
Abstract
Cardiorespiratory fitness and muscular strength are important components of health-related physical fitness. The criterion measures for cardiorespiratory fitness and dynamic muscular strength are maximal oxygen uptake (VO2max) and one-repetition maximum (1RM), respectively. VO2max testing requires expensive laboratory equipment and expert personnel. Such maximal intensity testing may require physician clearance or supervision for older, sedentary and/or unfit individuals. 1RM testing requires the performance of multiple resistance exercise sets at near-maximal and maximal intensities and may not be safe for many individuals who are unfamiliar with resistance exercise or who have medical contraindications to high intensity exercise. Therefore, administration of maximal fitness test protocols may not be possible, pragmatic or even desirable in health-fitness and clinical settings. As such, submaximal tests have been developed to predict both VO2max and 1RM. It is proposed that the use of submaximal test protocols is both safe and cost-effective. Statistical models to predict VO2max have been based on the positive relation between HR and VO2 during load-incremented exercise. Models to predict 1RM have been based on the inverse relation between weight lifted and repetitions performed to the point of muscular fatigue. However, both VO2max and 1RM can be predicted from submaximal RPE. The use of RPE as a predictor variable in such tests is valid, technically simple, and easily understood by most individuals. In addition, submaximal fitness tests including the measurement of RPE can be used as an assessment of training-induced fitness changes. The primary purpose of this laboratory experiment is to predict VO2max/peak and 1RM from submaximal RPE measured during an estimation protocol exercise test.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Cardiorespiratory fitness
- Maximal oxygen consumption (VO2max)
- Graded exercise test (GXT)
- One-repetition maximum (1RM)
- Maximal HR (HRmax)
- Prediction model
- Cross-validation
- Perceptually-regulated exercise test
Cardiorespiratory fitness and muscular strength are important components of health-related physical fitness. The criterion measures for cardiorespiratory fitness and dynamic muscular strength are maximal oxygen uptake (VO2max) and one-repetition maximum (1RM), respectively. VO2max testing requires expensive laboratory equipment and expert personnel. Such maximal intensity testing may require physician clearance or supervision for older, sedentary and/or unfit individuals. 1RM testing requires the performance of multiple resistance exercise sets at near-maximal and maximal intensities and may not be safe for many individuals who are unfamiliar with resistance exercise or who have medical contraindications to high intensity exercise. Therefore, administration of maximal fitness test protocols may not be possible, pragmatic or even desirable in health-fitness and clinical settings. As such, submaximal tests have been developed to predict both VO2max and 1RM. It is proposed that the use of submaximal test protocols is both safe and cost-effective. Statistical models to predict VO2max have been based on the positive relation between HR and VO2 during load-incremented exercise. Models to predict 1RM have been based on the inverse relation between weight lifted and repetitions performed to the point of muscular fatigue. However, both VO2max and 1RM can be predicted from submaximal RPE. The use of RPE as a predictor variable in such tests is valid, technically simple, and easily understood by most individuals. In addition, submaximal fitness tests including the measurement of RPE can be used as an assessment of training-induced fitness changes. The primary purpose of this laboratory experiment is to predict VO2max/peak and 1RM from submaximal RPE measured during an estimation protocol exercise test.
1 Background
1.1 Assessment of Cardiorespiratory Fitness
Cardiorespiratory fitness determines an individual’s ability to perform dynamic exercise of a moderate to vigorous intensity using large muscle groups for a prolonged period. Cardiorespiratory fitness depends on the functional capacity of the cardiovascular and respiratory systems and the oxidative capacity of skeletal muscle (ACSM 2013). The criterion or “gold-standard” assessment of cardiorespiratory fitness is VO2max (i.e., maximal aerobic power), defined as the maximal amount of oxygen an individual can use during dynamic exercise while breathing air at sea level. The assessment of VO2max requires an individual to perform a load-incremented aerobic exercise protocol, or GXT, where pulmonary ventilation (V E) and expired concentrations of VO2 and VCO2 are determined using a respiratory-metabolic measurement system. For most clinically normal individuals, a valid VO2max can only be achieved during upright, weight-bearing, total body exercise such as uphill walking or running on a treadmill. The term VO2peak is used rather than VO2max when the measure is obtained using cycle ergometer exercise and other partial- or non-weight-bearing exercise modalities (e.g., swimming, elliptical ergometer, rowing ergometer, and arm ergometer). However, it is of note that when elite cyclists perform a load-incremented GXT on a cycle ergometer they often demonstrate a higher VO2max than for uphill treadmill exercise. It is important to assess an individual’s VO2max/peak with a mode-specific GXT that matches their exercise experience and the mode of exercise for which the prescription is intended. For most individuals, a treadmill protocol is appropriate.
VO2max and VO2peak tests allow determination of the VT. The VT is an important physiological marker for aerobic training intensity. At test intensities above the VT, an individual can no longer achieve steady state metabolic energy production. HR and/or RPE can be measured throughout a GXT. The HR or RPE values corresponding to specific physiological intensities (e.g., %VO2max or %VT) can then be used to prescribe exercise intensity. However, the ability to calculate target HR or RPE ranges based on VO2 responses to an exercise test comes with inherent costs and risks. First, the measurement and interpretation of respiratory-metabolic responses are time-consuming procedures that require expensive laboratory equipment and expert personnel that are not available in many clinics and fitness facilities. Maximal exercise testing often requires physician clearance and test supervision, especially when older, sedentary and/or unfit individuals are evaluated. This imposes additional financial and testing burden on the client and testing facility. Therefore, it is often not possible, practical or even desirable to perform a maximal test with respiratory-metabolic measurement to establish an individual’s cardiorespiratory fitness prior to undertaking an aerobic exercise program.
