
Abstract
Breast conserving surgery (BCS), also known as quadrantectomy, sectorectomy, or lumpectomy, consists of surgical removal of the primary tumor, with negative margins and whole breast radiotherapy (RT). The addition of RT to conservative surgery reduces the local recurrence rate by 50%, with an impact on mortality at 15 years, according to a meta-analysis by the Early Breast Cancer Trialists Collaborative Group (EBCTCG), showing that the omission of radiotherapy in BCS is not recommended.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Breast conserving surgery (BCS), also known as quadrantectomy , sectorectomy, or lumpectomy , consists of surgical removal of the primary tumor, with negative margins and whole breast radiotherapy (RT). The addition of RT to conservative surgery reduces the local recurrence rate by 50%, with an impact on mortality at 15 years, according to a meta-analysis by the Early Breast Cancer Trialists Collaborative Group (EBCTCG), showing that the omission of radiotherapy in BCS is not recommended.
Oncologic Safety
Survival of BCS was equivalent to mastectomy in six randomized clinical trials , but patients in these studies experienced greater local recurrence (LR) when compared to radical surgery. The NSABP-06 study, for example, started in the 1970s, showed ipsilateral LR around 14%. The addition of systemic therapy, aimed at reducing distant metastases, also reduced local recurrences. In the 1990s, the NSABP trials had LR ranging from 3.5 to 6.5% in 10 years. Improvement in breast radiology, as well as pathologic evaluation, also contributed to this decrease in LR. Currently, available data suggest that LR is more related to tumor biology than to the surgical technique. Patients with triple-negative tumors have the highest rate of recurrence, either in BCS or mastectomy.
Surgical Technique
Besides adequate oncological control , the main objective of BCS is the maintenance of the corporal esthetics. Some dogmas have been incorporated into the surgical technique, although there is no scientific evidence to justify them. Systematic removal of the skin that is on the tumor, removal of the pectoral muscle fascia, resection of the percutaneous biopsy needle path, and the need to exit the drain near the cutaneous incision are examples of conducts that cause worse aesthetic outcome without improving local control and should therefore be avoided whenever possible.
There are several techniques outlined. In the simpler techniques, more cosmetic incisions are usually chosen, such as the periareolar or in the inframammary fold. Skin on the site can be mobilized, followed by tumor excision with macroscopic margins and appropriate guidance for histological analysis. The adjacent breast tissue can be approximated after resection, releasing any skin retractions and minimizing complications.
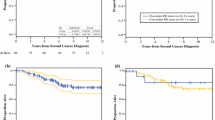
Occasionally, cutaneous incisions are necessary in other places. Arcuate incisions are preferably applied in the upper quadrant, while radial incisions are preferably applied in the inferior quadrants or on the lateral sulcus. Scars in the upper inner quadrant should generally be avoided, as shown in Fig. 1.

Preferential incisions in conservative breast operations. The demarcated area in the dashed line should be avoided
There is no fixed limit of tumor size, but the ideal situation is that tumors undergoing conservative techniques occupy up to 20% of the total volume of the breast. Above this ratio, oncoplasty techniques are generally necessary to obtain satisfactory results: in this scenario, the marking of the resection site of the neoplasia with metal clips can be done to guide the radiotherapy (boost).
Tumor Staging
The correct evaluation of the tumor extension is fundamental for a good performance of the surgery. Physical examination and mammography are usually sufficient in most cases. Some patients may need to be supplemented with ultrasonography and magnetic resonance imaging (MRI). The use of MRI is controversial. Some studies have shown an increase in the detection of new tumor foci in 6 to 34% of cases, more frequently in high-risk women and in women with invasive lobular carcinoma, although the multicentric/multifocal nature has been known for decades (the aim of BCS has never been to eradicate completely the disease found in the breast), and old randomized studies of BCS did not experience a higher recurrence rate due to the omission of MRI. The indication of the exam should therefore be assessed on a case-by-case basis, especially when there is suspicion of additional disease or when the imaging tests are inconclusive.
Surgical Margins
A margin is assessed by means of measuring the distance between the ink applied on the surface of the specimen for any tumor cell. The ideal minimum margin in BCS was a matter of debate for many years. This concern began in clinical practice after the main randomized studies on BCS: the only study that established free margin as criterion was the NSABP 06, and not touching the ink was the recommended distance. The other five classic studies did not establish a minimum margin criterion, and macroscopic resection of the tumor was sufficient, that is, the status of the margin was unknown. The rates of local recurrence were still high after the advent of BCS, and minimizing local recurrence is very important. Studies to evaluate this matter were necessary, since reoperation rates were very high, reaching 25%.
