
Abstract
Along with urinary storage, the emptying of urine is a key function of the bladder. Although this seems simple on the surface, the ability to completely empty the bladder safely and efficiently requires the intimate coordination of numerous organs, supporting structures, and neurotransmitters. While a low post-void residual (PVR) is often considered a surrogate for complete emptying, this value may not be consistent from void to void and may be affected by numerous factors. The PVR value should be evaluated as a single puzzle piece, in the scope of the patient’s history, findings on physical examination, and measures of actual emptying, such as uroflowmetry and/or pressure-flow studies. The goal of this chapter will be to focus on the emptying phase and what steps constitute complete emptying. The chapter will also illustrate examples of incomplete emptying, their pathophysiology, urodynamic and radiographic findings, and implications for the patient.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Stress Urinary Incontinence
- Detrusor Overactivity
- Bladder Outlet Obstruction
- Pelvic Floor Muscle Training
- Detrusor Contraction
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
While the bladder may be considered by some to be an “unreliable witness [1],” its functions in the big picture are relatively straightforward. The bladder must complete two functions: the storage and emptying of urine. In reality, the ability to complete these tasks safely and efficiently requires the intimate coordination of numerous organs, supporting structures, and neurotransmitters, the description of which is far beyond the confines of this chapter. The goal of this chapter will be to focus on the emptying phase and what steps constitute complete emptying. The chapter will also illustrate some examples of incomplete emptying, their pathophysiology, and potential implications for the patient.
What Is Complete Emptying?
Interestingly, little information can be located regarding the exact definition of “complete emptying.” This particular term is not covered in The Standardisation of Terminology of Lower Urinary Tract Function [2]; however, the “feeling of incomplete emptying” is mentioned as one of the post-micturition symptoms. It is described as “self-explanatory” and no additional details are given. Despite the lack of specific definition, it can be safely inferred that any definition of “complete emptying” should include a low urinary post-void residual (PVR), defined as the volume of urine left in the bladder at the end of micturition [2]. Conversely, a high PVR typically indicates incomplete emptying.
It is important to note that an isolated elevated PVR is a poor surrogate for incomplete emptying. First, inhibition or attempts at emptying an incompletely full bladder may result in a high PVR. Second, the voided volume (VV) is often not taken into account (i.e., a large VV with an elevated PVR represents a different scenario than a small VV and elevated PVR). Third, PVR alone does not reflect the voiding mechanism (i.e., detrusor contraction, valsalva straining, pelvic relaxation) and any element of detrusor underactivity or bladder outlet obstruction (BOO). Thus, any examination of incomplete emptying should include not only the PVR, but also a measure of voiding such as a non-instrumented uroflowmetry (UF) or an intubated pressure-flow study (PFS).
What Constitutes an Elevated PVR?
Once again, a single definition does not exist. Huang et al. examined 987 women 55–75 years of age culled from a group health plan in Washington State, of whom 10 % had a PVR of 50–99 mL and 11 % had a PVR ≥ 100 mL at baseline [3]. In adjusted analyses, women with a PVR of ≥ 100 mL were more likely to report urinating more than eight times during the day and women with a PVR of ≥ 200 mL were more likely to report weekly urinary urgency incontinence (UUI) than those with a PVR < 50 mL. High PVR was not associated with greater risk of stress urinary incontinence (SUI), nocturnal frequency, or urinary tract infection (UTI), indicating that many women with high PVR are asymptomatic. Similarly, the prevalence of elevated PVR (≥100 mL) was 11 % in approximately 1,400 women with pelvic floor disorders undergoing evaluation at a large urogynecological referral center [4]. Symptoms alone did not predict which women had an elevated PVR, but the finding of prolapse at or beyond the hymen was associated with incomplete emptying. In another retrospective study, 15.9 % of 107 women with predominantly SUI and absence of previous pelvic surgery, advanced pelvic prolapse, and/or neurological deficit had a PVR > 100 mL [5]. The prevalence of elevated PVR in the infirmed may be even higher. Tam et al. found that 22 % of 119 consecutive patients admitted into two convalescent wards were found to have a PVR > 100 mL and in 9.2 % the PVR exceeded 400 mL [6]. There was an increased risk of UTI when the PVR exceeded 100 mL.