1.2 Assessment of Dynamic Muscular Strength
Muscular strength reflects the ability of a muscle or muscle group to exert force. Muscular strength can be assessed statically, involving isometric muscular action with no change in muscle length or joint angle, or dynamically, involving concentric and/or eccentric muscular contractions and changes in muscle length. Since assessments of static muscular strength are only specific to the joint angle used in testing, dynamic muscular strength is considered more ecologically valid. The criterion or “gold-standard” assessment of dynamic muscular strength is the 1RM test. The 1RM is used to establish the maximal amount of force an individual can exert during one repetition of single maximal effort using a defined muscle or muscle group. The lift must be performed in a controlled manner through the full range of motion with proper technique (ACSM 2013). This test requires that an individual perform multiple resistance exercise sets at near-maximal and maximal intensities using a progressive protocol. Unlike VO2max testing, most clinics and fitness facilities have ample resistance exercise equipment and educated personnel to assess 1RM strength. The primary concern for an individual who is undergoing a 1RM baseline test prior to beginning a resistance exercise program is safety. Many individuals who are beginning a resistance exercise program, including children and adolescents, have little to no experience with resistance exercise. In particular, they lack instruction on proper exercise technique. For these individuals, performing a 1RM test is not practical and may result in musculoskeletal injury. Even a multiple-RM test, where the goal is to perform a set number of repetitions ending at maximal intensity (e.g., 5RM or 10RM), may not be safe for many individuals. If a 1RM or multiple-RM test is employed, it may be best to guide the individual through a brief orientation and practice period that employs the exercise protocol prior to maximal testing.
1.3 Submaximal Tests to Predict Maximal Aerobic Power and Muscular Strength
Due to the methodological and safety limitations of measuring maximal aerobic power (i.e., VO2max) and muscular strength (i.e., 1RM), researchers have designed submaximal exercise tests from which maximal values can be predicted. The methods used to predict VO2max and 1RM are based on the relations between the criterion variable and predictor variable(s). For aerobic exercise, VO2 serves as the criterion variable since VO2max/peak is the unknown that is estimated by prediction models. For resistance exercise, weight lifted serves as the criterion variable since 1RM is the unknown that is estimated by prediction models. The predictor variables are physiological and/or physical markers that rise concurrently with increases in exercise intensity.
Traditional prediction models for aerobic exercise are based on the strong positive correlation between VO2 and HR that has been consistently demonstrated in the literature. The model of VO2 max using submaximal HR is dependent on the relative accuracy of age-predicted maximal HR (APMHR) equations (e.g., APMHR = 220 − age) and the positive relation between VO2 and HR as measured during a load-incremented protocol. The prediction can be presented graphically and/or determined using linear regression analysis. For a graphic determination, VO2 and HR data points from multiple submaximal exercise intensities are plotted on separate axes. HR, the predictor variable, is on the x-axis. VO2, the criterion variable, is on the y-axis. A line of best fit that describes the relation between the two variables is drawn by visual determination. The point where the line intercepts APMHR is extended laterally to the VO2 axis, identifying predicted VO2max. Using a linear regression model a line of best fit is calculated that describes the relation between HR and VO2 where these variables are expected to change as a function of increasing exercise intensity. This calculation yields an equation, VO2max = s(APMHR) + i. In this equation, s is the slope of the line and i is the y-intercept. One solves for VO2max by entering APMHR into the prediction equation.
Although HR is relatively easy to measure during aerobic exercise and most clinics and fitness facilities have appropriate technology and/or personnel, APMHR is not always the most accurate prediction of actual HRmax. The primary prediction equations used in the health-fitness setting are: APMHR = 220 − age for males; APMHR = 226 − age for females. These equations are based on large sample data with standard deviations of ±11 b·min−1 (Londeree and Moeschberger 1982). A standard deviation can be defined as the average amount by which the scores in a distribution differ from the mean. Therefore, based on the above APMHR equation for men and women and the reported standard deviation for the derived value, the average 20-year-old will have a HRmax between 189 and 211 b·min−1, but could even have a HRmax below 189 b·min−1 or above 211 b·min−1. As such, APMHR can have a considerable amount of error for an individual resulting in even greater error for predicted VO2max. A target HR range for a prescribed training program that is based on a VO2max prediction model using APMHR, could then be either below or above that which provides an optimal overload stimulus for the individual. A target HR range set too low may not provide the individual with an appropriate overload stimulus to achieve health-fitness benefits. A target HR range set too high may not be tolerable for the individual, causing early termination of an exercise session and eventually leading to dropout from the exercise program.
The use of equations that employ APMHR to predict VO2max/peak as a basis for exercise prescription is not appropriate for many individuals with certain clinical conditions. Individuals taking beta-blocker medication to control hypertension exhibit a blunted HR response, especially during aerobic exercise. In such conditions, HRmax would be much lower than that estimated by the APMHR equation. Individuals with pulmonary limitations to exercise, such as chronic obstructive pulmonary disease (COPD) or cystic fibrosis, often terminate exercise because of dyspnea, or shortness of breath, and cannot reach maximal/peak HR levels similar to clinically normal individuals of the same age. Also, individuals with peripheral artery disease (PAD) experience claudication pain in active limbs, even at submaximal exercise intensities. In these patients, exercise is prescribed based on tolerable levels of perceived pain rather than a target HR range. For any clinical conditions where there may be an increased risk for adverse events during exercise, it is important to obtain physician clearance prior to participation in exercise testing or an exercise program. Often, exercise testing with physician supervision may be indicated.
The only way to ensure accuracy when prescribing aerobic exercise based on the expected positive relation between HR and VO2 is to actually measure HRmax and VO2max. This necessitates that the GXT terminates at maximal intensity. However, a maximal GXT may not be possible due to the lack of respiratory-metabolic instrumentation or trained testing personnel. In addition, a maximal GXT may not be appropriate because of time constraints when administering the test protocol and the possible error induced when developing a prediction based on APMHR. VO2 has shown strong correlations with RPE, a fact well-established in experiments demonstrating the concurrent validity of RPE scales. As such, submaximal RPE expressed as a function of either HR or VO2 can be used to predict VO2max/peak. Numerous investigations have shown the validity of RPE-based exercise tests to predict VO2max/peak (Davies et al. 2008; Eston et al. 2005, 2006, 2008, 2012; Faulkner et al. 2007; Faulkner and Eston 2007; Morris et al. 2009, 2010).
