
Abstract
Medullary thyroid cancer (MTC), an uncommon neoplasm stemming from the calcitonin-producing thyroid parafollicular C cells, accounts for approximately 5 % of cases of thyroid cancer. It exists in both sporadic and hereditary forms but is unique among all types of thyroid cancer because of the tight association of MTC with inherited tumor syndromes in approximately 20 % of patients. Activating mutations in the ret proto-oncogene account for the hereditary basis of MTC and contribute significantly to sporadic tumor development as well. These findings have a major impact on the diagnosis and therapy of MTC. The tumor was only first reported in 1959. MTC does not produce thyroglobulin and hence the latter protein does not serve as a tumor marker for residual or recurrent disease, but the neuropeptides, calcitonin, and carcinoembryonic antigen (CEA) are produced by C cell and do serve this function. The American Thyroid Association has published guidelines for the diagnosis and management of MTC along with commentary relevant to application of the guidelines for the care of adults and children.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Medullary thyroid cancer (MTC), an uncommon neoplasm stemming from the calcitonin-producing thyroid parafollicular C cells, accounts for approximately 5 % of cases of thyroid cancer. It exists in both sporadic and hereditary forms but is unique among all types of thyroid cancer because of the tight association of MTC with inherited tumor syndromes in approximately 20 % of patients. Activating mutations in the ret proto-oncogene account for the hereditary basis of MTC and contribute significantly to sporadic tumor development as well. These findings have a major impact on the diagnosis and therapy of MTC. The tumor was only first reported in 1959 [1]. MTC does not produce thyroglobulin and hence the latter protein does not serve as a tumor marker for residual or recurrent disease, but the neuropeptides, calcitonin, and carcinoembryonic antigen (CEA) are produced by C cell and do serve this function. The American Thyroid Association has published guidelines for the diagnosis and management of MTC [2] along with commentary relevant to application of the guidelines for the care of adults [3] and children [4].
Genetics
MTC is traditionally classified as sporadic versus hereditary. The three autosomal dominant hereditary MTC syndromes, collectively referred to as MEN 2, are described in Table 83.1. Multiple endocrine neoplasia type 2A (MEN2A) comprising MTC in 95 % of affected individuals, pheochromocytoma in approximately 50 %, and hyperparathyroidism in 10–15 % is the most common MEN2 syndrome. MEN2B comprises MTC (often with early onset), pheochromocytoma, ganglioneuromas of the oral mucosa and gastrointestinal tract, a characteristic elongated facies, a marfanoid body habitus, and no increase in hyperparathyroidism. The MTC in MEN 2B tends to be more aggressive and has presented earlier in life than MEN 2A tumors. FMTC (familial medullary thyroid cancer) is a term used to describe families with MTC but no other associated manifestations as are seen in MEN2A or MEN2B (see [5] for review). There is substantial overlap between ret mutations associated with MEN2A and FMTC. Two minor variants of MEN2A have been described: MEN2A associated with Hirschsprung’s disease (hypoplasia of intestinal myenteric plexus) and MEN2A associated with the skin disorder cutaneous lichen amyloidosis [6, 7].
The ret proto-oncogene encodes a receptor tyrosine kinase most closely related to the fibroblast growth factor receptor family. The physiologic role of ret is to activate growth-related signaling pathways in a limited range of neural crest-derived tissues that express the receptor. Downstream signaling pathways activated by ret include ras-MAPK and PI-3K/Akt [8]. Activating point mutations in ret lead to constitutive activity of the receptor, sometimes with altered substrate specificity. In the thyroid, these mutations lead to C-cell hyperplasia (CCH) and emergence of multiple foci of MTC that start as medullary microcarcinomata and eventually progress to larger tumors [9].
The range of ret codon mutations seen in the various forms of hereditary and sporadic MTC is listed in Table 83.1. Molecular screening for the ret proto-oncogene is more sensitive for the detection of subjects at risk for MTC than provocative testing, e.g., with calcium infusion. Ultimate clinical outcomes in patients at risk can be significantly enhanced after detection by screening and earlier treatment. From the standpoint of genetic testing, it is fortunate that >97 % of MEN2 families can be identified by analysis of six exons of the ret gene, including all of the mutant codons listed in Table 83.1 [5]. Exons 10 and 11 include mutation sites at codons 609, 611, 618, 620, 630, and 634 which are associated with both MEN2A and FMTC. Each of these codons encodes a cysteine residue in the extracellular domain of ret involved in the three-dimensional ligand binding pocket. Disruption of this pocket through mutation of any of these cysteine residues leads to ligand-independent dimerization and receptor activation. Exons 13–16 include intracellular domain mutation sites associated primarily with FMTC and in the case of exon 16 (codon 918), MEN 2B. The relatively limited variety of ret gene mutations within these six exons has facilitated genetic testing. Although a small percentage of MEN2 families have had no ret gene mutation detected, apparently all affected families studied to date exhibit genetic linkage to the ret gene locus [5].
Specific germline ret mutations carry important implications regarding the penetrance of MTC and associated lesions. For example, the most common germline ret mutation site, codon 634 (exon 11), accounts for approximately 60 % of all MEN2 families [9]. The majority of these families are classified as MEN2A rather than FMTC. Approximately 20 % of individuals with a codon 634 mutation develop hyperparathyroidism, whereas this manifestation is otherwise uncommon with other ret mutations [10]. Patients with codon 634 mutations have significantly earlier progression from CCH to MTC and earlier lymph node involvement than do patients with most other mutations associated with MEN2A and FMTC. A large European consortium study reported by Machens and colleagues offers detailed clinical penetrance data, analyzed according to individual mutations [9].
In MEN 2B, the great majority of patients exhibit a single mutation at codon 918 (methionine to threonine), resulting in an alteration of the substrate recognition pocket of the tyrosine kinase enzyme [11]. Unlike MEN2A, MEN2B germline mutations frequently arise de novo in the presenting individual, e.g., are not detectable in either parent. The de novo mutation is noted at a much higher frequency in the allele inherited from the patient’s father [12]. An alternate mutation at codon 883 in exon 15 has been found in a small number of MEN2B families [13].
When MTC patients with a negative family history are investigated with germline ret testing, approximately 3–6 % are found to harbor such mutations [14]. The ret mutations linked with cryptic heritable MTC tend to be disproportionately clustered in the intracellular domain (exons 13–15), associated with reduced MTC penetrance compared to the more classic familial patterns associated with extracellular mutations in exons 10–11. Based on this relatively high frequency of detection in family history-negative patients and the important “multiplier effect” of identifying other family members at risk, germline ret testing is currently recommended in all MTC patients, even in the absence of family history. Currently, a “complete” ret mutation test should include exons 10, 11, 13, 14, 15, and 16.
