
Abstract
The rate of blood flow through a tissue (F) is a critical parameter for assessing the functional efficiency of a blood vessel network following angiogenesis. This chapter aims to provide the principles behind the estimation of F, how F relates to other commonly used measures of tissue perfusion, and a practical approach for estimating F in laboratory animals, using small readily diffusible and metabolically inert radio-tracers. The methods described require relatively nonspecialized equipment. However, the analytical descriptions apply equally to complementary techniques involving more sophisticated noninvasive imaging.
Two techniques are described for the quantitative estimation of F based on measuring the rate of tissue uptake following intravenous administration of radioactive iodo-antipyrine (or other suitable tracer). The Tissue Equilibration Technique is the classical approach and the Indicator Fractionation Technique, which is simpler to perform, is a practical alternative in many cases. The experimental procedures and analytical methods for both techniques are given, as well as guidelines for choosing the most appropriate method.
Access provided by CONRICYT – Journals CONACYT. Download protocol PDF
Similar content being viewed by others


Key words
- Backflux
- Blood flow rate
- Cannulation
- Distribution volume
- Indicator fractionation
- Iodo-antipyrine
- Partition coefficient
- Radiotracer
- Tissue equilibration
1 Introduction
The maturation phase of angiogenesis results in a functional blood vessel network. In established tumors, this network is abnormal, but nevertheless sufficient to support tumor growth and metastasis. Blood flow rate through the vascular network is a measure of its functional efficiency, knowledge of which is central to understanding the angiogenic process. Its quantitative estimation provides the basis for determining oxygen, nutrient, and drug delivery to tissue (see Note 1 ). In pathological angiogenesis, such as in tumors, blood flow rate is the most sensitive and relevant pharmacodynamic end-point for determining the efficacy of drugs designed to disrupt blood vessel function. Therefore, estimation of blood flow rate is essential for both basic studies of the angiogenic process and applied studies of the effects of therapy. This chapter aims to provide the principles behind, and a practical approach to, the quantitative estimation of blood flow rate in experimental mice and rats.
Blood flow rate is the rate of delivery of arterial blood to the capillary beds within a particular mass of tissue. It is typically measured in units of mls of blood per g of tissue per minute (ml blood/g tissue/min), or, alternatively, per unit volume of tissue (ml blood/ml tissue/min).
The average time taken for blood to pass through a particular capillary bed (capillary mean transit time (τ)) is the parameter that relates tissue blood flow rate (F in ml/g/min) to fractional blood volume of the tissue (V in ml/g). This classical relationship is known as the central volume principle [1]:
For different tissues, F can vary widely, for example it is approximately 0.1 ml/g/min in rat skin and 4.0 ml/g/min in rat kidney. From Eq. 1 and using a value for V of 0.03 ml/g for skin and 0.06 ml/g for kidney, τ is approximately 18 s and 0.9 s, respectively, for these tissues. From Eq. 1, τ is only indirectly proportional to F, if V is constant, and so neither τ nor V can be used to estimate F unless they are both measured simultaneously. The same considerations apply to parameters related to τ, such as red blood cell velocity (RBC velocity ) and the blood supply time (BST); see below.
In order to estimate F, the most accurate approach is to measure the rate of delivery of an agent carried to the tissue by the blood. A contrast agent is injected into the blood-stream; its concentration time-course in arterial blood (input function) together with the kinetics of its uptake into tissue (tissue response function) are measured. F is then estimated from a mathematical model relating the tissue response function to the input function (see below). The contrast agent can be radio-active, whereby tissue concentrations can be measured by gamma or scintillation counting or by an external imaging system (e.g., a positron emitter for positron emission tomography). Alternatively, a contrast agent that is suitable for external magnetic resonance imaging, computed tomography, or ultrasound imaging can be used. Radio-active agents have the advantage that they can be administered at true tracer concentrations, therefore not interfering with physiological processes, and they do not necessarily need sophisticated imaging technology.
Some common methods for determining blood perfusion parameters are given below, most of which do not provide fully quantitative estimates of the blood flow rate, F:
-
1.
Intravital microscopy is a specialized technique that enables direct visualization of tissue microcirculation, usually via surgically implanted transparent chambers or single-sided windows. This enables measurement of RBC velocity (μm/s) in individual capillaries, as well as the blood supply time (BST, defined below). RBC velocity is measured either by directly tracking individual fluorescently labelled red blood cells through vessel segments [2] or matching the interference patterns of light reaching a camera through a slit system [3]. Modern computing techniques now enable comparison of optical signals at individual spatial locations with those in neighboring locations over time, so that two-dimensional maps of both speed and direction of blood flow can be constructed, based on similar principles to the classical slit system approach [4]. Measurements can be combined with measurements of red cell flux (number of red blood cells traversing a vessel segment per unit time) to calculate microvascular hematocrit [5] or with morphological measurements of individual blood vessel segments to obtain each segment’s volume flow rate (F seg), which assumes that RBCs are traveling with the bulk plasma flow [6]. Measurement of BST has been carried out in intravital studies of tumors, from images of the tumor vascular network over time, following the intravenous injection of a fluoresecent marker such as TRITC-dextran [7]. For each pixel of the vascular image, BST is defined as the time difference between the frame showing maximum fluorescence intensity and the frame showing maximum fluorescence intensity in a tumor-supplying artery, during a short timescale following intravenous injection. Both RBC and BST provide functional information on tumor perfusion, but are not directly related to F, as discussed above.