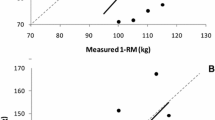
Prior to the initiation of a resistance training program for an untrained individual, the administration of 1RM testing may not be indicated because of safety concerns. The statistical basis for traditional models to predict 1RM is the strong inverse relation between weight lifted per repetition and the number of repetitions performed until fatigue. As weight increases, the number of repetitions that can be performed until fatigue decreases, ultimately resulting in the 1RM value. The linear relation between submaximal weight lifted and repetitions performed can be analyzed to predict the amount of weight lifted for 1RM. Weight lifted has shown strong correlations with RPE, a fact well-established in experiments demonstrating the concurrent validity of RPE scales. As such, the relation between resistance and RPE allows the prediction of 1RM. A number of investigations have shown the validity of RPE-based exercise tests to predict 1RM (Eston and Evans 2009; Gearhart et al. 2008; Robertson et al. 2008).
1.4 RPE-Based Models to Predict VO2max and 1RM
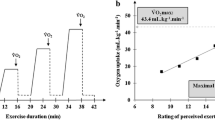
The development of RPE-based models to predict VO2max and 1RM follow the same design as models based on HR and weight lifted, respectively. Prediction of VO2max using RPE as the predictor variable is based on the positive relation between VO2 and RPE that occurs during load-incremented aerobic exercise. Likewise, prediction of 1RM using RPE as the predictor variable is based on the positive relation between weight lifted and RPE that occurs during load-incremented resistance exercise. These relations and their predictive properties can be presented graphically and/or determined using linear regression analysis. For a graphic prediction procedure, VO2 (or weight lifted) and RPE data points measured at multiple submaximal exercise intensities are plotted on separate axes. A line of best fit that describes the relation between the two variables is drawn by visual determination. When using a HR-based model to predict maximal aerobic power, the point where the line intercepts APMHR is extended laterally to the VO2 axis, identifying predicted VO2max. However, when using a category rating scale, the RPE used to predict VO2max or 1RM is a fixed value, i.e., the maximal RPE (RPEmax) on the category scale. The use of such a fixed upper rating category facilitates the prediction of the corresponding VO2max/1RM value when employing a graphic procedure.
Statistical prediction models that employ RPE as a predictor variable are based on Borg’s Range Model. According to Borg’s Range Model, when an individual reaches maximal intensity of the perceptual response range, they should report the highest numerical category, i.e., an RPEmax of 10 using the OMNI Scale, or 20 using the Borg Scale. Therefore, for visual determination of VO2max using the line of best fit derived from an RPE-based model, the point where the line of best fit intercepts RPEmax is extended laterally to the VO2 axis, identifying predicted VO2max. For visual determination of 1RM using submaximal RPE responses, the point where the line of best fit intercepts RPEmax is extended laterally to the y-axis to identify predicted 1RM. Using linear regression, the average positive relation as depicted by the line of best fit is calculated using submaximal VO2 (or weight lifted) and RPE responses to a load-incremented protocol. For aerobic exercise, this calculation yields an equation, VO2max = s(RPEmax) + i, where the predictor variable is RPE and the criterion variable is VO2. For resistance exercise, 1RM is predicted using the same linear regression model. In these linear regression equations, s is the slope of the line of best fit and i is the y-intercept. Then, one solves for VO2max or 1RM by entering RPEmax into the prediction equation.
1.5 Evaluating the Accuracy of RPE-Based Prediction Models
The accuracy of both HR- and RPE-based statistical models to predict VO2max can be evaluated in a laboratory setting where standardized testing instrumentation and control and experimental conditions are available. Using a statistical regression procedure where multiple measurements are required, the subject performs three different submaximal exercise intensities. On a treadmill, the intensities are progressively increased by changing speed and/or grade. On a cycle ergometer, the intensities are progressively increased by incremental changes in PO. The intensities on both a treadmill and cycle ergometer are presented in a load-incremented format. However, there are also less frequently employed protocols that present the different intensities in random order. HR and RPE are measured near the end of each 2–3-min exercise stage.
Using a computer program such as Microsoft Excel, plots of VO2 expressed as a function of HR and as a function of RPE are developed so the relation between variables can be depicted both graphically and using statistical linear regression analysis. VO2max can be predicted by extrapolating submaximal responses to intercept at APMHR or RPEmax using the graphic procedure. In addition, the computer program employs the linear regression equation to determine the line of best fit. The slope and intercept of this regression line can be used to predict VO2max as previously described. Alternatively, some computer programs, such as the Statistical Package for the Social Sciences (SPSS), use a linear regression equation to determine the line of best fit without inclusion of the graphic procedure. In order to compare measured VO2max with that predicted using both the HR and RPE models, the subject should perform an entire GXT terminating at maximal intensity.
For aerobic exercise, both undifferentiated RPE (RPE-O) and the dominant differentiated RPE (i.e., RPE-Legs) have been used in models to predict VO2max/peak (Faulkner and Eston 2007). In some instances, the dominant RPE for a given exercise mode may explain a greater amount of variance in VO2max (i.e., is a better predictor) than the undifferentiated RPE-O. For resistance exercise, only differentiated RPE for the active muscle mass (RPE-AM) has been used in statistical models to predict 1RM (Eston and Evans 2009; Robertson et al. 2008).
1.6 Cross-Validation of RPE-Based Prediction Models
From a research perspective, statistical prediction models can be developed for the field setting that do not require actual measurement of VO2. These statistical models must be validated in one sample of subjects then cross-validated in a separate but similar sample of subjects. For the initial validation study, subjects undergo two separate exercise trials: (1) a criterion VO2max test on a treadmill in a laboratory setting; and (2) a submaximal exercise protocol appropriate for administration in the field setting during which RPE are measured. A statistical regression procedure is used to develop an equation to predict criterion measured VO2max using submaximal RPE responses measured during the field test. This equation is used to calculate predicted VO2max for each subject. Criterion measured VO2max is then compared with predicted VO2max. If predicted VO2max is similar to actual measured VO2max (i.e., exhibiting no statistically significant difference), the field-based prediction model is deemed valid.