The definition of an elevated PVR in men is no clearer. Kolman et al. evaluated PVR in 477 randomly selected community-dwelling white men as part of a baseline urological evaluation and found that the distribution of PVR was highly skewed with a median of 9.5 mL and 25th and 75th percentiles equal to 2.5 mL and 35.4 mL, respectively [7]. There was a significant correlation of PVR with prostate volume and the odds of PVR > 50 mL were 2.5 times greater for men with prostate volume greater than 30 mL than those with smaller prostates. In regression analyses PVR, did not appear to be associated with the AUA symptom index, age, or peak urinary flow rate. Men with enlarged prostate volume or PVR greater than 50 mL at baseline were about three times as likely to have subsequent acute urinary retention with catheterization during 3–4 years of follow-up.
Finally, the relationship between elevated PVR and urinary retention is likewise unclear [8]. In their review of MEDLINE literature, Kaplan et al. point out that the threshold for elevated PVR is often 100 mL, while the definitions of chronic urinary retention range widely in the literature (100–500 mL). Additionally, PVR does not seem to be a strong predictor of acute urinary retention. Furthermore, the authors conclude that there is no actual numerical value or relative increase in the volume of PVR that has been universally accepted or adopted into clinical practice. As such, the PVR measurement should act as a noninvasive screening test for evaluating voiding dysfunction. Taken with a good history, physical examination, and uroflowmetry, PVR measurement may aid in identifying patients in need of further evaluation and to evaluate treatment effect during follow-up.
Implications of Elevated PVR
Both an elevated PVR and urinary retention may be associated with some significant sequelae. Pelvic and suprapubic pain and pressure, as well as lower urinary tract symptoms (LUTS) such as urinary urgency and frequency may result from overdistention. Urinary stasis may result in UTIs and bladder calculi. Additionally, elevated intravesical pressure may result in hydroureteronephrosis, upper tract deterioration, and renal insufficiency. As mentioned previously, elevated PVRs may be caused by detrusor hypocontractility or acontractility, BOO, or, in rare cases, anatomic abnormalities such as large bladder diverticula. BOO can stem from an anatomic blockage (prostatic enlargement, urethral stricture, meatal stenosis) or a functional obstruction from poor sphincter relaxation (dyssynergia). Poor bladder contractility can result from neurogenic, myogenic, psychogenic, or pharmacologic causes.
Cases
-
Case 1: 61 years of man who presents with urinary retention
-
History: Patient voided small volumes with 2,200 mL PVR and subsequently placed on clean intermittent catheterization (CIC). He states he has always been a “slow voider” and denies urgency or UUI. He is otherwise healthy. DRE: >90 g benign prostate.
-
Course: Patient started on α-adrenergic antagonist (α-blocker) and 5-α reductase inhibitor (5-αRI) and CIC. He has been voiding on own with volumes 100–200 mL at a time. CIC volumes after volitional voiding are 100–150 mL.
-
Urodynamics (Fig. 18.1): Unable to perform pre-procedure UF; slightly decreased cystometric bladder capacity (~330 mL); no detrusor overactivity (DO); high compliance; no leak with valsalva maneuver; incomplete emptying on PFS with high-pressure, low-flow pattern (P det@Q max = 57 cm H2O); PVR 115 mL.
Fig. 18.1 
CMG: slightly decreased cystometric bladder capacity (~330 mL); no DO; high compliance; no leak with valsalva maneuver; incomplete emptying on PFS with high-pressure, low-flow pattern (P det@Q max = 57 cm H2O); PVR = 115 mL
-
Cystoscopy: Trilobar prostatic hypertrophy, very large median lobe, bladder trabeculations.
-
CT (for microscopic hematuria work-up): Very large median lobe (Fig. 18.2).
Fig. 18.2 
CT: very large median lobe of the prostate
-
Diagnosis: BOO due to benign prostatic obstruction (BPO).
-
Options: Continue α-blocker and 5-αRI, transurethral resection of prostate (TURP), suprapubic prostatectomy.
-
Commentary: This gentleman has clear evidence of BOO and options for relieving outlet resistance are effective in improving symptoms.


-
Case 2: 67 years of man presents for evaluation of UUI.
