
Abstract
Ovarian carcinomas account for more deaths annually than any other gynecological cancer in the US. More than twice as many women die of ovarian cancer than endometrial cancer in spite of the fact that cancer of the endometrium is more frequent than that of the ovary. The 5-year survival of patients affected by these tumors has improved only modestly, from 45.4 to 48.6 % during the last two decades. The high mortality associated with ovarian carcinomas is due largely to the hidden anatomical location of the ovaries, which complicates the detection of abnormalities on physical examination, and the fact that these tumors typically remain asymptomatic until they spread outside the ovary, at which time they are difficult to eradicate. Hopefully, advances in our understanding of the histogenesis of ovarian epithelial tumors as well as of their underlying molecular mechanisms will lead to more effective strategies aimed at their early detection and prevention. This, in turn, should have a major impact on the morbidity and mortality associated with these tumors.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Ovarian cancer
- Ovarian carcinomas
- Ovarian epithelial tumors
- Reproductive factors
- Inflammatory factors
- Smoking
- Diet
- Genetic factors
- BRCA1
- BRCA2
- Coelomic epithelium hypothesis
- Müllerian hypothesis
33.1 Introduction
Ovarian carcinomas account for more deaths annually than any other gynecological cancer in the US. More than twice as many women die of ovarian cancer than endometrial cancer in spite of the fact that cancer of the endometrium is more frequent than that of the ovary. The 5 years survival of patients affected by these tumors has improved only modestly, from 45.4 to 48.6 % during the last two decades [1]. The high mortality associated with ovarian carcinomas is due largely to the hidden anatomical location of the ovaries, which complicates the detection of abnormalities on physical examination, and the fact that these tumors typically remain asymptomatic until they spread outside the ovary, at which time they are difficult to eradicate. Hopefully, advances in our understanding of the histogenesis of ovarian epithelial tumors as well as of their underlying molecular mechanisms will lead to more effective strategies aimed at their early detection and prevention. This, in turn, should have a major impact on the morbidity and mortality associated with these tumors.
The majority of ovarian tumors are epithelial (carcinomas). Tumors of this organ that are derived from other cell types, such as germ cell tumors, stromal tumors, and others, share little in common with those of epithelial origin and will not be addressed in this chapter.
33.2 Classification of Ovarian Epithelial Tumors
Ovarian epithelial tumors are a heterogeneous group that comprises several histological subtypes. Basic knowledge of the most common subtypes is essential to understand issues related to their cell of origin, risk factors, and other biological characteristics.
33.2.1 Histological Classificati on
The four most frequent subtypes of ovarian carcinomas as well as their distinctive morphological features and are shown in Table 33.1. The question of whether or not these different lesions share a common cell of origin has been the subject of debate among pathologists for several decades. Differences in the risk factors, clinicopathological characteristics, and molecular genetic features of individual subtypes suggest that they are distinct disease entities. However, the fact that different subtypes occasionally co-exist, resulting in mixed lesions that show features of two or more subtypes adjacent to each other within the same tumor mass, provides a strong argument that they are related.
An intriguing characteristic shared by the major subtypes of ovarian epithelial tumors is their resemblance to tumors that originate in other organs of the reproductive tract (Table 33.1). Serous ovarian carcinomas are morphologically similar to tumors arising in the fallopian tubes. This resemblance is so striking that pathologists have agreed several decades ago not to attempt to determine the exact origin of large serous tumors involving both the ovary and the fallopian tubes. It is by pure convention that these tumors are labeled as ovarian, except in rare cases where an origin from the tubes can unequivocally be demonstrated. Endometrioid ovarian carcinomas are morphologically identical to carcinomas arising in the endometrium. Here again, the striking resemblance has led to diagnostic dilemmas related to the fact that when an endometrioid ovarian tumor coexists with an endometrial tumor in the same patient, it is not possible to determine whether the ovarian tumor represents a primary lesion or a metastasis from the endometrial lesion. Mucinous ovarian carcinomas are identical to endocervical carcinoma. Clear cell carcinomas are identical to the clear cell variant of endometrial carcinomas. The observation that ovarian carcinomas are similar to tumors arising in these other sites of the reproductive tract is not based solely on morphological arguments, as recent studies have shown that the profile of homeobox genes expressed in serous, endometrioid, and mucinous ovarian carcinomas is similar to that expressed in tumors of the fallopian tubes, endometrium, and endocervix, respectively [2]. This phenomenon has implications regarding the site of origin of ovarian epithelial tumors.
33.2.2 Toward a Molecular Classification of Ovarian Carcinoma Subtypes
There are several examples of molecular genetic alterations in ovarian epithelial tumors that are strongly associated with specific tumor histological subtypes. For example, genetic factors associated with familial ovarian carcinoma predisposition are subtype-specific. Indeed, mutations in BRCA1 or BRCA2 are associated with strong predisposition to serous ovarian carcinomas but not with any of the other tumor subtypes. Germline mutations in DNA repair enzymes leading to microsatellite instability are associated with endometrioid ovarian carcinomas. In addition, specific somatic mutations are more common in certain subtypes of ovarian carcinomas than others. The association of PTEN mutations with endometrioid tumors [3, 4] and the more frequent (although not exclusive) presence of K-RAS or B-RAF mutations in mucinous and serous tumors [5–9] are additional examples. Mutations in ARID1A, a gene encoding a key component of the SWI–SNF chromatin remodeling complex called BAF250a, are associated with endometrioid and clear cell ovarian carcinomas but not with serous ovarian carcinomas [10]. These differences underscore the importance of not lumping different ovarian carcinoma subtypes as if they represented a single entity in research studies.
The development of analytical tools to examine global expression profiles over the last decade has allowed investigators to compare the spectrum of gene expression in different subtypes of ovarian epithelial tumors. Not surprisingly, the current data suggests fundamental differences in the expression profile of each major ovarian epithelial tumor subtype [11–14]. As more data accumulates, it might be possible to identify panels of markers specific for individual subtypes that might assist pathologists in the diagnosis of poorly differentiated ovarian tumors. This could be valuable in ruling out, for example, tumor subtypes associated with a less favorable prognosis such as clear cell carcinomas. In addition, profiling studies comparing tumors from patients with rapid clinical course to those from patients with more favorable outcomes suggest that panels of markers could be developed and used as predictors of clinical aggressiveness or therapeutic response independent of classical predictors such as tumor stage or grade [15, 16]. Finally, these studies could provide important clues about cell lineage derivation and histogenesis. For example, the expression profile of clear cell carcinoma of either the endometrium or the ovary was reported to be remarkably similar to that of clear cell carcinomas of the kidney [14]. This is interesting in light of the fact that the embryological origin of much of the reproductive tract is related to renal development.
33.3 Risk Factors for Ovarian Epithelial Tumors
Knowledge of genetic and environmental factors associated with predisposition to a specific cancer type can provide insight into the mechanisms underlying its development. This is particularly true of ovarian epithelial tumors, where strong predisposing factors have been well established.
33.3.1 Reproductive Factors
Most ovarian cancers occur sporadically, without evidence of genetic predisposition. Ovulation is the most well established risk factor for the sporadic form of these cancers [17, 18]. Interruption of ovulatory activity protects against the development of this disease independently of whether such interruption is achieved through pregnancy or oral contraceptives, although there is evidence of late pregnancies being more protective than earlier ones. For example, use of oral contraceptives for 5 years results in an approximately 40 % decrease in lifetime ovarian cancer risk, which is similar to the protective effect of five pregnancies after the first [19].
An initial explanation for the association between ovulation and ovarian cancer predisposition was based on the notion that these tumors originate in the coelomic epithelium lining the ovarian surface. Fatallah [20] reasoned over four decades ago that the chronic breakage and repair of the ovarian surface epithelium that results from monthly releases of the egg might lead to predisposition to malignant transformation of this epithelium (the incessant ovulation hypothesis). This hypothesis seemed attractive given the known association between cancer predisposition and cellular proliferation, one of the consequences of chronic repair. However, it fails to provide a comprehensive explanation for the current epidemiological data. For example, the disproportionately increased protective effect of late pregnancies compared to early pregnancies, as well as the progressive rise in ovarian cancer incidence after menopause, cannot be readily accounted for by the incessant ovulation hypothesis [17, 18]. Although the incessant ovulation theory is still widely quoted, a currently more favored hypothesis stipulates that it is the hormonal changes associated with the normal menstrual cycle that may have a lasting effect on predisposition of the cell of origin of ovarian epithelial tumors to neoplastic transformation. Estradiol, which is unopposed during the first half (follicular phase) of the menstrual cycle, stimulates growth of benign and malignant ovarian epithelial tumor cells in vitro, while progesterone, which is elevated during the second half (luteal phase) of the cycle, inhibits the growth of the same cells [21]. The fact that pituitary gonadotropins, which have high circulating levels around menopause, stimulate the growth of ovarian epithelial tumors in vitro suggests that hormonal changes associated with menopause may also play a role [21]
It is possible that each follicular phase of the menstrual cycle, characterized by unopposed estrogen stimulation and by elevated levels of follicular stimulating hormone, favors growth stimulation. Such stimulation may be accentuated at the end of the follicular phase due to the rapid surge in levels of luteinizing hormone that triggers ovulation. Each luteal phase, in contrast, is characterized by growth inhibition due to increased levels of progestins. This scenario of growth stimulation followed by growth inhibition might contribute to the increased risk of tumor development in women with uninterrupted menstrual cycles. The protective role of either pregnancy or oral contraceptive could, in turn, be partly due to the interruption of such a scenario. Alternatively, a study examining the long-term effects of oral contraceptives in macaques suggested that the direct action of progestins is primarily responsible for the protective effects of oral contraceptives [22].
Another explanation for the association between ovulation and ovarian cancer risk is known as the stromal hyperactivity hypothesis, which stipulates that although most ovarian follicular cells undergo apoptosis following release of the egg and the ensuing luteinization period, some may persist and retain their hormone-producing ability [23]. This would result in accumulation of steroid producing cells proportionate to the number of lifetime ovulations. Indeed, the basal levels of circulating estradiol were higher in premenopausal women with a greater lifetime number of ovulatory cycles in a longitudinal study [23].
In a recent population-based case-control study involving 477 patients with ovarian epithelial tumors and 660 controls, there was a 51 % reduction in risk of developing ovarian cancer in women who had given birth after the age of 35 compared to nulliparous women. Although prior births further reduced the risk, the magnitude of the protective effect of an early pregnancy was less than that of a pregnancy occurring after age 35 [17]. These observations underscore the complexity of the link between ovulatory activity and risk of sporadic ovarian cancer, which may in fact be the net result of several factors. In that regard, a role for androstenedione, which is the major ovarian hormone after the menopause and is suppressed by oral contraceptives, has also been suggested [24]. A role for this hormone is further supported by the fact that its circulating levels were found to be higher in the serum of patients with ovarian cancer compared to that of matched controls [25].
