
Abstract
This chapter is focused on the discussion and review of benign and malignant liver lesions. The differential diagnosis of a liver mass is broad, including both benign and malignant tumor. The liver is also frequently involved by the metastasis in cancer patients; therefore, the FNA cytology plays a critical role in the work up of liver masses. Although most liver lesions can be accurately diagnosed by FNA, the limitation of the FNA cytology should also be considered. For example, the diagnosis of focal nodular hyperplasia (FNH), hepatic adenoma, and regenerative nodule may not be made based on cytomorphology. Nevertheless, the false-positive diagnosis is rare in daily practice.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Small Cell Carcinoma
- Giant Tumor Cell
- Focal Nodular Hyperplasia
- Metastatic Adenocarcinoma
- Hyperchromatic Nucleus
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
7.1 Image-Based Questions 1–38

Fig. 7.1
-
Q-1. A 65-year-old smoker with both lung and liver masses had a CT-guided fine-needle aspiration (FNA) of the liver lesion. What is the diagnosis of the liver FNA?
-
(a)
Lymphoma
-
(b)
Metastatic small cell carcinoma
-
(c)
Poorly differentiated adenocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.2
-
(a)
-
Q-2. All of the following features are seen in a fine-needle aspiration (FNA) of a poorly differentiated hepatocellular carcinoma (HCC), EXCEPT:
-
(a)
Numerous dispersed naked nuclei
-
(b)
Cords and/or individual polygonal cells
-
(c)
Fine and evenly distributed chromatin
-
(d)
Prominent nucleoli

Fig. 7.3
-
(a)
-
Q-3. A 67-year-old male presented with abdominal pain and discomfort. A CT scan revealed a submucosal mass in the stomach and multiple liver mass. Subsequently, a CT-guided FNA was performed. The differential diagnosis of the lesion includes all of the following, EXCEPT:
-
(a)
Gastrointestinal stromal tumor (GIST)
-
(b)
Sarcomatoid mesothelioma
-
(c)
Angiomyolipoma (AML)
-
(d)
Poorly differentiated adenocarcinoma

Fig. 7.4
-
(a)
-
Q-4. A patient who had a history of a “skin tumor” developed multiple liver masses. In FNA smears of the liver mass, scattered “atypical spindle cells” were identified. Which one of the following panels is most useful in confirmation of the diagnosis of this lesion?
-
(a)
S100, HMB45, and Melanin A
-
(b)
C-kit, CD34, and cytokeratin
-
(c)
CK5/6, p63, and p40
-
(d)
CK20, synaptophysin, and chromogranin

Fig. 7.5
-
(a)
-
Q-5. An 80-year-old male presented with abdominal pain, jaundice, hematuria, and liver masses. An ultrasound-guided FNA was performed. What is the diagnosis of this liver FNA?
-
(a)
Lymphoma
-
(b)
Metastatic urothelial cell carcinoma
-
(c)
Poorly differentiated adenocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.6
-
(a)
-
Q-6. A patient with history of kidney cancer developed multiple liver masses and a rapidly enlarging liver. CT-guided FNA of the liver mass was performed. What is the diagnosis of this liver FNA?
-
(a)
Metastatic renal cell carcinoma (RCC)
-
(b)
Metastatic urothelial cell carcinoma
-
(c)
Poorly differentiated adenocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.7
-
(a)
-
Q-7. A 34-year-old female with a history of “skin cancer” now develops lung and liver masses. What is the diagnosis of this liver FNA?
-
(a)
Metastatic melanoma
-
(b)
Metastatic urothelial cell carcinoma
-
(c)
Poorly differentiated adenocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.8
-
(a)
-
Q-8. A 56-year-old male presented with abdominal pain, jaundice, and liver masses. What is the diagnosis of this liver FNA?
-
(a)
Metastatic poorly differentiated adenocarcinoma
-
(b)
Metastatic melanoma
-
(c)
Hepatocellular carcinoma
-
(d)
Metastatic poorly differentiated squamous cell carcinoma

Fig. 7.9
-
(a)
-
Q-9. A 38-year-old healthy female developed abdominal pain and discomfort. A mass in right liver was found, and a subsequent ultrasound-guided liver mass FNA was performed. What is the diagnosis of this liver FNA?
-
(a)
Granulomatous hepatitis
-
(b)
Leiomyosarcoma
-
(c)
Hepatocellular carcinoma
-
(d)
Hemangioma

Fig. 7.10
-
(a)
-
Q-10. A 61-year-old male with clinical presentation of lung and liver masses had an ultrasound-guided FNA of the liver mass. What is the diagnosis of cells seen in this liver FNA?
-
(a)
Metastatic adenocarcinoma of the lung
-
(b)
Hepatocellular carcinoma
-
(c)
Metastatic renal cell carcinoma
-
(d)
Metastatic small cell carcinoma

Fig. 7.11
-
(a)
-
Q-11. A 40-year-old female with bilateral kidney lesions and multiple small liver cystic lesions developed severe abdominal pain and discomfort. Ultrasound-guided liver nodule FNA was performed. What is the diagnosis of this liver FNA?
-
(a)
Metastatic adenocarcinoma
-
(b)
Bile duct hamartoma
-
(c)
Hepatocellular carcinoma
-
(d)
Liver cell adenoma

Fig. 7.12
-
(a)
-
Q-12. A 52-year-old male presented with obstructive jaundice, urticaria, and an enlarged abdomen. A large cystic lesion was found in the liver by ultrasound. If the lesion is aspirated, which one of the following features can be seen, EXCEPT:
-
(a)
Numerous dispersed naked nuclei
-
(b)
Acellular debris
-
(c)
Fragments of the laminated membrane
-
(d)
Scolices and hooklets

Fig. 7.13
-
(a)
-
Q-13. A 52-year-old male presented with obstructive jaundice, urticaria, and enlarged abdomen. A large liver mass was found by ultrasound study. What is the diagnosis of this liver FNA?
-
(a)
Metastatic adenocarcinoma
-
(b)
Bile duct hamartoma
-
(c)
Well-differentiated hepatocellular carcinoma
-
(d)
Liver cell adenoma

Fig. 7.14
-
(a)
-
Q-14. A patient presented with diarrhea, abdominal pain, and liver masses. An ultrasound-guided FNA was performed. What is the diagnosis?
-
(a)
Metastatic poorly differentiated adenocarcinoma
-
(b)
Metastatic small cell carcinoma
-
(c)
Hepatocellular carcinoma
-
(d)
Metastatic carcinoid

Fig. 7.15
-
(a)
-
Q-15. A 70-year-old female with a history of breast cancer developed lymphadenopathy, fever, weight loss, and multiple liver masses. What is the diagnosis of this liver FNA?
-
(a)
Metastatic poorly differentiated adenocarcinoma
-
(b)
Metastatic small cell carcinoma
-
(c)
Hepatocellular carcinoma
-
(d)
Diffuse large B-cell lymphoma (DLBCL)

Fig. 7.16
-
(a)
-
Q-16. A 70-year-old female with a history of primary sclerosing cholangitis developed obstructive jaundice, weight loss, and multiple liver masses. Endoscopic ultrasound-guided FNA (EUS-FNA) was performed. What is the diagnosis of this liver FNA?
-
(a)
Bile duct hamartoma
-
(b)
Metastatic melanoma
-
(c)
Hepatocellular carcinoma
-
(d)
Cholangiocarcinoma

Fig. 7.17
-
(a)
-
Q-17. A 66-year-old male with malignant history developed multiple liver masses. What is the diagnosis of cells seen in this liver FNA specimen?
-
(a)
Metastatic adenocarcinoma of the lung
-
(b)
Metastatic adenocarcinoma of the prostate
-
(c)
Metastatic adenocarcinoma of the colon
-
(d)
Metastatic small cell carcinoma

Fig. 7.18
-
(a)
-
Q-18. A 69-year-old female presented with a right adnexal mass and liver masses. What is the diagnosis of cells seen in this liver FNA?
-
(a)
Metastatic papillary adenocarcinoma of the lung
-
(b)
Metastatic mucinous adenocarcinoma of the ovary
-
(c)
Metastatic adenocarcinoma of the colon
-
(d)
Metastatic small cell carcinoma

Fig. 7.19
-
(a)
-
Q-19. An immunocompromised patient develops jaundice, fever, and multiple liver masses. What is the diagnosis of this liver FNA?
-
(a)
Metastatic adenocarcinoma
-
(b)
Lymphoma
-
(c)
Actinomysis
-
(d)
Metastatic small cell carcinoma

Fig. 7.20
-
(a)
-
Q-20. What is the diagnosis of this liver mass?
-
(a)
Metastatic small cell carcinoma
-
(b)
Hepatocellular carcinoma
-
(c)
Metastatic carcinoid of the GI tract
-
(d)
Metastatic poorly differentiated adenocarcinoma

Fig. 7.21
-
(a)
-
Q-21. What is the diagnosis of this large liver mass from a patient who also has a 1.0 cm mass in the pancreas?
-
(a)
Metastatic small cell carcinoma
-
(b)
Hepatocellular carcinoma
-
(c)
Metastatic endocrine tumor
-
(d)
Metastatic poorly differentiated adenocarcinoma

Fig. 7.22
-
(a)
-
Q-22. What is the diagnosis of this liver FNA?
-
(a)
Metastatic melanoma
-
(b)
Normal liver cells
-
(c)
Poorly differentiated adenocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.23
-
(a)
-
Q-23. A 58-year-old has a history of a stomach tumor and now develops liver masses. What is the diagnosis of this liver FNA?
-
(a)
Metastatic melanoma
-
(b)
Normal liver cells
-
(c)
Metastatic adenocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.24
-
(a)
-
Q-24. What is the diagnosis of this large liver mass?
-
(a)
Normal liver cells
-
(b)
Hepatocellular carcinoma
-
(c)
Endocrine tumor
-
(d)
Metastatic poorly differentiated adenocarcinoma
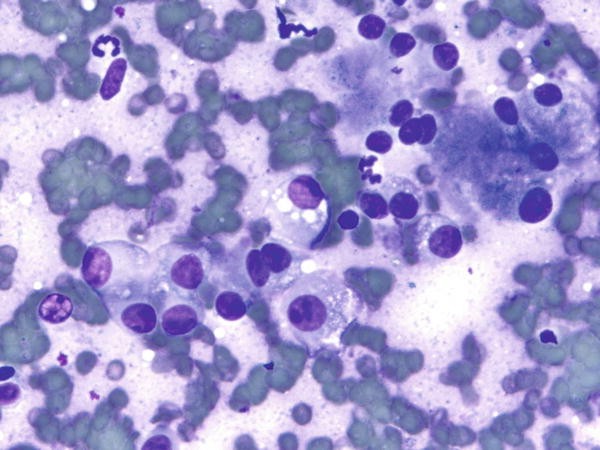
Fig. 7.25
-
(a)
-
Q-25. A 58-year-old male with a history of “skin cancer” now develops multiple liver masses. What is the diagnosis of this liver FNA?
-
(a)
Metastatic melanoma
-
(b)
Normal liver cells
-
(c)
Poorly differentiated adenocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.26
-
(a)
-
Q-26. A 68-year-old male with a history of alcohol abuse now develops multiple liver masses. What is the diagnosis of this liver FNA?
-
(a)
Metastatic melanoma
-
(b)
Normal liver cells
-
(c)
Poorly differentiated adenocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.27
-
(a)
-
Q-27. A 2-year-old boy with abdominal enlargement is found to have a large liver mass. What is the diagnosis of this liver FNA?
-
(a)
Metastatic small cell carcinoma
-
(b)
Normal liver cells
-
(c)
Hepatoblastoma
-
(d)
Hepatocellular carcinoma

