatric condition other than addiction treatment [50].
Methadone Induction
In contrast to buprenorphine, methadone is a full mu-opioid agonist which does not display the ceiling effect seen in buprenorphine in regard to respiratory depression. This is an important consideration when initiating methadone treatment and when evaluating other medications that are concomitantly being prescribed, such as benzodiazepines. Methadone has a long half-life of 8–59 hours and an analgesic effect lasting about 4–8 hours. The respiratory depressant effects of methadone peak later and last longer than the analgesic effects, so great care must be taken in titration. Fatal overdoses have occurred if the dose is increased too quickly, most frequently seen when methadone is prescribed for pain rather than by an opioid treatment program for addiction. Unlike with buprenorphine there is no risk of precipitated withdrawal with methadone, so it is not necessary that a person be in withdrawal when initiating treatment. Generally, in opioid treatment settings, dosing is initiated when withdrawal symptoms are present to confirm the presence of physiological dependence; however individuals who have not been recently using opioids but are at high risk of relapse such as those released from incarceration should still be initiated in treatment at a lower initial dose. Federal regulations limit the initial oral induction dose to 30 mg, and the total first day dose to a maximum of 40 mg. The next daily dose may be increased to a maximum of 50 mg if withdrawal symptoms are still present. During subsequent days, the dosage increase should not be greater than 10 mg per week as it is important to reach a steady-state concentration before escalating to avoid potentially toxic dose accumulation [51]. The target dose range for most patients is 80–100 mg which should eliminate craving and illicit opioid use. Doses may be titrated up or down based on clinical effect. There is tremendous individual variation in methadone pharmacokinetics, and some patients may require much higher dosages [52].
Methadone is metabolized in the liver by CYP3A4, CYP2D6, and possibly also CYP1A2. However, the majority of the N-demethylation of methadone to an inactive metabolite is done by CYP3A4, and the great variability of this isoenzyme seems to relate to the large range of half-life in individuals. Caution should be taken when evaluating concurrent medications that are known to induce or inhibit these enzymes of metabolism, as well as in patients with hepatic insufficiency [52]. There has also been some concern about the effects of consumption of grapefruit juice on plasma levels of methadone, which has been shown to have a modest effect with an increased bioavailability of methadone [53]. Constipation is a common side effect, and consideration should be given to prescribing a bowel regimen in addition to methadone. Drug-drug interactions can be expected with methadone, and many of the medications are used to treat HIV/AIDS, seizure disorders, and tuberculosis.
Lastly, there is a boxed warning with methadone for the potential to cause a prolonged QTc interval and serious arrhythmias , such as torsades de pointes. This is particularly noteworthy in patients on doses of methadone over 100 mg and should be taken into consideration in any patient with a history of syncope, a cardiac history, or a familial long QT. In patients at risk, it would be appropriate to monitor the QTc interval with an electrocardiogram prior to initiating treatment and during treatment at a frequency that is appropriate for each patient’s individual risk.
Methadone is currently regarded as the “gold-standard” for pharmacological treatment of OUD during pregnancy . Fetal outcomes are improved when the mother is engaged in a methadone treatment program. Breastfeeding should be encouraged while taking methadone, as long as there are no contraindications noted. Although there are case reports of sedation and respiratory depression in some nursing infants, there is poor correlation between maternal methadone dose and infant symptomatology . In addition, concentrations of methadone in breast milk are low supporting the American Academy of Pediatrics recommendation to breastfeed regardless of methadone dose [54]. Despite the known benefit of breastfeeding among women treated with methadone, there continues to be a lack of support from the healthcare community and misinformation which present significant barriers to breastfeeding success [55].
