
Abstract
Vascular disease usually involves arterial stenosis, aneurysms, and dissections caused by atherosclerosis. The high prevalence of atherosclerosis ensures that most general surgeons have experience managing patients with traditional vascular disease. In contrast, non-atheroslcerotic disorders affecting the arteries and veins occur less frequently and may not be familiar to most clinicians. Left untreated, non-atherosclerotic vascular conditions can have serious and potentially fatal consequences. This chapter reviews clinically relevant non-atherosclerotic vascular diseases including hypercoagulable states, popliteal entrapment syndrome, Buerger’s disease, vasculitis, and fibromuscular dysplasia. Patients with these disorders differ from traditional vascular patients by age, comorbidities, presentation, and treatment. A basic understanding of non-atherosclerotic vascular disease can help general surgeons recognize and appropriately manage patients with these rare conditions.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Hypercoagulable Disorders
Introduction
Hemostatic disorders increase the risk of perioperative and intraoperative complications. For patients with hypercoagulable states, the risk of venous thromboembolic (VTE) complications depends on the specific abnormality as well as the presence of additional stressors such as surgical intervention and immobilization. Table 22.1 shows the risk of the first VTE episode associated with various hypercoagulable states [1]. Approximately 60–80 % of patients with decreased anticoagulant activity have a VTE episode by 45 years of age [2]. Abnormalities that affect the arterial system are also relevant to surgeons who treat patients with arterial disease, including, for example, patients who require arteriovenous access for hemodialysis (Table 22.2) [3–5]. Although patients with bleeding disorders should also be assessed preoperatively, these conditions are not covered in this chapter.
Normal hemostasis involves a series of events culminating in platelet plug formation and thrombin generation. Abnormalities at any stage of this cascade can increase the risk of abnormal bleeding or thrombosis. Hypercoagulable disorders result from either an increase in procoagulant activity or a decrease in anticoagulant activity. Although abnormalities associated with decreased anticoagulant are rare, occurring in less than 1 % of the population, they place patients at higher risk for thrombosis than the more commonly encountered disorders associated with increased procoagulant activity [6].
Despite being recognized for centuries, the first hereditary hypercoagulable state, antithrombin deficiency, was not characterized until 1965 [7]. Over the last 50 years, additional hypercoagulable disorders have been identified including: protein C deficiency, protein S deficiency, factor V Leiden (or activated protein C resistance), prothrombin gene mutation (or G20210A), dysfibrinogenemia, and hyperhomocysteinemia. It is clear that other coagulation disorders exist but remain unspecified and undetectable by the currently available diagnostic tests. Therefore, patients with prior clotting episodes or a strong family history of thrombosis despite “negative” workups should be considered at higher risk for thrombosis when they are placed in prothrombotic situations such as surgery.
Hypercoagulable testing should be considered for patients with unexplained, recurrent, or atypically located VTE and for patients with a strong family history of VTE. Testing should generally be delayed until the thrombotic episode has resolved and the patient can safely stop anticoagulation. Most hypercoagulable disorders cannot be detected during the acute phase of thrombosis or during active anticoagulation therapy (Table 22.3). Patients with a VTE that was provoked by temporary or ongoing prothrombotic conditions usually do not benefit from hypercoagulable testing. Aside from hypercoagulable disorders, unexplained arterial or venous thromboembolism also raises the possibility of an occult cancer. Likewise, patients with a prior history of malignancy who develop a first-time or recurrent VTE episode should be assessed for cancer recurrence.
Reduced Level of Anticoagulants
Antithrombin (AT) Deficiency
The clinical manifestation of AT deficiency is usually deep vein thrombosis (DVT), but it can also cause arterial thromboses on rare occasions. AT deficiency increases the risk of a first-time VTE event by 20-fold [8]. Since AT acts as a cofactor for heparin, patients with AT deficiency often require excessively high doses of heparin to achieve therapeutic anticoagulation. Resistance to anticoagulation with heparin raises the possibility of AT deficiency and should prompt further testing. Unfortunately, diagnosing AT deficiency at the time of the acute VTE event is usually impossible because AT levels normally decrease in the postoperative and postpartum periods and during anticoagulation with heparin and sometimes warfarin. Assessment for AT deficiency should therefore be pursued after the acute thrombotic event has resolved and the patient has stopped anticoagulation therapy. Subclassifications of AT deficiency describe the underlying pathophysiology and include reduced AT activity levels, reduced AT antigen and activity levels, and a defective heparin-binding site.
Protein C Deficiency
Patients with Protein C deficiency have a tenfold increased risk of VTE and frequently develop recurrent DVT [9]. As a vitamin K-dependent enzyme produced in the liver, protein C is affected by liver disease, disseminated intravascular coagulation (DIC), and warfarin therapy [10]. Warfarin decreases protein C levels more quickly than it inhibits procoagulant factors (Factors II, VII, IX, and X) making patients with protein C deficiency temporarily hypercoagulable and at risk for warfarin-induced skin necrosis. Preventing this complication is the rationale behind overlapping heparin and warfarin therapy during the initial stages of anticoagulation. Testing for protein C deficiency should occur after the VTE event has resolved and the patient has stopped taking oral anticoagulation. Antigen or activity levels can be used to detect protein C deficiency.
Protein S Deficiency
Protein S deficiency is associated with DVT which can occur in atypical locations [11, 12]. Protein S functions as a cofactor for protein C, and patients with protein S deficiency have a comparable thrombotic risk to those with protein C deficiency [9]. Like protein C, protein S is a vitamin K-dependent enzyme produced by the liver. Patients with protein S deficiency are therefore at risk for warfarin-induced skin necrosis if they are not appropriately transitioned from heparin to warfarin therapy. Although protein S deficiency is a hereditary disorder, functional deficiencies can occur during inflammatory states due to increased C4b-binding protein which lowers free protein S levels. Other conditions that can lower protein S levels include liver disease, DIC, pregnancy, estrogen hormonal therapy, and acute VTE. Tests for protein S deficiency usually measure total protein S activity or free activity levels and should be performed after cessation of anticoagulation therapy.
Increased Levels of Procoagulants
Factor V Leiden
Factor V Leiden or activated protein C resistance is the most commonly identified hereditary disorder associated with VTE. The vast majority of thrombotic complications from this disorder involve DVT and pulmonary emboli (PE) [13]. Homozygotes for Factor V Leiden have a 50-fold increased risk of VTE and account for about 1.5 % of VTE events [14]. Factor V Leiden heterozygotes have a fourfold increased risk of VTE and account for 16 % of first-time VTE events and 7 % of all cases of VTE (initial and recurrent) [15–17]. Factor V Leiden predominantly affects Caucasians, with people of Scandinavian origin having the highest prevalence [18]. Some studies suggest that an acquired form of Factor V Leiden can also develop with estrogen use, pregnancy, and elevated levels of Factor VIII [19–22]. The risk of VTE associated with Factor V Leiden deficiency increases in the presence of other hypercoagulable states, including hyperhomocysteinemia, prothrombin gene mutation, protein C or S deficiency, and AT deficiency [23–27]. Prolonged airplane travel, immobility, and surgical interventions can also provoke thrombotic episodes. The laboratory diagnosis of Factor V Leiden involves a second-generation clotting assay which is 85 % specific and 100 % sensitive and usually requires PCR or genetic testing for confirmation [14, 28]. Diagnostic testing is not affected by the presence of an acute thromboembolic episode and may be performed at any time.
Prothrombin Gene Mutation
Patients with prothrombin gene mutation have a 2.5-fold increased risk for VTE [29]. Simioni and Ridker estimated a twofold increased risk of recurrent VTE similar to Factor V Leiden; however, other reports contradict this finding [30–33]. Patients with prothrombin gene mutation are also at increased risk for arterial complications associated with the coronary or cerebrovascular systems [34]. The disorder is essentially nonexistent in African American and Asian populations, and diagnostic testing is not affected by acute VTE [35].
Elevated Factors VIII, IX, and XI
Elevated levels of Factors VIII, IX, and XI can result in lower extremity DVT or PE [36]. Diagnosing these disorders can be challenging because common conditions such as bleeding and inflammation normally increase the levels of procoagulant factors. Laboratory tests to measure Factor VIII, IX, and XI levels should be performed in conjunction with an ESR or CRP to evaluate for concomitant inflammation [37, 38]. If the ESR or CRP levels are also elevated, the procoagulant factor levels must be considered nondiagnostic because of the potentially confounding presence of inflammation. Confirming that elevated levels of Factors VII, IX, and XI reflect a hypercoagulable state and not a temporary, acquired abnormality requires two tests at different time points demonstrating procoagulant factor elevations above the 90th percentile.