-
2.
Laser Doppler flowmetry (LDF) provides a means of estimating relative changes in red cell velocity, e.g., following treatment, via surface or tissue-inserted probes. This measures a frequency shift in light reflected from moving red cells, which is a measure of average red cell velocity [8]. Again, it should be noted that changes in red cell velocity may not accurately reflect changes in F.
-
3.
The fluorescent DNA-binding dye, Hoechst 33342, and certain carbo-cyanine dyes are examples of rapidly binding agents that have been used to determine a ‘perfused vascular volume’ (as a fraction of the total tissue volume) rather than blood flow rate per se. This method has been used especially in tumor studies [9, 10]. In this case, tissues are excised after several circulation times, following intra-venous injection of the dye, and functional vessels appear in tissue sections as fluorescent halos. Alternatively, a fluorescently tagged lectin that rapidly binds to endothelial cells in vivo can be used [11]. Conventional Chalkley point counting [12, 13] or image analysis provides the fractional tissue volume occupied by fluorescence. This is a useful measure of vascular function in many circumstances, but is insensitive because it cannot discriminate between perfused vessels with different flow rates.
-
4.
For contrast agents that are confined to the blood-stream, methods based on Eq. 1 can be used to calculate F [14]. However, this is difficult in practice because τ is only a few seconds, requiring highly sensitive techniques for its measurement. Radioactive or colored ‘microspheres’ of diameters around 15–25 μm are a special class of contrast agents that are confined to the blood-stream because they should be trapped on first-pass through tissue. Therefore, following injection directly into a major artery, they distribute to tissues in direct proportion to the fraction of the cardiac output received by the tissues, enabling calculation of blood flow rate [15]. With this technique, care needs to be taken to ensure adequate mixing of the microspheres in the arterial blood (which is challenging in mice, for instance) and enough microspheres are lodged in the tissue regions of interest to obtain statistical validity. In the case of tumors, care needs to be taken to determine and correct for microspheres that are re-circulated due to lack of trapping in large diameter vessels [16, 17].
-
5.
The principles used to calculate blood flow rate using microspheres can sometimes be used even when the indicator crosses the vascular wall into the tissue and re-circulates after the first pass through the tissue. If the tissue concentration of the indicator reaches a constant level that is maintained for the first minute or so after injection, this indicates that the extraction fraction by the tissue is equal to that of the whole body [18]. The fractional uptake of the indicator into the tissue must therefore equate to the blood flow fraction of the cardiac output received. In the original description of the technique, potassium and rubidium chloride behaved as ‘pseudo-microspheres’ in most normal tissues, with the notable exception of brain [18].
-
6.
Small, lipid-soluble, metabolically inert molecules, which rapidly cross the vascular wall and diffuse through the extra-vascular space, are also useful as blood flow markers. In this case, the fraction of marker crossing the capillary vascular wall from the blood in a single pass through the tissue (extraction fraction, E) is close to 1.0, and for fully perfused tissue, the accessible volume fraction (α) of the tissue is also close to 1.0. The inert radioactive gas, 133Xenon, or hydrogen can be administered by inhalation [19, 20]. However, safety issues with 133Xenon and the necessity for tissue insertion of polarographic electrodes for hydrogen have limited their use. A practical approach, which has utility for accessing the spatial heterogeneity of tissue blood flow rate, is the intravenous administration of a small, lipid-soluble, inert molecule dissolved in saline. In this case, net uptake rate into tissue over a short time (seconds) after intra-venous injection is determined primarily by blood flow rate. Methods for quantitative estimation of tissue blood flow rate and related parameters using these agents are described below (see Note 2 ).
2 Materials
2.1 Radioactive Tracer Preparation
-
1.
Any small, lipid-soluble molecule that can be suitably labelled and is not metabolized in tissue over the short time of the experiment can be used. Suitable radio-isotopes include 125I and 14C, where tissue and blood counts can be obtained using standard techniques and autoradiography/phosphor imaging can be applied if spatial variation in blood flow rate across a tissue of interest is required (see Note 3 ).
-
2.
One that has been used commonly for both normal tissue studies (primarily brain [21]) and tumor studies [22] is iodo-antipyrine (IAP) (Fig. 1). 125I-IAP is commercially available, for example from MP Biomedicals and 14C-IAP (4-Iodo[ N-methyl-14 C]antipyrine) from PerkinElmer. Alternatively, a technique for labelling IAP with 125I is described by Trivedi [23] (see Note 4 ).