Antagonist Therapy
Naltrexone
The only opioid antagonist that is FDA approved for maintenance therapy is naltrexone, which acts as a competitive antagonist at the mu-opioid receptor with long-lasting effects (generally about 24 hours per oral dose). In most patients, compliance with the oral formulation has been very poor. Efficacy for the treatment of OUD with the daily oral formulation has been better for patients in a formal and supervised setting, such as court ordered programs or physician monitoring programs, where adherence can be monitored. For the general population, compliance with the oral formulation is a problem, and it is strongly recommended that patients be prescribed the extended-release formulation of naltrexone (XR-NTX) which is given by intramuscular injection every 28 days. Prior to initiation of either the oral or XR-NTX medication, toxicology should be performed as naltrexone will precipitate opioid withdrawal if any amount of exogenous opioid is present. The patient must be abstinent from opioids for 7–10 days prior to induction.
A naloxone challenge test is recommended in patients when there is concern for precipitating withdrawal. This test involves giving a dose of naloxone to a patient when there are no longer any signs or symptoms of opioid withdrawal, and monitoring their response for 1 hour. If the naloxone precipitates signs or symptoms of opioid withdrawal, this should be relatively short lived due to the short half-life of naloxone. Naltrexone should not be initiated until there is no evidence of risk for precipitating withdrawal. Liver function testing should also be done prior to initiation and during treatment for monitoring, as naltrexone can rarely be hepatotoxic. It is often clinically determined that the benefit of the medication outweighs the risk of hepatotoxicity in cases of mild transaminitis, but it is contraindicated to use naltrexone if the patient is in liver failure [56].
A frequent barrier to success with XR-NTX is the induction process, since many patients are unable to achieve the required 7–10 days of abstinence prior to initiation of the medication. There have been several protocols developed to address this problem, as described above in the section on the treatment of withdrawal, such as very low dose naltrexone introduced orally and titrated up over 7 days to the daily dose of 50 mg at which point the patient can be transitioned to the XR-NTX [6]. With this approach it is anticipated that more patients would be induced on to XR-NTX . The efficacy of XR-NTX has been studied in comparison to sublingual buprenorphine. In intention-to-treat analysis, buprenorphine was superior to naltrexone with relapse detected in a greater percentage of XR-NTX -treated patients than buprenorphine-treated patients (65% compared to 57%). There was no statistically significant difference in outcomes in the two groups when comparing only those who were successfully induced on to either medication, but 28% of the XR-NTX group was not able to successfully complete induction, as compared to 6% of the buprenorphine group [18, 57]. Clinically, the use of XR-NTX is likely the best choice for patients in the following categories: those who are highly motivated, are unable to receive agonist treatment (due to availability or employment restrictions), and those who are able to complete medically supervised withdrawal to get to successful XR-NTX initiation.
Diversion Control
When prescribing any medication , the clinician must determine whether or not the risk is outweighed by the benefit. In the case of controlled substances, an important consideration when calculating risk is whether or not the medication is being used as prescribed. The CARA legislation required that clinicians develop a diversion plan to reduce diversion in their practice [33]. This must be reviewed periodically with their patients. Aside from misuse of the controlled substances, prescribers must also be alert to warning signs that the medication is being diverted. Clinically, toxicology can be a helpful tool to help monitor whether or not the substance is being ingested by the patient and if there are concurrent illicit or non-prescribed substances being used. It is important to coordinate with the testing laboratory to determine which substances are detectable in each assay, as a typical “opioid screen” may not include substances such as fentanyl or buprenorphine, or other opioid pharmaceuticals. Confirmation testing is also recommended if applicable, as the screening assays are often designed to have a high sensitivity, which can produce a relatively high percentage of false positives. The use of pill counts may also be implemented, with the patient being randomly requested to present between scheduled clinic visits to monitor whether an appropriate amount of medication remains.
Another important tool is the utilization of prescription drug monitoring programs (PDMPs) . PDMPs are state specific databases that can be searched by prescribers to receive a report of the recent prescriptions of controlled substances in that respective state. More recently, state PDMPs have been sharing data so that prescribers can query results from other states in addition to their own. A meta-analysis of studies on the overall impact of PDMPs on overdose showed insufficient evidence, with some studies demonstrating reduced overdoses and others showing an increase in heroin-related deaths [58].