The statistical model developed and validated in one subject group is then cross-validated by testing the equation on a separate sample of subjects. For such a cross-validation study, the subjects also undergo two separate exercise trials: (1) a criterion VO2max test on a treadmill in a laboratory setting; and (2) the same submaximal exercise field protocol used for the initial validation study, during which RPE are measured. This second, cross-validation sample should have similar characteristics (i.e., age, sex, PA level) as the initial validation sample used to develop the RPE-based prediction equation. Generally, the more specific the population for which the prediction equation is designed, the less error there will be in the predicted VO2max using criterion variables measured under field conditions. Predicted VO2max, calculated using the previously developed equation, is compared with actual measured VO2max using the cross-validation subject sample. If predicted VO2max is similar to actual measured VO2max, then the field-based prediction equation has been successfully cross-validated using an independently selected subject sample. The equation could then be used to predict VO2max for similar individuals in a health-fitness facility where respiratory-metabolic instrumentation is unavailable.
1.7 A Perceptually Regulated Exercise Test to Predict VO2peak
Eston and colleagues (2005) developed an alternative type of submaximal exercise test to predict cycle ergometer VO2peak in healthy adults. This exercise is in contrast to commonly used protocols that employ specific increments in power output to produce a systematic increase in exercise intensity. This exercise test is perceptually regulated using step-wise increments in RPE that are produced sequentially to progressively increase exercise intensity. Using the Borg (6–20) Scale, at each 2-min test stage subjects were asked to self-regulate exercise intensity by producing the following RPE’s: 9, 11, 13, 15, and 17. VO2 was recorded near the end of each stage. Linear regression was used to develop equations for the relation between RPE and the corresponding submaximal VO2 response. To predict VO2peak, RPEmax (i.e., Borg Scale RPE of 20) was entered into the regression equations. The perceptually regulated exercise test and subsequent prediction equation d procedures were repeated two additional times to test the effects of protocol familiarity on VO2peak prediction. The results of the investigation found that equations developed using RPE’s 9 through 15 and RPE’s 9 through 17 both predicted VO2peak with reasonable accuracy. However, the equation developed using RPE’s 9 through 17 was more precise, predicting most subjects’ VO2peak within 5–7 ml·kg−1 min−1. In addition, the accuracy of such prediction was improved with practice, evidenced by a closer agreement of predicted and measured VO2peak between trials two and three than between trials one and two (Eston et al. 2005). Subsequent investigations confirmed the ability of perceptually regulated exercise tests to predict VO2max/peak in both active and sedentary adults performing cycle ergometer exercise (Eston et al. 2006, 2008; Faulkner et al. 2007; Morris et al. 2009) and treadmill exercise (Eston et al. 2012; Morris et al. 2010), as well as in able-bodied individuals and paraplegics performing arm ergometery (Al-Rahamneh and Eston 2011).
1.8 Submaximal Tests to Assess Training-Induced Fitness Changes
An advantage of exercise tests used to predict VO2max/peak and 1RM is that they can also use submaximal end-points to assess training induced fitness changes. If the same procedures are performed prior to the initiation of an exercise training program and after a designated amount of time participating in the exercise program, pre- and post-training submaximal values can be compared. This can be accomplished using either load-incremented estimation protocols or perceptually regulated protocols. For an estimation protocol, HR and RPE measured during a given workload (i.e., exercise intensity) can be compared before and after training. For a given exercise intensity, decreases in HR reveal a lowered physiological strain to perform the fixed intensity and an improvement in cardiorespiratory fitness. Pre- to post-training decreases in RPE when measured at a given PO (intensity) indicates that the perception of effort associated with a given level of exercise is comparatively lower following a training program. A lower perception of exertion fatigue at a given workload indicates improved tolerance of that exercise intensity and as such an improvement in cardiorespiratory fitness. In addition, this perceptual training adaptation allows the individual to perform the given exercise intensity for a greater amount of time.
This perceptual training adaptation holds true for resistance exercise training programs as well. That is, for a given weight lifted, the perception of exertion decreases from pre- to post-training. A decrease in RPE for a given resistance load indicates improved muscular strength and the ability to perform a lift of that weight for a higher number of repetitions after training. Likewise, for a perceptually regulated aerobic exercise protocol, if a given RPE is produced by self-regulating exercise at a higher workload following training, this decreased perception of exertion indicates an improved exercise tolerance.
1.9 Case Study
1.9.1 Client Information
A 55-year-old female who works in a local office building comes to your fitness facility. During a pre-participation interview prior to exercise testing, she tells you that she walks her dog each evening after dinner. She describes how she recently completed an office fitness challenge that involved counting steps each week and learned that she does not exercise nearly as much as others in the office nor does she meet recommended guidelines for regular PA participation. She is slightly overweight and believes her fitness level to be below average. Her goals are to lose weight, increase aerobic fitness and improve muscular strength. She is very busy at the office and cannot increase her time available to exercise. She knows she should try to exercise at a higher intensity but is not sure what level is appropriate for her. Also, she wants to learn how she can keep her muscle tone using the resistance equipment that is available through her office wellness center.
1.9.2 Assessments, Results and Analysis
Perform submaximal exercise protocols to predict VO2max/peak and/or muscular strength (1RM) using RPE from which appropriate exercise intensities can be determined to achieve weight loss, aerobic fitness, and muscular strength goals.
-
1.
Calculate predicted VO2max/peak:
-
2.
Determine the appropriate exercise intensity for her initial aerobic exercise prescription.
-
3.
Calculate predicted 1RM:
-
4.
Determine an appropriate load for the resistance exercises to be performed for her initial resistance exercise prescription.
2 Methods
2.1 Treadmill Procedures: Prediction of VO2max
2.1.1 Equipment
-
1.
Adult OMNI-Walk/Run RPE Scale (Fig. A.2)
-
2.