Hyperhomocysteinemia
Hyperhomocysteinemia increases the risk of peripheral arterial disease, as well as arterial and venous thrombosis [39–42]. Several studies reported a 2–8-fold increased risk of stroke and myocardial infarction in patients with hyperhomocysteinemia [43, 44]. Although vitamin and folate replacement can reduce serum levels of homocysteine, normalizing the laboratory value of homocysteine does not affect clinical outcome or reduce cardiovascular risk. The only purpose of diagnosing hyperhomocysteinemia is to identify patients at higher risk for cardiovascular and thrombotic events. Patients with atypical arterial thromboses or premature atherosclerosis warrant an evaluation for hyperhomocysteinemia; however, measuring homocysteine levels in patients with VTE is not usually indicated.
Acquired Hypercoagulable States
Antiphospholipid Antibody Syndrome
Antiphospholipid antibody syndrome usually causes recurrent miscarriages in young women or lower extremity DVT; however, this syndrome also increases the risk of arterial thrombosis [45, 46]. The risk of recurrent VTE increases 4–7.7-fold after the initial episode, with the recurrence frequently localized to the site of the initial event [47–49]. Depending on the subtype of antiphospholipid antibody syndrome, the risk of initial DVT can be as high as 3.6-fold [50]. First-time VTE risk increases up to tenfold in patients who have antiphospholipid antibody syndrome and other concomitant hypercoagulable conditions [50]. Laboratory examination for antiphospholipid antibody syndrome involves two different assays: anticardiolipin antibody for IgG and IgM antibodies and anti-β2 glycoprotein 1 screening. Although ongoing infection and underlying malignancy can create erroneous test results, the presence of acute VTE does not affect test accuracy.
Cancer
In 1865, Trousseau first recognized that cancer increased the risk of VTE. The most common thrombotic manifestations of cancer are DVT and PE, and the risk of VTE ranges from 7- to 20-fold for patients with metastatic disease on chemotherapy [51, 52]. Multiple factors influence the risk of thrombotic complications in patients with cancer including: the type and stage of cancer, surgical vs. chemotherapy, comorbid conditions, immobility, and presence of central venous catheters. Some cancers cause vascular complications by exerting extrinsic compression on adjacent blood vessels. The risk of arterial thrombosis and embolization also increases in cancer patients including cerebral, myocardial, and peripheral thromboembolic episodes.
Low-molecular-weight heparin (LMWH) is more effective than warfarin at preventing thrombotic recurrence or propagation in patients with cancer [53, 54]. Patients with VTE and active cancer should be therefore maintained on long-term LMWH. Although newer anticoagulants may be equally effective in patients with cancer, more supporting data is required before they can be recommended for widespread use. Anticoagulation therapy in patients with cancer must be carefully monitored as bleeding complications occur more frequently in this population [55].
No specific testing for hypercoagulable conditions is recommended for cancer patients.
Pregnancy
Hypercoagulable disorders associated with pregnancy are the leading cause of maternal death in the United States with over half of the VTE episodes occurring postpartum [56–58]. Pregnancy creates a prothrombotic state by increasing fibrinogen and Factor VIII levels while decreasing fibrinolytic activity and the level of protein S. As the gravid uterus enlarges, it compresses the inferior vena cava and the left iliac vein which explains why the majority of DVTs during pregnancy occur in the left lower extremity [59–62]. Patients with any inherited coagulation disorder have a markedly increased risk of DVT during pregnancy and the postpartum period [63]. Hellgren et al. reported that 60 % of pregnant patients with VTE had Factor V Leiden deficiency [19]. Patients who develop VTE during pregnancy should be assessed for underlying hypercoagulable disorders to assess their overall thrombotic risk status and to determine the risk of recurrent VTE during future pregnancies.
Heparin-Induced Thrombocytopenia (HIT)
Patients with HIT develop heparin-induced antibodies directed against platelet factor-4. The antibodies trigger the activation and aggregation of platelets which ultimately releases prothrombotic platelet particles into the circulation. The clinical manifestation of HIT can include either venous or arterial thrombosis despite low levels of platelets [64]. HIT typically occurs 3–5 days after exposure to unfractionated heparin; however, HIT can also occur following treatment with LMWH. In patients with prior heparin exposure, HIT can occur as early as 24 h after receiving heparin.
All patients being treated with any form of heparin should have platelet monitoring for at least 5 days. The diagnosis of HIT should be considered in patients who develop thrombocytopenia or have a significant decrease in the platelet count after exposure to heparin. Any thrombotic event that occurs after heparin initiation should also raise the possibility of HIT. If HIT is suspected on clinical grounds, all forms of heparin should be stopped immediately and anticoagulation should continue using a direct thrombin inhibitor (argatroban, lepirudin) or anti-Xa inhibitor (fondaparinux). If HIT is confirmed, anticoagulation should transition to warfarin only when the platelet count normalizes. Testing for HIT can include a serotonin release assay or enzyme-linked immunosorbent assay (ELISA) which has a diagnostic accuracy approaching 100 % when used in combination [65].
Clinical Management
All surgeons regularly encounter patients suspected of having a hypercoagulable disorder. Effective management of these patients must address the following issues: thromboprophylaxis for patients undergoing procedures, appropriate length of treatment for patients who have a VTE, and indications for and timing of testing to diagnose hypercoagulable states.
Thromboprophylaxis
At least half of VTE events that occur in patients with hypercoagulable disorders are provoked by the clinical circumstances. This finding suggests that thromboprophylaxis could reduce the incidence of VTE for hypercoagulable patients who face clinical settings which are associated with an increased thrombotic risk such as surgery and immobility [9, 14, 66]. Multiple guidelines attempt to stratify the VTE risk of patients to determine the appropriate thromboprophylaxis for surgical procedures [67, 68]. Mechanical thromboprophylaxis includes early ambulation and intermittent compression stockings, while pharmacologic thromboprophylaxis typically involves unfractionated heparin, LMWH, or anti-Xa inhibitors. Current American College of Chest Physicians (ACCP) guidelines provide comprehensive recommendations for thromboprophylaxis based on the type of surgical intervention and risk stratification of the patient [69]. These consensus-based guidelines are updated every few years and should be familiar to all surgeons. Approximately one half of VTE events occurring in young patients are associated with inherited hypercoagulable states [70]. Estrogen replacement and hormonal methods of birth control add to the hypercoagulable state and should be avoided in this high-risk patient population [66].
Duration of Therapy
The optimal duration of anticoagulation for patients with hereditary hypercoagulable disorders varies depending on the clinical scenario. The average risk of recurrent VTE is about 5 %, and recurrence seems to be lower for patients with a provoked vs. spontaneous VTE [70]. Patients with a provoked VTE due to transient thrombotic risk factors such as surgery should be treated with a finite period of anticoagulation of 3–6 months [67]. In contrast, current treatment recommendations for patients with a spontaneous VTE are less specific ranging from 2 years to lifelong anticoagulation [32, 67]. The risk of bleeding complications and the high cost of therapy make lifelong anticoagulation an unappealing treatment option [71, 72]. Warfarin has a 3 % risk of significant bleeding per year and a 0.6 % risk of a fatal hemorrhage [6]. Since patients with hypercoagulable disorders have a less than 3 % risk of primary VTE, the risk-benefit calculation usually comes out against lifelong anticoagulation. Based upon these assumptions, few patients have an absolute indication for lifelong anticoagulation.
Regardless of whether the thrombotic episode was provoked or spontaneous, the majority of patients with hypercoagulable disorders should be treated in a similar fashion to patients without clotting abnormalities. This universal treatment strategy is based on the hypothesis that most, if not all patients, who develop thrombotic complications have abnormalities in the clotting cascade and that most, if not all, episodes of VTE are provoked. The only difference in clinical scenarios may be the clinician’s ability to diagnose the hypercoagulable disorder or detect the often subtle instigating event [73].
Testing
Diagnosing hereditary hypercoagulable disorders may be more important for the family and progeny of the affected individual. Knowledge of an increased VTE risk can help determine the need for thromboprophylaxis in patients who face high-thrombotic-risk situations such as pregnancy, hormone use, surgery, and prolonged air travel. Testing for hereditary hypercoagulable disorders should be considered in several scenarios listed in Table 22.4. Prophylactic anticoagulation is not recommended for asymptomatic individuals found to have hypercoagulable states.
