
Abstract
Chagas disease is an infectious disease caused by the parasite Trypanosoma cruzi. It affects approximately seven million people worldwide, most of them in Latin America, where insect vectors that transmit the infection are endemic. Besides, T. cruzi can also be transmitted through blood transfusion, organ transplant, and from mother to child. The infection is chronic in a majority of cases and remains asymptomatic for years. It is estimated that ~30% of those chronically infected will end up developing the life-threatening symptoms characteristic of the disease: heart and/or gastrointestinal tract tissue disruptions. In the last decades, large migratory flows between Latin American countries and non-endemic regions like Europe have spread Chagas disease impact. Its silent clinical progression and vector-independent transmission routes entail a health challenge in non-endemic countries too. In this chapter we present the epidemiological status of Chagas disease in Europe as well as the measures being taken to downsize its public health risk and to control the disease.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Chagas disease is a parasitic infection caused by the protozoan parasite Trypanosoma cruzi (T. cruzi). Although originally circumscribed to the Americas, where the vectors that generally transmit the infection are endemic, migratory flows in recent decades have spread the disease to non-endemic regions like Europe.
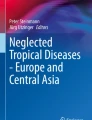
It is estimated that three million people arrived into Europe originating from Latin America (LA) [1]. The distribution of Latin American migrants among European countries has not been homogeneous. In addition to economic factors (chances of finding a job), political factors (ease of entry to countries, old colonial relations, current relationships between origin and reception states), and cultural features (shared language and/or customs) have been very important for migrant distribution [2]. Possibly that is why Spain and to a lesser extent Italy are the countries that have received a greater flow of people from LA (Fig. 1).

Map of Europe: countries that have received migrant population originating from Chagas disease endemic countries shaded according to the legend details; stripes pattern within each country limits indicates the number of estimated cases of Chagas disease per country. Data were extracted from reference [11] to plot the figure. [Photo Credit: Carme Subirà]
Prevalence of Chagas disease in endemic countries is not homogeneous. This has certainly contributed to shape important differences in the prevalence of Chagas disease in European receptor countries accordingly to the origin of migrants. Furthermore, the typology of migratory flows has also varied over time. Most recent migratory flows from LA are basically economic and come from rural areas that are highly endemic for Chagas disease [3].
Emergence of Chagas disease in Europe is manifest from the beginning of this century, as it has been evidenced by several studies [4,5,6]. Unlike other tropical diseases such as malaria or schistosomiasis, known through previous migratory flows originating in other latitudes and also through traveler’s medicine, Chagas disease was unknown to European health professionals. The clinical characteristics of this disease and its variety of forms of transmission have involved new challenges that, especially in those countries that have received a lower flow of people from LA, are still not completely solved. One of the characteristics of this migration is the tendency to feminization, which is relevant in the context of Chagas disease due to the possibility of congenital transmission.
The onset of the economic crisis in Europe in 2008 and the economy improvements seen in some Latin American countries have led to the return of a percentage of this immigration to their countries of origin. Nonetheless, part of this population still remains in Europe, and a percentage of it continued its journey within the European Union (EU), basically from Spain to richer northern countries, less affected by the economic crisis [7]. In any case, this phenomenon has not substantially changed the Chagas disease problem in Europe. It has rather made it more complex, as the preparedness of health systems and the knowledge to manage the disease are not equally set in all European countries. Thereof the importance of generalizing already acquired knowledge to reaching a consensus position for the management and control of Chagas disease in the continent.
2 Epidemiology of Chagas Disease in Europe
There are only a few studies conducted in Europe to measure the prevalence of Chagas disease in its countries [8]. Most of the figures currently being handled are estimates based on seroprevalence data from the countries of origin of the migrants and the number of migrants coming from each endemic country [2, 9, 10]. A systematic review identified only 18 prevalence studies as having been made in Europe [8]. Taking into account these studies, around 4.2% of migrants from LA are infected with T. cruzi. But in truth, that percentage is very heterogeneous, and it depends on the immigrants’ country of origin. For instance, migrants coming from Bolivia had the highest prevalence of Chagas disease (18.1%, 95% CI: 13.9–22.7), followed by those coming from Paraguay (5.5%, 95% CI: 3.5–7.9) [8]. The same review highlighted that prevalence estimates from studies conducted in blood bank screening were considerably lower than those derived from primary healthcare, community level, or antenatal screening [8].