Treadmill
-
3.
HR monitor
-
4.
Respiratory-metabolic measurement system
2.1.2 Pre-exercise Procedures
-
1.
Measure height (cm) and weight (kg) of subject.
-
2.
Read the standard instructions for the Adult OMNI-Walk/Run RPE Scale for RPE-O to the subject (Appendix B.1). For prediction of VO2max using differentiated RPE (RPE-L and RPE-C) as well, read the standard instructions for the Adult OMNI-Walk/Run RPE Scale for undifferentiated and differentiated RPE (Appendix B.2). Perform the memory anchoring procedure as described in Chap. 5.
2.1.3 Graded Exercise Test to Measure VO2max
-
1.
Position the HR monitor and respiratory-metabolic mouthpiece (with head support unit and nose clip if applicable) on the subject.
-
2.
Instruct the subject to step onto the treadmill and review exercise termination procedures: When the subject cannot continue exercise due to exhaustion or discomfort, he/she should grasp the treadmill hand rails, at which time the test administrator will gradually slow the treadmill down for performance of a cool-down. The subject should be reminded not to step off the treadmill belt while it is still in motion.
-
3.
Bruce Multistage Treadmill Test Protocol: this can be performed by manually adjusting treadmill speed and grade or using a program on a computer that is interfaced to the treadmill.
-
(a)
Begin the warm-up at 1.5 miles·h−1 and 0% grade for 3 min.
-
(b)
Each exercise test stage will last for 3 min. The stages progress as follows:
-
Stage 1—1.7 miles·h−1 and 10 % grade
-
Stage 2—2.5 miles·h−1 and 12 % grade
-
Stage 3—3.4 miles·h−1 and 14 % grade
-
Stage 4—4.2 miles·h−1 and 16 % grade
-
Stage 5—5.0 miles·h−1 and 18 % grade
-
Stage 6—5.5 miles·h−1 and 20 % grade
-
Stage 7—6.0 miles·h−1 and 22 % grade
-
Stage 8—6.5 miles·h−1 and 24 % grade
-
-
(c)
When the subject cannot continue any longer, terminate the exercise test by initiating the cool-down period at 1.5 miles h−1 and 0 % grade. The cool-down should be 5 min in duration.
-
(d)
Instruct the subject to estimate RPE starting at 2:30 of each exercise stage using the OMNI Scale (RPE-O; RPE-L and RPE-C if desired). The RPE’s should be rated in a counterbalanced sequence. Because the position of respiratory-metabolic mouth piece inhibits a verbal response, instruct the subject to point to the numbers on the RPE scale, which should be conveniently positioned within the subject’s arm reach. State aloud the numerical ratings for each momentary assessment to which the subject pointed and request a confirmatory nod that the number stated was correct. If incorrect, allow the subject to point to the appropriate rating on the RPE scale once more. Ask the subject to hold his or her finger on the appropriate number on the scale for approximately 1 s.
-
(e)
Record HR (b·min−1) at 2:55 of each exercise stage.
-
(f)
Record the final 15-s VO2 (ml·kg−1·min−1) for each exercise stage.
-
(g)
Record HRmax as the highest HR value recorded during the final exercise stage or immediately post-exercise.
-
(h)
Record VO2max as the highest 15-s VO2 value recorded at the end of the test.
-
(a)
2.1.4 Submaximal Protocol to Predict VO2max
-
1.
Position the HR monitor and respiratory-metabolic mouthpiece (with head support unit and nose clip if applicable) on the subject.
-
2.
Instruct the subject to step onto the treadmill and review termination procedures. The subject should be reminded not to step off the treadmill belt while it is still in motion.
-
3.
Three submaximal exercise intensities will be performed. Select the intensity sequence from Table 8.1 that is consistent with the subject’s training status.
Table 8.1 Exercise intensities for submaximal treadmill protocol -
(a)
The subject will perform each exercise intensity (A, B, and C) for 4 min with a 5-min seated recovery between each exercise.
-
(b)
Instruct the subject to estimate RPE-O (RPE-L and RPE-C are optional) at 1:30 and 3:30 of each exercise intensity using the OMNI Scale. The RPE’s should be rated in a counterbalanced sequence. Because the position of the respiratory-metabolic mouth piece inhibits a verbal response, instruct the subject to point to the numbers on the RPE scale, which should be conveniently positioned within the subject’s arm reach. State aloud the numerical ratings for each momentary assessment to which the subject pointed and request a confirmatory nod that the number stated was correct. If incorrect, allow the subject to point to the appropriate rating on the RPE scale once more. Ask the subject to hold his or her finger on the appropriate number on the scale for approximately 1 s.
-
(c)
Record HR (b·min−1) every 2 min of each exercise intensity.
-
(d)
Record the final 15-s VO2 (ml·kg−1·min−1) for each 2-min segment of exercise.
-
(a)
2.1.5 Data Organization and Analysis
-
1.
In a Microsoft Excel spreadsheet, label columns of data for the following variables: Exercise Intensity (A, B, C), VO2 (ml·kg−1·min−1), OMNI RPE-O, HR (b·min−1). Include columns for OMNI RPE-L and OMNI RPE-C if applicable.
-
2.
Plot of VO2 and OMNI RPE-O for prediction of VO2max.
-
(a)
Click on the INSERT tab and in the CHARTS section click on SCATTER. Select the first available chart option. A blank or example scatter plot will appear on your screen.
-
(b)
Click on the SELECT DATA tab. Remove any entries found in the LEGEND ENTRIES text box then click ADD. Under SERIES NAME, enter VO2 and OMNI RPE-O. Then click on the icon to the right of the SERIES X VALUES text box and highlight the OMNI RPE-O values. After the values are highlighted click the icon on the box that appeared. Then click on the icon to the right of the SERIES Y VALUES text box and highlight the VO2 values. After the values are highlighted click the icon on the box that appeared. Click OK on the next two screens.
-
(c)
You should now have a scatter plot with OMNI RPE-O on the x-axis and VO2 on the y-axis. Create a title for the plot and enter the appropriate axis labels and units of measure.
