
Abstract
The fine needle aspiration (FNA) cytology, either under CT- (computed tomography) or ultrasound-guidance, is a commonly used approach to obtain samples from renal and adrenal lesions. This chapter is focused on the discussion and review of cytomorphology of FNA specimens of benign and malignant diseases of the kidney and adrenal gland. Although the differential diagnosis of a kidney mass is broad, including both primary and metastatic tumors, the majority of kidney masses are primary kidney tumors. Whereas, in adrenal masses, the majority of tumors are metastatic tumors rather than primary adrenal tumors. The limitations of the FNA cytology in the diagnosis of renal and adrenal lesions are also discussed in the chapter. For example, the cytological differentiation of an oncocytoma from a chromophobe renal cell carcinoma may be difficult due to overlap cytomorphology. Nevertheless, the most renal and adrenal lesions can be accurately diagnosed by FNA cytology.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Renal Cell Carcinoma
- Papillary Renal Cell Carcinoma
- Hyperchromatic Nucleus
- Granular Cytoplasm
- Fuhrman Grade
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
10.1 Image-Based Questions 1–25

Fig. 10.1
-
Q-1. What is the diagnosis of the image?
-
(a)
Metastatic adenocarcinoma
-
(b)
Clear cell renal cell carcinoma (RCC)
-
(c)
Glomerulus
-
(d)
Papillary renal cell carcinoma (RCC)

Fig. 10.2
-
(a)
-
Q-2. A 65-year-old female had a right renal mass. A CT-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Metastatic adenocarcinoma
-
(b)
Clear cell renal cell carcinoma (RCC)
-
(c)
Benign renal tubular cells
-
(d)
Papillary renal cell carcinoma (RCC)

Fig. 10.3
-
(a)
-
Q-3. A 64-year-old male had a right renal mass. A CT-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Metastatic adenocarcinoma
-
(b)
Clear cell renal cell carcinoma (RCC)
-
(c)
Benign renal tubular cells
-
(d)
Papillary renal cell carcinoma (RCC)

Fig. 10.4
-
(a)
-
Q-4. A 50-year-old male had a large right cyst. An ultrasound-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Benign renal cyst
-
(b)
Cystic renal cell carcinoma (RCC)
-
(c)
Benign renal tubular cells
-
(d)
Papillary renal cell carcinoma (RCC)

Fig. 10.5
-
(a)
-
Q-5. What is the diagnosis of the image?
-
(a)
Psammoma bodies
-
(b)
Liesegang rings
-
(c)
Charcot-Leyden crystals
-
(d)
Michaelis-Gutmann bodies

Fig. 10.6
-
(a)
-
Q-6. A 70-year-old male had a left renal cyst. An ultrasound-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Metastatic adenocarcinoma
-
(b)
Papillary renal cell carcinoma (RCC)
-
(c)
Benign renal tubular cells
-
(d)
Cystic renal cell carcinoma (RCC)

Fig. 10.7
-
(a)
-
Q-7. A 23-year-old male had a left renal mass. An ultrasound-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Metastatic adenocarcinoma
-
(b)
Clear cell renal cell carcinoma (RCC)
-
(c)
Angiomyolipoma (AML)
-
(d)
Papillary renal cell carcinoma (RCC)

Fig. 10.8
-
(a)
-
Q-8. A 58-year-old male had a right renal mass. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Metastatic adenocarcinoma
-
(b)
Papillary renal cell carcinoma (RCC)
-
(c)
Benign renal tubular cells
-
(d)
Clear cell renal cell carcinoma (RCC)

Fig. 10.9
-
(a)
-
Q-9. A 77-year-old female had a right renal mass. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Papillary renal cell carcinoma (RCC)
-
(b)
Oncocytoma
-
(c)
Benign renal tubular cells
-
(d)
Cystic renal cell carcinoma (RCC)

Fig. 10.10
-
(a)
-
Q-10. A 58-year-old male had a left renal mass. An ultrasound-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Metastatic adenocarcinoma
-
(b)
Oncocytoma
-
(c)
Benign renal tubular cells
-
(d)
Urothelial cell carcinoma

Fig. 10.11
-
(a)
-
Q-11. A 60-year-old male had a right renal mass. An ultrasound-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Reactive lymphocyte hyperplasia
-
(b)
Oncocytoma
-
(c)
Benign renal tubular cells
-
(d)
Diffuse large B cell lymphoma (DLBCL)

Fig. 10.12
-
(a)
-
Q-12. A 63-year-old male had a left renal mass. An ultrasound-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Low-grade B cell lymphoma
-
(b)
Oncocytoma
-
(c)
Benign renal tubular cells
-
(d)
Reactive lymphocyte hyperplasia

Fig. 10.13
-
(a)
-
Q-13. A 65-year-old female had a left renal mass. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Benign renal tubular cells
-
(b)
Papillary renal cell carcinoma (RCC)
-
(c)
Differentiated, epithelial-predominant Wilms’ tumor
-
(d)
Metanephric adenoma (MA)
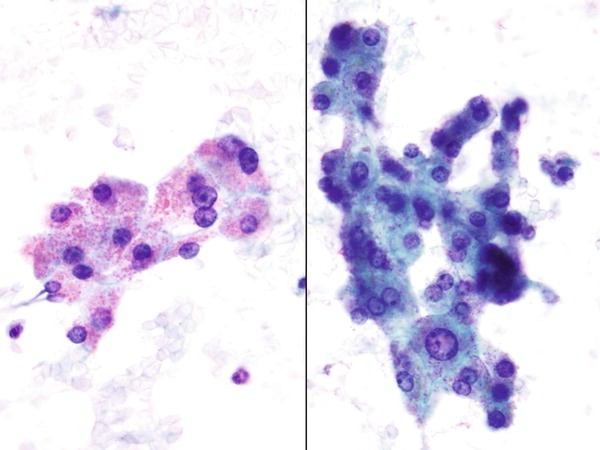
Fig. 10.14
-
(a)
-
Q-14. A 52-year-old male had a left adrenal mass. A CT-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Normal adrenal cortical cells
-
(b)
Oncocytoma
-
(c)
Clear cell renal cell carcinoma (RCC)
-
(d)
Adrenal cortical carcinoma

Fig. 10.15
-
(a)
-
Q-15. A 48-year-old female had a right adrenal mass. A CT-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Adrenal cortical adenoma
-
(b)
Oncocytoma
-
(c)
Clear cell renal cell carcinoma (RCC)
-
(d)
Adrenal cortical carcinoma

Fig. 10.16
-
(a)
-
Q-16. A 53-year-old female had a left adrenal mass. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Adrenal cortical adenoma
-
(b)
Oncocytoma
-
(c)
Adrenal cortical carcinoma
-
(d)
Clear cell renal cell carcinoma (RCC)

Fig. 10.17
-
(a)
-
Q-17. A 70-year-old male had a left renal cyst. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Lymphoma
-
(b)
Metastatic melanoma
-
(c)
Adrenal cortical carcinoma
-
(d)
Clear cell renal cell carcinoma (RCC)

Fig. 10.18
-
(a)
-
Q-18. An 83-year-old male has a lung mass and bilateral adrenal masses. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Lymphoma
-
(b)
Metastatic small cell carcinoma
-
(c)
Metastatic adenocarcinoma
-
(d)
Clear cell renal cell carcinoma (RCC)

Fig. 10.19
-
(a)
-
Q-19. A 47-year-old male has a bladder mass and left renal cyst. A CT-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Metastatic melanoma
-
(b)
Metastatic hepatocellular carcinoma (HCC)
-
(c)
Metastatic renal cell carcinoma (RCC)
-
(d)
Metastatic urothelial cell carcinoma

Fig. 10.20
-
(a)
-
Q-20. A 65-year-old female has a uterine mass and a right adrenal mass. A CT-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Metastatic endometrial carcinoma
-
(b)
Metastatic small cell carcinoma
-
(c)
Metastatic melanoma
-
(d)
Metastatic urothelial cell carcinoma

