
Abstract
In the last 40 years, only rifapentine and bedaquiline have been approved in the USA for the treatment of active tuberculosis. Therefore, one focus of research involves optimizing the current antituberculosis drugs’ pharmacokinetic and pharmacodynamic properties. The aim of this chapter is to review both the pharmacokinetics and pharmacodynamics of the antituberculosis drugs. Specifically, the pharmacokinetic properties of absorption, distribution, metabolism, and elimination are reviewed for each drug. Regarding pharmacodynamics, we discuss pharmacodynamic modeling, mechanisms of resistance, and current methodologies used to evaluate a drug’s susceptibility to Mycobacterium tuberculosis. As a whole, we highlight the importance of pharmacokinetic/pharmacodynamic (PK/PD) modeling and the challenges faced in applying PK/PD to tuberculosis. Finally, therapeutic drug monitoring (TDM) is discussed as a tool that provides clinicians a means to optimize a drug’s PK/PD relationship for an individual patient.
Access provided by CONRICYT – Journals CONACYT. Download protocol PDF
Similar content being viewed by others


Key words
1 Introduction
There is evidence of tuberculosis (TB) since prehistoric times, and it is hypothesized that Mycobacterium tuberculosis (Mtb) might have been responsible for more deaths than any other infection in history [1]. In 2012, an estimated 8.6 million people became ill with TB, and the disease caused an estimated 1.3 million deaths [2]. TB is considered to be the second leading killer as sole infectious agent , with the leading killer considered to be the human immunodeficiency virus (HIV). That said, TB is the leading cause of death among patients with HIV [3], and one of the major causes of death among women of reproductive age [2].
The initial drug used for TB treatment was streptomycin (SM) [4, 5]. However, the use of a single agent rapidly promoted the emergence of resistance [5]. In an effort to prevent drug resistance, combined therapy was evaluated. Initially p-aminosalicylic acid (PAS) was evaluated with SM, and in 1952, isoniazid (INH) was introduced [4, 5]. INH has strong early bactericidal activity (EBA), rapidly reducing the number of bacilli in sputum. INH is continued throughout therapy in an effort to prevent resistance. A three-drug regimen, with an initial 6-month intensive phase of SM, PAS, and INH, followed by PAS and INH for 12 more months, proved to be more effective than the two drug regimen. This regimen helped introduce the concept of an initial intensive phase, followed by a continuation phase [5]. Murine studies with pyrazinamide (PZA) demonstrated its sterilizing activity when combined with INH against Mtb [6]. Studies with rifampin (RIF) demonstrate similar sterilizing behavior [7, 8]. Sterilizing activity is the ability to kill off persisting organisms, and to prevent post-treatment relapses. Sterilizing activity thus is the most sought-after characteristic in a TB drug. Regimens containing INH and RIF could be completed in only 9 months, half of the prior duration without RIF. Further, studies proved that RIF and PZA had synergistic activities [4]. The addition of PZA to INH and RIF reduced the duration of therapy from 9 to 6 months. PZA appeared to produce most of its sterilizing activity during the first 2 months of therapy, while RIF has this effect throughout treatment [4]. A randomized clinical trial demonstrated that an intensive phase regimen of INH, RIF, PZA, and SM, followed by a 4-month continuation phase of INH and RIF promoted very low relapse rates. The current “first-line” regimen, according to the World Health Organization (WHO) follows the same pattern, substituting ethambutol (EMB) for SM [9]. EMB is recommended as the fourth drug, along with INH, RIF, and PZA, to further prevent the emergence of resistance, since susceptibility data often are delayed, or absent altogether. Further studies aimed at shortening the duration of therapy to less than 6 months were unsuccessful, primarily in terms of preventing post-treatment relapses [10]. The structures of the TB drugs are shown in Fig. 1.

Chemical structure of the main drugs used on the treatment of tuberculosis. The figures were drawn with the software Chemsketch version 14.01, 2012
Resistance to at least INH and RIF characterizes multidrug-resistant tuberculosis (MDR-TB ) [11]. The current treatment recommendation for MDR-TB is to use any remaining first-line drugs, plus a fluoroquinolone [levofloxacin (LEVO) or moxifloxacin (MOXI) ], and an injectable agent [amikacin (AK) , kanamycin (KM) , SM or capreomycin (CM)]. Other “second-line” drugs that might be used, depending on susceptibility data, include cycloserine (CS), ethionamide (ETA), and PAS. “Third-line” drugs also used for TB include clofazimine, linezolid, amoxicillin/clavulanate, imipenem, macrolides, and high-dose isoniazid. These drugs are especially important for the treatment of extensively drug-resistant tuberculosis (XDR-TB), characterized by MDR-TB plus resistance to a fluoroquinolone and at least one injectable agent. In 2012, bedaquiline (TMC-207) was approved by the US Food and Drug Administration (FDA) for the treatment of multidrug resistance as a part of the combination therapy [12]. In 2013, delamanid (OPC-67683) was similarly approved by the European Medications Agency (EMA) [13].
The aim of this chapter is to review different aspects of the pharmacokinetics (PK) and pharmacodynamics (PD) of TB drugs. We begin with a review of the mechanisms of action and mechanisms of resistance for the TB drugs, followed by current methodologies to evaluate TB drug susceptibility. Next, we review PD models and their application to TB drugs. Finally, we highlight the use of therapeutic drug monitoring (TDM) as a means of optimizing treatment for individual patients. We note why the current drugs are used, and point out important gaps in our knowledge. As a whole, we highlight the importance of PK/PD and the challenges faced in applying it to TB treatment.
2 Mechanism of Action
A general overview of the mechanisms of action for the TB drugs is shown in Fig. 2.

Known or proposed targets for the TB drugs
2.1 First Line Drugs
RIF inhibits the DNA-dependent RNA-polymerase, thus preventing the transcription of DNA to RNA [14]. The RNA polymerase enzyme has the following subunits: α 2 , β, β′, and σ. The inhibition occurs through the binding of the drug to the β subunit, encoded by the rpoB gene (same gene where mutations can cause drug resistance) [15]. RIF has potent, concentration-dependent bactericidal activity, and starts to kill microorganisms within minutes [8]. RIF displays sterilizing activity throughout the entire treatment period [4].
INH is a pro-drug , activated by the mycobacterial enzyme KatG [16]. The drug inhibits enzymes responsible for the synthesis of cell wall lipids. Specifically, INH inhibits the inhA protein activity for the synthesis of mycolic acids for the cell wall [17]. INH has strong bactericidal activity, and is particularly effective at the beginning of treatment against actively replicating microorganisms [18]. INH is not particularly effective against persisting bacilli [5]. INH use is maintained throughout treatment in an effort to prevent resistance. The absence of sterilizing activity is a characteristic seen among current TB drugs whose mechanism of action is based on cell wall inhibition.
PZA also is a pro-drug , and it is only active at an acidic pH. Mtb enzyme nicotinamidase/pyrazinamidase converts it to pyrazinoic acid (POA), which becomes trapped within the bacilli [19, 20]. Debate continues regarding its precise mode of action. It is hypothesized that POA, as an uncharged acidic conjugate (HPOA), causes acidification of the cytoplasm. This leads to the inhibition of important enzymes, and the disruption of the membrane potential. PZA only appears to kill microorganisms with low rates of metabolism, because they are unable to prevent HPOA accumulation and acidification [5]. The drug kills extracellular microorganisms, and in combination with RIF, it is responsible for the elimination of “persister” organisms. PZA’s sterilizing activity is evident primarily during the first 2 months of therapy.
EMB inhibits mycobacterial cell wall synthesis [21, 22]. The drug inhibits the synthesis of arabinogalactan by preventing the polymerization of arabinose by an arabinosyl-transferase. The drug has moderate bactericidal activity in the initial phase of the treatment but it lacks sterilizing activity [4, 23, 24]. EMB’s main use is to prevent further drug resistance while susceptibility data are pending. Once the susceptibility results are available, and if the microorganism is susceptible to the other three drugs, EMB can be stopped. EMB also is used as part of MDR-TB treatment regimens.
2.2 Second Line Drugs
Fluoroquinolones inhibit topoisomenrase II, also known as DNA gyrase , in Mtb. In other microorganisms these drugs also inhibit topoisomerase IV, absent in Mtb [25]. DNA gyrase is a bacterial enzyme responsible for preserving the superhelical twists in the DNA [26]. This enzyme consists of two subunits A and two subunits B, encoded by the genes gyrA and gyrB, respectively [25]. These drugs possess EBA and sterilizing activity [27].
Aminoglycosides inhibit protein synthesis by binding to the 16S ribosomal RNA sequence [28]. This inhibition does not affect human protein synthesis, since the ribosomal RNA structures are different [29]. Although CM is a polypeptide and not an aminoglycoside, it is often placed in the same category as the aminoglycosides, “the injectable agents,” because of similarities in terms of dose, route of administration, pharmacokinetics, and toxicity [30]. All injectable agents are highly bactericidal against Mtb [31]. However, they lack potent sterilizing activity.
CS inhibits two enzymes, preventing peptidoglycan synthesis and d-alanine metabolism : d-alanine-d-alanine ligase, and alanine racemase, respectively [32]. ETA is a pro-drug, activated within the microorganism by a mono-oxygenase enzyme that is encoded by the ethA gene [17]. ETA inhibits the inhA protein activity that is responsible for the synthesis of cell wall mycolic acid (similar mechanism as INH). The mechanism of action of PAS has been debated for many years but may involve the inhibition of dihydrofolate reductase [33]. PAS displays tuberculostatic activity against Mtb [34]. In combination, it enhances the activity of SM and INH [33].