Fig. 1 
Chemical structure of 4-Iodo[N-methyl- 14C]antipyrine (a) and the compartmental model used for the quantitative estimation of F (b). When the extraction fraction, E, of a blood-borne tracer is 1.0, the rate constant k 1 represents F. k 2 represents the back-flux and C a and C tiss represent the arterial blood and tissue concentrations of the tracer, respectively. In this model, the tissue is a single well-mixed compartment

2.2 Animal Preparation
Large vessel cannulation is required for intravenous administration and arterial blood sampling. Materials required:
-
1.
General anesthetic.
-
2.
Heparinized saline for cannulae (add 0.3 ml of 1000 U/ml heparin to 10 ml saline).
-
3.
General surgical equipment plus fine-angled forceps, small spring scissors, microvascular clip.
-
4.
Polythene tubing cut to suitable lengths, size appropriate to that of the vessel being cannulated (e.g., for rat 0.58 mm internal diameter; 0.96 mm outside diameter).
-
5.
Dissecting microscope.
-
6.
Cold light source.
-
7.
Thermostatically controlled heating blanket, with rectal thermometer.
2.3 Blood Flow Assay
-
1.
125I-labelled IAP (125I-IAP) and suitable protective equipment.
-
2.
Minimal dead-space glass syringe.
-
3.
General dissecting instruments for excising tissue.
-
4.
Stop-clock.
-
5.
Lidded container containing saline-soaked gauze.
-
6.
Gamma counter and suitable vials for tissue and blood samples.
-
7.
Analytical balance.
-
8.
Anesthetic (see Note 5 ).
-
9.
Fraction collector set to collect at 1 s intervals.
-
10.
Syringe pump for infusion and withdrawal.
-
11.
1000 U/ml heparin (use neat for rats and diluted 1 in 10 with saline for mice).
-
12.
Injection saline.
-
13.
High concentration solution of sodium pentobarbitone, e.g., Euthatal™.
3 Methods
3.1 Animal Preparation
In the rat , a tail artery and vein are most suitable for cannulation. In the mouse, either the carotid artery and jugular vein or femoral artery and vein can be used.
-
1.
Prepare 30 cm lengths of cannulae. For rat, use 0.96 mm outside diameter (o.d.); 0.58 mm internal diameter (i.d.). The cannula wall may be shaved down at the tip and the end may be slightly bevelled to aid insertion. Use a microscope to ensure that there are no sharp edges. For mouse, use a short length of 0.61 mm o.d.; 0.28 mm i.d. cannula, stretched to a smaller diameter at the tip and connected to a longer length of 0.96 mm o.d.; 0.58 mm i.d. cannula to reduce resistance to flow. Attach each length to a 1 ml syringe filled with heparinized saline.
-
2.
Anesthetize the animal, insert rectal thermocouple, and place on heating blanket. Also, an overhead lamp is a useful additional heat source.
-
3.
Illuminate surgical area with a cold light source.
-
4.
Expose the relevant vessel. For the rat tail, this involves making two 2 cm incisions through the skin, each side of the vessel, approximately 5 mm apart and approximately 2 cm from the base of the tail. Use artery forceps to clear the skin from the underlying connective tissue and cut the skin at the distal end to create a flap (see Note 6 ).
-
5.
Keep exposed vessels moist at all times using warmed saline.
-
6.
Free the vessel from surrounding connective tissue using fine blunt-end forceps.
-
7.
Place two lengths of suture under the vessel, tying off the most distal to the heart, which can be used to apply slight tension to the vessel.
-
8.
Occlude the vessels as far proximal as possible using a microvascular clip.
-
9.
Using spring scissors, make a v-shaped cut in the vessel close to the distal knot and insert cannula. Advance cannula into the vessel approximately 2 cm or more, by removing clip (see Note 7 ).
-
10.
Aspirate gently to ensure that blood is free flowing. It may not be possible to aspirate the vein, but a small volume of saline can be injected to check for patency.
-
11.
Tie both sutures securely around the cannula. Use tape or tissue-compatible glue to secure the cannula to the skin distal to the distal suture. Close the wound.
3.2 Blood Flow Assay
Two alternatives are described; the classic tissue equilibration method for rats and the indicator fractionation method for rats or mice. Graham et al. [24] directly compared results obtained with these two techniques in a rat brain tumor model and the main advantages and disadvantages of each method are given in Table 1.
3.2.1 Tissue Equilibration Technique
Cannulation of two tail veins and one tail artery are required, as described above.
-
1.
Remove 125I-IAP from the freezer and bring slowly to room temperature. Using suitable containment and a low dead-space glass syringe, carefully remove required volume 125I-IAP (0.2–0.3 MBq per rat ) and dispense into a vial.
-
2.
Evaporate the methanol using a very gentle stream of nitrogen and slowly add injection saline to the 125I-IAP (0.8 ml per rat plus extra to account for syringe dead spaces, etc.). Gently mix.
-
3.
Load a syringe of size suitable for infusion with the 125I-IAP solution (needle must be suitable size for the venous cannula).
-
4.