Fig. 10.21
-
(a)
-
Q-21. A 63-year-old male has a liver mass and a right adrenal mass. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Metastatic adenocarcinoma
-
(b)
Metastatic hepatocellular carcinoma (HCC)
-
(c)
Metastatic melanoma
-
(d)
Metastatic urothelial cell carcinoma

Fig. 10.22
-
(a)
-
Q-22. A 78-year-old male has a lung mass and a left adrenal mass. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Metastatic adenocarcinoma
-
(b)
Metastatic urothelial cell carcinoma
-
(c)
Metastatic squamous cell carcinoma
-
(d)
Metastatic melanoma

Fig. 10.23
-
(a)
-
Q-23. A 69-year-old male has a small bowel mass and a left renal mass. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Metastatic mucinous adenocarcinoma
-
(b)
Metastatic hepatocellular carcinoma (HCC)
-
(c)
Metastatic squamous cell carcinoma
-
(d)
Metastatic urothelial cell carcinoma

Fig. 10.24
-
(a)
-
Q-24. A 46-year-old male had a left adrenal mass. A CT-guided FNA was performed. What is the diagnosis of the FNA?
-
(a)
Metastatic melanoma
-
(b)
Metastatic hepatocellular carcinoma (HCC)
-
(c)
Pheochromocytoma
-
(d)
Metastatic squamous cell carcinoma

Fig. 10.25
-
(a)
-
Q-25. A 66-year-old male had a left renal cyst. An ultrasound-guided FNA was performed. What is the diagnosis of the image?
-
(a)
Metastatic small cell carcinoma
-
(b)
Metastatic prostate carcinoma
-
(c)
Metastatic squamous cell carcinoma
-
(d)
Metastatic urothelial cell carcinoma
-
(a)
