-
History: He complains of diurnal urgency, urinary frequency (10/day, 3/night), and UUI requiring 3–4 pads/24 h. He has subjective incomplete emptying. He denies weak stream or straining to urinate. DRE: 35 g benign prostate. The remainder of his history and exam are normal.
-
Course: Prostate specific antigen (PSA) is 0.45 ng/mL. Patient has been on dual therapy with α-blocker and 5-αRI for over a year and has also tried multiple muscarinic receptor antagonists (anticholinergics) in past without significant subjective improvement.
-
Urodynamics (Fig. 18.3): First sensation occurred at 106 mL, strong desire at 178 mL, and cystometric bladder capacity was 247 mL; Two episodes of DO at 150 mL of filling (pressures from 12 to 22 cm H2O). Both were associated with urgency but no leakage; high compliance; no leakage with cough or valsalva; during PFS (Fig. 18.4), P det@Q max = 65 cm H2O, P detmax = 84 cm H2O with a flow of 13.4 mL/s; Bladder Outlet Obstructive Index (BOOI) = 57.
Fig. 18.3 
CMG: first sensation at 106 mL; strong desire at 178 mL; cystometric bladder capacity at 247 mL; two episodes of DO at 150 mL of filling (pressures = 12–22 cm H2O); both episodes associated with urgency but no leakage; high compliance; no leakage with cough or valsalva
Fig. 18.4 
PFS: P det@Q max = 65 cm H2O; P detmax = 84 cm H2O; flow = 13.4 mL/s; Bladder Outlet Obstructive Index (BOOI) = 57
-
Cystoscopy: Posterior urethra remarkable for high bladder neck with co-apting lateral lobes; moderate bladder trabeculations; small-bladder diverticulum.
-
Diagnosis: DO and BOO (due to BPO).
-
Options: Additional anticholinergics, β-3 adrenergic agonist, sacral neuromodulation, intravesical onabotulinumtoxinA injection, TURP.
-
Commentary: The BOOI = P det@Q max − 2 × Q max, with a value <20 representing no obstruction, 20–40 representing an equivocal result, and >40 representing obstruction. This gentleman has both a problem during bladder filling (DO) and voiding (BOO). As such, he may require more than one treatment to alleviate his symptoms. While TURP may improve his BPO, he may continue to have bothersome storage symptoms. Conversely, medical or surgical treatment of his DO is unlikely to improve, and, in some cases may negatively impact his voiding.


-
Case 3: 50 years of woman with progressively worsening emptying.
-
History: She urinates frequently during day (diary: 10–14 voids/day, 2 voids/night; volumes 100–200 mL) and strains to urinate; (+) incomplete emptying; denies SUI or UUI; (+) UTIs, 2–3/year; (+) lumbar back injury after MVA 7 years ago; no spinal or pelvic surgery; (+) constipation; no pelvic prolapse on examination.
-
Course: She has not tried any active therapy.
-
Urodynamics: Unable to perform pre-procedure UF (Fig. 18.5; catheterized PVR = 350 mL); delayed first desire (Fig. 18.6; 693 mL); large bladder capacity (>800 mL); no DO; high compliance; unable to generate coordinated detrusor contraction during PFS (Fig. 18.7); PVR at end of procedure >1,000 mL.
Fig. 18.5 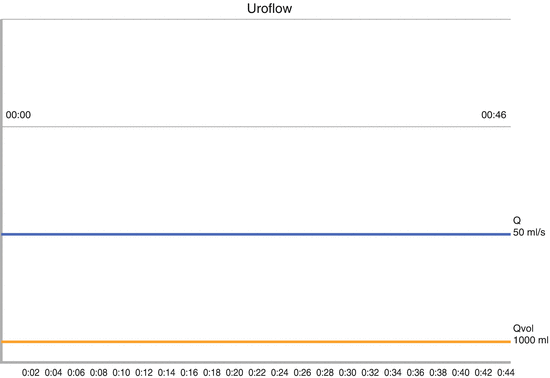
Patient was unable to perform pre-procedure UF (catheterized PVR = 350 mL)
Fig. 18.6 
CMG: delayed first desire (693 mL); large bladder capacity (>800 mL); no DO; high compliance
Fig. 18.7 
PFS: patient unable to generate coordinated detrusor contraction; PVR at end of procedure > 1,000 mL
-
Diagnosis: Urinary retention due to detrusor acontractility.