For anesthetized animals, keep warm, as described above. Check arterial blood pressure and heart rate by connecting the arterial cannula to a pressure transducer and recording device. Then clamp off the cannula and connect it to the fraction collector, loaded with pre-weighed glass tubes, for subsequent blood collection.
-
5.
Inject and flush in 0.1 ml neat heparin (=100 I.U.) via one of the venous cannulae to ensure the blood flows freely from the arterial cannula.
-
6.
Cut one of the venous cannulae to approx. 3 cm in length and connect a syringe containing approx. 0.5 ml Euthatal™. A small “T-connector” may also be used to allow drug administration via this cannula.
-
7.
Set syringe pump speed to 1.6 ml/min (see Note 8 ). Carefully place the 125I-IAP-containing syringe in the pump and connect it to the second venous cannula.
-
8.
Start the stop-clock and unclamp the artery, checking that blood is free-flowing. At 5 s, start syringe pump and fraction collector (see Note 9 ). At 35 s, inject Euthatal™ and stop pump; rapidly excise tissues of interest and stop fraction collector (see Note 10 ). Place tissues in the lidded container to prevent drying. Weigh the blood tubes and cap them. Weigh the tissues and place them in gamma counting tubes.
-
9.
Count the blood and tissue samples on the gamma counter.
3.2.2 Indicator Fractionation Technique
Cannulations of one artery and two veins are required. Alternatively, cannulae attached to shafts of hypodermic needles can be inserted into tail veins percutaneously instead of cannulating veins.
-
1.
Follow points 1–3 above, preparing 0.07 MBq 125I-IAP in 0.05 ml saline per mouse.
-
2.
For anesthetized animals, keep warm, as described above. Check arterial blood pressure and heart rate by connecting the arterial cannula to a pressure transducer and recording device.
-
3.
Set syringe pump speed to 150 μl/min (mouse) or 1.6 ml/min (rat ).
-
4.
Load a 250 μl syringe (for mouse) or 2 ml syringe (for rat) with approx 100 μl saline, attach a 23G needle and position in the pump.
-
5.
Cut the venous cannula as short as possible and inject 0.05 ml of diluted heparin (≡5 I.U.) for mouse or 0.1 ml neat heparin (≡100 I.U.) for rat. Disconnect heparin syringe and attach 125I-IAP syringe and a syringe containing injection saline via a T-piece. Connect syringe containing Euthatal™ to second venous cannula.
-
6.
Clamp the artery cannula, disconnect it from the pressure transducer, and connect it to the syringe pump. Ensure that the pump is set to withdraw and allow it to withdraw very briefly to ensure that the cannula is patent and the syringe is positioned correctly.
-
7.
Start the stop-clock and pump simultaneously. Check that the blood is flowing freely. At 3 s, inject 0.05 ml of 125I-IAP for mouse or 0.2 ml for rat , as a rapid bolus via the venous cannula, followed immediately by 0.05 ml saline from the second syringe. At 13–18 s (see Note 11 ), inject Euthatal™ and immediately pull out full length of arterial cannula and excise the tissue of interest. All the blood should be retained in the cannula. Place the tissue in a pre-weighed gamma counting tube.
-
8.
Attach a saline-filled syringe to the arterial cannula and eject all the blood into a gamma counting tube together with 1 ml of saline.
-
9.
Count the blood and tissue samples on the gamma counter.
3.3 Blood Flow Analysis
3.3.1 Tissue Equilibration Technique
-
1.
Analysis is based on a model which assumes a vascular compartment from which the input function derives a single (extra-vascular) well- mixed tissue compartment (Fig. 1). A small, highly soluble and inert tracer, such as IAP, is assumed to rapidly equilibrate between all blood components and the tissue compartment. In this case, the model based on Kety [25] describes the relationship between the tissue concentration of the tracer at time t, C t(t), and the arterial blood concentration of the tracer at time t, C a(t), by the Equation:
$$ {C}_{\mathrm{tiss}}(t)\kern0.28em =\kern0.28em {k}_1{C}_{\mathrm{a}}(t)\otimes \exp \left(-{k}_2t\right) $$(2)where k 1 is tissue blood flow rate (F) and k 2 is k 1/αλ; α is the effectively perfused fraction of tissue (i.e., the fraction of tissue that is immediately accessible to the tracer); and λ is the equilibrium partition coefficient of the tracer between tissue and blood; ⊗ denotes the convolution integral; in imaging studies, αλ is often referred to as the apparent volume of distribution (VDapp) of the tracer in the tissue [26], C tiss(t) and C a(t) are expressed in radioactivity counts per g tissue and per ml blood, respectively, using 1.05 for the density of blood.
-
2.
In this method, C tiss(t) is measured at only one time-point, i.e., after tissue excision. Hence, only one parameter, k 1 (F), can be estimated from the data (see Note 12 ). λ is approximated from literature values or estimated from separate experiment [27] and α is taken as 1.0 (see Notes 12 and 13 ). Studies have shown that the method is relatively insensitive to small changes in λ because of the short time-scale of the experiment [28]. Also see Table 1.
-
3.
