
Abstract
Despite increased public awareness of the substantial health risks, tobacco use remains one of the greatest public health concerns around the world. Although cultural influences contribute to tobacco use, the principal reason for sustained tobacco use is the highly addictive nature of nicotine, its primary psychoactive component. One in three individuals who try tobacco will become addicted, and more people use tobacco than any other drug of abuse. Thus, research into the neurobiological mechanisms of nicotine addiction is of great public health relevance, and decades of clinical and pre-clinical studies have substantially improved our understanding of these processes. Like other drugs of abuse, the addictive properties of nicotine are mediated through the mesolimbic dopamine system, where it exerts its reinforcing and rewarding effects. Nicotine acts through specific interactions with nicotinic acetylcholine receptors (nAChRs), a class of ionotropic neurotransmitter receptors expressed throughout the brain. Because of the broad expression of these nAChRs, nicotine exerts broad effects on the nervous system that likely underlie its high degree of co-morbidity with other neuropsychiatric disorders. In this chapter we will discuss our current understanding of how nicotine acts through nAChRs to promote the cellular and physiological changes underlying the behavioral manifestations of tobacco use. We will also consider developmental consequences of nicotine exposure, coincidence of nicotine use with other neuropsychiatric disorders, and current challenges in the field of nicotine and tobacco research.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Addiction
- Animal Models
- Acetylcholine
- Alcohol consumption
- CHRNA4 gene
- Conditioned place preference (CPP)
- Depression
- Diagnostic and Statistical Manual of Mental Disorders (DSM-5)
- Dopamine (DA) system
- Ion Channels
- Interpeduncular nucleus (IPN)
- Locomotor sensitization
- Long-term potentiation (LTP)
- Medium spiny neurons (MSNs)
- Medial habenula (MHb)
- Nicotine addiction
- Nucleus Accumbens (NAc)
- Nicotinic Acetylcholine Receptors (nAChRs)
- Receptor Desensitization
- Obsessive compulsive disorder (OCD)
- Prepulse-inhibition
- Psychiatric disorders
- Schizophrenia
- Self-administration model
- Smoking
- Substance use disorders
- Tobacco
- Ventral tegmental area (VTA)
A Brief History of Tobacco Use
The tobacco plant is indigenous to North and South America, and its use in this region for religious, medical, and recreational purposes dates back thousands of years. Tobacco was introduced to Europe after Christopher Columbus’ discovery of the New World in the fifteenth century and has been prevalent in Western culture ever since. Traditionally chewed or smoked in pipes, American Indians believed that tobacco could cure many ailments, and this belief continued into colonial America. By the middle of the seventeenth century, tobacco had become a major cash crop for American colonists and was major driver of slavery in the following centuries. A precursor to the modern-day cigarette became popular after the American Civil War, and the invention of an automated cigarette rolling machine by James Bonsack in 1880 revolutionized the tobacco industry.
Though scientific and medical journals began publishing articles on health risks associated with tobacco use in the early part of the twentieth century, it was not until 1964 that first Surgeon General’s report on “Smoking and Health” was released. The report revealed many of the health risks associated with smoking and paved the way for new federal regulations of cigarette sales and marketing. As a result, the report is largely credited for the precipitous decline in US smoking rates beginning in the late 1960s. Since then, scientists, medical professionals, and public health officials have continued to study the effects of tobacco use on human health and advocate for policy measures aimed at further reducing smoking prevalence. Policies such as increased taxation and restrictions on public smoking have proven to be effective measures.
Tobacco Use Is One of the World’s Largest Public Health Concerns
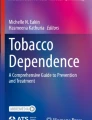
Though smoking rates have declined substantially in the last few decades (Fig. 1a), tobacco use remains one of the greatest threats to public health around the world (Fig. 1b). Tobacco smoke contains more than 4,000 chemicals, many of which are known carcinogens. As a result, smoking is a direct cause of many diseases, including multiple forms of cancer, heart disease, stroke, pulmonary disease, and even depression. Tobacco smoking is the leading cause of preventable death worldwide, killing nearly six million people every year. Included in this number are deaths resulting from exposure to second-hand smoke, which kills ~600,000 nonsmokers each year, more than a quarter of which are children.

Epidemiology of tobacco use. (a) Adult smoking rates in the USA (blue line) have declined steadily since the first Surgeon General’s report on health risks associated with smoking in 1964. Reporting of smoking rates among US high school students (green line) began in 1990 and peaked in the late 1990s. High school smoking rates experienced a rapid decline from 2013 to 2015, possibly due, in part, to the emergence of electronic cigarettes (e-cigarettes), which may now be more popular among high school students than traditional cigarettes (red line) (Data from the American Lung Association, CDC, and Campaign for Tobacco Free Kids). (b) Tobacco use poses a major public health concern and accounts for a significant portion of global mortality. Shown are deaths in millions attributed to the eight leading causes of death worldwide in 2005; the hashed boxes at the top of each bar indicate the number of tobacco-related deaths in that category. All tobacco-related deaths are combined in the right-most bar and color coded to match cause of death (Data from the World Health Organization)
In addition to public health concerns, the tobacco epidemic imposes a major economic burden to society. In the USA alone, smoking-related illness results in more than $300 billion annually in direct medical costs and lost productivity. Tobacco use represents a significant obstacle to global economic development, especially because nearly 80 % of smokers live in low- or middle-income countries.