Fig. 7.28
-
(a)
-
Q-28. A 9-year-old boy with kidney and liver masses had a liver mass FNA. What is the diagnosis of this liver FNA?
-
(a)
Metastatic small cell carcinoma
-
(b)
Normal liver cells
-
(c)
Hepatoblastoma
-
(d)
Metastatic Wilm’s tumor

Fig. 7.29
-
(a)
-
Q-29. A 22-year-old female who has a history of a “uterus tumor” develops a liver mass. What is the diagnosis of this liver FNA?
-
(a)
Fibrolamellar hepatocellular carcinoma
-
(b)
Well-differentiated hepatocellular carcinoma
-
(c)
Cholangiocarcinoma
-
(d)
Metastatic melanoma

Fig. 7.30
-
(a)
-
Q-30. A 30-year-old female who has a history of “uterus tumor” develops multiple liver masses. What is the diagnosis of this liver FNA?
-
(a)
Metastatic spindle cell carcinoma
-
(b)
Metastatic spindle cell melanoma
-
(c)
Hemangioma
-
(d)
Metastatic leiomyosarcoma

Fig. 7.31
-
(a)
-
Q-31. What is the diagnosis of this liver FNA?
-
(a)
Metastatic melanoma
-
(b)
Normal liver cells
-
(c)
Poorly differentiated adenocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.32
-
(a)
-
Q-32. A 40-year-old anemic patient develops liver enlargement. What is the diagnosis of this liver FNA?
-
(a)
Reed-Sternberg cells of Hodgkin lymphoma
-
(b)
Normal liver cells
-
(c)
Extramedullary hematopoiesis
-
(d)
Hepatocellular carcinoma

Fig. 7.33
-
(a)
-
Q-33. What is the diagnosis of this liver FNA?
-
(a)
Carcinoid
-
(b)
Normal liver cells
-
(c)
Benign bile duct epithelial cells
-
(d)
Hepatocellular carcinoma

Fig. 7.34
-
(a)
-
Q-34. What is the diagnosis of this liver FNA?
-
(a)
Carcinoid
-
(b)
Normal liver cells
-
(c)
Poorly differentiated hepatocellular carcinoma
-
(d)
Well-differentiated hepatocellular carcinoma

Fig. 7.35
-
(a)
-
Q-35. What is the diagnosis of this liver FNA from a 42-year-old female?
-
(a)
Liver cell adenoma
-
(b)
Focal nodular hyperplasia
-
(c)
Cholangiocarcinoma
-
(d)
Well-differentiated hepatocellular carcinoma

Fig. 7.36
-
(a)
-
Q-36. An 83-year-old has a history of a skin tumor and develops multiple liver masses. What is the diagnosis of this liver FNA?
-
(a)
Metastatic poorly differentiated adenocarcinoma
-
(b)
Metastatic squamous cell carcinoma
-
(c)
Poorly differentiated hepatocellular carcinoma
-
(d)
Well-differentiated hepatocellular carcinoma

Fig. 7.37
-
(a)
-
Q-37. What is the diagnosis of this liver FNA?
-
(a)
Carcinoid
-
(b)
Normal liver cells
-
(c)
Cholangiocarcinoma
-
(d)
Hepatocellular carcinoma

Fig. 7.38
-
(a)
-
Q-38. A liver FNA was performed on a patient with multiple liver masses. The diagnosis of metastatic adenocarcinoma was made. Which one is the most possible primary site of the tumor?
-
(a)
Breast
-
(b)
Lung
-
(c)
Colon
-
(d)
Renal
-
(a)





