Non-pharmacological Treatment
There has been some recent interest in the use of non-pharmacological interventions for the treatment of substance use disorders. Primarily, research is occurring to establish whether or not there is a role for deep brain stimulation (DBS) as well as repeated transcranial magnetic stimulation (rTMS) . The current focus of rTMS studies has been addiction to nicotine, alcohol, and stimulants, with most focusing on nicotine. Furthermore, there have been a few case reports of the use of DBS showing some potentially limited effects in decreasing use of opioids. The number of patients in the case reports for DBS is very low and the procedure is invasive, requiring placement of the electrode by neurosurgery. There is insufficient evidence to recommend use of these treatments at this time.
Treatment of Opioid Overdose
All patients with OUD should receive education about opioid overdose prevention and should be prescribed a naloxone rescue kit. Particularly, those who have recently completed medical withdrawal treatment or have been abstinent from opioids for a significant period of time should be warned about the loss of tolerance and increased risk of overdose if they resume the use of opioids. It would also be wise to provide overdose prevention education to patients who misuse illicit substances other than opioids, such as stimulants, designer drugs, or counterfeit medications, as these may be prepared in facilities that also process fentanyl and could be contaminated with this potent opioid.
When approaching an unconscious person who is not breathing, the possibility of opioid poisoning should be high on the differential. Signs of opioid poisoning are respiratory depression, cyanosis, miosis (with the exception of poisoning with meperidine), and a limp body. Initial management is to dial 911 and to ask for help from bystanders, specifically requesting an automated external defibrillator (AED) and naloxone. After determining that the environment is safe to intervene physically, initiate cardiopulmonary necessitation (CPR) until either an AED or naloxone arrives, at which point CPR should pause to utilize these aids. Naloxone should be used immediately whenever available, via intranasal or intramuscular delivery. Repeated doses of naloxone may be required. If there is no response to naloxone even after repeated dosages, continue CPR and use the AED until additional help arrives. If there is a response to naloxone, continue to monitor and provide appropriate care as indicated until additional help arrives. It is necessary to warn patients that the effect of naloxone is short-lived, and if the opioid ingested has a longer half-life than naloxone, respiratory depression could resume without subsequent treatment. When providing care after an overdose, a thorough evaluation for safety should occur to help determine whether it was an accidental poisoning or a suicide attempt. All overdose patients should be referred for treatment for a substance use disorder. At the very least, there should be a referral placed for mental health services following acute treatment [59].
The introduction of intranasal naloxone was correlated with a rapid and drastic decrease in the amount of heroin-related deaths shown in data from the San Francisco Medical Examiner’s reports from 1993 to 2010 [60]. Despite this strong evidence of utility, concerns have been raised about the potential legal implications of providing medical care in an overdose scenario. As such, most states, but not all, have Good Samaritan laws in place to help promote intervention. It is recommended that each provider be aware of the laws specific to the state in which they practice.
Additional Considerations
Acute Pain
When patients with OUD are experiencing acute pain, special care must be taken when providing treatment. Single daily doses of methadone or buprenorphine do not provide 24-hour analgesia. Mild to moderate acute pain can usually be managed with the addition of non-opioid analgesics such as nonsteroidal anti-inflammatory drugs (NSAID) to the daily maintenance medication. If that is not adequate, the daily buprenorphine dose can be divided to provide better analgesia and supplemented with an additional 2/0.5 mg BUP/NX as needed for breakthrough pain. In methadone patients, their daily maintenance dose can be supplemented with an additional 10 mg methadone or another full agonist as needed. In cases of severe pain in patients receiving agonist treatment with buprenorphine, supplemental doses of a full agonist may be added, or it may be necessary to transition from buprenorphine to a full agonist to provide necessary analgesia and then re-induce buprenorphine after the pain subsides [TIP 63 from SAMHSA]. For the management of the pain associated with childbirth, the mother should continue on her normal maintenance dose of methadone or buprenorphine and then should also be treated with standard of care acute pain management options.