As many as 80 % of all MTCs are of the sporadic form [15] and acquired or somatic ret gene mutations (occurring in the tumor DNA only) also may be critical to pathogenesis in these tumors. Approximately 50 % of specimens contain ret mutations [16], most frequently the codon 918 mutation seen in MEN2B [17]. However, the discovery that mutation-positive and mutation-negative regions coexist in MTC tumors suggests that these mutations may not always be initiating or essential [18]. To further assess this tumor heterogeneity phenomenon, Schilling and colleagues examined multiple lymph nodes from sporadic MTC patients for somatic codon 918 mutations. Seventy-six percent of patients had concordant mutation results in all lymph nodes tested (43 % all positive, 33 % all negative) [19]. Patients with somatic codon 918 mutations had a significantly increased rate of metastases to the lung, bone, or liver and reduced overall survival. Greater understanding of the molecular genetics of MTC is leading to identification of molecular targets for new therapies [20]. Although the clinical utility of somatic ret mutation analysis is currently undefined, clinical trials are starting to correlate somatic ret mutation status with response to therapy.
Biochemistry
The characteristic secreted product of thyroid C cells and the most useful circulating marker for MTC is the polypeptide hormone calcitonin. The mature 32-amino acid polypeptide is synthesized as a large 135-amino acid precursor, which is processed by prohormone convertases in the C cell. Calcitonin is encoded by a multi-exon gene which produces two principal messenger RNA species. In addition to calcitonin itself, alternative splicing of the primary calcitonin transcript yields calcitonin gene-related peptide (CGRP). The resulting polypeptide hormones are unique and interact with distinct receptors. Calcitonin secretion predominates in normal thyroid C cells whereas CGRP predominates in neural tissue [21]. In MTC, abnormal RNA splicing permits an approximately equal ratio of calcitonin to CGRP, although CGRP measurement is not employed clinically. Whereas substantial elevations of calcitonin (>100 pg/ml) are usually diagnostic for MTC, modest elevations can be seen from extrathyroidal disorders including pulmonary inflammatory diseases, small-cell lung cancer, gastrinoma, carcinoid tumors, and renal failure [22]. An important thyroidal cause of calcitonin hypersecretion is C-cell hyperplasia (CCH). CCH may be genetic – as a precursor lesion in the three hereditary MTC disorders – or sporadic, either idiopathic or associated with such conditions as autoimmune thyroiditis, papillary thyroid cancer, or primary hyperparathyroidism [23]. At low levels of calcitonin excess, CCH can be very difficult to distinguish from microscopic MTC. In otherwise healthy individuals, extrathyroidal sources of calcitonin are usually undetectable in serum, using a specific, highly sensitive assay. Thus patients in remission following successful thyroidectomy characteristically have serum calcitonin values <1 pg/ml.
Current-generation calcitonin immunoradiometric assays (IRMA) with a detection limit of approximately 1 pg/ml are significantly more sensitive and specific than older calcitonin radioimmunoassays. Use of the calcitonin IRMA has coincided with reduced use of provocative testing with the calcitonin secretagogues calcium and pentagastrin in the USA, although several large European centers continue routine provocative testing. In normal adults given a pentagastrin infusion of 0.5 mcg/kg, normal peak values are less than 30 pg/ml. Pentagastrin is not available in the USA and will soon no longer be available in Europe as well.
In addition to calcitonin, MTC cells express biochemical markers typifying secretory cells of the diffuse neuroendocrine system. Polypeptide hormones produced by MTC cells include somatostatin [24], ACTH [25], gastrin-releasing peptide [26], substance P [27], and vasoactive intestinal peptide [28]. Other neuroendocrine markers include neuron specific enolase, NCAM, chromogranin A, prohormone convertases, synaptophysin, and the amine synthetic enzyme L-dopa decarboxylase [29]. Approximately 80 % of MTCs express the thyroid and lung-related foregut transcription factor TTF-1 [30]. In addition, many MTC tumors express two surface markers that have been exploited for diagnostic and therapeutic purposes, carcinoembryonic antigen (CEA) and somatostatin receptor.
Diagnosis
The clinical diagnosis of MTC can be challenging, due to a potential for misdiagnosis as a more common form of thyroid cancer or metastatic tumor from another site. Early accurate diagnosis is critical, to avoid the possibility of undiagnosed pheochromocytoma and to allow for an appropriate surgical approach. The important differences in surgical approach to MTC versus papillary and follicular cancer are detailed in Chap. 85.
Sporadic MTC: Clinical Presentation
Outside of the 20 % of cases where there is known heritable disease, the diagnosis of MTC most commonly begins with the palpation of an asymptomatic thyroid nodule. Because the majority of C cells are located in the upper lobes of the thyroid, most MTC will present in these locations. The nodule as well as any lymph nodes harboring tumor metastases may contain calcifications that will be identified on CT scan or ultrasound examination. The calcifications tend to be more dense than the speckling seen with papillary thyroid carcinoma. Sporadic cases present typically in the third to seventh decades of life with a nearly equal prevalence in males and females with a slight preponderance in women. In most instances, the history and physical exam do not offer any distinctive information compared to typical patients with thyroid nodules. A sufficiently detailed family history is warranted to detect the presence of thyroid cancer, pheochromocytoma, or hyperparathyroidism in first-degree relatives. Fine-needle aspiration cytology will allow a diagnosis of MTC in a thyroid nodule in perhaps 60–70 % of these tumors. Positive cytologic diagnosis may be aided by specific staining for calcitonin. Ultrasonography or CT scanning of the neck for detection of lymph nodes suspicious for metastasis should follow a positive FNA diagnosis. As many as half the patients will have lymph node metastases at presentation, and approximately 20 % of patients present with locally advanced disease with dysphagia, painful lymph node metastases, or recurrent laryngeal nerve invasion and about 5 % will have distant metastases. Uncommon individuals may present with a chief complaint related to paraneoplastic manifestation of MTC, such as flushing, secretory diarrhea, or symptoms of hypercortisolism and the ectopic ACTH syndrome. If prominent, such paraneoplastic manifestations usually indicate a significant tumor burden.
An increasing number of patients with sporadic MTC are now being identified with primary tumors that are incidentally discovered by imaging directed at another condition, such as carotid ultrasonography or staging of an unrelated tumor. Although the appearance of incidentally discovered MTC on ultrasound, CT or FDG-PET is not sufficiently distinctive to provide a radiologic diagnosis, MTC lesions (like PTC) may contain calcifications [31]. Even clinically unapparent sub-centimeter MTC lesions have a potential for metastasis and warrant appropriate surgical intervention. A MTC may also be incidentally discovered in the thyroid surgical specimen after thyroidectomy performed for another indication or for a nodule with a false-negative fine-needle aspiration cytology [32]. These circumstances of missed preoperative diagnosis are potentially hazardous insofar as they may miss coexisting hyperparathyroidism or pheochromocytoma the identification of which would have altered the surgical management.