10.2 Text-Based Questions 26–50
-
Q-26. All of the following cytological features are seen in clear cell renal cell carcinomas (RCCs), except:
-
(a)
Abundant clear and/or granular cytoplasm
-
(b)
Cohesive clusters and dispersed individual cells
-
(c)
Eccentrically placed large round nuclei
-
(d)
Numerous naked nuclei
-
(a)
-
Q-27. All of the following cytological features are seen in benign renal tubular cells, except:
-
(a)
Nuclear enlargement and variation in size and shape
-
(b)
Abundant granular cytoplasm
-
(c)
Round nuclei and small nucleoli
-
(d)
Small sheets and scattered individual cells
-
(a)
-
Q-28. Which statement about cystic renal cell carcinoma (RCC) is more accurate?
-
(a)
Scant specimen with rare scattered tumor cells
-
(b)
Trabecular, cord, and nest arrangement of tumor cells
-
(c)
Large nuclei, scant cytoplasm, and high N:C ratios of tumor cells
-
(d)
Numerous naked nuclei
-
(a)
-
Q-29. All of the following features are seen in a fine-needle aspiration (FNA) specimen containing benign renal tubular cells, except:
-
(a)
Granular cytoplasm and indistinct cell borders
-
(b)
Sheets and dispersed polygonal cells
-
(c)
Uniform cells with centrically placed round nuclei
-
(d)
Granular chromatin and small nucleoli
-
(a)
-
Q-30. Which statement about adrenal cortical adenoma is correct?
-
(a)
The tumor involves bilateral adrenals.
-
(b)
Clusters of uniform cells and numerous naked nuclei.
-
(c)
Most of tumors are functioning and secret hormones.
-
(d)
Tumor necrosis is a common finding.
-
(a)
-
Q-31. All of the following cytological features are seen in adrenal cortical carcinomas, except:
-
(a)
Nuclear enlargement and variation in size and shape
-
(b)
Clusters, sheets, and dispersed individual cells
-
(c)
Large oval nuclei and coarse chromatin
-
(d)
Numerous naked nuclei
-
(a)
-
Q-32. All descriptions of cytological features of angiomyolipoma (AML) in a renal FNA are correct, except:
-
(a)
Thick-walled blood vessels are a common finding on the slide.
-
(b)
Tumor consists of fat, myoid cells, and blood vessels.
-
(c)
AML can be diagnosed by FNA.
-
(d)
Some of the tumor may have virtually no fat component.
-
(a)
-
Q-33. A 68-year-old male presents with a right kidney mass and retroperitoneal lymphadenopathy. An ultrasound-guided FNA of the kidney mass was performed. On cytology smear and cell block section, numerous discohesive small- to intermediate-sized cells with high N:C ratio, hyperchromatic nuclei, and scant cytoplasm are identified. What is the most likely diagnosis of the FNA?
-
(a)
Benign renal tubular cells
-
(b)
Clear cell renal cell carcinoma (RCC)
-
(c)
Lymphoma
-
(d)
Small cell carcinoma
-
(a)
-
Q-34. Which statement regarding the angiomyolipoma (AML) is not correct?
-
(a)
The tumors are commonly seen in elderly male patients.
-
(b)
The tumor derives from perivascular epithelial cells.
-
(c)
Tumor cells are positive for HMB45 and MART-1.
-
(d)
Epithelioid cell variant of AMLs has metastatic potentials.
-
(a)
-
Q-35. Which statement about cystic renal cell carcinomas (RCCs) is correct?
-
(a)
Adequate sampling of a cystic RCC is difficult.
-
(b)
Cystic RCCs are difficult to distinguish from benign cysts.
-
(c)
The diagnostic rate of cystic RCCs is low.
-
(d)
All of the above.
-
(a)
-
Q-36. Which statement about adrenal cortical carcinomas is correct?
-
(a)
The tumor involves bilateral adrenals.
-
(b)
Clusters of uniform cells and numerous naked nuclei.
-
(c)
Tumor cells have marked nuclear variations and atypia.
-
(d)
Tumor necrosis is a rare finding.
-
(a)
-
Q-37. Which statement about translocation-associated renal cell carcinomas (Xp11 TRCCs) is correct?
-
(a)
Tumors only involve children.
-
(b)
Xp11 TRCCs have better prognosis than clear cell RCCs.
-
(c)
The tumor has a distinct histomorphology and without clear cell morphology.
-
(d)
Translocations on chromosome X involves the transcription factor E3 (TFE3) gene.
-
(a)
-
Q-38. Which statement about cytological features of glomeruli is correct?
-
(a)
Glomerulus can only be found in the FNA of a benign lesion.
-
(b)
It may be confused with papillary RCCs.
-
(c)
Marked nuclear variations and atypia are characteristics.
-
(d)
It contains flat sheets of cells.
-
(a)
-
Q-39. All of the following cytological features of oncocytomas in a renal FNA are correct, except:
-
(a)
Tumor cells with bland nuclei and abundant granular cytoplasm.
-
(b)
Tumor cells are arranged in small flat sheets and dispersed individual cells.
-
(c)
No mitosis or tumor necrosis.
-
(d)
Tumor cells with marked nuclear variations and atypia.
-
(a)
-
Q-40. On a cell block preparation, which of following cytological findings is the most useful feature in the differential diagnosis of an oncocytoma from a chromophobe renal cell carcinoma (RCC)?
-
(a)
Tumor cells with bland nuclei, abundant granular cytoplasm, and distinct cell borders.
-
(b)
Tumor cells are arranged in round circumscribed nests.
-
(c)
Positive Hale’s colloidal iron stains.
-
(d)
Tumor cells with distinct cell borders.
-
(a)
-
Q-41. In a renal FNA specimen, cercariform cells are identified. What is the most likely diagnosis?
-
(a)
Metastatic squamous cell carcinoma
-
(b)
Metastatic melanoma
-
(c)
Benign renal tubular cells
-
(d)
Urothelial cell carcinoma
-
(a)
-
Q-42. In the FNA specimen of a kidney mass, which one of following features favors the diagnosis of a lymphoma?
-
(a)
Numerous clusters of cells
-
(b)
Monomorphous population of cells
-
(c)
Lymphoglandular bodies
-
(d)
Vesicular chromatin and inconspicuous nucleoli
-
(a)
-
Q-43. All of the following cytological features of Wilms’ tumors in a renal FNA are correct, except:
-
(a)
Bland nuclei and abundant granular cytoplasm
-
(b)
Numerous discohesive small blue cells
-
(c)
Mitoses and tumor necrosis
-
(d)
Marked nuclear atypia
-
(a)
-
Q-44. Which statement about clear cell renal cell carcinomas (RCCs) is correct?
-
(a)
Focally, tumor cells may show large hyperchromatic nuclei, multinucleation, and eosinophilic cytoplasm.
-
(b)
The tumor may be composed of clear cells or granular cells or both. Sarcomatoid and other variants also occur.
-
(c)
The smear reveals prominent small vessels (hypervascularity).
-
(d)
All of the above.
-
(a)
-
Q-45. In an FNA specimen, which one of following features favors the diagnosis of a diffuse large B cell lymphoma (DLBCL)?
-
(a)
Three-dimensional clusters of atypical large cells
-
(b)
Discohesive and/or dispersed individual large atypical cells
-
(c)
Clusters of large cells have markedly atypical nuclei and abundant cytoplasm
-
(d)
Acini/papillary groups of large cells with pleomorphic nuclei and abundant cytoplasm
-
(a)
-
Q-46. All of the following cytological features of urothelial cell carcinomas in a renal FNA are correct, except:
-
(a)
Tumor cells with bland nuclei and abundant granular cytoplasm
-
(b)
Large tumor cells with hyperchromatic nuclei and inconspicuous nucleoli
-
(c)
Dense cytoplasm
-
(d)
Tumor cells with marked nuclear variations and atypia
-
(a)
-
Q-47. Which statement about adrenal cortical neoplasms is correct?
-
(a)
Focally, tumor cells of carcinomas can be bland, whereas adenoma can be atypical.
-
(b)
The tumor may be composed of clear cells or granular cells or both.
-
(c)
Normal adrenal cortex and adenomas can be difficult to distinguish by cytology alone.
-
(d)
All of the above.
-
(a)
-
Q-48. All of the following cytological features of pheochromocytoma in a renal FNA are correct, except:
-
(a)
Three-dimensional clusters of cells with bland nuclei and abundant granular cytoplasm
-
(b)
Large tumor cells with hyperchromatic nuclei and inconspicuous nucleoli
-
(c)
Dense cytoplasm
-
(d)
Tumor cells with marked nuclear variations and atypia
-
(a)
-
Q-49. Which of the features is not seen in a metastatic squamous cell carcinoma in an FNA specimen?
-
(a)
Large nuclei with smudgy chromatin
-
(b)
Nuclei with variation in size and shape
-
(c)
Small pyknotic nuclei
-
(d)
Large prominent nucleoli
-
(a)
-
Q-50. In an FNA specimen of a kidney mass, epithelioid cells with “clear cytoplasm” are identified. All of the following tumors can have this cytological feature, except:
-
(a)
Oncocytoma
-
(b)
Clear cell renal cell carcinoma (RCC)
-
(c)
Papillary renal cell carcinoma (RCC)
-
(d)
Benign renal tubular cells
-
(a)
10.3 Answers and Discussions of Image-Based Questions 1–25
-
A-1. (c) Glomerulus
In a renal FNA, glomeruli are large globular and/or lobulated structures with scalloped borders and contain spindled endothelial cells, oval-shaped mesangial cells, and capillary loops. Cells of glomeruli reveal normal N:C ratios, dense chromatin, and moderate cytoplasm. In clear cell RCCs, tumor cells form cohesive two-dimensional clusters and have large eccentrically placed nuclei, vesicular chromatin, and granular or vacuolated cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain. Nucleoli vary in size depending on the Fuhrman grade. In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background. In metastatic adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production).
-
A-2. (c) Benign renal tubular cells
Benign renal tubular cells, particularly proximal tubular cells, are arranged in loosely formed sheets and dispersed individual cells; they have a uniform appearance with round nuclei, fine granular chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios. In clear cell RCCs, tumor cells form cohesive two-dimensional clusters and have large eccentrically placed nuclei, vesicular chromatin, and granular or clear cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain. Nucleoli vary in size depending on the Fuhrman grade. In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular or clear cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background. In metastatic adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production).