If a patient on opioid antagonist treatment experiences acute pain, it may be necessary to involve anesthesia to administer agents such as ketamine or to utilize high doses of fentanyl or buprenorphine to override the naltrexone blockade. As with any patient, caution should be taken to prescribe opioid medications only when clinically appropriate. Alternatives to opioids such as NSAIDs and nerve blocks should be considered whenever appropriate.
Concurrent OUD and Other Mental Illness
It is not uncommon to encounter OUD in patients also diagnosed with additional mental health disorders. Data from the National Survey on Drug Use and Health examining patients aged 18 and older from 2008 to 2014 estimated that of the 20.2 million diagnosed with a substance use disorder, 7.9 million also had additional mental health diagnoses. When treating these “dual-diagnosis” patients , it is important to coordinate care with all members of the treatment team and carefully consider medication choices. Medications with misuse potential, especially those that have profiles of having a rapid onset and a short half-life, such as some benzodiazepines, should be avoided [61]. Otherwise, patients on any of the approved medications for OUD will respond to the standard pharmacotherapies and psychological interventions for other mental health disorders. Methadone metabolism maybe altered by some of the psychiatric drugs metabolized by the CYP3A4 system; this is not an issue for naltrexone or buprenorphine.
Integrating Medication Treatment into a Comprehensive Recovery Program for OUD
Research has shown that long-term medication treatment for OUD is an essential element of recovery and that short-term treatment providing only medically supervised withdrawal is rarely an effective strategy [62]. Nonetheless, most patients will also benefit from a full range of psychosocial services to support stable recovery. Structured individual or group counseling based on cognitive behavioral models has the best evidence for efficacy, though patients should also be encouraged to participate in mutual support programs which are highly associated with long-term recovery. For patients on methadone or buprenorphine, participation in Alcoholics Anonymous (AA) may be more beneficial than Narcotics Anonymous (NA) since the AA fellowship is more accepting of patients on medication. Alternative mutual help organizations such as SMART Recovery are also more accepting of medication treatments, although evidence for recovery-related benefits specifically from SMART Recovery participation is limited. Whenever possible, families should also be engaged in the treatment process. Finally, and equally important, all patients with OUD should be screened for co-occurring psychiatric disorders. Given the high prevalence of co-occurring disorder, identifying psychiatric illness and offering concurrent treatment are crucial. Recovery is unlikely unless these conditions are also treated. It is useful to consider medication for OUD as a platform for recovery. It is necessary to support recovery, but patients should also have access to a full range of addiction services to promote successful recovery. While access to comprehensive psychosocial services must be available to all, designing systems which mandate participation may limit access for certain marginalized patient populations. By contrast, lower threshold treatment models which make medication readily accessible in conjunction with voluntary participation in comprehensive services that meet the needs of the individual patient are more likely to create the broad access that is needed to ensure the greatest number of individuals with OUD is able to get lifesaving treatment.
References
Musto DF. The American disease: origins of narcotic control. 3rd ed. New York: Oxford University Press; 1999.
Dole VP, Nyswander M. A medical treatment for diacetylmorphine (heroin) addiction: a clinical trial with methadone hydrochloride. JAMA. 1965;193:646–50.
Kosten TR, Kleber HD. Buprenorphine detoxification from opioid dependence: a pilot study. Life Sci. 1988;42:635–71.
Porter J, Jick H. Addiction rare in patients treated with narcotics. N Engl J Med. 1980;302(2):123.
Gowing L, Ali R, White J. Buprenorphine for the management of opioid withdrawal (Cochrane review). Cochrane Database Syst Rev. 2006;(2):CD002025.
Sullivan M, Bisaga A, Pavlicova M, et al. Long-acting injectable naltrexone induction: a randomized trial of outpatient detoxification with naltrexone versus buprenorphine. Am J Psychiatry. 2017;174:459–67.