All patients suspected of having MTC should have blood tested for calcitonin, CEA, calcium, and RET analysis. A controversial approach to MTC diagnosis is the routine use of calcitonin testing in patients with nodular goiter. Two large European studies found significantly elevated calcitonin levels and MTC in a combined 0.6 % of patients undergoing surgery for multinodular goiter. According to these authors, only one third of these MTC cases were diagnosed independently by fine-needle aspiration biopsy [33, 34]. A follow-up Italian study found a prevalence of 0.4 % of significant hypercalcitoninemia and MTC in over 10,000 patients undergoing thyroidectomy for nodular thyroid disease (basal calcitonin range 20–6,200 pg/ml). In this subset of patients, 65 % of individuals had an FNA result that was positive for MTC or other cancer [35]. The 2014 Guidelines of the American Thyroid Association [36] do not recommend either for or against calcitonin assay as part of the routine evaluation of a thyroid nodule or a nodular goiter, although some endocrinologists add this to standard assessment using FNA and TSH, especially if any clinical features suggest MTC. The 2014 guidelines do recommend ultrasonographic imaging of the neck for lymph node mapping although some workers have reported that preoperative levels of calcitonin may be more predictive of lymph node metastases than ultrasound findings [37]. The degree of calcitonin elevation correlates with tumor size and metastases for both familial and sporadic forms of MTC.
Sporadic MTC: Biopsy
The standard diagnostic procedure of choice for sporadic MTC is thyroid fine-needle aspiration biopsy for cytologic examination, either with direct palpation or ultrasound guidance. The sensitivity of thyroid cytopathology for MTC is theoretically equivalent to that in papillary cancer. In practice, the cytopathologist needs an adequate index of suspicion for atypical, cellular, colloid-poor specimens, in order to employ the diagnostic calcitonin immunostaining. In cases where there is clinical suspicion but insufficient cytologic material, a serum calcitonin level can help confirm or rule out the diagnosis. Occasionally specimens are misdiagnosed as atypical follicular neoplasms, or poorly differentiated/anaplastic cancers. The practice of referring patients directly to thyroidectomy without preceding biopsy is especially discouraged. Where lymph node enlargement is first identified rather than a thyroid nodule, fine-needle aspiration biopsy is favored over lymph node excisional biopsy, in order to preserve the lymph node compartment for subsequent comprehensive neck dissection.
Calcitonin Testing
Virtually all patients with clinically evident MTC have elevated basal levels of calcitonin. For clinically occult early MTC, basal calcitonin values may merge with the upper limit of the normal range, which is typically 8 pg/ml in men and 4 pg/ml in women. Although very rare, medullary microcarcinomas have been reported in patients with a normal basal calcitonin level [38]. At what calcitonin level is the presence of MTC confirmed and in what range is CCH or nonspecific elevation more likely? This question cannot be answered precisely owing to conflicting results in multiple studies [39]. A reasonable generalization is that basal calcitonin IRMA values between 10 and 100 pg (prior to thyroidectomy) include both early MTC and CCH, with an overall prevalence of MTC in the 15–30 % range [39]. Above 100 pg/ml, the prevalence of MTC rises substantially although rare CCH cases can still be observed in this range.
Preoperative calcitonin levels correlate generally with tumor size. In a large French series, a calcitonin level above 1,000 pg/ml corresponded to a median tumor diameter of 2.5 cm, whereas calcitonin levels below 1,000 pg/ml corresponded to a median tumor size of 0.7 cm and levels below 100 pg/ml to 0.3 cm. A calcitonin level greater than 1,000 pg/ml was associated with a 10 % risk of distant metastases versus 3 % for levels less than 1,000 [40]. Similarly, the degree of preoperative calcitonin elevation is an important predictor of the chances of normalizing the serum calcitonin with surgery. The chance of postop normalization falls from 97 % (if the preop level is less than 50 pg/ml) to 42 % (preop greater than 50 pg/ml) and 8 % (preop greater than 4,000 pg/ml) [40].
Sporadic MTC: Other Preop Testing
In our institutions, individuals with newly diagnosed MTC, even in the absence of a family history of MTC, are evaluated with ret proto-oncogene DNA testing, 24 h urine metanephrines or plasma fractionated metanephrines, serum calcium, and CEA, in addition to calcitonin. The objective is to detect those cases of MTC that may represent MEN2 and have associated hyperparathyroidism or pheochromocytoma.
Sporadic MTC: Preoperative Imaging
The preoperative imaging workup varies from patient to patient. Differences in the application of optimal imaging modalities for sporadic and hereditary MTC, including PET-CT, have been reviewed recently [41]. At a minimum, a high-quality thyroid and neck ultrasound is useful to detect multifocal thyroid involvement and metastasis to central compartment and jugular chain nodes. False-negative neck ultrasound has been reported in approximately one third of patients with MTC [37]. The absence of abnormal lymph nodes on palpation or ultrasound does not obviate the need for lymph nodal dissection however. Lymph node prevalence in sporadic MTC can be estimated from the surgical-pathological data analyzed by Scollo et al. Both central compartment and ipsilateral jugular chain node involvement occurred in more than 50 % of patients, whereas contralateral jugular chain nodes had a 25–30 % prevalence [42]. Even in the absence of central compartment lymph node involvement, positive node metastases may be found in the lateral neck in 10 % of patients and will be found with virtually 100 % of patients when there is involvement of four or more central compartment nodes [43]. Chapter 85 provides a detailed description of operative management for MTC. The ATA Guidelines [2] recommend total thyroidectomy with both central and lateral compartment dissection in patients with ultrasonographic evidence of lateral regional node involvement. Dralle and Machens [44] have urged caution for lateral neck dissection to balance potential benefit vs. risk of nerve damage. Less aggressive surgery is warranted when distant metastases are present. In our institutions, the choice of additional imaging modalities is guided by the degree of calcitonin elevation. Very high levels may indicate metastatic disease with the most frequent sites being to the lungs, liver, and bones. Neck and chest CT with contrast and dual-phase (early and late) contrast scan of the abdomen are most commonly employed in preoperative staging. Postoperatively, a neck ultrasound should be obtained when calcitonin levels are detectable but <150 pg/ml [2], and CT or MRI is recommended when calcitonin is >150 pg/ml or when calcitonin levels are noted to be rising. MRI may be most useful for bone metastases and FDG-PET may be more useful than CT for lower neck or mediastinal metastases [45]. FDG-PET has been found to be less sensitive than other imaging modalities [46] especially when serum calcitonin levels are less 500 pg/ml [47].
