
Abstract
Crohn’s disease is a chronic transmural inflammatory condition that primarily affects the terminal ileum and colon; however, it can affect all portions of the gastrointestinal tract. The course that the disease takes is variable, often manifesting acute attacks on a chronic underlying potentially debilitating condition. Though Crohn’s disease, at this time, is not curable, the goal of treatment is to induce and maintain remission of the disease to control symptoms as well as decrease the complications from this disease. This is accomplished primarily through medications; however, surgery plays an important role in the treatment of this disease.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Crohn’s disease
- Incidence
- Prevalence
- Indications
- Preoperative evaluations
- Imaging
- Operative considerations
- Nutritional assessment
- Recurrence
-
Crohn’s disease is a chronic inflammatory bowel disease which primarily affects the terminal ileum and colon but can involve all portions of the GI tract.
-
Surgery is utilized in the treatment of Crohn’s disease when medical therapy fails to control the disease or when there are complications from the disease (obstruction, perforation, fistulization, bleeding).
-
Preoperative evaluation includes appropriate imaging, nutritional assessment, as well as consideration of current medications and comorbidities.
-
Surgical intervention for Crohn’s disease should seek to alleviate symptoms while preserving small bowel length whenever possible.
-
An ileocolic resection is the most common operative procedure performed on Crohn’s patients.
-
In cases of toxic colitis, aggressive medical therapy includes corticosteroids and/or rescue infliximab. If the patient fails to respond, total colectomy with end ileostomy is necessary.
Surgery in the Treatment of Crohn’s Disease
-
Crohn’s disease is a chronic transmural inflammatory condition that primarily affects the terminal ileum and colon and however can involve all portions of the gastrointestinal tract.
-
Transmural inflammation leads to the complications that are attributed to this disease including strictures, obstructions, fistula, and abscesses.
-
Although Crohn’s disease is not curable, the goal of treatment is to induce and maintain remission of the disease, to control symptoms, and decrease complications.
-
This is accomplished primarily through medications; however, surgery plays an important role in treatment.
-
The specific goals of the surgeon are to determine the ideal timing of surgery, maximize patient conditioning to decrease postoperative complications, preserve as much small bowel as possible, and decrease recurrence rates.
-
Thorough planning and preparation, as well as attention to the patient’s preoperative state including their overall health status, nutritional status, and current medication are all key factors that affect the outcome of surgery.
-
>90% of patients have significant relief or complete resolution of their symptoms after surgery.
Changing Trends in the Era of Immunomodulators and Biologics
-
Immunomodulators and biologics may impact the outcomes of surgical intervention.
-
The rate of surgical intervention for Crohn’s disease has decreased over the years, presumably owing to the advances in medical therapy.
-
The longer a patient has the disease, the more likely they are to need surgical intervention.
-
Patients that are younger than 40 years of age at the time of diagnosis are more likely to require surgical intervention.
-
Patients with terminal ileal or ileocecal disease are more likely to require surgery compared with those that present with colonic disease.
-
Those with a penetrating pattern of disease are more likely to require surgery.
-
Factors associated with earlier need for surgery included smoking, disease of the small bowel without colonic involvement, nausea, vomiting and abdominal pain at presentation, neutrophil count, and steroid use in the first 6 months of diagnosis.
-
Numerous studies have been done looking at the effect medications have had on outcomes.
-
Most studies support the finding that long-term use of anti-TNF therapy decreases the risk of surgery.
-
However, the data needs to be viewed carefully as many factors can confound analysis over time, including length of follow-up and improved diagnostics with earlier detection of the disease in more recent years.
-
Indications for Surgery
-
Crohn’s disease is a very complex and heterogeneous disease.
-
A multidisciplinary approach including the gastroenterologist, radiologist, and colorectal surgeon is ideal.
-
Non-emergent indications for surgery include failure of medical therapy, chronic obstruction, fistulas, abscesses, cancer, and occasionally quality of life issues.
-
The most common of these is failure of medical therapy to adequately control symptoms.
-
Emergent indications include acute obstruction, perforation, hemorrhage, and toxic colitis.
-
Failure of Medical Management
-
Thirty-three to 47% of patients have surgery for Crohn’s disease owing to failure of medical management.