7.2 Text-Based Questions 39–75
-
Q-39. All of the following features are seen in a fine-needle aspiration (FNA) containing benign hepatocytes, EXCEPT:
-
(a)
Numerous dispersed naked nuclei
-
(b)
Sheets of polygonal cells and individual hepatocytes
-
(c)
Centrally placed nuclei with binucleation
-
(d)
Prominent nucleoli
-
(a)
-
Q-40. Which statement about the liver cell adenoma is correct?
-
(a)
It is a benign tumor and has no risk to progress into malignancy
-
(b)
The tumor reveals clusters of pleomorphic cells and numerous naked nuclei
-
(c)
It commonly occurs in females under the age of 30 and is related to long-term use of oral contraceptives
-
(d)
Tumor necrosis is a common finding
-
(a)
-
Q-41. All of these cytological features are seen in cholangiocarcinomas, EXCEPT:
-
(a)
Nuclear enlargement and variation in size and shape
-
(b)
Trabeculae, cords, and nested arrangements
-
(c)
Large oval nuclei and coarse chromatin
-
(d)
Numerous naked nuclei
-
(a)
-
Q-42. Which statement regarding fatty change of the liver is correct?
-
(a)
Fatty change is reported in 40 % of early HCC
-
(b)
Fatty change is only observed in benign hepatocellular lesion
-
(c)
Prevalence of fatty change increases along with increase in tumor size
-
(d)
Fatty change is only observed in benign hepatocellular nodules
-
(a)
-
Q-43. All of the following cytological features of benign bile duct epithelial cells on a liver FNA specimen are correct, EXCEPT:
-
(a)
The size of bile duct epithelial cells is similar to normal hepatocytes
-
(b)
Bile duct epithelial cells have hyperchromatic nuclei
-
(c)
In benign ductal epithelial cells, nuclear overlapping and disarray are common
-
(d)
Benign bile duct epithelial cells have scant cytoplasm
-
(a)
-
Q-44. Which cytological feature is most useful in the separation of hepatocellular carcinoma (HCC) from cholangiocarcinoma:
-
(a)
The size of tumor cells, i.e., the tumor cell of HCC is bigger than that of cholangiocarcinoma.
-
(b)
Nuclear enlargement and variation in size and shape
-
(c)
Identification of bile and sinusoidal capillaries
-
(d)
Presence of prominent nucleoli
-
(a)
-
Q-45. All descriptions of cytological features of hepatic angiomyolipoma (AML) on a liver FNA specimen are correct, EXCEPT:
-
(a)
Presence of extramedullary hematopoiesis
-
(b)
Tumor consists of fat, epithelioid spindle cells (myoid cells), and an increased vascularity
-
(c)
Hepatic AML cannot be diagnosed accurately by FNA
-
(d)
Some of the tumor may have virtually no fat
-
(a)
-
Q-46. Which immuno panel is most useful in the separation of HCC from a cholangiocarcinoma?
-
(a)
Positive alpha-fetoprotein (AFP), negative CD10
-
(b)
Positive HepPar1, negative CD10
-
(c)
Positive HepPar1 and CD10, negative epithelial membrane antigen (EMA), monoclonal carcinoembryonic antigen (CEA), and CK7
-
(d)
Negative alpha-fetoprotein (AFP), negative CD10
-
(a)
-
Q-47. For the diagnosis of liver malignancy, ultrasound- and/or CT-guided percutaneous FNA have similar sensitivity and specificity as endoscopic ultrasound-guided FNA (EUS-FNA), true or false?
-
(a)
True
-
(b)
False
-
(a)
-
Q-48. Which risk factor is NOT significantly associated with cholangiocarcinoma?
-
(a)
Primary sclerosing cholangitis
-
(b)
Cirrhosis
-
(c)
Infection with the parasitic liver flukes Opisthorchis viverrini or Clonorchis sinensis
-
(d)
Exposure to thorotrast
-
(a)
-
Q-49. Which cytological feature is NOT seen in liver cell adenoma?
-
(a)
Spindle-shaped endothelial cells
-
(b)
Preserved reticulin scaffold
-
(c)
Prominent bile pigment
-
(d)
Benign bile duct epithelial cells
-
(a)
-
Q-50. All of the following features can be seen in a well-differentiated HCC, EXCEPT:
-
(a)
Preserved reticulin scaffold pattern
-
(b)
Dense cytoplasm
-
(c)
Prominent nucleoli
-
(d)
Shared cell borders
-
(a)
-
Q-51. A 65-year-old patient with cirrhosis developed a rapidly enlarged liver mass. On a liver FNA specimen, numerous clusters of liver cells with mild nuclear atypia are identified. Which one of the following tumors is most likely to be diagnosed?
-
(a)
Cholangiocarcinoma
-
(b)
Poorly differentiated hepatocellular carcinoma
-
(c)
Well-differentiated hepatocellular carcinoma
-
(d)
Small cell carcinoma
-
(a)
-
Q-52. A 60-year-old male patient presents with retroperitoneal lymphadenopathy and diffuse enlargement of the liver. An ultrasound-guided liver FNA was performed. On cytology smear and cell block section, numerous dyscohesive small to intermediate-sized cells with high N:C ratios, hyperchromatic coarse chromatin, and prominent nucleoli are identified. Rare scattered hepatocytes are also present. What is the likely diagnosis of the liver FNA?
-
(a)
Cholangiocarcinoma
-
(b)
Poorly differentiated hepatocellular carcinoma
-
(c)
Lymphoma
-
(d)
Small cell carcinoma
-
(a)
-
Q-53. A liver FNA was performed on a 60-year-old female smoker who presented with a right liver infiltration and right pleural effusion. On the cytological preparation, large sheets and tight clusters of atypical epithelioid cells are identified; some of them have “signet ring” cell features. What is the diagnosis of the liver FNA?
-
(a)
Metastatic adenocarcinoma of the colon
-
(b)
Metastatic adenocarcinoma of the lung
-
(c)
Cholangiocarcinoma
-
(d)
Well-differentiated hepatocellular carcinoma
-
(a)
-
Q-54. Immuno marker HepPar1 is positive for hepatocellular carcinoma and negative for cholangiocarcinoma, true or false?
-
(a)
True
-
(b)
False
-
(a)
-
Q-55. Which of the following cytological feature is most useful in the separation of a metastatic poorly differentiated adenocarcinoma from a metastatic small cell carcinoma in liver FNA specimen?
-
(a)
Prominent nucleoli
-
(b)
Fine or coarse chromatin pattern
-
(c)
Tumor necrosis
-
(d)
Organoid and/or rosettes arrangement of tumor cells
-
(a)
-
Q-56. A cytological smear of liver FNA reveals a bloody smear with numerous two-dimensional clusters and/or sheets of spindle cells, the differential diagnosis of the lesion includes all of the following, EXCEPT:
-
(a)
Cholangiocarcinoma
-
(b)
Hemangioma
-
(c)
Metastatic melanoma
-
(d)
Angiomyolipoma
-
(a)
-
Q-57. All of the following cytological features can be seen in metastatic prostate carcinoma, EXCEPT:
-
(a)
Microacini arrangement
-
(b)
Intermediate-sized tumor cells
-
(c)
Paranuclear blue bodies in the cytoplasm
-
(d)
Prominent nucleoli
-
(a)
-
Q-58. The cytological feature of fibrolamellar hepatocellular carcinoma includes all of them, EXCEPT:
-
(a)
Large polygonal tumor cells with abundant cytoplasm
-
(b)
Intermediate-sized tumor cells
-
(c)
Intracytoplasmic hyaline globules
-
(d)
Prominent nucleoli
-
(a)
-
Q-59. A liver FNA was performed on a patient with multiple liver masses. On the FNA preparation, it revealed three-dimensional clusters of tall columnar cells with hyperchromatic nuclei, coarse chromatin, prominent nucleoli, irregular nuclear membrane, and feathering cytoplasm. Tumor necrosis is also identified. Which one is the most possible primary site of the tumor?
-
(a)
Breast
-
(b)
Lung
-
(c)
Colon
-
(d)
Kidney
-
(a)
-
Q-60. A female patient with a breast mass developed liver masses. All of the following features can be seen in a metastatic breast carcinoma. EXCEPT:
-
(a)
Prominent nucleoli
-
(b)
Intracytoplasmic lumina (Magenta body)
-
(c)
Three-dimensional cell clusters
-
(d)
Naked nuclei
-
(a)
-
Q-61. All of the following features can be seen in a well-differentiated HCC, EXCEPT:
-
(a)
Preserved reticulin scaffold pattern
-
(b)
Dense cytoplasm
-
(c)
Prominent nucleoli
-
(d)
Shared cell borders
-
(a)
-
Q-62. Cytological features of a metastatic carcinoid tumor may include all of the following, EXCEPT:
-
(a)
Fine chromatin pattern (so-called “salt-and-pepper” pattern)
-
(b)
Inconspicuous or small nucleoli
-
(c)
Scant cytoplasm
-
(d)
Nuclear grooves
-
(a)
-
Q-63. Which of the following cytological features is helpful in the differential diagnosis of a metastatic carcinoid tumor from cholangiocarcinoma in a liver FNA specimen?
-
(a)
Fine chromatin pattern
-
(b)
Three-dimensional and/or pseudoacinar arrangements of tumor cells
-
(c)
Lacy cytoplasm with vacuolization
-
(d)
Dispersed tumor cells with marked atypia and enlargement
-
(a)
-
Q-64. A liver FNA specimen characteristic of a metastatic small cell carcinoma includes all of the following, EXCEPT:
-
(a)
Hyperchromatic nuclei and prominent nucleoli
-
(b)
Scant cytoplasm
-
(c)
Three-dimensional cell clusters with nuclear molding
-
(d)
Individual tumor cells with fine chromatin
-
(a)
-
Q-65. In a FNA specimen, cells reveal “pseudointranuclear inclusions” and mild cytological atypia. All of the following lesions/tumors can have this cytological feature, EXCEPT:
-
(a)
Focal nodular hyperplasia
-
(b)
Liver cell adenoma
-
(c)
Cholangiocarcinoma
-
(d)
Hepatocellular carcinoma
-
(a)
-
Q-66. In a FNA specimen, atypical cells reveal “clear cytoplasm.” All of the following lesions/tumors can have this cytological feature, EXCEPT:
-
(a)
Focal nodular hyperplasia
-
(b)
Renal cell carcinoma
-
(c)
Cholangiocarcinoma
-
(d)
Hepatocellular carcinoma
-
(a)
-
Q-67. In a FNA specimen, which one of the following features is indicative of a well-differentiated hepatocellular carcinoma (HCC)?
-
(a)
Numerous large clusters of cells
-
(b)
Lacunae spaces on cell block preparation
-
(c)
Presence of a “second population” of cells
-
(d)
Sinusoidal capillaries surrounding the markedly thickened trabeculae of neoplastic cells
-
(a)
-
Q-68. In a FNA specimen, which one of the following features is best seen in a bile duct hamartoma but not in a metastatic adenocarcinoma?
-
(a)
Sheets or loosely formed clusters of columnar cells
-
(b)
Benign-appearing hepatocytes
-
(c)
Presence of a “second population” of cells
-
(d)
Three-dimensional, dark colored cellular clusters
-
(a)
-
Q-69. Which of the feature is NOT seen in a metastatic squamous cell carcinoma in a liver FNA specimen?
-
(a)
Large nuclei with smudgy chromatin
-
(b)
Nuclei with variation in size and shape
-
(c)
Pyknotic nuclei
-
(d)
Cytokeratin formation
-
(a)
-
Q-70. A HIV positive patient developed a diffusely enlarged liver and peripheral lymphadenopathy. Which one of the following lymphomas is associated with c-myc gene rearrangement and shows no evidence of HHV-8 infection?
-
(a)
Burkitt’s or Burkitt’s-like lymphoma (BL)
-
(b)
Diffuse large B-cell lymphoma (DLBCL)
-
(c)
Peripheral T-cell non-Hodgkin lymphoma (NHL)
-
(d)
Primary effusion lymphoma (PEL)
-
(a)
-
Q-71. In a FNA specimen, which one of the following features favors the diagnosis of diffuse large B-cell lymphoma (DLBCL) over a metastatic poorly differentiated adenocarcinoma?
-
(a)
Numerous large clusters of cells
-
(b)
Dispersed individual large atypical cells
-
(c)
Presence of a “second population” of cells on the slides
-
(d)
Pseudointranuclear inclusions
-
(a)
-
Q-72. Which of the following features favors the diagnosis of a metastatic melanoma over the diagnosis of a hepatocellular carcinoma (HCC) in a liver FNA specimen?
-
(a)
Large nuclei with prominent nucleoli
-
(b)
Binucleation with “mirror” image
-
(c)
Variation of nuclear size
-
(d)
Predominantly isolated large cells with “cherry red” nuclei
-
(a)
-
Q-73. Which statement regarding cholangiocarcinoma is NOT correct?
-
(a)
Cholangiocarcinoma is virtually indistinguishable from a metastatic adenocarcinoma
-
(b)
Cholangiocarcinoma is always seen in a cirrhotic liver
-
(c)
Tumor cells have large oval nuclei and coarse chromatin
-
(d)
Crowded sheets and clusters of tumor cells
-
(a)
-
Q-74. The most notable features of hepatocellular carcinoma (HCC) include all of the following, EXCEPT:
-
(a)
Polygonal large cells with centrally placed nuclei
-
(b)
Dense cytoplasm and distinct cell border
-
(c)
Large oval nuclei and coarse chromatin
-
(d)
Numerous naked nuclei
-
(a)
-
Q-75. Which statement regarding the benign hepatocyte is correct?
-
(a)
Numerous dispersed naked nuclei
-
(b)
Clusters of polygonal cells and individual hepatocytes with hyperchromatic nuclei
-
(c)
Centrally placed nuclei with binucleation
-
(d)
Marked variation of size of nuclei
-
(a)
7.3 Answers and Discussion of Image-Based Questions 1–38
-
A-1. (b) Metastatic small cell carcinoma