Popliteal Artery Entrapment
Introduction
Popliteal artery entrapment syndrome (PAES) encompasses a group of anatomic anomalies that cause compression of the popliteal artery and occasionally the popliteal vein. The hemodynamically significant stenosis that occurs in PAES usually manifests as claudication but can cause progressive ischemia and limb loss if not diagnosed and appropriately treated. Stuart first described the anatomy of popliteal artery entrapment in 1879, but the associated clinical manifestations of PAES were not recognized until 1958 [74, 75]. Although the incidence remains unclear, PAES appears to be the most common cause of claudication symptoms in young people. Bouhoutsos et al. reported a 0.165 % prevalence of PAES in young men entering the Greek military while Turnipseed et al. reported that PAES caused atypical claudication in 0.15–4 % of young patients, and Gibson et al. reported a 3.5 % prevalence of PAES in postmortem specimens [76–79].
Pathophysiology
During embryologic growth, the popliteal artery normally develops after the medial head of the gastrocnemius muscle has migrated to the medial femoral condyle. Derangements in the timing and sequence of these events lead to the various types of PAES. Abnormally, early development of the popliteal artery or delayed migration of the medial head of the gastrocnemius causes compression and medial displacement of the artery by the gastrocnemius muscle (Type I). In Type II PAES, early development of the popliteal artery interferes with the normal migration of the medial head of the gastrocnemius muscle causing abnormal muscle insertion into the femur. If mesodermal remnants of the medial head of the gastrocnemius fail to involute, they form abnormal fibrous bands or muscle slips that compress the popliteal artery (Type III). These bands can attach to the femoral condyles or the intercondylar space. The rarest form of PAES, Type IV, involves persistence of the primitive axial artery which is compressed by the popliteus muscle. Compression of the vein and artery by any mechanism is classified as Type V.
Type VI PAES can be a catch all term for other anatomic variants or it can designate functional popliteal artery entrapment. The term functional PAES is usually applied when none of the anatomic abnormalities are present, but arterial compression is documented by radiologic imaging during positions of stress or activity. The etiology, incidence, natural history, and treatment of functional PAES remain controversial. Leading theories regarding the pathophysiology of functional entrapment speculate that compression results from muscular hypertrophy or the soleal sling [80]. Pillai et al. reviewed MRI findings and found that patients with functional PAES had more extensive attachment of the medial head of the gastrocnemius muscle to the midline of the bone and the intercondylar notch as well as greater muscle bulk adjacent to the neurovascular bundle [81]. Other imaging studies have questioned the clinical relevance of functional PAES by showing that some form of compression occurs in up to 80 % of healthy adults during forced plantar flexion of the foot [80, 82, 83].
Regardless of the mechanism or PAES type, external compression of the popliteal artery gradually damages the vessel leading to fibrotic occlusion in advanced stages. As the popliteal artery slowly narrows, some patients form a poststenotic aneurysm with thrombus formation and distal embolization. Tibial nerve involvement has also been reported.
Clinical Presentation
PAES should be considered in patients younger than 50 who present with claudication or exertional calf muscle pain. The majority of patients with PAES present before 30 years of age and the male-to-female ratio is about 2:1 [84]. Roche-Nagle et al. found that young athletes participating in basketball, football, rugby, or martial arts were most commonly affected by PAES and 25 % of patients had bilateral involvement [85, 86].
All forms of PAES cause repetitive trauma to the artery which can potentially lead to aneurysmal degeneration, thrombosis, or distal embolization. The clinical signs and symptoms depend on the stage at which the patient seeks medical attention. A delayed presentation of PAES frequently occurs when young patients dismiss muscle cramps as a sign of being “out of shape” and primary care physicians overlook early signs and symptoms of arterial insufficiency. If weakness, paresthesias, and edema are also present, PAES may involve simultaneous nerve and or vein compression. In some patients, the discomfort caused by walking paradoxically improves with more vigorous exercise. These atypical claudication symptoms can create a confusing clinical picture causing further delays in the diagnosis of PAES.
Claudication symptoms due to PAES may not occur until the patient has walked for miles. The onset of exertional leg pain depends on the extent of arterial compression and the physical conditioning of the patient. Due to their young age, long walking distance, and lack of atherosclerotic risk factors, many patients with PAES are initially referred to orthopedic or sports medicine physicians, and a vascular etiology for their symptoms is not considered until late in the course of disease. The sudden onset of severe claudication usually signifies acute occlusion of the popliteal artery. Although critical limb ischemia (CLI) can result from popliteal artery occlusion or emboli to the tibial vessels, only 20 % of patients with PAES present with symptoms of CLI [87, 88]. In most patients, the entrapped popliteal artery undergoes gradual injury allowing time for collateral formation, similar to that seen in atherosclerotic occlusive disease.
The differential diagnosis of PAES should include compartment syndrome and popliteal adventitial cystic disease. Eliminating adventitial cystic disease from the differential diagnosis is usually straightforward since it does not have a predisposition to athletes and usually occurs in less active young patients. Several studies reported that PAES was the cause of symptomatic claudication in up to 60 % of young athletes [87, 89]. In contrast, Turnipseed et al. found that functional entrapment accounted for only 4 % of cases of claudication in young patients with chronic compartment syndrome causing the majority of symptoms [79]. Different referral patterns may explain the contradictory conclusions reached by these studies. Other non-atherosclerotic vascular complications in young, otherwise, healthy athletes can include exercise-induced fibrosis of the external iliac artery most often described in avid cyclists and arterial thoracic outlet syndrome that can occur in baseball pitchers and other athletes engaged in repetitive overhead arm motion.
Diagnosis and Treatment
Patients with PAES typically have palpable pedal pulses at rest which decrease or disappear with active plantar flexion of the foot. Any patient with suspected PAES should undergo exercise testing in the noninvasive vascular lab. Unless the patient is presenting with an advanced stage of entrapment, the popliteal and tibial arteries should have normal triphasic waveforms when the leg is in the neutral position. Active knee extension and forced plantar flexion of the foot occlude the popliteal artery in most patients with PAES. Likewise, a normal ABI at rest (greater than 1.0) should fall to less than 0.9 with exercise in patients with PAES. Well-conditioned athletes with PAES may need to perform more vigorous exercise than the standard vascular lab protocol to induce changes in ABI. Similarly, patients with functional entrapment frequently are usually athletes who develop symptoms at distances measured in miles, not blocks.
MRA or CTA imaging studies can confirm the diagnosis of PAES, identify specific muscular or tendinous abnormalities, and detect the presence of aneurysmal degeneration which warrants repair of the artery. Assessment of the contralateral limb should also be performed as the prevalence of bilateral PAES ranges from 30 to 67 % [90–93]. Angiography usually helps determine whether an arterial bypass is necessary by assessing the extent of intimal damage and identifying distal runoff vessels. All diagnostic modalities should attempt to reproduce the popliteal artery compression that occurs during exercise. Unless the popliteal artery is already occluded or anatomic abnormalities for PAES identified, images of the leg in neutral position should be compared to images obtained with forced active dorsiflexion of the foot against resistance with the knee fully extended. Failure to perform these maneuvers may lead to a false-negative result. Eliminating compartment syndrome from the differential diagnosis may involve taking pressure measurements in the muscle compartments of the lower leg. Left untreated, PAES can acutely occlude the popliteal artery which causes severe, short-distance claudication. DiMarzo et al. and Levien also found a higher rate of distal embolization in patients who had delayed diagnosis and treatment of PAES [87, 94].
Functional Entrapment
In 1985, Rignault described functional popliteal artery entrapment syndrome (FPAES) in symptomatic young military recruits who had no anatomic abnormality [80]. Lower extremity MRI demonstrated compression of the popliteal artery in positions of stress which appeared to result from hypertrophy of the muscles in the popliteal fossa. Other studies confirmed the two levels of compression described by Rignault: one between plantaris and medial head of the gastrocnemius and the other between the popliteus and plantaris muscles. Turnipseed further defined FPAES by identifying hypertrophy of the gastrocnemius as the primary etiology [83, 90, 95]. Although partial resection of the medial head of gastrocnemius muscle provides symptomatic relief for patients with FPAES, Deshpande found that decreasing activity alone obviated the need for surgical intervention in patients willing to abstain from extreme athletics [96].
Treatment
Treatment for PAES should be performed by experienced surgeons with a detailed understanding and experience operating in this area. Surgery is the only effective treatment for anatomic PAES (Types I through V). Percutaneous, catheter-directed thrombolysis has a limited role in the treatment of PAES which involves restoring patency to an acutely occluded popliteal artery in anticipation of definitive surgical repair. Unlike arteries affected by atherosclerotic disease, the popliteal artery in patients with PAES is fibrotic and usually resists dilation with balloon angioplasty and stent placement. Endoluminal interventions are also destined to fail because they do not relieve the underlying problem of extrinsic compression.