33.3.2 Inflammatory Factor s
Although reproductive factors associated with the menstrual cycle are by far the strongest risk determinants of ovarian cancer, a role for inflammation has also been suggested [26]. Application of talc on the perineal area has consistently been associated with increased risk of ovarian cancer. Inflammatory conditions such as pelvic inflammatory disease have also been associated with such increase [27–32]. The association between endometriosis and endometrioid ovarian carcinoma [26, 33–38] is often regarded as further support for a role of inflammation in ovarian cancer predisposition, but this association can also be explained by the hypothesis that ovarian epithelial tumors arise in components of the secondary Müllerian system. However, the apparent association between pelvic inflammatory diseases not involving endometriosis and ovarian cancer risk [39, 40], as well as the evidence for a protective effect of anti-inflammatory drugs [41–44] provide further support for the notion that inflammation can influence the risk of ovarian cancer.
33.3.3 Smoking
Multiple studies have linked cigarette smoking with risk of mucinous ovarian cancer, but not of other ovarian cancer subtypes [45–47]. This parallels the reported effect of smoking on histologically similar cancers of both the gastrointestinal tract and cervix. The proposed mechanism of carcinogenesis is a combination of direct DNA damage by carcinogens in cigarette smoke and the ability of these carcinogens to accumulate in mucin-secreting cells. Interestingly, not only is smoking not shown to increase serous or endometrioid cancer rates, but also it has been shown to decrease the relative risk of clear cell ovarian cancer. This suggests that the mechanism of carcinogenesis may be different for mucinous cancer than for other ovarian epithelial tumor types and may be more related to environmental carcinogens than to hormonal influences, as smoking is known to lower circulating estrogen levels.
33.3.4 Diet
The influence of diet has also been studied as it pertains to ovarian cancer. Data regarding the role of dietary saturated fat is controversial. One retrospective study showed an increased risk of mucinous tumors in women with diets high in saturated fats [48] while another large study found only a weakly positive, non-linear association between ovarian cancers of all subtypes and no difference for the mucinous subtype [49]. Although milk consumption and, more precisely, consumption of galactose , which is high in countries with elevated risks of ovarian carcinoma, has been proposed as a risk factor for this disease, recent data could not confirm this association, including in individuals with a functional polymorphism in an enzyme involved in galactose metabolism [50–52].
33.3.5 Genetic Factors
Approximately 15 % of all ovarian carcinomas are familial [53]. Almost all of these cases are due to germline mutations in the BRCA1 or BRCA2 genes, which are also associated with hereditary breast cancer. Approximately 40 % of women carrying a germline BRCA1 mutation will develop ovarian cancer in their lifetime while the risk for BRCA2 mutation carriers is about 20 % [54–60]. Given that the risk of ovarian cancer in the general population is only 1.7 %, cancer-causing mutations in either one of these two genes are highly penetrant. The only major subtype of ovarian epithelial tumors that has a well-defined familial component other than serous tumors is endometrioid. These tumors, which are often associated with microsatellite instability due to replication error repair deficiencies, are the fourth most common cancer type associated with the HNPCC syndrome [61].
Although the isolation of the BRCA1 gene more than a decade ago [62] raised hopes that elucidation of its biological function would shed light on the mechanisms underlying ovarian (as well as breast) cancer development, little progress has been made to date in spite of extensive data on the cellular function(s) of this gene. Part of the difficulty comes from the fact that although BRCA1 influences a large number of cellular functions potentially important in controlling cancer development, there is little insight into which function is most closely associated with familial cancer. The fact that the BRCA1 locus is associated with several splice variants, with at least one, IRIS, possibly showing effects that are opposite to those of the full-length BRCA1 protein, complicates this issue further [63].
Individuals with germline BRCA1 mutations are predisposed almost exclusively to cancers of the breast and ovaries in spite of the fact that this gene product is expressed ubiquitously in most cell types. Cellular processes associated with the full-length BRCA1 nuclear protein that are often invoked as potentially underlying the alleged tumor suppressor function of this protein include cell cycle regulation, regulation of apoptosis, DNA repair, chromatin remodeling, transcriptional regulation, X chromosome inactivation, and post-translational modification [64–68]. These are global processes important in most cells. Thus, if any of these processes were primarily responsible for cancer predisposition in mutation carriers, the resulting cancers would be expected to affect a large number of cell types. Thus, current knowledge of the normal function of BRCA1 is difficult to reconcile with the site specificity of the tumors that develop in mutation carriers. This, plus the fact that BRCA1 mutations are rare in the sporadic form of ovarian cancer, suggests that this gene may act indirectly, perhaps by controlling cells that are not direct precursors, but that nevertheless influence the cells of origin of ovarian tumors.
It is with this idea in mind that Chodankar et al. [69] hypothesized that loss of BRCA1 function could influence ovarian tumorigenesis cell non-autonomously, by disrupting interactions between cells that control the menstrual cycle, the most important risk factor for sporadic ovarian carcinoma, and cells from which ovarian epithelial tumors originate. Given the central role of granulosa cells in regulating progression through the normal menstrual cycle, plus the fact that these cells secrete a variety of hormones such as estradiol, Müllerian inhibiting substance, and others that are known to influence ovarian cancer cell growth in vitro, these authors used the cre-lox system to inactivate the Brca1 gene in mouse granulosa cells specifically. The mice indeed developed benign tumors that were clearly of epithelial origin (as opposed to an origin from granulosa cells) in strong support of a cell non-autonomous mechanism. Although it is not clear whether a similar mechanism is also applicable to humans, these results strongly suggest that ovarian cancer predisposition in BRCA1 mutation carriers is due, at least in part, to decreased BRCA1 expression in ovarian granulosa cells, thereby disrupting control mechanisms that these cells exert on the cells from which ovarian epithelial tumors originate. The finding by Hu et al. [70] that down-regulation of BRCA1 in primary cultures of human granulosa cells results in increased expression of aromatase, the rate-limiting enzyme in estradiol biosynthesis, is well in line with this hypothesis. It is not clear whether the same mechanism is also responsible for breast cancer predisposition in BRCA1 mutation carriers. The fact that ovulatory activity, which is largely controlled by ovarian granulosa cells, has a strong influence on sporadic breast cancer predisposition in addition to ovarian cancers suggests that the mechanisms of predisposition to breast cancer in mutation carriers could indeed be similar. This idea is further strengthened by the demonstration that oophorectomy can protect against breast cancer in BRCA1 mutation carriers [71].
33.3.6 Potential Link Between Genetic and Reproductive Risk Factor s
Another intriguing aspect of the genetic risk factors for ovarian carcinoma is that BRCA1 and BRCA2 are rarely abnormal in the sporadic form of this disease. A possible explanation that would also account for the site specificity of the tumors that develop in BRCA1 and BRCA2 mutation carriers is that inactivation of either one of these two genes might amplify the effects of risk factors for sporadic ovarian carcinoma. It is possible, for example, that such mutations could result in slight alterations in the dynamics of the menstrual cycle by increasing the length of the follicular phase resulting in increased estrogen stimulation unopposed by progesterone. The net result would be an amplification of the consequences of the menstrual cycle on ovarian cancer risk. The fact that pregnancy or oral contraceptive use, both of which have a strong protective effect against sporadic ovarian cancer, are also protective in BRCA1-2 mutation carriers [72, 73] is supportive of this idea. Hong et al. [74] tested this hypothesis by measuring the relative lengths of the different phases of the estrus cycle in mice harboring a Brca1 mutation in their ovarian granulosa cells and showed that indeed, the average length of the proestrus phase, which corresponds to the follicular phase of the human menstrual cycle, was longer than in wild type littermates. In addition, circulating levels of estradiol were higher in mutant mice than in wild type following inoculation of gonadotropins. They concluded that mice carrying a Brca1 mutation had both increased and prolonged estrogen stimulation unopposed by estrogen, raising the possibility that similar changes are also present in human BRCA1 mutation carriers [74].
33.4 Origin of Ovarian Epithelial Tumors
A fascinating aspect of ovarian cancer research is the persisting debate among scientists as to where and from which cell type these tumors actually originate. An answer to this fundamental question is essential to the understanding of the biology of the normal counterpart of these tumors, of the risk factors for this disease, and to the development of effective protective measures. This is also important for the identification and characterization of ovarian carcinoma precursor lesions and for the development of strategies aimed at their early detection.
33.4.1 Origin of the Theory That Ovarian Epithelial Tumors Arise in the Coelomic Epitheliu m
It has been widely accepted for the most part of the last century that ovarian epithelial tumors arise from the single mesothelial cell layer that lines the ovarian surface, which is also called ovarian surface epithelium [75]. This cell layer is also called coelomic epithelium because it is continuous with and identical to the mesothelial cell layer that lines all pelvic and abdominal surfaces. It was once believed, in the early part of the last century, that various cell types present in the normal mature ovary, including follicular and germ cells, were embryologically derived from the portion of the coelomic epithelium that lines the ovarian surface. It is for this reason that this cell layer was named germinal epithelium, a name that continues to be used today. The idea that ovarian epithelial tumors arose from this cell layer was attractive given such an alleged role in ovarian development. It is now well established that germ cells do not form from the coelomic epithelium and although the exact origin of ovarian follicular cells continues to be debated, there are strong morphological, functional, and molecular arguments that they are of mesonephric origin [76]. It is intriguing that although the original embryological arguments that led to the development of the theory that ovarian carcinomas originated in the overlying coelomic epithelium are no longer valid, this theory persisted, probably due to delays in the formulation of an alternative hypothesis.
33.4.2 Issues Relevant to the Identification of the Cell of Origin of Ovarian Epithelial Tumors
33.4.2.1 Morphological Argument s
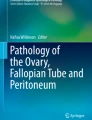
Several histological observations cannot be readily accounted for by the idea that ovarian epithelial tumors are derived from the coelomic epithelium. First, this cell layer rarely, if ever, shows pre-neoplastic changes. Although a handful of microscopic cancers have been described in the coelomic epithelium lining the ovarian surface, these are extremely rare and an origin from the fallopian tubes or other components of the Müllerian tract is difficult to rule out. Second, and even more compelling, ovarian epithelial tumors do not resemble mesotheliomas, which is what would be expected if they originated from the coelomic epithelium, but are similar to epithelial tumors arising from other organs of the female reproductive tract as already pointed out (Fig. 33.1, Table 33.1). The fact that the most common ovarian epithelial tumor subtypes resemble tumors originating in either fallopian tubes, endometrium, or endocervix is intriguing because not only do these other components of the reproductive tract share a common embryological origin that is different than that of the ovary, but there are also no normal cells resembling either fallopian tubes, endometrium, or endocervix within normal ovaries. If ovarian carcinomas indeed arose from the ovarian surface, they would be the only example of somatic tumors that are better differentiated than their cell of origin.

Morphological comparison between the ovarian surface epithelium, serous or mucinous cystadenomas and peritoneal mesothelium. Photographs of benign tumors are shown because they better illustrate the morphological features of interest due to better differentiation. (a) Serous cystadenoma characterized by tall columnar cells with prominent cilia. Such cells are reminiscent of the epithelial cells lining normal fallopian tubes. The mucin-secreting cells lining the mucinous cystadenoma shown in (b) are reminiscent of cells lining normal endocervix. The differences between the epithelial lining of these two cystadenoma subtypes and that of the ovarian surface (c) are readily apparent. The morphological characteristics of cells lining normal ovarian surface epithelium, which are flat to low cuboidal, are much closer to those of the cells lining the abdominal peritoneum shown in (d). (Reproduced from Gynecol Oncol vol 72, p. 438, 1999 with permission).