Spain is currently the European country with the greatest number of cases in absolute numbers (between 48,000 and 86,000 people) [2] and in percentage (between 2.7% and 4.9% of the Latin American population) of patients infected with T. cruzi (including undocumented immigrants and adopted children) [11] (Fig. 1). In Italy, the seroprevalence of T. cruzi infection has been estimated to range between 1.5% and 2.9% depending on whether the seroprevalence estimates used to calculate it are 1990s figures [12] or more recent data from the year 2005 [9]. A serological survey performed by Angheben and coworkers among at-risk population residing in Italy described a 4.3% seroprevalence rate (36 positive participants out of 867) [6]. In Switzerland, up to 2009, a total of 258 cases had been diagnosed, although it is estimated that there may be some 3,000 people infected throughout the country [7]. In the UK, between 6,000 and 12,000 people could have the disease, which would mean a prevalence of 1.3–2.4% [11]. In other European countries that also present Latin American immigration to a lesser extent (Belgium, France, Germany, Holland, or Portugal), absolute numbers are estimated to be below 3,000 infected persons [11] (see Fig. 1). Data from other European countries is not available, although the estimated number of immigrants from LA is much lower than in the countries mentioned above.
In summary , it is estimated that in Europe absolute figures of T. cruzi-infected people range between 68,000 and 123,000 [11]. However, up until 2009 only 4,290 cases had been reported [11]. A study carried out in England illustrates the degree of infra-diagnosis that occurs. In this work, the total number of reported cases of T. cruzi infection diagnosed in London from 2001 to 2014 was 41, which yielded a prevalence of 0.043% among the Latin American migrants in the city. However, the ratio between the observed and the expected prevalence of T. cruzi infection was 3.34%, resulting in an index of underdiagnosis of 96.6% [13].
3 Routes of Transmission of T. cruzi
The triatomine vectors (order Hemiptera; family Reduviidae) that generally transmit the disease in America are not present in Europe [14]. Vector-independent transmission routes, like organ transplant, blood transfusion, and from mother to child, are of relevance in endemic and non-endemic regions, such as Europe [15].
3.1 Blood Banks and Transplants Recipients
In Europe there have been a few cases of Chagas disease acquired through blood transfusion [16,17,18]. Although disease acquisition through organ transplant has also been reported [19], no prevalence studies have been published in organ donors.
Regarding blood bank surveillance, a study performed in Spain reported that 0.62% (11/1,777) of blood donors from LA were seropositive to T. cruzi antigens [20]. The highest rate (10.2%) was observed in Bolivian people. Other studies from France and Italy showed figures of 0.3% (3/972) and 1.0% (1/102) positive donors, respectively [21, 22]. In contrast, a work performed in the Netherlands showed 0.0% seropositive samples out of 1,333 at-risk donors tested, which mostly were from Suriname and Brazil [23]. Results from these studies come to illustrate the heterogeneous parasite prevalence rates found between different European countries in relation to the immigrants’ countries of origin.
3.2 Congenital Transmission
Several studies in pregnant women of Latin American origin have shown that prevalence rates of T. cruzi infection range between 1.5% and 4.7% of women [24,25,26,27,28,29]. In a study performed between 2005 and 2007 at two maternity hospitals in Barcelona (Spain), 3.4% of the LA women were positive for Chagas disease (46 out of 1,350 tested) [27]. Furthermore, a 7.5% rate of T. cruzi congenital transmission was found [27]. The incidence of Chagas disease clinical cases due to vertical transmission have been published in several European countries [28,29,30,31,32].
4 Chagas Control in Europe and Current Challenges
Chagas disease has a number of connotations that go beyond a simple parasitic infection. In many areas of LA, it is stigmatizing to endure Chagas disease, which makes of it a forgotten disease. The late onset of symptoms, linked to the fact that they are not pathognomonic of infection and are confused with cardiac or gastrointestinal symptoms of other etiologies, has historically led to a great deal of ignorance. When symptoms do exist, patients’ quality of life is impaired. Besides, T. cruzi infection does sometimes co-occur with other morbidities and affects other pathological processes. However, despite the high number of people that has arrived from endemic countries, studies on the health status of LA migrants are scarce [33].
In Europe, a major challenge posed by Chagas disease to public health systems and healthcare professionals is the generalized lack of knowledge of the disease, which may preclude an appropriate clinical management of patients. Another big issue is that T. cruzi infection is underdiagnosed [11, 13]. Poor access to diagnosis is an acknowledged massive hurdle toward disease control in endemic regions, which is most frequently observed in rural areas that are distantly located from microbiological reference laboratories [34]. Motivated by other features perhaps, but it is a phenomenon that also occurs in Europe despite the availability of wealthier healthcare systems.