-
Options: CIC, sacral neuromodulation.
-
Commentary: This patient’s symptoms stem from suboptimal emptying due to a lack of detrusor contractility. Her upper tracts are likely safe owing to high compliance and absence of DO. Her volitional voids during the day are most likely due to either valsalva voiding or overflow events.



-
Case 4: 55 years of man with overactive bladder symptoms.
-
History: He complains of urinary urgency and UUI 1–2 days/week. He voids 8/day and 2/night. Stream is “fair.” He has tried two anticholinergics without significant benefit. He has had one recent culture-proven UTI (E. coli). Patient is otherwise healthy. DRE: 60 g benign prostate. He had a PVR of 198 and 187 mL on two consecutive visits.
-
Course: He had minimal improvement after a combination of an anticholinergic and α-blocker.
-
Urodynamics: Pre-CMG UF reveals Q max 20 and continuous flow curve with adequate voided volume (277 mL; Fig. 18.8); PVR is high (375 mL); delayed first desire on CMG (463 mL; Fig. 18.9) and delayed normal desire (810 mL); no DO; high compliance; high-pressure, low-flow pattern on PFS (Fig. 18.10), small volume void, high PVR; low-flow and high PVR on post-PFS UF (Fig. 18.11).
Fig. 18.8 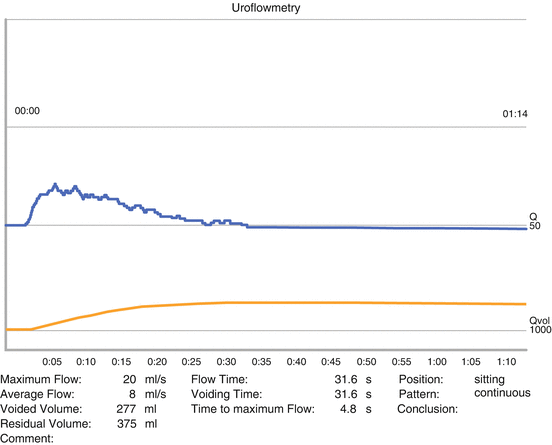
Pre-CMG UF: Q max = 20 mL/s with continuous flow curve with adequate voided volume (277 mL); PVR = 375 mL
Fig. 18.9 
CMG: delayed first desire to void (463 mL); delayed normal desire (810 mL); no DO; high compliance
Fig. 18.10 
PFS: high-pressure, low-flow pattern; small-volume void; high PVR
Fig. 18.11 
Post-PFS UF: low-flow; high PVR
-
Cystography: Large posterior bladder diverticulum (bladder is on the left) (Fig. 18.12); attempt to void (Fig. 18.13); post-void film showing empty bladder and full diverticulum (Fig. 18.14).
Fig. 18.12 
Cystography: large posterior bladder diverticulum (bladder is on the left)
Fig. 18.13 
Cystography during attempt to void
Fig. 18.14 
Post-void cystography: empty bladder and full diverticulum
-
Cystoscopy: Mild trilobar prostatic enlargement, multiple trabeculations with small-bladder diverticula, and one large posterior bladder diverticulum with 24 F ostium.
-
CT (for work-up of microscopic hematuria): Large bladder diverticulum (Fig. 18.15).
Fig. 18.15 
CT: large bladder diverticulum
-
Diagnosis: Stable bladder with evidence of BOO and large acquired bladder diverticulum.
-
Options: CIC, TURP, suprapubic prostatectomy ± bladder diverticulectomy, additional anticholinergics, β-3 adrenergic agonist.
-
Commentary: As with the man in Case 2, this gentleman has a problem with urinary storage and emptying, and thus may benefit from multiple treatments. Additionally, he has a large bladder diverticulum that is trapping urine and may be falsely elevating his PVR. Treating the outlet obstruction either first or concomitantly with the diverticulectomy is recommended.








-
Case 5: 62 years of man presents for evaluation of post-prostatectomy incontinence.