33.4.2.2 Embryological Arguments
The fallopian tubes, endometrium, and endocervix all share a common embryological origin that is distinct from that of the ovaries. They are derived from two ducts, called Müllerian ducts, which are completely separate from each other initially as they develop adjacent to the ureters of the mesonephros, which is the functioning kidney of the embryo. It is because of the close association with this renal system that the Müllerian ducts are also called paramesonephric. The distal portions of the two Müllerian ducts converge and eventually fuse in the midline during fetal development. It is this fused segment that develops into the upper third of the vagina, the exocervix and endocervix, and the body of the uterus. The proximal portions of the Müllerian ducts remains unfused, giving rise to the fallopian tubes. In the adult, the epithelial lining of the exocervix and upper vagina is replaced by squamous epithelium derived from the lower vagina. The epithelial linings of the endocervix, endometrium, and fallopian tubes form a continuum, with gradual transitions but no sharp boundaries between those different organs. It is puzzling how the ovary, which is not derived from the Müllerian ducts, could give rise to tumors identical to tumors of Müllerian origin.
33.4.2.3 Molecular Biological Arguments
The notion that ovarian epithelial tumors resemble tumors derived from the Müllerian tract is not only supported by morphological arguments. Cheng et al. [2] studied the expression status of genes involved in body segmentation and morphogenesis in different components of the female reproductive tract. Expression of individual members of this gene family, called HOX genes, is highly specific for different body segments. These authors showed that ovarian surface mesothelium, fallopian tube epithelium, endometrium, and endocervix each expressed a different set of HOX genes. When they examined the expression status of these genes in different subtypes of ovarian epithelial tumors, they found that serous ovarian carcinomas expressed the same set of HOX genes expressed in normal fallopian tube epithelium. Likewise, endometrioid ovarian carcinomas expressed the same set of HOX genes as normal endometrium and mucinous ovarian carcinomas had a HOX gene expression profile similar to that of the endocervix. These results are highly supportive of the idea that these different ovarian tumor subtypes originate in Müllerian epithelium as opposed to the coelomic epithelium.
33.4.2.4 Primary Peritoneal Tumors
Hypotheses about the origin of ovarian epithelial tumors must take into account the fact that tumors that are histologically and clinically indistinguishable from ovarian carcinomas can arise outside the ovary. Such tumors, which are often referred to as primary peritoneal carcinomas, are confined to women and may be seen in individuals in whom the ovaries were removed several years ago for reasons other than cancer.
33.4.3 The Coelomic Epithelium Hypothesi s
The idea that ovarian epithelial tumors arise from the portion of the coelomic epithelium that lines the ovarian surface is still favored by many in spite of the arguments discussed. Proponents of this theory account for the fact that these tumors have morphological and molecular features characteristic of Müllerian tumors by stipulating that the coelomic epithelium is not the direct precursor of ovarian tumors, but must first change into Müllerian-like epithelium through a process known as metaplasia. According to this theory, it is the rich hormonal environment of the ovary that triggers such changes. It is further hypothesized that this is most likely to happen in portions of the coelomic epithelium that have invaginated within the ovarian parenchyma, resulting in the formation of small cystic structures referred to as inclusion cysts. This readily accounts for the fact that benign ovarian epithelial tumors as well as most carcinomas are cystic in nature. This theory also accounts for the observation that small cysts within the ovary are often lined by cells with features suggestive of Müllerian differentiation while such features are extremely rare on the ovarian surface itself. Finally, proponents of this theory account for the presence of primary peritoneal tumors by stipulating that the hormonal environment in fertile women can trigger Müllerian metaplasia in coelomic epithelial cells away from the ovary in addition to cells on or within the ovary.
33.4.4 The Müllerian Hypothesi s
There is little evidence that hormonal stimuli can trigger metaplastic changes within the coelomic epithelium although such changes are central to the notion that this epithelium is the site of origin of these tumors. Because of the various arguments raised so far, it was proposed by the author nearly two decades ago that this theory, in spite of its wide acceptance, should be revisited and that the notion that ovarian epithelial tumors arise directly from Müllerian elements should be given due consideration [77]. An obvious site in the Müllerian tract that might contribute to tumors likely to be diagnosed as ovarian carcinomas is the fallopian tubes. Indeed, pathologists have acknowledged for several decades that many lesions diagnosed as primary serous ovarian tumors are in fact of fallopian tube origin because these two organs are so close to each other and the morphology of the tumors is so similar that it is usually impossible to tell them apart. It is by pure convention that serous tumors from this area are categorized as ovarian unless morphological features are present that clearly reveal an origin from fallopian tubes. Strong support for this notion comes from reports from several groups that the fimbriated end of the fallopian tubes is a frequent site of pre-neoplastic changes such as dysplasia in surgical specimens from women undergoing prophylactic procedures due to familial predisposition to ovarian cancer [78–81]. These dysplastic lesions also showed differences in expression of regulators of cell cycle progression and of apoptosis such as p53, p21, and p27 [80].
It is clear that the fallopian tubes are not the only site of origin of serous carcinomas arising in the tubo-ovarian region because some tumors do not involve the tubes and because benign serous cysts that are lined by the same cell type present in ovarian carcinomas are frequently seen within the ovary as well as in the para-tubal region with no connection to the tubes. In addition, a tubal origin is unlikely for endometrioid and mucinous ovarian carcinomas. It was proposed that these lesions could originate in other derivatives of the Müllerian ducts, which are common in the tubo-ovarian region and often impinge on the ovary [77]. Such derivatives are often referred to as the secondary Müllerian system [82] and include structures such as endosalpingiosis, which are lined by cells similar to those lining the fallopian tubes, endometriosis, which are lined by cells similar to endometrial glands, and endocervicosis, which are lined by cells similar to those lining the endocervix. In fact, small cysts lined by serous or mucinous epithelium and morphologically indistinguishable from ovarian serous or mucinous cystadenomas are frequent outside the ovaries (para-ovarian and para-tubal cystadenomas). The frequency of such extra-ovarian cysts is so high that pathologists often do not mention them in surgical pathology reports unless they are large enough to be clinically relevant. Such extra-ovarian cysts, when they increase in size, usually engulf the ovary within their wall because of their close proximity to this organ, at which point they would be categorized as ovarian cystadenomas.
Further support for the notion that endometrioid carcinomas arise in endometriosis is available from epidemiological [26, 33, 35, 38], histopathological [34, 36], as well as molecular biological evidence [37]. Additional evidence that primary peritoneal tumors arise in Müllerian tissues comes from a statistical argument made by Quddis et al. [83]. These authors reviewed all cases of endosalpingiosis and endometriosis of the omentum seen at their institution over a 12-year period. They reported that the endosalpingiosis to endometriosis ratio in this cohort was similar to the ratio of primary peritoneal serous to endometrioid carcinomas, [84] supporting the view that these two malignant tumor types arise from these two benign lesions, respectively.
Dubeau used these arguments to suggest that ovarian epithelial tumors develop exclusively in derivatives of the Müllerian ducts [77, 85]. Many serous ovarian carcinomas originate in fallopian tubes, a notion that has been accepted by pathologists for several decades. Serous tumors that do not originate in the tubes arise in endosalpingiosis, which is defined as tubal epithelium outside the tubes. Most serous carcinomas from the tubo-ovarian area, even if they originate outside the ovary, have reached a large enough size to involve the ovary by the time they come to medical attention and are thus categorized as ovarian. Those that arise in foci of endosalpingiosis that are far enough from the ovaries or tubes to spare both of these organs are categorized as primary peritoneal. Thus, the 3 serous tumor types currently categorized to as ovarian, tubal, or primary peritoneal all originate in serous Müllerian epithelium according to this hypothesis and are regarded as a single disease entity. With regard to the other histological subtypes of ovarian epithelial tumors, it is proposed that mucinous tumors arise in endocervicosis (defined as endocervical tissue outside the cervix) while endometrioid tumors arise in endometriosis (defined as endometrial tissues outside the uterus). Endosalpingiosis, endometriosis, and endocervicosis, which are the most important components of what is referred to as the secondary Müllerian system, can also give rise to intra- and extra-ovarian cystadenomas, which are the benign counterparts of ovarian carcinomas. This theory provides a straightforward explanation for the otherwise unaccounted finding that either tubal ligation or hysterectomy, which undoubtedly result in the destruction of components of the secondary Müllerian system, is protective against ovarian cancer based on numerous epidemiological studies [86–95].
The main differences between the classical theory invoking the ovarian surface epithelium as the site of origin of ovarian epithelial tumors and the Müllerian hypothesis are illustrated diagrammatically in Fig. 33.2. The Müllerian hypothesis implies that the term ovarian in ovarian carcinomas is somewhat of a misnomer given that most of these tumors arise outside the ovary. Dubeau suggested the term extra-uterine Müllerian carcinomas, further subdivided into serous, endometrioid, mucinous, and clear cell, as being more appropriate [85].

Coelomic versus Müllerian hypotheses for the origin of ovarian, tubal, and primary peritoneal carcinomas. According to the coelomic hypothesis, cortical invaginations and cortical inclusion cysts, which are initially lined by coelomic epithelium (thin black line), undergo metaplasia, and change to Müllerian-like epithelium (thicker blue lines) before undergoing malignant transformation (lightning signs). The coelomic epithelium covering peritoneal surfaces outside the ovary can give rise to primary peritoneal tumors only after undergoing metaplasia to acquire characteristics of Müllerian epithelium. No intermediary metaplastic step is necessary with the Müllerian hypothesis, which stipulates that Müllerian-like tumors arise directly and exclusively from Müllerian epithelium that is already present, either in the fimbriae or in components of the secondary Müllerian system. (Reproduced with minor modifications from Lancet Oncol vol 9, p. 1193, 2008 with permission).
33.5 Animal Models of Ovarian Cancer
33.5.1 Spontaneous Ovarian Tumor Development in Animals
Until recently, the development of a suitable animal model for spontaneous ovarian carcinoma has been complicated by the fact that these tumors are rare in most animals including lower mammals. Knowledge of the reasons for the relatively low incidence of spontaneous ovarian epithelial tumors in lower mammals compared to humans could provide important clues about the origin and risk factors of the human tumors. Tumors resembling human ovarian carcinomas are frequently present in the domestic hen [84]. The high frequency of ovarian tumors in those animals has been linked to the activity of incessant egg production, similar to the relationship between incessant ovulation and ovarian cancer risk in humans. Wild hens or other wild birds, in which continuous egg production is not artificially induced, do not develop ovarian tumors. These observations raise the possibility that ovarian carcinomas result from an artifact of civilization, that of incessant ovulation, as chronic menstrual cycling was unlikely in early humans due to more frequent pregnancies and longer lactation periods.