The diagnosis is metastatic small cell carcinoma of the lung. In small cell carcinomas, tumor cells are relatively small, and they are two- to threefold the size of mature lymphocytes; however, in small cell carcinoma large cell variant, the size of tumor cells can be much larger. Tumor cells show a high N:C ratio, have large nuclei with fine chromatin (salt-and-pepper) pattern, nuclear crowding and molding, and paranuclear blue bodies in the cytoplasm. The prominent nucleolus is not usually seen in a small cell carcinoma. The nucleoli are inconspicuous in small cell carcinomas. In some cases, tumor cells may reveal rare nucleoli, but they are small in size. The background of the smear may also reveal “blue strips” (indicative of breakdown nuclear material). In poorly differentiated adenocarcinomas, tumor cells are larger in size with hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm; the tumor also reveals acinar and three-dimensional arrangement. In lymphoma, tumor cells have a high N:C ratio with coarse chromatin and nucleoli, without nuclear molding and crowding. In hepatocellular carcinoma (HCC), tumor cells form cords, tubules, sheets, or isolated individual cells. Tumor cells with hyperchromatic nuclei, coarse chromatin, large prominent nucleoli, intranuclear pseudoinclusion, and cytoplasmic bile/lipofuscin pigments are characteristics seen in HCC. Numerous naked nuclei are also seen in HCC, particularly in poorly differentiated tumor.
-
A-2. (c) Fine and evenly distributed chromatin
In HCC, tumor cells arrange in cords, clusters, tubules, or dispersed individual cells. Tumor cells reveal hyperchromatic nuclei, coarse chromatin, large prominent “cherry-red” nucleoli and intranuclear pseudoinclusions. Dense cytoplasm with cytoplasmic bile/lipofuscin pigments is also characteristic of HCC. Numerous naked nuclei and tumor necrosis are also seen in HCC. In a poorly differentiated HCC, tumor cell pleomorphism and giant tumor cells are also present. Fine and evenly distributed chromatin are features seen in benign hepatocytes rather than HCC. In benign hepatocytes, cells are usually arranged in sheets or isolated cells.
-
A-3. (d) Poorly differentiated adenocarcinoma
The diagnosis of the lesion is a metastatic gastrointestinal stromal tumor (GIST). The cytological features of GIST include sheets or loosely formed clusters of spindle cells with oval or bipolar nuclei, bland chromatin, inconspicuous nucleoli, and vesicular cytoplasm. IHC of tumor cells are positive for c-kit and CD34. The differential diagnosis of a spindle cell lesion in liver FNA cytology is broad, including virtually all tumors with spindle cell morphology such as spindle cell carcinoma, sarcomatoid mesothelioma, melanoma, angiomyolipoma, and others. Therefore, the correlation of cytological features with clinical and image findings is extremely important and may help to narrow down the differential diagnosis. In a poorly differentiated adenocarcinoma, tumor cells form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm. In AML, cytological features include clusters of epithelioid and spindle cells, fat cells, blood vessels, and extramedullary hematopoiesis. In sarcomatoid mesothelioma, tumor cells have an epithelioid appearance with hyperchromatic oval nuclei, prominent nucleoli, and dense cytoplasm.
-
A-4. (a) S100, HMB45, and Melanin A
The diagnosis is metastatic desmoplastic/spindle melanoma. Tumor cells reveal oval or bizarre nuclei, prominent nucleoli, and no cytoplasmic melanin pigment. Immuno markers S100, HMB45, and MelanA/Mart1 are helpful in the confirmation of the diagnosis. S100 stains the nuclei and cytoplasm with 90 % sensitive but is not specific. HMB45 stains cytoplasm; it is more specific but less sensitive than S100 (only 0–20 % positive in desmoplastic/spindle cell melanoma). MelanA/Mart1 stains cytoplasm and is negative in desmoplastic/spindle cell melanoma. IHC markers of C-kit, CD34, and cytokeratin are for GIST. CK5/6, p63, and p40 are for squamous cell carcinoma. CK20, synaptophysin and chromogranin are for Merkel cell carcinoma.
-
A-5. (b) Metastatic urothelial cell carcinoma
The diagnosis is metastatic urothelial cell carcinoma. The smears reveal clusters and dispersed large malignant epithelial cells with dense cytoplasm. Tumor cells show high N:C ratios, hyperchromatic nuclei with coarse (chunk of charcoal) chromatin, irregular nuclear membrane, and round esosinophilic cytoplasmic inclusions (Melamed-Wolinska body). Melamed-Wolinska bodies are commonly seen in degenerated urothelial cells, particularly in voided urine. The pathogenesis of these bodies is still not fully understood, and they can be found in both benign and malignant conditions. The finding of Melamed-Wolinska bodies is nonspecific; however, when seen in an extraurinary cytological specimen, the finding may suggest that the lesion is of urothelial origin. The main differential diagnosis of metastatic urothelial cell carcinoma is HCC, since both tumors reveal dense cytoplasm and cytoplasmic material. In HCC, tumor cells have large prominent nucleoli and cytoplasmic bile and/or lipofuscin pigments, which stain golden and brown color with Papanicolaou method. Numerous naked nuclei are also seen in HCC.
-
A-6. (a) Metastatic renal cell carcinoma (RCC)
The diagnosis is metastatic clear cell RCC. In RCC, the most common sites of metastasis are the lung, liver, lymph nodes, and bones. Tumor cells of clear cell RCC arrange in clusters or dispersed individual cells, reveal round to ovoid hyperchromatic nuclei, irregular nuclear membrane, with or without prominent nucleoli, and clear cytoplasm. Focally, tumor cells may also show large, hyperchromatic nuclei with multinucleated giant cells, eosinophilic cytoplasm, and associated areas of necrosis, particularly in Fuhrman Grade III and IV tumors. The background of the smear is bloody with prominent small vessels (hypervascularity).
-
A-7. (a) Metastatic melanoma
In metastatic melanoma, tumor cells are usually arranged in loose clusters or dispersed individual cells. Nuclei of tumor cells are eccentrically located (plasmacytoid appearance) and highly variable in size with finely to coarsely granular chromatin and a single prominent cherry-red nucleoli. The cytoplasm tends to be abundant and may or may not contain melanin pigment. The N/C ratio may not be high. Melanin pigment appears coarsely granular and dark brown on Papanicolaou stain. Other characteristic features include multinucleation, binucleation, and intranuclear inclusions. The main differential diagnosis is hepatocellular carcinoma. In HCC, tumor cells also have large prominent nucleoli and dense cytoplasm which contains cytoplasmic bile and/or lipofuscin pigments, staining golden and brown in color with the Papanicolaou method. Numerous naked nuclei are also seen in HCC.
-
A-8. (c) Hepatocellular carcinoma
The diagnosis is hepatocellular carcinoma. In HCC, tumor cells arrange in cords, clusters, or dispersed individual cells with centrally located nuclei, large prominent nucleoli, and dense cytoplasm containing cytoplasmic bile and/or lipofuscin pigments, and are golden and brown in color with Papanicolaou staining. Numerous naked nuclei are also seen in HCC. In a poorly differentiated tumor, numerous pleomorphic individual cells with hyperchromatic nuclei, prominent nucleoli, and dense granular cytoplasm are characteristic. In adenocarcinomas, tumor cells form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm.
-
A-9. (d) Hemangioma
The diagnosis is hemangioma. On FNA specimen, several cytological features can be seen, including bloody smear, aggregates of closely packed, thin-walled capillaries with spindle cell clusters, scant benign liver cells, stromal cells, and hemosiderin-laden macrophages. The causes of this liver tumor are not clear. About 30 % of cases have the lesion at the time of birth (indicative of a congenital defect). Studies also show that the development of hemangioma is related to hormonal imbalance, since the usage of steroids and oral contraceptives can exacerbate the growth of the tumor in the liver. The tumor is more commonly seen in the right lobe of the liver than the left. The differential diagnosis includes spindle cell lesions of the liver, such as granulomatous hepatitis, leiomyosarcoma, melanoma, spindle cell carcinoma, and others. Glut1 is an immunohistochemical marker, highly specific for hemangioma, and can be used to differentiate hemangioma from vascular malformations.
-
A-10. (a) Metastatic adenocarcinoma of the lung
The diagnosis is a metastatic adenocarcinoma of the lung. Metastatic adenocarcinoma may have several cytological appearances. In adenocarcinomas, particularly well-differentiated adenocarcinomas, tumor cells form acinar/papillary arrangements or three-dimensional clusters. Tumor cells are intermediate or large in size and reveal hyperchromatic nuclei with coarse chromatin, prominent nucleoli, and vacuolated or clear cytoplasm. Small cell carcinoma has fine (salt-and-pepper) chromatin, nuclear crowding, and molding. Renal cell carcinoma reveals a bloody smear. Tumor cells have hyperchromatic nuclei with coarse chromatin, with or without prominent nucleoli, and clear/eosinophilic cytoplasm. In HCC, tumor cells arrange in cords, clusters, or dispersed individual cells with centrally located nuclei, large prominent nucleoli, and dense cytoplasm containing cytoplasmic bile and/or lipofuscin pigments. Numerous naked nuclei are also seen in HCC.
-
A-11. (b) Bile duct hamartoma
The diagnosis is bile duct hamartoma characterized by multiple small nodules dispersed throughout the liver. The FNA reveals bland-appearing columnar cells haphazardly arranged in tubules, sheets and two-dimensional clusters, scattered stromal cells, and benign-appearing hepatocytes. Bile duct hamartoma, also known as von Meyenburg complex, Meyenburg complex, and biliary hamartoma, is a benign tumor-like malformation of the liver and classically associated with polycystic liver disease, may be seen in polycystic kidney disease and Caroli’s disease. In adenocarcinomas, tumor cells form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm. Liver cell adenoma is a benign tumor related to long-term use of oral contraceptives. It is commonly seen in females under the age of 30 and the lesion reveals benign liver cells.
-
A-12. (a) Numerous dispersed naked nuclei
The diagnosis is hydatid cyst (echinococcal cyst). The hydatid cyst is caused by infection with the larval stage of the cestode (or tapeworm) Echinococcus spp. Transmission is from eggs found in feces of dogs which are accidentally swallowed, usually by children. Larvae develop over many years to form fluid-filled cysts in various organs, particularly the liver. Cysts can grow to considerable size and contain a large amount of fluid and infectious scolices. The cysts have a wall made from both host tissue (pericyst) and larval origin (endocyst). All above cytological features can be seen in the lesion, except numerous dispersed naked nuclei of liver cells, which is the feature seen in HCC.
-
A-13. (c) Well-differentiated hepatocellular carcinoma
The diagnosis is a well-differentiated HCC. In HCC, tumor cells arrange in cords, clusters, tubules, or dispersed individual cells. Tumor cells reveal hyperchromatic nuclei, coarse chromatin, large prominent nucleoli, and intranuclear pseudoinclusion. Dense cytoplasm with cytoplasmic bile/lipofuscin pigments is also characteristic of HCC. Numerous naked nuclei and tumor necrosis are also seen in HCC. In a poorly differentiated HCC, tumor cell pleomorphism and giant tumor cells are also present. In bile duct hamartoma, the FNA reveals bland-appearing columnar cells haphazardly arranged in tubules, sheets and two-dimensional clusters, scattered stromal cells, and benign-appearing liver cells. In adenocarcinomas, tumor cells form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm. Liver cell adenoma reveals benign-appearing liver cells.
-
A-14. (d) Metastatic carcinoid
The diagnosis is a metastatic carcinoid of GI tract. Carcinoids are the most common gastrointestinal endocrine tumors and frequently involve the liver. Primary hepatic carcinoids are extremely rare. In FNA specimens, tumor cells reveal acini and/or rosette arrangements and consist of intermediate-sized cells with fine (salt-and-pepper) chromatin with inconspicuous or small nucleoli. Mitoses are rare (low ki67 labeling). In small cell carcinoma, nuclear crowding and molding, and tumor necrosis are characteristic. In HCC, tumor cells reveal hyperchromatic nuclei, coarse chromatin, large prominent nucleoli, and intranuclear pseudoinclusion. Numerous naked nuclei and tumor necrosis are also seen in HCC. In adenocarcinomas, tumor cells form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm.
-
A-15. (d) Diffuse large B-cell lymphoma (DLBCL)