-
A-3. (b) Clear cell renal cell carcinoma (RCC)
The clear cell RCC variant (conventional renal cell carcinomas) is the most common histologic subtype of malignant renal tumors and accounts for 70 % of renal cell carcinomas. The “clear cell” appearances of tumor cells are due to the cytoplasmic glycogen and lipid that are dissolved during tissue processing. In RCCs, particularly in clear cell RCCs, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain. Focally, tumor cells may also show large hyperchromatic nuclei, multinucleation, and eosinophilic cytoplasm. Tumor necrosis may be seen, particularly in the Fuhrman grade III and IV tumors. The background of smear is bloody and with prominent small vessels (hypervascularity). In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background. In metastatic adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production). In benign renal tubular cells, particularly proximal tubular cells, they are arranged in loosely formed sheets and have round nuclei, fine chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios.
-
A-4. (a) Benign renal cyst
An FNA of a benign renal cyst reveals scant cellularity with scattered foamy macrophages and amorphous material in the background. The main differential diagnosis of benign renal cysts is cystic RCCs. In cystic RCCs, tumor cells are scant and reveal dispersed individual cells with round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background. In benign renal tubular cells, particularly proximal tubular cells, they are arranged in loosely formed sheets and have round nuclei, fine chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios.
-
A-5. (b) Liesegang rings
Liesegang rings are large laminated ringlike structures with double-layer outer walls, radial cross striations, and an amorphous central nidus. They are most commonly seen in a benign cystic fluid such as in renal and breast cysts and are composed of organic substances most likely formed by the precipitation from the cystic fluid. They stain blue in color with the hematoxylin-eosin (H&E) and the Papanicolaou methods. The differential diagnoses include parasites, parasitic eggs, algae, calcifications, and psammoma bodies. Awareness of the Liesegang phenomenon within cystic lesions will decrease the possibility of erroneous misdiagnosis as another type of pathologic process. The Charcot-Leyden crystals are a needle-shaped, orangeophilic structure derived from degenerated eosinophils; they may be found in a variety of lung diseases associated with increased eosinophils. Psammoma bodies are structures with concentrically laminated calcifications and a circumferential thin layer of epithelial cells; it is commonly seen in both carcinomas and benign conditions. The Michaelis-Gutmann bodies are small intracytoplasmic basophilic inclusions and measure 2–10 μm in diameter. They are composed of iron and calcium and associated with malakoplakia.
-
A-6. (d) Cystic renal cell carcinoma (RCC)
The main differential diagnosis of renal cysts is cystic RCCs. In cystic RCCs, tumor cells are scant and reveal dispersed individual cells with round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background. In benign renal tubular cells, particularly proximal tubular cells, they are arranged in loosely formed sheets and have round nuclei, fine chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios. In metastatic adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production).
-
A-7. (c) Angiomyolipoma (AML)
AML is a rare benign mesenchymal tumor and composed of mature fat cells, epithelioid spindle cells (smooth muscle cells), and blood vessels. The diagnosis depends on the identification of the triad. However, proportions of these components vary considerably from tumor to tumor. Some tumors are composed predominantly of fat, whereas others have virtually no fat and almost exclusive myoid cells (smooth muscle). In difficult cases, the immunohistochemical (IHC) stain of HMB45 is helpful and positive for the neoplastic cells. In RCCs, particularly in clear cell RCCs, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain. Focally, tumor cells may also show large hyperchromatic nuclei, multinucleation, and eosinophilic cytoplasm. Tumor necrosis may be seen, particularly in the Fuhrman grade III and IV tumors. The background of smear is bloody and with prominent small vessels (hypervascularity). In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background. In metastatic adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production).
-
A-8. (d) Clear cell renal cell carcinoma (RCC)
In clear cell RCC, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain. Focally, tumor cells may also show large hyperchromatic nuclei, multinucleation, and eosinophilic cytoplasm. Tumor necrosis may be seen, particularly in the Fuhrman grade III and IV tumors. The background of smear is bloody and with prominent small vessels (hypervascularity). In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background. In benign renal tubular cells, particularly proximal tubular cells, they are arranged in loosely formed sheets and have round nuclei, fine chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios. In metastatic adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production).
-
A-9. (b) Oncocytoma
Oncocytoma is a benign tumor and comprises less than 5 % of all renal tumors. The FNA reveals a cellular specimen. Tumor cells are arranged in small flat clusters and dispersed individual cells and reveal bland nuclei and abundant granular cytoplasm. Nuclei are round in shape with fine chromatin, inconspicuous or small nucleoli, abundant dense granular cytoplasm, and distinct cytoplasmic borders. In cystic RCCs, tumor cells are scant and reveal dispersed individual cells with round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background. In benign renal tubular cells, particularly proximal tubular cells, they are arranged in loosely formed sheets and have round nuclei, fine chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios.
-
A-10. (d) Urothelial cell carcinoma
Urothelial cell carcinomas arise in the renal pelvis. Tumor cells are large in size and arranged in cohesive two-dimensional clusters and dispersed individual cells with large hyperchromatic nuclei, dense chromatin, inconspicuous nucleoli, and dense cytoplasm. Some of the tumor cells with elongated cytoplasm and flared cytoplasmic ends form the so-called cercariform cells, characteristics of urothelial cell neoplasm. The cercariform appearance is the result of pseudostratification of urothelial cells. In metastatic adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production). In oncocytomas, tumor cells are arranged in small flat clusters and dispersed individual cells and reveal bland nuclei and abundant granular cytoplasm. Nuclei are round in shape with fine chromatin, inconspicuous or small nucleoli, abundant dense granular cytoplasm, and distinct cytoplasmic borders. In benign renal tubular cells, particularly proximal tubular cells, they are arranged in loosely formed sheets and have round nuclei, fine chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios.
-
A-11. (d) Diffuse large B cell lymphoma (DLBCL)
DLBCL is a biological and clinical diverse group of diseases. The FNA reveals a cellular specimen with discohesive large atypical lymphoid cells. Three morphological variants are most commonly seen: centroblastic, immunoblastic, and anaplastic variant. Centroblastic variant is the most common subtype and reveals medium- to large-sized tumor cells with high N:C ratios, oval or round nuclei, fine chromatin, and single or multiple prominent nucleoli. Immunoblasts have a basophilic cytoplasm and a central nucleolus. The third morphologic variant, anaplastic variant, consists of large tumor cells with pleomorphic nuclei and may resemble the Hodgkin cells or Reed-Stemberg cells. Most cases of DLBCL are polymorphic, with a mixture of centroblastic and immunoblastic cells. Reactive lymphoid hyperplasia contains a heterogeneous mixture of lymphocytes, including small lymphocytes, centrocytes/centroblasts, immunoblasts, tingible body macrophages, and other cells. There is a great variation of cellular sizes and appearances, characteristic of polymorphous population of cells. In oncocytomas, tumor cells are arranged in small flat clusters and dispersed individual cells and reveal bland nuclei and abundant granular cytoplasm. Nuclei are round in shape with fine chromatin, inconspicuous or small nucleoli, abundant dense granular cytoplasm, and distinct cytoplasmic borders. In benign renal tubular cells, particularly proximal tubular cells, they are arranged in loosely formed sheets and have round nuclei, fine chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios.
-
A-12. (a) Low-grade B cell lymphoma
The FNA of a lymphoma reveals a cellular specimen with monomorphous population of lymphocytes, particularly in low-grade B cell lymphoma and/or small lymphocytic lymphomas/chronic lymphocytic leukemia (SLL/CLL). It represents a monoclonal proliferation of lymphoma cells. Other cytological features of a low-grade B cell lymphoma include discohesive tumor cells with hyperchromatic nuclei, clumped (soccer-ball-like) chromatin, irregular nuclear membranes, inconspicuous nucleoli and scant cytoplasm, and rare or absence of tingible body macrophages. Reactive lymphoid hyperplasia contains a heterogeneous mixture of lymphocytes, including small lymphocytes, centrocytes/centroblasts, immunoblasts, tingible body macrophages, and other cells. There is a great variation of cellular sizes and appearances, characteristic of polymorphous population of cells.