-
Failure of medical therapy includes failure of the medications to control symptoms and unacceptable side effects from the medications.
-
Inability to wean off corticosteroids within 3–6 months is also considered failure of medical management.
-
Timing is important to avoid a worsening health status, development of malnutrition or weight loss, or need for escalating steroid dosages; all could have significant deleterious effects on surgical outcomes.
Obstruction
-
Approximately 20–25% of surgeries for Crohn’s disease are secondary to obstruction .
-
Transmural inflammation causes fibrosis and scarring; the resulting stricture can lead to chronic obstruction.
-
Since these strictures develop slowly over time, the bowel slowly accommodates to the obstruction.
-
Patients may experience intermittent crampy pain, bloating, and intolerance to certain foods.
-
Other etiologies of obstruction in Crohn’s patients include anastomotic stricture or cancer.
-
When a patient presents with obstructive symptoms, it is important to try to differentiate between an inflammatory stricture, a fibrotic stricture, and an anastomotic stricture.
-
An inflammatory stricture usually responds to steroids with symptomatic improvement of the patient without emergent surgical intervention.
-
Fibrotic strictures are more likely to ultimately require surgical intervention.
-
If the obstruction is secondary to an anastomotic stricture, endoscopic dilation may be employed.
-
-
Endoscopic balloon dilation can be considered as part of the therapeutic options for treatment of Crohn’s obstructions secondary to strictures.
Perforation
-
Free perforation is a rare indication for surgery for Crohn’s disease occurring only 1–3% of the time.
-
When this does occur, it is usually associated with a complete obstruction or toxic colitis.
-
Patients are often septic and require immediate surgical treatment.
-
Small bowel perforation is usually best treated with resection and primary anastomosis, with consideration of a proximal diversion.
-
Colonic perforation is typically treated by total abdominal colectomy with end ileostomy.
Bleeding
-
Massive hemorrhage is a rare event in Crohn’s disease accounting for only 2–13% of operations for Crohn’s disease.
-
The evaluation and treatment are similar to other etiologies of gastrointestinal bleed.
-
At presentation, the patient should be resuscitated and stabilized.
-
Next, an attempt to localize the source of the bleed is undertaken typically with endoscopic evaluation, bleeding scans, or the use of selective angiography.
-
Identification of the source is particularly important in this group of patients so that excessive and unnecessary bowel resection is not performed. Localization with angiography is successful in 40–45% of cases.
Abscesses
-
Abscesses are a common indication for surgery in the Crohn’s patient and account for 7–25% of surgeries.
-
The abscess usually results from microperforation that originates from transmural inflammation of the diseased bowel.
-
The most common location in the abdomen is the ileocecal region.
-
An inflammatory “mass” may be an abscess or a phlegmon.
-
If there is an abscess, percutaneous drainage should be considered. The majority of patients who develop a spontaneous abscess will ultimately require surgery. If the abscess is small, or not amenable to percutaneous drainage, a trial of antibiotics may be attempted.
-
Percutaneous drainage allows for clinical improvement of the patient and may convert emergent surgery to an elective surgery. If the abscess is successfully controlled with percutaneous drainage, there is a significant decrease in the risk of septic complications following surgery.
-
-
Postoperative abscesses are more likely to be successfully treated with percutaneous drainage alone than spontaneous abscesses.
Fistula
-
Fistulas account for 15–24% of surgeries performed for Crohn’s disease.
-
Fistulas can be internal or external.
-
The internal fistulas may be enteroenteric but can also be from the bowel to any surrounding structure or organ such as the bladder, vagina, or retroperitoneum.
-
Enterocutaneous fistulas are considered external fistulas. Often, there is a stenotic area in the bowel wall distal to where the fistula originates, which increases the intraluminal pressure.
-
-
Only fistulas that are symptomatic require treatment. For example, a fistula that extends from the terminal ileum to a closely adjacent loop of the small bowel would not necessarily require treatment.
-
Enteroenteric fistulas are the most common type of abdominal fistula found in Crohn’s disease with the majority originating from the terminal ileum.