3 Development of Resistance
Mycobacterium tuberculosis acquires spontaneous chromosomal mutations that generate resistance to antimicrobials, with different frequencies depending on the drug [35]. The frequencies are approximately 1 in 106 microorganisms for INH and 1 in 108 microorganisms for RIF. Considering that a TB lesion may contain 108 microorganisms or more, mutant organisms are likely to be present. These will be spared when administering a single antimicrobial agent. When administering drugs with different mechanisms of resistance, the probability of resistance to both being present in a single bacterium is the sum of the probability for each drug. For INH and RIF, the probability of selecting a dual-resistant mutant would be 1 in 1014 microorganisms. INH and RIF have among the strongest early bactericidal effects , and therefore are effective in reducing the bacillary burden and preventing resistance in combined therapy. EMB has intermediate EBA, and PZA has the lowest EBA of the first line drugs.
Spontaneous mutations that confer resistance to fluoroquinolones happen in the frequency range of 2 in 106 microorganisms to 1 in 108 microorganisms [25]. Therefore 1–100 resistant Mtb are expected within the TB lesion. Cross-resistance also has been described for the fluoroquinolones. If there is diminished susceptibility to one of the drugs within the class, it is likely that the susceptibility is reduced for all fluoroquinolones [25].
The genes associated with resistance mutations, and the corresponding gene products, are shown for each TB drug in Table 1. The relationship with the mechanism of action with the resistance gene is described in Sect. 2 for the majority of the drugs.
Patient adherence to treatment is thought to play an important role in the prevention of drug resistance. This topic presents an important challenge, considering the long treatment duration, and the need for multiple drugs, each with adverse effects. After a study demonstrated the possibility of domiciliary treatment as opposed to long stays in a sanatorium, treatment costs were drastically reduced [5]. At the same time, the means for assuring regular drug administration, directly observed therapy (DOT), was initiated only gradually. Large numbers of patients failing to take drugs regularly often is blamed for much of the current drug resistance. In the US, DOT consists of the direct supervision of drug intake by a member of the healthcare team, and now is offered to a majority of TB patients throughout their treatment.
Considering the difficulty of seeing a patient 7 days a week, most TB programs provide a drug holiday over the weekend [36]. A study conducted by Drusano and colleagues evaluated the effect of drug holidays on the emergence of resistance to rifampin and moxifloxacin, using an in vitro system. They concluded that the 5/7 days regimen generated resistance to moxifloxacin, while the 7/7 days regimen did not. Another study by Srivastava et al., based on clinical trial simulations, concluded that around 1 % of TB patients develop drug resistance solely due to PK variability [37]. Dartois, however, points out the influence of PK variability on noncompliance [38]. She states that a patient with high drug exposure might not develop resistance because of missing doses while a patient with low drug exposure may. The impact of PK variability on resistance reinforces the importance of therapeutic drug monitoring (TDM) discussed in Sect. 17.
In addition to the factors discussed above, other limitations exist in the current treatment of TB. The flexibility of doses with regard to differences in body weight is low and this factor can provide variability in drug exposure among patients . The current doses were optimized many years ago when the mean population weight was significantly lower than today. In addition, due to evolution Mtb strains present MIC distributions that might differ from place to place [39, 40]. Therefore, there is a need for revising the current TB drug doses in order to avoid resistance.
4 Susceptibility Testing
The ultimate aim of the drug susceptibility test (DST) is to verify if the isolate differs from the wild-type Mtb in terms of susceptibility to specific antimicrobials [41]. DSTs can be classified as qualitative or quantitative. Qualitative tests suggest susceptibility or resistance, but do not provide a specific value. Quantitative tests determine the MIC, the smallest concentration that produces 99 % or more of inhibition on the microorganism population. The interpretation of the qualitative test is restricted to “susceptible,” “intermediate,” and “resistant” without a final MIC value. To interpret MIC results it is important to take into consideration the relationship with the drug concentrations achieved at the infection site, the correlation between the isolate MIC, and the MIC from other strains of the same species, as well as previous use of antimicrobial agents. The results of DST are solely suggestive. It is the clinician’s responsibility to consider the drug’s metabolism and pharmacology, patient specific characteristics, and the use of concomitant drugs, among other factors [42].
Drug susceptibility testing on TB patients’ samples is performed with the objective of evaluating the adequacy of the drugs for treatment, to confirm if a treatment failure is due to drug resistance, and to estimate the prevalence of drug resistance [43]. Some of the limitations of drug susceptibility testing include the fact that the environment conditions are different than the ones in the host [42]. This includes the fact that a unique microorganism is grown in an environment with plenty of nutrients. However, one result that can always be used in the clinic is the evaluation of resistance. If the microorganism is resistant to a certain antibiotic in vitro, there is a good chance that it will be resistant in the patient as well.
Direct and indirect methods have been used for DST on TB isolates [44]. The direct method refers to the direct inoculation of the sample. The advantage of this approach is a shorter time for obtaining results. The indirect method requires the isolation of the microorganism prior to susceptibility testing. Advantages of the indirect approach include a more precise inoculum size, and reduced contamination by other organisms.
The most common solid media used for Mtb are the egg-based Löwenstein–Jensen (L–J) and the agar based 7H11 [45]. L–J media presents some disadvantages, such as a high batch-to-batch variation (depending on the egg quality), difficulties on distinguishing colonies from debris, and obtaining consistent drug concentrations. In contrast, the 7H11 media is transparent, promoting an easy differentiation of colonies from debris and therefore small colonies can be detected earlier. However, plates are expensive, with a short half-life (1 month) and they have to be protected from light that can cause degradation and formation of formaldehyde, toxic to the mycobacteria.
Both direct and indirect methods can be used in agar plates by the proportion method [44]. “Critical” drug concentrations are incorporated in the agar. Those concentrations are empirical without relationship to concentrations obtained in the human body. It is presumed that the patient will not respond to the treatment if the result of the test is “resistant.” The sample is inoculated in quadrants with and without drug and the percentage of resistance is calculated based on this relationship. The isolate is considered susceptible if the drug completely inhibits growth and at least 100 colonies are found on the control (agar without drug), and resistant if there is at least 1 % of growth on the agar containing drug in relation to the control.
Different systems have been used for liquid media [45]. The Bactec 460 TB system is based on the use of radioisotopes. The microorganisms metabolize [14C] palmitic acid to 14CO2, detected by the equipment [45]. The production and quantity of 14CO2 is directly proportional to the growth of the microorganism. Some limitations of this system include the impossibility of evaluating colony morphology, the overgrowth of contaminants, cost, the disposal of the radioisotopes and safety, considering the necessity of using syringes with needles. This system was discontinued due to the use of radioisotopes.
The BACTEC 960 MGIT system is a continuous monitoring system based on the use of mycobacterial growth indicator tubes (MGIT) [45]. These tubes contain a fluorescence sensor that is bound to oxygen. The sensor consists of silicon rubber that contains ruthenium pentahydrate. Initially, there is no fluorescence. However, as the mycobacteria (or other microorganisms) metabolize the bound oxygen, the indicator starts to fluoresce. The instrument then is able to detect the change in fluorescence, and it calculates a number (growth index) that is used in an algorithm to determine growth.
Both indirect qualitative and quantitative analysis can be performed for the BACTEC systems [44]. Regarding the qualitative analysis, resistance is indicated if the daily growth index in the drug containing-vial is higher than the observed growth of the control diluted 1:100. For the quantitative analysis (MIC definition), three drug concentrations are necessary. The lowest concentrations correspond to the highest MIC found for wild strains [41] and the sample is considered susceptible if the MIC is lower or equal to this concentration. The MIC is the sample with the lowest drug concentration where minimal or no growth index increase is detected.
It has been demonstrated that both sensitivity and time to growth are similar for Bactec 460 TB and BACTEC 960 MGIT system and superior to solid media [45]. The advantage of the BACTEC 960 MGIT system over the BACTEC 460 TB system is the lack of need for radioisotopes, the reduced potential for cross-contamination, reduced labor, the possibility of continuous monitoring and electronic data management [45].
To perform DST with PZA, the pH of the broth has to be reduced to 6 (usually 6.8–7), due to the fact that the drug is more active at lower pH values [44]. For more details about DST and critical drug concentrations we recommend the following books by Leonid Heifets [41, 44].
Molecular tools can be used to reduce diagnostic time through the evaluation of mutations associated with resistance [46]. Campbell and colleagues used molecular methods to detect TB drug resistance and compared the results with the phenotypic data, as well as calculated accuracy values. The results of the study support the use of molecular methods to detect resistance to TB drugs. However, it is important to emphasize that molecular tests do not replace the use of culture and the DST [47]. Phenotypic and genotypic results need to be evaluated together to provide more accurate clinical information.
The adequacy of the current recommended susceptibility breakpoints and their clinical relevance has been a topic of much discussion. Mtb’s evolution was pointed out as a reason for the inadequacy of the previously established breakpoints, as well as the variability in the MIC values according to different regions, in addition to PK variability [39, 48]. Gumbo evaluated the currently used critical concentrations in terms of the probability of achieving an area under the curve/MIC that correlates with 90 % or more of maximal Mtb kill in 90 % or more of patients [40]. This study embraced the use of Monte Carlo simulations using 10,000 virtual patients. The author proposed that the susceptibility breakpoints of isoniazid, rifampin, and pyrazinamide should be lowered, while the concentrations of moxifloxacin and ethambutol were adequate. A change in the current ofloxacin breakpoint from 2 to 0.5 μg/mL was suggested by a study that also used Monte Carlo simulations to evaluate the probability of target attainment [49].