-
A-13. (d) Metanephric adenoma (MA)
MA is a rare benign tumor and most commonly occurs in females in the fifth decade. Histologically, MA is composed of closely packed acinar or tubular structures lined by bland cells with scanty interposed stroma. On cytological preparations, cells are arranged in tight clusters and loose sheets and have small round nuclei, inconspicuous or small nucleoli, and scant cytoplasm. Mitoses are conspicuously absent. Cells of MA are also positive for WT1 stain. The main differential diagnoses of MA are papillary RCC and differentiated, epithelial-predominant Wilms’ tumor. In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background. Wilms’ tumors involve infants and young children and are triphasic neoplasms, which contain blastemal components (closely packed small blue cells), mesenchymal components (spindle cells), and epithelial components (packed tubular structures). Therefore, MA can be difficult to distinguish from differentiated, epithelial-predominant Wilms’ tumor. In differentiated, epithelial-predominant Wilms’ tumor, cells are more hyperchromatic and with abundant mitoses.
-
A-14. (a) Normal adrenal cortical cells
Normal adrenal cortical cells are arranged in small sheets and dispersed individual cells with small round nuclei, granular chromatin, small centrically located nucleoli, and abundant clear and/or granular cytoplasm. In adrenal cortical carcinomas, tumor cells have marked nuclear variations and atypia, abundant mitoses, and necrotic debris. In oncocytomas, tumor cells are arranged in small flat clusters and dispersed individual cells and reveal bland nuclei and abundant granular cytoplasm. Nuclei are round in shape with fine chromatin, inconspicuous or small nucleoli, abundant dense granular cytoplasm, and distinct cytoplasmic borders. In clear cell RCC, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain. Focally, tumor cells may also show large hyperchromatic nuclei, multinucleation, and eosinophilic cytoplasm. Tumor necrosis may be seen, particularly in the Fuhrman grade III and IV tumors. The background of smear is bloody and with prominent small vessels (hypervascularity).
-
A-15. (a) Adrenal cortical adenoma
Adrenal cortical adenomas contain normal-appearing adrenal cortical cells, which are arranged in small sheets and dispersed individual cells. Tumor cells have small round nuclei, granular chromatin, small centrically located nucleoli, and abundant clear and/or granular cytoplasm. No mitosis is identified. Numerous naked nuclei floating in a frothy granular background is also a characteristic. Tumor necrosis is not a common finding in adrenal cortical adenomas. In adrenal cortical carcinomas, tumor cells have marked nuclear variations and atypia, abundant mitoses, and necrotic debris. In oncocytomas, tumor cells are arranged in small flat clusters and dispersed individual cells and reveal bland nuclei and abundant granular cytoplasm. Nuclei are round in shape with fine chromatin, inconspicuous or small nucleoli, abundant dense granular cytoplasm, and distinct cytoplasmic borders. In clear cell RCC, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm.
-
A-16. (c) Adrenal cortical carcinoma
Histologically, the diagnosis of adrenal cortical carcinomas requires to follow strict criteria, such as nuclear grade, necrosis, capsular invasion, mitotic rate, and atypical mitoses. These features are difficult to evaluate on a cytological specimen. Nevertheless, most of the adrenal masses can be correctly classified as benign or malignant by FNAs. In adrenal cortical carcinomas, FNA reveals a cellular specimen. Tumor cells are arranged in loose clusters, sheets, and dispersed individual cells and have marked nuclear variations and atypia, abundant mitoses, and necrotic debris. Adrenal cortical adenomas contain normal-appearing adrenal cortical cells, which are arranged in small sheets and dispersed individual cells with small round nuclei, granular chromatin, small centrically located nucleoli, and abundant clear and/or granular cytoplasm. No mitosis or necrosis is identified. Numerous naked nuclei floating in a frothy granular background is also a characteristic. In oncocytomas, tumor cells are arranged in small flat clusters and dispersed individual cells and reveal bland nuclei and abundant granular cytoplasm. Nuclei are round in shape with fine chromatin, inconspicuous or small nucleoli, abundant dense granular cytoplasm, and distinct cytoplasmic borders. In clear cell RCC, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm.
-
A-17. (b) Metastatic melanoma
In metastatic melanoma, tumor cells are usually arranged in loose clusters or dispersed individual cells. The nuclei of tumor cells are eccentrically located (plasmacytoid appearance) and highly variable in size with finely to coarsely granular chromatin and a single prominent cherry-red nucleoli. The cytoplasm tends to be abundant and may or may not contain melanin pigment. The N:C ratio may not be high. Melanin pigment appears coarsely granular and dark brown on the Papanicolaou stain. Other characteristic features include multinucleation, binucleation, and intranuclear inclusions. In lymphomas, tumor cells reveal a monomorphous appearance and lymphoglandular bodies. In adrenal cortical carcinomas, FNA reveals a cellular specimen. Tumor cells are arranged in loose clusters and dispersed individual cells and have marked nuclear variations and atypia, abundant mitoses, and necrotic debris. In clear cell RCC, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. In difficult cases, immunomarkers S100, HMB45, and MelanA/Mart1 are helpful in the differential diagnosis of melanomas.
-
A-18. (b) Metastatic small cell carcinoma
In small cell carcinomas, the size of tumor cells is smaller. Tumor cells reveal acini and/or pseudorosette arrangements, with hyperchromatic nuclei, fine (salt-and-pepper) chromatin, inconspicuous nucleoli, and scant cytoplasm. Nuclear crowding and molding are characteristic features. The background of the smear may also reveal “blue strips” (indicative of breakdown of nuclear material), abundant mitoses, and tumor necrosis. In adenocarcinoma, tumor cells form acini and/or three-dimensional clusters and can be confused with rosettes in a suboptimal prepared slides; tumor cells reveal hyperchromatic nuclei, vesicular or coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production). In lymphoma, tumor cells are discohesive with clump chromatin and scant cytoplasm. Lymphoglandular bodies may be identified in the background of the smear. Metastatic melanoma reveals large discohesive tumor cells with prominent nucleoli and cytoplasmic pigment. In clear cell RCC, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm.
-
A-19. (d) Metastatic urothelial cell carcinoma
The smears reveal a cellular specimen. Tumor cells are large in size and arranged in cohesive two-dimensional clusters and dispersed individual cells with large hyperchromatic nuclei, dense chromatin, inconspicuous nucleoli, and dense cytoplasm. Some of the tumor cells with elongated cytoplasm form the so-called cercariform cells, characteristics of urothelial cell neoplasm. In HCCs, tumor cells have large prominent nucleoli and cytoplasmic bile and/or lipofuscin pigments, which stain golden and brown color with the Papanicolaou method. Numerous naked nuclei are also seen in HCCs. Metastatic melanoma reveals large discohesive tumor cells with prominent nucleoli and cytoplasmic pigment. In clear cell RCC, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm.
-
A-20. (a) Metastatic endometrial carcinoma
The smears reveal cohesive two-dimensional clusters, acini, and dispersed individual cells with high N:C ratios. Tumor cells have large hyperchromatic nuclei, coarse chromatin, conspicuous nucleoli, irregular nuclear membranes, and vesicular cytoplasm. These findings are consistent with a metastatic adenocarcinoma of the uterus primary. In metastatic urothelial cell carcinomas, tumor cells are large in size and arranged in cohesive two-dimensional clusters and dispersed individual cells with large hyperchromatic nuclei, dense chromatin, inconspicuous nucleoli, and dense cytoplasm. Some of the tumor cells with elongated cytoplasm form the so-called cercariform cells, characteristics of urothelial cell neoplasm. Metastatic melanoma reveals large discohesive tumor cells with prominent nucleoli and cytoplasmic pigment. In small cell carcinomas, the size of tumor cells is smaller. Tumor cells reveal acini and/or pseudorosette arrangements, with hyperchromatic nuclei, fine (salt-and-pepper) chromatin, inconspicuous nucleoli, and scant cytoplasm. Nuclear crowding and molding are characteristic features. The background of the smear may also reveal “blue strips” (indicative of breakdown nuclear material), abundant mitoses, and tumor necrosis.
-
A-21. (b) Metastatic hepatocellular carcinoma (HCC)