-
Symptomatic fistulas (e.g., ileosigmoid) are typically treated with excision of the diseased bowel and repair of the non-inflamed bowel wall.
-
Enterocutaneous fistulas can occur either spontaneously or as a result of prior surgery.
-
Seventy-five to 85% of enterocutaneous fistulas occur in the post-op period and are secondary to either anastomotic leaks or inadvertent injuries to the bowel.
-
Because this bowel is healthy, the fistula is more likely to close with conservative measures.
-
Fifteen to 25% are spontaneous enterocutaneous fistulas caused by Crohn’s disease, radiation, or cancer. These types of fistulas are unlikely to heal without surgical intervention.
-
Cancer and Dysplasia
-
Patients with Crohn’s disease have an increased risk of developing cancer in their lifetime.
-
A patient with CD has a two- to threefold increased risk of colorectal cancer compared to the general population.
-
With regard to small bowel cancer, there is an almost 20-fold increase.
-
A number of studies have found a male predominance in the development of cancer in Crohn’s disease.
-
The average age at diagnosis is 49–56 years, which is about 10–15 years younger than the average age for sporadic bowel cancers.
-
The mean duration of disease from onset of Crohn’s disease to diagnosis of cancer is 20 years.
-
-
Survival seems to be worse for patients with Crohn’s disease. Overall, a 5-year survival is approximately 40%.
-
There is a higher risk of developing cancer in bypassed segments, which is associated with a poor prognosis.
-
There is an increased risk of developing cancer in the area of a stricture. Colonic strictures need to be closely monitored if not surgically resected.
-
High-grade dysplasia (HGD) found in patients with Crohn’s colitis is an indication for colectomy.
Toxic Colitis
-
Severe colitis is a serious and potentially life-threatening condition if not treated appropriately and in a timely manner.
-
The addition of dilation of the colon (toxic megacolon) to this compilation of symptoms further increases the risk of complications and can lead to a potentially fatal outcome (Table 49.1).
-
A multidisciplinary approach for the treatment of these patients is critical to effectively manage these patients.
-
Initial medical management of these patients includes efforts to resuscitate the patient, including intravenous hydration and correction of electrolyte abnormalities, in particular potassium and magnesium. Total parenteral nutrition may be necessary to optimize the nutritional status of the patient.
-
It is important to rule out other possible causes of diarrhea including Clostridium difficile as well as cytomegalovirus.
-
Daily abdominal films should typically be obtained if there is presence of abdominal distension, so colonic dilation can be assessed and monitored.
-
Patients with inflammatory bowel disease have a higher risk for thromboembolic disease, so special attention needs to be made for prophylaxis.
-
The mainstay of medical therapy is the administration of corticosteroids in a daily equivalent dose of hydrocortisone 300 mg (in divided doses) or methylprednisolone 60 mg (in divided doses).
-
Those patients that do not respond or have a decline in their clinical status within 24–72 h of initiation of treatment require emergent surgery. Delays in surgery can lead to increased postoperative complications or worse.
-
Mortality rates dramatically increase in those that have suffered a perforation, increasing from 2–8% up to 27–40%.
-
The procedure of choice for these patients is a total abdominal colectomy with end ileostomy.
-
Emergent proctectomy is rarely indicated for rectal hemorrhage or rectal perforation.
Surgical Considerations
-
Surgery for Crohn’s disease is not curative, so preserving the small bowel when possible is paramount.
-
Recurrence occurs in the majority of patients and so should be considered in operative planning.
Preoperative Evaluation
-
Information obtained from the history and physical, past medical, and surgical records, endoscopy, as well as imaging studies will be critical to operative planning and timing.
-
Nutritional assessment as well as medication usage deserves special attention as this will effect healing and may increase postoperative complications.
-
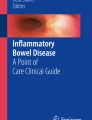
Preoperative imaging will give information regarding severity, involvement of surrounding structures, concurrent infections, resectability, and possible risk of short bowel syndrome (Fig. 49.1).

CT scan in a patient with Crohn’s disease demonstrating fluid-filled bowel loops, thickened terminal ileum, and a subcutaneous right lower quadrant abscess
History and Physical
-
Accurate and detailed information regarding the patient’s current symptoms is very important and helpful in deciding if surgery is indicated.