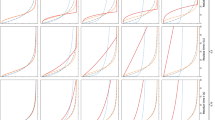
Solving Eq. 2: Data can be fitted to Eq. 2 using a simple ‘Table Lookup Method’. In this method, since the input function is known, the expected tissue activity at the time of excision C tiss (T) can be calculated for each of a range of realistic values of F, using Eq. 2. Direct comparison of the observed C tiss (T) against the table then gives the required estimate of F (Fig. 2). Evaluation of the Integral in Eq. 2 requires a numerical integration routine, which are commonly available in statistical analysis packages, or can be programmed using computer applications such as MATLAB (The Mathworks, USA ©). A further issue, which needs to be taken into account when assessing the accuracy of this type of technique, is the possibility that the input function time course may not be accurately measured because of a time delay between the radioactivity reaching the tissue and reaching the blood collection tubes and because of smearing or dispersion effects occurring on the arterial cannula before blood collection. These delay and dispersion effects can be corrected for (see Note 14 ), but do add further complication to the analysis.
Fig. 2 
Estimation of tissue blood flow rate (F) in the P22 rat sarcoma and several normal rat tissues using the tissue equilibration method with 125I-IAP (a) and 14C-IAP (b). Results in panel (a) were obtained by calculating C tiss from gamma counts of large tissue samples. Data shows effects of the vascular disrupting agent combretastatin A4-P and the nitric oxide synthase inhibitor L-NNA plus the combination of the two. Asterisk represents a significant difference between treated and control untreated tumors. The image in panel (b) was obtained from an untreated P22 tumor by calculating multiple values for C tiss from quantitative autoradiography of tumor sections. The mean F is 3.8 ml/g/min. The image in panel (c) illustrates the vascular networks in the P22 tumor obtained by multi-photon fluorescence microscopy

3.3.2 Indicator Fractionation Technique
-
1.
This method was first used by Goldman and Sapirstein [29], with later modifications [30]. It simplifies the model used in Eq. 2 by assuming that the backflux of the tracer from tissue into the blood is negligible compared with its influx into the tissue, for a short period of time after injection of the tracer (see Note 15 ). Under these conditions, Eq. 2 reduces to:
$$ {k}_1=\kern0.28em {C}_{\mathrm{tiss}}(T)\kern0.28em /\underset{0}{\overset{T}{{\displaystyle \int }}}{C}_{\mathrm{a}}(t)\mathrm{d}t $$(3)where k 1, t, C a(t) are as defined above and C tiss(T) is concentration of tracer in the tissue at the end of the experiment (at time t = T).
-
2.
T is typically set at 10–15 s, during which time collection of sufficient blood samples, as described for the tissue equilibration technique, is difficult. Instead, the constant withdrawal technique can be used. Here, blood is withdrawn from an artery at a constant rate using a pump from t = –T′ to t = T, where –T′ is the time at which the pump is started. A bolus injection of tracer is given at t = 0. Under these conditions,
$$ \underset{0}{\overset{T}{{\displaystyle \int }}}{C}_{\mathrm{a}}(t)\mathrm{d}t={C}_{\mathrm{c}}\left(T+{T}^{\prime}\right)={C}_{\mathrm{c}}{V}_{\mathrm{b}}/r=X/r $$(4)where C c is mean concentration of tracer in the blood sample; V b is volume of blood collected; X is total radioactive counts in the collected blood sample, and r is rate of withdrawal of blood.
-
3.
X/r can be substituted into Eq. 3 and blood flow rate, k 1, can be calculated from a knowledge of the counts, X, pump rate, r, and concentration of the tracer in the tissue at the end of the experiment, C tiss (T). As for the tissue equilibration technique, there are inaccuracies in the measurement of the input function using this technique, associated with delay and dispersion along the plastic cannula. However, the constant withdrawal method means that definition of a concentration-time curve is not required and only the last part of the actual arterial time-course is lost by the blood sampling method. In addition, the experimental set-up of the indicator fractionation method means that the arterial cannula can be kept short, minimizing the delay involved.
3.3.3 Comparison of the Two Blood Flow Methods
The advantages and disadvantages of the classic tissue equilibration method and the indicator fractionation method are summarized in Table 1. Patlak et al. [28] carried out an evaluation of errors involved in the two techniques, which can be summarized as follows:
-
1.
Errors in the tissue equilibration method are minimized if an optimal infusion schedule is used (a ramped schedule is best but a constant infusion is reasonable), timing is measured precisely, and corrections are made for delay and dispersion. Under these conditions, 10–15 % inaccuracy in the value used for λ is well-tolerated in the calculation of F. If precise measurement of λ can be made, this is the method of choice.
-
2.
If λ cannot be measured reasonably accurately, the indicator fractionation technique may be the better option for estimating F. Errors associated with backflux are minimized by a short experimental time. Errors associated with imprecise timing are minimized by bolus administration of the tracer (so that arterial concentration is low at tissue excision). The constant withdrawal method is an added advantage for its simplicity and accuracy. However, backflux cannot be completely prevented (especially with bolus administration) and may introduce significant errors where F is high and/or α is low. Delay and dispersion effects are reasonably well-tolerated.