Handelsman L, Cochrane KJ, Aronson MJ, et al. Two new rating scales for opiate withdrawal. Am J Alcohol Abuse. 1987;13:293–308.
Wesson D, Ling W. The clinical opiate withdrawal scale (COWS). Psychoactive Drugs. 2003;35(2):253–9.
Polydorou S, Kleber HD. Detoxification of opioids. In: Galanter M, Kleber HD, editors. Textbook of substance abuse treatment. 4th ed. Washington, DC: American Psychiatric Publishing; 2008.
Kreek MJ, Wardlaw SL, Hartman N, et al. Circadian rhythms and levels of beta-endorphin, ACTH, and cortisol during chronic methadone maintenance treatment in humans. Life Sci. 1983;33(Suppl 1):409–11.
Ling W, Amass L, Shoptaw S. A multi-center randomized trial of buprenorphine-naloxone versus clonidine for opioid, detoxification: findings from the National Institute on Drug Abuse Clinical Trials Network. Addiction. 2005;100(8):1090–100.
Weiss RD, Potter JS, Fiellin DA, et al. Adjunctive counseling and brief and extended buprenorphine-naloxone treatment for prescription opioid dependence. Arch Gen Psychiatry. 2011;68(12):1238–46.
Ball J, Ross A. The effectiveness of methadone maintenance treatment. New York: Springer; 1991.
Sordo L, Barrio G, Bravo MJ, et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies. BMJ. 2017;357:j1550.
O’Connor PG, Waugh ME, Carroll KM, et al. Primary care-based ambulatory opioid detoxification: the results of a clinical trial. J Gen Intern Med. 1995;10:255–60.
Riordan CE, Kleber HD. Rapid opiate detoxification with clonidine and naloxone (letter). Lancet. 1980;1:1079–80.
Lee JD, Nunes EV Jr, Novo P, et al. Comparative effectiveness of extended-release naltrexone versus buprenorphine-naloxone for opioid relapse prevention (X:BOT): a multicentre, open-label, randomised controlled trial. Lancet. 2018;391:309.
Gowing L, Ali R, White J. Opioid antagonists with minimal sedation for opioid withdrawal (Cochrane review). Cochrane Database Syst Rev. 2006;(1):CD002021.
United States Food and Drug Administration News Release. FDA grants marketing authorization of the first device for use in helping to reduce the symptoms of opioid withdrawal. Available at https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm585271.htm. Accessed on 30 July 2018.
Miranda A, Taca A. Neuromodulation with percutaneous electrical nerve field stimulation is associated with reduction in signs and symptoms of opioid withdrawal: a multisite, retrospective assessment. Am J Drug Alcohol Abuse. 2018;44:56–63.
Mattick RP, Hall W. Are detoxifications programmes effective? Lancet. 1996;347:97–100.
O’Connor PG, Oliveto AH, Shi JM, et al. A randomized trial of buprenorphine maintenance for heroin dependence in a primary care clinic for substance users vs a methadone clinic. Am J Med. 1998;105:100–5.
Jones CM, Logan J, Gladden RM, et al. Vital signs: demographic and substance use trends among heroin users – United States, 2002–2013. MMWR Morb Mortal Wkly Rep. 2015;64(26):719–25.
Kakko J, Svanborg KD, Kreek MJ, et al. 1-year retention and social function after buprenorphine-assisted relapse prevention treatment for heroin dependence in Sweden: a randomized, placebo-controlled trial. Lancet. 2003;361(9358):662–8.
Ling W, Charuvastra C, Collins JF, et al. Buprenorphine maintenance treatment of opiate dependence: a multicenter, randomized clinical trial. Addiction. 1998;93:475–86.
Strain EC, Stitzer ML, Liebson IA, et al. Comparison of buprenorphine and methadone in the treatment of opioid dependence. Am J Psychiatry. 1994;151:1025–30.
Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Prescription drug use and misuse in the United States: results from the 2015 National Survey on Drug Use and Health: HSDUH data review. Retrieved from http://samhsa.gov/data/.