All symptomatic patients with confirmed PAES should have surgery to resect the offending muscle or band. Surgery usually involves resection of the gastrocnemius medial head which can be guided by intraoperative duplex assessment of the vessel to confirm successful decompression. This procedure alone may provide definitive treatment for patients with early-stage PAES in whom the artery has not degenerated. Surgery for early-stage PAES can be performed with a posterior popliteal approach using a lazy “S” incision. An adequate length of artery should be exposed to evaluate for other fibrous compressive bands. If the medial head of the gastrocnemius muscle is causing compression of the popliteal artery or vein, it should be divided from its insertion on the medial femoral condyle. Techniques for excising the plantaris muscle, soleal sling, and popliteus muscle have also been described.
Advanced-stage PAES which causes occlusion or aneurismal dilation of the popliteal artery mandates treatment with an intersegmental arterial bypass, generally using the small saphenous or great saphenous veins as a bypass conduit. Some patients have chronic occlusion of the popliteal artery without symptoms of vein or nerve compression. These patients do not require division of the muscle bands and can be treated from a medial approach with the vein bypass tunneled subcutaneously, not anatomically.
Prophylactic intervention for patients with contralateral PAES should be performed electively if imaging studies confirm early-stage compression of the popliteal artery without vessel injury. Early surgical decompression can avoid the need for vascular repair or bypass. Surgical intervention usually allows young patients with PAES to resume their sports and athletic endeavors.
Outcomes
Follow-up information is somewhat limited to relatively small series. Kim et al. followed 22 bypasses in 18 patients with PAES dividing the patients into those with short-segment occlusions and those with occlusion extending beyond the popliteal artery [97]. Both posterior and medial surgical approaches were used in this series. Overall graft patency was 75 % at 3 and 5 years. Patients who had a bypass originating from the distal superficial femoral artery had a significantly lower patency compared to patients with a bypass originating from the above-knee popliteal artery (30 % vs. 86 % at 5 years).
A recent meta-analysis by Sinha et al. attempted to describe the clinical presentation, natural history, and treatment outcome of patients with PAES. Claudication was the most common symptom of PAES with 38 % of patients having bilateral disease, 23 % exhibiting functional entrapment, and only 11 % of patients presenting with critical limb ischemia [84]. At the time of presentation, 24 % of the popliteal arteries were occluded and 13.5 % had aneurismal degeneration. The median duration of symptoms prior to diagnosis was 12 months; however, there was no association between duration of symptoms and presence of significant arterial damage. Three studies in the meta-analysis reported outcomes on a handful of patients treated nonoperatively for PAES: 1 patient required amputation, 1 patient reoccluded 2 months after thrombolysis requiring bypass, 1 patient had persistent symptoms, and 1 patient with functional entrapment had symptom resolution. Although surgery had an overall success rate of 77 %, surgical complications included amputation, wound infection, hematoma, seroma, and deep vein thrombosis. Fewer reports exist for popliteal vein entrapment, and clinical outcomes may differ from PAES due to the predominantly female patient cohort [93, 98, 99].
Thromboangiitis Obliterans
Thromboangiitis obliterans (TAO) was first recognized in 1879, but not well described until 1908 when Leo Buerger published the pathologic findings of the disease that now bears his name. TAO or Buerger’s disease is a vasculitis characterized by segmental thrombotic inflammatory changes [100]. TAO involves medium- and small-sized arteries, which are infrapopliteal or infrabrachial in location. Three pathologic phases have been described [101].
-
1.
Acute phase which involves an occlusive cellular thrombus. Microabscesses and multinucleated giant cells may be seen.
-
2.
Subacute phase involves organization of the thrombus.
-
3.
Chronic phase characterized by organized thrombus and fibrosis. This may be more difficult to differentiate from atherosclerotic disease.
Etiology and Presentation
Despite extensive clinical and pathologic studies, the etiology of TAO remains unclear. Although tobacco use is central to the disease process, immunologic factors, hereditary disposition, and endothelial dysfunction may also play a role in the pathophysiology of TAO. Patients with TAO typically present with ischemic symptoms caused by occlusive small-vessel disease of the lower leg, forearm, or both. The most characteristic clinical scenario for TAO involves a man under the age of 40 who smokes and has digital ischemia. TAO occurs less commonly in women and rarely affects other vascular beds. Superficial thrombophlebitis and rheumatologic symptoms such as arthralgias, arthritis, and carpal tunnel syndrome have also been described as clinical manifestations of TAO [101, 102].
Diagnosis
The diagnosis of TAO begins with a thorough physical exam including palpation of distal pulses, auscultation for bruits, inspection of the digits, and evaluation for superficial venous thrombophlebitis. Ankle brachial indices (ABIs) should be obtained to detect and quantify the severity of arterial occlusive disease. A neurologic exam should be performed, as up to 70 % of patients have sensory findings [103]. Clinical diagnostic criteria for TAO include [103]:
-
Age younger than 45
-
Recent tobacco use
-
Distal extremity ischemia
-
Absence of autoimmune disease, thrombophilia, diabetes, or proximal embolic source
-
Consistent radiographic findings
Adjunctive diagnostic studies for TAO include arterial duplex, CTA, MRA, or catheter-directed angiography. These imaging studies can exclude a proximal embolic source and confirm that the occlusive lesions only involve arteries distal to the elbow or knee. Although corkscrew collateral vessels have been associated with TAO, this pattern is not specific to TAO and may occur in other types of arterial occlusive disease.
Treatment and Outcomes
Smoking cessation is the primary treatment strategy for patients with TAO. Patients who completely stop smoking have significantly more favorable outcomes than patients who continue to smoke. In a relatively large study, no amputations were performed on patients with TAO who stopped smoking, while 43 % of active smokers required an amputation [104]. Endovascular and surgical interventions have limited success in patients with TAO due to the distal nature of the disease. Small studies have described the use of vasodilators for TAO including iloprost, alpha-blockers, calcium channel blockers, and sildenafil. The use of sympathectomy to relieve the symptoms of TAO has not proven to be successful.
Vasculitis
Introduction
Vasculitis refers to inflammation of the blood vessel wall that can lead to arterial damage in the form of aneurismal degeneration or thrombosis of the involved vessel. This inflammatory process can occur in several different types of arteries affecting patients from a variety of demographic groups. Vasculitis therefore encompasses an uncommon group of disorders with a wide range of pathologic features and clinical presentations that can be challenging to concisely summarize. Despite the rarity and complexity of vasculitis, general surgeons should be familiar with the diagnosis and initial management of this group of vascular diseases. Patients with vasculitis often present with vague symptoms that require immediate recognition and appropriate treatment to avoid potentially devastating complications such as thrombosis, aneurysm rupture, blindness, and hemoptysis. Mistakenly treating vasculitis as a manifestation of atherosclerotic disease can have significant adverse consequences.
The diagnosis and management of some forms of vasculitis remains controversial with considerable disagreement between and within medical disciplines. Debate continues over even the most fundamental issues including whom to biopsy, when to initiate steroids, and how long to continue therapy. Because of this lack of consensus, surgeons often take the lead in determining the indication for a biopsy and the timing of medical treatment. Surgeons must also recognize the appropriate role for revascularization because it is clear that patients with vasculitis do not follow the same clinical course as patients with atherosclerotic disease. The following section will review the different classes of vasculitides with attention to presentation, pathophysiology, diagnosis, and treatment options. Particular attention will be paid to giant cell or temporal arteritis (GCA), as it is one of the more commonly encountered forms of vasculitis and one that stimulates considerable debate regarding diagnosis and treatment.
Classification and Pathophysiology
Vasculitis can be classified by the size of arteries it affects: large, medium, or small. Parameters to subclassify vasculitis include ANCA status (positive or negative) and patient age at presentation. The more common forms of vasculitis can be summarized as follows (some less common vasculitides have been omitted for clarity) [105]:
Large-vessel disease | |
Takayasu’s arteritis | (Age < 30) |
Giant cell (temporal) arteritis | (Age > 50) |
Medium-vessel disease | |
Kawasaki’s disease | (Age < 5) |
Behcet’s disease | (Age 20–40) |
Polyarteritis nodosa | |
Small | |
Henoch-Schonlein purpura | |
Arteritis of connective tissue disease | |
Wegener’s granulomatosis | (ANCA+) |
Large-Vessel Vasculitis
As the name implies, large-vessel vasculitis involves the aorta and its major branches; however, GCA can also affect small vessels such as the temporal, ophthalmic, retinal, and ciliary arteries. While Takayasu’s arteritis is more prevalent in the Mediterranean and Asia, GCA is more common among patients in North America [106].
An accurate diagnosis and prompt treatment is paramount to achieving a good clinical outcome in patients with GCA. Delayed treatment puts patients at risk for blindness due to ischemic optic neuropathy. Other consequences of untreated arteritis include an increased incidence of peripheral arterial disease, the development of aortic aneurysms (particularly of the ascending aorta), an increased risk of cardiovascular events, and potentially increased mortality [107]. The complex pathophysiology of GCA involves recruitment and activation of CD-4 T cells by local dendritic cells. Macrophages damage the vessel resulting in luminal narrowing. Histologic findings include granulomatous changes and multinucleated giant cells [108].