-
3.
Both techniques require accurate measurement of tracer concentration in the tissue (C tiss).
4 Notes
-
1.
The methodology presented here is based on a single tissue compartment model. This can be derived from the classic Renkin-Crone unit capillary model [31, 32], which gives an explicit relationship between flow, the extraction of substances from blood into tissue, and the mean permeability surface area product of the capillary bed. Recent simulation studies show that the degree of local heterogeneity in capillary architecture and transit times of blood through the capillaries may also affect the precise relationship between flow and extraction of substances from the blood into tissue [33, 34].
-
2.
The basic experimental principles and analytical methods described here also apply to various external imaging techniques that are now available for use in small animals, e.g., positron emission tomography [35]. These techniques allow repeated evaluation of blood flow rate (and other pharmacodynamic end-points) in the same animal, as long as the biological and radioactive half-lives of the tracer are compatible with the time-scale of the experiment. In addition, they allow definition of more than one vascular parameter (see Note 12 below).
-
3.
Instead of obtaining a single value for the blood flow rate within a tissue (usually by calculating C tiss from gamma counts of tissue activity), the variation of blood flow rate within a tissue can be obtained at high spatial resolution (~50 μm) by using a radiotracer that is suitable for autoradiography or phosphor imaging (Fig. 2). In these cases, C tiss is obtained in raster fashion across tissue sections for calculation of corresponding k 1 (F) values [36].
-
4.
Local radiation safety procedures need to be followed for all the techniques described to avoid contamination of personnel and equipment.
-
5.
General anesthesia seriously affects mean arterial blood pressure in rodents, especially in mice, and its effects on tissue blood flow rates need to be considered in planning experiments. Animals can be allowed to recover from general anesthesia induced by inhalational anesthetics following cannulation, but, in this case, procedures for preventing cannula disturbance and minimising pain and distress to the animals need to be implemented [37].
-
6.
Tail cannulations: the tail artery lies relatively deep within a cleft in the cartilage and requires an incision to be made through the overlying connective tissue for it to be accessible. Once freed, it is robust for cannulation; the vein is much more superficial and easily located, although more fragile than the artery and liable to constriction and tearing.
-
7.
A topical vasodilator such as procaine can be used to aid cannula insertion.
-
8.
Volumes of saline solutions of IAP for intravenous administration are chosen to compensate for rate of blood loss during the course of the experiments.
-
9.
A constant infusion schedule for delivery of the radiotracer is described, as it is simple to achieve in practice. However, an infusion schedule that increases with time (ramped) could be employed because this reduces the influence of an incorrect value for λ, on the calculated value of F [28]. The movement of the fraction collector and the infusion/withdrawal rates of the pump need to be carefully calibrated prior to experiments.
-
10.
Timing errors can be significant if blood flow to tissues of interest is not stopped at the instant that the pump is stopped. Also see Table 1.
-
11.
A short duration increases timing errors, but a longer one increases errors associated with backflux of the tracer from the tissue into blood. Also see Table 1.
-
12.
A disadvantage of this particular technique is that the tissue concentration of the tracer is assayed at only one time point. Hence, as noted above, only one parameter (F) can be estimated, whereas values for α and λ have to be assumed. Other, more sophisticated techniques involving noninvasive imaging, such as PET (see Note 2 ), involve a full time course of the tissue to be assayed, allowing estimation of αλ (VDapp) for example, as well as F. This is of particular interest in the case of tumor blood flow, where the effectively perfused tissue fraction (α) (i.e., the fraction of tissue that is immediately accessible to the tracer) is often less than 1.0 because of large intercapillary distances or ischemic regions [26]. However, the spatial resolution of noninvasive imaging cannot compete with the high spatial resolution achievable with the invasive techniques described here (see Note 3 ). In the invasive technique, α is usually assumed to be 1.0. If it is actually less than 1.0, for a sampled tissue region of interest, the measured tissue concentration of the tracer, C tiss, will be low because it is averaged over the whole region, including the inaccessible part. Thus, the calculated value of F will reflect average blood flow for the region and underestimate that of the perfused tissue fraction.
-
13.
Beyond the short time-scale of these experiments, IAP redistributes in tissue in a space-dominated rather than a flow-dominated pattern. At equilibrium, IAP might be expected to distribute in proportion to the tissue water content, such that λ would be similar in all tissues and close to 1.0. However, experimental evidence indicates that, although λ for IAP is close to 1.0 in many tissues, it is somewhat variable [27]. This may relate to its high lipid solubility or it may be a reflection of problems in accessing true values of λ because of loss of the radioactive label from the molecule at long times (hours) after injection.
-
14.