33.5.2 Models Based on Targeted or Conditional Manipulations of the Mouse Genom e
The isolation of BRCA1 and BRCA2, the main genetic determinants of familial ovarian carcinoma, first raised the hopes that inactivating the genes encoding the analogous proteins in mice would lead to the creation of animal models for ovarian cancer based on genetic manipulations relevant to the human disease. These approaches initially failed because mice lacking a functional Brca1 die during early embryological development. Also disappointing was the fact that none of the mice carrying heterozygous inactivation of any of these two genes were prone to cancer development. Although mutants encoding the Brca1-delta11 splice variant of Brca1, which lacks the nuclear localization signal of the full-length protein, are viable, most of the tumors that developed in these animals were lymphomas or sarcomas [96]. Models of Brca2 knockout compatible with survival were likewise associated with predisposition to lymphomas predominantly [97–99].
Models based on conditional Brca1 and Brca2 alleles have mostly been targeted to mammary epithelium. A model where Brca1 inactivation was targeted to the ovary was developed by Chodankar et al. [69], who used a truncated form of the Fshr promoter, which is expressed in granulosa cells specifically, to create a conditional Brca1 knockout. The embryos were viable and fertile. A majority of Brca1 knockout mice had grossly visible cystic tumors either attached to the ovary, to the uterine horns, or with no demonstrable attachment to either of these organs. All tumors except one resembled human serous cystadenomas, the benign counterparts of ovarian serous carcinomas. Strikingly, these tumors carried only the non-recombined (wild type) form of the floxed Brca1 allele; the recombined (mutant) form was present only in granulosa cells. These findings provide strong support to the notion that tumor predisposition in BRCA1 mutation carriers is mediated, at least in part, via a cell non-autonomous mechanism where granulosa cells control from a distance, in a BRCA1-dependent manner, neoplastic transformation in the tissue from which ovarian epithelial tumors originate. Elucidation of the mediator(s) of such transformation in this mouse model could lead to the development of better strategies for the prevention of these tumors in human populations at risk. The fact that the tumors that developed in this model were not confined to the ovary, but were seen along the entire Müllerian tract including in tissues from the para-ovarian and para-uterine areas, is supportive of the hypothesis that ovarian epithelial tumors are of Müllerian origin.
Several authors have succeeded in inducing tumors in mouse ovarian surface epithelium using conditional manipulations of the mouse genome targeted to ovarian surface epithelial cells. Orsulic et al. [100] demonstrated that the superimposition of a p53 mutation on any two of the oncogenes c-Myc, k-Ras, or Akt in targeted ovarian surface epithelial cells was sufficient to induce tumors in those cells. Flesken-Nikitin et al. [101] performed intrabursal administration of a vector expressing Cre recombinase in mice carrying floxed alleles of both p53 and Rb1, resulting in malignant transformation of the ovarian surface epithelium. Dinulescu et al. [102] similarly used intrabursal inoculations of a vector expressing Cre recombinase to induce expression of a conditional oncogenic allele of K-ras in the ovarian surface epithelium. The authors argued that the epithelial cells expressing this allele resembled the endometrial lining, providing us with an experimental model for endometriosis. Endometrial stroma, an important diagnostic feature of human endometriosis, was absent in these lesions. When inactivation of the Pten tumor suppressor was superimposed on the oncogenic K-ras allele, invasive tumors were obtained that were morphologically similar to the endometrioid subtype of ovarian carcinoma. Wu et al. [103] targeted the ovarian surface epithelium for dysregulation of the PI3K/Pten and Wnt/beta-catenin pathways, both of which are constitutively active in human endometrioid carcinomas, by conditional inactivation of Pten and Apc. Mice carrying those mutations developed carcinomas morphologically similar to human endometrioid carcinomas. These models are all based on the assumption that the targeted tissue, the ovarian coelomic epithelium, is the site of origin of ovarian epithelial tumors, a hypothesis that was favored by a majority of scientists.
Conditional inactivation of Brca1 in mouse ovarian surface epithelium resulted in hyperplasia, epithelial invaginations, and inclusion cysts [104]. This model could be valuable in understanding the potential relationship between such changes and ovarian carcinoma development. Epithelial ovarian inclusion cysts were also observed in Cd1 and Smad2 dominant negative mice after chronic superovulation from inoculations of gonadotropin hormones [105].
A transgenic model for ovarian cancer was developed by Connolly et al. [106], who used the mouse homolog of the human mullerian inhibitory substance type two receptor to drive expression of SV40 large T antigen. This receptor, which has a highly restricted tissue distribution, is expressed in a large majority of human ovarian epithelial tumors. The resulting transgenic mice developed highly invasive and metastatic tumors at a young age in the tubo-ovarian areas. A specific area where this model can be particularly attractive is for investigating the merit of targeting the Müllerian inhibitory substance type two receptor for the treatment of ovarian cancer [107, 108].
33.6 Ovarian Epithelial Tumors as Models of Cancer Progression
33.6.1 Classification of Ovarian Epithelial Tumors Based on Their Malignant Potential
Serous, mucinous, and endometrioid ovarian epithelial tumors can be further subdivided based on their malignant potential (Fig. 33.3). At one end of the spectrum are benign tumors lacking the ability to infiltrate into adjacent tissues and lacking metastatic ability. These tumors are often fluid-filled cysts (hence their designation as cystadenomas) lined by a single layer of epithelial cells resembling the lining of either fallopian tubes (serous cystadenomas) or endocervix (mucinous cystadenomas). Benign tumors of the endometrioid subtype (endometriomas) are usually filled with bloody material because they respond to the cyclic hormonal events of the normal menstrual cycle resulting in bleeding at the time of menses. At the opposite end of the spectrum are fully malignant lesions, which can be further subdivided based on histological grade. Increasing the attractiveness of ovarian epithelial tumors as a model for cancer progression is the existence of an additional category, called tumors of low malignant potential (LMP) or tumors of borderline malignancy, which are regarded as intermediate between the clearly benign and fully malignant lesions. This concept of semi-malignant tumors, which is not a feature of most other cancer models, was first advanced by Howard Taylor in 1929 [109]. It took an additional 40 years before such ovarian tumors, which are associated with a more favorable prognosis than their frankly malignant counterparts regardless of stage of presentation, became accepted as a clinical entity [110, 111]. Both the International Federation of Gynecology and Obstetrics (FIGO) and the World Health Organization (WHO) have classified ovarian epithelial tumors as benign, malignant, and low malignant potential [112].

Classification of ovarian epithelial tumors based on their malignant potential.
Ovarian tumors of low malignant potential are characterized by absent or minimal invasive potential, although they can spread outside the ovary and implant onto peritoneal surfaces. Since they are distinguished from carcinomas primarily based on differences in their invasive ability, progress in understanding their molecular determinants and in elucidating the basic molecular differences between these tumors and ovarian carcinomas could shed light on the mechanisms underlying this hallmark of the malignant phenotype. Unfortunately, the data so far have not been telling in that regard.
A fundamental molecular genetic difference between tumors of low malignant potential and carcinomas seems to be that mitotic errors leading to somatic losses of heterozygosity, a hallmark of malignancy, are rare in LMP tumors [113]. Although such losses can be demonstrated in these tumors, it is clear that these events are not frequent enough to play an important role in their development. On the other hand, some of the molecular features associated with the malignant phenotype are present in LMP tumors. For example, these tumors usually express telomerase [114], a feature of the malignant phenotype, and global DNA methylation levels or levels of DNA methylation status in centromeric and juxtacentromeric sequences in these tumors are closer to those seen in carcinomas than in cystadenomas [115, 116]. Although these results strengthen the notion that LMP tumors are intermediate between benign and frankly malignant ovarian epithelial tumors, they shed little light on their underlying mechanisms. Studies at the individual gene level have likewise been unrevealing. Although mutations in specific protein kinases have been associated with LMP tumors and may be more frequent in these tumors than in carcinomas [6, 117–119], such mutations are nevertheless seen in a large number of cancers of various types as well as in some ovarian cystadenomas and their presence in LMP tumors sheds little light on the distinguishing molecular features responsible for the phenotypic differences between these tumors and either ovarian cystadenomas or carcinomas. Along the same lines, expression profiling studies have suggested that although a panel of genes or specific pathways may be more frequently associated with LMP tumors [11, 16, 120], there are so far no clues as to the molecular determinants of the fundamental difference between these tumors and carcinomas, the ability of the latter to infiltrate into adjacent tissues.
33.6.2 Insights from Work with In Vitro Systems
Scientists have attempted to obtain further insight into the biology and molecular mechanisms of ovarian cystadenomas, tumors of low malignant potential, and carcinomas by studying the behavior of these cells in tissue culture. Several authors succeeded in culturing the mesothelial cell layer lining the ovarian surface [121–124]. Cultures of epithelial cells derived from rete ovarii, which could be of Müllerian origin and play a role in ovarian tumorigenesis although this structure is usually regarded as of mesonephric origin [76, 77], were also reported [125]. Godwin et al. [126] reported a high transformation rate in cultured ovarian surface mesothelial cells, suggesting that they may indeed be prone to malignant development.
One of the difficulties in investigating the molecular mechanisms underlying the development of ovarian tumors of low malignant potential has been the inability to culture these tumors beyond primary explants [127]. The same problem also applies to benign tumors (cystadenomas). It is possible to extend the in vitro life span of either cystadenomas or LMP tumors by introducing viral oncoproteins such as SV40 large T antigen [128], but studies based on such models are complicated by the consequences of such oncoproteins on the malignant phenotype. Nevertheless, these approaches have led to a number of observations with potentially important implications. Although these tumors clearly show continuous growth in vivo and, like carcinomas, almost always express telomerase, expression of this enzyme is not detected in cultures of LMP tumors transfected with SV40 large T antigen. Also, these cells are not immortal in culture despite the fact that this antigen prolongs their in vitro life span to about 50 population doublings [129, 130]. It is therefore possible that only a small fraction of tumor cells, perhaps with stem cell features, are primarily responsible for sustained proliferation in vivo.
Work with in vitro cultures of cystadenomas and tumors of low malignant potential transfected with SV40 large T antigen also led to the observation that although ovarian cystadenomas typically undergo severe numerical chromosomal alterations resulting in aneuploidy when they reach the phenomenon of in vitro crisis toward the end of their in vitro lifespan, cultures of tumors of low malignant potential remain remarkably stable through the crisis period [129, 130]. It is tempting to relate such chromosome stability in culture to the fact that these tumors are typically diploid and genetically stable in vivo [131, 132]. In fact, aneuploid LMP tumors are associated with a more aggressive clinical course and their response to chemotherapeutic agents may be more typical of ovarian carcinomas, raising the possibility that at least some of those tumors are carcinomas incorrectly diagnosed as LMP tumors [132–135]. Indeed, the possibility of using ploidy status as a diagnostic tool to help distinguish ovarian LMP tumors from carcinomas has been suggested [131]. Further understanding of the mechanisms underlying the apparent protection against chromosomal instability that appear to be present in LMP tumors should further increase our understanding of the development of aneuploidy, one of the hallmarks of cancer.