Giant Cell Arteritis Diagnosis
GCA affects patients over the age of 50 with a higher prevalence in patients in their seventh and eighth decades. Although the disease process of GCA remains poorly understood, more women are diagnosed than men (female-to-male ratio 3:1), and genetics seems to have an etiologic role. The clinical diagnosis of GCA can be challenging because patients present with a variety of signs and symptoms. Arterial occlusive disease affecting the brachial or femoral arteries in the absence of atherosclerotic disease or risk factors should raise suspicion for GCA. Patients may also have fever of unknown origin and complain of headache, jaw pain, and vision changes. The physical exam in patients with GCA may demonstrate prominent, tender temporal arteries or scalp ischemia. Biochemical markers can provide supporting evidence for diagnosis of GCA in patients with relatively nonspecific findings from the history and physical exam. Estimated sedimentation rate (ESR) greater than 50 and C-reactive protein (CRP) greater than 2.45 g/dL are both predictive of a positive biopsy result for GCA [109]. Elevated platelet counts, although nonspecific, may be predictive as well.
Ultrasonography can function as a valuable diagnostic tool for evaluating patients with suspected GCA. An ultrasound exam of the temporal arteries in patients with GCA often demonstrates a hypoechoic line within the vessel wall. This line or “halo” appears to be related to edema and inflammation and has a sensitivity of 68–73 % and a specificity of 91–100 % for the diagnosis of GCA. Specificity increases when bilateral halos are present, while sensitivity diminishes after the initiation of steroids as the halo fades away and completely disappears after 14 days of therapy [107, 110]. Given the ease, availability, and noninvasive nature, ultrasonography is an excellent starting point for diagnosing patients with GCA. A positive ultrasound exam should prompt treatment and may obviate the need for a temporal artery biopsy. A negative ultrasound result may require further evaluation depending on the clinical scenario. Other imaging studies such as MRI and PET scanning may assist in the diagnosis of GCA; however, their role in general practice remains poorly defined [106, 107].
Temporal artery biopsy was first described in 1932 and is often invoked as the gold standard for diagnosing GCA [108]. Despite the widespread use and recognition of temporal artery biopsy, this technique has several shortcomings and still generates debate regarding its necessity as a diagnostic exam. According to some studies, temporal artery biopsy has a 20–40 % false-negative rate, possibly related to the initiation of steroids before biopsy or inadequate specimen. No consensus has ever been reached regarding the minimal length of the specimen or the need for unilateral versus bilateral temporal artery biopsy. The presence of skip lesions highlights the need to obtain an adequate length of temporal artery to avoid a false-negative biopsy result.
In 1990, the American College of Rheumatologists (ACR) proposed that patients meeting three of the following five clinical criteria could be diagnosed with GCA:
-
1.
Age > 50
-
2.
New-onset headache
-
3.
Temporal artery tenderness or decreased temporal artery pulse
-
4.
ESR greater than 50 mm/h
-
5.
Abnormal temporal artery biopsy
Although the ACR guidelines suggest that a temporal artery biopsy is not always necessary, the issue has not been settled. The titles of two recent journal articles demonstrate how polarized this issue remains: “Temporal artery biopsy is not required in all cases of suspected giant cell arteritis” versus “Temporal artery biopsy: skip it at your patient’s peril” [110, 111]. A recent abstract questioned the value of a biopsy by reporting that steroids were stopped in only 36.5 % of patients with a negative biopsy result [112]. It seems hard to justify a nontherapeutic intervention that carries a small risk of facial nerve injury if the requesting physician has no intention of altering the treatment plan based on the biopsy results.
Until wider consensus can be achieved, the diagnosis of GCA requires an individualized approach. Patients with clinical findings and elevated biochemical markers consistent with GCA should begin treatment without waiting for confirmation with a temporal artery biopsy. An ultrasound exam demonstrating a halo sign can then confirm the diagnosis and a biopsy can be reserved for patients with a negative or nondiagnostic ultrasound in whom the diagnosis remains unclear. Initiating steroid treatment 2 weeks or more in advance does not appear to affect the diagnostic accuracy of a temporal artery biopsy in patients with clinical indications of active disease [113].
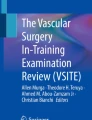
Although a temporal artery biopsy is a minor procedure, potential adverse outcomes include a nondiagnostic result and injury to the facial nerve. These complications can be avoided by adhering to a few sound techniques when performing the biopsy. To increase the diagnostic yield, the biopsy should be performed on the symptomatic side or the side with a diminished or absent temporal artery pulse. Before beginning the procedure, a Doppler probe can locate and mark the path of the temporal artery as it courses superiorly from its origin anterior to the ear [114]. Figure 22.1 shows the course of the temporal artery. Making the incision over the parietal branch of the artery within the patient’s hairline decreases the risk of injuring the facial nerve. The incision should be long enough to remove a 2–3 cm segment of the artery to ensure that an adequate sample is obtained for diagnosis [115]. Skin closure using subcuticular absorbable sutures gives the best cosmetic result.

Course of the superficial temporal artery. Danger zone delineated by box showing proximity of frontal branch of facial nerve to the frontal branch of superficial temporal artery (Illustration courtesy of Marie Kim. Iowa Head and Neck Protocols, Iowa City, IA. http://wiki.uiowa.edu/display/protocols/Home)
Giant Cell Arteritis Treatment
First described in 1953, glucocorticoid treatment for giant cell arteritis has significantly reduced the number of patients who go blind because of GCA. Steroids should be started as soon as possible because a delay of more than 24 h past symptom recognition reduces the rate of visual symptom resolution from 50 % to only 6 % [107]. The initial recommended dose of prednisone is 0.8–1.0 mg/kg/day. Protocols to taper the steroid dose usually target resolution of symptoms and normalization of biochemical markers over a time period of less than 6 months [107]. Unfortunately, steroids can cause significant side effects including diabetes, hypertension, infection, fractures, and heart failure. In some studies, high-dose steroids for longer than 6 months increased mortality, although confounding variables were present [107]. The fact that steroids are nonspecific mediators of the immune system with an unfavorable side effect profile has sparked interest in more directed medical therapy including the use of methotrexate, TNF-alpha antagonists, azathioprine, hydroxychloroquine, cyclophosphamide, dapsone, and cyclosporine. While these alternative agents can mitigate the systemic effects of GCA and prevent blindness, their ability to reduce the vascular morbidity remains unclear. Low-dose aspirin may also play a role in decreasing the rate of cerebrovascular events in patients with GCA [18].
Takayasu’s Arteritis Diagnosis
Takayasu’s arteritis involves large arteries such as the aorta and its branches, resulting in stenosis, occlusion, and aneurysm formation. One of the diagnostic criteria for Takayasu’s arteritis is age younger than 40 and most cases occur in patients 20–40 years of age [108]. Takayasu’s arteritis should be considered in young patients with unexplained bruits or decreased pulses on physical exam and in patients with hypertension related to renal artery stenosis. The initial presentation of Takayasu’s arteritis can include stroke, cerebrovascular symptoms, and upper extremity pain with exertion. Stenosis involving the lower extremity and visceral arteries and aneurysm formation are less common clinical manifestations of Takayasu’s arteritis.
Takayasu’s Arteritis Treatment
Although steroids can effectively treat Takayasu’s arteritis, symptoms often relapse during attempts to taper the steroid dose [116]. Alternative pharmaceutical agents may allow for steroid sparing and more targeted therapy; however, supporting evidence for these treatment strategies remains insufficient. Surgical intervention for Takayasu’s arteritis requires careful consideration given the increased risk of technical failure and the relatively high rates of restenosis and recurrent aneurysm. Cardiac risk in patients with Takayasu’s arteritis may also be higher than age-matched controls [117]. If surgery is necessary, it should be performed in the quiescent stage of the disease, and steroid treatment plays an important role in preoperative preparation. Significant doubt remains as to whether endovascular interventions have any role in the treatment of Takayasu’s arteritis.
Medium-Vessel Vasculitides
Several vasculitides are described below – Kawasaki’s vasculitis, Behcet’s disease, and Polyarteritis nodosa.