Despite indisputable negative consequences, tobacco use remains common around the world. Globally, 21 % of adults, about 1.1 billion people, use tobacco. Tobacco use is even more prevalent in high-income countries, which have a combined usage rate of 25 %. Though smoking is more common in men than in women (36 % of adult men vs. 7 % of adult women in the world; 32 % vs. 17 % in high-income countries), women have a more difficult time quitting and are at greater risk for resuming smoking after a quit attempt. Although women smoke less than men, they sometimes report experiencing greater pleasurable effects from smoking and are more sensitive to its effects on body weight.
The primary psychoactive component of tobacco is nicotine, a highly addictive alkaloid which is largely to blame for the continued prevalence of tobacco use. About one third of individuals who try smoking will become addicted and the prevalence of nicotine dependence is higher than that of any other drug of abuse. Furthermore, smoking cessation can be extremely difficult, despite the fact that most smokers report a desire to quit. Some estimates suggest that less than 5 % of unaided quit attempts are successful. In addition, many people report continued smoking in order to curb appetite, relieve stress, or improve mood. In fact, smoking is highly coincident with several neuropsychiatric disorders, including depression, schizophrenia, and other addictions (see Box 2).
A number of genetic loci have been identified that alter susceptibility to smoking, most of which occur in or around genes encoding nicotinic acetylcholine receptor (nAChR) subunits, the primary molecular target of nicotine (Fig. 2). The greatest effects are conferred by allelic variation in a gene cluster encoding α3, β4, and α5 nAChR subunits (located on 15q25), which significantly increases risk of tobacco addiction in humans. A common and well-studied single nucleotide polymorphism (SNP; rs16969968) in CHRNA5, the gene that encodes the α5 nAChR subunit, increases the risk of tobacco dependence by ~30 % in individuals carrying one copy of the variant and more than doubles risk in those with two copies. This is one of the largest effects identified of a naturally occurring polymorphism on human behavior. Among smokers, the same SNP is a major risk factor for the development of lung cancer and chronic obstructive pulmonary disease (COPD) . There are at least four other SNPs in the same gene cluster which are associated with increased incidence of tobacco dependence. Several rare mutations in the CHRNA4 gene are underrepresented in smokers, and biochemical data suggest that the same mutations may confer increased nicotine sensitivity. Lastly, polymorphisms in CYP2A6, an enzyme which metabolizes nicotine, have been associated with smoking behavior and increased cancer risk.

Nicotinic acetylcholine receptors (nAChRs). (a) A schematic of a single nAChR subunit illustrating the large, amino-terminal domain, four transmembrane (TM) domains, two intracellular loops, and a short carboxy terminus. A large intracellular loop between TM3 and TM4 (intracellular domain, ICD) is a likely site for protein-protein interactions. Note that both termini are located in the extracellular domain (Image adapted from Vithani et al. (2011) Physiol Rev 91:1009–1022). (b) Illustration of a pentameric nAChR. Five individual nAChR subunits assemble in neuronal membranes to form a channel that fluxes positively charged ions. ACh binding sites are indicated (Adapted from Changeux J-P (2010) Nat Rev Neurosci 11:389–401, 2010). (c) A top view of the two most highly expressed nAChR subtypes in the brain: the homomeric α7 subunit-containing nAChRs (blue) and heteromeric α4β2 subunit-containing nAChRs (orange and green). Triangles indicate nicotine/acetylcholine binding sites and grey circles represent the channel pore
Animal Models Are Useful for Studying Nicotine Addiction
According to the latest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) , tobacco use disorder is diagnosed when a patient meets at least two of the 11 criteria, which include measures such as increasing amounts of tobacco taken over time, unsuccessful attempts to control use, cravings or strong desire to use tobacco, continued tobacco use despite the presence of a health concern precipitated by tobacco use, requiring higher amounts of tobacco over time in order to achieve the same effect (i.e., tolerance), and presence of withdrawal symptoms during abstinence. Thus, nicotine addiction is characterized by a heterogeneous collection of behaviors revolving around nicotine use. Since addictive behaviors can be influenced by many factors, including genes, environment, and route of administration, nicotine addiction can manifest differently across individuals. Two of the strongest predictors of addiction are the total number of cigarettes smoked in a day and the amount of time from waking to the first cigarette.
Much of what is known about the biological basis of nicotine addiction has resulted from studies in animal models of the disease. Though modeling human behavior in laboratory animals is challenging, rats and mice develop addiction-like behaviors in response to chronic nicotine exposure. Animal models cannot capture the full range of human psychiatric illness, but several paradigms have been established to measure specific aspects of the behavioral effects of nicotine, including reinforcement, drug seeking, and withdrawal.
Conditioned place preference (CPP) and self-administration are two behavioral paradigms used to model drug reward and drug-seeking behavior in rodents. For acquisition of CPP, a rewarding stimulus, such as nicotine, is administered repeatedly to an animal in a specific environmental context. Over time, the animal learns to associate the context with the drug and eventually develops a preference for the reward-paired environment compared with a control environment, an indication of reinforcement and drug seeking. In the self-administration model , rodents are trained to complete operant tasks, such as pressing a lever or nose poking, in order to receive an infusion of nicotine. Self-administration paradigms more closely resemble human addiction, since the animal controls the level and frequency of drug administration. In addition to measuring the reinforcing properties of nicotine, variations of this task can be used to measure motivation (i.e., how hard an animal is willing to work for nicotine), extinction, and reinstatement of drug seeking (i.e., relapse).