-
During the abdominal examination, special attention is paid to areas of tenderness, prior scars, evidence of draining fistula, as well as palpable masses.
-
Knowledge of rectal or perianal involvement based on physical examination is often important when planning operative management.
Nutritional Assessment and Role of TPN in Crohn’s Treatment
-
Poor nutrition has been linked to delayed wound healing, decline in physiologic and psychiatric function, altered immune function, and increased postoperative complications.
-
Various markers of nutrition have been evaluated including weight loss, protein depletion, serum albumin, and prealbumin. Each of these has shown a link between malnutrition and poor surgical outcomes.
-
Hypoalbuminemia has also been shown to be a good predictor of postoperative morbidity and mortality.
-
It is estimated that 80% of Crohn’s patients will have some degree of malnutrition; weight loss has been reported in 65–76% of patients with Crohn’s disease depending on severity of disease.
-
Total parenteral nutrition may be appropriate to improve the patient’s nutritional status when enteral feeds are not possible.
-
Correction of malnutrition preoperatively lessens the risk of postoperative complications.
-
TPN in CD is used also for treatment of intestinal fistulas, for treatment of short bowel syndrome, and for nutritional support when enteric feeds are not possible.
-
Complications can be divided into those related to either access, gastrointestinal, metabolic, or infectious.
-
Access-related complications include injuries sustained during insertion of catheters, thrombosis, and embolization.
-
Liver complications are the most important gastrointestinal complication related to treatment with TPN. This includes cholestasis, cholangitis, liver dysfunction, as well as elevation of transaminases.
-
Metabolic imbalances can occur with either excess or inadequate administration of water, glucose, electrolytes, amino acids, fat, and minerals. Close monitoring is necessary to avoid such complications.
-
There can be infectious complications with the most common being catheter-related infection.
-
-
Consideration should be given to either proximal diversion if an anastomosis is formed or the avoidance of an anastomosis with creation of an end stoma in patients who cannot be nutritionally repleted.
Impact of Medications
-
A major concern with CD medications is the effect that their immunomodulatory activity may have on surgical outcomes.
-
Corticosteroids negatively affect wound healing and increase postoperative complications; 10 mg of prednisone may be a threshold.
-
No clear and consistent association between the use of anti-TNF agents and postoperative complications has been established.
-
There is no clear association between postoperative complications and the use of thiopurines.
Operative Considerations: Overview
-
Complete exploration of the abdomen should typically be performed, assessing the extent of disease as well as involvement of surrounding bowel or other structures.
-
Every attempt should be made to preserve uninvolved bowel.
-
Care should be taken when handling the bowel and its mesentery because the mesentery can be quite friable and even gentle retraction can lead to troublesome bleeding.
-
Typically in the case of fistulas, the diseased bowel loop will need resection, while the “innocent bystander” can be preserved.
-
Extent of resection is based on macroscopic disease alone, so a grossly disease-free margin is all that is needed.
-
Stapled side-to-side anastomosis may be associated with fewer anastomotic leaks, shorter OR time, as well as lower rate of reoperation for recurrence of disease.
Laparoscopic Surgery and Crohn’s Disease
-
Laparoscopic surgery has proven benefit over open surgery with respect to return of bowel function, hospital stay, postoperative pain, as well as cosmesis.
-
Multiple studies have shown that using the laparoscopic technique in Crohn’s patients is both feasible and safe, at least in CD patients with “simple” disease.
-
The presence of extensive inflammatory adhesions, multiple areas of diseased bowel, large inflammatory masses, and the presence of fistula and abscesses may necessitate open technique (Video 49.1).
-
Contraindications for laparoscopic surgery include hypotension and sepsis, inability to tolerate pneumoperitoneum, an extensive inflammatory mass that would require a large incision for extraction, and those with extensive, complex adhesions.
Operative Considerations for Specific Locations
Upper Small Bowel Disease
-
Upper small bowel disease includes any involvement of the small bowel proximal to the terminal ileum.
-
Disease in this area, when present, can be quite extensive; this phenotype has a poorer prognosis.