4.1 T. cruzi Infection Diagnosis
Similarly to what is made in endemic countries, the diagnostic algorithms applied in Europe differ depending on whether congenital (acute) or chronic infection is to be diagnosed. In the former, due to potential false-positive confounders from parasite-specific mother-derived immunoglobulins, diagnosis in Europe is largely performed by molecular methods like that described by Piron et al. [35]. Commercial polymerase chain reaction methodologies are also available [29, 36] although at high prices. Since the sensitivity of molecular methods is not perfect, newborns to seropositive mothers (and their kin) must be serologically assayed when maternally derived antibody levels decline. In this regards, an algorithm to reduce the number of tests and restrict serological testing to months 9 and 12 of age of the child has been proposed in order to save costs [37].
At the chronic stage diagnosis is made serologically. At this stage parasitemia is low, and sensitivity of molecular detection is much poorer than indirect detection of anti-T. cruzi immunoglobulins in sera. Serological diagnosis involves two assays based on different antigenic sets due to the parasite high antigenic variability. If discordant results are obtained, then a third assay must be performed for tipping the scales. A recent work has questioned this procedure as it reported that a single highly specific and sensitive chemiluminescent assay (Chagas Architect, Abbott) would suffice to discard negative cases and only doubtful positive results (“gray zone”) should need to be confirmed by another serological test [38].
In general , the inconveniences faced to get access to Chagas disease diagnosis in Europe are not as cumbersome as those encountered in many areas of endemic regions. However, unawareness of the disease and its characteristic silent clinical progression involves that a large percentage of patients are not timely diagnosed. Thus, specific programs have been set in place to directly bring information and promote disease screening to target populations like immigrants coming from Chagas disease endemic countries [39, 40].
On the other hand, a feature observed upon talking to experts from several European countries was the high level of heterogeneity among diagnostic algorithms used in each place. Certainly , arrival to a consensus could be of great help to standardize the diagnosis and ulterior access to treatment of patients, but also, very importantly, to save costs in the process.
4.2 Treatment and Management of Patients
The two anti-parasitic drugs used to date (benznidazole and nifurtimox) to treat T. cruzi infection are available in Europe. However, the routes of acquisition of these drugs may vary from country to country depending on whether benznidazole or nifurtimox is prescribed. Mirroring what occurs in endemic areas, there is also an open debate in Europe about whether all patients infected with T. cruzi should or should not be treated. In general, international consensus is followed, which means that anti-parasitic drug treatment is recommended for patients in the acute stage, for those at chronic stage with infection reactivation, and for chronic patients under 50 years of age without clinical symptoms or mild cardiologic compromise (Kushnir level I) [41]. It is especially relevant to treat women at child-bearing age as it has been shown that benznidazole treatment of women before pregnancy significantly reduces the risk of transmission of the infection to their newborns [42, 43]. Whether older patients may receive treatment or not depends on each clinician’s judgment. The lack of biomarkers of therapeutic efficacy is certainly a handicap when it comes to establishing more solid consensuses [44].
Benznidazole is the most widespread drug due to its availability. The regime indicated for adults involves a 5 mg/kg daily dose (up to a maximum of 400 mg per day) administered in two doses for 60 days. In children, benznidazole should be indicated with an 8–10 mg/kg daily administered in two or three doses for 60 days as well. A pediatric formulation of benznidazole has been successfully assessed in a clinical trial and will be produced soon in Argentina [45, 46]. Nifurtimox should be prescribed at a 15 mg/kg daily dose for children and 8–10 mg/kg for adults in three doses for 60 days [15]. Nifurtimox daily accumulated dose should not surpass 600 mg. Both drugs are well tolerated by children, and even a more specific age-related dosing has been proposed [47]. Once treatment is initiated, patients are regularly observed for the onset of adverse drug reactions (ADRs) which are mostly skin-related manifestations, digestive disorders, and general ADRs like headache, asthenia, and fever [48]. ADRs such as muscular-articular and neurological complains are less common [48, 49]. Nonetheless, in a very low percentage of cases, hospitalization is required, and updated clinical guidelines are of major importance to closely monitor these events [48, 49].