Locomotor activity is also commonly assessed following drug treatment. Acute administration of certain doses of nicotine can induce hyperlocomotion in rodents, and repeated administration of the same dose generates progressively greater responses. This so-called locomotor sensitization is a reflection of the ability of drugs to stimulate the dopamine system and can be used as an assay of the ability of nicotine to induce activity in the mesolimbic dopamine circuit.
Importantly, nicotine-mediated behaviors in rodents reflect behaviors observed in human smokers. In mice and rats, cues paired with drug administration, such as presentation of a light, can themselves become reinforcing. The same is true for humans who may, for instance, experience craving when observing someone else smoke or smoke only their preferred brand of cigarettes. Such cues are sufficient to induce reinstatement of drug seeking after forced extinction of the behavior in rodents. Likewise, nicotine-associated cues are thought to contribute to relapse in humans after a period of abstinence from smoking. Thus, drug-paired cues are likely to contribute to the acquisition and maintenance of addictive behavior in rodents and in humans. Furthermore, adolescence appears to be a period of higher susceptibility for nicotine dependence in humans and other species. Adolescent rats acquire CPP at lower doses of nicotine than are required in adult rats. Likewise, both CPP and self-administration of nicotine in adult rodents are enhanced by previous exposure to nicotine. These studies reflect human behavior, since nicotine use during adolescence increases the likelihood of nicotine addiction later in life, and a majority of adult smokers begin smoking prior to 20 years of age.
In addition to the positive reinforcing effects of nicotine, chronic exposure to the drug can induce physical dependence and subsequent cessation can induce a withdrawal syndrome in both humans and laboratory animals. Human nicotine withdrawal is characterized by symptoms such as irritability, restlessness, anxiety, depression, insomnia, increased appetite/weight gain, and craving for tobacco. Similar symptoms are observed in nicotine withdrawn rodents, including negative affect (anxiety and depressive-like behavior), anhedonia, weight gain, and drug craving/seeking. A series of somatic withdrawal symptoms, such as tremors, writhes, teeth chattering, and reduced locomotion, are also observed in rodents. Though not typically experienced by humans, somatic signs can be useful in evaluating withdrawal severity in rodent models of addiction.
Thus, rats and mice develop addiction-like behaviors in response to chronic nicotine exposure, and studies in these animals have been instrumental to our understanding of the neural basis of nicotine addiction. Looking forward, these models will continue to aid in our development of novel treatments by providing a system in which we might identify new therapeutic targets and screen for drug efficacy.
Neurobiological Studies Inform Understanding of Nicotine Addiction
Nicotinic Acetylcholine Receptors Are the Primary Targets for Nicotine in the Brain
Nicotine exerts its effects on the nervous system by binding to, activating, and then desensitizing nicotinic acetylcholine receptors (nAChRs, Fig. 2). Normally activated by the neurotransmitter acetylcholine, nAChRs are highly expressed throughout the brain and are found on both pre- and postsynaptic terminals. Nicotinic receptors belong to the cis-loop family of pentameric ligand-gated ion channels, which also includes receptors for the neurotransmitters, GABA, glycine, and serotonin. There are 17 known nicotinic subunits in mammals (α1-α10, β1-β4, γ, δ, and ε), which assemble in various combinations to form nonselective cation channels. While the α7 subunit can form homomeric receptors [(α7)5], most nicotinic receptors are heteromers, containing at least one alpha-type subunit and one beta-type subunit. The result is a large and highly heterogeneous set of nicotinic receptor subtypes which vary in their expression patterns, channel kinetics, desensitization properties, and affinity for nicotine. α1, β1, γ, δ, and ε subunits are primarily found in muscle, while α2-10 and β2-4 subunits are expressed in the brain and are the most well-studied in the context of nicotine.
The importance of nicotinic receptor diversity is further highlighted by their precise subunit coassembly and unique expression patterns. For example, the widely expressed α4 and β2 subunits nearly always assemble together and their interface forms a high-affinity nicotine binding site. As a result, α4/β2-containing nicotinic receptors are required for many of the neurobiological and behavioral changes associated with nicotine use. The α6 subunit can also assemble with α4 and β2 but only in catecholaminergic (dopaminergic and noradrenergic) neurons. As mentioned, α7 subunits form homomeric receptors, which have a lower affinity for nicotine in vitro but are highly permeable to calcium ions. Receptors containing α3/β4/α5 subunits are essential for fast neurotransmission in the autonomic nervous system, but in the brain are most highly expressed in neurons of the medial habenula (MHb), where they contribute to the aversive effects of nicotine and nicotine withdrawal.
nAChRs Are Activated, Upregulated, and Desensitized by Nicotine
Each nAChR subunit contains a large extracellular N-terminal domain followed by four transmembrane domains, a large intracellular loop, and a short extracellular C-terminus. Nicotine as well as the receptor’s endogenous ligand, acetylcholine, binds to the extracellular interface between two subunits. Once bound, ligands cause a conformational change in the receptor, which opens the ion channel and promotes membrane depolarization. Stimulation of postsynaptic nicotinic receptors increases neuronal excitability and promotes action potentiation, while activation of presynaptic receptors stimulates neurotransmitter release. The sensitivity of nAChRs to nicotine is determined by their composition and stoichiometry. For instance, receptors containing two alpha subunits and three beta subunits are more sensitive to nicotine than receptors containing three alpha subunits and two beta subunits.
