
Abstract
Deep brain stimulation (DBS) is a therapy that has been used for more than half a century to treat chronic pain. The first use of these treatments occurred in the 1950s when neurosurgeons stimulated the septal region nuclei in patients with psychiatric diseases who also suffered from chronic pain. Over the next 20 years, the therapy evolved to include the sensory thalamic nuclei to treat pain of neuropathic origin. Stimulation of the periventricular grey matter (PVG) has generally been recommended for the treatment of nociceptive pain, whereas the sensory thalamus (ST) remains the preferred stimulation site for neuropathic pain. Currently several new targets are under investigation. Outcomes for both facial and extremity pain have been positive with appropriate patient and target selection. The use of DBS in the neuromodulation algorithm is increasingly helpful to those who have severe pain. Because of its invasiveness and the risks associated with DBS, it is restricted to a selected group of patients in whom conservative treatment of chronic pain syndromes has been ineffective.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Deep brain stimulation (DBS) is a therapy that has been used for more than half a century to treat chronic pain. The first use of these treatments occurred in the 1950s when neurosurgeons stimulated the septal region nuclei in patients with psychiatric diseases who also suffered from chronic pain. Over the next 20 years, the therapy evolved to include the sensory thalamic nuclei to treat pain of neuropathic origin. Stimulation of the periventricular grey matter (PVG) has generally been recommended for the treatment of nociceptive pain, whereas the sensory thalamus (ST) remains the preferred stimulation site for neuropathic pain. Currently several new targets are under investigation. Outcomes for both facial and extremity pain have been positive with appropriate patient and target selection. The use of DBS in the neuromodulation algorithm is increasingly helpful to those who have severe pain. Because of its invasiveness and the risks associated with DBS, it is restricted to a selected group of patients in whom conservative treatment of chronic pain syndromes has been ineffective.
Effective application of DBS requires a thorough knowledge of the theory of modulating the central pain matrix including neuroanatomy, neural circuits, and individual targets involved in pain processing. Many patients have mixed pain syndromes of neuropathic and nociceptive character. It is now thought that white matter pathways passing through the PVG may be involved in stimulation-induced pain relief. Increased activation of the medial dorsal nucleus of the thalamus, an area associated with the limbic system including the amygdala and cingulate cortex, has been observed during PVG stimulation. Thus, in addition to activating the descending opioid system, stimulation of the PVG may also modify the patient’s emotional response to pain. The mechanism of analgesia elicited by electrical stimulation of the ST is similarly incompletely understood. Its effect may be mediated by activation of the inhibitory corticofugal fibers that prevent the pathological spread of painful stimuli.
2 Technical Overview
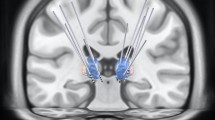
DBS electrodes are implanted to the desired target using either a frame-based or a frameless stereotactic approach. Numerous variations in surgical technique—general anesthesia versus local anesthesia with or without sedation, use of microelectrode recording, use of intraoperative imaging, and staging of implantation of electrodes and pulse generators—exist, often determined by surgeon preference and the circumstances of the individual patient. A preoperative high-resolution stereotactic magnetic resonance imaging (MRI) and/or computed tomography (CT) scan is obtained (Fig. 32.1). After completion of the imaging and planning, the patient is brought to the operating room, where she or he is carefully positioned on the operating table and local anesthesia along with mild intravenous sedation is administered.

Frame-based stereotactic guidance for deep brain lead placement (left). Frameless stereotactic guidance for deep brain lead placement (right)
Stereotactic localization of bilateral entry points is performed and these areas are then marked. The head is shaved, prepared, and draped in the standard sterile fashion. Incisions are opened and meticulous hemostasis achieved. Two 14-mm bur holes are then drilled bilaterally centered over the prior stereotactic localization points. A number of frame, miniframe, or frameless systems are now available; however, the general principles are similar. Registration is performed with the intraoperative navigation station and less than 0.5 mm error is preferred.