5 PK/PD Indices
When evaluating the PK/PD indices it is important to take into account the role of protein binding . The binding of drugs to proteins is an important factor that influences the amount of drug that can penetrate into the tissues (at the site of infection) and exert its effect [50, 51]. The serum protein binding is especially important when it is higher than 70–80 %, considering that any small change in the binding can have a significant effect on the free fraction [51].
Anti-infective drugs have been classified into two major groups according to the killing profile: time-dependent killing and concentration-dependent killing [52, 53]. The parameters associated with the concentration-dependent killing drugs are given by the ratio of the area under the curve of the free drug concentration over the MIC (fAUC/MIC) or the ratio of the maximum drug concentration over the MIC (f Cmax/MIC) [35]. The effect of the concentration-dependent drugs increases with an increase in dose. Fluoroquinolones, aminoglycosides and rifamycins are examples of concentration-dependent drugs. Once above the MIC by twofold to fourfold, the effects of the time-dependent drugs do not increase with an increase in dose. For these compounds the effect depends on the time that the drug concentration remains above the MIC (T > MIC). Beta-lactams are examples of time-dependent killing compounds. Considering that the effect within the PK/PD parameter is given by the ratio of an exposure variable to a potency variable (MIC), the higher the MIC value, the lower the microbiological effect of a drug [54].
5.1 Limitations of the Use of PK/PD Indices
The PK/PD indices use the drug concentrations in the plasma or serum [53]. This approach has the drawback of not taking into consideration the tissue distribution, and historically, protein binding was not considered. Additionally, the MIC provides important information regarding the potency of the interaction between the microorganism and the drug, but does not offer information about the effect of the drug over time [55]. The MIC does not generate specific information regarding the rate of antibactericidal effect and how different doses can affect this rate [53]. The MIC is a static parameter that relies on the bacterial count at a certain time point. It does not take into consideration that different microorganism growth and death rates can generate the same final MIC value. The MIC also does not supply information about a possible postantibiotic effect of the compound [55].
6 Pharmacodynamic Models
An alternative approach in relation to the PK/PD parameters is to evaluate the efficacy of antimicrobials with time-kill curves [53]. This methodology considers the microbial growth and kill as a function of time and drug concentration. In some systems, it is possible to mimic the human PK drug profile and therefore expose the microorganism to this change in concentration over the time. Mathematical models can be used to analyze the data and through the use of simulations, the optimal dosage regimen can be identified. This approach presents several advantages over the use of the MIC: direct comparison of the effect of different drug concentrations, more detailed information regarding the PK–PD relationship, and information about the effect of the antimicrobial over time. Time-kill curves can be obtained from in vitro systems as well as animal models. In this section we will provide information about some commonly used in vitro systems for mycobacteria, as well as animal models for TB.
6.1 In Vitro Models
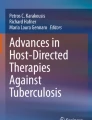
Regarding in vitro models, the hollow fiber system (HFS) frequently has been used to perform time-kill curves with different drugs and Mtb [36, 56, 57]. The HFS contains hollow fiber cartridges and the microorganisms are placed in a peripheral compartment, as shown in Fig. 3a. Semipermeable hollow fibers separate the central compartment from the peripheral and allow the transference of nutrients and drug, but not microorganisms, according to the membrane pore cutoff [56]. The drug is added in a dosing port located in the central compartment. Peristaltic pumps continuously infuse broth into the central compartment and at the same rate remove broth containing drug from the central compartment to waste. The pump rates are set in such a manner that the human plasma drug profile can be mimicked within the system. Media samples are serially collected and plated. Time-kill curves are obtained by plotting the change in the colony-forming unit per mL (CFU/mL) over time.

The hollow fiber system cartridge (a) and the dilution system (b). Adapted from Vaddady PK et al. 2010 [59]
An alternative model was developed by Budha and collaborators based on previously developed in vitro systems and is shown in Fig. 3 b [58]. A peristaltic pump continuously infuses broth into the main double-armed flask while a second pump is set at the same rate and removes broth from the main flask through a filter that prevents microorganism elimination. Drug doses are added on a lateral arm. The rates at which the pumps work allow the bacteria to be exposed to the human PK profile of the drug within the main flask. The double-armed flask is kept at 37 °C by water recirculation through a water jacket and the culture is maintained homogeneous through the use of a magnetic stirrer. The samples are collected and further plated in the same manner as described for the HFS.
The in vitro models represent a simplification of what occurs in vivo [59]. The differences are related to pathogen, host and PK factors . Regarding the pathogen factors, the majority of the microorganisms present different growth rates in vitro in relation to in vivo. Additionally, host factors, such as the immune response, are not fully captured, and plasma protein binding may not be taken into account.
6.2 Animal Models
Animal models take into account the interaction between the microorganism, the host and the drug, which is not possible with in vitro systems [60]. The vast majority of preclinical TB studies were performed with mice, rabbits, and guinea pigs [61]. In addition, nonhuman primates and cattle models have been used. Considering the three species, mice are the least vulnerable to infection (even less vulnerable than humans) followed by the rabbit and then the guinea pig, which is extremely vulnerable. Infection is commonly done by aerosol, but it can also be done by intravenous injection.
The mouse model has proved to generate reliable data regarding sterilizing and bactericidal drug activity [60]. In addition this model is able to represent the activity of the current TB drugs reasonably well, though mice do not develop necrotic granulomas as humans do [52, 60]. More recent models with the so-called Kramnic mouse may be more human-like [62]. After infection the granuloma in the guinea pig and in the rabbit progress to caseation. Due to the low cost, small size, and large amount of data available, the mice model is still the method of choice, with the exception of studies that require caseation [63]. In order to describe the drug’s bactericidal effect, lung tissue homogenates are obtained to determine the CFU/mL. During these studies the emergence of resistance also can be evaluated. To study the sterilizing drug activity, studies longer than 2 months are necessary.
Some of the drawbacks in using animal TB infection models are related to the fact they do not entirely reflect human disease. Some of the factors that differ are the course of the disease over time, drug susceptibility, and the disease characteristics such as granuloma formation .
7 Challenges to Obtaining Clinical Pharmacodynamic and Tissue Pharmacokinetic Data
Tuberculosis affects different organs in the human body. The main targets are the lungs, and for a drug to reach the site of action it needs to be transported from the blood to the lesions—which may not be vascularized—and penetrate into caseous granulomas to reach Mtb [64]. Doses for the first line TB treatment were established many years ago at a time when pharmacokinetics and pharmacodynamics were used sparingly as dose optimization tools. Therefore, drug penetration was not taken into account and this represents a major factor why today we have suboptimal doses. The unique structure of the lungs make the acquisition of human data difficult regarding drug penetration, information about the temporal kill profile of the microorganisms during treatment, as well as data about resistance patterns.
Data from drug concentrations in the epithelial lining fluid (ELF ) is often equated to the extracellular drug concentrations in the pulmonary tissue [65]. Although these drug concentrations are considered to be in equilibrium with the extracellular fluid, it does not represent the drug concentration inside the TB lesion. The TB granuloma is protected by a fibrous wall and may contain caseous material with different pH values in relation to healthy tissue. These factors could promote different patterns of drug penetration into the lesions as compared to healthy tissue. Although this approach offers an alternative considering the protected location of the infection, its clinical significance has not been proven yet.
Sputum samples are used to evaluate the resistance of clinical isolates. However, it has been demonstrated that the lung cavity presents an environment that favors the development of resistance [66, 67]. Additional drug resistance has been demonstrated in the cavity in relation to sputum [66, 67]. The lack of vascularization in the caseous lesions results in diminished delivery of oxygen and nutrients, generating metabolic quiescence that leads to a reduction of Mtb cellular proliferation [64]. In addition, the lack of vascularization leads to a reduced penetration of drugs as well as T lymphocytes. These factors lead to an increase in drug tolerance within the lesion.
7.1 Rifamycins
The rifamycins consist of three drugs used in the treatment of TB : rifampin, rifabutin, and rifapentine. First introduced in the late 1960s, rifampin is the most important of TB drugs. The rifamycins work by inhibiting RNA polymerase. Consequently, mutations in the rpoB gene encoding RNA polymerase can result in the formation of resistant organisms.
The rifamycins are concentration-dependent killers of TB. Both Cmax/MIC or AUC/MIC are associated with mycobacterial killing. Studies reveal that the rifamycins concentrate within macrophages, although higher intracellular concentrations may not equal higher intracellular activity [68]. Burman et al. point out that there is large variability in study results [69].
Clinically evaluating the PD properties of the rifamycins can be difficult. Rifamycin monotherapy leads to resistance by most pathogens, necessitating the use of combination therapy. However, separating the extent of the rifamycins’ effectiveness from companion drugs is problematic. Additionally, unless measured in vitro, the immune system “interferes” with evaluating the killing of Mtb by rifampin (or any antimicrobial), thus, HFS are often used to assess the clinical utility of anti-TB drugs , including the rifamycins .
7.2 Rifampin
The current recommended rifampin dose for active TB disease is 600 mg. Arrival at this dose is somewhat cloudy, but Van Ingen et al. give three reasons initial investigators chose this particular dose: (1) cost of the drug at the time was prohibitive due to its semisynthetic nature (2), concern over possible toxicity at higher doses, and (3) a 600 mg dose provided a Cmax between 8.8 and 12 μg/mL, which is 40–60 times the MIC of Mtb, not taking into account protein binding [70]. This Cmax/MIC suggests that 600 mg would be more than sufficient to eradicate Mtb. However, even a modest reduction in dose to 450 mg resulted in a significant decline in rifampin’s activity [71]. EBA also decreases with a 300 mg dose, but increases with higher doses [72].