*Methodological note: During aerobic exercise, RPE increases linearly with increases in both physical (PO, speed, grade) and physiological (HR, VO2) analogs of exercise intensity. Therefore, this laboratory experiment uses a linear equation to predict VO2max.
-
(d)
To determine the equation from which VO2max will be predicted, click on one of the data points to highlight the entire data series. Right click on one of the data points and a menu will appear. Click ADD TRENDLINE and the FORMAT TRENDLINE menu will appear. Select LINEAR and DISPLAY EQUATION ON CHART then click CLOSE. The trendline and equation will be displayed on the chart.
-
(e)
Use this linear equation to calculate predicted VO2max. Use the OMNI RPE-O of 10 as the “x” value in the equation and solve for “y.” The calculated “y” value is the predicted VO2max (ml·kg−1·min−1).
-
(a)
-
3.
Repeat the above steps for VO2 and HR to determine VO2max predicted from submaximal HR, using APMHR as the “x” value in the prediction equation. You may also determine predicted VO2max using differentiated OMNI RPE’s (RPE-L and RPE-C), also using the OMNI RPE-L and -C of 10.
-
4.
An example of these procedures with a screenshot depicting each step as performed using Microsoft Excel 2013 can be found in Appendix E.
2.2 Cycle Ergometer Procedures: Prediction of VO2peak
2.2.1 Equipment
-
1.
Adult OMNI-Cycle RPE Scale (Fig. 2.4)
-
2.
Cycle ergometer
-
3.
Metronome
-
4.
HR monitor
-
5.
Respiratory-metabolic measurement system
2.2.2 Pre-exercise Procedures
-
1.
Measure height (cm) and weight (kg) of subject.
-
2.
Read the standard instructions for the Adult OMNI-Cycle RPE Scale for RPE-L to the subject (Appendix B.4). For prediction of VO2peak using undifferentiated RPE (RPE-O) and differentiated RPE for chest/breathing (RPE-C) as well, read the standard instructions for the Adult OMNI-Cycle RPE Scale for undifferentiated and differentiated RPE to the subject (Appendix B.5). Perform the memory anchoring procedure as described in Chap. 5.
2.2.3 Graded Exercise Test to Measure VO2peak
-
1.
Position the HR monitor and respiratory-metabolic mouthpiece (with head support unit and nose clip if applicable) on the subject.
-
2.
Set the proper seat height on the cycle ergometer according to leg length. When the foot is flat on the right pedal and the pedal is in the extreme down position, there should be a flexion of the right knee of approximately 5°.
-
3.
Load-incremented protocol for electronically braked and friction-braked cycle ergometers:
-
(a)
Instruct the subject to maintain a 50 rev min−1 pedal cadence. Set the metronome to 100 b·min−1 so each downward movement of each foot is synchronized with a beat of the metronome. The subject may also use the digital monitor on the cycle control panel to regulate pedal cadence.
-
(b)
For electronically braked cycle ergometers (e.g., Lode), begin stage 1 at 50 W then increase the resistance 25 W every 2 min.
-
(c)
For friction-braked cycle ergometers (e.g., Monark), begin stage 1 at 1 kg resistance then increase the resistance 0.5 kg every 2 min.
-
(d)
When the subject cannot maintain the pedal cadence for 10 consecutive seconds, terminate the exercise test.
-
(e)
Instruct the subject to estimate RPE starting at 1:30 of each exercise stage using the OMNI Scale (RPE-L; RPE-O, and RPE-C if desired). The RPE’s should be rated in a counterbalanced sequence. Because the position of the respiratory-metabolic mouth piece inhibits a verbal response, instruct the subject to point to the numbers on the RPE scale, which should be conveniently positioned within the subject’s arm reach. For each momentary assessment, state aloud the numerical ratings to which the subject pointed and request a confirmatory nod that the number stated was correct. If incorrect, allow the subject to point to the appropriate rating on the RPE scale once more. Ask the subject to hold his or her finger on the appropriate number on the scale for approximately 1 s.
-
(f)
Record HR (b·min−1) at 1:55 of each exercise stage.
-
(g)
Record the final 15-s VO2 (l·min−1) for each exercise stage.
-
(h)
Record HRpeak as the highest HR value recorded during the final exercise stage or immediately post-exercise.
-
(i)
Record VO2peak as the highest 15-s VO2 value recorded at the end of the test.
-
(a)
2.2.4 Submaximal Protocol to Predict VO2peak
-
1.
Position the HR monitor and respiratory-metabolic mouthpiece (with head support unit and nose clip if applicable) on the subject.
-
2.
Instruct the subject to maintain a 50 rev min−1 pedal cadence. Set the metronome to 100 b·min−1 so each downward movement of each foot is synchronized with a beat of the metronome. The subject may also use the digital monitor on the cycle control panel to regulate pedal cadence.
-
3.
Three submaximal exercise intensities will be performed. Select the intensity sequence from Tables 8.2 or 8.3 that is consistent with the subject’s training status.
Table 8.2 Exercise intensities for submaximal, electronically braked cycle ergometer protocol Table 8.3 Exercise intensities for submaximal, friction-loaded cycle ergometer protocol -
(a)
The subject will perform each exercise intensity (A, B, and C) for 4 min with a 5-min seated recovery between each exercise. Terminate exercise if the subject cannot maintain the 50 rev min−1 pedal cadence for 10 consecutive seconds owing to fatigue.
-
(b)
Instruct the subject to estimate RPE-L at 1:30 and 3:30 of each exercise intensity using the OMNI Scale (RPE-O and RPE-C are optional). The RPE’s should be rated in a counterbalanced sequence. Because the position of the respiratory-metabolic mouth piece inhibits a verbal response, instruct the subject to point to the numbers on the RPE scale, which should be conveniently positioned within the subject’s arm reach. State aloud the numerical ratings for each momentary assessment to which the subject pointed and request a confirmatory nod that the number stated was correct. If incorrect, allow the subject to point to the appropriate rating on the RPE scale once more. Ask the subject to hold his or her finger on the appropriate number on the scale for approximately 1 s.