Diagnosis of Hereditary MTC
Since the late 1990s, a consensus has emerged that ret proto-oncogene testing, rather than calcitonin provocative testing, is the preferred method for diagnosis of hereditary MEN2. The sensitivity of ret testing is excellent, currently estimated at approximately 98 % for known families [5]. The test is widely available through commercial laboratories. Efficient family testing focuses on identifying the mutation in a known affected individual and then proceeding systematically through first-degree relatives. The primary goal of this testing is to identify presymptomatic young individuals at risk for MTC and allow for appropriate prophylactic thyroidectomy. Additional goals are identification of subjects with existing MTC needing treatment, as well as subjects at risk for pheochromocytoma and hyperparathyroidism. Prophylactic thyroidectomy, at the stage of CCH or microscopic MTC, is associated with marked improvements in morbidity and mortality, compared with historical patterns of tumor detection later in life [5]. Earlier stage disease will be found with prophylactic thyroidectomy resulting in less need for subsequent aggressive node dissections and in higher cure rates [48]. Indeed, most individuals with FMTC and MEN2A have normal life expectancy after undergoing childhood prophylactic thyroidectomy.
The optimal timing of genetic testing (and prophylactic surgery) is somewhat controversial. These decisions are predicated on data for the earliest onset of MTC and nodal metastases for a particular ret mutation site. The most complete data currently available, from Machens et al., indicate that for the most common mutation at codon 634, microscopic MTC can occur as early as age 15 months and lymph nodal metastases can begin as early as age 6, although ages 14–20 are more common [9]. For other extracellular codons including 609, 611, 618, and 620, no patients have been reported to develop MTC prior to age 6 [9]. Smaller numbers of patients have been studied for the intracellular mutant codons 768, 790, 791,804, and 891, associated predominantly with FMTC. With the exception of patients with codon 804 mutations that may variably develop cancer at an earlier age, few patients with these intracellular codon lesions have developed MTC prior to age 20. For individuals with a 918 mutation and the MEN2B phenotype, metastatic MTC has been reported in the first year of life. Thyroidectomy should be considered as early as the first month of life in those infants with high-risk mutations in 883, 918, and 922 [45].
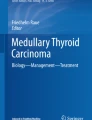
Based on data for MTC onset and metastasis, an international consensus panel has recommended prophylactic thyroidectomy by age 5 for subjects harboring mutations in codon 611, 618, 620, or 634 [45, 49]. For codons 609, 768, 790, 791, 804, and 891, no consensus was reached, with either a range of 5–10 years chosen [5] or ongoing close monitoring with serum calcitonin and CEA levels [45]. Because of frequent de novo mutations, patients with MEN2B are often first suspected not on the basis of family history but because of a characteristic elongated facies and oral ganglioneuromas involving the lips and tongue (see Fig. 83.1). DNA diagnosis then provides confirmation. Clearly identification of MEN2B should be as early as possible, with surgical cure increasingly unlikely after the first 5 years of life.

Photograph of a patient with MEN2B showing the typical mucosal neuromas associated with a marfanoid habitus. a Lips; b tongue; c hyperextensibility of the hands
Hereditary MTC: Preoperative Studies
All patients diagnosed with hereditary MEN 2 should have an assessment of catecholamine secretion prior to surgical procedures, as well as a basal calcitonin determination, CEA, and serum calcium. For young patients undergoing prophylactic thyroidectomy, no imaging studies are usually employed. Patients in their teens and beyond or patients with significant calcitonin elevations are considered for imaging studies, as described above for sporadic disease. The choice of operation, particularly the extent of lymph nodal dissection and prophylactic parathyroid resection, depends on a knowledge of natural history of inherited MTC and the impact of different ret mutations. In general, this surgery should be performed in a specialized center by surgeons familiar with these issues, as discussed in Chap. 85.
Tumor Progression and Complications
Of typical patients with a palpable sporadic MTC who have undergone thyroidectomy and neck exploration, the majority will have persistent elevations of calcitonin [50]. Those patients who prove to be node negative with appropriate comprehensive lymph nodal exploration have a 95 % chance of an undetectable basal calcitonin level [42]. On the other hand, the presence of lymphadenopathy reduces the likelihood of calcitonin normalization to 32 % [42]. Even patients considered to have undergone complete resection at the time of surgery have a strong likelihood of persistent hypercalcitoninemia. In the absence of overt adenopathy or extensive distant metastases, the clinical course is usually characterized by slow disease progression. Patients with minimal calcitonin elevations and no radiologically detectable metastasis after primary surgery have an 86 % 10-year survival rate and relatively little tumor-associated morbidity [51]. Similarly a Memorial Sloan-Kettering series reported 94 % 5-year survival in patients with nodal disease alone versus 41 % in patients with Stage IV disease [52] (see Table 83.2). Thus, Stage III or IV disease is associated with a significant reduction in disease-specific survival.
In addition to regional lymphadenopathy, the most common metastatic sites include lung and hilar or mediastinal lymph nodes, liver and abdominal lymph nodes, and bone. Lung and liver metastases occur in a diffuse, hematogenous pattern, usually with slow growth. Fortunately, modest metastatic burdens in the lung, and to a lesser extent liver, can be compatible with lengthy survival. Standard imaging modalities including contrast CT, MRI, and PET are quite insensitive for detecting early liver metastases [53]. The inclusion of an arterial phase-contrast protocol with MRI apparently improves sensitivity for liver metastasis detection [45]. Laparoscopic liver visualization and biopsy or hepatic venous sampling are more invasive approaches to this diagnosis. Occasionally, liver metastases can become bulky and painful. Extensive liver metastases are also frequently associated with diarrhea. Although liver resection is not routinely advocated for MTC liver metastases because of the multifocality of the process, surgical debulking of symptomatic masses can provide useful palliation [54].
The most frequent serious complications observed in advanced MTC relate to local tumor invasion into the thyroid bed, trachea, carotid sheath, and brachial plexus or progressive metastasis in the upper mediastinum, lung, or pericardium. Recurrent laryngeal nerve paresis, tracheal and esophageal invasion, superior vena cava syndrome, aspiration-related and post-obstructive pneumonia, and hemoptysis all may be seen in patients with advanced disease and contribute to disease mortality. Another significant cause of morbidity is lytic bone metastasis. Although MTC lesions are not generally considered radiation sensitive, external beam radiation is a useful palliative measure for painful bone lesions or lytic metastases in weight-bearing sites.
The principal paraneoplastic humoral complications of MTC are flushing, diarrhea, and the ectopic ACTH syndrome. The etiology of flushing in MTC patients is still a cause of some debate. One likely mediator is CGRP, a potent vasodilator capable of inducing prolonged cutaneous erythema with intradermal administration [55]. Symptomatic flushing sometimes can be improved by subcutaneous octreotide injection [56]. Unfortunately, octreotide has little efficacy in MTC-associated diarrhea; some patients paradoxically worsen.