33.6.3 Molecular Genetic Model for Ovarian Carcinoma Development
Table 33.2 lists a number of abnormalities that have been associated with the development of these tumors, none of which are specific for ovarian cancer. A diagram illustrating global as well as selected specific abnormalities distinguishing ovarian cystadenomas, LMP tumors, and carcinomas is shown in Fig. 33.4. This diagram is primarily applicable to the serous subtype of ovarian tumors, as K-RAS, H-RAS, and B-RAF mutations are not common in all subtypes and PTEN mutations, which are frequent in endometrioid carcinomas, are not featured in this illustration. Mutations in BAF250a [10], which are frequent only in the endometrioid and clear cell subtypes (Table 33.2), are likewise not mentioned in the Fig. 33.4. The complexity of molecular genetic changes present in ovarian carcinomas clearly increases with increasing tumor histological grades, which can be regarded as a measure of a tumor’s biological aggressiveness [113, 136–138]. However, as is apparent from Fig. 33.4, the grade of ovarian carcinomas is not only a function of the mere number of molecular genetic abnormalities present in a given tumor genome, as specific molecular abnormalities appear strongly associated with high histological grades [113, 136–139]. For example, losses of heterozygosity in certain chromosomal regions, such as 6q, 17p, and 17q, appear frequent in ovarian tumors of all histological grades [113] while losses in chromosome 13 are frequent only in those of high histological grades [139, 140]. It may be that the gene(s) targeted by losses of heterozygosity in chromosome 13 control(s) cellular pathways associated perhaps not with cell cycle regulation, but with differentiation or other determinants of tumor grade. Another point illustrated in Fig. 33.4 is that although loss of heterozygosity, which is an important mechanism of inactivation of tumor suppressor genes in most human cancers, is frequent in ovarian carcinomas, this abnormality is rare in the biologically less aggressive ovarian epithelial tumors. Perhaps tumor suppressor gene inactivation, which is an important consequence of such losses, is not a feature of cystadenoma or low malignant potential tumor development. Mutations in the p53 gene, which are among the most frequent tumor suppressor gene alterations in all cancers, are present in nearly 100 % of high grade serous ovarian carcinomas but are very rare in low grade carcinomas as well as in ovarian low malignant potential tumors and cystadenomas [141]. Alterations in DNA methylation are associated with tumors of low malignant potential as well as carcinomas but not with cystadenomas, suggesting fundamental differences in the mechanisms underlying the development of these benign ovarian tumors [115, 116]. This conclusion is further strengthened by the fact that telomerase is usually not detected in cystadenomas while it is expressed in most tumors of low malignant potential and carcinomas [114]. Given that this enzyme is regarded as necessary for continuous cell growth, its absence in most cystadenomas suggests that these tumors may have a limited life span in vivo, an idea consistent with the observation that benign ovarian cysts frequently regress or remain unchanged in post-menopausal women [142].

A genetic model for ovarian epithelial tumor development. This diagram is not meant to feature all molecular genetic changes that have been associated with the development of ovarian epithelial tumors. It emphasizes the global genetic mechanisms as well as the most important locus-specific differences that distinguish ovarian cystadenomas, tumors of low malignant potential, and carcinomas. It is mostly applicable to serous tumors.
The only exception to the rarity of losses of heterozygosity in LMP tumors is losses affecting the X chromosome, which are present in about 50 % of the cases [113]. However, these losses appear to arise through a different mechanism than that responsible for most losses occurring in carcinomas because they are small interstitial chromosomal deletions as opposed to losses involving large segments such as entire chromosomes or chromosomal arms, which usually result from mitotic errors. The gene(s) targeted by the interstitial allelic losses in LMP tumors is/are still not known. The fact that the reduced allele invariably affects the inactive copy of the chromosome suggests that the targeted gene(s) escape(s) X chromosome inactivation. This suggestion is attractive because individuals born with a single X chromosome (Turner syndrome) show abnormal ovarian development (gonadal dysgenesis). Thus, the presence of the inactive X chromosome is necessary for normal ovarian development. It is conceivable that abnormalities in the same gene during adult life may lead to tumorigenesis. In that regard, it is intriguing that BRCA1, a protein involved in the control of familial ovarian carcinoma, is thought to interact with the X chromosome and has been suggested to play a role in X chromosome inactivation [143–146].
33.6.4 Relationship Between Ovarian Cystadenomas, Tumors of Low Malignant Potential , and Carcinomas
The fact that ovarian epithelial tumors are subdivided into benign, low malignant potential, and malignant lesions raises the question of whether these represent distinct disease processes or are part of a single disease continuum where tumors first develop as cystadenomas and later progress to more aggressive lesions. The answer is not only important for our understanding of ovarian tumor development, but is also relevant to the clinical management of cystadenomas and tumors of low malignant potential, which often occur in women of reproductive ages. Arguments in favor of a continuum come from morphological observations that areas histologically indistinguishable from typical ovarian cystadenomas are sometimes found contiguous to carcinomas. The most straightforward interpretation for these lesions, which are sometimes called cystadenocarcinomas, is that the histologically malignant areas arose from the pre-existing morphologically benign areas. This interpretation implies that any molecular genetic change associated with carcinomas, but normally not present in solitary cystadenomas, should be confined to the histologically malignant portions of cystadenocarcinomas. However, losses of heterozygosity and p53 mutations, which are both frequent in carcinomas and absent or at least very rare in solitary cystadenomas, are usually concordant in all portions of ovarian cystadenocarcinomas including the morphologically benign areas [147, 148]. Concordance for aneuploidy was likewise shown in different regions of cystadenocarcinomas using interphase cytogenetic approaches [149]. It seems clear, based on these observations, that the histologically benign portions of cystadenocarcinomas are genetically different from typical (solitary) cystadenomas. This conclusion supports the idea that cystadenomas do not generally progress to malignancy unless they carry a genetic predisposition to such progression such as, for example, a mutation in the p53 gene.
Another argument against the notion of a disease continuum is the presence of specific genetic abnormalities that are more frequent in tumors of low malignant potential than in carcinomas. Interstitial deletions of a small region of the X chromosome are a feature of LMP tumors but not of carcinomas [113]. In addition, mutations in the K-RAS and B-RAF genes appear to be more frequent in LMP tumors. Since mutations in these genes are also seen in low grade carcinomas [5–9], Shih and Kurman [150] suggested a dual mechanism for carcinoma development where high grade tumors develop de novo while low grade lesions arise in pre-existing LMP tumors. The fact that LMP tumors appear to be intrinsically more stable than either cystadenomas or carcinomas also argues against the notion that they are precursors of high grade ovarian carcinomas, which are typically highly aneuploid [130].
33.7 Strategies for Early Detection of Ovarian Carcinoma
33.7.1 Screening Strategies for Early Detection in Populations at Risk
The ability to detect ovarian carcinoma precursor lesions before they develop into fully mature cancers would undoubtedly have a profound effect on morbidity and mortality. The poor prognosis currently associated with these lesions is largely due to the fact that they are most often detected after they spread outside the ovary, at which time they are difficult to eradicate. All cancer screening tests that have had a significant impact on disease morbidity and mortality allow detection of pre-cancerous or pre-invasive lesions in addition to localized cancers. This is true of the PAP test used for the detection of pre-invasive cervical cancers (cervical dysplasia ), of mammography for the detection of pre-invasive breast cancer (detection of microcalcifications associated with atypical ductal hyperplasia and ductal carcinoma in situ), of prostate biopsy for the detection of prostatic epithelial neoplasia in individuals with elevated PSA, etc. Although this has not been fully established, it is perhaps not the ability to detect localized cancers, but the ability to detect pre-malignant lesions that accounts for the bulk of the impact that these various screening methods have had on disease mortality. Although it is clear that localized cancers (stage I) generally have a better prognosis than disseminated cancers, these cancers could be inherently less aggressive biologically, implying that they are less likely to metastasize. Their prognosis could therefore remain more favorable even if they are not detected until they become clinically manifest. This view is supported in the ovarian model by expression profiling studies comparing localized versus metastatic ovarian cancers, which suggest that they indeed could be regarded as distinct disease entities [151].
One of the problems with developing a sensitive screening protocol for precursors of ovarian carcinomas is that not only the nature of the precursor lesion itself is unclear, but also there is still debate as to where these tumors actually originate. There is therefore a great deal of effort focused on the development of alternate approaches with enough sensitivity and specificity for ovarian carcinomas to allow detection of early disease in populations at risk. Given that transabdominal and transvaginal ultrasound is commonly used in the evaluation of pelvic masses, the potential of this technique as a screening tool was extensively investigated. However, current data suggest that this approach alone not only lacks specificity, but may be of little value to diagnose ovarian carcinomas before they metastasize [152]. Measurement of serum CA125, a glycoprotein encoded by the MUC16 gene that has been used extensively as a marker of disease recurrence following adjuvant chemotherapy for ovarian carcinoma, is not specific for this disease and is elevated in only 50–60 % of patients with stage I ovarian carcinomas. Although measurements of rate of change in serial CA-125 measurements can increase the sensitivity of this marker based on the fact that it tends to gradually increase in women with cancer while it remains stable in those with benign conditions, the sensitivity of this approach falls short of meeting the needs of a practical screening tool [153]. Combining serial measurements of CA-125 with transvaginal ultrasound was evaluated as a means of further increasing both sensitivity and specificity. However, there was no difference in overall incidence of ovarian cancer or stage at diagnosis in women screened by this method compared to matched controls in a study of 21,935 women [154]. We are still awaiting data from an ongoing trial based on utilizing rate of rise of CA-125 as an adjunct to ultrasound as a mode of increasing positive predictive value [155].
More recently, investigators have used gene expression profiling technologies and proteomic tools in an effort to identify novel markers associated with ovarian cancer. Lu et al. [156] were able to distinguish normal from malignant ovarian epithelial cells based on expression levels of 5 markers identified from gene expression profiling analyses. In another study, proteomic approaches based on a panel of three markers, combined with CA-125 measurements, distinguished patients with stage I/II ovarian cancer from healthy controls with a specificity of 94 % [157]. Similarly, Gorelik et al. [158] used multianalyte profiling to compare the amounts of multiple cytokines in women with stage I/II ovarian carcinoma and healthy controls. These authors showed strong correlation between marker levels and early stage disease. It is hoped that further progress with these approaches will lead to the development of a panel of markers which, when used alone or in combination with CA-125 measurements or transvaginal sonography, will increase our ability to detect early ovarian carcinomas in populations at risk.
33.7.2 Early Detection of Residual or Recurrent Diseas e
Patients diagnosed with advanced ovarian carcinoma are usually first treated with surgical debulking of all visible disease greater than 1 cm, followed by adjuvant chemotherapy. Although most patients show good initial therapeutic responses, a large proportion with no evidence of residual disease after completion of the initial chemotherapeutic regimen undergo later recurrences. The development of sensitive methods for the detection of minimal residual disease in treated patients should therefore enhance our ability to identify those at higher risk of recurrence. In addition, it is possible that further therapeutic interventions may be most effective for small, subclinical tumors. Of all current surveillance modalities, second-look procedures provide the most accurate assessment of response to chemotherapy in patients with advanced epithelial ovarian cancer [159–161]. These procedures refer to laparotomies or laparoscopies, performed usually 6 weeks after completion of chemotherapy, in patients who display no clinical evidence of residual disease. These procedures were widely used to aid physicians in deciding whether to stop, change, or continue chemotherapy in patients undergoing treatment until recently. However, the fact that up to 50 % of patients in whom no residual carcinoma was detected during such procedures subsequently developed disease recurrence [160] has prompted most centers to abandon these procedures except when mandated by research protocols. Currently, most patients are followed up with serial measurements of CA-125 and CT scan. Although rising CA-125 levels constitute a good indicator of disease recurrence, this approach is not sensitive enough to allow detection of residual disease immediately after adjuvant chemotherapy.