DLBCL is a biological and clinical diverse group of diseases. The FNA reveals a cellular specimen with dyscohesive large atypical lymphoid cells. Three morphological variants are most commonly seen: centroblastic, immunoblastic, and anaplastic variant. Centroblastic variant is the most common subtype and reveals medium-to-large-sized tumor cells with high N:C ratios, oval or round nuclei, fine chromatin, and single or multiple prominent nucleoli. Immunoblasts have a basophilic cytoplasm and a central nucleolus. Most cases are polymorphic, with a mixture of centroblastic and immunoblastic cells. The third morphologic variant, anaplastic variant, consists of large tumor cells with pleomorphic nuclei and may resemble Hodgkin cells or Reed-Sternberg cells. In small cell carcinoma, nuclear crowding and molding, and tumor necrosis are characteristic. In HCC, tumor cells reveal hyperchromatic nuclei, coarse chromatin, large prominent nucleoli, and intranuclear pseudoinclusion. Numerous naked nuclei and tumor necrosis are also seen in HCC. In adenocarcinomas, tumor cells form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm.
-
A-16. (d) Cholangiocarcinoma
Cholangiocarcinoma can affect any area of the bile ducts, either within or outside the liver. The FNA cytomorphology of the tumor reveals clusters, sheets, or dispersed individual tumor cells with hyperchromatic and variable sized nuclei, coarse chromatin, and prominent nucleoli. The FNA of bile duct hamartoma reveals bland-appearing columnar cells haphazardly arranged in tubules, sheets and two-dimensional clusters, and benign-appearing hepatocytes. In HCC, tumor cells reveal hyperchromatic nuclei, coarse chromatin, large prominent nucleoli, and intranuclear pseudoinclusion. Numerous naked nuclei and tumor necrosis are also seen in HCC. In adenocarcinomas, tumor cells form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm.
-
A-17. (b) Metastatic adenocarcinoma of the prostate
In metastatic prostate adenocarcinoma, tumor cells form microacinar arrangements or three-dimensional small clusters. Tumor cells are small to intermediate in size, with hyperchromatic nuclei, coarse granular chromatin, prominent nucleoli, and vacuolated or clear cytoplasm. Small cell carcinoma has fine (salt-and-pepper) chromatin, nuclear crowding, and molding. In lung adenocarcinoma, tumor cells have a more pleomorphic appearance with large nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm. In colonic adenocarcinoma, tumor cells reveal large elongated nuclei (pencil-shaped nuclei), coarse chromatin, prominent nucleoli, and marked tumor necrosis. Immunostains with prostate markers such as PSA (prostate specific antigen), PSAP (prostate specific acid phosphatase), prostate specific membrane antigen, and NKX3 are positive for metastatic tumor cells.
-
A-18. (b) Metastatic mucinous adenocarcinoma of the ovary
Cytological features of mucinous adenocarcinomas include three-dimensional clusters and acinar groups of tumor cells with large round or oval shape nuclei, coarse chromatin, irregular nuclear membrane, and prominent nucleoli. The cytoplasm of tumor cells is vacuolated (indicative of mucin production). Mucinous material can be seen in the background of smears and cell block preparation. In true papillary adenocarcinoma of the lung, numerous papillary structures can be identified. A metastatic colonic adenocarcinoma has hyperchromatic pencil-shaped nuclei and tumor necrosis. Small cell carcinoma has fine (salt-and-pepper) chromatin, nuclear crowding, and molding.
-
A-19. (c) Actinomysis
Actinomysis is caused by systemic dissemination of Actinomyces israelii species. The characteristic feature of the smear is the presence of sulfur granules and filamentous bacteria. Sulfur granule forms in the center of purulence surrounded by neutrophils and filamentous bacteria. Sulfur granules look yellow on gross examination and stain blue to purple in color. Actinomyces bacteria stain blue with the Papanicolaou method and purple with the Diff-Quik method. They appear as large blue- or purple-colored “cotton balls” on the slide. Clinically, actinomysis is frequently confused with neoplasms due to the formation of mass lesions. However, no malignant features are identified in liver cells.
-
A-20. (c) Metastatic carcinoid of the GI tract
In FNA specimen, the tumor reveals acini and/or rosette arrangements or dispersed individual cells. The tumor consists of intermediate sized cells with fine (salt-and-pepper) chromatin, inconspicuous or small nucleoli. Mitoses are rare (low ki67 labeling). Carcinoids are the most common gastrointestinal endocrine tumors and frequently involve the liver. Primary hepatic carcinoids are extremely rare. In small cell carcinoma, nuclear crowding and molding, and tumor necrosis are characteristic. In HCC, tumor cells reveal hyperchromatic nuclei, coarse chromatin, large prominent nucleoli, and intranuclear pseudoinclusion. Numerous naked nuclei and tumor necrosis are also seen in HCC. In adenocarcinomas, tumor cells form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm.
-
A-21. (c) Metastatic endocrine tumor
The diagnosis is metastatic endocrine tumor of the pancreas (pancreatic endocrine tumor, PEN). In FNA specimens, the smear is cellular and reveals sheets and clusters of tumor cells with acini and/or rosette arrangements or dispersed individual cells. Tumor cells are small to intermediate in size with round to oval nuclei, fine (salt-and-pepper) chromatin, and inconspicuous nucleoli. PENs occur most commonly in adults. The liver is often involved, even if the primary tumor is only 1–2 cm. The majority of tumors are functional tumors and secrete a variety of hormones, such as insulin, glucagon, somatostatin, vasoactive intestinal polypeptide (VIP), pancreatic polypeptide, serotonin, adrenocorticotropic hormone (ACTH), or calcitonin. The tumor also stains positive for amyloid.
-
A-22. (b) Normal liver cells
This liver FNA reveals normal hepatocytes. A FNA of benign liver may reveal several patterns, including clusters, sheets of cells, or dispersed individual cells. The normal liver cells have centrally placed round- to oval-shaped nuclei, granular chromatin, inconspicuous or small nucleoli, and no hyperchromasia or marked nuclear atypia. Cells also reveal normal N:C ratios. Binucleation is common in cells. Bile and lipofusion pigment can be identified in the cytoplasm. In contrast, in hepatocellular carcinoma (HCC), tumor cells form cords, tubules, sheets, or isolated individual cells. Tumor cells have hyperchromatic nuclei, coarse chromatin, and high N:C ratios. Large prominent nucleoli, marked variation of size of nuclei, and numerous naked nuclei are features seen in HCC.
-
A-23. (c) Metastatic adenocarcinoma
The diagnosis is a metastatic adenocarcinoma of the stomach. In metastatic adenocarcinoma, particularly metastasis from stomach, tumor cells form large three-dimensional clusters. Tumor cells are intermediate or large in size and reveal hyperchromatic nuclei with coarse chromatin, prominent nucleoli, and vacuolated cytoplasm. In melanoma, tumor cells are predominantly dispersed as individual cells with large eccentric hyperchromatic nuclei, coarse chromatin, large prominent nucleoli, and cytoplasmic pigment. In HCC, tumor cells arrange in cords, clusters, or dispersed individual cells with centrally located nuclei, large prominent nucleoli, and dense cytoplasm containing cytoplasmic bile and/or lipofuscin pigments. Numerous naked nuclei are also seen in HCC.
-
A-24. (c) Endocrine tumor
In FNA specimens, the smear reveals sheets and clusters of tumor cells with acini and/or rosette arrangements or dispersed individual cells. Tumor cells are small to intermediate in size with round to oval nuclei, fine (salt-and-pepper) chromatin, and inconspicuous nucleoli. Almost all endocrine tumors of the liver are metastatic tumors either from the GI tract, pancreas, lung, and other organs. A primary endocrine tumor of the liver is extremely rare.
-
A-25. (a) Metastatic melanoma
In metastic melanoma, tumor cells are usually arranged in loose clusters or dispersed individual cells. Nuclei of tumor cells are eccentrically located (plasmacytoid appearance) and highly variable in size with finely to coarsely granular chromatin and a single prominent cherry-red nucleoli. The cytoplasm tends to be abundant and may or may not contain melanin pigment. The N/C ratio may not be high due to abundant cytoplasm. Melanin pigment appears coarsely granular and dark brown on Papanicolaou stain. Other characteristic features include multinucleation, binucleation, and intranuclear inclusions. The main differential diagnosis is hepatocellular carcinoma. In HCC, tumor cells also have large prominent nucleoli and dense cytoplasm which contains cytoplasmic bile and/or lipofuscin pigments, staining golden and brown color with the Papanicolaou method. Numerous naked nuclei are also seen in HCC.
-
A-26. (b) Normal liver cells
This liver FNA reveals normal hepatocytes. A FNA of benign liver reveals sheets of cells and dispersed individual cells. The normal liver cells have centrally placed round- to oval-shaped nuclei, granular chromatin, inconspicuous or small nucleoli, and no hyperchromasia or marked nuclear atypia. Cells also reveal normal N:C ratio. Binucleation is common in cells. Bile and lipofusion pigment can be identified in cytoplasm. In contrast, in hepatocellular carcinoma (HCC), tumor cells form cords, tubules, sheets, or isolated individual cells. Tumor cells have hyperchromatic nuclei, coarse chromatin, and high N:C ratios. Large prominent nucleoli, marked variation of size of nuclei, and numerous naked nuclei are features seen in HCC. The finding of benign liver cells may be seen in cirrhosis, liver cell adenomas, focal nodular hyperplasia, nodular regenerative hyperplasia, and others. In this case the FNA findings may be suggestive of cirrhosis and/or nodular regenerative hyperplasia in a cirrhotic liver.
-
A-27. (c) Hepatoblastoma
The diagnosis is hepatoblastoma of embryonal cell type. Hepatoblastoma is a rare tumor of infancy and childhood. In FNA specimens, findings vary and depend on the cell type of the tumor. In embryonal variant, the tumor reveals a primitive and undifferentiated appearance with hyperchromatic nuclei and scant cytoplasm, and form rosettes and trabeculae. In anaplastic variant, tumor cells reveal a more pleomorphic appearance. In fetal cell variant, tumor cells resemble normal liver cells. The main differential diagnosis of the tumor is hepatocellular carcinoma and other metastatic small round blue cell tumors. The positive stain of HePar1 supports the diagnosis of liver primary rather than a nonhepatic origin. Hepatoblastoma is positive for high molecular weight cytokeratin, whereas HCC is negative for high molecular weight cytokeratin. Both tumors are positive for low molecular weight cytokeratin.
-
A-28. (d) Metastatic Wilm’s tumor
Wilm’s tumor is a rare tumor of infancy and childhood. The tumor is bimodal with a mixture of epithelial and mesenchymal component. Occasionally it is triphasic. Generally, in the FNA specimen, numerous dyscohesive small round blue cells are found. Tumor epithelial cells form characteristic tubular-like structure and tight clusters. Tumor cells have hyperchromatic nuclei and scant cytoplasm. The mesenchymal cells are elongated. The main differential diagnosis is rhabdomyosarcoma and PNET. In rhabdomyosarcoma, tumor cells have more eosinophilic cytoplasm. In PNET, tumor cells are more pleomorphic and reveal a tigroid appearance.
-
A-29. (a) Fibrolamellar hepatocellular carcinoma
The fibrolamellar variant of hepatocellular carcinoma is usually seen in young patients under the age of 30. It has a favorable prognosis. The cytomorphological features of fibrolamellar hepatocellular carcinoma reveal large polygonal tumor cells separated by fibrous tissue. The size of tumor cells is much larger than well-differentiated HCC. Tumor cells have large nuclei and abundant eosinophilic cytoplasm; therefore, the N:C ratio of tumor cells is normal to slightly increased. Tumor cells also reveal prominent nucleoli and intracytoplasmic hyaline globules. The dense lamellar material is also seen in the slides, separating loosely cohesive tumor cells.
-
A-30. (d) Metastatic leiomyosarcoma