Like flushing, the pathophysiology of diarrhea in MTC requires further clarification. The small minority of MEN2A patients with Hirschsprung’s disease, as well as MEN2B patients, have well-characterized abnormalities in enteric nerve development with resulting obstruction and megacolon [57]. In contrast, there are no reproducible structural abnormalities in most MTC patients with diarrhea. Functional studies have shown no consistent evidence for either malabsorption or a secretory abnormality in the small intestine. Instead, patients exhibit colonic hypermotility and a decreased ability to absorb water [58]. Intravenous CGRP can increase colonic output of water and electrolytes [59], although the relative importance of other mediators including vasoactive intestinal peptide, histamine, and prostaglandins remains unclear. ATA Guidelines recommend use of antimotility agents such as loperamide and diphenoxylate to lengthen colonic transit time and provide symptomatic relief [2]. Calcitonin excess, per se, is not associated with any clinically significant changes in bone or mineral metabolism.
Prognosis
Medullary thyroid cancer occupies an intermediate position among thyroid cancer histologic types with respect to biologic behavior and long-term prognosis. Although there is intrinsic variability in patients’ clinical course, prognostic factors apparent at the time of diagnosis and initial surgery have important utility in predicting long-term outcomes of MTC. An accurate understanding of the influence of prognostic factors in both sporadic and hereditary contexts is essential for selecting appropriate levels of therapeutic intervention.
Sporadic MTC
The most comprehensive reviews of prognostic factors in MTC to date are based on nationwide cancer surveillance in Sweden, with follow-up to 30 years [60, 61]. These studies have revealed several important predictors of survival. Among all sporadic MTC patients, relative survival (the ratio between observed and expected survival) was 63 % at 10 years and 50 % at 20 years. The most important prognostic factor was initial clinical stage (see Table 83.2). Stage III (nodal disease) and Stage IV (distant metastases) were associated with relative hazards of 3.3 and 4.1 compared to patients with no nodal or distant disease. Similarly, a French study including 79 patients with Stage IV disease and a US study found a 5-year survival of 35–40 % [52, 56]. Initial clinical stage remains highly predictive of future mortality even up to 20 years after diagnosis [61]. Other important negative prognostic indicators include tumor size >3 cm, capsular invasion, weak or heterogeneous calcitonin staining, male gender, and older age. By contrast, patients with a tumor measuring <1 cm without known metastases do not differ in survival from the general population [61, 62]. The impact of new molecular markers on MTC prognostic assessment is still unclear. Although somatic mutations in ret at codon 918 appear to be associated with an adverse prognosis, the impact in a large multivariate analysis is unknown. Patients with codons 918, 883, and 992 mutations will have the highest likelihood of persistent residual disease after initial therapy and the highest mortality rates [63]. It is likely, though unproven, that different ret gene mutations will impact on response to tyrosine kinase inhibitors and other experimental therapies.
Hereditary MTC
The significant improvement in outcome seen over the last three decades for patients with heritable MTC can be attributed to the success of presymptomatic screening programs, first with calcitonin secretagogues and more recently with genetic testing. Survival rates of MEN 2A subjects identified in early childhood are projected to be indistinguishable from the general population [61, 62]. An unsettled question is whether the MTC in MEN2A behaves intrinsically less aggressively than sporadic tumors when matched for clinical stage. Swedish MTC registry data suggest statistically similar outcomes for non-screened MEN2A and sporadic patients [62]. At either extremes of the hereditary MTC spectrum, FMTC associated with some intracellular codons appears significantly less aggressive than classic MEN2A in terms of disease latency and survival [64]. MEN2B is generally more aggressive [5, 9].
The age-specific likelihood that a MEN2A gene carrier would present with detectable calcitonin hypersecretion or with symptomatic MTC has been studied by Ponder and colleagues [65]. Approximately 65 % of obligate gene carriers exhibit calcitonin hypersecretion at age 20 years. By age 35, fully 95 % of gene carriers have a positive provocative test. In contrast, the likelihood of a clinical presentation with MTC is only 25 % at age 35 and only approximately 60 % at age 70 [65]. These data cannot be extrapolated to less penetrant hereditary MTC associated with intracellular domain mutations however.
Clinical Surveillance
Goals of clinical surveillance in MTC are to detect recurrences in patients in surgical remission and especially to prevent morbidity from cancer progression in patients with persistent disease. It is reasonable to restage patients prior to performing neck reoperation, for the purpose of excluding Stage IV, inoperable disease. An emerging aim is to select patients who could potentially benefit from clinical trials of systemic therapies for MTC. The intensity of clinical surveillance depends on the risk of death and morbidity and the likelihood of a beneficial intervention.
For patients with modest calcitonin elevations after primary surgery, follow-up testing utilizes a combination of biochemical tumor markers and radiologic studies to screen for disease progression. In one commonly used scheme, serum calcitonin, CEA, and thyroid function tests are obtained 6 weeks after surgery and then at approximately 6-month intervals. The timing of the postoperative calcitonin nadir may be variable [66] and calcitonin levels may vary considerably from measurement to measurement. This variability likely stems from variable secretion by tumors rather than assay variability. In contrast to calcitonin, CEA levels exhibit less inconsistency and, if elevated at baseline, are useful to detect disease progression. Measurements of a combination of calcitonin and CEA every 6 months, with repeated testing for outlying results, will allow estimation of doubling times and identify most patients with progressive disease [67]. A particularly worrisome pattern over time is a flat calcitonin level coupled with rapid doubling in CEA. Overall, the most typical doubling time for calcitonin and CEA is approximately 18 months, reflecting the generally indolent course of this disease. The ATA Guidelines recommend initiation of treatment, perhaps in a clinical trial, when the doubling time is less than 2 years [2]. Certainly, imaging studies such as FDG-PET/CT should be considered to attempt to identify the source of the calcitonin or CEA in order to rule in or out other therapeutic interventions such as surgery, radiation, or local ablative techniques.
Of the available imaging modalities, high-quality neck ultrasound appears to have greatest sensitivity for lymphadenopathy in the central compartment and jugular chains [68]. Because of variability in imaging protocols and interpretation, high-quality neck ultrasound imaging is not available in all centers. Distinct advantages of ultrasound compared to CT/MRI are precise lesional measurements, assessment of the presence of a fatty hilum (characteristic of reactive nodes), and especially the ability to perform ultrasound-guided FNA of lymph nodes if needed. Neck CT and MRI are complementary to ultrasound by providing wider coverage in the neck and more detailed anatomic localization of lymph nodes, once they are detected. Patients with small elevations of calcitonin (<50 pg/ml) frequently do not have disease detectable by imaging. Patients with more significant calcitonin elevations (>500 pg/ml) are frequently followed with periodic whole-body imaging in addition to ultrasound, including either CT (neck, chest, dual-phase abdomen) or FDG-PET [47].