-
(c)
Record HR (b·min−1) every two minutes of each exercise intensity.
-
(d)
Record the final 15-s VO2 (l·min−1) for each two minute segment of exercise.
-
(a)
2.2.5 Data Organization and Analysis
-
1.
In a Microsoft Excel spreadsheet, label columns of data for the following variables: Exercise Intensity (A, B, C), VO2 (l min−1), OMNI RPE-L, HR (b·min−1). Include columns for OMNI RPE-O and OMNI RPE-C if applicable.
-
2.
Plot of VO2 and OMNI RPE-L for prediction of VO2peak.
-
(a)
Click on the INSERT tab and in the CHARTS section click on SCATTER. Select the first available chart option. A blank or example scatter plot will appear on your screen.
-
(b)
Click on the SELECT DATA tab. Remove any entries found in the LEGEND ENTRIES text box then click ADD. Under SERIES NAME, enter VO2 and OMNI RPE-L. Then click on the icon to the right of the SERIES X VALUES text box and highlight the OMNI RPE-L values. After the values are highlighted click the icon on the box that appeared. Then click on the icon to the right of the SERIES Y VALUES text box and highlight the VO2 values. After the values are highlighted click the icon on the box that appeared. Click OK on the next two screens.
-
(c)
You should now have a scatter plot with OMNI RPE-L on the x-axis and VO2 on the y-axis. Create a title for the plot and enter the appropriate axis labels and units of measure.
*Methodological note: During aerobic exercise, RPE increases linearly with increases in both physical (PO, speed, grade) and physiological (HR, VO2) analogs of exercise intensity. Therefore, this laboratory experiment uses a linear equation to predict VO2max.
-
(d)
To determine the equation from which VO2peak will be predicted, click on one of the data points to highlight the entire data series. Right click on one of the data points and a menu will appear. Click ADD TRENDLINE and the FORMAT TRENDLINE menu will appear. Select LINEAR and DISPLAY EQUATION ON CHART then click CLOSE. The trendline and equation will be displayed on the chart.
-
(e)
Use this linear equation to calculate predicted VO2peak. Use the OMNI RPE-L of 10 as the “x” value in the equation and solve for “y.” The calculated “y” value is the predicted VO2peak (l min−1).
-
(a)
-
3.
Repeat the above steps using submaximal VO2 and HR to predict VO2peak. Then calculated regression model uses APMHR as the “x” value in the prediction equation. You may also determine predicted VO2peak from OMNI RPE-O and RPE-C. This procedure uses the OMNI RPE of 10 as the “x” value.
-
4.
An example of these procedures with a screenshot depicting each step as performed using Microsoft Excel 2013 can be found in Appendix E.
2.3 Resistance Exercise Procedures: Prediction of 1RM
2.3.1 Equipment
-
1.
Adult OMNI-Resistance Exercise RPE Scale (Fig. A.5)
-
2.
Resistance exercise equipment for performance of flat bench press
-
3.
Metronome
2.3.2 Pre-exercise Procedures
Read the standard instructions for the Adult OMNI-Resistance Exercise RPE Scale for RPE-AM to the subject (Appendix B). Perform the memory anchoring procedure as described in Chap. 5.
2.3.3 1RM Maximum Strength Test
Administer a 1RM procedure for assessment of muscular strength according to the procedures of Baechle and Earle (2008).
-
1.
Instruct the subject to warm-up with a light resistance that can be performed for 5–10 repetitions, then provide a 1-min rest.
-
2.
Estimate a warm-up load that will allow the subject to complete 3–5 repetitions by adding 10–20 lb (5–10% of previous weight lifted) for upper body exercise or 30–40 lb (10–20% of previous weight lifted) for lower body exercise. At the conclusion of the warm-up, provide a 2-min rest.
-
3.
Estimate a conservative, near maximal load that will allow the subject to complete 2–3 repetitions by adding 10–20 lb (5–10% of previous weight lifted) for upper body exercise or 30–40 lb (10–20% of previous weight lifted) for lower body exercise. Following completion of the lift, provide a 2-minute rest.
-
4.
Increase the resistance load by 10–20 lb (5–10% of previous weight lifted) for upper body exercise or 30–40 lb (10–20% of previous weight lifted) for lower body exercise and instruct the subject to attempt a 1RM.
-
5.
If the subject successfully completes the lift using proper technique, provide a 2–4-min rest and repeat the previous step. If the subject failed to complete the lift owing to improper technique or having reached maximum muscle tension production, provide a 2–4-min rest then decrease the resistance by 5–10 lb (2.5–5% of previous weight lifted) for upper body exercise or 15–20 lb (5–10% of previous weight lifted) for lower body exercise and instruct the subject to attempt a 1RM using the adjusted weight.
-
6.
Continue increasing or decreasing the load until the subject can complete a 1RM with proper exercise technique.
-
7.
Instruct the subject to estimate OMNI RPE-AM at the end of each resistance exercise set.
2.3.4 Submaximal Protocol to Predict 1RM
-
1.
Three submaximal exercise intensities will be performed. Select the intensity sequence from Table 8.4 that is consistent with the subject’s resistance training status.
Table 8.4 Exercise intensities for submaximal resistance exercise protocol for bench press -
2.
The subject will perform each exercise intensity (A, B, and C) for one set of five repetitions with a 5-min seated recovery between sets.
-
3.
Remind the subject to rate the intensity of feelings of exertion for the active muscle(s) during the concentric phase of the final repetition of each set.
-
4.
Instruct the subject to estimate OMNI RPE-AM at the end of each resistance exercise set.
2.3.5 Data Organization and Analysis
-
1.
In a Microsoft Excel spreadsheet, label columns of data for the following variables: Exercise Intensity (A, B, C), Weight Lifted, and OMNI RPE-AM.
-
2.
Plot of Weight Lifted and OMNI RPE-AM for prediction of 1RM.