In addition to activating nAChRs, nicotine increases receptor number, particularly of high-affinity α4/β2-containing receptors. Nicotinic receptor upregulation has been observed in animal models of nicotine dependence as well as in the brains of human smokers, even 3 or more weeks after nicotine withdrawal. The mechanism for upregulation is posttranslational and involves intracellular binding of nicotine to assembling nAChR subunits and subsequent intracellular trafficking of nAChRs. The brains of smokers, therefore, have increased capacity for nicotine binding, which may contribute to altered neuronal signaling once nicotine is cleared from the brain and acetylcholine signals through these nAChRs.
Although nicotine is a potent nAChR agonist, chronic nicotine exposure results in long-term receptor desensitization and inactivation of nAChRs, the extent of which varies with receptor composition and nicotine concentration. α7 receptors, for example, are rapidly desensitized by extremely high concentrations of nicotine but do not desensitize in the presence of much lower concentrations, which are still capable of activating the receptor. β2 subunit-containing nAChRs, on the other hand, display rapid desensitization in response to very low concentrations of nicotine, which might be maintained by chronic nicotine use. Studies in rodents have shown that differential desensitization of these nAChR subtypes contributes to the dynamics of dopamine neuron firing. For example, desensitization of β2 subunit-containing nAChRs decreases DA release when DA neurons are firing tonically but enhances DA release when DA neurons are firing phasically, as occurs in response to a reward or to reward-associated environmental cues. The physiological consequences of nAChR desensitization are complex and not entirely understood, but it is likely that the chronically elevated nicotine levels experienced by smokers result in phases of activation and desensitization of nAChRs, both of which contribute to physiological and behavioral responses to nicotine in tobacco smoke. It is possible that variability in the balance of nAChR activation and desensitization contributes to individual differences in susceptibility to nicotine addiction. In addition, due to nicotine-induced increases in receptor number, reversal of desensitization following abstinence from nicotine may result in a robust potentiation of nicotinic signaling which contributes to symptoms of withdrawal.
Nicotine Activates the Dopamine System
As for all drugs of abuse, the mesolimbic dopamine (DA) system is required for the rewarding and reinforcing properties of nicotine (Fig. 3). DA neurons of the ventral tegmental area (VTA) send projections to the nucleus accumbens (NAc) prefrontal cortex (PFC), amygdala, hippocampus, and many other brain regions. The VTA receives excitatory and inhibitory inputs from many of the regions to which it projects, as well as a number of brain stem nuclei. Nicotine increases DA transmission from the VTA through a number of nAChR-mediated mechanisms. Activation of α4/β2-containing nAChRs on DA neuron cell bodies increases their excitability and action potential firing, one of the primary mechanisms underlying many of the addiction-related behavioral responses to nicotine. Furthermore, activation of α4/β2/α6* receptors (where * indicates other possible subunits) on DA terminals increases DA release onto medium spiny neurons in NAc. Nicotine can also activate presynaptic α7 nAChRs on glutamatergic terminals in the VTA, resulting in increased glutamate release onto DA neurons, further stimulating these neurons. Nicotine-induced glutamate release results in induction of long-term potentiation (LTP) of those synapses, which contributes to heightened excitability of DA neurons over a longer period of time. Likewise, sustained low levels of nicotine, as occurs in the brains of smokers, can desensitize α4/β2* nAChRs on GABAergic terminals in the VTA resulting in decreased GABA release onto DA cell bodies. This desensitization-mediated reduction in inhibitory tone thus further shifts the excitatory-inhibitory balance in the VTA, again promoting activation. Although α4/β2* nAChRs on DA neurons in the VTA are required for behaviors related to nicotine addiction, the ability of nicotine to induce burst firing of DA neurons and to maintain nicotine self-administration requires expression on both DA and GABA neurons in this structure.

The ventral tegmental area ( VTA ) in nicotine addiction. Schematic highlighting the cellular and molecular mechanisms underlying nicotine-mediated increases in dopamine (DA) signaling. ACh acetylcholine, Glu glutamate, MSN medium spiny neuron, VTA ventral tegmental area, NAc nucleus accumbens (Adapted from Picciotto MR et al. (2008) Prog Neurobiol 84:329–342)
Aversive Effects of Nicotine Are Mediated by the Habenulo-Interpeduncular Pathway
Whereas nAChRs in the VTA are required for the rewarding effects of nicotine, studies of withdrawal and the aversive effects of nicotine have revealed an important role for nicotinic signaling in the habenulo-interpeduncular pathway (Fig. 4). Just posterior to the thalamus, the medial habenula (MHb) is a collection of cholinergic and substance P expressing nerve cells, most of which also corelease glutamate. The MHb has a high density of nicotinic receptors and expresses the highest levels of the α3, β4, and α5 nAChR subunits in the brain. It sends projections through the fasciculus retroflexus to the interpeduncular nucleus (IPN) . Genetic and pharmacological studies have shown that both activation of α3/β4/α5 receptors and activation of the MHb-IPN pathway are required for the negative effects of nicotine, such as the sedative effects induced by high concentrations, as well as withdrawal symptoms. Furthermore, animals in which this pathway is disrupted self-administer more nicotine than wild-type controls, while increased MHb signaling diminishes sensitivity to the reinforcing properties of nicotine. Indeed, the human polymorphism discovered in the α5 subunit may alter smoking behavior by disrupting nAChR signaling in the MHb. Thus, nicotine-mediated activation of the MHb-IPN pathway may elicit a negative motivational signal that serves to limit nicotine intake. Though there appears to be a reciprocal relationship between activity in the VTA and the MHb, the mechanisms by which the habenulo-interpeduncular pathway sends information back to the mesolimbic DA system are not yet clear

The medial habenula ( MHb ) in nicotine aversion and withdrawal. Schematic of the habenulo-interpeduncular pathway, which mediates aversive effects of nicotine and signs of nicotine withdrawal
.