A simple model which can be used to describe dispersion effects is given by the equation:
$$ {C}_{\mathrm{m}}(t)={C}_{\mathrm{a}}(t)\otimes {k}_{\mathrm{d}} \exp \kern0.28em \left(-{k}_{\mathrm{d}}t\right) $$(5)where C m(t) is the measured tracer concentration at the cannula outflow, C a(t) is the inflow concentration, and k d (min−1) is a dispersion constant, which is dependent on flow rate, length, and internal diameter of the cannula and the interaction with blood on its internal surface. k d for a particular cannula and flow rate of blood can be calculated from Eq. 5, if experiments are undertaken in vitro whereby the blood pumped through a cannula at a particular rate is switched rapidly between labelled blood and unlabelled blood and the dispersion effect measured in the outflow. Results from such an experiment are presented in Table 2. Delay (t d) can be estimated directly from the known volume of the cannula and the blood flow rate down the cannula. These values for k d and t d can be incorporated in Eq. 2 to give a working form of the Equation:
Table 2 Example of expressions used to calculate the dispersion constant k d (min−1) from the linear speed (ν in cm per min) of blood flowing down various types of cannulae $$ {C}_{\mathrm{tiss}}(t)\kern0.28em =\kern0.28em \left({k}_1/{k}_{\mathrm{d}}\right){C}_{\mathrm{m}}\left(t+{t}_{\mathrm{d}}\right)+\left(1-{k}_2/{k}_{\mathrm{d}}\right){k}_1{C}_{\mathrm{m}}\left(t+{t}_{\mathrm{d}}\right)\otimes \exp \left(-{k}_2t\right) $$(6)If dispersion effects are small, i.e., large k d, this Equation reduces to Eq. 2. If dispersion effects are marked, i.e., small k d, then the Equation illustrates that failing to take dispersion effects into account has a marked effect on estimates of F. These issues were first quantitatively described by Meyer [38] (but note that a dispersion time constant equivalent to 1/k d was used in this case).
-
15.
In addition to using a short experimental time,T, errors associated with backflux in this technique are minimized if blood flow rate is low and there is a big accessible space in the tissue for the tracer (high α). Note that the short T gives the potential for large timing errors and great care must be taken to time the experiment accurately. As for the tissue equilibration technique, this means that blood flow to tissues needs to be stopped precisely at T. Interestingly, timing errors appear to be less of an issue with this technique than with the tissue equilibration technique for measurement of cerebral blood flow rate [28].
References
Stewart GN (1894) Researches on the circulation time in organs and on the influences which affect it: parts I-III. J Physiol (Lond) 15:1–89
Reyes-Aldasoro CC, Akerman S, Tozer GM (2008) Measuring the velocity of fluorescently labelled red blood cells with a keyhole tracking algorithm. J Microsc 229:162–173
Intaglietta M, Tompkins WR (1973) Microvascular measurements by video image shearing and splitting. Microvasc Res 5:309–312
Fontanella AN, Schroeder T, Hochman DW, Chen RE, Hanna G, Haglund MM, Secomb TW, Palmer GM, Dewhirst MW (2013) Quantitative mapping of hemodynamics in the lung, brain, and dorsal window chamber-grown tumors using a novel, automated algorithm. Microcirculation 20:724–735
Brizel DM, Klitzman B, Cook JM, Edwards J, Rosner G, Dewhirst MW (1993) A comparison of tumor and normal tissue microvascular hematocrits and red cell fluxes in a rat window chamber model. Int J Radiat Oncol Biol Phys 25:269–276
Tozer GM, Prise VE, Wilson J, Cemazar M, Shan S, Dewhirst MW, Barber PR, Vojnovic B, Chaplin DJ (2001) Mechanisms associated with tumor vascular shut-down induced by combretastatin A-4 phosphate: intravital microscopy and measurement of vascular permeability. Cancer Res 61:6413–6422
Oye KS, Gulati G, Graff BA, Gaustad JV, Brurberg KG, Rofstad EK (2008) A novel method for mapping the heterogeneity in blood supply to normal and malignant tissues in the mouse dorsal window chamber. Microvasc Res 75:179–187
Stern MD (1975) In vivo evaluation of microcirculation by coherent light scattering. Nature 254:56–58
Smith KA, Hill SA, Begg AC, Denekamp J (1988) Validation of the fluorescent dye hoechst 33342 as a vascular space marker in tumours. Br J Cancer 57:247–253
Hill SA, Tozer GM, Chaplin DJ (2002) Preclinical evaluation of the antitumour activity of the novel vascular targeting agent Oxi 4503. Anticancer Res 22:1453–1458
Lunt SJ, Akerman S, Hill SA, Fisher M, Wright VJ, Reyes-Aldasoro CC, Tozer GM, Kanthou C (2011) Vascular effects dominate solid tumor response to treatment with combretastatin A-4-phosphate. Int J Cancer 129:1979–1989
Chalkley HW (1943) Method for quantitative morphologic analysis of tissues. J Natl Cancer Inst 4:47–53