For rifampin, many early studies pointed to Cmax/MIC as the parameter most associated with efficacy. However, recent studies by Jayaram and Gumbo suggest a greater correlation with the AUC/MIC [57, 73]. Gumbo et al. used a HFS to show increased killing of Mtb with increasing AUC [57]. In agreement, Jayaram et al. identified the AUC/MIC as the PK/PD parameter most associated with microbial killing using an aerosol infection model [73]. However, Cmax/MIC was the parameter most associated with prevention of resistance. Gumbo et al. noted that a fCmax/MIC > 175 is required for the prevention of rifampin monoresistance [57].
Caution is necessary when attempting to translate model results to humans. Human pulmonary TB primarily consists of extracellular bacilli while murine TB models are primarily intracellular. Additionally, as many researchers point out, animal models may have many features that limit their usefulness. We discuss this further in the rifapentine section..
7.3 Rifabutin
Rifabutin shares some structural features with rifampin, but differences exist in their PK properties due to rifabutin’s increased lipid solubility [74]. This increased lipophilicity leads to a larger volume of distribution, a decreased clearance and, thus, a much longer half-life. Despite a much lower Cmax/MIC (approximately 7.5 μg/mL) compared to rifampin, rifabutin seems to be as active as rifampin [69, 75]. Additionally; rifabutin’s inductive capabilities are much less than rifampin’s (~40 %) [76]. Unfortunately, rifabutin is a CYP3A4 substrate, resulting in many bidirectional interactions with CYP inhibitors (e.g., protease inhibitors). Rifabutin, unlike rifampin, is limited by concentration-related toxicities. The risk of patients experiencing anterior uveitis, neutropenia and thrombocytopenia increases with increasing concentrations.
7.4 Rifapentine
A cyclo-pentyl derivative of rifampin, rifapentine has a much longer half-life (~12 h) than rifampin. The longer half-life was thought to lend itself to intermittent dosing, but in humans, that has not proven to be the case. Additionally, early in vitro and murine studies indicated rifapentine was more potent than rifampin [77–79]. However, clinical trials show rifapentine to be no more active than rifampin [80–82]. Study 29 compared 10 mg/kg rifampin plus standard therapy (INH, PZA, EMB) to 10 mg/kg rifapentine plus standard therapy during the first 2 months of treatment. The study showed no difference in outcomes (time to culture conversion ) between the two groups [81]. Three possible reasons were offered by the authors: (1) rifapentine’s high protein binding might have detracted from its effect, (2) the dichotomous endpoint used in the study reduced statistical power, and (3) the medications generally were taken without food, which increases rifampin absorption but decreases rifapentine absorption.
One reason for this discrepancy between preclinical and clinical studies may be the animal model used. In the murine model, rifapentine looked superior to rifampin, but in the guinea pig model, the two rifamycins were similar, just as in Study 29 [83]. Guinea pigs, when infected with TB, develop necrotic granulomas similar to humans with Mtb concentrated extracellularly rather than intracellularly. Mice, on the other hand, do not develop necrotic granulomas and Mtb are primarily intracellular. Rifapentine is believed to penetrate macrophages better than rifampin, which would account for the greater efficacy in in vitro and murine studies [68]. Extracellular activity is comparable between the two [68].
Increasing the dose of rifapentine could result in greater efficacy. However, unlike rifampin, rifapentine’s dose–response curve appears to flatten just short of a 1200 mg dose. Doubling the dose from 600 to 1200 mg does not result in a proportional increase in exposure. In a recent POP PK analysis by Savic et al., modeling and simulation showed that, while rifapentine exposure increased less than proportionally, there was no plateau in exposures from 450 to 1800 mg [84].
As with isoniazid , Dr. Mitchison makes a case for rifapentine’s Cmax as the parameter most associated with efficacy rather than AUC, citing Study 29 as an example [85]. He advises that future murine studies are conducted with a “chronic” disease model whereby mice are infected for months rather than a couple of weeks [86]. This model would allow for the presence of persister populations of Mtb. Further, he suggests using liquid media rather than solid media [85]. However, Neuremberger et al. argue that the duration infection in the murine studies is long enough to produce persisters [87].
8 Isoniazid
Along with rifampin, isoniazid is a main drug in TB treatment . The complex interplay between isoniazid pharmacokinetics and pharmacodynamics is often difficult to unravel. Mutations in the N-acetyl transferase (NAT-2) gene lead to two distinct rates of clearance. Whether or not this difference in clearance affects outcomes is often debated.
Isoniazid is a prodrug, converted to its active form by the catalase peroxidase enzyme (KatG) . The activated intermediate is believed to be an isonicotinoyl radical which couples to NAD+/NADPH and forms an adduct [88]. This INH-NAD adduct is responsible for antitubercular activity by blocking mycolic acid synthesis [16]. Mutations disrupt catalase peroxidase’s activity, resulting in an INH resistant organism [89, 90]. The most common mutation, accounting for 30–60 % of KatG mutations, is a point mutation, S315T [90, 91]. This alteration in the KatG enzyme confers complete resistance to INH at 1–2 μg/mL. A mutation in the inhA gene also confers resistance to isoniazid but to a lesser extent. InhA, an enoyl reductase enzyme, looks to be the main target for the INH-NAD adduct. Resistance to this target occurs in approximately 1 in 107 bacteria. Mutations in inhA confer resistance to not only isoniazid, but the structurally similar antitubercular drug ethionamide [92, 93]. Some evidence exists that higher doses of isoniazid (16–18 mg/kg/day) can overcome low-level resistance [94].
Isoniazid is considered bactericidal and produces a post-antibiotic effect which can last up to 5 days [95]. The clinical relevance of this effect is not known. Isoniazid eliminates Mtb in the log-phase stage of growth, causing a rapid decline in bacilli within the first few days of administration. This decline in bacillary rate is referred to as early bactericidal activity (EBA). Isoniazid’s decline in bactericidal activity is attributed to the reduction of bacteria in log phase; however, Gumbo et al. believe it is due to the emergence of isoniazid resistance within the bacterial population [96]. Mitchison et al. disagree, stating there are no clinical data to support this and growth rates are slower in actual patients [97]. Regardless of the mechanism, the PD parameter primarily associated with efficacy is either Cmax or AUC. Gumbo et al. identified the AUC/MIC as the PK/PD parameter primarily associated with both microbial kill and prevention of resistance [98]. However, Mitchison et al. maintain Cmax as the PK parameter primarily associated with efficacy [85]. Knowing the appropriate PK parameter associated with efficacy may determine what TB drugs are used together. For instance, Weiner et al. state that the reason once weekly isoniazid/rifapentine was less effective than a twice weekly regimen was due to low isoniazid concentrations, in other words, a “pharmacokinetic mismatch.” [99] The authors suggest a companion drug with a higher AUC may prove more effective. However, Srivastava et al. contend that a pharmacokinetic mismatch does not lead to emergence of resistance to either isoniazid or rifampin [100].
9 Pyrazinamide
A prodrug, PZA is converted to its active form, pyrazinoic acid, by the bacterial pyrazinamidase enzyme . Most mycobacterial species are resistant to PZA. PZA’s activity is limited to Mtb, and M. africanum. Resistance is conferred through mutations in the pncA gene that encodes pyrazinamidase [101]. The exact mechanism of action has yet to be fully elucidated [102–104]. Pyrazinoic acid seems to be the active constituent. PZA is most effective in an acidic environment but Mtb appears not to consume any significant amount of acid, thus, it is believed that only pyrazinoic acid created within Mtb is active [19, 104]. PZA’s preference for an acidic environment makes it difficult to assess resistance through culture methods. Alternative methods for assessing resistance include genetic sequencing of pncA, the Wayne Assay, a color metric assay, which assesses pyrazinamidase activity, or molecular based assays [105].
PZA’ s efficacy appears to be dose-dependent . Currently, the recommended US dose is 25 mg/kg daily or 50 mg/kg twice weekly. Some studies suggest higher doses should be used to maximize efficacy (>30 mg/kg/day). A murine and guinea pig study by Ahmad et al. showed dose-dependent activity at human-equivalent doses. Utilizing an in vitro PK/PD model examining PZA’s sterilizing activity against Mtb (pH of 5.8) Gumbo et al. state that the current PZA dosing recommendation of 20–25 mg/kg/day is suboptimal. The authors’ modeling suggests doses of 3000–4000 mg per day (40–60 mg/kg/day) are necessary.
The PK/PD parameter primarily associated with PZA activity is believed to be AUC/MIC [106]. Gumbo et al., utilizing a HFS, showed that PZA’s sterilizing effect correlated best with AUC/MIC while the time above the MIC correlated with suppression of resistance [106]. However, as stated previously, the MIC depends on the pH of the media used. For example, the highest PZA MIC against 21 susceptible Mtb strains was shown to be eightfold lower at a pH of 5.5 (less than 50 μg/mL) than at a pH of 5.95 (400 μg/mL) [107]. The variability seen in vitro may be less than the variability seen within the lysosomes of macrophages, which is believed to range between a pH of 4.8–7 [108].