Kawasaki’s vasculitis is an example of a medium-vessel vasculitis that typically occurs in children younger than five although there have been reports of adult disease. The American Heart Association guidelines for the diagnosis of Kawasaki’s vasculitis include:
-
Fever of unknown origin
-
Bilateral bulbar conjunctival injection
-
Oral mucous membrane and tongue changes
-
Erythema of the palms and soles
-
Rash
-
Lymphadenopathy
The treatment for Kawasaki’s disease consists of intravenous immunoglobulin and high-dose aspirin early in the course of the disease in an effort to prevent complications such as coronary artery disease, heart failure, and coronary artery aneurysms. Echocardiography and nonspecific serum markers such as CRP can be useful in the diagnosis and monitoring of the disease process.
Behcet’s disease affects people between the ages of 20 and 40 and has a higher incidence in the Middle East. Affected arteries including the aorta, renal, pulmonary, and peripheral vessels can thrombose or become aneurismal, while veins can develop deep vein thrombosis or thrombophlebitis [18]. Many patients with Behcet’s disease have recurrent skin ulcers as well as oral and genital ulcers [116]. One of the unique diagnostic criteria for Behcet’s disease is pathergy, which is defined as development of a pustule after a prick of the skin. Like the other vasculitides, a delay in the diagnosis of Behcet’s disease can result in blindness. Immunosuppression forms the mainstay of therapy for Behcet’s disease. The benefit of long-term anticoagulation in these patients remains unclear [18].
Polyarteritis nodosa is a necrotizing vasculitis of medium vessels that can lead to thrombosis and aneurysm formation. Symptoms of mesenteric ischemia often occur.
Small-Vessel Vasculitis
Wegener’s granulomatosis is a small-vessel vasculitis characterized by necrotizing and granulomatous changes affecting arteries or veins. In addition to the general treatment strategies already discussed, statins may help reduce inflammation; however, clear evidence for this is lacking [18].
Fibromuscular Dysplasia
Introduction and Pathophysiology
Fibromuscular dysplasia (FMD) is a non-atherosclerotic, noninflammatory disease that can result in stenosis, thrombosis, emboli, and aneurysm formation in numerous arterial beds. Although FMD was first described in 1938, this disease remains poorly understood. Pathologically, FMD can be classified into one of four types based on the predominant layer of the arterial wall involved in the disease process: [118]
-
Intimal fibroplasia – A less common type that typically occurs in the younger population, intimal fibroplasia is characterized by subendothelial deposits of collagen within the intima. Radiographic findings include long, smooth stenotic segments.
-
Medial hyperplasia – The rarest type is characterized by an increase in medial smooth muscle and may appear as concentric stenosis in the mid-renal artery. Some consider this type of FMD a precursor to medial fibroplasia and therefore do not include it as a distinct category.
-
Medial fibroplasia – This type accounts for 80–90 % of diagnoses and is what most people think of when referring to “FMD.” Medial fibroplasia most commonly occurs in women between the ages of 30 and 50. Pathologically, the lesions consist of media with fibrous tissue, collagen, and ground substance. The alternating thickening and thinning of the media results in the radiographic string of beads appearance and may lead to aneurysm formation.
-
Perimedial dysplasia – The second most common type of FMD involves accumulation of elastic tissue between the media and adventitia; however, perimedial dysplasia is not associated with aneurysm formation. Perimedial dysplasia may present as multiple high-grade renal artery stenotic lesions in young patients.
Etiology and Presentation
The etiology of FMD may involve multiple factors including mechanical stress and relative ischemia to the vasa vasorum as well as patient-specific factors such as smoking, hormone levels, and genetics [119]. Although FMD can occur in numerous arterial beds, it most commonly affects the renal and cerebrovascular systems, specifically the mid to distal internal carotid artery. Screening for intracranial aneurysms should be considered, as the reported prevalence ranges from 7 to 50 % [119]. Overall, the prevalence of FMD is 4 %; however, the number of incidentally identified lesions will most likely rise as the volume and quality of radiographic studies increase [120].
Presenting symptoms for FMD vary. Olin et al. suggest that the diagnosis of FMD should be considered in patients with any of the following clinical conditions [120]:
-
Onset of hypertension <35 years of age
-
Resistent hypertension
-
Epigastric bruit and hypertension
-
Cervical bruit at <10 years of age
-
Pulsatile tinnitus
-
Severe and recurrent headaches
-
TIA or stroke in those <60 years of age
-
Peripheral dissection
-
Intracranial or visceral aneurysm
-
Aortic aneurysm in those <60 years of age
-
Subarachnoid hemorrhage
-
Renal infarction
Diagnosis and Treatment
The clinical circumstances usually raise the possibility of FMD. Imaging studies including ultrasound duplex, CTA, MRA, conventional angiography, or IVUS often demonstrate characteristic stenotic lesions further supporting the diagnosis of FMD [121]. Treatment for FMD depends on the symptoms. Asymptomatic patients should be started on aspirin 81 mg daily and educated to recognize signs and symptoms that could indicate cerebrovascular or renal disease. These patients should also be informed that FMD increases the risk of arterial dissection associated with participation in contact sports, physical activities, and chiropractic manipulations. A CT scan of the head to screen for intracranial aneurysms should be considered since patients with FMD appear to have a greater risk for these aneurysms than the general population [118]. Although it does not have strong supporting evidence, systemic anticoagulation remains a widely used treatment strategy for patients with a carotid dissection due to FMD [119]. Symptomatic arterial occlusive lesions caused by FMD respond well to percutaneous balloon angioplasty, and endovascular intervention represents a first-line therapy despite a lack of randomized controlled studies. Endovascular stent grafts have also successfully treated cerebrovascular pseudoaneurysms and aneurysms caused by FMD; however, comparative studies have not been performed. Open surgical repair and revascularization is a reasonable treatment option in patients with complex lesions that are not amenable to endovascular intervention [118].
Conclusion
Vascular disease is not always confined to elderly patients with a history of smoking and systemic atherosclerosis. Patients with non-atherosclerotic vascular disorders come from a wide range of demographic groups and have a different presentation, natural history, and treatment compared to patients with traditional vascular disease. Failure to recognize and treat these non-atherosclerotic vascular diseases can have significant and potentially fatal consequences. General surgeons who are familiar with non-atherosclerotic vascular disease can recognize and appropriately manage patients with these rare conditions.
References
Kearon C, Crowther M, Hirsh J. Management of patients with hereditary hypercoagulable disorders. Annu Rev Med. 2000; 51:169–85.
Rao AK, Sheth S, Kaplan R. Inherited hypercoagulable states. Vasc Med. 1997;2:313–20.
Ray SA, Rowley MR, Loh A, et al. Hypercoagulable states in patients with leg ischemia. Br J Surg. 1994;81:811–4.
Eldrup-Jorgensen J, Flanigan DP, Brace L, et al. Hypercoagulable states and lower limb ischemia in young adults. J Vasc Surg. 1989;9:334–41.
Donaldson MC, Weinberg DS, Belkin M, et al. Screening for hypercoagulable states in vascular surgical practice: a preliminary study. J Vasc Surg. 1990;11:825–31.
Crowther MA, Kelton JG. Congenital thrombophilic states associated with venous thrombosis: a qualitative overview and proposed classification system. Ann Intern Med. 2003;138(2):128–34.
Egeberg O. Inherited antithrombin deficiency causing thrombophilia. Thromb Diath Haemorrh. 1965;13:516–30.
Mateo J, Oliver A, Borrell M, et al. Laboratory evaluation and clinical characteristics of 2,132 consecutive unselected patients with venous thromboembolism. Results of the Spanish Multicentric Study on Thrombophilia (EMET-study). Thromb Haemost. 1997;77:444.
Van Den Belt AGM, Huisman MV, Hirsh J. Familial thrombophilia: a review analysis. Clin Appl Thromb Hemost. 1996; 2(4):227–36.
Weiss P, Soff GA, Halkin H, et al. Decline of protein C and S and factors II, VII, IX and X during the initiation of warfarin therapy. Thromb Res. 1987;45(6):783–90.
Borgel D, Gandrille S, Aiach M. Protein S deficiency. Thromb Haemost. 1997;78:351.
Clark DA, Williams WL, Marlar RA. Mesenteric vein thrombosis associated with familial deficiency of free protein S. Arch Pathol Lab Med. 1991;115:617.
Baglin T, Gray E, Greaves M, et al. British Committee for Standards in Haematology. Clinical guidelines for testing for heritable thrombophilia. Br J Haematol. 2010;149:209–20.
Rodeghiero F, Tosetto A. Activated protein C resistance and factor V Leiden mutation are independent risk factors for venous thromboembolism. Ann Intern Med. 1999;130:643–50.
Rees DC, Cox M, Clegg JB. World distribution of factor V Leiden. Lancet. 1995;346:1133–4.
Koster T, Rosendaal FR, de Ronde H, et al. Venous thrombosis due to poor anticoagulant response to activated protein C: Leiden thrombophilia study. Lancet. 1993;342:1503–6.