Once exposure is achieved, physiological microelectrode recording is performed to achieve optimal electrode positioning. It is a key point to remember that the stereotactic coordinates represent the starting point for target identification, but that the end target is identified in the operating room.
The dura, pia, and cortical surface are coagulated and incised on one side, beginning contralateral to the patient’s worst symptoms. The trajectory is aligned using the previous target and entry projection. Initial depth is commonly set to 10 mm above target, ensuring that the patient’s blood pressure is normotensive. Electrophysiological activity is typically used to identify exact targets. This is done by microelectrode recording and microelectrode stimulation followed by macrostimulation. The microelectrode is advanced in a stepwise fashion, continuously recording. A DBS electrode is then measured to the appropriate length and introduced to the target point (Fig. 32.2). Test stimulation is carried out with the goal of minimal adverse effects with good therapeutic benefit. Once the lead position has been confirmed, the outer cannula is withdrawn and a skull fixation device is fastened to ensure that the electrode is held firmly in place. The leads are connected to temporary externalized extensions for a trial phase of stimulation.

Final lead placement for DBS target
In the postoperative period, close attention to blood pressure control is performed and the postoperative CT or MRI performed to confirm accurate electrode placement and to rule out any evidence of intracranial hemorrhage. In general, combined stimulation of periventricular gray (PVG) and ventral posterior lateral thalamus (VPL) has been superior to single-lead stimulation. In most patients a certain subperception threshold is needed to produce a pain-relieving effect. If appropriate and acceptable pain relief is achieved, the patient is brought back to the operating room, where the temporary connector is removed and a permanent extension cable is used to connect to the lead to the implanted pulse generator. A subcutaneous pocket is prepared for the internal generator and the extensions are passed through the subcutaneous tissue to connect the system. If the system fails to provide relief, the patient is not a candidate for a permanent device, and the lead is explanted.
3 Risk Assessment
-
1.
Mortality from DBS is a rare complication that occurs in less than 0.4 % of patients.
-
2.
Neurological compromise occurs in less than 1.3 % of patients on a permanent basis.
-
3.
The most devastating risk of DBS is intracranial hemorrhage. Hemorrhages are identified in 2–5 % of patients receiving DBS and can occur at the time of implant or at the time of removal. Asymptomatic hemorrhage occurs in 1.9 % of implanted patients, where symptomatic hemorrhage occurs in 2.1 % and hemorrhage resulting in death or permanent deficit in 1.1 %. Postimplantation infarcts occur in under 1 % of patients [1].
-
4.
Infection rates vary among institutions and have been reported between 1% and 13 %. Infectious complications can include meningitis, encephalitis, skin infection, sepsis, and death [2].
-
5.
Hardware-related complications including lead fracture, short circuit, and electrode migration occur in under 4 % of cases. Loss of effective stimulation coupled with imaging evidence of fracture or persistent high or extremely low impedance readings across several contacts of the electrode are most indicative of a hardware failure [3].
-
6.
Less serious but troubling complications include seizures and stimulation-related side effects such as diplopia, nausea, vertical gaze palsies, nystagmus, oscillopsia, and blurred vision depending on lead location and stimulation side effects that are often overcome with proper programming. In infrequent instances, a misplaced electrode must be surgically relocated to a more effective target site [4].
4 Risk Avoidance
-
1.
Preoperative screening for DBS should be similar to screening performed for other neurosurgical procedures including preadmission testing, a focus on comorbidities, and an evaluation of current medications. Preoperative anesthesia consultation is a necessity to improve overall outcomes.
-
2.
Prior to surgery the physician should review the patient’s medications and ensure that all medical conditions are under adequate control prior to moving forward. Drugs that affect bleeding should be discussed with the proper medical specialist and discontinued when safe and advisable.
-
3.
Preoperative and intraoperative antibiotics are recommended. Most infections with deep brain implants resolve with proper antibiotics and only if severe and refractory, require wound debridement and/or removal of all hardware.
-
4.