-
History: He has mild urinary urgency and frequency, mild incomplete emptying and mild weak stream. He does not strain to void. AUA SSI 7/35. He wears 1–2 pads/day for urinary incontinence that is worse with activity. His PSA is 0.0 ng/mL. He has a history of post-prostatectomy bladder neck contracture (BNC) and has undergone two previous BN incisions. The remainder of his history and physical examination are normal.
-
Course: He has not improved on Kegel exercises and has tried one anticholinergic without significant benefit.
-
Urodynamics: (Figs. 18.16 and 18.17) First sensation, strong desire, and bladder capacity were 61, 91, and 184 mL (leakage volumes subtracted), respectively; compliance was high; multiple episodes of DO starting at 65 mL, several with high-pressure (up to 70 cm H2O) and leakage; SUI with VLPP 67–79 cm H2O; continuous leakage of urine at bladder capacity and patient was given permission to void (Fig. 18.18); P detmax ~ 62 cm H2O with a flow of 10 mL/s (BOOI = 42).
Fig. 18.16 
CMG: First sensation (61 mL); strong desire (91 mL); bladder capacity (184 mL) after leakage volumes subtracted; high compliance; multiple episodes of DO starting at 65 mL, several with high-pressure (up to 70 cm H2O) and leakage; SUI with VLPP = 67–79 cm H2O
Fig. 18.17 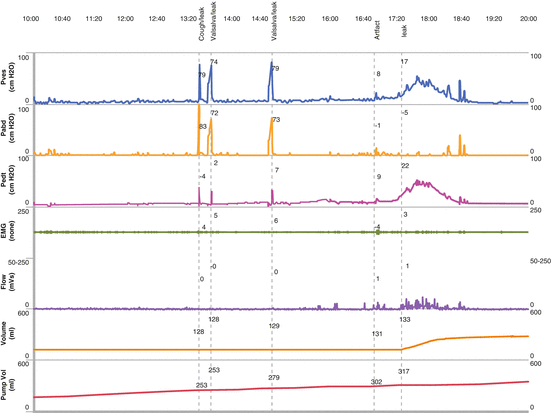
Continuation of the tracing in 18.16. Additional episodes of DO and leakage following Valsalva maneuvers
Fig. 18.18 
CMG/PFS: continuous leakage of urine at bladder capacity; patient was given permission to void; P detmax ~ 62 cm H2O with flow = 10 mL/s (BOOI = 42)
-
Cystoscopy: Unable to pass scope through a ~12 F bladder neck contracture.
-
Diagnosis: BOO due to bladder neck contracture with SUI (ISD) and significant DO.
-
Options: Observation, BN incision, anticholinergics, urethral stent, artificial urinary sphincter (AUS), Cunningham clamp, and condom catheter.
-
Commentary: As with previous cases, this gentleman has complex urinary dysfunction that may require multiple therapeutic options to achieve symptom improvement. Regardless of the options chosen, BOO needs to be relieved in order to improve emptying, with subsequent pharmaceutical or surgical intervention to improve this gentleman’s storage symptoms.



-
Case 6: 60 years of woman with SUI and mild emptying dysfunction
-
History: She has minimal diurnal urgency which is controlled with behavioral modification. She has some subjective incomplete emptying. She underwent one previous “bladder suspension” at time of abdominal hysterectomy 20 years ago. She has SUI with coughing, sneezing, and laughing, and requires 3 pads/day. No prolapse on exam (+). Urethral hypermobility.
-
Course: No improvement on behavioral modification, Kegel exercises. Patient did not want to pursue formal biofeedback and pelvic floor muscle training (PFMT).
-
Urodynamics: Adequate volume on pre-CMG UF with relatively low Q max; PVR is low (Fig. 18.19); mildly decreased bladder capacity, one episode of DO (at 173 mL of filling) without leakage, and high compliance (Fig. 18.20); VLPP 92 and 126 cm H2O; patient could not void on PFS despite detrusor contraction (Fig. 18.21); good post-procedure UF with Q max = 20 mL/s, Q ave = 11 mL/s, and continuous, bell-shaped flow curve (Fig. 18.22).