Leroyer C, Mercier B, Escoffe M, et al. Factor V Leiden prevalence in venous thromboembolism patients. Chest. 1997;111:1603–6.
Springer J, Villa-Forte A. Thrombosis in vasculitis. Curr Opin Rheumatol. 2012;24:1–7.
Hellgren M, Svensson PI, Dahlback B. Resistance to activated protein C as a basis for venous thromboembolism associated with pregnancy and oral contraceptives. Am J Obstet Gynecol. 1995;173:210.
Olivieri O, Friso S, Manzato F, Guella A, Bernardi F, Lunghi B, Girelli D, Azzini M, Brocco G, Russo C. Resistance to activated protein C in healthy women taking oral contraceptives. Br J Haematol. 1995;91:465–70.
Henkens CMA, van der Bom JG, van der Meer FJ. Lowered activated protein C-sensitivity ratio related to increased factor VIII-clotting activity. Thromb Haemost. 1995;74:1198–9.
Cumming AM, Tait RC, Fildes S, Young A, Keeney S, Hay CR. Development of resistance to activated protein C during pregnancy. Br J Haematol. 1995;90:725–7.
Vandenbroucke JP, Koster T, Briet E, et al. Increased risk of venous thrombosis in oral-contraceptive users who are carriers of factor V Leiden mutation. Lancet. 1994;344:1453–7.
McColl MD, Ramsay JE, Tait RC, et al. Risk factors for pregnancy associated venous thromboembolism. Thromb Haemost. 1997;78:1183–8.
Ridker PM, Hennekens CH, Selhub J, et al. Interrelation of hyperhomocyst(e)inemia, factor V Leiden, and risk of future venous thromboembolism. Circulation. 1997;95:1777–82.
Gandrille S, Greengard JS, Alhenc-Gelas M, et al. Incidence of activated protein C resistance caused by the ARG 506 GLN mutation in factor V in 113 unrelated symptomatic protein C-deficient patients. Blood. 1995;86:219–24.
Zoller B, Holm J, Svensson P, Dahlback B. Elevated levels of prothrombin activation fragment 1 + 2 in plasma from patients with heterozygous Arg506 to Gln mutation in the factor V gene (APC resistance) and/or inherited protein S deficiency. Thromb Haemost. 1996;75:270–4.
Lane DA, Mannucci PM, Bauer KA, et al. Inherited thrombophilia: part 2. Thromb Haemost. 1996;76(6):824–34.
Ridker PM, Hennekens CH, Miletich JP. G20210A mutation in prothrombin gene and risk of myocardial infarction, stroke and venous thrombosis in a large cohort of US men. Circulation. 1999; 99:999–1004.
Ridker PM, Miletich JP, Stampfer MJ, et al. Factor V Leiden and risks of recurrent idiopathic venous thromboembolism. Circulation. 1995;92:2800–2.
Simioni P, Prandoni P, Lensing AWA, et al. The risk of recurrent venous thromboembolism in patients with an Arg506Gln mutation in the gene for factor V (factor V Leiden). N Engl J Med. 1997; 336:399–403.
Kearon C, Gent M, Hirsh J, et al. A comparison of three months of anticoagulation with extended anticoagulation for a first episode of idiopathic venous thromboembolism. N Engl J Med. 1999; 340:901–7.
Eichinger S, Pabinger I, Stumpflen A, et al. The risk of recurrent venous thromboembolism in patients with and without factor V Leiden. Thromb Haemost. 1997;77(4):624–8.
Doggen CJ, Cats VM, Bertina RM, Rosendaal FR. Interaction of coagulation defects and cardiovascular risk factors: increased risk of myocardial infarction associated with factor V Leiden or prothrombin 20210A. Circulation. 1998;97(11):1037–41.
Rosendaal FR, Doggen CJM, Zivelin A, et al. Geographic distribution of the 20210 G to a prothrombin variant. Thromb Haemost. 1998;79:706–8.
Koster T, Blann AD, Briet E, et al. Role of clotting factor VIII in effect of von Willebrand factor on occurrence of deep-vein thrombosis. Lancet. 1995;345:152.
O’Donnell JO, Tuddenham EGD, Manning R, et al. High prevalence of elevated factor VIII levels in patients referred for thrombophilia screening: role of increased synthesis and relationship to acute phase reaction. Thromb Haemost. 1997;77:825.
Kamphusien PW, Eikenboom JCJ, Bertina RM. Elevated factor VIII levels and the risk of thrombosis. Arterioscler Thromb Vasc Biol. 2001;21:731.
Stampfer MJ, Malinow MR, Willett WC, et al. A prospective study of plasma homocyst(e)ine and risk of myocardial infarction in US physicians. JAMA. 1992;268:877–81.
Clarke R, Daly L, Robinson K, et al. Hyperhomocysteinemia: an independent risk factor for vascular disease. N Engl J Med. 1991;324(17):1149–55.
den Heijer M, Koster T, Bloom HJ, et al. Hyperhomocysteinemia as a risk factor for deep vein thrombosis. N Engl J Med. 1996;334:759–62.
Simioni P, Prandoni P, Burlina A, et al. Hyperhomocysteinemia and deep-vein thrombosis: a case controlled study. Thromb Haemost. 1996;76:883.
Arnesen E, Refsum H, Bonaa KH, et al. Serum total homocysteine and coronary heart disease. Int J Epidemiol. 1995;24:704–9.
Nygard O, Nordrehaug JE, Refusum H, et al. Plasma homocysteine levels and mortality in patients with coronary artery disease. N Engl J Med. 1997;337:230.
Lim W, Crowther MA. Antiphospholipid antibodies: a critical review of the literature. Curr Opin Hematol. 2007;14:494.
Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006; 4:295.
Turiel M, Sarzi-Puttini P, Peretti R, et al. Thrombotic risk factors in primary antiphospholipid syndrome. A 5 year prospective study. Stroke. 2005;36:1490.
Rosove MH, Brewer PMC. Antiphospholipid thrombosis: clinical course after the first thrombotic event in 70 patients. Ann Intern Med. 1992;117:303.
Khamashta MA, Cuadrado MD, Mukic F, et al. The management of thrombosis in the antiphospholipid antibody syndrome. N Engl J Med. 1995;332:993.
de Groot PG, Lutters B, Derksen RH, et al. Lupus anticoagulants and the risk of a first episode of deep venous thrombosis. J Thromb Haemost. 2005;3:1993.
Trousseau A. Phlegmasia Alba Dolen. In: Clinique Medicale De L’Hotel-Dieu de Paris. Paris: JB Balliere; 1865. p. 654.
Blom JW, Doggen CJ, Osanto S, Roendaal FR. Malignancies, prothrombotic mutations and the risk of venous thrombosis. JAMA. 2005;293:715–22.
Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003; 349(2):146–53.
Hull RD, Pineo GF, Brant RF, et al. LITE Trial Investigators. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am J Med. 2006; 119:1062.
Prandoni P, Lensing AW, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002;100:3484.
Heit JA, Kobervig CE, James AH, et al. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30 year population-based study. Ann Intern Med. 2005;143:697.
Andres RL, Miles A. Venous thromboembolism and pregnancy. Obstet Gynecol Clin North Am. 2001;28:613.
James AH, Tapson VF, Goldhaber SZ. Thrombosis during pregnancy and the postpartum period. Am J Obstet Gynecol. 2005; 193:216.
Faught W, Garner P, Jones G, et al. Changes in protein C and protein S levels in normal pregnancy. Am J Obstet Gynecol. 1995;172:147.
Comp PC, Thurnau GR, Welsh J, et al. Functional and immunologic protein S levels are decreased during pregnancy. Blood. 1986;68:881.
Johnson CM, Mureebe L, Silver D. Hypercoagulable states: a review. Vasc Endovascular Surg. 2005;39(2):123–33.
Ginsberg J, Brill-Edwards P, Burrows RF, et al. DVT during pregnancy: leg and trimester presentation. Thromb Haemost. 1992; 67:519.
Martinelli I, DeStafano V, Taioli E, et al. Inherited thrombophilias and first venous thromboembolism during pregnancy and puerperium. Thromb Haemost. 2002;87:791–5.
Warkentin TE. Clinical presentation of heparin-induced thrombocytopenia. Semin Hematol. 1998;35(4 Suppl 5):9.
Warkentin TE, Elavathil LJ, Hayward CP, et al. The pathogenesis of venous limb gangrene associated with heparin-induced thrombocytopenia. Ann Intern Med. 1997;127:804.
Simioni P, Sanson BJ, Prandoni P, et al. Incidence of venous thromboembolism in families with inherited thrombophilia. Thromb Haemost. 1999;81:198–202.
Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 suppl):7S–47S.