The FNA of the lesion reveals clusters of spindle cells with cigar-shaped hyperchromatic nuclei, coarse chromatin, inconspicuous nucleoli, and fibrillar cytoplasm. Tumor necrosis is also present. In desmoplastic/spindle melanoma, tumor cells reveal oval or bizarre nuclei, prominent nucleoli, and do not contain cytoplasmic melanin pigment. In spindle cell carcinoma, tumor cells reveal elongated or bizarre nuclei, prominent nucleoli, and scant cytoplasm. In hemangioma, several cytological features can be seen, including bloody smear, aggregates of closely packed, thin-walled capillaries with spindle cell clusters, scant benign liver cells, and hemosiderin-laden macrophages. Immunostains with muscle markers are helpful in the differential diagnosis of the tumor.
-
A-31. (b) Normal liver cells
This liver FNA reveals normal hepatocytes. A FNA of benign liver reveals sheets of cells and dispersed individual cells. The normal liver cells have centrally placed round- to oval-shaped nuclei, granular chromatin, inconspicuous or small nucleoli, and no hyperchromasia or marked nuclear atypia. Cells also reveal normal N:C ratios. Binucleation is common in cells. Bile and lipofusion pigment can be identified in cytoplasm. In contrast, in hepatocellular carcinoma (HCC), tumor cells form cords, tubules, sheets, or isolated individual cells. Tumor cells have hyperchromatic nuclei, coarse chromatin, and high N:C ratio. Large prominent nucleoli, marked variation in the size of nuclei, and numerous naked nuclei are features seen in HCC. The finding of benign liver cells may be seen in cirrhosis, liver cell adenomas, focal nodular hyperplasia, nodular regenerative hyperplasia, and others.
-
A-32. (c) Extramedullary hematopoiesis
The diagnosis of this liver FNA is an extramedullary hematopoiesis. It can be caused by myelofibrosis and commonly involves the liver and spleen. The FNA cytology reveals numerous megakaryocytes, nucleated red blood cells, and different stages of nuclear cells. However, no malignant features are seen in the aspirate, excluding the diagnosis of carcinoma. The megakaryocytes are much larger than the Reed-Sternberg cells seen in the Hodgkin’s lymphoma and have 3–5 lobes. In addition, other features of Hodgkin’s lymphoma are absent in this specimen.
-
A-33. (c) Benign bile duct epithelial cells
Benign bile duct epithelium appears as small clusters and/or sheets of cohesive uniform cells. These cells have round to ovoid nuclei, dark granular chromatin, inconspicuous or occasional small nucleoli, and scant cytoplasm. The size of benign bile duct epithelial cells is smaller than that of normal hepatocytes. Nuclear overlapping and nuclear disarray are common findings, mimicking adenocarcinoma. In adenocarcinomas, particularly metastatic adenocarcinomas, tumor cells reveal high N:C ratios, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm.
-
A-34. (c) Poorly differentiated hepatocellular carcinoma
The diagnosis is a poorly differentiated hepatocellular carcinoma. In HCC, tumor cells show a wide range of cytomorphology. In poorly differentiated forms, malignant cells are polygonal and dyscohesive with pleomorphic nuclei and giant tumor cells. In well-differentiated forms, tumor cells resemble normal hepatocytes and form trabeculae, cords, and nests with slightly increased N:C ratios, large round nuclei, prominent nucleoli, naked nuclei, and bile pigment in the cytoplasm. The most notable feature of HCC, particularly in well-differentiated tumors, is the identification of sinusoidal capillaries surrounding markedly thickened trabeculae of neoplastic cells. This feature is not seen in cholangiocarcinoma or other tumors.
-
A-35. (b) Focal nodular hyperplasia
The diagnosis is focal nodular hyperplasia. The FNA specimen reveals clusters or dispersed individual benign-appearing hepatocytes with mild nuclear atypia. Cells have abundant granular cytoplasm and normal N:C ratios. Bile ductular epithelial cells are also identified. However, in liver cell adenomas, the bile duct epithelial cells are absent. In a well-differentiated hepatocellular carcinoma, tumor cells resemble normal hepatocytes and form trabeculae, cords, and nests with slightly increased N:C ratios, large round nuclei, prominent nucleoli, naked nuclei, and bile pigment in the cytoplasm. The most notable feature of HCC, particularly in well-differentiated tumors, is the identification of sinusoidal capillaries surrounding markedly thickened trabeculae of neoplastic cells.
-
A-36. (b) Metastatic squamous cell carcinoma
The diagnosis is a metastatic squamous cell carcinoma. Metastatic squamous cell carcinoma usually form loose clusters or dispersed individual tumor cells. The cytological features of tumor cells include large nuclei with smudgy chromatin, nuclei with variation in size and shape, and dense cytoplasm (indicative of cytokeratin formation). The dense cytoplasm is blue in color with the Diff-Quik stain and red-pink (eosinophilic) in color with the Papanicolaou stain. Finally, prominent nucleoli can be seen in poorly differentiated squamous cell carcinomas and should not be confused with poorly differentiated adenocarcinomas. Tumor cells of adenocarcinoma have vesicular nuclei, coarse chromatin, and vacuolated cytoplasm.
-
A-37. (d) Hepatocellular carcinoma
The diagnosis is hepatocellular carcinoma (moderately differentiated). In HCC, tumor cells show a wide range of cytomorphology. In poorly differentiated forms, malignant cells are polygonal and dyscohesive with pleomorphic nuclei and giant tumor cells. In well-differentiated forms, tumor cells resemble normal hepatocytes and form trabeculae, cords, and nests with slightly increased N:C ratios, large round nuclei, prominent nucleoli, naked nuclei, and bile pigment in the cytoplasm. The most notable feature of HCC, particularly in well-differentiated tumors, is the identification of sinusoidal capillaries surrounding markedly thickened trabeculae of neoplastic cells. This feature is not seen in cholangiocarcinoma or other tumors.
-
A-38. (c) Colon
A metastatic colonic adenocarcinoma has unique cytological features. Tumor cells show a tall columnar “picket fence” appearance, hyperchromatic pencil-shaped nuclei, coarse chromatin, and prominent nucleoli. The presence of “dirty” necrosis is also seen. In breast carcinomas, tumor cells form tight three-dimensional “cannon ball” clusters. The size of tumor cells is smaller than that of colon adenocarcinoma. They may have intranuclear inclusion. Renal cell carcinoma usually reveals a centrally located nuclei and clear cytoplasm. Lung adenocarcinoma may have a variety of morphological features. The finding of tall columnar cells favors a colonic primary rather than lung primary. IHC stain of TTF, Napsin A, CK7, CK20, and CDX2 may aid the differential diagnosis in difficult cases. TTF, Napsin A, and CK7 are positive in lung adenocarcinoma, whereas CK20 and CDX2 are positive in colon adenocarcinoma.
7.4 Answers and Discussions of Text-based Questions 39–75
-
A-39. (a) Numerous dispersed naked nuclei
A FNA of benign liver reveals sheets of large polygonal and dispersed individual cells. The specimen may also reveal trabeculae arrangements and tissue fragments. Cells have centrally placed round- to oval-shaped nuclei with variation in size, granular chromatin, prominent nucleoli, and normal N:C ratio. Binucleation is common in cells. Bile and lipofusion pigment can be identified in the cytoplasm. Bile stains dark-green by Papanicolaou and Diff-Quik methods, whereas lipofusion stains golden-brown by Papanicolaou and green-brown by Diff-Quik methods. In contrast, in hepatocellular carcinoma (HCC), tumor cells form cords, tubules, sheets, or isolated individual cells. Tumor cells have hyperchromatic nuclei, coarse chromatin, and high N:C ratios. Large prominent nucleoli as well as naked nuclei in the smear are features seen in HCC.
-
A-40. (c) It commonly occurs in females under the age of 30 and is related to long-term use of oral contraceptives
The liver cell adenoma is an uncommon benign tumor. It commonly occurs in female under the age of 30 and is related to long-term use of oral contraceptives. Cytologically, the FNA specimen reveals clusters or dispersed individual benign-appearing hepatocytes with mild nuclear atypia. Cells have abundant granular cytoplasm and a normal N:C ratio. No bile duct epithelial cells are present. It is important to distinguish liver cell adenoma from other benign liver tumors, such as hemangiomas (spindle cell lesion, mixed with benign liver cells) and focal nodular hyperplasia (presence of bile duct epithelial cells), because liver cell adenomas have a risk of progressing into a malignancy. When the adenoma grows to a size of more than 6–8 cm, it is considered high risk of developing into an invasive hepatocellular carcinoma. Tumor necrosis, pleomorphic tumor cells, and numerous naked nuclei are features characteristic of hepatocellular carcinoma. The cytological diagnosis of liver cell adenomas can be aided by reticulin stains. In liver cell adenomas, the reticulin scaffold is preserved and hepatocytes do not form layers of more than three cells thick, as is seen in hepatocellular carcinomas.
-
A-41. (d) Numerous naked nuclei
Cholangiocarcinoma is known to have the histological and molecular features of adenocarcinoma. Cholangiocarcinoma can affect any area of the bile ducts, either within or outside the liver. The cytomorphology of the tumor includes trabeculae, cords, and nested arrangements, or dispersed individual tumor cells with large oval nuclei and coarse chromatin with scant cytoplasm. The presence of numerous naked nuclei is the feature most commonly seen in HCC. The differential diagnosis of cholangiocarcinoma includes HCC, metastatic adenocarcinomas, and other gastrointestinal tumors.
-
A-42. (a) Fatty change is reported in 40 % of early HCC
Fatty change can occur in both benign and malignant liver lesions, as well as all sizes and grades of HCC. It has been reported that fatty change can be identified in 40 % of early HCC. It is also interesting that the prevalence of fatty change decreases along with the increase in tumor size. Fatty change is best appreciated by a Diff-Quik stain as intracytoplasmic vacuoles or as dispersed bubbles in the background of the slide. In a well-differentiated HCC, the finding of tumor cells with prominent fatty change should not be confused as a benign process or benign nodule.
-
A-43. (a) The size of bile duct epithelial cells is similar to normal hepatocytes
Benign bile duct epithelium appears as small clusters and/or sheets of cohesive uniform cells. These cells have round to ovoid nuclei, dark granular chromatin, inconspicuous or occasional small nucleoli, and scant cytoplasm. The size of benign bile duct epithelial cells is smaller than that of normal hepatocytes. Nuclear overlapping and nuclear disarray are common findings, mimicking adenocarcinoma. In adenocarcinomas, particular metastatic adenocarcinomas, tumor cells reveal high N:C ratios, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm.
-
A-44. (c) Identification of bile and sinusoidal capillary
In HCC, tumor cells show a wide range of cytomorphology. In well-differentiated forms, tumor cells resemble normal hepatocytes and form trabeculae, cords, and nests with a slightly increased N:C ratio, large round nuclei, prominent nucleoli, naked nuclei, and bile pigment in cytoplasm. In poorly differentiated forms, malignant cells are polygonal and dyscohesive with pleomorphic nuclei and giant tumor cells. The most notable feature of HCC, particularly in well-differentiated tumors, is the identification of sinusoidal capillaries surrounding markedly thickened trabeculae of neoplastic cells. This feature is not seen in cholangiocarcinoma. Other features in the question are seen in both HCC and cholangiocarcinoma.
-
A-45. (c) Hepatic AML cannot be diagnosed accurately by FNA
Hepatic AML shares many clinical and cytological features with its renal counterpart. Similar to kidney tumor, it consists of fat, epithelioid spindle cells (myoid cells) with an increased vascularity and frequent extramedullary hematopoiesis. The correct diagnosis depends on the identification of the triad of fat, vessels, and myoid component. The proportions of these components vary considerably from tumor to tumor. Some tumors are composed predominantly of fat, whereas others have virtually no fat and are almost exclusively myoid cells (smooth muscle). In difficult cases, immunohistochemical (IHC) staining with HMB45 is helpful and positive for the neoplastic cells.
-
A-46. (c) Positive HepPar1 and CD10, negative epithelial membrane antigen (EMA), monoclonal carcinoembryonic antigen (CEA), and CK7