Box 1 Nicotine Alters Neuronal Developmental and Subsequent Behavior
One risk factor for smoking initiation is parental smoking. While environmental factors likely account for some of the association, there is significant data from rodent studies to suggest that nicotine exposure during development results in changes in reward processing that can predispose an individual to addiction. Between 10–12 % of pregnant women in the USA smoked during pregnancy in 2005, suggesting that exposure to nicotine during early development as a result of tobacco smoking is still a public health concern. With the advent of e-cigarettes (see Outlook) and a growing perception that these are safer than tobacco smoking, the level of fetal nicotine exposure is likely to rise.
Human epidemiological studies show that tobacco exposure during gestation results in increased risk of low birth weight, preterm delivery, still birth, and sudden infant death syndrome. While the effects of gestational smoking may be due to exposure to carbon monoxide and other constituents of tobacco smoke, it is possible that nicotine in tobacco may also contribute to morbidity. In utero exposure to tobacco smoke is also associated with increased risk of attention deficit hyperactivity disorder, conduct disorder, antisocial behavior, and substance abuse.
In addition to increased likelihood of nicotine self-administration in rodents and smoking in humans, early nicotine exposure results in deficits in use of auditory, visual, and somatosensory stimuli in attentional and cognitive tasks. This suggests that alterations in circuitry involved in sensory processing may be a particularly prominent neurobiological consequence of exposure to nicotine during critical periods of brain development.
The fetal brain expresses nAChRs at very early stages of development. Rodent and human studies have identified persistent changes in synaptic plasticity, molecular and cellular processes, nAChR number, and neurochemistry of several neurotransmitter systems following developmental nicotine exposure. These molecular and circuit-level changes contribute to the persistent behavioral changes observed in rodent and human studies.
Nicotine exerts a variety of effects on the developing brain. A number of rodent studies have focused on the role of nAChRs in alterations in development of circuits involved in transmitting sensory information between the thalamus and cortex. Developmental nicotine exposure disrupts the synaptic tuning of these circuits, inducing a change in the response of the system in adulthood, and disrupting the transmission of feedback from cortex back to thalamus. This results in impairment in the threshold for transmission of sensory information to the cortex for use in cognitive tasks. Human imaging studies have confirmed that pathways defined in rodents exposed to nicotine are also compromised following fetal and adolescent tobacco smoke exposure. Alterations in brain circuitry following early nicotine exposure have also been identified in pathways related to reward-related behavior. Persistent changes have been identified in dopamine, serotonin, and norepinephrine dynamics. This could be important for changes in likelihood of cigarette smoking and nicotine dependence in exposed individuals but could also result in changes in susceptibility to psychiatric disorders such as depression.
It is clear that developmental nicotine exposure activates and desensitizes nAChRs in many brain areas, resulting in persistent alterations of neuronal function in adulthood. Disruption in thalamus and cortex could contribute to the association between fetal tobacco exposure and attention deficit hyperactivity disorder, whereas changes in the dopamine system may be more critical for changes in rates of smoking and use of other drugs, and alterations in other monoamine signaling may result in predisposition to affective disorders. Acetylcholine is important for all these neuronal functions, so alterations in nAChR signaling as a result of early nicotine exposure would have broad effects on cholinergic signaling in the mature brain.
Overall, it is plausible that the epidemiological association between developmental tobacco exposure and increased risk of deficits in cognition, attention, sensory processing, and neuropsychiatric disorders is due to exposure to nicotine, based on animal studies of early nicotine administration. Further, this may suggest that medications that reverse the plasticity due to nicotine during development could be useful for treating long-term behavioral consequences of tobacco exposure.
Box 2 Nicotine Dependence Is Highly Comorbid with Psychiatric Disorders
While tobacco smoking is driven by nicotine addiction, it is important to note that smokers exhibit a high degree of comorbidity with psychiatric illness (Fig. 5). Cigarette smoking is 2–5 times more common among individuals with psychiatric disorders or other substance use disorders than in the general public, and smokers with coincident psychiatric disorders are significantly less likely to quit smoking than other smokers. Schizophrenia, major depression, bipolar disorder, post-traumatic stress disorder, alcoholism, and cocaine addiction (among others) are all associated with high smoking rates. One notable exception is obsessive compulsive disorder (OCD) , which is associated with lower smoking rates than average (although the reason for this is not clear, it may result, at least in part, from the nature of OCD pathology, which often includes symptoms such as extreme cleanliness and fear of disease).