Patients’ access to diagnosis and treatment within Europe differs accordingly to the health systems of each country and the personal status of immigrants (legal entitlements). For instance, in Spain universal access to the healthcare system facilitates the entry of patients into the system. Despite this, there are other barriers (work schedules, permits, language, unfamiliarity with rights, entitlements, and the overall health system gaps in health literacy, social exclusion, and direct and indirect discrimination) that hinder their care [50]. On the other hand, health systems of recipient countries should ensure that health professionals are aware of the existence of Chagas disease and have adequate clinical guidelines. In Spain, the most affected European country, a series of clinical guidelines and consensus documents have been produced and published in national and international journals with the aim to help health professionals to know about Chagas disease and to provide protocols for chronic Chagas cardiologic and digestive disease [51,52,53]. The management of Chagas disease has been as well documented in the context of primary healthcare [54] and under immunosuppression conditions like in patients with HIV/AIDS [55] or organ and tissue transplants recipients [56].
Patient management after access to diagnosis and treatment is not easy. In one study focusing on process of care for Chagas disease in Italy, less than 30% of patients completed treatment with dropouts along the cascade of care. The authors concluded that there is an urgent need to involve affected communities and local regional health authorities to take part in the model of care, adapting it to the local needs [57]. Probably similar facts occur in other European countries. In complex cases with advanced disruption of heart and/or gastrointestinal tract tissues, the referral to specialists in cardiology or gastroenterology should follow the usual circuits of the different health systems.
5 Efforts to Control Transmission
5.1 Blood Banks
Most European countries follow the EU Directive 2004/23/EC on safety and quality of blood. In this document, an antecedent of Chagas disease is specified as a permanent exclusion criterion for homologous donors. But there are many patients at risk of T. cruzi infection who have never had a screening test and therefore do not know whether or not they carry and may transmit the parasite. Only France, Spain, and the UK currently have a legal regulation that makes explicit the screening of T. cruzi prior to donation; this includes not only migrants from endemic areas but also children born to mothers of endemic areas and persons who have received transfusions in endemic countries [58,59,60].
Italy is in the process of approving a new law in the parliament that allows systematic screening in patients at risk of infection [61]. The legislation in Sweden directly excludes people who have lived more than 5 years in countries endemic to the disease, although they do not refer to children of mothers born in endemic areas [62]. As a rule, donation is excluded in Switzerland in case of diagnosis of Chagas disease, but some cantons such as Geneva and Vaud have now implemented unofficial screening measures at the hospital level. There is no data from other European countries, although the Latin American presence in these countries is practically nonexistent.
5.2 Transplants
The use of donor organs with acute infection is contraindicated, and the use of a donor heart with chronic infection is also contraindicated. However, the use of other organs from donors with chronic infection has a relative contraindication. If transplantation is decided, periodic monitoring of the recipient should be recommended using parasitological and serological methods [56].
There are few European countries with a current legislation that considers transplants and Chagas disease. But in the EU directives on organ transplantation, there is no mention of Chagas disease [63]. It only points out that it is necessary to investigate certain epidemiological situations that may affect the suitability of the transplant and that may imply a risk in the transmission of some disease. In Italy, since 2012, a legal regulation has been approved obliging the screening of T. cruzi in donors at risk [64]. In Spain, although the legislation concerning this issue is vague [65], the National Transplant Organization (ONT) has made some official recommendations [66].
5.3 Congenital Transmission
It is of special interest the management of T. cruzi infection in pregnancy, during which, although it is of vital importance to carry out the diagnosis, it is not possible to administer treatment to the pregnant woman. Treatment in newborns is highly effective, and the early treatment during the first months of life will prevent future complications of the disease, thereby the great relevance of adequately diagnosing mothers before delivery. Diagnosis of T. cruzi infection during pregnancy will allow careful monitoring of the affected women and early control of the newborns, which should be immediately treated in case the parasite is transmitted. Several studies have shown that congenital transmission control programs are cost-effective in endemic countries [67]. In European countries, where health systems are widely established and health economics less stringent, timely screening of pregnant women suspected of at risk of infection should be mandatory. Furthermore, preventive widespread diagnosis and treatment of T. cruzi-infected women in child-bearing age has been shown to be beneficial to control transmission of the infection during pregnancy [42, 43]. For this particular group of patients, it would then be very advisable to implement diagnostic algorithms to limit the transmission and save newborns from receiving treatment.
In some areas of Spain, specifically in Catalonia and Valencia, and in Tuscany in Italy, control measures for T. cruzi infection in pregnant women at risk of infection and control programs of newborns have already been approved by regional governments [68,69,70]. In other regions of several European countries (at least four in Spain, three in Italy, one in Germany, two in Switzerland, and two in Portugal, and there might be more the authors do not currently know about), there are local initiatives, generally promoted by hospitals or research centers, implemented for the early detection of T. cruzi infection in pregnant women and the screening of newborns born to positive mothers. However, up to now there is yet no official recommendation or guide at national or EU levels.