Recent progress in our understanding of the molecular genetic changes associated with cancer development may provide us with novel sensitive approaches to better evaluate the presence or absence of residual disease in patients treated for advanced ovarian carcinoma. In that regard, the presence of detectable telomerase activity in abdominal washings may be of some value. Duggan et al. [162] showed that the presence of such activity is a more sensitive indicator of the presence of disease than cytological examination. Half of patients with negative second-look procedures tested positive for telomerase in a subsequent study [163]. A follow up study of these patients is not yet completed, but preliminary results show that patients with negative second-look procedures have a shorter survival if they test positive for telomerase (unpublished results from the author’s laboratory), raising the possibility that this marker could identify a subset of patients for whom further chemotherapy could be beneficial.
33.8 Concluding Remarks
Although progress in decreasing the incidence and improving mortality rates associated with ovarian carcinoma has lagged behind progress made with other gynecological cancers, it is hoped that current efforts will have a significant impact in the foreseeable future. A better understanding of the precursor lesion for these tumors, combined with efforts aimed at the identification of specific serum markers expressed early in disease development, should lead to better screening strategies applicable to the general population. In addition, further progress in understanding the biology of these tumors as well as of their underlying genetic mechanisms should lead to more effective therapeutic protocols based on specific molecular profiles.
References
Chan JK, Cheung MK, Husain A, et al. Patterns and progress in ovarian cancer over 14 years. Obstet Gynecol. 2006;108:521–8.
Cheng W, Liu J, Yoshida H, Rosen D, Naora H. Lineage infidelity of epithelial ovarian cancers is controlled by HOX genes that specify regional identity in the reproductive tract. Nat Med. 2005;11:531–7.
Obata K, Morland SJ, Watson RH, et al. Frequent PTEN/MMAC mutations in endometrioid but not serous or mucinous epithelial ovarian tumors. Cancer Res. 1998;58:2095–7.
Sato N, Tsunoda H, Nishida M, et al. Loss of heterozygosity on 10q23.3 and mutation of the tumor suppressor gene PTEN in benign endometrial cyst and clear cell carcinoma of the ovary. Cancer Res. 2000;60:7052–6.
Caduff RF, Svoboda-Newman SM, Ferguson AW, Johnston CM, Frank TS. Comparison of mutations of Ki-RAS and p53 immunoreactivity in borderline and malignant ovarian tumors. Am J Surg Pathol. 1999;23:323–8.
Mok SC-HB. Mutation of k-ras protooncogene in human ovarian epithelial tumors of borderline malignancy. Cancer Res. 1993;53:1489–92.
Sieben NL, Macropoulos P, Roemen GM, et al. In ovarian neoplasms, BRAF, but not KRAS, mutations are restricted to low-grade serous tumors. J Pathol. 2004;202:336–40.
Singer G, Kurman RJ, Chang HW, Cho SK, Shih I-M. Diverse tumorigenic pathways in ovarian serous carcinoma. Am J Pathol. 2002;160:1223–8.
Singer G, Oldt III R, Cohen Y, et al. Mutations in BRAF and KRAS characterize the development of low-grade ovarian serous carcinoma. J Natl Cancer Inst. 2003;95:484–6.
Wiegand KC, Shah SP, Al-Agha OM, et al. ARID1A mutations in endometriosis-associated ovarian carcinomas. N Engl J Med. 2010;363:1532–43.
Bonome T, Lee J-Y, Park D-C, et al. Expression profiling of serous low malignant potential, low-grade, and high-grade tumors of the ovary. Cancer Res. 2005;65:10602–12.
Tsuda H, Ito YM, Ohashi Y, et al. Identification of overexpression and amplification of ABCF2 in clear cell ovarian adenocarcinomas by cDNA microarray analyses. Clin Cancer Res. 2005;11:6880–8.
Wamunyokoli FW, Bonome T, Lee J-Y, et al. Expression profiling of mucinous tumors of the ovary identifies genes of clinicopathologic importance. Clin Cancer Res. 2006;12:690–700.
Zorn KK, Bonome T, Gangi L, et al. Gene expression profiles of serous, endometrioid, and clear cell subtypes of ovarian and endometrial cancer. Clin Cancer Res. 2005;11:6422–30.
Jazaeri AA, Awtrey CS, Chandramouli GVR, et al. Gene expression profiles associated with response to chemotherapy in epithelial ovarian cancers. Clin Cancer Res. 2005;11:6300–10.
Ouellet V, Guyot M-C, Le Page C, et al. Tissue array analysis of expression microarray candidates identifies markers associated with tumor grade and outcome in serous epithelial ovarian cancer. Int J Cancer. 2006;119:599–607.
Pike MC, Pearce CL, Peters R, et al. Hormonal factors and the risk of invasive ovarian cancer: a population-based case-control study. Fertil Steril. 2004;83:186–95.
Whittemore AS, Harris R, Itnyre J. Characteristics relating to ovarian cancer risk: collaborative analysis of 12 US case-control studies. II. Invasive epithelial ovarian cancers in white women. Collaborative Ovarian Cancer Group. Am J Epidemiol. 1992;136:1184–203.
Pike MC. Age-related factors in cancers of the breast, ovary, and endometrium. J Chronic Dis. 1987;40:59S–69.
Fathalla MF. Factors in the causation and incidence of ovarian cancer. Gynecol Surv. 1972;27:751–77.
Zhou H, Luo MP, Schonthal AH, et al. Effect of reproductive hormones on ovarian epithelial tumors: I. Effect on cell cycle activity. Cancer Biol Ther. 2002;1:300–6.
Rodriguez GC, Nagarsheth NP, Lee KL, et al. Progestin-induced apoptosis in the macaque ovarian epithelium: differential regulation of the transforming growth factor beta. J Natl Cancer Inst. 2002;94:50–60.
Cramer DW, Barbieri RL, Fraer AR, Harlow BL. Determinants of early follicular phase gonadotrophin and estradiol concentrations in women of late reproductive age. Hum Reprod. 2002;17:221–7.
Risch HA. Hormonal etiology of epithelial ovarian cancer, with hypothesis concerning the role of androgens and progesterone. J Natl Cancer Inst. 1998;90:1774–86.
Helzlsouer KJ, Alberg AJ, Gordon GB, et al. Serum gonadotropins and steroid hormones and the development of ovarian cancer. JAMA. 1995;274:1926–30.
Ness RB, Cottreau C. Possible role of ovarian epithelial inflammation in ovarian cancer. J Natl Cancer Inst. 1999;91:1459–67.
Cook LS, Kamb ML, Weiss NS. Perineal powder exposure and the risk of ovarian cancer. Am J Epidemiol. 1997;145:459–65.
Cramer DW, Liberman RF, Titus-Ernstoff L, et al. Genital talc exposure and risk of ovarian cancer. Int J Cancer. 1999;81:351–6.
Gertig DM, Hunter DJ, Cramer DW, et al. Prospective study of talc use and ovarian cancer. J Natl Cancer Inst. 2000;92:351–6.
Ness RB, Grisso J, Cottreau C, et al. Factors related to inflammation of the ovarian epithelium and risk of ovarian cancer. Epidemiology. 2000;11:111–7.
Whittemore AS, Wu ML, Pafenbarger RS, et al. Personal and environmental characteristics related to epithelial ovarian cancer. Am J Epidemiol. 1988;128:1228–40.
Wong C, Hempling RE, Piver MS, Natarajan N, Mettlin CJ. Perineal talc exposure and subsequent epithelial ovarian cancer. Obstet Gynecol. 1999;93:372–6.
Brinton LA, Gridley G, Persson I, Baron J, Bergqvist A. Cancer risk after a hospital discharge diagnosis of endometriosis. Am J Obstet Gynecol. 1997;176:572–9.
Heaps JM, Nieberg RK, Berek JS. Malignant neoplasms arising in endometriosis. Obstet Gynecol. 1990;75:1023–8.
Ness RB. Endometriosis and ovarian cancer: thoughts on shared pathophysiology. Am J Obstet Gynecol. 2003;189:280–94.
Prefumo F, Todeschini F, Fulcheri E, Venturini PL. Epithelial abnormalities in cystic ovarian endometriosis. Gynecol Oncol. 2002;84:280–4.
Prowse AH, Manek S, Varma R, et al. Molecular genetic evidence that endometriosis is a precursor of ovarian cancer. Int J Cancer. 2006;119:556–62.
Vignali M, Infantino M, Matrone R, et al. Endometriosis: novel etiopathogenetic concepts and clinical perspectives. Fertil Steril. 2002;78:665–78.
Risch HA, Howe GR. Pelvic inflammatory disease and the risk of epithelial ovarian cancer. Cancer Epidemiol Biomarkers Prev. 1995;4:447–51.
Shu XO, Brinton LA, Gao YT, Yuan JM. Population-based case-control study of ovarian cancer in Shanghai. Cancer Res. 1989;49:3670–4.
Akhmedkhanov A, Toniolo P, Zeleniuch-Jacquotte A, et al. Aspirin and epithelial ovarian cancer. Prev Med. 2001;33:682–7.
Cramer DW, Harlow BL, Titus-Ernstoff L, et al. Over-the-counter analgesics and risk of ovarian cancer. Lancet. 1998;351:104–7.
Moysich KB, Mettlin C, Piver MS, et al. Regular use of analgesic drugs and ovarian cancer risk. Cancer Epidmiol Biomarkers Prev. 2001;10:903–6.
Tavani A, Gallus S, La Vecchia C, et al. Aspirin and ovarian cancer: an Italian case-control study. Ann Oncol. 2000;11:1171–3.
Jordan SJ, Whiteman DC, Purdie DM, Green AC, Webb PM. Does smoking increase risk of ovarian cancer? A systematic review. Gynecol Oncol. 2006;103:1122–9.
Pan SY, Ugnat AM, Mao Y, Wen SW, Johnson KC. Association of cigarette smoking with the risk of ovarian cancer. Int J Cancer. 2004;111:124–30.
Purdie DM, Webb PM, Siskind V, Bain CJ, Green AC. The different etiologies of mucinous and nonmucinous epithelial ovarian cancers. Gynecol Oncol. 2003;88:S145–8.
Risch HA, Marrett LD, Jain M, Howe GR. Differences in risk factors for epithelial ovarian cancer by histologic type. Results of a case-control study. Am J Epidemiol. 1996;144:363–72.
Genkinger JM, Hunter DJ, Spiegelman D, et al. A pooled analysis of 12 cohort studies of dietary fat, cholesterol and egg intake and ovarian cancer. Cancer Causes Control. 2006;17:273–85.
Cramer DW, Greenberg ER, Titus-Ernstoff L, et al. A case-control study of galactose consumption and metabolism in relation to ovarian cancer. Cancer Epidmiol Biomarkers Prev. 2000;9:95–101.
