
Abstract
Systemic lupus erythematosus (SLE) is a systemic inflammatory disease, characterized serologically by an autoantibody response to nucleic antigens and clinically by injury and/or malfunction in any organ system. During their disease course, up to 50 % of SLE patients will develop lung disease. Pulmonary manifestations of SLE include pleuritis (with or without effusion), inflammatory and fibrotic forms of interstitial lung disease, alveolar hemorrhage, shrinking lung syndrome, pulmonary hypertension, airways disease, and thromboembolic disease. This chapter will focus on the clinical presentation, pathogenesis, pathology, management, and prognosis of these SLE-associated lung conditions.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Systemic Lupus Erythematosus
- Pulmonary Hypertension
- Systemic Lupus Erythematosus Patient
- Interstitial Lung Disease
- Right Heart Catheterization
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Systemic lupus erythematosus (SLE) is a systemic inflammatory disease, characterized serologically by an autoantibody response to nucleic antigens and clinically by injury and/or malfunction in any organ system. During their disease course, up to 50 % of SLE patients will develop pulmonary manifestations [1]. These include pleuritis (with or without effusion), inflammatory and fibrotic forms of interstitial lung disease, alveolar hemorrhage, shrinking lung syndrome, pulmonary hypertension, airways disease, and thromboembolic disease. Table 6.1 summarizes relevant clinical factors and frequency of the major pulmonary manifestations of SLE discussed in this chapter. As with SLE in general, its pulmonary manifestations are variable, yielding a heterogeneous clinical phenotype—from mild or essentially asymptomatic to severe and life-threatening. Although pulmonary disease is recognized as a leading cause of death and disability in SLE, over time, it has become increasingly clear that many patients with SLE have subclinical impairment in lung diffusing capacity and/or respiratory mechanics. The focus of this chapter will be on the clinical presentation, pathogenesis, pathology, management, and prognosis of SLE-associated lung conditions. Although lung cancer and pulmonary infections occur frequently in patients with SLE, they are not necessarily directly attributable to SLE disease activity and, therefore, will not be discussed here [2].
General
Before we begin the discussion of SLE-related pulmonary manifestations, we urge the reader to bear in mind that given the potential for subtle or subclinical pulmonary manifestations, the heterogeneity in clinical phenotype, and the potential for serious disease, clinicians must keep in mind a broad differential diagnosis anytime an SLE patient presents with chest or respiratory symptoms, and the etiology of those symptoms can be confidently identified and treated only through interdisciplinary dialogue/discussion. Because this chapter covers all the various ways SLE can affect the respiratory system, we begin the discussion with a brief overview of anatomy before moving to a general discussion of presenting symptoms. From there, we use a “compartments” approach to discuss how SLE may affect the vascular, parenchymal, pleural, or airways compartments of the respiratory system.
Overview of Thoracic Cavity Anatomy
The pulmonary system, which includes the airways (trachea, bronchi and bronchioles, and alveoli), pleural, pulmonary vasculature, and parenchyma, is housed along with the esophagus, thymus, lymph nodes, heart, and its major blood vessels, in the thoracic cavity [3]. The thoracic cavity is surrounded by an osteocartilaginous complex (thoracic cage) comprised of thoracic vertebrae, ribs, sternum, and costal cartilage and is enveloped by intercostal muscles, nerves, and vessels; the thoracic cage is separated from the abdomen by the diaphragm [3]. Certain muscles that arise from the upper limb and neck (serratus anterior, pectoral muscles, latissimus dorsi, scalenes), and attach to the thoracic cage, can function as accessory muscles of respiration [3]. The larynx, which contains the vocal chords, is an extrathoracic structure, situated above the trachea, and comprised of small joints and cartilage. Vocal chord integrity, which can be threatened by direct involvement of the vocal chords or indirect damage/disease to structures within the larynx, is essential to voice quality and respiration. Any of these structures may be directly or indirectly affected by SLE.