Comorbidity with nicotine addiction. Graph showing approximate smoking prevalence among populations of people with psychiatric disorders and other substance use disorders. With the exception of obsessive compulsive disorder (OCD) , smoking is significantly more common in people with psychiatric illness than in the general public (green hashed bar) (Adapted from Kalman et al. (2005) Am J Addict 14(2):106–123)
There are several possible explanations for the high coincidence of smoking with psychiatric illness. The first is that common genetic or environmental factors may predispose certain individuals to multiple disorders. This theory is supported by human genetic studies which have identified gene variants in dopamine receptors and the dopamine transporter that are linked to both smoking behavior and psychiatric illness. Another possibility is that individuals with an underlying psychiatric disorder self-medicate with nicotine in attempt to control symptoms like negative affect and impaired cognitive function. Indeed, nicotine may improve working memory and attention deficits in individuals with schizophrenia, and many smokers cite reduced anxiety and improved mood as reasons for continued nicotine use.
These possibilities are not mutually exclusive, and some combination of genes, environment, and biological interaction is likely to underlie observed comorbidities. The role of nicotine in psychiatric illness and the mechanisms underlying the coincidence remain very active areas of research. While there is still much to be learned, our current understanding of some of the more well-studied comorbidities is discussed below.
Tobacco Smoking Is Associated with Higher Incidence of Other Substance Use Disorders
Individuals with substance use disorders have the highest rates of coincident nicotine use. Not only does this population have some of the highest smoking rates, but these individuals tend to be heavy smokers who are highly dependent on nicotine. In fact, smoking-related deaths among alcoholics outnumber alcohol-related deaths, and it is thought that much of the reduced lifespan associated with serious mental illness can be attributed to tobacco use.
Since all drugs of abuse act by perturbing dopaminergic signaling, the mechanisms underlying high smoking coincidence with other substance use disorders are perhaps the most intuitive. Like nicotine, cocaine directly influences DA transmission by inhibiting reuptake of the neurotransmitter and enhancing downstream signaling. Alcohol and opiates can inhibit VTA inhibitory neurons, thereby disinhibiting DA neurons and potentiating DA transmission. When combined with nicotine, DA signaling is further enhanced, thus exacerbating the reinforcing properties of these drugs and facilitating dependence. Human and animal studies support this model, since nicotine enhances alcohol and cocaine consumption. Furthermore, genetic or pharmacological blockade of nAChR signaling can reduce alcohol and cocaine seeking in rodents, and cue-induced craving for cocaine is reduced in humans treated with the nAChR antagonist, mecamylamine. Alcohol consumption also increases smoking behavior in humans, indicating that the effects are likely bidirectional.
Individuals with Schizophrenia Exhibit a High Rate of Smoking
Schizophrenia is a psychiatric disorder that affects close to 1 % of the population. Clinically, it is characterized by a collection of positive and negative symptoms such as hallucinations, delusions, disordered thought, blunted affect, depressed mood, and anhedonia. Comorbidity with tobacco use has been well documented, with most accounts finding that up to 80 % of schizophrenics regularly smoke cigarettes. Smokers with schizophrenia (SCZ) also typically have a much more difficult time quitting. Highly coincident smoking among schizophrenic patients is likely to be the result of genetic or biological predispositions, the ability of nicotine to alleviate some symptoms of schizophrenia, as well as side effects of antipsychotic medications. Evidence from human and animal studies suggests that nicotine may serve to normalize some of the underlying physiological abnormalities in the brain resulting from schizophrenia.
One line of evidence suggests that nicotine-mediated increases in DA signaling serve to alleviate some of the negative symptoms of schizophrenia. In addition to the VTA-NAc circuit discussed above, the VTA sends dopaminergic afferents to the PFC, and activity of these projections is also potentiated by nicotine. Since schizophrenia is associated with low levels of dopamine in the forebrain, nicotine may serve to normalize cortical dopamine levels in these individuals. Potentiation of the mesocortical DA pathway following chronic nicotine exposure results in improved attention and working memory, even in nonpsychotic individuals. Nicotine and smoking have been reported to reduce cognitive disability in schizophrenics, although nicotine-based medication development has not yet resulted in effective treatments for schizophrenia. The effect of nicotine-mediated increases in midbrain DA levels on schizophrenia is not clear, especially since, unlike PFC, midbrain DA levels appear to be elevated in the brain of individuals with schizophrenia at baseline. It is worth noting that antipsychotic medications which share the ability to block DA D2 receptor signaling are largely effective in treating positive symptoms, with little effect on the negative symptoms improved by elevation of cortical dopamine levels.
Additional mechanistic insight comes from studies suggesting that aberrant nAChR signaling, particularly through α7 nAChRs, may contribute to the pathophysiology of schizophrenia. The CHRNA7 gene, which encodes the α7 nAChR subunit, has been implicated in the heritability of endophenotypes associated with schizophrenia, and genetic linkage studies have identified a polymorphism in the CHRNA7 gene as a potential risk factor for the disease. Furthermore, α7 nAChR subunit expression is reduced in the PFC, hippocampus, and thalamus of nonsmokers with schizophrenia, but not in the brains of smokers with schizophrenia, suggesting that nicotine may normalize α7 nAChR-mediated signaling in individuals with schizophrenia. Conversely, normal nicotine-induced upregulation of β2-containing nAChRs is not observed in the brains of smokers with schizophrenia. Indeed, multiple nAChR subunits have been linked to the pathology of schizophrenia, suggesting that signaling through these receptors may be altered across nAChR subtypes.