Caprini JA. Risk assessment as a guide for the prevention of the many faces of venous thromboembolism. Am J Surg. 1991; 1S:S3–10.
Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, Lassen MR, Colwell CW, American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133:381S–453.
Anderson JA, Weitz J. Hypercoagulable states. Crit Care Clin. 2011;27:933–52.
Landefeld CS, Beyth RJ. Anticoagulant-related bleeding: clinical epidemiology, prediction, and prevention. Am J Med. 1993;95: 315–28.
Palareti G, Leali N, Coccheri S, et al. Bleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative study (ISCOAT). Lancet. 1996;348:423–8.
Schafer AI, Levine MN, Konkle BA, et al. Thrombotic disorders: diagnosis and treatment. Hematology. 2003;520–39.
Stuart TP. Note on a variation in the course of the popliteal artery. J Anat Physiol. 1879;13:162.
Hamming JJ. Intermittent claudication at an early age, due to an anomalous course of the popliteal artery. Angiology. 1959;10: 369–70.
Bouhoutsos J, Daskalakis E. Muscular abnormalities affecting the popliteal vessels. Br J Surg. 1981;68:501–6.
Gibson MHL, Mills JG, Johnson GE, et al. Popliteal entrapment syndrome. Ann Surg. 1977;185:341–8.
Turnipseed WD. Popliteal entrapment syndrome. J Vasc Surg. 2002;35:910–5.
Turnipseed WD. Clinical review of patients treated for atypical claudication: a 28-year experience. J Vasc Surg. 2004;40:79–85.
Rignault DP, Pailler JL, Lunel F. The “functional” popliteal entrapment syndrome. Int Angiol. 1985;4:341–3.
Pillai J. A current interpretation of popliteal vascular entrapment. J Vasc Surg. 2008;48:61S–5.
Chernoff DM, Walker AT, Khorasani R, et al. Asymptomatic functional popliteal artery entrapment: demonstration at MR imaging. Radiology. 1995;195:176–80.
Turnipseed WD, Pozniak M. Popliteal entrapment as a result of neurovascular compression by the soleus and plantaris muscles. J Vasc Surg. 1992;15:285–94.
Sinha S, Houghton J, Holt P, et al. Popliteal entrapment syndrome. J Vasc Surg. 2012;55(1):252–62.
Roche-Nagle G, Wong KT, Oreopolulos G. Vascular claudication in a young patient: popliteal entrapment syndrome. Hong Kong Med J. 2009;15(5):388–90.
Ehsan O, Darwish A, Edmundson C, et al. Non-traumatic lower limb vascular complications in endurance athletes. Review of literature. Eur J Vasc Endovasc Surg. 2004;28:1–8.
Levien L. Popliteal artery thrombosis caused by popliteal entrapment syndrome. In: Greenhalgh RM, Powell JT, editors. Inflammatory and thrombotic problems in vascular surgery. London: WB Saunders Co Ltd; 1997. p. 159–68.
Gibson MHL, Mills JG, Johnson GE, et al. Popliteal entrapment syndrome. Ann Surg. 1997;185:341–8.
Murray A, Halliday M, Croft RJ. Popliteal artery entrapment syndrome. Br J Surg. 1991;78:1414–9.
Di Cesare J, Marsili L, Marino G, Masciocchi C, et al. Stress MR imaging for evaluation of popliteal artery entrapment. J Magn Reson Imaging. 1994;4:617–22.
Collins PS, McDonald PT, Lim RC. Popliteal artery entrapment: an evolving syndrome. J Vasc Surg. 1989;10:484–90.
Zund G, Brunner U. Surgical aspects of popliteal artery entrapment syndrome: 26 years of experience with 26 legs. Vasa. 1995; 24:29–33.
DiMarzo L, Cavallaro A, Mingoli A, et al. Popliteal artery entrapment syndrome: the role of early diagnosis and treatment. Surg. 1997;122:26–31.
DiMarzo L, Cavallaro A, Sciacca V, et al. Natural history of entrapment of the popliteal artery. J Am Coll Surg. 1994;178: 553–6.
Akkersdijk WL, de Ruyter JW, Lapham R, et al. Colour duplex ultrasonographic imaging and provocation of popliteal artery compression. Eur J Vasc Endovasc Surg. 1995;10:342–5.
Deshpande A, Denton M. Functional popliteal entrapment syndrome. Aust N Z J Surg. 1998;68:660–3.
Kim SY, Min SK, Ahn S, et al. Long-term outcomes after revascularization for advanced popliteal artery entrapment syndrome with segmental arterial occlusion. J Vasc Surg. 2012;55(1): 90–7.
Papaioannou S, Tsitouridis K, Giataganas G, et al. Evaluation of popliteal arteries with CT angiography in popliteal artery entrapment syndrome. Hippokratia. 2009;13:32–7.
Rich NM, Collins Jr GJ, McDonald PT, et al. Popliteal vascular entrapment. Its increasing interest. Arch Surg. 1979;114: 1377–84.
Espinoza LR. Buerger’s disease: thromboangitis obliterans 100 years after the initial description. Am J Med Sci. 2009;337(4): 285–6.
Piazza G, Creager M. Thromboangitis obliterans. Circulation. 2010;121:1858–61.
Puechal X, Fiessinger JN, Kahan A, et al. Rheumatologic manifestations in patients with thromboangitis obliterans. J Rheumatol. 1999;26:1764–8.
Olin JW. Thromboangitis obliterans. N Engl J Med. 2000;343: 864–9.
Ohta T, Ishioashi H, Hosaka M, et al. Clinical and social consequences of Buerger disease. J Vasc Surg. 2001;39:176–80.
Jayne D. Update on the European Vasculitis Study Group trials. Curr Opin Rheumatol. 2001;13:48–55.
Luqmani R. Large vessel vasculitides. Update for the cardiologist. Curr Opin Cardiol. 2012;27(6):578–84.
Devauchell-Pensec V, Jousee S, Destombe C, et al. Epidemiology, imaging and treatment of GCA. Joint Bone Spine. 2008;75(3): 267–72.
Weyand C, Liao JY, Goronzy JJ, et al. The immunopathology of GCA: diagnostic and therapeutic implications. J Neuroophthalmol. 2012;32(3):259–65.
Wlavick MD, Walvick MP. GCA: laboratory predictors of a positive temporal artery biopsy. Ophthalmology. 2011;118:1201–4.
Danesh-Meyer H. Temporal artery biopsy: skip it at your patient’s peril. Am J Ophthalmol. 2012;154(4):617–9.
Quinn EM, Kearney DE, Keohane C. Temporal artery biopsy is not required in all cases of suspected GCA. Ann Vasc Surg. 2012;26(5):649–54.
Cowey S, Reynolds C, Joglekar S, et al. Does temporal artery biopsy influence management of GCA? Int J Surg. 2010;8:501.
Achkar AA, Lie JT, Hunder GG, O’Fallon WM, Gabriel SE. How does previous glucocorticosteroid treatment affect the biopsy findings in giant cell (temporal) arteritis? Ann Intern Med. 1994; 120:987–92.
Dastgir G, Gutman J, Shinder R. Facial nerve injury: a complication of superficial temporal artery biopsy. Am J Ophthalmol. 2011;153(1):187.
Ypilantis E, Courtney ED, Chopra N, et al. Importance of specimen length during temporal artery biopsy. Br J Surgery. 2011; 98:1556–60.
Scafer V, Zwerina J. Biologic treatment of large vessel vasculitides. Curr Opin Rheumatol. 2012;24(1):31–7.
Talwar KD, Kumar K, Copra P, et al. Cardiac involvement in non-specific arteritis. Am Heart J. 1991;122:1666–70.
Curry TK, Messina LM. Fibromuscular dysplasia: when is intervention warranted? Semin Vasc Surg. 2003;16(3):190–9.
Bornak A, Milner R. Diagnosing and treating atypical arterial pathologies of aortic arch vessels: dissection and fibromuscular dysplasia. Semin Vasc Surg. 2011;24:36–43.
Olin JW, Froehlich J, Xiaokui G, et al. The United States registry for fibromuscular dysplasia results in the first 447 patients. Circulation. 2012;125:3182–90.
Weinberg I, Jaff MR. Nonatherosclerotic disorders of the lower extremities. Circulation. 2012;126:213–22.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Harris, L.M., Lukan, J. (2015). Non-atherosclerotic Vascular Disease: Vasculitis, Popliteal Entrapment, Hypercoagulable. In: Gahtan, V., Costanza, M. (eds) Essentials of Vascular Surgery for the General Surgeon. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1326-8_22
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1326-8_22
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1325-1
Online ISBN: 978-1-4939-1326-8
eBook Packages: MedicineMedicine (R0)