In metastatic HCCs, tumor cells show a wide range of cytomorphology. In poorly differentiated forms, malignant cells are polygonal and discohesive with pleomorphic nuclei and giant tumor cells. In well-differentiated forms, tumor cells resemble normal hepatocytes and form trabeculae, cords, and nests with slightly increased N:C ratios, large round nuclei, prominent nucleoli, naked nuclei, and bile pigment in the cytoplasm. The most notable features of HCCs are large polygonal cells with prominent nucleoli, dense cytoplasm which contains cytoplasmic bile and/or lipofuscin pigments, and numerous naked nuclei. In metastatic urothelial cell carcinomas, tumor cells are large in size and arranged in cohesive two-dimensional clusters and dispersed individual cells with large hyperchromatic nuclei, dense chromatin, inconspicuous nucleoli, and dense cytoplasm. Some of the tumor cells with elongated cytoplasm form the so-called cercariform cells, characteristics of urothelial cell neoplasm. Metastatic melanoma reveals large discohesive tumor cells with prominent nucleoli and cytoplasmic pigment. In metastatic adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production).
-
A-22. (c) Metastatic squamous cell carcinoma
Metastatic squamous cell carcinoma usually forms loose clusters or dispersed individual tumor cells. The cytological features of tumor cells include large nuclei with smudgy chromatin, nuclei with variation in size and shape, and dense cytoplasm (indicative of cytokeratin formation). The dense cytoplasm is blue in color with the Diff-Quik stain and red pink (eosinophilic) in color with the Papanicolaou stain. Prominent nucleoli can be seen in poorly differentiated squamous cell carcinomas and should not be confused with poorly differentiated adenocarcinomas. In metastatic adenocarcinomas, tumor cells form acini and/or three-dimensional clusters and reveal hyperchromatic nuclei, coarse chromatin, prominent nucleoli, and vacuolated cytoplasm (indicative of mucin production). In metastatic urothelial cell carcinomas, tumor cells are large in size and arranged in cohesive two-dimensional clusters and dispersed individual cells with large hyperchromatic nuclei, dense chromatin, inconspicuous nucleoli, and dense cytoplasm. Some of tumor cells with elongated cytoplasm form the so-called cercariform cells, characteristics of urothelial cell neoplasm. Metastatic melanoma reveals large discohesive tumor cells with prominent nucleoli and cytoplasmic pigment.
-
A-23. (a) Metastatic mucinous adenocarcinoma
The smears reveal abundant mucinous material and cohesive three-dimensional clusters of tumor cells with high N:C ratios. Tumor cells have large hyperchromatic nuclei, coarse chromatin, conspicuous nucleoli, irregular nuclear membranes, and cytoplasmic mucin. These findings are consistent with a metastatic mucinous adenocarcinoma of the intestinal primary. In metastatic urothelial cell carcinomas, tumor cells are large in size and arranged in cohesive two-dimensional clusters and dispersed individual cells with large hyperchromatic nuclei, dense chromatin, inconspicuous nucleoli, and dense cytoplasm. Some of the tumor cells with elongated cytoplasm form the so-called cercariform cells, characteristics of urothelial cell neoplasm. Metastatic melanoma reveals large discohesive tumor cells with prominent nucleoli and cytoplasmic pigment. In metastatic squamous cell carcinomas, cytological features of tumor cells include large nuclei with smudgy chromatin, nuclei with variation in size and shape, and dense cytoplasm (indicative of cytokeratin formation). In metastatic HCCs, the most notable features are large polygonal cells with prominent nucleoli, dense cytoplasm which contains cytoplasmic bile and/or lipofuscin pigments, and numerous naked nuclei.
-
A-24. (c) Pheochromocytoma
Pheochromocytoma is rarely aspirated due to the risk of hypertensive crisis. However, about 10 % of tumors are nonfunctional and may be aspirated. The FNA specimen reveals dispersed pleomorphic tumor cells with large hyperchromatic nuclei, granular chromatin, prominent nucleoli, and dense cytoplasm. Giant tumor cells with multinucleation and bizarre tumor cells are also common findings. Numerous mitoses may be present. Tumor cells are positive for chromogranin and synaptophysin. In metastatic squamous cell carcinomas, cytological features of tumor cells include large nuclei with smudgy chromatin, nuclei with variation in size and shape, and dense cytoplasm (indicative of cytokeratin formation). In metastatic HCCs, the most notable features are large polygonal cells with prominent nucleoli, dense cytoplasm which contains cytoplasmic bile and/or lipofuscin pigments, and numerous naked nuclei. Metastatic melanoma reveals large discohesive tumor cells with prominent nucleoli and cytoplasmic pigment. Finally, pheochromocytomas can behave in a benign or malignant fashion; morphology is not always predictive of clinical behaviors.
-
A-25. (b) Metastatic prostate carcinoma
The smears reveal three-dimensional clusters of hyperchromatic cells with acinar arrangements and high N:C ratios. In metastatic prostate carcinomas, tumor cells are intermediate in size with hyperchromatic nuclei, coarse chromatin, irregular nuclear membrane, prominent nucleoli, and vacuolated cytoplasm. In metastatic small cell carcinomas, tumor cells are small with fine (salt-and-pepper) chromatin and scant cytoplasm. Nuclear crowding and molding and tumor necrosis are also characteristics of a small cell carcinoma. In metastatic squamous cell carcinomas, cytological features of tumor cells include large nuclei with smudgy chromatin, nuclei with variation in size and shape, and dense cytoplasm (indicative of cytokeratin formation). In metastatic urothelial cell carcinomas, tumor cells are large in size and arranged in cohesive two-dimensional clusters and dispersed individual cells with large hyperchromatic nuclei, dense chromatin, inconspicuous nucleoli, and dense cytoplasm. Some of the tumor cells with elongated cytoplasm form the so-called cercariform cells, characteristics of urothelial cell neoplasm.
10.4 Answers and Discussions of Text-Based Questions 26–50
-
A-26. (d) Numerous naked nuclei
The clear cell RCC variant (conventional renal cell carcinomas) is the most common histologic subtype of malignant renal tumors and accounts for 70 % of renal cell carcinomas. The “clear cell” appearances of tumor cells are due to the cytoplasmic glycogen and lipids that are dissolved during tissue processing. In clear cell RCCs, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain. Focally, tumor cells may also show large hyperchromatic nuclei, multinucleation, and eosinophilic cytoplasm. Tumor necrosis may be seen, particularly in the Fuhrman grade III and IV tumors. The background of smear is bloody and with prominent small vessels (hypervascularity). Numerous naked nuclei are the feature seen in adrenal cortical adenomas; it is not the feature seen in clear cell RCCs.
-
A-27. (a) Nuclear enlargement and variation in size and shape
Benign renal tubular cells, particularly proximal tubular cells, are arranged in loosely formed sheets and dispersed individual cells; they have a uniform appearance with round nuclei, fine granular chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic borders. Cells also reveal minimal nuclear variations and normal N:C ratios. Nuclear enlargement and variation in size and shape are not features seen in benign renal tubular cells.
-
A-28. (a) Scant specimen with rare scattered tumor cells
In cystic renal lesions, the main differential diagnosis is cystic RCC. In cystic RCCs, tumor cells are scant and have low N:C ratios; therefore, it is difficult to make the diagnosis. Tumor cells of cystic RCCs have similar cytological features as seen in clear cell RCCs, including dispersed individual cells with round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. Trabecular, cord, and nest arrangements of tumor cells with large nuclei, scant cytoplasm, high N:C ratios, and numerous naked nuclei are not features seen in cystic RCCs. Finally, the diagnosis of cystic RCCs should be correlated with radiographic findings.
-
A-29. (b) Sheets and dispersed polygonal cells
Benign renal tubular cells, particularly proximal tubular cells, are arranged in loosely formed sheets and dispersed individual cells; they have a uniform appearance with round nuclei, fine granular chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios. Sheets and dispersed polygonal cells are not features seen in benign renal tubular cells.
-
A-30. (b) Clusters of uniform cells and numerous naked nuclei
Adrenal cortical adenomas are quite common and involve approximately 5 % of adults. In contrast to adrenal cortical carcinomas, more than 85 % of adenomas are nonfunctioning. The tumor usually occurs unilaterally. The adrenal cortical adenomas contain normal-appearing adrenal cortical cells, which are arranged in small sheets and dispersed individual cells. Tumor cells have small round nuclei, granular chromatin, small centrically located nucleoli, and abundant clear and/or granular cytoplasm. No mitosis is identified. Numerous naked nuclei floating in a frothy granular background are also characteristics. Tumor necrosis is not a common finding in adrenal cortical adenomas.
-
A-31. (d) Numerous naked nuclei
In adrenal cortical carcinomas, FNA reveals a cellular specimen. Tumor cells are arranged in loose clusters, sheets, and dispersed individual cells and have marked nuclear variations and atypia, abundant mitoses, and necrotic debris. Histologically, the diagnosis of adrenal cortical carcinomas requires to follow strict criteria, such as nuclear grade, tumor necrosis, capsular invasion, mitotic rate, and atypical mitoses. These features are difficult to evaluate in a cytological specimen. Nevertheless, most of the adrenal masses can be correctly classified as benign or malignant by FNAs. Numerous naked nuclei floating in a frothy granular background are characteristics of adrenal cortical adenomas.