6 Conclusions
-
1.
Population movements during the last decades between Chagas disease endemic countries in Latin America and Europe have contributed to extend the impact of the disease, which should now be considered an emerging infectious disease due to the number of cases registered and its relevance as public health threat.
-
2.
There are between 68,000 and 123,000 people infected with T. cruzi in Europe, a majority of them residing in Spain, Italy, the UK, and France.
-
3.
The distribution and epidemiology of the infection in Europe is very heterogeneous and depends on the origin of the immigrants received by each country.
-
4.
There is a lack of knowledge of the disease and how to manage it clinically, which entails a public health risk in countries where it is a new challenge.
-
5.
Access to diagnosis is still shaded by the stigma that accompanies this disease, which along with miscommunication and unawareness complicate widespread testing of at-risk populations.
-
6.
Diagnostic algorithms are diverse and may lead to delays in treatment administration to congenital cases as well as to excessive costs due to cost-ineffectiveness.
-
7.
Although treatment with benznidazole and nifurtimox is generally widely available, there are still issues that preclude access to it, most importantly the huge level of underdiagnosed cases.
-
8.
Treatment is highly effective and well tolerated by children, and it should therefore be administered to them as soon as a positive diagnosis is known.
-
9.
Transmission routes in non-endemic regions are vector-independent (blood transfusion, organ transplant, and from mother to child), and control measures must be put on place for each of them correspondingly.
-
10.
Blood bank screening in European countries most affected by Chagas disease is well established. Serological testing of at-risk organ donors is not that obvious.
-
11.
Control of congenital transmission should be particularly enforced due to the great benefits it provides. Both by early identifying potentially infected newborns and immediately treating them, as well as preventively treating women at child-bearing age to reduce chances of vertical transmission of the parasite.
References
Yépez del Castillo I. Las migraciones entre América Latina y Europa: una dimensión de las relaciones entre estas dos regiones. In: Yépez del Castillo I, Herrera G, editors. Nuevas migraciones latinoamericanas a Europa. Balances y desafíos. Quito: Biblioteca FLACSO; 2007. p. 19–30.
Gascon J, Bern C, Pinazo MJ. Chagas disease in Spain, the United States and other non-endemic countries. Acta Trop. 2010;115:22–7.
López de Lera D, Oso Casas L. La inmigración latinoamericana en España. Tendencias y estado de la cuestión. In: Yépez del Castillo I, Herrera G, editors. Nuevas migraciones latinoamericanas a Europa. Balances y desafíos. Quito: Biblioteca FLACSO; 2007. p. 31–68.
Roca C, Pinazo MJ, López-Chejade P, Bayó J, Posada E, López-Solana J, Gállego M, Portús M, Gascón J. Chagas disease among the Latin American adult population attending in a primary care center in Barcelona, Spain. PLoS Negl Trop Dis. 2011;5:e1135.
Jackson Y, Chappuis F. Chagas disease in Switzerland: history and challenges. Euro Surveill. 2011;16:pii 19963.
Angheben A, Anselmi M, Gobbi F, et al. Chagas disease in Italy: breaking an epidemiological silence. Euro Surveill. 2011;16:pii 19969.
Jackson Y, Herrera MV, Gascon J. Economic crisis and increased immigrant mobility: new challenges in managing Chagas disease in Europe. Bull World Health Organ. 2014;92:771–2.
Requena-Méndez A, Aldasoro E, de Lazzari E, Sicuri E, Brown M, Moore DAJ, Gascon J, Muñoz J. Prevalence of Chagas disease in Latin-American migrants living in Europe: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2015;9:e0003540.
Jannin J, Salvatella R. Estimación cuantitativa de la enfermedad de Chagas en las Américas. Organización Panamericana de la Salud; OPS/HDM/CD/425-06. Geneva: Department of Control of Neglecled Tropical Diseases (NTD). Innovative and Intensified Disease Management (IDM). WHO/NTD/IDM; 2006.
WHO. Control and prevention of Chagas disease in Europe. Issue December 2009; 69 p.
Basile L, Jansa JM, Carlier Y, et al. Chagas disease in European countries: the challenge of a surveillance system. Euro Surveill. 2011;16:pii 19968.