In spite of the wide range of imaging options now available, a vexing problem for clinicians and patients is the issue of occult residual MTC, i.e., elevated calcitonin and negative imaging studies. At low levels of calcitonin, this problem generally reflects low disease burden, below threshold sensitivities of even sensitive techniques such as neck ultrasound. Even with higher levels of calcitonin and ostensibly greater disease burdens, patients may undergo frustrating and expensive rounds of unproductive imaging. The issue of which whole-body modality is best for imaging occult disease remains unsettled. There is general consensus that octreotide, DMSA (dimercaptosuccinic acid), and 131-MIBG scintigraphy have lower overall sensitivity, whereas CT and FDG-PET have greater sensitivity overall [69]. The choice between CT and FDG-PET is not clear-cut, with advantages at different metastatic sites for both modalities, as discussed in Chap. 87. In patients in whom baseline calcitonin levels are undetectable but levels rise minimally after stimulation, identification of the source of the calcitonin is unlikely and such follow-up retesting is not recommended [2].
Therapeutic Choice in Residual MTC
Faced with a rising calcitonin level and/or metastatic lesions seen on imaging studies, patients and clinicians can choose between a course of watchful waiting or intervention with surgery, radiotherapy, or systemic therapy. Specific surgical, radiation, and chemotherapeutic approaches to MTC are discussed elsewhere in this text. The decision to undertake these interventions presupposes an understanding of MTC natural history and appropriate use of biochemical and imaging data, as well as an effective treatment option.
Patients with only biochemical evidence of persistent MTC and negative imaging studies are frequently managed expectantly. In patients with mild hypercalcitoninemia and negative imaging, an excellent overall prognosis supports such a conservative approach [51, 52]. A more aggressive approach with neck reoperation with a potential curative intent seems justified in some patients who have not had recommended primary surgery, as described in Chap. 85. On the other hand, the low to moderate success rates in normalizing the calcitonin level following repeat lymph nodal dissection suggest that this approach be used highly selectively [70–72].
Radioactive iodine is ineffective for patients with MTC as are somatostatin analogues. Cytotoxic chemotherapy is not routinely recommended [2] but may be attempted for recurrent metastatic disease in patients who are ineligible for clinical trials with targeted molecular therapy. Locoregional recurrence is frequently managed surgically. In the presence of Stage IV disease, especially with distant progression, the goals of such neck surgery become focused on symptom palliation and to a lesser extent on the prevention of anticipated complications. The importance of locoregional control, even in patients with Stage IV disease, has been emphasized [73]. The limited potential role of adjuvant neck radiation following surgery is discussed in Chap. 88 and has been reviewed [74]. ATA Guidelines [2] note that radiation is not a substitute for surgery for patients with neck involvement and recommend consideration of postoperative radiation for incompletely resected disease in the neck or in bones, for brain metastases not amenable to surgical excision, and for painful bone metastases. There was no recommendation either for or against the use of bisphosphonates in patients with bone metastases.
Patients with distant metastases should be considered as potential candidates for investigational systemic therapy or clinical trials, as no currently available regimen produces frequent, durable responses. The decision to undertake such a therapy rests on a variety of factors including the rate of metastatic progression on interval scanning, study availability, comorbidities, and patient preference. At this writing, a variety of experimental therapies have been under active investigation for MTC including sunitinib, sorafenib, motesanib, axitinib, cabozantinib, and vandetanib [75]. These therapies are targeted at ret kinase inhibition, additional cellular kinases, tumor angiogenesis, and protein chaperone function. One of the more promising tyrosine kinase inhibitors is vandetanib [76–80] which has been effective in stabilizing disease although worrisome side effects like QTc prolongation are a concern. Conceivably, combinations of targeted therapies or targeted plus cytotoxic therapies will prove most effective.
References
Hazard JB, Crile Jr G. Medullary (solid) carcinoma of the thyroid: a clinic-pathologic entity. J Clin Endocrinol Metab. 1959;19:152–61.
Wells SA, et al., Revised American Thyroid Association Guidelines for the Management of Medullary Thyroid Carcinoma prepared by the American Thyroid Association Guidelines Task Force on Medullary Thyroid Carcinoma. Thyroid. 2015; 25: 567–610.
Ball DW. American Thyroid Association guidelines for management of medullary thyroid cancer: an adult endocrinology perspective. Thyroid. 2009;19:547–50.
Waguespack SG, Rich TA, Perrier ND, Jimenez C, Cote GJ. Management of medullary thyroid carcinoma and MEN2 syndromes in childhood. Nature Reviews Endocrinology. 2011;7(10):596–607.
Brandi ML, Gagel RF, Angeli A, Bilezikian JP, et al. Guidelines for diagnosis and therapy of MEN type 1 and type 2. J Clin Endocrinol Metab. 2001;86:5658–71.
Frilling A, Becker H, Roehr H-D. Unusual features of multiple endocrine neoplasia. Henry Ford Hosp Med J. 1992;40:233–5.
Gagel RF, Levy ML, Donovan DT, et al. Multiple endocrine neoplasia type 2a associated with cutaneous lichen amyloidosis. Ann Intern Med. 1989;111:802–6.
De Vita G, Melillo RM, Carlomagno F, et al. Tyrosine 1062 of RET-MEN2A mediates activation of Akt (protein kinase B) and mitogen-activated protein kinase pathways leading to PC12 cell survival. Cancer Res. 2000;60:3727–31.
Machens A, Niccoli-Sire P, Hoegel J, et al. Early malignant progression of hereditary medullary thyroid cancer. N Engl J Med. 2003;349:1517–25.
Schuffenecker I, Virally-Monod M, Brohet R, et al. Risk and penetrance of primary hyperparathyroidism in multiple endocrine neoplasia type 2A families with mutations at codon 634 of the RET proto-oncogene. J Clin Endocrinol Metab. 1998;83:487–91.
Santoro M, Carlomagno F, Romano A, Bottaro DP, et al. Activation of RET as a dominant transforming gene by germline mutations of MEN2A and MEN2B. Science. 1995;267:381–3.
Carlson KM, Bracamontes J, Jackson CE, Clark R, et al. Parent-of-origin effects in multiple endocrine neoplasia type 2B. Am J Hum Genet. 1994;5:1076–82.
Gimm O, Marsh DJ, Andrew SD, Frilling A, et al. Germline dinucleotide mutation in codon 883 of the RET proto-oncogene in multiple endocrine neoplasia type 2B without codon 918 mutation. J Clin Endocrinol Metab. 1997;82:3902–4.
Wohllk N, Cote GJ, Bugalho MM, et al. Relevance of RET proto-oncogene mutations in sporadic medullary thyroid carcinoma. J Clin Endocrinol Metab. 1996;81:3740–5.
Pitman MB, Oertel YC, Geisinger KR. Medullary thyroid carcinoma. In: Ali SZ, Cibas ES, editors. The Bethesda system for reporting thyroid cytopathology. 1st ed. New York: Springer; 2010. p. 117–28.
Elisei R, Cosci B, Romei C, et al. Prognostic significance of somatic RET oncogene mutations in sporadic medullary thyroid cancer: a 10-year follow-up study. J Clin Endocrinol Metab. 2008;93:682–7.