Fung WLA, Risch HA, McLaughlin J, et al. The N314D polymorphism of galactose-1-phosphate uridyl transferase does not modify the risk of ovarian cancer. Cancer Epidmiol Biomarkers Prev. 2003;12:678–80.
Qin L-Q, Xu J-Y, Wang P-Y, et al. Milk/dairy products consumption, galactose metabolism and ovarian cancer: meta-analysis of epidemiological studies. Eur J Cancer Prev. 2005;14:13–9.
Claus EB, Schildkraut JM, Thompson WD, Risch NJ. The genetic attributable risk of breast and ovarian cancer. Cancer. 1996;77:2318–24.
Antoniou A, Pharoah PD, Narod S, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72:1117–30.
Brose MS, Rebbeck TR, Calzone KA, et al. Cancer risk estimates for BRCA1 mutation carriers identified in a risk evaluation program. J Natl Cancer Inst. 2002;94:1365–72.
Ford D, Easton DF, Bishop DT, Narod SA, Goldgar DE. Risks of cancer in BRCA1-mutation carriers. Breast cancer linkage consortium. Lancet. 1994;343:692–5.
Ford D, Easton DF, Stratton M, et al. Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer families. The breast cancer linkage consortium. Am J Hum Genet. 1998;62:676–89.
King MC, Marks JH, Mandell JB, et al. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science. 2003;302:643–6.
Risch HA, MaLaughlin JR, Cole DE, et al. Prevalence and penetrance of germline BRCA1 and BRCA2 mutations in a population series of 649 women with ovarian cancer. Am J Hum Genet. 2001;68:700–10.
Thompson D, Easton DF, Breast Cancer Linkage Consortium. Variation in cancer risks, by mutation position, in BRCA2 mutation carriers. Am J Hum Genet. 2001;68:410–9.
Chung DC, Rustgi AK. The hereditary nonpolyposis colorectal cancer syndrome: genetic and clinical implications. Ann Int Med. 2003;138:560–70.
Miki Y, Swensen J, Shattuck-Eidens D, et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science. 1994;266:66–71.
ElShamy WM, Livingston DM. Identification of BRCA1-IRIS, a BRCA1 locus product. Nat Cell Biol. 2004;6:954–67.
Deng CX, Scott F. Role of the tumor suppressor gene Brca1 in genetic stability and mammary gland tumor formation. Oncogene. 2000;19:1059–64.
Scully R, Livingston DM. In search of the tumour-suppressor functions of BRCA1 and BRCA2. Nature. 2000;408:429–32.
Starita LM, Parvin JD. The multiple nuclear functions of BRCA1: transcription, ubiquitination and DNA repair. Curr Opin Cell Biol. 2003;15:345–50.
Venkitaraman AR. Cancer susceptibility and the functions of BRCA1 and BRCA2. Cell. 2002;108:171–82.
Zheng L, Li S, Boyer TG, Lee WH. Lessons learned from BRCA1 and BRCA2. Oncogene. 2000;19:6159–75.
Chodankar R, Kwang S, Sangiorgi F, et al. Cell-nonautonomous induction of ovarian and uterine serous cystadenomas in mice lacking a functional Brca1 in ovarian granulosa cells. Curr Biol. 2005;15:561–5.
Hu Y, Ghosh S, Amleh A, et al. Modulation of aromatase expression by BRCA1: a possible link to tissue-specific tumor suppression. Oncogene. 2005;24:8343–8.
Kramer JL, Velazquez IA, Chen BE, et al. Prophylactic oophorectomy reduces breast cancer penetrance during prospective, long-term follow-up of BRCA1 mutation carriers. J Clin Oncol. 2005;23:8629–35.
McLaughlin JR, Risch HA, Lubinski J, et al. Reproductive risk factors for ovarian cancer in carriers of BRCA1 or BRCA2 mutations: a case-control study. Lancet Oncol. 2007;8:26–34.
Narod SA, Risch HA, Moslehi R, et al. Oral contraceptives and the risk of hereditary ovarian cancer. N Engl J Med. 1998;339:424–428
Hong H, Yen HY, Brockmeyer A, et al. Changes in the mouse estrus cycle in response to Brca inactivation suggest a potential link between risk factors for familial and sporadic ovarian cancer. Cancer Res. 2010;70:221–8.
Scully RE. Ovarian tumors. Am J Pathol. 1977;87:686–718.
Rodriguez M, Dubeau L. Ovarian tumor development: insights from ovarian embryogenesis. Eur J Gynecol Oncol. 2001;22:175–83.
Dubeau L. The cell of origin of ovarian epithelial tumors and the ovarian surface epithelium dogma: does the emperor have no clothes? Gynecol Oncol. 1999;72:437–42.
Colgan TJ, Murphy J, Cole DE, Narod S, Rosen B. Occult carcinoma in prophylactic oophorectomy specimens: prevalence and association with BRCA germline mutation status. Am J Surg Pathol. 2001;25:1283–9.
Leeper K, Garcia R, Swisher E, et al. Pathologic findings in prophylactic oophorectomy specimens in high-risk women. Gynecol Oncol. 2002;87:52–6.
Piek JM, van Diest PJ, Zweemer RP, et al. Dysplastic changes in prophylactically removed Fallopian tubes of women predisposed to developing ovarian cancer. J Pathol. 2001;195:451–6.
Tonin P, Weber B, Offit K, et al. Frequency of recurrent BRCA1 and BRCA2 mutations in 222 Ashkenazi Jewish breast cancer families. Nat Med. 1996;2:1179–83.
Lauchlan SC. The secondary mullerian system revisited. Int J Gynecol Pathol. 1994;13:73–9.
Quddus MR, Sung CJ, Lauchlan SC. Benign and malignant serous and endometrioid epithelium in the omentum. Gynecol Oncol. 1999;75:227–32.
Fredrickson TN. Ovarian tumors of the hen. Environ Health Perspect. 1987;73:35–51.
Dubeau L. The cell of origin of ovarian epithelial tumors. Lancet Oncol. 2008;9:1191–7.
Cornelison TL, Natarajan N, Piver MS, Mettlin CJ. Tubal ligation and the risk of ovarian carcinoma. Cancer Detect Prev. 1997;21:1–6.
Cramer DW, Xu H. Epidemiologic evidence for uterine growth factors in the pathogenesis of ovarian cancer. Ann Epidemiol. 1995;5:310–4.
Green AC, Purdie DM, Bain CJ, et al. Tubal sterilization, hysterectomy and decreased risk of ovarian cancer. Survey of Women’s Health Group. Int J Cancer. 1997;71:948–51.
Hankinson SE, Hunter DJ, Colditz GA, et al. Tubal ligation, hysterectomy, and risk of ovarian cancer. A prospective study. JAMA. 1993;270:2813–8.
Irwin KL, Weiss NS, Lee NC, Peterson HB. Tubal sterilization, hysterectomy, and the subsequent occurrence of epithelial ovarian cancer. Am J Epidemiol. 1991;134:362–9.
Kreiger N, Sloan M, Cotterchio M, Parsons P. Surgical procedures associated with risk of ovarian cancer. Int J Epidemiol. 1997;26:710–5.
Loft A, Lidegaard O, Tabor A. Incidence of ovarian cancer after hysterectomy: a nationwide controlled follow up. Br J Obstet Gynaecol. 1997;104:1296–301.
Miracle-McMahill HL, Calle EE, Kosinski AS, et al. Tubal ligation and fatal ovarian cancer in a large prospective cohort study. Am J Epidemiol. 1997;145:349–57.
Rosenblatt KA, Thomas DB. Reduced risk of ovarian cancer in women with a tubal ligation or hysterectomy. Cancer Epidmiol Biomarkers Prev. 1996;5:933–5.
Weiss NS, Harlow BL. Why does hysterectomy without bilateral oophorectomy influence the subsequent incidence of ovarian cancer? Am J Epidemiol. 1986;124:856–8.
Ludwig T, Fisher P, Ganesan S, Efstratiadis A. Tumorigenesis in mice carrying a truncated Brca1 mutation. Gene Dev. 2001;15:1188–93.
Connor F, Bertwistle D, Mee PJ, et al. Tumorigenesis and a DNA repair defect in mice with a truncating Brca2 mutation. Nat Genet. 1997;17:423–30.
Friedman LS, Thistlethwaite FC, Patel KJ, et al. Thymic lymphomas in mice with a truncating mutation in Brca2. Cancer Res. 1998;58:1338–43.
McAllister KA, Bennett LM, Houle CD, et al. Cancer susceptibility of mice with a homozygous deletion in the COOH-terminal domain of the Brca2 gene. Cancer Res. 2002;62:990–4.
Orsulic O, Soslow RA, Vitale-Cross LA, Gutkind JS, Varmus HE. Induction of ovarian cancer by defined multiple genetic changes in a mouse model system. Cancer Cell. 2002;1:53–62.
Flesken-Nikitin A, Choi K-C, Eng JP, Shmidt EN, Nikitin AY. Induction of carcinogenesis by concurrent inactivation of p53 and Rb1 in the mouse ovarian surface epithelium. Cancer Res. 2003;63:3459–63.
Dinulescu DM, Ince TA, Quade BJ, et al. Role of K-ras and Pten in the development of mouse models of endometriosis and endometrioid ovarian cancer. Nat Med. 2005;11:63–70.
Wu R, Hendrix-Lucas N, Kuick R, et al. Mouse model of human ovarian endometrioid adenocarcinoma based on somatic defects in the Wnt/beta-catenin and PI3K/Pten signaling pathways. Cancer Cell. 2007;11:321–33.
Clark-Knowles KV, Garson K, Jonkers J, Vanderhyden BC. Conditional inactivation of BBrca1 in the mouse ovarian surface epithelium results in an increase in preneoplastic changes. Exp Cell Res. 2007;313:133–45.
Burdette JE, Oliver RM, Ulyanov V, et al. Ovarian epithelial inclusion cysts in chronically superovulated cd1 and smad2 dominant negative mice. Endocrinology. 2007;148:3595–604.
Conolly DC, Bao R, Nikitin AY, et al. Female mice chimeric for expression of the simian virus 40 TAg under control of the MISIIR promoter develop epithelial ovarian cancer. Cancer Res. 2003;63:1389–97.
Pieretti-Vanmarcke R, Donahoe PK, Pearsall LA, et al. Mullerian inhibiting substance enhances subclinical doses of chemotherapeutic agents to inhibit human and mouse ovarian cancer. Proc Natl Acad Sci U S A. 2006;103:17426–31.
Pieretti-Vanmarcke R, Donahoe PK, Szotek P, et al. Recombinant human mullerian inhibiting substance inhibits long term growth of MIS type II receptor-directed transgenic mouse ovarian cancers in vivo. Clin Cancer Res. 2006;12:1593–8.
Taylor JHC. Malignant and semimalignant tumors of the ovary. Surg Gynecol Obstet. 1929;48:204–8.
Aure JC, Hoeg K, Kolstad P. Clinical and histologic studies of ovarian carcinoma: long-term follow-up of 990 cases. Obstet Gynecol. 1971;37:1–9.