-
When the upper small bowel is involved, there may be multiple areas of diseased bowel between areas of normal bowel.
-
Surgical options include resection with primary anastomosis, stricturoplasty, or in some instances, when there is significant distal disease present, proximal diversion.
-
Resection with anastomosis is commonly the appropriate option if the area to be resected is limited and the patient has not had significant small bowel resections in the past.
-
Those loops that have a perforation, associated fistula or abscess, or significant inflammation require resection.
-
Resection may also be considered if there are multiple strictures in a short segment of the bowel.
-
Resection is carried out to grossly negative margins.
-
Stricturoplasty is a method by which obstruction from a stricture in the bowel can be relieved without resection. There are multiple techniques by which this can be accomplished.
-
The Heineke-Mikulicz is the most common stricturoplasty performed and is ideal for short strictures. It is easy to perform with a low complication rate (Fig. 49.2). A variation of this is the Moskel-Walske-Neumayer stricturoplasty (Fig. 49.3).
-
For those strictures that are slightly longer (>10 cm, but <25 cm), a Jaboulay or Finney procedure may be indicated (Fig. 49.4).
-
For those strictures that are even longer (>20 cm), a Michelassi or Poggioli stricturoplasty may be applicable (Fig. 49.5).
-
-
Indications for stricturoplasty include situations where there are multiple strictures; there has been previous significant small bowel resection (>100 cm), in patients that are at risk of short bowel syndrome, duodenal strictures, or recurrent strictures.
-
Contraindications to performing a stricturoplasty include severe inflammation, strictures associated with fistulas, abscesses, or a phlegmon or those with diffuse peritonitis from a perforation. Stricturoplasty should also be avoided if there is concern for cancer and tension or the area of the stricturoplasty is adjacent to an area of resection.
-
Multiple studies have suggested comparable recurrence rates to resection.
-
In actual practice, the majority of these patients are treated with a combination of resection and stricturoplasty.

Heineke-Mikulicz stricturoplasty

Moskel-Walske-Neumayer stricturoplasty

Finney stricturoplasty

Michelassi stricturoplasty
Terminal Ileal Disease
-
Since terminal ileal disease is the most common location for Crohn’s disease to occur, ileocolic resection is the most common operative procedure performed on Crohn’s disease patients.
-
The point of division is 1–2 cm beyond the palpably thickened bowel. Microscopic negative margins are not necessary (Figs. 49.6 and 49.7).
-
Once the bowel has been resected, an anastomosis is typically performed.
-
In high-risk situations, the anastomosis may be protected with a diverting loop ileostomy; taking down a loop ileostomy has lower morbidity than laparotomy for takedown of an end ileostomy.

Following laparoscopic mobilization , an energy device is being used to divide the thickened mesentery of a patient with Crohn’s disease

Ileocecectomy specimen in a patient with Crohn’s disease
Colonic and Rectal Disease
-
Patients requiring an emergent operation for Crohn’s colitis typically undergo a total abdominal colectomy with end ileostomy regardless of the presence of rectal involvement.
-
Once diverted, symptoms and disease activity will typically subside.
-
The decision to either leave the rectum in situ, perform an ileorectal anastomosis, or perform a proctectomy can be determined at a later date.
-
The decision as to which operation to perform for a patient with Crohn’s colitis in the elective setting is more complex as more options are available.
-
Patients with refractory colonic and rectal disease typically undergo total proctocolectomy with end ileostomy.
-
The most common complication is perineal wound sepsis (36%).
-
Total abdominal proctocolectomy with a micro-Hartmann’s stump and end ileostomy is a viable alternative. At a later date, completion proctectomy can be performed via a perineal approach.
-
Total abdominal colectomy with end ileostomy and delayed proctectomy might be considered in younger patients that are concerned about sexual function and are in their childbearing years. Surveillance of the rectum is necessary until the time of the proctectomy.
-
-
For those patients with Crohn’s colitis with rectal sparing, a more limited resection can be entertained. Ileorectal anastomosis may be proposed for selected patients with intact rectal reservoir function.
-
Segmental resection for Crohn’s colitis is controversial but is appropriate for patients with limited disease.