Blaugrund JE, Johns Jr MM, Eby YJ, Ball DW, et al. RET proto-oncogene mutations in inherited and sporadic medullary thyroid cancer. Hum Mol Genet. 1994;3:1895–7.
Eng C, Mulligan LM, Healey CS, et al. Heterogeneous mutation of the RET proto-oncogene in subpopulations of medullary thyroid carcinoma. Cancer Res. 1996;56:2167–70.
Schilling T, Burck J, Sinn HP, Clemens A, et al. Prognostic value of codon 918 (ATG-->ACG) RET proto-oncogene mutations in sporadic medullary thyroid carcinoma. Int J Cancer. 2001;95:62–6.
Cerrato A, De Falco V, Santoro M. Molecular genetics of medullary thyroid carcinoma: the quest for novel therapeutic agents. J Mol Endocrinol. 2009;43:143–55.
Amara SG, Jonas V, Rosenfeld MG, Ong ES, Evans RM. Alternative RNA processing in calcitonin gene expression generates mRNAs encoding different polypeptide products. Nature. 1982;298:240–4.
Becker KL, Nash D, Silva OL, et al. Increased serum and urinary calcitonin in patients with pulmonary disease. Chest. 1981;79:211–6.
Perry A, Molberg K, Albores-Saavedra J. Physiologic versus neoplastic C-cell hyperplasia of the thyroid: separation of distinct histologic and biologic entities. Cancer. 1996;77:750–6.
Roos BA, Lindall AW, Ells J, et al. Increased plasma and tumor somatostatin-like immuno reactivity in medullary thyroid carcinoma and small cell lung cancer. J Clin Endocrinol Metab. 1981;52:187–94.
Melvin KE, Tashjian Jr AH, Cassidy CE, Givens JR. Cushing’s syndrome caused by ACTH and calcitonin-secreting medullary carcinoma of the thyroid. Metabolism. 1970;19:831–8.
Kameya T, Bessho T, Tsumuraya M, et al. Production of gastrin-releasing peptide in medullary carcinoma of the thyroid. Virchows Arch [A]. 1983;401:99–107.
Skrabanek P, Cannon D, Dempsey J, et al. Substance P in medullary carcinoma of the thyroid. Experientia. 1979;35:1259–60.
Said SI. Evidence for secretion of vasoactive intestinal peptide by tumours of pancreas, adrenal medulla, thyroid and lung. Clin Endocrinol (Oxf). 1976;5(Suppl):201S–4.
Baylin SB, Mendelsohn G. Medullary thyroid carcinoma: a model for the study of human tumor progression and cell heterogeneity. In: Owens Jr AH, Coffey DS, Baylin SB, editors. Tumor cell heterogeneity, origins and implications. New York: Academic; 1982. p. 12.
Katoh R, Miyagi E, Nakamura N, Li X, et al. Expression of thyroid transcription factor-1 (TTF-1) in human C cells and medullary thyroid carcinomas. Hum Pathol. 2000;31:386–93.
McDonnell 3rd CH, Fishman EK, Zerhouni EA. CT demonstration of calcified liver metastases in medullary thyroid carcinoma. J Comput Assist Tomogr. 1986;10:976–8.
Ahmed SR, Ball DW. Incidentally discovered medullary thyroid cancer: diagnostic strategies and treatment. J Clin Endocrinol Metab. 2011;96:1237–45.
Pacini F, Fontanelli M, Fugazzola L, et al. Routine measurement of serum calcitonin in nodular thyroid diseases allows the preoperative diagnosis of unsuspected sporadic medullary thyroid carcinoma. J Clin Endocrinol Metab. 1994;78:826–9.
Rieu M, Lame MC, Richard A, et al. Prevalence of sporadic medullary thyroid carcinoma: the importance of routine measurement of serum calcitonin in the diagnostic evaluation of thyroid nodules. Clin Endocrinol (Oxf). 1995;42:453–60.
Elisei R, Bottici V, Luchetti F, Di Coscio G, et al. Impact of routine measurement of serum calcitonin on the diagnosis and outcome of medullary thyroid cancer: experience in 10,864 patients with nodular thyroid disorders. J Clin Endocrinol Metab. 2004;89:163–8.
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1–133.
Machens A, Dralle H. Biomarker-based risk stratification for previously untreated medullary thyroid cancer. J Clin Endocrinol Metab. 2010;95:2655–63.
Niccoli P, Wion-Barbot N, Caron P, Henry JF, et al. Interest of routine measurement of serum calcitonin: study in a large series of thyroidectomized patients. J Clin Endocrinol Metab. 1997;82:338–41.
Hodak SP, Burman KD. The calcitonin conundrum – is it time for routine measurement of serum calcitonin in patients with thyroid nodules? J Clin Endocrinol Metab. 2004;89:511–4.
Cohen R, Campos JM, Salaun C, Heshmati HM, et al. Preoperative calcitonin levels are predictive of tumor size and postoperative calcitonin normalization in medullary thyroid carcinoma. J Clin Endocrinol Metab. 2000;85:919–22.
Ganeshan D, Paulson E, Duran C, Cabanillas ME, Busaidy NL, Charnsangavej C. Current update on medullary thyroid carcinoma. AJR. 2013;201:W867–76.
Scollo C, Baudin E, Travagli JP, Caillou B, et al. Rationale for central and bilateral lymph node dissection in sporadic and hereditary medullary thyroid cancer. J Clin Endocrinol Metab. 2003;88:2070–5.
Machens A, Hauptmann S, Dralle H. Prediction of lateral lymph node metastases in medullary thyroid cancer. Br J Surg. 2008;95:586–91.
Dralle H, Machens A. Surgical management of the lateral neck compartment for metastatic thyroid cancer. Curr Opin Oncol. 2013;25:20–6.
Roman S, Mehta P, Sosa JA. Medullary thyroid cancer: early detection and novel treatments. Curr Opin Oncol. 2008;21:5–10.
Giraudet AL, Vanel D, Leboulleux S, Auperin A, Dromain C, et al. Imaging medullary thyroid carcinoma with persistent elevated calcitonin levels. J Clin Endocrinol Metab. 2007;92:4185–90.
Ong SC, Schoder H, Patel SG, Tabangay-Lim IM, Doddamane I, et al. Diagnostic accuracy of 18F-FDG-PET in restaging patients with medullary thyroid carcinoma and elevated calcitonin levels. J Nucl Med. 2007;48:501–7.
Castellone MD, Santoro M. Dysregulated RET signaling in thyroid cancer. Endocrinol Metab Clin N Am. 2008;37:363–74.
Zenaty D, Aigrain Y, Peuchmaur M, et al. Medullary thyroid carcinoma identified within the first year of life in children with hereditary multiple endocrine neoplasia type 2A (codon 634) and 2B. Eur J Endocrinol. 2009;160:807–13.