It is critical to have the patient keep a good diary of the pain level and patterns prior to the implant and during the course of the trial. The patient should experience significant relief of the pain and be educated about the system prior to the permanent generator placement.
-
5.
When tunneling the permanent system, the clinician must be careful to avoid blood vessels along the path of the extension. The carotid and jugular vessels are of particular concern.
-
6.
The position of the generator pocket should be carefully planned to allow patient comfort and to avoid tissue irritation or skin erosion. Most of these devices are placed in the infraclavicular soft tissue superficial to the pectoralis fascia. In thinner individuals an abdominal or flank location may be considered.
5 Conclusions
DBS has been a treatment option for over 50 years and the therapy continues to evolve. Current studies geared toward expanding our understanding of DBS for the treatment of pain may lead to improved patient outcomes related to better matching of pain patterns with the optimal DBS target. The use of DBS offers hope to those who have failed other pain treatment modalities for severe neuropathic pain. The use of DBS should be considered a last resort when spinal cord stimulation and peripheral nerve stimulation are not reasonable options.
References
Zrinzo L, Foltynie T, Limousin P, Hariz MI. Reducing hemorrhagic complications in functional neurosurgery: a large case series and systematic literature review. J Neurosurg. 2012;116:84–94.
Falowski S, Ooi YC, Smith A, Verhargen Metman L, Bakay RA. An evaluation of hardware and surgical complications with deep brain stimulation based on diagnosis and lead location. Stereotact Funct Neurosurg. 2012;90:173–80.
Baizabal Carvallo JF, Mostile G, Almaguer M, Davidson A, Simpson R, Jankovic J. Deep brain stimulation hardware complications in patients with movement disorders: risk factors and clinical correlations. Stereotact Funct Neurosurg. 2012;90:300–6.
Coley E, Farhadi R, Lewis S, Whittle IR. The incidence of seizures following deep brain stimulating electrode implantation for movement disorders, pain and psychiatric conditions. Br J Neurosurg. 2009;23:179–83.
Suggested Reading
Abosch A, Timmermann L, Bartley S, Rietkerk HG, Whiting D, Connolly PJ, et al. An international survey of deep brain stimulation procedural steps. Stereotact Funct Neurosurg. 2013;91(1):1–11.
Boccard SG, Pereira EA, Moir L, Aziz TZ, Green AL. Long-term outcomes of deep brain stimulation for neuropathic pain. Neurosurgery. 2013;72:221–30.
Hosobuchi Y. Dorsal periaqueductal gray matter stimulation in humans. Pacing Clin Electrophysiol. 1987;10:213–6.
Kumar K, Toth C, Nath RK. Deep brain stimulation for intractable pain: a 15-year experience. Neurosurgery. 1997;40:736–46.
Kumar K, Wyant GM, Nath R. Deep brain stimulation for control of intractable pain in humans, present and future: a ten-year follow-up. Neurosurgery. 1990;26:774–82.
Levy RM, Lamb S, Adams JE. Treatment of chronic pain by deep brain stimulation: long-term follow-up and review of the literature. Neurosurgery. 1987;21:885–93.
Pool JL, Clark WD, Hudson P, Lombardo M. Hypothalamic-hypophyseal interrelationships. Springfield: Charles C. Thomas; 1956.
Rinaldi PC, Young RF, Albe-Fessard D, Chodakiewitz J. Spontaneous neuronal hyperactivity in the medial and intralaminar thalamic nuclei of patients with deafferentation pain. J Neurosurg. 1991;74:415–21.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media New York
About this chapter
Cite this chapter
Lad, S.P., Petersen, E.A., Marky, A., Deer, T.R., Levy, R.M. (2016). Neurostimulation: Stimulation of the Cranium and Head: Stimulation of the Deep Brain for the Treatment of Chronic Pain. In: Deer, T., Pope, J. (eds) Atlas of Implantable Therapies for Pain Management. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-2110-2_32
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2110-2_32
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-2109-6
Online ISBN: 978-1-4939-2110-2
eBook Packages: MedicineMedicine (R0)