The primary concern with using higher doses is the fear of hepatotoxicity. INH and RIF are potential hepatotoxins, so the rate of hepatotoxicity due solely to PZA is difficult to determine. Early PZA studies using higher doses showed an association between PZA and an increased incidence of hepatotoxicity. However, a meta-analysis by Pasipanodya and Gumbo suggests that a majority of cases may be idiosyncratic [109]. Additional adverse reactions include GI upset, arthralgia and an increase in uric acid concentrations [110]. The 1959 USPHS study of PZA and INH showed PZA dose-related increases in hepatotoxicity. In the study, 4 of 160 (2 %) patients given PZA 25 mg/kg daily, developed hepatotoxicity while 11 of 167 (7 %) given PZA 40 mg/kg daily developed hepatotoxicity [111]. Hepatotoxicity in the high dose group was associated with elevated bilirubin and symptoms of liver dysfunction. A meta-analysis of 29 studies by Pasipanodya and Gumbo suggest hepatotoxicity is not dose related but idiosyncratic [109]. They did note a trend toward increasing frequency of hepatotoxicity at doses greater than 40 mg/kg but that doses of up to 60 mg/kg were not predicted to have a significant increase in hepatotoxicity. The mechanism through which toxicity occurs is unclear. In the same study, the most frequent adverse event was arthralgia which was associated with higher doses, however, the clinical importance of this side effect was considered “nonsevere” [109].
10 Ethambutol
EMB is a synthetic agent that was specifically designed to be used against Mtb. It is believed EMB targets arabinosyltransferases that are necessary for the synthesis of arabinan (in arabinogalactan), a cell wall component. Inhibiting this synthesis leads to mycolic acid accumulation and eventually cell death [21, 112]. EMB is bacteriostatic at lower doses with MICs in the 0.5–2 μg/mL range, depending upon the media used. Higher doses of EMB can be bactericidal in vitro. Resistance occurs from mutations primarily in one of the genes encoding arabinosyltransferases, designated embC, embA, and embB (embCAB operon).
The most important adverse event seen with EMB is optic neuritis . The incidence of optic neuritis is low with standard doses in patients with normal renal function. It may add to visual problems in patients with preexisting ocular conditions, such as cataracts or diabetic retinopathy. Ezer et al. report a cumulative incidence of visual impairment of 22.5 per 1000 persons with permanent impairment at 4.3 persons per 1000 [113]. Snellen charts are used to test for visual acuity while Ishihara color plates are used for green–red color discrimination. Tests should be conducted at baseline and throughout treatment. Adverse vision changes are dose related with an increased incidence seen with 30 mg/kg/day compared with 15–25 mg/kg/day. Visual changes in patients on EMB generally are reversible once EMB is discontinued, though not always. Additional adverse events include GI disturbance, arthralgia, and neutropenia and thrombocytopenia .
11 Fluoroquinolones
11.1 Levofloxacin and Moxifloxacin
Oral LEVO bioavailability is close to 100 % and absorption is fast, with a Tmax range of 0.8–2.4 h [114]. The drug penetrates well into most tissues with a volume of distribution of 1.1 L/Kg. LEVO binds mainly to albumin with protein binding ranging from 24 to 38 %. The protein binding does not depend on serum drug concentrations. MOXI bioavailability is higher than 85 %. The TMAX is about 2 h, while the volume of distribution is around 2.7 L/kg [115]. MOXI protein binding is around 50 %. Fluoroquinolones can cross the placenta and can be detected in breast milk. The kidneys primarily clear LEVO, while MOXI is eliminated by the liver (52 %) and by the kidney (20 %). The elimination half-life is 7.4 h for LEVO and 6.5 h for MOXI when measured in TB patients [116]. Considering that the kidneys eliminate the majority of LEVO, caution has to be taken with patients that present renal dysfunction and MOXI might be a better option [30]. The fluoroquinolones present GI side effects such as nausea, diarrhea and vomiting. They also can cause tendinitis, tendon rupture and phototoxicity. MOXI seems to be more toxic then LEVO in terms of QT interval prolongation. Currently, the recommended doses for LEVO are 750 and 1000 mg once a day (orally or intravenously), while the MOXI dose is 400 mg once a day.
In vitro and in vivo studies demonstrated absence of induction or inhibition of the cytochrome CYP P450 and as a consequence no drug interactions associated with this metabolizing enzyme are expected, however, RIF reduces MOXI concentrations 25–30%, probably through induced sulphation or glucuronidation [117]. An increase on the effect of warfarin and its derivatives was noticed in patients taking the drug concomitantly with LEVO [117]. In addition, altered blood glucose concentrations have been described for patients taking diabetic drugs. LEVO interactions with other drugs used for TB is not common [25]. The drug absorption might be reduced by the concomitant ingestion of antacids with multivalent cations [25].
12 Aminoglycosides and Polypeptides
12.1 Amikacin, Kanamycin, Streptomycin, and Capreomycin
These drugs are commonly prescribed once resistance to SM has been demonstrated [30]. The drugs are intravenously administered at a dose of 12–15 mg/kg 5–7 days a week, and 20–27 mg/kg 2 or 3 days per week [115]. When administered intramuscularly, the drugs take between 30 and 90 min to be absorbed. The intravenous infusions typically last 30 min. The drugs present low plasma protein binding, with a volume of distribution in the range of 0.25–0.30 L/kg. No metabolites have been described so far. The drugs are eliminated by the kidneys with elimination half-lives in the range of 2–4 h and with the clearance in parallel to the creatinine clearance. The main side effects for these drugs are related to auditory, vestibular and renal toxicities. Reversible non-oliguric acute tubular necrosis might increase the serum creatinine. Renal cation loss also has been demonstrated. Periodic monitoring of blood urea nitrogen, serum creatinine, calcium, potassium, magnesium is recommended. Physical examinations for vestibular changes also are recommended. Injectable TB drugs may enhance the nephrotoxicity of other drugs, such as amphotericin B, and they may enhance the effects of neuromuscular blocking agents in selected patients [115].
13 Ethionamide
A structural analog of INH, ETA also inhibits mycolic acid synthesis. Cross-resistance between INH and ETA is possible. Mutations in the inhA structural gene or in the promotor region typically cause resistance to both INH and ETA. Mutations in the katg gene affect only INH, allowing the use of ETA [118, 119].
ETA is usually administered twice a day at the doses of 250–500 mg [115]. The drug is adequately absorbed, and the Tmax is in the range of 1.5–2.5 h (500 mg dose). The plasma protein binding ranges from 10 to 30 %. Some ETA reaches the CSF, but CSF concentrations may be below the MIC. It also promptly crosses the placenta. The PK/PD of ETA have not been adequately studied. Based on some similarity to INH, one might posit that AUC/MIC is the most important parameter. In light of that, it is easy to see why ETA is a weak TB drug, because both Cmax/MIC and AUC/MIC are low. Further, Time > MIC is brief, so ETA has very little going for it. The drug is mostly metabolized in the liver and the sulphoxide metabolite can be converted back to the parent drug [30]. ETA has significant GI side effects manifested in the majority of patients as nausea and in many patients as vomiting. ETA suppositories can be taken together (or singularly) with a reduced oral dose in order to prevent the GI side effects [115]. Another important side effect is hypothyroidism that is more common in patients also treated with PAS .
14 Para-Amino Salicylic Acid
PAS, structurally similar to aspirin, is available as a granule dosage form . Its exact mechanism of action is unknown. It is believed PAS inhibits dihydropteroate synthase (DHPS) in Mtb by competing with its structural analog, para-aminobenzoate (PABA), a necessary precursor in folate synthase, though research continues [33, 120].
As with aspirin, PAS may cause GI upset. GI complaints are the most common side effects experienced with PAS and increases with increasing dose. PASER®, a sustained-release, enteric-coated, granule dosage form was created to lessen these side effects. The granules typically are administered as a packet of small beads, which can be sprinkled onto soft food (provided that they are not chewed), or poured into the mouth and washed down with liquid.
PAS is given two to three times daily. It is metabolized by N-acetyl transferase 1 (NAT-1) . The parent drug is predominately cleared by the liver, with metabolites renally cleared. As noted, PAS has the potential to cause hypothyroidism and patients should be monitored for this side effec t.
15 Cycloserine
Cycloserine, sometimes called “psycho-serine” because of its untoward CNS side effects, is one of the less pleasant drugs taken by TB patients. A small molecule (molecular weight = 102 g/mol), cycloserine easily penetrates the CNS. The drug works by disrupting the incorporation of d-alanine into peptidoglycan, an integral component of the bacterial cell wall. The appropriate PK/PD parameter associated with efficacy is unknown, while toxicity appears to be concentration-dependent. CNS side effects are the primary concern with administering cycloserine. Vega et al. estimate the incidence of anxiety, depression, and psychosis each occurs in 12–13 % of patients [121]. The exact mechanism for causing CNS effects is unknown, but may be through its actions as a partial agonist of the N-methyl-d-aspartate (NMDA) receptor [122, 123].
16 Bedaquiline
At the time of this writing, bedaquiline (Sirturo®) is the latest drug to be approved for use in TB treatment in the US. A diarylquinoline, bedaquiline represents the first novel class of anti-TB drugs in over four decades. Bedaquiline inhibits the proton pump of adenosine triphosphate (ATP) synthase, a necessary enzyme in the synthesis of Mtb [124]. No cross-resistance with first- and second-line TB drugs occurs, due to its unique mechanism of action. Some cross-resistance may be seen with the reserve TB drug clofazimine [125]. Currently only approved for use in MDR TB, bedaquiline shows bactericidal activity against other mycobacterial species. Bedaquiline is active against both sensitive and drug resistant strains with an MIC of 0.03 μg/mL [126]. An early murine study indicates AUC as the PD parameter most associated with efficacy [127]. Rouan et al. administered bedaquiline to mice at doses of 15, 30, or 60 mg/kg divided daily (5 days per week), twice weekly, or once weekly. Bactericidal activity correlated with total weekly dosing (and exposure) rather than frequency of administration [127].