Santesson L, Kottmeier HL. General classification of ovarian tumors. Ovarian cancer, U.I.C.C. Monograph Series. New York: Springer; 1968.
Serov SF, Scully RE, Sobin LH. Histological typing of ovarian tumors. In: International histological classification of tumours. Vol 9, Geneva; 1973.
Cheng PC, Gosewehr J, Kim TM, et al. Potential role of the inactivated X chromosome in ovarian epithelial tumor development. J Natl Cancer Inst. 1996;88:510–8.
Wan M, Li W-Z, Duggan B, et al. Telomerase activity in benign and malignant epithelial ovarian tumors. J Natl Cancer Inst. 1997;89:437–41.
Cheng PC, Schmutte C, Cofer KF, et al. Alterations in DNA methylation are early, but not initial events in ovarian tumorigenesis. Br J Cancer. 1997;75:396–402.
Qu G, Dubeau L, Narayan A, Yu MC, Ehrlich M. Satellite DNA hypomethylation vs. overall genomic hypomethylation in ovarian epithelial tumors of different malignant potential. Mutat Res. 1999;423:91–101.
Cheng EJ, Kurman RJ, Wang M, et al. Molecular genetic analysis of ovarian serous cystadenomas. Lab Invest. 2004;84:778–84.
Ho C-L, Kurman RJ, Dehari R, Wang T-L, Shih I-M. Mutations of BRAF and KRAS precede the development of ovarian serous borderline tumors. Cancer Res. 2004;64:6915–8.
Teneriello MG, Ebina M, Linnoila RI, et al. p53 and Ki-ras gene mutations in epithelial ovarian neoplasms. Cancer Res. 1993;53:3103–8.
Mougeot J-L, Bahrani-Mostafavi Z, Vachris JC, et al. Gene expression profiling of ovarian tissues for determination of molecular pathways reflective of tumorigenesis. J Mol Biol. 2006;358:310–29.
Nicosia SV, Johnson JH, Streibel EJ. Growth characteristics of rabbit ovarian mesothelial (surface epithelial) cells. Int J Gynecol Pathol. 1985;4:58–74.
Siemens CH, Auersperg N. Serial propagation of human surface ovarian epithelium in tissue culture. J Cell Physiol. 1988;134:347–56.
Tsao SW, Mok SC, Fey EG, et al. Characterization of human ovarian surface epithelial cells immortalized by human papilloma viral oncogenes (HPV-E6E7). Exp Cell Res. 1995;218:499–507.
Yang G, Rosen DG, Mercado-Uribe I, et al. Knockdown of p53 with expression of the catalytic subunit of telomerase is sufficient to immortalize primary human ovarian surface epithelial cells. Carcinogenesis. 2006;28:174–82.
Dubeau L, Velicescu M, Sherrod AE, Schreiber G, Holt G. Culture of human fetal ovarian epithelium in a chemically-defined, serum-free medium. Anticancer Res. 1990;10:1233–40.
Godwin AK, Testa JR, Handel LM, et al. Spontaneous transformation of rat ovarian surface epithelial cells: association with cytogenetic changes and implications of repeated ovulation in the etiology of ovarian cancer. J Natl Cancer Inst. 1992;84:592–601.
Crickard K, Marinello MJ, Crickard U, et al. Borderline malignant serous tumors of the ovary maintained on extracellular matrix. Evidence for clonal evolution and invasive potential. Cancer Genet Cyrogenet. 1986;23:135–43.
Luo MP, Gomperts B, Imren S, et al. Establishment of long-term in vitro cultures of human ovarian cystadenomas and LMP tumors and examination of their spectrum of expression of matrix-degrading proteinases. Gynecol Oncol. 1997;67:277–84.
Velicescu M, Yu J, Herbert BS, et al. Aneuploidy and telomere attrition are independent determinants of crisis in SV40-transformed epithelial cells. Cancer Res. 2003;63:5813–20.
Yu J, Roy D, Dubeau L. Increased chromosomal stability of ovarian tumors of low malignant potential compared to cystadenomas. Br J Cancer. 2007;96:1908–13.
Friedlander ML, Russell P, Taylor IW, Hedley DW, Tattersall MH. Flow cytometric analysis of cellular DNA content as an adjunct to the diagnosis of ovarian tumours of borderline malignancy. Pathology. 1984;16:301–6.
Lai CH, Hsueh S, Chang TC. The role of DNA flow cytometry in borderline malignant ovarian tumors. Cancer. 1996;78:794–802.
Burger CW, Prinssen HM, Baak JPA, Wagenaar N, Kenemans P. The management of borderline epithelial tumors of the ovary. Int J Gynecol Cancer. 2000;10:181–97.
Kaern J, Trope CG, Kjorstad KE, Abeler VM, Pettersen EO. Cellular DNA content as a new prognostic tool in patients with tumors of the ovary. Gynecol Oncol. 1990;38:452–7.
Sykes PH, Quinn MA, Rome RM. Ovarian tumors of low malignant potential: a retrospective study of 234 patients. Int J Gynecol Cancer. 1997;7:218–26.
Dodson MK, Hartmann LC, Cliby WA, et al. Comparison of loss of heterozygosity patterns in invasive low-grade and high-grade epithelial ovarian carcinomas. Cancer Res. 1993;53:4456–60.
Iwabuchi H, Sakamoto M, Sakunaga H, et al. Genetic analysis of benign, low-grade, and high-grade ovarian tumors. Cancer Res. 1995;55:6172–80.
Zheng JP, Robinson WR, Ehlen T, Yu MC, Dubeau L. Distinction of low grade from high grade human ovarian carcinomas on the basis of losses of heterozygosity on chromosomes 3, 6, and 11 and HER-2/neu gene amplification. Cancer Res. 1991;51:4045–51.
Kim TM, Benedict WF, Xu H-J, et al. Loss of heterozygosity on chromosome 13 is common only in the biologically more aggressive subtypes of ovarian epithelial tumors and is associated with normal retinoblastoma gene expression. Cancer Res. 1994;54:605–9.
Dodson MK, Cliby WA, Xu H-J, et al. Evidence of functional RB protein in epithelial ovarian carcinomas despite loss of heterozygosity at the RB locus. Cancer Res. 1994;54:610–3.
Ahmed AA, Etemadmoghadam D, Temple J, et al. Driver mutations in TP53 are ubiquitous in high grade serous carcinoma of the ovary. J Pathol. 2010;221:49–56.
Vuento MH, Pirhonen JP, Makinen JI, Gronroos M, Salmi TA. Evaluation of ovarian findings in asymptomatic postmenopausal women with color Doppler ultrasound. Cancer. 1995;76:1214–8.
Chadwick BP, Lane TF. BRCA1 associates with the inactive X chromosome in late S-phase, coupled with transient H2AX phosphorylation. Chromosoma. 2005;114:432–9.
Ganesan S, Silver DP, Greenberg RA, et al. BRCA1 supports XIST RNA concentration on the inactive X chromosome. Cell. 2002;111:393–405.
Pageau GL, Hall LL, Lawrence JB. BRCA1 does not paint the inactive X to localize XIST RNA but may contribute to broad changes in cancer that impact XIST and Xi heterochromatin. J Cell Biochem. 2007;100:835–50.
Silver DP, Dimitrov SD, Feunteun J, et al. Further evidence for BRCA1 communication with the inactive X chromosome. Cell. 2007;128:991–1002.
Zheng J, Benedict WF, Xu H-J, et al. Genetic disparity between morphologically benign cysts contiguous to ovarian carcinomas and solitary cystadenomas. J Natl Cancer Inst. 1995;87:1146–53.
Zheng J, Wan M, Zweizig S, et al. Histologically benign or low-grade malignant tumors adjacent to high-grade ovarian carcinomas contain molecular characteristics of high-grade carcinomas. Cancer Res. 1993;53:4138–42.
Wolf NG, Abdul-Karim FW, Schork NJ, Schwartz S. Origins of heterogeneous ovarian carcinomas. A molecular cytogenetic analysis of histologically benign, low malignant potential, and fully malignant components. Am J Pathol. 1996;149:511–20.
Shih IM, Kurman RJ. Molecular pathogenesis of ovarian borderline tumors: new insights and old challenges. Clin Cancer Res. 2005;11:7273–379.
Berchuck A, Iversen ES, Lancaster JM, et al. Patterns of gene expression that characterize long-term survival in advanced stage serous ovarian cancers. Clin Cancer Res. 2005;11:3686–96.
Horiuchi A, Itoh K, Shimizu M, et al. Towards understanding the natural history of ovarian carcinoma development: a clinicopathologic approach. Gynecol Oncol. 2003;88:309–17.
Skates SJ, Xu FJ, Yu YH, et al. Toward an optimal algorithm for ovarian cancer screening with longitudinal tumor markers. Cancer. 1995;76:2004–10.
Jacobs IJ, Skates SJ, MacDonald N, et al. Screening for ovarian cancer: a pilot randomised controlled trial. Lancet. 1999;353:1207–10.
Menon U, Skates SJ, Lewis S, et al. Prospective study using the risk of ovarian cancer algorithm to screen for ovarian cancer. J Clin Oncol. 2005;23:7919–26.
Lu KH, Patterson AP, Wang L, et al. Selection of potential markers for epithelial ovarian cancer with gene expression arrays and recursive descent partition analysis. Clin Cancer Res. 2004;10:3291–300.
Zhang Z, Bast Jr RC, Yu Y, et al. Three biomarkers identified from serum proteomic analysis for the detection of early stage ovarian cancer. Cancer Res. 2004;64:5882–90.
Gorelik E, Landsittel DP, Marrangoni AM, et al. Multiplexed immunobead-based cytokine profiling for early detection of ovarian cancer. Cancer Epidemiol Biomarkers Prev. 2005;14:981–7.
Gershenson DM, Copeland LJ, Wharton JT, et al. Prognosis of surgically determined complete responders in advanced ovarian cancer. Cancer. 1985;55:1129–35.
Muderspach L, Muggia FM, Conti PS. Second-look laparotomy for stage III epithelial ovarian cancer: rationale and current issues. Cancer Treat Rev. 1995;21:499–511.
Podratz KC, Cliby WA. Second-look surgery in the management of epithelial ovarian carcinoma. Gynecol Oncol. 1994;55:S128–33.
Duggan BD, Wan M, Yu MC, et al. Detection of ovarian cancer cells: comparison of a telomerase assay and cytologic examination. J Natl Cancer Inst. 1998;90:238–42.
Nouriani M, Bahador A, Berek JS, et al. Detection of residual subclinical ovarian carcinoma after completion of adjuvant chemotherapy. Clin Cancer Res. 2004;10:2681–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Science+Business Media New York
About this chapter
Cite this chapter
Brockmeyer, A.D., Dubeau, L. (2017). Ovarian Cancer. In: Coleman, W., Tsongalis, G. (eds) The Molecular Basis of Human Cancer. Humana Press, New York, NY. https://doi.org/10.1007/978-1-59745-458-2_33
Download citation
DOI: https://doi.org/10.1007/978-1-59745-458-2_33
Published:
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-934115-18-3
Online ISBN: 978-1-59745-458-2
eBook Packages: MedicineMedicine (R0)