For HCC, the panel should include Hep Par 1, CD10, and CAM5.2 or CK8/18. For cholangiocarcinoma, the panel should include poly- or monoclonal carcinoembryonic antigen (CEA), CK7, and CD15. pCEA (and CD10) demonstrate a canalicular staining pattern in HCC but a cytoplasmic pattern in cholangiocarcinoma. The demonstration of AFP positivity points toward a malignant tumor of hepatocellular origin, however, it is also positive in nonseminomatous germ cell tumors and extrahepatic AFP-producing carcinomas. Cautious use of Hep Par1 antibody in a panel with other positive (alpha-fetoprotein, CD10, polyclonal carcinoembryonic antigen) and negative (epithelial membrane antigen, monoclonal carcinoembryonic antigen, CD15) markers of hepatocellular differentiation may aid in the accurate diagnosis of HCC.
-
A-47. (a) True
The sensitivity and specificity of percutaneous FNA biopsy for detection of liver malignancy have been reported to be around 90 % (range, 67–100 %) and 100 %, respectively. A variety of factors may affect the sensitivity, such as the size and location of the lesion, number of FNA passes, operator’s skill and experience, quality of smears, and cytopathologist’s expertise. The positive and negative predictive values and overall accuracy of percutaneous FNA biopsy for liver malignancy were reported in one large study to be 100, 59.1, and 92.4 %. Endoscopic ultrasound-guided FNA (EUS-FNA) is the latest diagnostic and staging tool with a sensitivity of 82–94 % and specificity of 90–100 %. The procedure is safe and accurate, but highly operator dependent. Furthermore, EUS-FNA can access the left lobe of liver, hilum, proximal right lobe, gallbladder, extrahepatic biliary system, and perihilar lymph nodes. It is especially useful for small and deep-seated left lobe lesions, which cannot be easily accessed by percutaneous FNA.
-
A-48. (b) Cirrhosis
Known risk factors for cholangiocarcinoma include primary sclerosing cholangitis, congenital liver malformations, infection with the parasitic liver flukes Opisthorchis viverrini or Clonorchis sinensis, and exposure to thorotrast (thorium dioxide), a chemical formerly used in medical imaging. However, most patients with cholangiocarcinoma have no identifiable specific risk factors. Cirrhosis has not been found to associate with cholangiocarcinoma, although it is a significant risk factor for HCC.
-
A-49. (d) Benign bile duct epithelial cells
In liver cell adenomas, the FNA specimen reveals clusters or dispersed individual benign-appearing hepatocytes with mild nuclear atypia. Cells have abundant granular cytoplasm and normal N:C ratio. However, bile ductular epithelial cells are not identified. The cytological diagnosis of liver cell adenomas can be aided by reticulin stains. In liver cell adenomas, the reticulin scaffold is preserved and hepatocytes do not form layers of more than three cells thick, as is seen in hepatocellular carcinoma. It is important to distinguish liver cell adenomas from other benign liver tumors, such as hemangiomas (spindle cell lesion, mixed with benign liver cells) and focal nodular hyperplasia (presence of bile duct epithelial cells), because liver cell adenomas have a risk of progressing into a malignancy.
-
A-50. (a) Preserved reticulin scaffold pattern
In a well-differentiated HCC, tumor cells resemble normal hepatocytes and form trabeculae, cords, and nests with a slightly increased N:C ratio, have large round nuclei with prominent nucleoli, and may contain prominent bile pigment in cytoplasm. Naked nuclei can also be present. In poorly differentiated tumors, malignant cells are polygonal and dyscohesive with pleomorphic nuclei and giant tumor cells. The most notable feature in HCC, particularly in well-differentiated tumors, is the loss of reticulin scaffold pattern and the presence of sinusoidal capillaries surrounding the markedly thickened trabeculae of neoplastic cells. This feature is best seen on cell block preparations.
-
A-51. (c) Well-differentiated hepatocellular carcinoma
Cirrhotic liver is a well-known risk factor for the development of HCC. In this liver FNA, the most important differential diagnosis is a well-differentiated HCC. In HCC, tumor cells show a wide range of cytomorphology. In well-differentiated forms, tumor cells resemble normal hepatocytes and form trabeculae, cords, and nests and have an increased N:C ratio, large round nuclei, prominent nucleoli, naked nuclei, and bile pigment in cytoplasm. In poorly differentiated forms, malignant cells are markedly polygonal and dyscohesive with pleomorphic nuclei and giant tumor cells. The most notable feature of HCC, particularly in well-differentiated tumors, is the identification of sinusoidal capillaries surrounding the markedly thickened trabeculae of neoplastic cells. This feature is not seen in cholangiocarcinoma. In addition, mild nuclear atypia of hepatocytes can be seen in nodular regenerative hyperplasia of cirrhosis; however, the patient’s clinical presentation of “rapidly enlarged liver mass” precludes the diagnosis.
-
A-52. (c) Lymphoma
The most likely diagnosis of this liver FNA is lymphoma. The cytological features of numerous dyscohesive small- to intermediate-sized cells with high N:C ratios and hyperchromatic coarse chromatin are characteristic of lymphoma. The monomorphic appearance of the lesion represents a monoclonal proliferation of lymphoma cells. Other cytological features of lymphoma include hyperchromatic nuclei with clumped (soccer-ball-like) chromatin, irregular nuclear membrane, and scant basophilic cytoplasm. Lymphoglandular bodies can also be seen in the background. In cholangiocarcinoma, tumor cells form clusters with large nuclei, hyperchromatic nuclei, and prominent nucleoli. In HCC, tumor cells are large with centrally located nuclei and large nucleoli, dense cytoplasm, and numerous naked nuclei. In small cell carcinomas, tumor cells reveal fine (salt-and-pepper) chromatin with nuclear crowding and molding.
-
A-53. (b) Metastatic Adenocarcinoma of the lung
The differential diagnosis of carcinoma with “signet ring” cells features is broad, including breast, lung, stomach, and other carcinomas. In metastatic adenocarcinomas of the lung, tumor cells form three-dimensional clusters with hyperchromatic nuclei, prominent nucleoli, and vacuolated cytoplasm. In metastatic adenocarcinoma of colon, tumor cell reveals elongated nuclei and prominent tumor necrosis. Cholangiocarcinoma has many overlapping cytological features with metastatic adenocarcinomas, and it is difficult to separate the tumor from metastatic adenocarcinoma based on morphology alone. The immunostains of TTF1 and Napsin A may help in the differential diagnosis of lung adenocarcinoma from other carcinomas. In a metastatic lung adenocarcinoma, TTF1 and Napsin A are usually positive.
-
A-54. (b) False
Hep Par 1 (hepatocyte Paraffin 1) antibody (clone OCH1E5.2.10) was developed in 1993 by Wennerberg et al. and it stains normal and neoplastic hepatocytes. Several studies have reported this antibody to be a sensitive marker for HCC (80–90 %). However, recent studies also found that it also frequently stains gastric carcinomas (30–47 %). It is not, however, entirely specific, showing frequent staining in gastric carcinomas. Several other tumors also stain occasionally, including yolk sac tumors as well as carcinomas of the adrenal cortex, lung, colon, and ovary. It also stains cholangiocarcinoma (50 %). In addition, poorly differentiated HCCs are more likely to be negative for Hep Par 1 than are better differentiated cases.
-
A-55. (a) Prominent nucleoli
The presence of prominent nucleoli is not a feature seen in small cell carcinoma. All other features can be seen in both adenocarcinoma and small cell carcinoma. In adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, vesicular or coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indication of mucin production). In small cell carcinoma, tumor cells reveal acini/rosettes arrangements with hyperchromatic nuclei, fine (salt-and-pepper) chromatin, inconspicuous nucleoli, and scant cytoplasm. In addition, in small cell carcinoma, nuclear crowding and molding are common features. Tumor necrosis can be seen in both adenocarcinoma and small cells carcinoma.
-
A-56. (a) Cholangiocarcinoma
The differential diagnosis of spindle cells lesion is broad, including all of tumors in the question except cholangiocarcinoma. In hemangiomas, several cytological features can be seen, including bloody smear, aggregates of closely packed, thin-walled capillaries with spindle cell clusters, scant benign liver cells, and hemosiderin-laden macrophages. In cholangiocarcinomas, tumor cells resemble adenocarcinoma and form clusters with large nuclei, hyperchromatic nuclei, and prominent nucleoli. In angiomyolipoma, the tumor reveals fat, spindle myoid cells, blood vessels, and extramedullary hematopoiesis. Glut1 is an immunohistochemical marker, highly specific for hemangioma and can be used to differentiate hemangioma from vascular malformations.
-
A-57. (c) Paranuclear blue bodies in the cytoplasm
In metastatic prostate carcinoma, tumor cells are intermediate in size and reveal microacini arrangement or small three-dimensional clusters. Tumor cells show high N:C ratios, large nuclei with fine chromatin, small prominent nucleoli, and vesicular cytoplasm. Paranuclear blue bodies in the cytoplasm are features seen in small cell carcinoma. Some prostate carcinomas may have neuroendocrine differentiation and reveal salt-and-pepper chromatin pattern. Immunostains of prostate markers such as PSA (prostate specific antigen), PSAP (prostate specific acid phosphatase), prostate specific membrane antigen, and NKX3 are positive for metastatic tumor cells.
-
A-58. (b) Intermediate-sized tumor cells
The cytomorphological features of fibrolamellar hepatocellular carcinoma reveal large polygonal tumor cells separated by fibrous tissue. The size of tumor cells is much larger than well-differentiated HCC. Tumor cells have large nuclei and abundant eosinophilic cytoplasm; therefore, the N:C ratio of tumor cells is normal to slightly increased. Tumor cells also reveal prominent nucleoli and intracytoplasmic hyaline globules. The fibrolamellar variant of hepatocellular carcinoma is usually seen in young patient under the age of 30. It has a favorable prognosis.
-
A-59. (c) Colon
A metastatic colonic adenocarcinoma has these classic cytological features. Tumor cells show a tall columnar “picket fence” appearance, hyperchromatic pencil-shaped nuclei, coarse chromatin, and prominent nucleoli. The presence of “dirty” necrosis is usually not as apparent as seen in histological sections. In breast carcinomas, tumor cells form tight three-dimensional “cannon ball” clusters. The size of tumor cells is smaller than that of colon adenocarcinoma; they may have intranuclear inclusions. Renal cell carcinoma usually reveals a centrally located nuclei and clear cytoplasm. Lung adenocarcinoma may have a variety of morphological features. The finding of tall columnar cells favors a colonic primary rather than the lung primary. IHC stain of TTF, Napsin A, CK7, CK20, and CDX2 may aid to the differential diagnosis in difficult cases. TTF, Napsin A, and CK7 are positive in lung adenocarcinoma, whereas CK20 and CDX2 are positive in colon adenocarcinomas.
-
A-60. (d) Naked nuclei
The presence of naked nuclei is not a feature seen in metastatic breast carcinoma. In a metastatic breast carcinoma, tumor cells form tight three-dimensional clusters. The size of tumor cells is relatively smaller than that of metastatic adenocarcinoma from the lung and/or GI tract. The presence of intracytoplasmic lumina, so-called Magenta body, is also one of the characteristics of metastatic breast carcinoma. Magenta bodies are variably sized red-to-purple perinuclear inclusions seen by Diff-Quik stains. The prominent nucleoli are a common cytological feature seen in a variety of adenocarcinomas. Naked nuclei can be seen in metastatic melanoma and hepatocellular carcinoma.
-
A-61. (a) Preserved reticulin scaffold pattern
In a well-differentiated HCC, tumor cells resemble normal hepatocytes and form trabeculae, cords, and nests with a slightly increased N:C ratio and have large round nuclei with prominent nucleoli, naked nuclei, and may contain prominent bile pigment in the cytoplasm. In poorly differentiated tumors, malignant cells are polygonal and dyscohesive with pleomorphic nuclei and giant tumor cells. The most notable feature in HCC, particularly in well-differentiated tumors, is the loss of reticulin scaffold pattern and the presence of sinusoidal capillaries surrounding the markedly thickened trabeculae of neoplastic cells. This feature is best seen on cell block preparations.