Special Considerations
Ileosigmoid Fistula
-
This is the most common abdominal fistula encountered.
-
Most often, the sigmoid colon is not involved with Crohn’s disease but happens to be adjacent to the inflamed terminal ileum (Fig. 49.8).
-
If there is any question as to active Crohn’s disease in the sigmoid colon, a flexible endoscopic exam during surgery should answer the question.
-
Wedge resection with primary repair is typically all that is needed.
-
Occasionally, the inflammation will be so severe that wedge resection is not safe; in these cases a sleeve resection can be done.

Coronal CT image in a patient with Crohn’s disease demonstrating an ileal-sigmoid fistula from the thickened ileum to the sigmoid colon right above the level of the bladder
Complex Perineal Wounds After Proctectomy
-
Perineal wound complications can be a devastating problem after proctectomy for Crohn’s disease leading to postoperative pain, significant wound care issues, and prolonged recovery.
-
It has been estimated that the rate of unhealed perineal wounds after proctectomy for Crohn’s disease ranges from 23% to 70%.
-
Strategies to prevent this complication include smoking cessation prior to surgery, improvement of the nutritional status of the patient, as well as preoperative management of sepsis.
-
In cases of severe perianal disease, creation of a low Hartmann’s stump instead of complete proctectomy will avoid a perineal wound yet still remove majority of the disease.
-
When full resection is necessary, an intersphincteric dissection should be performed when possible. This decreases the amount of tissue removed as well as leaves well-vascularized muscle to bolster the closure.
-
At times, a wide excision is necessary either because of severe perianal disease, significant scarring, or the presence of cancer.
-
In these cases, primary closure may not be possible; wound healing can be achieved with the use of advanced tissue flaps (e.g., gluteus maximus advancement flap, posterior thigh fasciocutaneous flap, chimeric posterior thigh flap, rectus abdominis myocutaneous flap).
-
Recurrence of Disease
-
Recurrence can be described as being endoscopic, clinical, or surgical.
-
Postoperative recurrence rates have been shown to be 33% and 44% at 5 and 10 years.
-
The rate of surgical recurrence ranges from 9.5% to 20% at 5 years and 18.6% to 44% at 10 years. The rate continues to increase up to 57% at 20 years.
-
The strongest predictor of postoperative recurrence is smoking.
-
Other risk factors that have been linked to a higher rate of recurrence include prior surgical resection and penetrating/perforating phenotype.
-
Risk factors that have had mixed predictive value for postoperative recurrence include gender and location of disease.
-
Steroids and probiotics do not appear to have a role in the prevention of postoperative recurrence.
-
Mesalamine has been shown to reduce the risk of clinical recurrence when compared to placebo in some studies but not all.
-
A randomized control trial demonstrated that those patients who received metronidazole for 3 months after ileocolic resection had a decrease in severity of early recurrence compared to placebo.
-
Studies have shown a modest effect impact with thiopurines; one study showed that azathioprine seemed to delay endoscopic postoperative recurrence compared to a historical cohort or placebo groups.
-
Biologics have shown the most promise in reducing postoperative recurrence.
-
In one study, endoscopic recurrence rate at 1 year was 9.1% in the infliximab group compared to 84.6% in the placebo group.
-
Clinical recurrence was seen in 0% of the infliximab patients, 38% in the azathioprine patients, and 70% in the mesalamine patients in another study.
-
These studies are relatively small but suggest that infliximab can change the natural history of Crohn’s disease.
-
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Electronic Supplementary Material
Laparoscopic ileocolic resection (MP4 234762 kb)
Rights and permissions
Copyright information
© 2019 ASCRS (American Society of Colon and Rectal Surgeons)
About this chapter

Cite this chapter
Muldoon, R., Herline, A.J. (2019). Crohn’s Disease: Surgical Management. In: Steele, S., Hull, T., Hyman, N., Maykel, J., Read, T., Whitlow, C. (eds) The ASCRS Manual of Colon and Rectal Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-01165-9_49
Download citation
DOI: https://doi.org/10.1007/978-3-030-01165-9_49
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-01164-2
Online ISBN: 978-3-030-01165-9
eBook Packages: MedicineMedicine (R0)