Vermeulen PB, Gasparini G, Fox SB, Colpaert C, Marson LP, Gion M, Belien JA, de Waal RM, Van Marck E, Magnani E, Weidner N, Harris AL, Dirix LY (2002) Second international consensus on the methodology and criteria of evaluation of angiogenesis quantification in solid human tumours. Eur J Cancer 38:1564–1579
Weiskoff RM (1993) Pitfalls in MR measurement of tissue blood flow with intravascular tracers: which mean transit time? Magn Reson Med 29:553–559
Messmer K (1979) Radioactive microspheres for regional blood flow measurements. Actual state and perspectives. Bibl Anat 18:194–197
Jirtle RL (1980) Blood flow to lymphatic metastases in conscious rats. Eur J Cancer 17:53–60
Jirtle RL, Hinshaw WM (1981) Estimation of malignant tissue blood flow with radioactively labelled microspheres. Eur J Cancer Clin Oncol 17:1353–1355
Sapirstein LA (1958) Regional blood flow by fractional distribution of indicators. Am J Physiol 193:161–168
Obrist WD, Thompson HK, King CH, Wang HS (1967) Determination of regional cerebral blood flow by inhalation of 133-xenon. Circ Res 20:124–135
Young W (1980) H2 clearance measurement of blood flow: a review of technique and polarographic principles. Stroke 11:552–564
Sakurada O, Kennedy C, Lehle J, Brown JD, Carbin JL, Sokoloff L (1978) Measurement of local cerebral blood flow with iodo [14C] antipyrine. Am J Physiol 234:H59–H66
Tozer GM, Shaffi KM (1993) Modification of tumour blood flow using the hypertensive agent, angiotensin II. Br J Cancer 67:981–988
Trivedi MA (1996) A rapid method for the synthesis of 4-iodoantipyrine. J Labelled Compd Radiopharm 38:489–496
Graham MM, Spence AM, Abbott GL, O’Gorman L, Muzi M (1987) Blood flow in an experimental rat brain tumor by tissue equilibration and indicator fractionation. J Neuro-Oncol 5:37–46
Kety SS (1960) Theory of blood tissue exchange and its application to measurements of blood flow. Methods Med Res 8:223–227
Tozer GM, Shaffi KM, Prise VE, Cunningham VJ (1994) Characterisation of tumour blood flow using a “tissue-isolated” preparation. Br J Cancer 70:1040–1046
Tozer GM, Morris C (1990) Blood flow and blood volume in a transplanted rat fibrosarcoma: comparison with various normal tissues. Radiother Oncol 17:153–166
Patlak CS, Blasberg RG, Fenstermacher JD (1984) An evaluation of errors in the determination of blood flow by the indicator fractionation and tissue equilibration (Kety) methods. J Cerebr Blood Flow Metab 4:47–60
Goldman H, Sapirstein LA (1973) Brain blood flow in the conscious and anaesthetized rat. Am J Physiol 224:122–126
Gjedde SB, Gjedde A (1980) Organ blood flow rates and cardiac output of the Balb/c mouse. Comp Biochem Physiol 67A:671–674
Renkin EM (1959) Transport of potassium-42 from blood to tissue in isolated mammalian skeletal muscles. Am J Physiol 197:1205–1210
Crone C (1963) The permeability of capillaries in various organs as determined by use of “indicator diffusion” method. Acta Physiol Scand 58:292–305
Jespersen SN, Ostergaard L (2012) The roles of cerebral blood flow, capillary transit time heterogeneity, and oxygen tension in brain oxygenation and metabolism. J Cerebr Blood flow Metab 32:264–277
Ostergaard L, Tietze A, Nielsen T, Drasbek KR, Mouridsen K, Jespersen SN, Horsman MR (2013) The relationship between tumor blood flow, angiogenesis, tumor hypoxia, and aerobic glycolysis. Cancer Res 73:5618–5624
Herrero P, Kim J, Sharp TL, Engelbach JA, Lewis JS, Gropler RJ, Welch MJ (2006) Assessment of myocardial blood flow using 15O-water and 1-11C-acetate in rats with small-animal pet. J Nucl Med 47:477–485
Tozer GM, Prise VE, Wilson J, Locke RJ, Vojnovic B, Stratford MRL, Dennis MF, Chaplin DJ (1999) Combretastatin A-4 phosphate as a tumor vascular-targeting agent: early effects in tumors and normal tissues. Cancer Res 59:1626–1634
Richardson CA, Flecknell PA (2005) Anaesthesia and post-operative analgesia following experimental surgery in laboratory rodents: are we making progress? Altern Lab Anim 33:119–127
Meyer E (1989) Simultaneous correction for tracer arrival delay and dispersion in CBF measurements by the H215O autoradiographic method and dynamic PET. J Nucl Med 30:1069–1078
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media New York
About this protocol
Cite this protocol
Tozer, G.M., Prise, V.E., Cunningham, V.J. (2016). Quantitative Estimation of Tissue Blood Flow Rate. In: Martin, S., Hewett, P. (eds) Angiogenesis Protocols. Methods in Molecular Biology, vol 1430. Humana Press, New York, NY. https://doi.org/10.1007/978-1-4939-3628-1_18
Download citation
DOI: https://doi.org/10.1007/978-1-4939-3628-1_18
Published:
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-4939-3626-7
Online ISBN: 978-1-4939-3628-1
eBook Packages: Springer Protocols