The primary concern with bedaquiline is the potential for QT prolongation. An additive, or even synergistic, prolongation in the QT interval may be seen when administered with other QT-prolonging agents such as the FQs and the macrolides [128]. Thus, close monitoring of ECGs are necessary .
17 TDM
As with many other conditions, TDM can benefit TB patients by individualizing drug therapy. TDM can reduce the risk of toxicity, or increase the likelihood of efficacy. Drug therapy can be modified to achieve specific, targeted concentrations. Patients with TB often experience reduced serum drug concentrations because of (1) a low initial dose, (2) malabsorption, or (3) drug–drug interactions. All of these problems can be alleviated through TDM [129].
Multiple factors may influence drug absorption, including: disease states (e.g., diabetes, HIV), food, antacids, or gut transporters altered by concurrent medications. Drugs may be malabsorbed, undergo delayed absorption. Measuring serum concentrations at two time points (typically 2 and 6 h post dose) can distinguish between the two problems. TDM allows for a prompt change in dose, and contributes to a more rapid and complete response to treatment [129].
18 Conclusions
The clinical pharmacodynamics of the TB drugs were insufficiently studied in the past, but significant efforts have been made in recent years to better understand and control therapy. Many treatment centers in developing nations still rely on clinical diagnosis, perhaps supplemented with sputum microscopy. Under such conditions, treatment remains empiric. Other centers use cultures and susceptibility testing. Most often, “critical” concentrations are used, but more focus has been placed on using MICs, similar to what is done in most other infections. Combining MIC values with PK parameters, such as Cmax, the AUC, or Time > MIC, gives clinicians the ability to target desired PK/PD values.
Determining the appropriate targets can be difficult with TB, because multiple drugs are used simultaneously. Lacking clear data regarding synergist combinations, it seems reasonable to optimize each drug within these combination regimens. New drugs are being developed to treat Mtb and MDR-TB, but these new drugs will be combined with older, weaker second- and third-line TB drugs. Further research is needed to optimize these new combination regimens.
Several studies suggest that higher doses of TB drugs should be used, especially RIF and PZA, in order to increase efficacy. Certain diseases, including diabetes and HIV, may reduce TB drug concentrations. Further, high interindividual and intraindividual PK variability can be seen with TB drugs. The current standard doses might not be adequate for certain patients. TDM is a useful tool for determining the appropriate doses of the TB drugs on a case-by-case basis.
References
Daniel TM (2006) The history of tuberculosis. Respir Med 100:1862–1870
World Health Organization (2013) WHO Global tuberculosis report 2013
World Health Organization (2012) HIV and TB (TB/HIV).
Fox W, Ellard GA, Mitchison DA (1999) Studies on the treatment of tuberculosis undertaken by the British Medical Research Council tuberculosis units, 1946-1986, with relevant subsequent publications. Int J Tuberc Lung Dis 3:S231–S279
Mitchison DA (2004) Antimicrobial therapy of tuberculosis: Justification for currently recommended treatment regimens. Semin Respir Crit Care Med 25:307–315
McCune RM Jr, Tompsett R (1956) Fate of Mycobacterium tuberculosis in mouse tissues as determined by the microbial enumeration technique. I. The persistence of drug-susceptible tubercle bacilli in the tissues despite prolonged antimicrobial therapy. J Exp Med 104:737–762
Grosset J (1978) The sterilizing value of rifampicin and pyrazinamide in experimental short-course chemotherapy. Bull Int Union Tuberc 53:5–12
Dickinson JM, Mitchison DA (1981) Experimental models to explain the high sterilizing activity of rifampin in the chemotherapy of tuberculosis. Am Rev Respir Dis 123:367–371
Organization WH (2010) Treatment of tuberculosis: guidelines, 4th edn. WHO Press, Geneva, Switzerland
Fox W (1981) Whither short-course chemotherapy? Br J Dis Chest 75:331–357
Francis J Curry National Tuberculosis Center and California Department of Public Health (2008) Drug resistant tuberculosis: a survival guide for clinicians, 2nd edn. Francis J Curry National Tuberculosis Center and California Department of Public Health
FDA news release (2012) http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm333695.htm. Accessed 2 Dec 2014.
EM Agency (2013) (CHMP) CfMPfHU, London
Wehrli W (1983) Rifampin: mechanisms of action and resistance. Rev Infect Dis 5(Suppl 3):S407–S411
Floss HG, Yu T-W (2005) Rifamycins-mode of action, resistance, and biosynthesis. Chem Rev 105(2):621–632
Timmins GS, Deretic V (2006) Mechanisms of action of isoniazid. Mol Microbiol 62:1220–1227
Vadwai V, Ajbani K, Jose M et al (2013) Can inhA mutation predict ethionamide resistance? Int J Tuberc Lung Dis 17:129–130
Jindani A, Dore CJ, Mitchison DA (2003) Bactericidal and sterilizing activities of antituberculosis drugs during the first 14 days. Am J Respir Crit Care Med 167:1348–1354
Zhang Y, Mitchison D (2003) The curious characteristics of pyrazinamide: a review. Int J Tuberc Lung Dis 7:6–21
Zhang Y, Wade MM, Scorpio A, Zhang H, Sun Z (2003) Mode of action of pyrazinamide: disruption of Mycobacterium tuberculosis membrane transport and energetics by pyrazinoic acid. J Antimicrob Chemother 52:790–795
Mikusova K, Slayden RA, Besra GS, Brennan PJ (1995) Biogenesis of the mycobacterial cell wall and the site of action of ethambutol. Antimicrob Agents Chemother 39:2484–2489
Sreevatsan S, Stockbauer KE, Pan X et al (1997) Ethambutol resistance in Mycobacterium tuberculosis: critical role of embB mutations. Antimicrob Agents Chemother 41:1677–1681
Botha FJ, Sirgel FA, Parkin DP, van de Wal BW, Donald PR, Mitchison DA (1996) Early bactericidal activity of ethambutol, pyrazinamide and the fixed combination of isoniazid, rifampicin and pyrazinamide (Rifater) in patients with pulmonary tuberculosis. S Afr Med J 86:155–158
Mitchison DA (2000) Role of individual drugs in the chemotherapy of tuberculosis. Int J Tuberc Lung Dis 4:796–806
Ginsburg AS, Grosset JH, Bishai WR (2003) Fluoroquinolones, tuberculosis, and resistance. Lancet Infect Dis 3:432–442
Wolfson JS, Hooper DC (1985) The fluoroquinolones: structures, mechanisms of action and resistance, and spectra of activity in vitro. Antimicrob Agents Chemother 28:581–586
Mitnick CD, McGee B, Peloquin CA (2009) Tuberculosis pharmacotherapy: strategies to optimize patient care. Expert Opin Pharmacother 10:381–401
Blanchard SC, Fourmy D, Eason RG, Puglisi JD (1998) rRNA chemical groups required for aminoglycoside binding. Biochemistry 37:7716–7724
Forge A, Schacht J (2000) Aminoglycoside antibiotics. Audiol Neurootol 5:3–22
Peloquin C. Pharmacometrics and tuberculosis. In: Derendorf HSS (ed), Applied pharmacometrics: (in press)
Heifets L, Lindholm-Levy P (1989) Comparison of bactericidal activities of streptomycin, amikacin, kanamycin, and capreomycin against Mycobacterium avium and M. tuberculosis. Antimicrob Agents Chemother 33:1298–1301
Prosser GA, de Carvalho LP (2013) Reinterpreting the mechanism of inhibition of Mycobacterium tuberculosis D-alanine:D-alanine ligase by D-cycloserine. Biochemistry 52:7145–7149
Rengarajan J, Sassetti CM, Naroditskaya V, Sloutsky A, Bloom BR, Rubin EJ (2004) The folate pathway is a target for resistance to the drug para-aminosalicylic acid (PAS) in mycobacteria. Mol Microbiol 53:275–282
Youmans GP, Raleigh GW, Youmans AS (1947) The tuberculostatic action of para-aminosalicylic acid. J Bacteriol 54:409–416
Nuermberger E, Grosset J (2004) Pharmacokinetic and pharmacodynamic issues in the treatment of mycobacterial infections. Eur J Clin Microbiol Infect Dis 23:243–255
Drusano GL, Sgambati N, Eichas A, Brown D, Kulawy R, Louie A (2011) Effect of administration of moxifloxacin plus rifampin against Mycobacterium tuberculosis for 7 of 7 days versus 5 of 7 days in an in vitro pharmacodynamic system. MBio 2:e00108–e00111
Srivastava S, Pasipanodya JG, Meek C, Leff R, Gumbo T (2011) Multidrug-resistant tuberculosis not due to noncompliance but to between-patient pharmacokinetic variability. J Infect Dis 204:1951–1959
Dartois V (2011) Drug forgiveness and interpatient pharmacokinetic variability in tuberculosis. J Infect Dis 204:1827–1829