One of the hallmarks of schizophrenia is the inability to appropriately filter sensory information, which is thought to contribute to higher-order cognitive deficits, like impaired working memory. In unaffected individuals, the neural response to the second of two closely spaced stimuli is significantly smaller than the response to the initial stimulus, a process known as prepulse inhibition . Individuals with schizophrenia, however, display much less sensory inhibition in this and other tests, and this deficit can be normalized by administration of nicotine or pharmacological activation of α7 nAChRs. This process is thought to be mediated, at least indirectly, through acetylcholine signaling in the PFC, which activates α7 nAChRs on inhibitory neurons, shaping the response to the second stimulus. Since α7 nAChR expression is reduced in the brains of individuals with schizophrenia, this ACh-driven inhibition is thought to be disrupted, whereas chronic nicotine exposure may normalize α7 nAChR expression and improve sensory gating.
Neurobiological Factors May Underlie the Comorbidity Between Smoking and Depression
Nicotine dependence is more than twice as prevalent among people with major depression or bipolar disorder than in the general public, and smokers with a history of major depression are 2–3 times more likely to have failed quit attempts than nondepressed smokers. In addition to the primary reinforcing effects of nicotine, many smokers report continued tobacco use in an attempt to control negative affect. Smokers often experience increased feelings of anxiety between cigarettes, and smoking cessation is commonly associated with depressed mood. Nicotine patch has antidepressant effects in humans, and antidepressant drugs have been effective in reducing nicotine intake, suggesting common neurobiological mechanisms. Since nicotine alleviates withdrawal symptoms, it is often reported as having positive effects on mood; however, there is also evidence that nicotine use contributes to the development of depressive symptoms. Smokers are twice as likely to have depressive disorders as nonsmokers, and prolonged abstinence from smoking is associated with decreased stress levels. Thus, chronic nicotine use and mood may have a bidirectional relationship, whereby negative affect results in increased smoking behavior, and smoking promotes negative affect.
Originally proposed by David Janowsky and colleagues in 1972, the cholinergic hypothesis of depression suggests that increased activation of cholinergic signaling in the brain is an underlying cause of depression. This idea is supported by pharmacological evidence from human and animal studies. Depressed individuals have increased levels of choline, the precursor to acetylcholine (ACh). Both unipolar and bipolar subjects show decreased nAChR availability (i.e., fewer free receptors) in imaging studies when actively depressed, but no change in receptor number, suggesting a higher level of ACh signaling during a depressive episode. Individuals with unipolar depression show higher levels of receptor occupancy than subjects who have never been depressed, suggesting that increased ACh signaling may be a risk factor for depression. Furthermore, blockade of acetylcholine esterase, the enzyme which breaks down ACh, results in increased ACh levels and induces depressive symptoms in humans and in rodents.
The fact that nicotine, a nAChR agonist, can alleviate depressive symptoms first appears to contradict this hypothesis, until one considers that chronic nicotine exposure causes long-term desensitization of nAChRs, thus effectively blocking cholinergic signaling. Nicotine replacement therapies (such as the nicotine patch) provide low, desensitizing doses of nicotine which have been effective in alleviating symptoms of depression, even in nonsmokers. In addition, pharmacological blockade of nAChRs has been shown to have antidepressant effects in some human studies (although one large clinical trial of a nicotinic antagonist failed to show efficacy). Together, these data support a model in which signaling through nAChRs promotes depressive symptoms, and nicotine may alleviate these symptoms by desensitizing nAChRs. In smokers, withdrawal symptoms such as depressed mood and anxiety may be precipitated, at least in part, by recovery of desensitized receptors. The same symptoms may therefore promote craving for nicotine and be alleviated by smoking/nAChR desensitization. Thus, fluctuating levels of nicotine in the brains of smokers may result in self-propagating cycles of heightened and depressed mood.
Outlook
The reduction of smoking rates by more than half since the Surgeon General’s Report of 1964 is an incredible public health success. The consequence of changing the perception of cigarette smoking from a ubiquitous social habit to a dangerous addiction that is one of the major causes of heart disease and cancer has been a dramatic change in the number of adolescents who start smoking and an enormous increase in the number of adults who have quit smoking. The number of lives saved as a result of this shift in public perception and behavior is enormous.
Another major success has been the great progress in understanding the basic molecular and circuit-level mechanisms underlying nicotine reward and reinforcement, aversion, and withdrawal. The combination of pharmacology, molecular genetics, anatomy, neurophysiology, and behavior has been extremely fruitful in moving forward the field studying the neurobiology of nicotine addiction. This has resulted in the development of a scientifically based medication for smoking cessation and represents a real success in translation of basic science to address this critical public health challenge. The ability to offer tools to aid individuals who have decided to quit smoking has been another important piece contributing to the dramatic decrease in smoking rates since the middle of the twentieth century.