Schmunis GA, Yadon ZE. Chagas disease: a Latin American health problem becoming a world health problem. Acta Trop. 2010;115:14–21.
Requena-Méndez A, Moore DAJ, Subirà C, Muñoz J. Addressing the neglect: Chagas disease in London, UK. Lancet Glob Heal. 2016;4:e231–3.
Bern C, Kjos S, Yabsley MJ, Montgomery SP. Trypanosoma cruzi and Chagas’ disease in the United States. Clin Microbiol Rev. 2011;24:655–81.
Gascon J, Pinazo MJ. Chagas disease: from Latin America to the world. Re Parasitol. 2015;2015:7–14.
Villalba R, Fornes G, Alvarez MA, Roman J, Rubio V, Fernandez M, Garcia JM, Vinals M, Torres A. Acute Chagas’ disease in a recipient of a bone marrow transplant in Spain: case report. Clin Infect Dis. 1992;14:594–5.
Forés R, Sanjuán I, Portero F, et al. Chagas disease in a recipient of cord blood transplantation. Bone Marrow Transplant. 2007;39:127–8.
Valls FV, Puy RV, Bassany EE, Cano ML, Sánchez JL, Lozoya R, Azem J, Naval X, Armengol M. Caso clínico de enfermedad de Chagas transfusional. Emf Emerg. 2008;10(Suppl 1):14–8.
Rodriguez-Guardado A, González ML, Rodriguez M, Flores-Chavez M, Boga JA, Gascon J. Trypanosoma cruzi infection in a Spanish liver transplant recipient. Clin Microbiol Infect. 2015;21:687.
Piron M, Vergés M, Muñoz J, et al. Seroprevalence of Trypanosoma cruzi infection in at-risk blood donors in Catalonia (Spain). Transfusion. 2008;48:1862–8.
El Ghouzzi MH, Boiret E, Wind F, Brochard C, Fittere S, Paris L, Mazier D, Sansonetti N, Bierling P. Testing blood donors for Chagas disease in the Paris area, France: first results after 18 months of screening. Transfusion. 2010;50:575–83.
Gabrielli S, Girelli G, Vaia F, Santonicola M, Fakeri A, Cancrini G. Surveillance of Chagas disease among at-risk blood donors in Italy: preliminary results from Umberto I Polyclinic in Rome. Blood Transfus. 2013;11:558–62.
Slot E, Hogema BM, Molier M, Bart A, Zaaijer HL. Risk factors and screening for Trypanosoma cruzi infection of Dutch blood donors. PLoS One. 2016;11:e0151038.
Martinez de Tejada B, Jackson Y, Paccolat C, Irion O. Congenital Chagas disease in Geneva: diagnostic and clinical aspects. Rev Méd Suisse. 2009;5:2091–2–4–6.
Muñoz-Vilches MJ, Salas J, Cabezas T, Metz D, Vázquez J, Soriano MJ. Chagas screening in pregnant Latin-American women. Experience in Poniente Almeriense (Almeria, Spain). Enferm Infecc Microbiol Clin. 2012;30:380–2.
Paricio-Talayero JM, Benlloch-Muncharaz MJ, Collar-del-Castillo JI, et al. Epidemiological surveillance of vertically-transmitted Chagas disease at three maternity hospitals in the Valencian Community. Enferm Infecc Microbiol Clin. 2008;26:609–13.
Muñoz J, Coll O, Juncosa T, et al. Prevalence and vertical transmission of Trypanosoma cruzi infection among pregnant Latin American women attending 2 maternity clinics in Barcelona, Spain. Clin Infect Dis. 2009;48:1736–40.
Francisco-González L, Gastañaga-Holguera T, Jiménez Montero B, Daoud Pérez Z, Illán Ramos M, Merino Amador P, Herráiz Martínez MÁ, Ramos Amador JT. Seroprevalencia y transmisión vertical de enfermedad de Chagas en una cohorte de gestantes latinoamericanas en un hospital terciario de Madrid. An Pediatr (Barc). 2018;88:122. pii: S1695-4033(17)30148-0.
Barona-Vilar C, Gimenez-Marti MJ, Fraile T, et al. Prevalence of Trypanosoma cruzi infection in pregnant Latin American women and congenital transmission rate in a non-endemic area: the experience of the Valencian Health Programme (Spain). Epidemiol Infect. 2012;140:1896–903.
Jackson Y, Myers C, Diana A, Marti HP, Wolff H, Chappuis F, Loutan L, Gervaix A. Congenital transmission of Chagas disease in Latin American immigrants in Switzerland. Emerg Infect Dis. 2009;15:601–3.