Fig. 18.19 
Pre-CMG UF: adequate volume with low Q max; PVR low
Fig. 18.20 
CMG: mildly decreased bladder capacity; one episode of DO (173 mL of filling) without leakage; high compliance
Fig. 18.21 
CMG: VLPP = 92 and 126 cm H2O; patient could not void on PFS despite generating detrusor contraction
Fig. 18.22 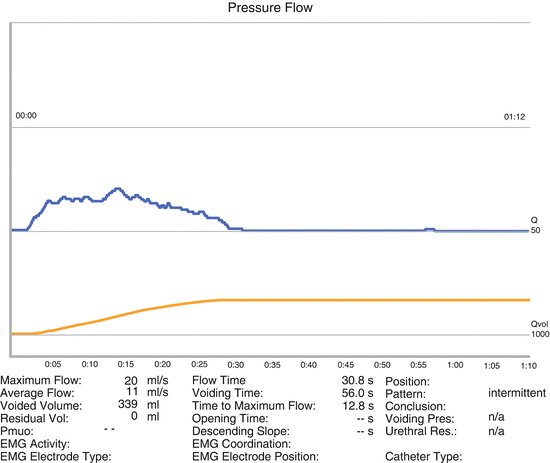
Post-CMG UF: good (Q max = 20 mL/s, Q ave = 11 mL/s) with continuous, bell-shaped flow curve
-
Diagnosis: SUI with high VLPP, DO, unobstructed emptying.
-
Options: Midurethral sling (MUS), pubovaginal sling (PVS), anticholinergics.
-
Commentary: This case represents a common scenario, where the whole is more than just the sum of the parts. If the initial uroflow and attempt at voiding on PFS are to be believed, then the patient may be thought to have some element of emptying dysfunction. However, the post-procedure uroflow (with a higher VV) provides some evidence to the contrary. The inability to void during a PFS may indicate some element of psychogenic inhibition (paruresis). Additionally, the patient appears to have tolerated a relatively modest amount of filling during the CMG indicating a potentially decreased bladder capacity. However, the VV on post-procedure uroflow was approximately twice the amount of infused volume, indicating that the patient may have produced a significant amount of urine during the study.




-
Case 7: 72 years of woman with Stage 2 cystocele and no overt SUI
-
History: (+) Positional emptying and often returning to commode 5 min later to complete voiding. No urinary incontinence. She underwent a previous hysterectomy without any concomitant procedures for incontinence or prolapse. There is no rectocele and minimal vault prolapse on pelvic exam (+). Urethral hypermobility. She is otherwise healthy.
-
Course: Voiding symptoms improved after pessary, but patient now complains of SUI. She had difficulty removing and reinserting several different pessaries and was interested in surgical intervention.
-
Urodynamics: Patient unable to perform pre-CMG UF, but PVR was low (30 mL) (Fig. 18.23); no DO, high compliance, and VLPP (with prolapse reduction) was 86 and 93 cm H2O at 306 mL of filling (Fig. 18.24); she had a small-volume void on PFS (92 mL) with a combination of detrusor contraction and valsalva (Fig. 18.25); good post-procedure UF with Q max = 20 mL/s, Q ave = 10 mL/s, and continuous, bell-shaped flow curve (Fig. 18.26).
Fig. 18.23 
Pre-CMG UF: patient unable to perform; PVR low (30 mL)
Fig. 18.24 
CMG: no DO; high compliance; VLPP (with prolapse reduction) = 86 and 93 cm H2O at 306 mL of filling
Fig. 18.25 
PFS: small-volume void (92 mL) with a combination of detrusor contraction and valsalva maneuver
Fig. 18.26 
Post-procedure UF: good (Q max = 20 mL/s, Q ave = 10 mL/s) with continuous, bell-shaped flow curve
-
Diagnosis: Cystocele with occult SUI.
-
Options: Pessary with anti-incontinence knob, PFMT, anterior colporrhaphy with MUS / PVS / bulking therapy.
-
Commentary: This is similar to Case 5 in that the voiding pattern becomes clearer on a post-procedure uroflow when there is a sufficient amount of urine in the bladder. The significant straining during PFS may be a response to the urethral catheter. Once again, the VV after PFS and uroflow significantly exceeds the filling volume.




-
Case 8: 30 years of woman with C7 spinal cord injury (SCI).