Bhatraju EP, Grossman E, Tofighi B, McNeely J, et al. Public sector low threshold office-based buprenorphine treatment: outcomes at year 7. Addict Sci Clin Pract. 2017;12(1):7.
Alford DP, LaBelle CT, Richardson JM, O’Connell JJ, Hohl CA, Cheng DM, Samet JH. Treating homeless opioid dependent patients with buprenorphine in an office-based setting. J Gen Intern Med. 2007;22(2):171–6.
Potter JS, Marino EN, Hillhouse MP, Nielsen S, et al. Buprenorphine/naloxone and methadone maintenance treatment outcomes for opioid analgesic, heroin, and combined users: findings from starting treatment with agonist replacement therapies (START). J Stud Alcohol Drugs. 2013;74(4):605–13.
Riggins DP, Cunningham CO, Ning Y, Fox AD. Recent incarceration and buprenorphine maintenance treatment outcomes among human immunodeficiency virus-positive patients. Subst Abus. 2017;38(3):297–302.
Drug Addiction Treatment Act of 2000, Pub L, No. 106–310. Available at www.congress.gov/bill/106th-congress/house-bill/4365. Accessed 30 July 2018.
Comprehensive Addiction and Recovery Act of 2016, Pub L, No. 114–198. Available at www.congress.gov/bill/114th-congress/senate-bill/524. Accessed 30 July 2018.
Lee JD, Grossman E, DiRocco D, Gourevitch MN. Home buprenorphine/naloxone induction in primary care. J Gen Intern Med. 2009;24(2):226–32.
Fareed A, Vayalapalli S, Casarella J, Drexler K. Effect of buprenorphine dose on treatment outcome. J Addict Dis. 2012;31(1):8–18.
Hser YI, Saxon AJ, Huang D, Hasson A, et al. Treatment retention among patients randomized to buprenorphine/naloxone compared to methadone in a multi-site trial. Addiction. 2014;109(1):79–87.
Greenwald MK, Comer SD, Fiellin DA. Buprenorphine maintenance and mu-opioid receptor availability in the treatment of opioid use disorder: implications for clinical use and policy. Drug Alcohol Depend. 2014;144:1–11, 25179217.
Ling W, Casadonte P, Kampman KM, et al. Buprenorphine implants for treatment of opioid dependence: a randomized controlled trial. JAMA. 2010;304(4):1576–83.
SUBLOCADE – Prescribing information. Indivior Inc. North Chesterfield, VA. November 2017.
Ling W, Hillhouse M, Ang A, et al. Comparison of behavioral treatment conditions in buprenorphine maintenance. Addiction. 2013;108(10):1788–98.
Fiellin DA, Pantalon MV, Chawarski MC, Moore BA, Sullivan LE, O’Connor PG, Schottenfeld RS. Counseling plus buprenorphine-naloxone maintenance therapy for opioid dependence. N Engl J Med. 2006;355:365–74.
VA/DoD SUD Practice Guidelines 2015, p. 23. Available at www.healthquality.va.gov. Accessed 30 July 2018.
World Health Organization. Guidelines for the psychosocially assisted pharmacological treatment of opioid dependence. Available at: http://apps.who.int/iris/bitstream/handle/10665/43948/9789241547543_eng.pdf?sequence=1.
Jones HE, Kaltenbach K, Heil S, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363:2320–31.
Jones HE, Fischer G, Heil SH, Kaltenback K, Martin PR, Coyle MG, Selby P, Stine SM, O’Grady KE, Arria AM. Maternal Opioid Treatment: Human Experimental Research (MOTHER) – approach, issues and lessons learned. Addiction. 2012;107(Suppl 1):28–35.
Lund I, Fischer G, Welle-Strand G, O’Grady K, Debelak K, Morrone W, Jones H. A comparison of buprenorphine + naloxone to buprenorphine and methadone in the treatment of opioid dependence during pregnancy: maternal and neonatal outcomes. Subst Abus. 2013;7:61–74.