-
A-32. (a) Thick-walled blood vessels are a common finding on the slide
The diagnosis of AML depends on the identification of the triad of mature fat, spindle ells (smooth muscle cells), and blood vessels. However, proportions of three components vary considerably from tumor to tumor. Some tumors are composed predominantly of fat, whereas others have virtually no fat and almost exclusively myoid cells (smooth muscle cells). In general, tumor reveals cohesive clusters of spindle-shaped smooth muscle cells, fat cells, and vessels. Occasionally, thick-walled blood vessels are seen on FNA slides. But it is not a common finding. In difficult cases, the immunohistochemical (IHC) stain of HMB45 is helpful and positive for the neoplastic cells.
-
A-33. (c) Lymphoma
The most likely diagnosis of this FNA is a lymphoma. The cytological features of numerous discohesive small- to intermediate-sized cells with high N:C ratio, hyperchromatic nuclei, and scant cytoplasm are characteristics of lymphomas. The monomorphous appearance of the lesion represents a monoclonal proliferation of lymphoma cells. Other cytological features of lymphoma include hyperchromatic clumped (soccer-ball-like) chromatin, irregular nuclear membrane, and scant basophilic cytoplasm. Lymphoglandular bodies can also be seen in the background. In small cell carcinomas, tumor cells reveal salt-and-pepper chromatin, nuclear molding and crowding, numerous apoptotic bodies, and mitotic figures. Benign renal tubular cells, particularly proximal tubular cells, are arranged in loosely formed sheets and dispersed individual cells; they have a uniform appearance with round nuclei, fine granular chromatin, small nucleoli, abundant granular cytoplasm; and indistinct cytoplasmic borders. Cells also reveal minimal nuclear variations and normal N:C ratios. In clear cell RCCs, tumor cells form cohesive two-dimensional clusters and have large eccentrically placed nuclei, vesicular chromatin, and granular or vacuolated cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain.
-
A-34. (a) The tumors are commonly seen in elderly male patients
AML is a rare benign mesenchymal tumor and occurs in two distinct clinical settings: in young adults with tuberous sclerosis (TS) and/or in young and middle-aged females without clinical syndrome. The diagnosis of the tumor depends on the identification of the triad of mature fat, spindle cells (smooth muscle cells), and blood vessels. However, proportions of the three components vary considerably from tumor to tumor. Some tumors are composed predominantly of fat, whereas others have virtually no fat and almost exclusive myoid cells (smooth muscle). In difficult cases, the immunohistochemical (IHC) stain of HMB45 is helpful and positive for the neoplastic cells. Although AML is considered as a benign tumor, the epithelioid cell variant has a potential risk for metastasis.
-
A-35. (d) All of the above
In cystic renal lesions, the main differential diagnosis is cystic RCC. In cystic RCCs, tumor cells are scant and have low N:C ratios; therefore, it is difficult to make the diagnosis. Tumor cells of cystic RCCs have similar cytological features as seen in clear cell RCCs, including dispersed individual cells with round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. Adequate sampling of a cystic RCC is difficult. The cytological diagnostic rate of cystic RCCs is low. Finally, the diagnosis of cystic RCCs should be correlated with radiographic findings.
-
A-36. (c) Tumor cells have marked nuclear variation and atypia
In adrenal cortical carcinomas, FNA reveals a cellular specimen. Tumor cells are arranged in loose clusters, sheets, and dispersed individual cells and have marked nuclear variations and atypia, abundant mitoses, and necrotic debris. Histologically, the diagnosis of adrenal cortical carcinomas requires to follow strict criteria, such as nuclear grade, tumor necrosis, capsular invasion, mitotic rate, and atypical mitoses. These features are difficult to evaluate on a cytological specimen. Nevertheless, most of the adrenal masses can be correctly classified as benign or malignant by FNAs. Clusters of uniform cells and numerous naked nuclei floating in a frothy granular background are characteristics of adrenal cortical adenoma.
-
A-37. (d) Translocations on chromosome X involves the transcription factor E3 (TFE3) gene
Xp11 TRCC is a rare variant of RCCs and may be found in both pediatric and adult population. Tumors usually present at an advanced stage with metastases and universally have an aggressive clinical course and poor prognosis. The gross pathologic feature of Xp11 TRCCs reveals a well-circumscribed tumor without areas of hemorrhage or necrosis. Histological examination of the tumor reveals nests, loosely formed clusters, and papillary arrangements of cells with granular and/or clear cytoplasm. These features are often confused with papillary RCCs and/or clear cell RCCs. The most common genetic abnormality of Xp11 TRCCs is the Xp11 mutations, which result in gene fusion products between the helix-loop-helix leucine zipper transcription factor (TFE3) and the alveolar soft part sarcoma locus (ASPL). A strong clinical suspicion and a positive immunostain of TEF3 are necessary to distinguish Xp11 TRCCs from papillary and clear cell RCCs.
-
A-38. (b) It may be confused with papillary RCCs
Normal elements are frequently encountered on renal FNAs, particularly when a small lesion is sampled. Therefore, glomeruli can be found on slides from both benign and malignant lesions. In a renal FNA, glomeruli are large globular and/or lobulated structures with scalloped borders and contain spindled endothelial cells, oval-shaped mesangial cells, and capillary loops. Cells of glomeruli reveal normal N:C ratios, dense chromatin, and moderate cytoplasm. Marked nuclear variations and atypia are not seen in glomerulus. Glomerulus may be confused with papillary RCCs. In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background.
-
A-39. (d) Tumor cells with marked nuclear variations and atypia
Oncocytoma is a benign tumor and comprises less than 5 % of all renal tumors. The FNA reveals a cellular specimen. Tumor cells are arranged in small flat clusters and dispersed individual cells and reveal bland nuclei and abundant granular cytoplasm. Nuclei are round in shape with fine chromatin, inconspicuous or small nucleoli, abundant dense granular cytoplasm, and distinct cytoplasmic borders. No mitosis or tumor necrosis is present. Tumor cells with marked nuclear variations and atypia are not features seen in oncocytomas.
-
A-40. (b) Tumor cells are arranged in round circumscribed nests
The distinction between oncocytomas and chromophobe RCCs can be difficult due to overlapping cytological features between the two tumors. In oncocytomas, tumor cells reveal bland nuclei and abundant granular cytoplasm. Nuclei are round in shape with fine chromatin, inconspicuous or small nucleoli, abundant dense granular cytoplasm, and distinct cytoplasmic borders. In chromophobe RCCs, tumor cells reveal similar cytological features, such as bland nuclei, abundant granular cytoplasm, and distinct cell borders. Furthermore, both tumors can be positive for Hale’s colloidal iron stain, although oncocytoma is focally positive and chromophobe RCC is diffusely positive. Therefore, the most useful cytological feature for the differential diagnosis of oncocytomas is the cellular arrangement on cell block preparations. Tumor cells of oncocytomas are arranged in round circumscribed nests, whereas tumor cells of chromophobe RCCs are arranged in “endless sheets.”
-
A-41. (d) Urothelial cell carcinoma
Cercariform cells are urothelial cells with elongated cytoplasm and flared cytoplasmic ends. They are tadpole-like cells and a characteristic of urothelial cell carcinomas. Other cytological findings of urothelial cell carcinomas include large tumor cells with hyperchromatic nuclei, dense chromatin, inconspicuous nucleoli, and dense cytoplasm. In metastatic melanoma, tumor cells are usually arranged in loose clusters or dispersed individual cells. The nuclei of tumor cells are eccentrically located (plasmacytoid appearance), highly variable in size with finely to coarsely granular chromatin, and a single prominent cherry-red nucleoli. Cytoplasmic melanin pigments may also be present. In benign renal tubular cells, particularly proximal tubular cells, they are arranged in loosely formed sheets and have round nuclei, fine chromatin, small nucleoli, abundant granular cytoplasm, and indistinct cytoplasmic border. Cells also reveal minimal nuclear variations and normal N:C ratios. In metastatic squamous cell carcinomas, polygonal tumor cells have large nuclei, smudgy chromatin, and dense cytoplasmic keratin formation.
-
A-42. (b) Monomorphous population of cells
The FNA of a lymphoma reveals a cellular specimen with monomorphous population of lymphocytes, particularly in low-grade B cell lymphoma, and/or small lymphocytic lymphomas/chronic lymphocytic leukemia (SLL/CLL). It represents a monoclonal proliferation of lymphoma cells. Other cytological features of a lymphoma include discohesive tumor cells with hyperchromatic nuclei, clumped (soccer-ball-like) chromatin, irregular nuclear membranes, inconspicuous nucleoli, scant cytoplasm, and rare or absent tingible body macrophages. Reactive lymphoid hyperplasia contains a heterogeneous mixture of lymphocytes, including small lymphocytes, centrocytes/centroblasts, immunoblasts, tingible body macrophages, and other cells. There is a great variation of cellular sizes and appearances, characteristic of polymorphous population of cells. Lymphoglandular bodies can be seen in both lymphomas and reactive lymphocytes.