Muñoz J, Portús M, Corachan M, Fumadó V, Gascon J. Congenital Trypanosoma cruzi infection in a non-endemic area. Trans R Soc Trop Med Hyg. 2007;101:1161–2.
Riera C, Guarro A, El Kassab H, et al. Congenital transmission of Trypanosoma cruzi in Europe (Spain): a case report. Am J Trop Med Hyg. 2006;75:1078–81.
Roura M, Domingo A, Leyva-Moral JM, Pool R. Hispano-Americans in Europe: what do we know about their health status and determinants? A scoping review. BMC Public Health. 2015;15:472.
Egüez KE, Alonso-Padilla J, Terán C, Chipana Z, García W, Torrico F, Gascon J, Lozano-Beltran D-F, Pinazo M-J. Rapid diagnostic tests duo as alternative to conventional serological assays for conclusive Chagas disease diagnosis. PLoS Negl Trop Dis. 2017;11:e0005501.
Piron M, Fisa R, Casamitjana N, López-Chejade P, Puig L, Vergés M, Gascón J, Gómez i Prat J, Portús M, Sauleda S. Development of a real-time PCR assay for Trypanosoma cruzi detection in blood samples. Acta Trop. 2007;103:195–00.
Seiringer P, Pritsch M, Flores-Chavez M, et al. Comparison of four PCR methods for efficient detection of Trypanosoma cruzi in routine diagnostics. Diagn Microbiol Infect Dis. 2017;88:225–32.
Abras A, Muñoz C, Ballart C, et al. Towards a new strategy for diagnosis of congenital Trypanosoma cruzi infection. J Clin Microbiol. 2017;55:1396–07.
Abras A, Llovet T, Tebar S, Herrero M, Berenguer P, Ballart C. Serological diagnosis of chronic Chagas disease: is it time for a change? J Clin Microbiol. 2016;54:1566–72.
ISGlobal site. Barcelona’s Bolivian community spreads the word about Chagas disease. 2016. http://www.isglobal.org/en/-/la-comunidad-boliviana-en-barcelona-pasa-la-voz-contra-el-chagas. Accessed 10 Nov 2017.
Navarro M, de los Santos JJ. Access to Chagas disease treatment in non-endemic countries: the case of Spain. Lancet Glob Health. 2017;5:e577.
Bern C, Montgomery SP, Herwaldt BL, et al. Evaluation and treatment of Chagas disease in the United States: a systematic review. JAMA. 2007;298:2171–81.
Alvarez MG, Vigliano C, Lococo B, Bertocchi G, Viotti R. Prevention of congenital Chagas disease by benznidazole treatment in reproductive-age women. An observational study. Acta Trop. 2017;174:149–52.
Fabbro DL, Danesi E, Olivera V, Codebó MO, Denner S, Heredia C, Streiger M, Sosa-Estani S. Trypanocide treatment of women infected with Trypanosoma cruzi and its effect on preventing congenital Chagas. PLoS Negl Trop Dis. 2014;8:e3312.
Viotti R, Alarcón De Noya B, Araujo-Jorge T, et al. Towards a paradigm shift in the treatment of chronic Chagas disease. Antimicrob Agents Chemother. 2014;58:635–9.
DNDi site. Paediatric dosage form of benznidazole (Chagas). https://www.dndi.org/diseases-projects/portfolio/paediatric-benznidazole/. Accessed 15 Nov 2017.
MundoSano site. An Argentine laboratory will develop the pediatric formula for Chagas disease treatment. https://www.mundosano.org/en/an-argentine-laboratory-will-develop-the-pediatric-formula-for-chagas-disease-treatment/. Accessed 15 Nov 2017.
Wagner N, Jackson Y, Chappuis F, Posfay-Barbe KM. Screening and management of children at risk for Chagas disease in nonendemic areas. Pediatr Infect Dis J. 2016;35:335–7.
Pinazo MJ, Muñoz J, Posada E, López-Chejade P, Gállego M, Ayala E, del Cacho E, Soy D, Gascon J. Tolerance of benznidazole in treatment of Chagas’ disease in adults. Antimicrob Agents Chemother. 2010;54:4896–9.
Sperandio da Silva GM, Felix Mediano MF, Hasslocher-Moreno AM, et al. Benznidazole treatment safety: the Médecins Sans Frontières experience in a large cohort of Bolivian patients with Chagas’ disease. J Antimicrob Chemother. 2017;72:2596–601.