-
A-62. (d) Nuclear grooves
Metastatic carcinoids in the liver most often come from a primary tumor in the intestine, pancreas, or the lungs. Carcinoids, despite differing embryological origin, have common phenotypic characteristics. The cytological features of carcinoids are characterized by acini arrangements, small clusters, and dispersed individual tumor cells. Tumor cells reveal a fine chromatin (salt-and-pepper chromatin) pattern, inconspicuous or small nucleoli, and scant cytoplasm. Mitoses are extremely rare. Nuclear grooves are not features seen in carcinoid. In addition, the cellular proliferative rate (Ki67 labeling) should be performed in tumors, since it has been considered as a useful marker for the classification of the tumor. An increased labeling pattern may indicate an adverse prognosis.
-
A-63. (d) Dispersed tumor cells with marked atypia and enlargement
As discussed in A-24, the cytological features of carcinoid are characterized by small acini/pseudorosette arrangements, small clusters, and/or dispersed individual tumor cells. Tumor cells reveal a fine chromatin (salt-and-pepper chromatin) pattern, inconspicuous or small nucleoli, and scant cytoplasm; mitoses are extremely rare. Whereas, cholangiocarcinoma form two- or three-dimensional clusters, crowded sheets, or dispersed large typical cells. Tumor cells have coarse granular rather than fine chromatin, and lacy or vacuolated cytoplasm. In difficult cases, diagnosis of carcinoid versus a cholangiocarcinoma depends on IHC staining with neuroendocrine markers. Carcinoid tumors are positive for synaptophysin, chromogranin, and CD56.
-
A-64. (a) Hyperchromatic nuclei and prominent nucleoli
The presence of prominent nucleoli is not a feature seen in small cell carcinomas. All other features can be seen in small cell carcinoma. In small cell carcinoma, tumor cells form three-dimensional clusters or dispersed individual cells, reveal hyperchromatic nuclei with fine (salt-and-pepper) chromatin, and scant cytoplasm. In addition, nuclear crowding, molding, apoptotic bodies, and mitotic figures are common features. The background of the smear may also reveal “blue strips” (indicative of breakdown nuclear material). Tumor necrosis is also a feature commonly seen in metastatic small cell carcinomas.
-
A-65. (c) Cholangiocarcinoma
“Pseudointranuclear inclusions” have been found in normal hepatocyte, benign and malignant liver lesions. A mild cytological atypia can also be found in both benign and malignant liver lesions. Pseudointranuclear inclusions and mild cytological atypia are not features seen in cholangiocarcinoma. In cholangiocarcinoma, tumor cells form two- or three-dimensional clusters, crowded sheets, or dispersed large typical cells. They have large hyperchromatic nuclei with coarse chromatin, prominent nucleoli, scant cytoplasm, high N:C ratios, and lacy or vacuolated cytoplasm.
-
A-66. (c) Cholangiocarcinoma
The cytological finding of clear cytoplasm can be seen in a variety of tumors, such as mucin producing adenocarcinoma, renal cell carcinoma, hepatocellular carcinoma, and steroid/lipid producing tumors. This feature is not seen in cholangiocarcinoma. The cytological features of renal cell carcinoma (clear cell renal cell carcinoma) include loosely cohesive clusters and/or scattered individual tumor cells. They have slightly enlarged round nuclei with or without nucleoli depending on the Fuhrman grade of the tumor. The background of smears can be bloody with vascular structures, best seen on cell block preparations. In hepatocellular carcinoma, particularly in poorly differentiated forms, 10 % of tumors may have prominent clear cytoplasm.
-
A-67. (d) Sinusoidal capillaries surrounding the markedly thickened trabeculae of neoplastic cells.
In HCC, tumor cells show a wide range of cytomorphology. In well-differentiated forms, tumor cells resemble normal hepatocytes and form trabeculae, cords, and nests and have a slightly increased N:C ratio, large round nuclei, prominent nucleoli, naked nuclei, and bile pigment in the cytoplasm. In poorly differentiated forms, malignant cells are markedly polygonal and dyscohesive with pleomorphic nuclei and giant tumor cells. The most notable feature of HCC, particularly in well-differentiated tumors, is the identification of sinusoidal capillaries surrounding the markedly thickened trabeculae of neoplastic cells. This feature is not seen in benign liver lesions or cholangiocarcinoma. The presence of lacunae spaces on a cell block preparation is the feature seen in adenocarcinomas.
-
A-68. (a) Sheets or loosely formed clusters of columnar cells
Bile duct hamartoma (also known as von Meyenburg complex, Meyenburg complex, and biliary hamartoma) is a benign tumor-like malformation of the liver. It is classically associated with polycystic liver disease and may be seen in polycystic kidney disease and Caroli’s disease. The bile duct hamartoma is characterized by multiple small nodules dispersed throughout the liver. The FNA reveals bland-appearing columnar cells haphazardly arranged in tubules, sheets and two-dimensional clusters, scattered stromal cells, and benign-appearing hepatocytes. In adenocarcinomas, tumor cells form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm.
-
A-69. (c) Pyknotic nuclei
Metastatic squamous cell carcinomas usually form loose clusters and dispersed individual tumor cells. The cytological features of tumor cells include large nuclei with smudgy chromatin, nuclei with variation in size and shape, dense cytoplasm (indicative of cytokeratin formation). The dense cytoplasm is blue in color with a Diff-Quik stain and red-pink (eosinophilic) color with Papanicolaou stain. Pyknotic nuclei are usually seen in reactive and/or benign squamous cells. Finally, prominent nucleoli can be seen in poorly differentiated squamous cell carcinomas and should not be confused with poorly differentiated adenocarcinomas. Tumor cells of adenocarcinoma have vesicular nuclei, coarse chromatin, and vacuolated cytoplasm.
-
A-70. (a) Burkitt’s or Burkitt’s-like lymphoma (BL)
The most common types of AIDS-related non-Hodgkin lymphoma (ARL) include Burkitt’s or Burkitt’s-like lymphoma (BL), diffuse large B-cell lymphoma (DLBCL) (including the subtypes of immunoblastic and centroblastic lymphoma), plasmablastic lymphoma (including oral cavity involved and multicentric Castleman’s disease [MCD] associated), and primary effusion lymphoma (PEL). Among them, BL tumor cells are positive for the characteristic c-myc gene rearrangement and show no evidence of HHV-8 infection. Peripheral T-cell NHLs can usually be distinguished by routine immunohistochemistry for T-cell markers or T-cell receptor (TCR) gene rearrangement studies. Both DLBCL and PEL can have similar cytomorphology. In DLBCL, tumor cells are positive for Epstein-Barr virus, but negative for HHV-8. In PEL, tumor cells are negative for Epstein-Barr virus, but positive for HHV-8.
-
A-71. (b) Dispersed individual large atypical cells
DLBLC is a good mimic of carcinoma. In DLBCL, the FNA reveals a cellular specimen with dyscohesive large atypical lymphoid cells. Tree morphological variants are most commonly seen: centroblastic, immunoblastic, and anaplastic variant. Centroblastic variant is the most common subtype and reveals medium-to-large-sized tumor cells with high N:C ratios, oval or round nuclei, fine chromatin, and single or multiple prominent nucleoli. Immunoblasts have a basophilic cytoplasm and a central nucleolus. Most cases are polymorphic, with a mixture of centroblastic and immunoblastic cells. The third morphologic variant, anaplastic variant, consists of large tumor cells with pleomorphic nuclei, and may resemble Hodgkin cells or Reed-Sternberg cells. In a poorly differentiated adenocarcinoma, tumor cells can be dyscohesive and presented as dispersed individual cells or form three-dimensional clusters with large hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm. In difficult cases, IHC stains for lymphoma and adenocarcinoma markers are necessary for an accurate diagnosis.
-
A-72. (d) Predominantly isolated large cells with “cherry red” nuclei
The cytological differential diagnosis of a metastatic melanoma and HCC can be difficult. The cytological features of a metastatic melanoma include: individual large cells with prominent large nucleoli, intranuclear inclusion, cytoplasmic melanin pigment, binucleation, and the presence of plasmacytoid cells. In HCC, tumor cells form loose clusters or dispersed individual cells and reveal hyperchromatic nuclei, coarse chromatin, large prominent nucleoli, and intranuclear pseudoinclusion. Numerous naked nuclei and tumor necrosis are also seen in HCC. The predominant dyscohesive arrangement of tumor cells favors the diagnosis of a metastatic melanoma. In difficult cases, IHC stains of HMB45 and Melanin A may help.
-
A-73. (b) Cholangiocarcinoma is always seen in a cirrhotic liver
Cholangiocarcinoma is known to have the histological and molecular features of adenocarcinoma. Cirrhotic liver is not a significant risk factor for developing cholangiocarcinoma. The cytomorphology of the tumor includes trabeculae, cords, crowded sheets and nests arrangements, or dispersed individual tumor cells with large oval nuclei and coarse chromatin, and scant cytoplasm. The differential diagnosis of cholangiocarcinoma includes HCC, metastatic adenocarcinoma, and other gastrointestinal tumors.
-
A-74. (b) Dense cytoplasm and distinct cell border
In hepatocellular carcinoma, tumor cells form cords, tubules, sheets, or isolated individual cells. Tumor cells have hyperchromatic nuclei, coarse chromatin, and high N:C ratio. Large prominent nucleoli, marked variation of size of nuclei, and numerous naked nuclei are also features seen in HCC. However, the cytoplasm of HCC is vesicular, granular, and/or clear. The dense cytoplasm and distinct cell border are not seen in HCC.
-
A-75. (c) Centrally placed nuclei with binucleation
A FNA of benign liver reveals sheets of large polygonal and dispersed individual cells. The specimen may also reveal trabecular arrangements and tissue fragments. Cells have centrally placed round- to oval-shaped nuclei with mild variation in size, granular chromatin, prominent nucleoli, no hyperchromasia, and a normal N:C ratio. Binucleation is common in cells. Bile and lipofusion pigment can be identified in the cytoplasm. In contrast, in hepatocellular carcinoma (HCC), tumor cells form cords, tubules, sheets, or isolated individual cells. Tumor cells have hyperchromatic nuclei, coarse chromatin, and high N:C ratios. Large prominent nucleoli, marked variation of size of nuclei, and numerous naked nuclei are features seen in HCC.
Reading List
Balani S, Malik R, Malik R, Kapoor N. Cytomorphological variables of hepatic malignancies in fine needle aspiration smears with special reference to grading of hepatocellular carcinoma. J Cytol. 2013;30:116–20.
Bibbo M, Wood MD, Fitzpatrick BT. Peritoneal washings and ovary. In: Bibbo M, Wilbur D, editors. Comprehensive cytopathology. 3rd ed. Philadelphia: Saunders/Elsevier; 2008.
Cibas ES. Peritoneal washings. In: Cibas ES, Ducatman BS, editors. Cytology: diagnostic principles and clinical correlates. Philadelphia: Saunders/Elsevier; 2009.
DeMay RM. Chapter 6. Cerebrospinal fluid. In: The art and science of cytopathology, exfoliative cytology, vol. 1. 2nd ed. Chicago: ASCP Press; 2012. p. 490–525.
Geramizadeh B, Asadi N, Tabei SZ. Cytologic comparison between malignant and regenerative nodules in the background of cirrhosis. Hepat Mon. 2012;12:448–52.
Khalbuss WE, Monaco SE, Pantanowitz L. Chapter 16. Liver. In: The ASCP Quick Compendium (QC) of cytopathology. Chicago: ASCP Press; 2013. p. 340–65.
VandenBussche C, Gocke CD, Li QK. Fine needle aspiration of metastatic papillary thyroid carcinoma found in the liver. Diagn Cytopathol. 2013;41:418–24.
Wee A. Fine needle aspiration biopsy of hepatocellular carcinoma and hepatocellular nodular lesions: role, controversies and approach to diagnosis. Cytopathology. 2011;22:287–305.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Li, Q.K., Khalbuss, W.E. (2015). Liver Fine-Needle Aspiration. In: Khalbuss, W., Li, Q. (eds) Diagnostic Cytopathology Board Review and Self-Assessment. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1477-7_7
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1477-7_7
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1476-0
Online ISBN: 978-1-4939-1477-7
eBook Packages: MedicineMedicine (R0)