Despite these important successes, there are still many challenges that remain for the field. The rapid increase in e-cigarette use presents many new questions that remain to be answered. E-cigarette users are carrying out an epidemiological experiment, and the outcome will not be known for many years. If e-cigarette use contributes to a further decrease in the prevalence of tobacco smoking, there could be an ongoing decrease in tobacco-related deaths; however, if e-cigarette users become dual users and also start smoking, the number of smokers may begin to rise again. The perception that nicotine use is less harmful than tobacco use could contribute to an erosion of the current negative perception of tobacco products.
It is also not yet known what the long-term consequences of e-cigarette use may be. It is clear that developmental exposure to nicotine can result in long-term changes in neuronal function and behavior, and an increase in use of e-cigarettes during pregnancy could increase those risks. The neurobiological effects of flavorants added to e-cigarette liquid, including menthol, sugars, and other tastants, are also relatively unknown. It is likely that menthol decreases irritation and increases intake of nicotine, but it may have additional effects on nicotine addiction. Sugars and flavors are attractive to adolescents and likely contribute to e-cigarette use in younger individuals but may also act as cues that maintain nicotine use and may potentiate nicotine reinforcement directly through shared neurobiological pathways. More study is necessary to clarify these issues.
Another area that needs further study is the comorbidity between smoking and psychiatric illnesses, particularly depression and schizophrenia. The neurobiological basis for these comorbidities is still not fully understood, and there is a need for medication development to help individuals with psychiatric illness quit smoking. While it is more difficult for individuals with schizophrenia or depression to quit smoking, there have been clinical trials with these populations, often neglected in initial development of smoking cessation treatments, which have shown promising results. On the other side, the comorbidity between smoking and psychiatric illness has shed some light on potential nicotinic mechanisms that contribute to depression and schizophrenia. However, while there have been some suggestions that nicotinic medications may be helpful for a subset of patients, there have not yet been successful new medications for schizophrenia or depression based on nicotinic targets. New approaches may be necessary to move beyond nAChRs to novel neurobiological interventions for these psychiatric illnesses that take into account biophysical studies of receptor desensitization, pleiotropic localization, and effects on reciprocally inhibitory circuits that require precise balance for optimal behavioral function.
Finally, there is still a need for new therapeutics to help smokers who wish to quit. Current medications are significantly better than an unaided quit attempt, but more than half of smokers who quit using even the most effective medications still relapse. Like all addictions, tobacco smoking is complex and results from behavioral responses to cues in the environment associated with smoking, stressful life events that precipitate smoking relapse, and neuronal plasticity that increases the likelihood that cues and stress will reactivate the pathways leading to nicotine craving. Novel interventions that interrupt these associations, reverse nicotine- and DA-induced plasticity, and provide new behavioral responses to cues and situations that elicit craving would be the ideal outcome and one that the field is working toward.
References
Abbott LC, Winzer-Serhan UH (2012) Smoking during pregnancy: lessons learned from epidemiological studies and experimental studies using animal models. Crit Rev Toxicol 42:279–303
Antolin-Fontes B, Ables JL, Gorlich A, Ibanez-Tallon I (2015) The habenulo-interpeduncular pathway in nicotine aversion and withdrawal. Neuropharmacology 96:213–222
Bierut LJ (2011) Genetic vulnerability and susceptibility to substance dependence. Neuron 69:618–627
Changeux JP (2012) The nicotinic acetylcholine receptor: the founding father of the pentameric ligand-gated ion channel superfamily. J Biol Chem 287:40207–40215
Freedman R (2014) α7-nicotinic acetylcholine receptor agonists for cognitive enhancement in schizophrenia. Annu Rev Med 65:245–261
Kalkhoran S, Glantz SA (2015) Modeling the health effects of expanding e-Cigarette sales in the United States and United Kingdom: a Monte Carlo analysis. JAMA Intern Med. [Epub ahead of print]. http://www.ncbi.nlm.nih.gov/pubmed/26322924
Mineur YS, Picciotto MR (2010) Nicotine receptors and depression: revisiting and revising the cholinergic hypothesis. Trends Pharmacol Sci 31:580–586
Mwenifumbo JC, Tyndale RF (2009) Molecular genetics of nicotine metabolism. Handb Exp Pharmacol 192:235–259
Picciotto MR, Kenny PJ (2013) Molecular mechanisms underlying behaviors related to nicotine addiction. Cold Spring Harb Perspect Med 3:a012112
Simon P, Kong G, Cavallo DA, Krishnan-Sarin S (2015) Update of adolescent smoking cessation interventions: 2009–2014. Curr Addict Rep 2:15–23
Wing VC, Wass CE, Soh DW, George TP (2012) A review of neurobiological vulnerability factors and treatment implications for comorbid tobacco dependence in schizophrenia. Ann N Y Acad Sci 1248:89–106
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media New York
About this entry
Cite this entry
Miller, M.B., Picciotto, M.R. (2016). Nicotine Pharmacology, Abuse, and Addiction. In: Pfaff, D., Volkow, N. (eds) Neuroscience in the 21st Century. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-3474-4_157
Download citation
DOI: https://doi.org/10.1007/978-1-4939-3474-4_157
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-3473-7
Online ISBN: 978-1-4939-3474-4
eBook Packages: Biomedical and Life SciencesReference Module Biomedical and Life Sciences