The meta-analysis published in 2014 by Houssami et al. [3, 4] met such need: using 33 studies, with 28,162 patients, 1506 cases of LR (5.3%) were observed; after 79.2 months of follow-up, no difference in LR taking margin distances of 1, 2, and 5 mm was found. This study concluded that positive margins affect local control, while the absence of ink on the tumor border (i.e., no cancer cells adjacent to any border) is considered adequate in the era of multidisciplinary therapy. Therefore, if the tumor does not “touch” the ink, the margin is negative. This is the current recommendation of the Society of Surgical Oncology (SSO), the American Society for Radiation Oncology (ASTRO), and the American Society of Clinical Oncology (ASCO) for invasive carcinoma, also recently endorsed during St. Gallen’s consensus in 2017. These recommendations have already had a significant impact on mastology, as reoperation rates have decreased and so have mastectomy rates, according to a recent study.
The margin in ductal carcinoma in situ (DCIS) was also recently discussed and a consensus published in 2016 stipulated 2 mm as the appropriate minimum margin, although free margins below this measurement may not need to be expanded and can be evaluated case by case. The meta-analysis published by Luke Marinovich, with 20 studies (8651 patients), showed that margins wider than 2 mm are not related to lower LR rates.
There are several techniques for evaluating the margins, the main ones being macroscopy, cytology and frozen section. There are no studies that conclude on the ideal technique; however, intraoperative evaluation has declined over the years, especially after the consensus of margins.
Adjuvant Treatment
The use of systemic therapy has a substantial impact on the reduction of LR. The Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) found that the 10-year LR rate with tamoxifen was 8.7% compared to 18.6% without hormone therapy, a relative reduction of just over 50%. In addition, the use of anthracycline or cyclophosphamide chemotherapy, methotrexate, and fluorouracil (CMF) reduced the relative risk of RL by 30% to 40%. Improvement in systemic treatment was also important: the use of aromatase inhibitors or prolonged endocrine therapy with tamoxifen followed by an aromatase inhibitor showed a 20% to 50% reduction in the risk of RL compared to treatment with tamoxifen alone, as well as the addition of taxane to anthracycline results in an even greater drop in LR. The target therapy, through trastuzumab in women with HER2 expression , showed a significant reduction in LR regardless of the surgery chosen, use of radiation therapy or menopausal status, according to a study by the Memorial Sloan Kettering Cancer Center.
Conclusion
Breast conserving surgery is the ideal treatment for most cases of breast cancer. The conditions for performing it are the following: the patient’s desire, possibility of oncological control, and preservation of breast aesthetics.
Flowchart

Steps for performing conservative breast surgery
Recommended Reading
Barrio AV, Morrow M. Appropriate margin for lumpectomy excision of invasive breast cancer. Chin Clin Oncol. 2016;5(3):35. Review of the literature on available data regarding the relationship between margin status and local control for invasive breast cancer and the impact of molecular subtypes and systemic therapy on local control.
Bodilsen A, Bjerre K, Offersen BV, Vahl P, Amby N, Dixon JM, Ejlertsen B, Overgaard J, Christiansen P. Importance of margin width in breast-conserving treatment of early breast cancer. J Surg Oncol. 2016;113(6):609–15. A cohort study with 11,900 women, with a follow-up period of 4.9 years, with LR rates of 2.4% in 5 years and 5.9% in 9 years. It showed increased LR rates significantly associated with young age (<50 years), estrogen receptor negative, grade III, more than 4 positive lymph nodes and re-intervention.
Houssami N, Macaskill P, Marinovich ML, Morrow M. The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2014;21(3):717–30. Meta-analysis on margins in invasive carcinomas. 33 studies, with 28,162 patients, found 1,506 cases of LR (5.3%), with a follow-up of 79.2 months. There was no difference in LR considering the distances of the margins of 1, 2 and 5 mm.
Houssami N, Turner RM, Morrow M. Meta-analysis of pre-operative magnetic resonance imaging (MRI) and surgical treatment for breast cancer. Breast Cancer Res Treat. 2017. Revisions on mammary staging with MRI with 19 studies concluded that preoperative MRI is associated with an increased indication of ipsilateral mastectomy and contralateral prophylactic mastectomy.
Marinovich ML, Azizi L, Macaskill P, Irwig L, Morrow M, Solin LJ, Houssami N. The association of surgical margins and local recurrence in women with ductal carcinoma in situ treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2016;23(12):3811–21. A meta-analysis of 20 studies evaluating patients with ductal carcinoma in situ and observing the LR according to the state of the margins. It has been shown that margins wider than 2 mm are not related to lower LR rates.
Author information
Authors and Affiliations
Consortia
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
BBSG – Brazilian Breast Study Group. (2019). Breast Conserving Surgery. In: Novita, G., Frasson, A., Millen, E., Zerwes, F., Cavalcante, F. (eds) Breast Diseases. Springer, Cham. https://doi.org/10.1007/978-3-030-13636-9_31
Download citation
DOI: https://doi.org/10.1007/978-3-030-13636-9_31
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-13635-2
Online ISBN: 978-3-030-13636-9
eBook Packages: MedicineMedicine (R0)