Rechel B, Mladovsky P, Ingleby D, Mackenbach JP, McKee M. Migration and health in an increasingly diverse Europe. Lancet. 2013;381:1235–45.
Pinazo MJ, Cañas E, Elizalde JI, et al. Diagnosis, management and treatment of chronic Chagas’ gastrointestinal disease in areas where Trypanosoma cruzi infection is not endemic. Gastroenterol Hepatol. 2010;33:191–00.
Gascon J, Albajar P, Canas E, et al. Diagnosis, management and treatment of chronic Chagas’ heart disease in areas where Trypanosoma cruzi infection is not endemic. Enferm Infecc Microbiol Clin. 2008;26:99–106.
González-Tomé MI, Rivera M, Camaño I, et al. Recommendations for the diagnosis, treatment and follow-up of the pregnant woman and child with Chagas disease. Enferm Infecc Microbiol Clin. 2013;31:535–42.
Roca Saumell C, Soriano-Arandes A, Solsona Díaz L, Gascón Brustenga J. Consensus document for the detection and management of Chagas disease in primary health care in a non-endemic areas. Aten Primaria. 2015;47:308–17.
Pérez-Molina J, Rodríguez-Guardado A, Soriano A, et al. Guidelines on the treatment of chronic coinfection by Trypanosoma cruzi and HIV outside endemic areas. HIV Clin Trials. 2011;12:287–98.
Pinazo MJ, Miranda B, Rodríguez-Villar C, et al. Recommendations for management of Chagas disease in organ and hematopoietic tissue transplantation programs in nonendemic areas. Transplant Rev. 2011;25:91–101.
Repetto EC, Zachariah R, Kumar A, et al. Neglect of a neglected disease in Italy: the challenge of access-to-care for Chagas disease in Bergamo area. PLoS Negl Trop Dis. 2015;9:e0004103.
Ministerio de Sanidad y Consumo. Real Decreto 1088/2005. Boletín Oficial del Estado. 2005. pp. 31288–304.
National Blood Service. Guidelines for the blood services in the United Kingdom. 2005.
Ministère de la Santé et des Sports. Arrêté du 12 janvier 2009 fixant les critères de sélection des donneurs de sang. NOR: SJSP0901086A.
Ministerio della Salute. Protocolli per l’accertamento della idoneita del donatore di sangue e di emocomponenti. GU n.85 del 13-04-2005. 2005. https://infoleges.it. Accessed 5 Nov 2017.
Källstrand Nord E. Socialstyrelsens författningssamling. SOSFS 2009:28 (M).
Directiva 2010/45/UE. Diario Oficial de la Unión Europea. 2010; 1–8.
Criteri generali per la valutazione di idoneita del donatore. Allegato E. Centro Nazionale Trapanti. 9 Agosto 2012.
Ministerio de Sanidad, Servicios Sociales e Igualdad. Real Decreto 1732/2012. Boletín Oficial del Estado. pp. 89315–48.
Criterios de Selección de donantes de órganos respecto a la transmisión de infecciones. 2004. Organización Nacional de Trasplantes. 2ª Ed. pp. 1–37.
Sicuri E, Muñoz J, Pinazo MJ, Posada E, Sanchez J, Alonso PL, Gascon J. Economic evaluation of Chagas disease screening of pregnant Latin American women and of their infants in a non endemic area. Acta Trop. 2011;118:110–7.
Protocol de cribatge i diagnòstic de malaltia de Chagas en dones embarassades llatinoamericanes i en els seus nadons. Planificació i avaluació Salut Pública - Protocol Chagas. Departamente de Salut. Generalitat de Catalunya. 2010.
Regulación del control de las infecciones congénitas y perinatales en la Comunidad Valenciana. Circ. 3/2007/8/1. Conselleria de Sanitat de la Comunitat Valenciana. 2007.
Programma regionale per la prevenzione e il controllo della malattia di Chagas congenita: indicazione per l’assistenza in gravidanza. Delibera Regione Toscana n. 489 del 04/0672012.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Alonso-Padilla, J., Pinazo, M.J., Gascón, J. (2019). Chagas Disease in Europe. In: Altcheh, J., Freilij, H. (eds) Chagas Disease. Birkhäuser Advances in Infectious Diseases. Springer, Cham. https://doi.org/10.1007/978-3-030-00054-7_5
Download citation
DOI: https://doi.org/10.1007/978-3-030-00054-7_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-00053-0
Online ISBN: 978-3-030-00054-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)