-
A-43. (a) Bland nuclei and abundant granular cytoplasm
Wilms’ tumor is a rare tumor of infancy and childhood. Histologically, the tumor contains blastemal component (closely packed small blue cells) and mesenchymal component (spindle cells). Therefore, it may be confused with the other so-called small blue round cell tumors, such as Ewing/PNETs, rhabdomyosarcomas, and small cell carcinomas. In the FNA specimen of Wilms’ tumor, numerous discohesive small round blue cells are found and arranged in tubular-like structure and dispersed individual cells. Tumor cells have hyperchromatic nuclei and scant cytoplasm. The mesenchymal cells are elongated spindle-shaped cells. In rhabdomyosarcoma, tumor cells have more eosinophilic cytoplasm. In Ewing/PNET, tumor cells are more pleomorphic and reveal a tigroid appearance. In small cell carcinomas, tumor cells reveal acinar/rosette arrangements with hyperchromatic nuclei, fine (salt-and-pepper) chromatin, inconspicuous nucleoli, scant cytoplasm, nuclear crowding, and molding.
-
A-44. (d) All of the above
The clear cell RCC variant (conventional renal cell carcinomas) is the most common histologic subtype of malignant renal tumors and accounts for 70 % of renal cell carcinomas. The “clear cell” appearances of tumor cells are due to the cytoplasmic glycogen and lipid that are dissolved during tissue processing. In RCCs, particularly in clear cell RCCs, tumor cells are arranged in clusters or dispersed individual cells and have round- to oval-shaped hyperchromatic nuclei; granular chromatin, with or without prominent nucleoli (depending on the Fuhrman grade); and clear or granular cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain. Focally, tumor cells may also show large hyperchromatic nuclei, multinucleation, and eosinophilic cytoplasm. Tumor necrosis may be seen, particularly in the Fuhrman grade III and IV tumors. The background of smear is bloody and with prominent small vessels (hypervascularity).
-
A-45. (b) Discohesive and/or dispersed individual large atypical cells
In DLBCL, the FNA reveals a cellular specimen with discohesive large atypical lymphoid cells. Three morphological variants are most commonly seen: the centroblastic, immunoblastic, and anaplastic variant. Centroblastic variant is the most common subtype and reveals medium- to large-sized tumor cells with high N:C ratio, oval or round nuclei, fine chromatin, and single or multiple prominent nucleoli. Immunoblasts have basophilic cytoplasm and a central nucleolus. The third morphologic variant, anaplastic variant, consists of large tumor cells with pleomorphic nuclei and may resemble the Hodgkin cells (Reed-Stemberg cells). Most cases are mixtures of centroblastic and immunoblastic cells.
-
A-46. (a) Tumor cells with bland nuclei and abundant granular cytoplasm
In urothelial cell carcinomas, tumor cells are large in size and arranged in two-dimensional clusters and dispersed individual cells with large hyperchromatic nuclei, dense chromatin, inconspicuous nucleoli, and dense cytoplasm. Some of the tumor cells with elongated cytoplasm and flared cytoplasmic ends form the so-called cercariform cells, characteristics of urothelial cell neoplasm. The cercariform appearance is the result of pseudostratification of urothelial cells.
-
A-47. (d) All of the above
There is some morphological overlapping between adrenal cortical adenomas and carcinomas. Adrenal cortical adenomas contain normal-appearing adrenal cortical cells, which are arranged in small sheets and dispersed individual cells. Tumor cells have small round nuclei, granular chromatin, small centrically located nucleoli, and abundant clear and/or granular cytoplasm. No mitosis is identified. Numerous naked nuclei floating in a frothy granular background are also characteristics. Tumor necrosis is not a common finding in adrenal cortical adenomas. Histologically, the diagnosis of adrenal cortical carcinomas requires to follow strict criteria, such as nuclear grade, necrosis, capsular invasion, mitotic rate, and atypical mitoses. These features are difficult to evaluate on a cytological specimen. Nevertheless, most of the adrenal masses can be correctly classified as benign or malignant by FNAs. In adrenal cortical carcinomas, FNA reveals a cellular specimen. Tumor cells are arranged in loose clusters, sheets, and dispersed individual cells and have marked nuclear variations and atypia, abundant mitoses, and necrotic debris.
-
A-48. (a) Three-dimensional clusters of cells with bland nuclei and abundant granular cytoplasm
Pheochromocytoma is rarely aspirated due to the risk of hypertensive crisis. However, about 10 % of tumors are nonfunctional and may be aspirated. The FNA specimen reveals dispersed pleomorphic tumor cells with large hyperchromatic nuclei, granular chromatin, prominent nucleoli, and dense cytoplasm. Giant tumor cells with multinucleation and bizarre tumor cells are also common findings. Numerous mitoses may be present. Tumor cells are positive for chromogranin and synaptophysin. Pheochromocytomas can behave in a benign or malignant fashion; morphology is not always predictive of clinical behaviors.
-
A-49. (c) Small pyknotic nuclei
In metastatic squamous cell carcinomas, tumor cells are predominately arranged in clusters and/or dispersed as individual tumor cells. Tumor cells have large nuclei with smudgy or coarse chromatin, prominent nucleoli, and dense cytoplasm with cytokeratins. Pyknotic nuclei are features seen in benign squamous cells and usually not seen in squamous cell carcinomas. The presence of prominent nucleoli should not be confused with poorly differentiated adenocarcinomas. Tumor cells of adenocarcinomas have vesicular nuclei, coarse chromatin, and vacuolated cytoplasm.
-
A-50. (a) Oncocytoma
In oncocytomas, tumor cells reveal bland round nuclei with fine chromatin, inconspicuous or small nucleoli, abundant dense granular cytoplasm, and distinct cytoplasmic borders. Benign renal tubular cells, particularly proximal tubular cells, have a uniform appearance with round nuclei, fine granular chromatin, small nucleoli, abundant granular or clear cytoplasm, and indistinct cytoplasmic borders. Cells also reveal minimal nuclear variations and normal N:C ratios. In clear cell RCCs, tumor cells form cohesive two-dimensional clusters and have large eccentrically placed nuclei, vesicular chromatin, and clear cytoplasm. Intercellular pink color strand-like material (basement membrane material) may be seen by the Diff-Quik stain. Nucleoli vary in size depending on the Fuhrman grade. In papillary RCCs, tumor cells form papillae with true fibrovascular cores and reveal dense nuclei and scant-to-moderate granular or clear cytoplasm. Type 1 variant of papillary RCC reveals mild nuclear atypia, and type 2 variant reveals marked nuclear atypia. Foamy macrophages may also be identified in the background.
Reading List
Argani P, Lal P, Hutchinson B, et al. Aberrant nuclear immunoreactivity for TFE3 in neoplasms with TFE3 gene fusions: a sensitive and specific immunohistochemical assay. Am J Surg Pathol. 2003;27:750–61.
Bibbo M, Wood MD, Fitzpatrick BT. Peritoneal washings and ovary. In: Bibbo M, Wilbur D, editors. Comprehensive cytopathology. 3rd ed. Philadelphia: Saunders/Elsevier; 2008.
Cibas ES. Peritoneal washings. In: Cibas ES, Ducatman BS, editors. Cytology: diagnostic principles and clinical correlates. Philadelphia: Saunders/Elsevier; 2009.
DeMay RM. The art and science of cytopathology, exfoliative cytology, vol. 1. 2nd ed. Chicago: ASCP Press; 2012.
Dusenbery D, Dekker A. Needle biopsy of the adrenal gland: retrospective review of 54 cases. Diagn Cytopathol. 1996;14:126–34.
Jhala NC, Darshana J, Eloubeidi MA, Chhieng DC, Ralph Crowe D, Janie R, Isam E. Endoscopic ultrasound-guided fine-needle aspiration biopsy of the adrenal glands. Cancer Cytopathol. 2004;102:308–14.
Khalbuss WE, Monaco SE, Pantanowitz L. Chapter 20. Renal, adrenal & retroperitoneum. In: The ASCP Quick Compendium (QC) of cytopathology. Chicago: ASCP Press; 2013. p. 448–83.
Lam KY, Lo CY. Metastatic tumors of the adrenal glands: a 30-year experience in a teaching hospital. Clin Endocrinol (Oxf). 2002;56:95–101.
Powers CN, Elbadawi A. “Cercariform” cells: a clue to the cytodiagnosis of transitional cell origin of metastatic neoplasms? Diagn Cytopathol. 1995;13:15–21.
Raso DS, Greene WB, Finley JL, Silverman JF. Morphology and pathogenesis of Liesegang rings in cyst aspirates: report of two cases with ancillary studies. Diagn Cytopathol. 1998;19:116–9.
Subhawong AP, Subhawong TK, Li QK. Fine needle aspiration of a metastatic prostate carcinoma simulating a primary adrenal cortical neoplasm: A case report and review of literature. Diagn Cytopathol. 2010;38:147–53.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Li, Q.K., Khalbuss, W.E. (2015). Renal and Adrenal Fine-Needle Aspiration. In: Khalbuss, W., Li, Q. (eds) Diagnostic Cytopathology Board Review and Self-Assessment. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1477-7_10
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1477-7_10
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1476-0
Online ISBN: 978-1-4939-1477-7
eBook Packages: MedicineMedicine (R0)