Pasipanodya J, Srivastava S, Gumbo T (2012) New susceptibility breakpoints and the regional variability of MIC distribution in Mycobacterium tuberculosis isolates. Antimicrob Agents Chemother 56:5428
Gumbo T (2010) New susceptibility breakpoints for first-line antituberculosis drugs based on antimicrobial pharmacokinetic/pharmacodynamic science and population pharmacokinetic variability. Antimicrob Agents Chemother 54:1484–1491
Heifets L (1991) Drug susceptibility in the chemotheraphy of mycobacterial infections. CRC, Boca Raton
Isenberg HD (1988) Antimicrobial susceptibility testing: a critical evaluation. J Antimicrob Chemother 22(Suppl A):73–86
Canetti G, Froman S, Grosset J et al (1963) Mycobacteria: laboratory methods for testing drug sensitivity and resistance. Bull World Health Organ 29:565–578
Heifets L (1996) Clinics in laboratory medicine, Clinical mycobacteriology. WB Saunders, Philadelphia, PA
Murray PR (ed) (2003) Manual of clinical microbiology, 8th edn. American Society of Microbiology, Washington DC
Campbell PJ, Morlock GP, Sikes RD et al (2011) Molecular detection of mutations associated with first- and second-line drug resistance compared with conventional drug susceptibility testing of Mycobacterium tuberculosis. Antimicrob Agents Chemother 55:2032–2041
Metchock B (2013) National Consultancy on proposed CDC guidance for the use of bedaquiline in the treatment of multidrug-resistant tuberculosis: laboratory perspective and review of CDC laboratory services. National Center for HIV/AIDS, Viral Hepatitis, STD & TB Prevention. Division of Tuberculosis Elimination (Power Point presentation)
Pasipanodya J, Gumbo T (2011) An oracle: antituberculosis pharmacokinetics-pharmacodynamics, clinical correlation, and clinical trial simulations to predict the future. Antimicrob Agents Chemother 55:24–34
Chigutsa E, Meredith S, Wiesner L et al (2012) Population pharmacokinetics and pharmacodynamics of ofloxacin in South African patients with multidrug-resistant tuberculosis. Antimicrob Agents Chemother 56:3857–3863
Zeitlinger MA, Derendorf H, Mouton JW et al (2011) Protein binding: do we ever learn? Antimicrob Agents Chemother 55:3067–3074
Craig WA, Kunin CM (1976) Significance of serum protein and tissue binding of antimicrobial agents. Annu Rev Med 27:287–300
Budha NR, Lee RE, Meibohm B (2008) Biopharmaceutics, pharmacokinetics and pharmacodynamics of antituberculosis drugs. Curr Med Chem 15:809–825
Mueller M, de la Pena A, Derendorf H (2004) Issues in pharmacokinetics and pharmacodynamics of anti-infective agents: kill curves versus MIC. Antimicrob Agents Chemother 48:369–377
Drusano GL (2004) Antimicrobial pharmacodynamics: critical interactions of ‘bug and drug’. Nat Rev Microbiol 2:289–300
Craig WA (1998) Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis 26:1–10, quiz 1-2
Gumbo T, Louie A, Deziel MR, Parsons LM, Salfinger M, Drusano GL (2004) Selection of a moxifloxacin dose that suppresses drug resistance in Mycobacterium tuberculosis, by use of an in vitro pharmacodynamic infection model and mathematical modeling. J Infect Dis 190:1642–1651
Gumbo T, Louie A, Deziel MR et al (2007) Concentration-dependent Mycobacterium tuberculosis killing and prevention of resistance by rifampin. Antimicrob Agents Chemother 51:3781–3788
Budha NR, Lee RB, Hurdle JG, Lee RE, Meibohm B (2009) A simple in vitro PK/PD model system to determine time-kill curves of drugs against Mycobacteria. Tuberculosis (Edinb) 89:378–385
Vaddady PK, Lee RE, Meibohm B (2010) In vitro pharmacokinetic/pharmacodynamic models in anti-infective drug development: focus on TB. Future Med Chem 2:1355–1369
Nuermberger E (2008) Using animal models to develop new treatments for tuberculosis. Semin Respir Crit Care Med 29:542–551
Dharmadhikari AS, Nardell EA (2008) What animal models teach humans about tuberculosis. Am J Respir Cell Mol Biol 39:503–508
Harper J, Skerry C, Davis SL et al (2012) Mouse model of necrotic tuberculosis granulomas develops hypoxic lesions. J Infect Dis 205:595–602
Davies GR, Nuermberger EL (2008) Pharmacokinetics and pharmacodynamics in the development of anti-tuberculosis drugs. Tuberculosis (Edinb) 88(Suppl 1):S65–S74
Dartois V (2014) The path of anti-tuberculosis drugs: from blood to lesions to mycobacterial cells. Nat Rev Microbiol 12:159–167
Rodvold KA, Yoo L, George JM (2011) Penetration of anti-infective agents into pulmonary epithelial lining fluid: focus on antifungal, antitubercular and miscellaneous anti-infective agents. Clin Pharmacokinet 50:689–704
Kempker RR, Rabin AS, Nikolaishvili K et al (2012) Additional drug resistance in Mycobacterium tuberculosis isolates from resected cavities among patients with multidrug-resistant or extensively drug-resistant pulmonary tuberculosis. Clin Infect Dis 54:e51–e54
Kaplan G, Post FA, Moreira AL et al (2003) Mycobacterium tuberculosis growth at the cavity surface: a microenvironment with failed immunity. Infect Immun 71:7099–7108
Mor N, Simon B, Mezo N, Heifets L (1995) Comparison of activities of rifapentine and rifampin against Mycobacterium tuberculosis residing in human macrophages. Antimicrob Agents Chemother 39:2073–2077
Burman WJ, Gallicano K, Peloquin C (2001) Comparative pharmacokinetics and pharmacodynamics of the rifamycin antibacterials. Clin Pharmacokinet 40:327–341
van Ingen J, Aarnoutse RE, Donald PR et al (2011) Why do we use 600 mg of rifampicin in tuberculosis treatment? Clin Infect Dis 52:E194–E199
Long MW, Snider DE Jr, Farer LS (1979) U.S. Public Health Service Cooperative trial of three rifampin-isoniazid regimens in treatment of pulmonary tuberculosis. Am Rev Respir Dis 119:879–894
Jindani A, Aber VR, Edwards EA, Mitchison DA (1980) The early bactericidal activity of drugs in patients with pulmonary tuberculosis. Am Rev Respir Dis 121:939–949
Jayaram R, Gaonkar S, Kaur P et al (2003) Pharmacokinetics-pharmacodynamics of rifampin in an aerosol infection model of tuberculosis. Antimicrob Agents Chemother 47:2118–2124
Blaschke TF, Skinner MH (1996) The clinical pharmacokinetics of rifabutin. Clin Infect Dis 22(Suppl 1):S15–S21, discussion S-2
McGregor MM, Olliaro P, Wolmarans L et al (1996) Efficacy and safety of rifabutin in the treatment of patients with newly diagnosed pulmonary tuberculosis. Am J Respir Crit Care Med 154:1462–1467
Li AP, Reith MK, Rasmussen A et al (1997) Primary human hepatocytes as a tool for the evaluation of structure-activity relationship in cytochrome P450 induction potential of xenobiotics: evaluation of rifampin, rifapentine and rifabutin. Chem Biol Interact 107:17–30
Rosenthal IM, Zhang M, Williams KN et al (2007) Daily dosing of rifapentine cures tuberculosis in three months or less in the murine model. PLoS Med 4:e344
Bemer-Melchior P, Bryskier A, Drugeon HB (2000) Comparison of the in vitro activities of rifapentine and rifampicin against Mycobacterium tuberculosis complex. J Antimicrob Chemother 46:571–576
Sirgel FA, Fourie PB, Donald PR et al (2005) The early bactericidal activities of rifampin and rifapentine in pulmonary tuberculosis. Am J Respir Crit Care Med 172:128–135
Tam CM, Chan SL, Kam KM, Goodall RL, Mitchison DA (2002) Rifapentine and isoniazid in the continuation phase of a 6-month regimen. Final report at 5 years: prognostic value of various measures. Int J Tuberc Lung Dis 6:3–10
Dorman SE, Goldberg S, Stout JE et al (2012) Substitution of rifapentine for rifampin during intensive phase treatment of pulmonary tuberculosis: study 29 of the tuberculosis trials consortium. J Infect Dis 206:1030–1040
Benator D, Bhattacharya M, Bozeman L et al (2002) Rifapentine and isoniazid once a week versus rifampicin and isoniazid twice a week for treatment of drug-susceptible pulmonary tuberculosis in HIV-negative patients: a randomised clinical trial. Lancet 360:528–534
Dutta NK, Illei PB, Peloquin CA et al (2012) Rifapentine is not more active than rifampin against chronic tuberculosis in guinea pigs. Antimicrob Agents Chemother 56:3726–3731
Savic RM, Lu Y, Bliven-Sizemore E et al (2014) Population pharmacokinetics of rifapentine and desacetyl rifapentine in healthy volunteers: nonlinearities in clearance and bioavailability. Antimicrob Agents Chemother 58(6):3035–3042
Mitchison DA (2012) Pharmacokinetic/pharmacodynamic parameters and the choice of high-dosage rifamycins. Int J Tuberc Lung Dis 16:1186–1189
Coates AR, Hu Y, Jindani A, Mitchison DA (2013) Contradictory results with high-dosage rifamycin in mice and humans. Antimicrob Agents Chemother 57:1103
Nuermberger EL, Rosenthal IM, Tasneen R et al (2013) Reply to “Contradictory results with high-dosage rifamycin in mice and humans”. Antimicrob Agents Chemother 57:1104–1105