-
(a)
Click on the INSERT tab and in the CHARTS section click on SCATTER. Select the first available chart option. A blank or example scatter plot will appear on your screen.
-
(b)
Click on the SELECT DATA tab. Remove any entries found in the LEGEND ENTRIES text box then click ADD. Under SERIES NAME, enter Weight Lifted and OMNI RPE-AM. Then click on the icon to the right of the SERIES X VALUES text box and highlight the OMNI RPE-AM values. After the values are highlighted click the icon on the box that appeared. Then click on the icon to the right of the SERIES Y VALUES text box and highlight the Weight Lifted values. After the values are highlighted click the icon on the box that appeared. Click OK on the next two screens.
-
(c)
You should now have a scatter plot with OMNI RPE-AM on the x-axis and Weight Lifted on the y-axis. Create a title for the plot and enter the appropriate axis labels and units of measure.
*Methodological note: During resistance exercise, RPE increases linearly with increases in both physical (absolute weight lifted, %1RM) and physiological (blood lactate concentration) analogs of exercise intensity. Therefore, this laboratory experiment uses a linear equation to predict 1RM.
-
(d)
To determine the equation from which 1RM will be predicted, click on one of the data points to highlight the entire data series. Right click on one of the data points and a menu will appear. Click ADD TRENDLINE and the FORMAT TRENDLINE menu will appear. Select LINEAR and DISPLAY EQUATION ON CHART then click CLOSE. The trendline and equation will be displayed on the chart.
-
(e)
Use this linear regression equation to calculate predicted 1RM. Use the OMNI RPE-AM of 10 as the “x” value in the equation and solve for “y.” The calculated “y” value is the predicted 1RM (lbs).
-
(a)
-
3.
An example of these procedures with a screenshot depicting each step as performed using Microsoft Excel 2013 can be found in Appendix E.
3 Discussion Questions
-
1.
How does VO2max/peak or 1RM that is predicted using responses from a submaximal exercise protocol compare to the actual measured VO2max/peak or 1RM? List some possible reasons why predicted values may differ from actual measured values.
-
2.
How can fitness be tracked over time using a VO2max/peak or 1RM prediction protocol? What must be done to ensure the methods are sensitive to changes in aerobic or muscular fitness?
-
3.
How could RPE be used to prescribe aerobic and resistance exercise intensity based on the results from a submaximal protocol to predict VO2max/peak or 1RM?
References
Al-Rahamneh H, Eston RG. Prediction of maximal oxygen uptake from the ratings of perceived exertion during a graded and ramp exercise test in able-bodied and persons with paraplegia. Arch Phys Med Rehabil. 2011;92:277–83.
American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013.
Baechle TR, Earle RW. Essentials of strength training and conditioning. 3rd ed. Champaign, IL: Human Kinetics; 2008.
Davies RC, Rowlands AV, Eston RG. The prediction of maximal oxygen uptake from sub-maximal ratings of perceived exertion elicited during the multistage fitness test. Br J Sports Med. 2008;42:1006–10.
Eston RG, Lamb KL, Parfitt G, King N. The validity of predicting maximal oxygen uptake from a perceptually-regulated graded exercise test. Eur J Appl Physiol. 2005;94:221–7.
Eston RG, Faulkner J, Mason E, Parfitt G. The validity of predicting maximal oxygen uptake from perceptually-regulated exercise tests of different durations. Eur J Appl Physiol. 2006;97:535–41.
Eston R, Lambrick D, Sheppard K, Parfitt G. Prediction of maximal oxygen uptake in sedentary males from a perceptually regulated, sub-maximal graded exercise test. J Sports Sci. 2008;26:131–9.
Eston R, Evans HJL. The validity of submaximal ratings of perceived exertion to predict one repetition maximum. J Sports Sci Med. 2009;8:567–73.
Eston R, Evans H, Faulkner J, Lambrick D, Al-Rahamneh H, Parfitt G. A perceptually-regulated, graded exercise test predicts peak oxygen uptake during treadmill exercise in active and sedentary participants. Eur J Appl Physiol. 2012;112:3459–68.
Faulkner J, Eston R. Overall and peripheral ratings of perceived exertion during a graded exercise test to volitional exhaustion in individuals of high and low fitness. Eur J Appl Physiol. 2007;101:613–20.
Faulkner J, Parfitt G, Eston R. Prediction of maximal oxygen uptake from the ratings of perceived exertion and heart rate during a perceptually-regulated sub-maximal exercise test in active and sedentary participants. Eur J Appl Physiol. 2007;101:397–407.
Gearhart Jr RF, Lagally KM, Riechman SE, Andrews RD, Robertson RJ. RPE at relative intensities after 12 weeks of resistance-exercise training by older adults. Percept Motor Skills. 2008;106:893–903.
Londeree B, Moeschberger ML. Effect of age and other factors on maximal heart rate. Res Q Exerc Sport. 1982;53:297–304.
Morris M, Lamb KL, Cotterell D, Buckley J. Predicting maximal oxygen uptake via a perceptually regulated exercise test (PRET). J Exerc Sci Fit. 2009;7:122–8.
Morris M, Lamb KL, Hayton J, Cotterell D, Buckley J. The validity and reliability of predicting maximal oxygen uptake from a treadmill-based sub-maximal perceptually regulated exercise test. Eur J Appl Physiol. 2010;109:983–8.
Robertson RJ, Goss FL, Aaron DJ, Gairola A, Kowallis RA, Liu Y, Randall CR, Tessmer KA, Schnorr TL, Schroeder AE, White B. One repetition maximum prediction models for children using the OMNI RPE scale. J Strength Cond Res. 2008;22:196–201.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Haile, L., Gallagher, M., J. Robertson, R. (2015). Prediction of Maximal Aerobic Power and Dynamic Muscular Strength Using RPE. In: Perceived Exertion Laboratory Manual. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1917-8_8
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1917-8_8
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1916-1
Online ISBN: 978-1-4939-1917-8
eBook Packages: Behavioral ScienceBehavioral Science and Psychology (R0)