Wells Jr SA, Dilley WG, Farndon JA, Leight GS, Baylin SB. Early diagnosis and treatment of medullary thyroid carcinoma. Arch Intern Med. 1995;145:1248–52.
van Heerden JA, Grant CS, Gharib H, et al. Long-term course of patients with persistent hypercalcitoninemia after apparent curative primary surgery for medullary thyroid carcinoma. Ann Surg. 1990;212:395–400.
Ellenhorn JD, Shah JP, Brennan MF. Impact of therapeutic regional lymph node dissection for medullary carcinoma of the thyroid gland. Surgery. 1993;114:1078–81.
Tung WS, Vesely TM, Moley JF. Laparoscopic detection of hepatic metastases in patients with residual or recurrent medullary thyroid cancer. Surgery. 1995;118:1024–9.
Chen H, Roberts JR, Ball DW, Eisele DW, et al. Effective long-term palliation of symptomatic, incurable metastatic medullary thyroid cancer by operative resection. Ann Surg. 1998;227:887–95.
Brain SD, Williams TJ, Tippins JR. Calcitonin gene-related peptide is a potent vasodilator. Nature. 1985;313:54–6.
Modigliani E, Cohen R, Joannidis S, Siame-Mourot C, et al. Results of long-term continuous subcutaneous octreotide administration in 14 patients with medullary thyroid carcinoma. Clin Endocrinol (Oxf). 1992;36:183–6.
Cohen MS, Phay JE, Albinson C, DeBenedetti MK, et al. Gastrointestinal manifestations of multiple endocrine neoplasia type 2. Ann Surg. 2002;235:648–54.
Rambaud JC, Jian R, Flourie B, et al. Pathophysiological study of diarrhoea in a patient with medullary thyroid carcinoma: evidence against a secretory mechanism and for the role of shortened colonic transit time. Gut. 1988;29:537–43.
Rolston RK, Ghatei MA, Mulderry PK, Bloom SR. Intravenous calcitonin gene-related peptide stimulates net water secretion in rat colon in vivo. Dig Dis Sci. 1989;34:612–6.
Bergholm U, Adami HO, Auer G, et al. Histopathologic characteristics and nuclear DNA content as prognostic factors in medullary thyroid carcinoma: a nationwide study in Sweden. The Swedish MTC Study Group. Cancer. 1989;64:135–42.
Bergholm U, Bergstrom R, Ekbom A. Long-term follow-up of patients with medullary carcinoma of the thyroid. Cancer. 1997;79:132–8.
Modigliani E, Cohen R, Campos JM, Conte-Devolx B, et al. Prognostic factors for survival and for biochemical cure in medullary thyroid carcinoma: results in 899 patients. Clin Endocrinol (Oxf). 1998;48:265–73.
Pelizzo MR, Boschin IM, Bernante P, Toniato A, Piotto A, et al. Natural history, diagnosis, treatment and outcome of medullary thyroid cancer: 37 years experience on 157 patients. Eur J Surg Oncol. 2007;33:493–7.
Farndon JR, Leight GS, Dilley WG, et al. Familial medullary thyroid carcinoma without associated endocrinopathies: a distinct clinical entity. Br J Surg. 1986;73:278–81.
Ponder BA, Ponder MA, Coffey R, et al. Risk estimation and screening in families of patients with medullary thyroid carcinoma. Lancet. 1989;1:397–401.
Stepanas AV, Samaan NA, Hill Jr CS, Hickey RC. Medullary thyroid carcinoma: importance of serial serum calcitonin measurement. Cancer. 1979;43:825–37.
Barbet J, Campion L, Kraeber-Bodere F, Chatal J-F, et al. Prognostic impact of serum calcitonin and carcinoembryonic antigen doubling-times in patients with medullary thyroid carcinoma. J Clin Endocrinol Metab. 2005;90:6077–84.
Kouvaraki MA, Shapiro SE, Fornage BD, et al. Role of preoperative ultrasonography in the surgical management of patients with thyroid cancer. Surgery. 2003;134:946–54.
Gotthardt M, Battmann A, Hoffken H, et al. 18F-FDG PET, somatostatin receptor scintigraphy, and CT in metastatic medullary thyroid carcinoma: a clinical study and an analysis of the literature. Nucl Med Commun. 2004;25:439–43.
Kebebew E, Kikuchi S, Duh QY, Clark OH. Long-term results of reoperation and localizing studies in patients with persistent or recurrent medullary thyroid cancer. Arch Surg. 2000;135:895–901.
Fleming JB, Lee JE, Bouvet M, Schultz PN, et al. Surgical strategy for the treatment of medullary thyroid carcinoma. Ann Surg. 1999;230:697–707.
Moley JF, Dilley WG, DeBenedetti MK. Improved results of cervical reoperation for medullary thyroid carcinoma. Ann Surg. 1997;225:734–40.
Yen TW, Shapiro SE, Gagel RF, Sherman SI, Lee JE, Evans DB. Medullary thyroid carcinoma: results of a standardized surgical approach in a contemporary series of 80 consecutive patients. Surgery. 2003;134:890–9.
Brierley JD. Update on external beam radiation therapy in thyroid cancer. J Clin Endocrinol Metab. 2011;96:2289–95.
Sugawara M, Geffner DL, Martinez D, Hershman JM. Novel treatment of medullary thyroid cancer. Curr Opin Endocrinol Diabetes Obes. 2009;16:367–72.
Campbell MJ, Seib CD, Gosnell J. Vandetanib and the management of advanced medullary thyroid cancer. Curr Opin Oncol. 2013;25:39–43.
Solomon B, Rischin D. Progress in molecular targeted therapy for thyroid cancer: vandetanib in medullary thyroid cancer. J Clin Oncol. 2012;30:119–21.
Wells SA, Robinson BG, Gagel RF, et al. Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: a randomized double-blind phase III trial. J Clin Oncol. 2012;30:134–41.
Robinson BG, Paz-Ares L, Krebs A, et al. Vandetanib (100 mg) in patients with locally advanced or metastatic hereditary medullary thyroid cancer. J Clin Endocrinol Metab. 2010;95:2664–71.
Wells SA, Gosnell JE, Gagel RF, et al. Vandetanib for the treatment of patients with locally advanced or metastatic hereditary medullary thyroid cancer. J Clin Oncol. 2010;28:767–72.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media New York
About this chapter
Cite this chapter
Ball, D.W., Wartofsky, L. (2016). Clinical Aspects of Medullary Thyroid Carcinoma. In: Wartofsky, L., Van Nostrand, D. (eds) Thyroid Cancer. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-3314-3_83
Download citation
DOI: https://doi.org/10.1007/978-1-4939-3314-3_83
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-3312-9
Online ISBN: 978-1-4939-3314-3
eBook Packages: MedicineMedicine (R0)