Lee SC, Klein-Schwartz W, Doyon S, Welsh C. Comparison of toxicity associated with nonmedical use of benzodiazepines with buprenorphine or methadone. Drug Alcohol Depend. 2014;138:118–23.
Sees KL, Delucchi KL, Masson C, Rosen A, et al. Methadone maintenance vs 180-day psychosocially enriched detoxification for treatment of opioid dependence: a randomized controlled trial. JAMA. 2000;283(10):1303–10.
Mattick RP, Breen C, Kimber J, Davoli M. Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence. Cochrane Database Syst Rev. 2009;(3):CD002209.
Code of Federal Regulations Title 42. Available at https://www.gpo.gov/fdsys/pkg/CFR-2007-title42-vol1/pdf/CFR-2007-title42-vol1-part8.pdf. Accessed on 30 July 2018.
Methadone package insert. Available at https://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM142842.pdf. Accessed on 30 July 2018.
Ferrari A, Coccia CP, Bertonlini A, Sternieri E. Methadone—metabolism, pharmacokinetics and interactions. Pharmacol Res. 2004;50(6):551–9.
Benmebarek M, Devaud C, Gex-Fabry M, Powell Golay K, Brogli C, Baumann P, Gravier B, Eap CB. Effects of grapefruit juice on the pharmacokinetics of the enantiomers of methadone. Clin Pharmacol Ther. 2004;76(1):55–63.
Bogen DL, Perel JM, Helsel JC, Hanusa BH, Thompson M, Wisner KL. Estimated infant exposure to enantiomer-specific methadone levels in breastmilk. Breastfeed Med. 2011;6(6):377–84.
Demirci JR, Bogen DL, Klionsky Y. Breastfeeding and methadone therapy: the maternal experience. Subst Abus. 2015;36(2):203–8.
Package insert for Vivitrol ®. Available at https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021897s015lbl.pdf (package insert for vivitrol). Accessed on 30 July 2018.
Tanum L, Solli KK, Latif ZE, et al. Effectiveness of injectable extended-release naltrexone vs daily buprenorphine-naloxone for opioid dependence: a randomized clinical noninferiority trial. JAMA Psychiat. 2017;74:1197.
Fink DS, Schleimer JP, Sarvet A, Grover KK, et al. Association between prescription drug monitoring programs and nonfatal and fatal drug overdoses: a systematic review. Ann Intern Med. 2018;168(11):783–90.
Opioid-associated life-threatening emergency (Adult) algorithm – New 2015. American Heart Association. Available at https://eccguidelines.heart.org/wp-content/uploads/2015/10/BLS-Opioid-Associated-Emergency-Algorithm.png. Accessed on 30 July 2018.
Office of the Chief Medical Examiner, City and County of San Francisco. Fiscal year annual reports. Available at https://sfgov.org/medexaminer/.
Substance Abuse and Mental Health Services Administration. Behavioral health trends in the United States: results from the 2014 National Survey on Drug Use and Health. Available at https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf. Accessed on 30 July 2018.
Substance Abuse and Mental Health Services Administration. Treatment improvement protocol 63. Medications for opioid use disorder, for healthcare and addiction professionals, policymakers, patients, and families. Available at https://store.samhsa.gov/shin/content/SMA18-5063FULLDOC/SMA18-5063FULLDOC.pdf. Accessed on 30 July 2018.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

{kind=link}
Cite this chapter
Renner, J.A., Crawford, M.B. (2019). Medication for the Treatment of Opioid Use Disorder. In: Kelly, J., Wakeman, S. (eds) Treating Opioid Addiction. Current Clinical Psychiatry. Humana, Cham. https://doi.org/10.1007/978-3-030-16257-3_5
Download citation
DOI: https://doi.org/10.1007/978-3-030-16257-3_5
Published:
Publisher Name: Humana, Cham
Print ISBN: 978-3-030-16256-6
Online ISBN: 978-3-030-16257-3
eBook Packages: MedicineMedicine (R0)