-
History: S/p automobile accident 1 year ago. Performs CIC every 4 h and leaks in between. She has an effective bowel protocol. On exam, there is skeletal spasticity, hyperreflexic deep tendon reflexes, and abnormal plantar response.
-
Course: She is currently on oxybutynin 15 mg twice/daily without significant benefit.
-
Urodynamics (Fig. 18.27): Stable detrusor until ~150 mL of filling; DO demonstrated with a peak detrusor pressure of 55 cm H2O; increased EMG activity at time of DO.
Fig. 18.27 
CMG: stable detrusor until ~150 mL of filling; DO with a peak P det = 55 cm H2O; increased EMG activity at time of DO
-
Cystography (Fig. 18.28): Narrowing at external sphincter at the time of unstable detrusor contraction.
Fig. 18.28 
Cystography: narrowing at external sphincter at the time of DO
-
Diagnosis: Small-bladder capacity, detrusor-external sphincter dyssynergia (DESD).
-
Options: Additional anticholinergics, intravesical onabotulinumtoxinA injection, bladder augmentation (with or without catheterizable channel), urinary diversion.
-
Commentary: DESD is caused when the coordinated voiding reflex between the bladder and external sphincter is disrupted. This finding is typically seen in patients with SCI or multiple sclerosis, but can also be seen in any lesion between the brainstem and sacral spinal cord (e.g., myelodysplasia or transverse myelitis). Symptomatically, people with DESD experience diurnal incontinence, urinary retention, and often have a history of UTIs. A build-up of pressures in the bladder can result in vesicoureteral reflux, UTIs, hydronephrosis, urinary tract calculi, and renal insufficiency. The goal of therapy for DESD is to decrease bladder storage pressures and facilitate bladder emptying. Since this patient is already performing CIC, the remaining goal is to eliminate DO to re-establish continence and potentially increase the interval between catheterizations. The bladder may be paralyzed pharmacologically or may be surgically converted to a low-pressure urinary reservoir by augmentation cystoplasty. Urinary diversion is typically reserved for patients failing less-complex measures and/or those unable to perform CIC. In men, additional options include an external sphincterotomy or urethral stent and an external urinary appliance (condom catheter). Without proper treatment over 50 % men with DESD develop serious urological complications within 5 years, while in women the complications are less common [9].


References
Bates CP, Whiteside CG, Turner WR. Synchronous urine pressure flow cystourethrography with special reference to stress and urge incontinence. Br J Urol. 1970;42:714–23.
Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, van Kerrebroeck P, Victor A, Wein A. Standardisation of terminology of lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21:167–78.
Huang AJ, Brown JS, Boyko EJ, Moore EE, Scholes D, Walter LC, Lin F, Vittinghoff E, Fihn SD. Clinical significance of postvoid residual volume in older ambulatory women. J Am Geriatr Soc. 2011;59:1452–8.
Lukacz ES, DuHamel E, Menefee SA, Luber KM. Elevated postvoid residual in women with pelvic floor disorders: prevalence and associated risk factors. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18:397–400.
Tseng LH, Liang CC, Chang YL, Lee SJ, Lloyd LK, Chen CK. Postvoid residual urine in women with stress incontinence. Neurourol Urodyn. 2008;27:48–51.
Tam CK, Wong KK, Yip WM. Prevalence of incomplete bladder emptying among elderly in convalescent wards: a pilot study. Asian J Gerontol Geriatr. 2006;1:66–71.
Kolman C, Girman CJ, Jacobsen SJ, Lieber MM. Distribution of post-void residual urine volume in randomly selected men. J Urol. 1999;161:122–7.
Kaplan SA, Wein AJ, Staskin DR, Roehrborn CG, Steers WD. Urinary retention and post-void residual urine in men: separating truth from tradition. J Urol. 2008;180:47–54.
Chancellor MB, Kaplan SA, Blaivas JG. Detrusor-external sphincter dyssynergia. Ciba Found Symp. 1990;151:195–206.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Gomelsky, A., Kaufman, M.R. (2015). Bladder Emptying: Complete Emptying. In: Rovner, E., Koski, M. (eds) Rapid and Practical Interpretation of Urodynamics. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1764-8_18
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1764-8_18
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1763-1
Online ISBN: 978-1-4939-1764-8
eBook Packages: MedicineMedicine (R0)