Cade CE, Dlouhy AC, Medzihradszky KF, Salas-Castillo SP, Ghiladi RA (2010) Isoniazid-resistance conferring mutations in Mycobacterium tuberculosis KatG: catalase, peroxidase, and INH-NADH adduct formation activities. Protein Sci 19:458–474
Parsons LM, Salfinger M, Clobridge A et al (2005) Phenotypic and molecular characterization of Mycobacterium tuberculosis isolates resistant to both isoniazid and ethambutol. Antimicrob Agents Chemother 49:2218–2225
Barry CE 3rd, Slayden RA, Mdluli K (1998) Mechanisms of isoniazid resistance in Mycobacterium tuberculosis. Drug Resist Updat 1:128–134
Slayden RA, Barry CE 3rd (2000) The genetics and biochemistry of isoniazid resistance in mycobacterium tuberculosis. Microbes Infect 2:659–669
Banerjee A, Dubnau E, Quemard A et al (1994) inhA, a gene encoding a target for isoniazid and ethionamide in Mycobacterium tuberculosis. Science 263:227–230
Guo H, Seet Q, Denkin S, Parsons L, Zhang Y (2006) Molecular characterization of isoniazid-resistant clinical isolates of Mycobacterium tuberculosis from the USA. J Med Microbiol 55:1527–1531
Katiyar SK, Bihari S, Prakash S, Mamtani M, Kulkarni H (2008) A randomised controlled trial of high-dose isoniazid adjuvant therapy for multidrug-resistant tuberculosis. Int J Tuberc Lung Dis 12:139–145
Awaness AM, Mitchison DA (1973) Cumulative effects of pulsed exposures of mycobacterium tuberculosis to isoniazid. Tubercle 54(2):153–158
Gumbo T, Louie A, Liu W et al (2007) Isoniazid’s bactericidal activity ceases because of the emergence of resistance, not depletion of Mycobacterium tuberculosis in the log phase of growth. J Infect Dis 195:194–201
Mitchison DA, Jindani A, Davies GR, Sirgel F (2007) Isoniazid activity is terminated by bacterial persistence. J Infect Dis 195:1871–1872, author reply 2-3
Gumbo T, Louie A, Liu W et al (2007) Isoniazid bactericidal activity and resistance emergence: integrating pharmacodynamics and pharmacogenomics to predict efficacy in different ethnic populations. Antimicrob Agents Chemother 51:2329–2336
Weiner M, Burman W, Vernon A et al (2003) Low isoniazid concentrations and outcome of tuberculosis treatment with once-weekly isoniazid and rifapentine. Am J Respir Crit Care Med 167:1341–1347
Srivastava S, Sherman C, Meek C, Leff R, Gumbo T (2011) Pharmacokinetic mismatch does not lead to emergence of isoniazid- or rifampin-resistant Mycobacterium tuberculosis but to better antimicrobial effect: a new paradigm for antituberculosis drug scheduling. Antimicrob Agents Chemother 55:5085–5089
Somoskovi A, Dormandy J, Parsons LM et al (2007) Sequencing of the pncA gene in members of the Mycobacterium tuberculosis complex has important diagnostic applications: Identification of a species-specific pncA mutation in “Mycobacterium canettii” and the reliable and rapid predictor of pyrazinamide resistance. J Clin Microbiol 45:595–599
Shi W, Zhang X, Jiang X et al (2011) Pyrazinamide inhibits trans-translation in Mycobacterium tuberculosis. Science 333:1630–1632
Zimhony O, Vilcheze C, Arai M, Welch JT, Jacobs WR Jr (2007) Pyrazinoic acid and its n-propyl ester inhibit fatty acid synthase type I in replicating tubercle bacilli. Antimicrob Agents Chemother 51:752–754
Boshoff HI, Mizrahi V, Barry CE 3rd (2002) Effects of pyrazinamide on fatty acid synthesis by whole mycobacterial cells and purified fatty acid synthase I. J Bacteriol 184:2167–2172
Martin A, Takiff H, Vandamme P, Swings J, Palomino JC, Portaels F (2006) A new rapid and simple colorimetric method to detect pyrazinamide resistance in Mycobacterium tuberculosis using nicotinamide. J Antimicrob Chemother 58:327–331
Gumbo T, Dona CS, Meek C, Leff R (2009) Pharmacokinetics-pharmacodynamics of pyrazinamide in a novel in vitro model of tuberculosis for sterilizing effect: a paradigm for faster assessment of new antituberculosis drugs. Antimicrob Agents Chemother 53:3197–3204
Salfinger M, Heifets LB (1988) Determination of pyrazinamide MICs for mycobacterium-tuberculosis at different pHs by the radiometric method. Antimicrob Agents Chemother 32:1002–1004
Chicurel M, Garcia E, Goodsaid F (1988) Modulation of macrophage lysosomal PH by mycobacterium-tuberculosis-derived proteins. Infect Immun 56:479–83
Pasipanodya JG, Gumbo T (2010) Clinical and toxicodynamic evidence that high-dose pyrazinamide is not more hepatotoxic than the low doses currently used. Antimicrob Agents Chemother 54:2847–2854
Girling DJ (1982) Adverse effects of antituberculosis drugs. Drugs 23:56–74
Girling DJ (1978) The hepatic toxicity of antituberculosis regimens containing isoniazid, rifampicin and pyrazinamide. Tubercle 59:13–32
Srivastava S, Ayyagari A, Dhole TN, Nyati KK, Dwivedi SK (2009) emb nucleotide polymorphisms and the role of embB306 mutations in Mycobacterium tuberculosis resistance to ethambutol. Int J Med Microbiol 299:269–280
Ezer N, Benedetti A, Darvish-Zargar M, Menzies D (2013) Incidence of ethambutol-related visual impairment during treatment of active tuberculosis. Int J Tuberc Lung Dis 17:447–455
Fish DN, Chow AT (1997) The clinical pharmacokinetics of levofloxacin. Clin Pharmacokinet 32:101–119
Peloquin C, Alsultan A. Clinical pharmacology of the anti-tuberculosis drugs. In: Davies PDO BP, Gordon SB (eds) Clinical tuberculosis. 5th edn. (in press)
Peloquin CA, Hadad DJ, Molino LP et al (2008) Population pharmacokinetics of levofloxacin, gatifloxacin, and moxifloxacin in adults with pulmonary tuberculosis. Antimicrob Agents Chemother 52:852–857
(2008) Levofloxacin. Tuberculosis (Edinb) 88: 119-121
Canetti G (1965) Present aspects of bacterial resistance in tuberculosis. Am Rev Respir Dis 92:687–703
Morlock GP, Metchock B, Sikes D, Crawford JT, Cooksey RC (2003) ethA, inhA, and katG loci of ethionamide-resistant clinical Mycobacterium tuberculosis isolates. Antimicrob Agents Chemother 47:3799–3805
Chakraborty S, Gruber T, Barry CE 3rd, Boshoff HI, Rhee KY (2013) Para-aminosalicylic acid acts as an alternative substrate of folate metabolism in Mycobacterium tuberculosis. Science 339:88–91
Vega P, Sweetland A, Acha J et al (2004) Psychiatric issues in the management of patients with multidrug-resistant tuberculosis. Int J Tuberc Lung Dis 8:749–759
Bakhla AK, Gore PS, Srivastava SL (2013) Cycloserine induced mania. Ind Psychiatry J 22:69–70
Emmett MR, Mick SJ, Cler JA, Rao TS, Iyengar S, Wood PL (1991) Actions of D-cycloserine at the N-methyl-D-aspartate-associated glycine receptor site in vivo. Neuropharmacology 30:1167–1171
Matteelli A, Carvalho AC, Dooley KE, Kritski A (2010) TMC207: the first compound of a new class of potent anti-tuberculosis drugs. Future Microbiol 5:849–858
Hartkoorn RC, Uplekar S, Cole ST (2014) Cross-resistance between clofazimine and bedaquiline through upregulation of MmpL5 in Mycobacterium tuberculosis. Antimicrob Agents Chemother 58:2979–2981
Andries K, Verhasselt P, Guillemont J et al (2005) A diarylquinoline drug active on the ATP synthase of Mycobacterium tuberculosis. Science 307:223–227
Rouan MC, Lounis N, Gevers T et al (2012) Pharmacokinetics and pharmacodynamics of TMC207 and its N-desmethyl metabolite in a murine model of tuberculosis. Antimicrob Agents Chemother 56:1444–1451
(2013) Sirturo [package insert]. Janssen, Titusville, NJ
Peloquin CA (2002) Therapeutic drug monitoring in the treatment of tuberculosis. Drugs 62:2169–2183
Almeida Da Silva PE, Palomino JC (2011) Molecular basis and mechanisms of drug resistance in Mycobacterium tuberculosis: classical and new drugs. J Antimicrob Chemother 66:1417–1430
Blanchard JS (1996) Molecular mechanisms of drug resistance in Mycobacterium tuberculosis. Annu Rev Biochem 65:215–239
Caceres NE, Harris NB, Wellehan JF, Feng Z, Kapur V, Barletta RG (1997) Overexpression of the D-alanine racemase gene confers resistance to D-cycloserine in Mycobacterium smegmatis. J Bacteriol 179:5046–5055
Acknowledgements
Many thanks to Justin May for his technical expertise, and Natan Andres for graphical assistance.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media New York
About this protocol
Cite this protocol
Barth, A.B., Egelund, E.F., Peloquin, C.A. (2016). Pharmacokinetics and Pharmacodynamics of the Tuberculosis Drugs. In: Rotschafer, J., Andes, D., Rodvold, K. (eds) Antibiotic Pharmacodynamics. Methods in Pharmacology and Toxicology. Humana Press, New York, NY. https://doi.org/10.1007/978-1-4939-3323-5_16
Download citation
DOI: https://doi.org/10.1007/978-1-4939-3323-5_16
Published:
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-4939-3321-1
Online ISBN: 978-1-4939-3323-5
eBook Packages: Springer Protocols