Clinical Presentation and Mimicry of Pulmonary Disease in SLE
Cough, chest pain, and dyspnea are the most frequent respiratory system symptoms in SLE, and although they are suggestive, they are not specific for disease within the pulmonary system. In patients with SLE, cough may be caused by an airway or lung parenchymal problem, but as in the general population, it is more often a symptom of gastrointestinal reflux (GERD) or postnasal drip [4]. Like patients with other connective tissue diseases, those with SLE are at risk for esophageal disease, including GERD and dysmotility. They have been linked with the development and worsening of pulmonary complications including aspiration pneumonitis, aspiration pneumonia, and progression of interstitial lung disease [5–9]. Patients with SLE may present with SLE-related laryngeal involvement, such as paradoxical vocal fold motion, the symptoms of which may be difficult to distinguish from thoracic pathology. Patient with SLE can develop chest pain from musculoskeletal, cardiac, pulmonary, esophageal, or psychiatric causes. An SLE patient presenting with chest pain and/or dyspnea should be evaluated for a cardiovascular disease (accelerated atherosclerosis leading to coronary syndromes and/or congestive heart failure) given the high frequency and rate of cardiovascular mortality in this patient population [10, 11]. In this population, mimics of cardiovascular chest pain include pleural disease, esophageal spasm, costochondritis, or sternoclavicular arthritis (from SLE disease activity). The astute clinician will also be on the lookout for comorbid conditions commonly found in SLE, such as fibromyalgia or mood disorders (anxiety/depression) [12–15].
Vascular Compartment
Pulmonary Hypertension
Epidemiology and Clinical Presentation
In various studies, the prevalence of pulmonary hypertension (PH) in SLE ranges from 0.5 to 17.5 %, depending on the case definition [16]. As in other CTDs, in SLE there are multiple potential reasons for PH to develop, so a number of causes must be carefully considered. Before a confident diagnosis of SLE-related PH (SLE-PH) is rendered (i.e., World Health Organization [WHO] Group 1 or pulmonary arterial hypertension [PAH]), the causes of WHO Groups 2–5 PH must be excluded [17]. Patients with SLE may develop WHO Group 2 PH, from either left ventricular dysfunction or left heart valvular abnormalities (related to SLE or not). SLE patients with significant interstitial lung disease (ILD) can develop PH from chronic hypoxia (WHO Group 3 PH), and those with antiphospholipid syndrome are at risk for developing WHO Group 4 PH (chronic thromboembolic PH or CTEPH). WHO Group 5 PH includes a number of disparate entities, including extrinsic compression of the pulmonary arteries, that are not particularly germane to SLE patients, but, as in other patients, these entities must be excluded in the evaluation of PH in the patient with SLE.
Typically, SLE patients develop PH within 5 years from SLE onset; there is no association between extrathoracic SLE disease activity and the development of PH. Most SLE patients with PH are adult women under the age of 40 years [18]. Although some patients with SLE-PH are asymptomatic, most present with one or more symptoms, including chest pain, shortness of breath, or cough [19]. Approximately a third of SLE-PH patients will have pleural effusions, often associated with high right atrial pressure and right heart failure [16, 20]. Physical examination may reveal a prominent pulmonic component and/or fixed split of the second heart sound, murmurs of tricuspid or pulmonic regurgitation, a right ventricular heave, a palpable pulsation along the left sternal border, and, in advanced cases, overt signs of right heart failure. In a case-control study of 147 SLE patients, Raynaud’s phenomenon and the presence of anticardiolipin and anti-U1 ribonucleoprotein (RNP) antibodies were predictive of PH, with odds ratios (ORs) of 3.2, 3.8, and 5.4, respectively [21]. In another study, investigators found that rheumatoid factor positivity was significantly more likely among SLE patients with PH compared to those without PH [19].
Pathophysiology
The main mechanisms driving the development of SLE-PH are believed to be organ-altering autoimmune effects directed at the pulmonary vasculature. Chronic inflammation, immune dysregulation, and vascular damage and remodeling are contributory. Rarely, vasculitis or pulmonary venoocclusive disease (PVOD) leads to SLE-PH [22]. With the exception of PVOD, the pathologic findings of SLE-PH include medial hypertrophy, intimal fibrosis, and, in severe cases, plexiform lesions.
Evaluation, Prognosis, and Management
Patients suspected to have SLE-PH may undergo screening evaluation with a transthoracic echocardiogram (TTE); however, TTE is notoriously inaccurate when the estimated right ventricular systolic pressure is not significantly elevated or other signs of right heart stress (e.g., dilation, impaired systolic function) are absent. Right heart catheterization (RHC) is needed to definitively diagnose PH. During RHC, the hemodynamic definition of PH is made when the mean pulmonary artery pressure is ≥25 mmHg in the face of a pulmonary capillary wedge pressure <15 mmHg [23]. As in patients without SLE, those with SLE-PH should undergo evaluation for other causes of PH. A thorough history looking for current or past use of anorexigens or illicit drugs; testing that includes a screening polysomnogram to rule out obstructive sleep apnea, chest computed tomography (CT) angiogram and ventilation perfusion scan to evaluate for acute or chronic thromboembolic disease, and serologic testing for human immunodeficiency virus and chronic liver disease are suggested as part of the work-up for PH. If the history, physical exam, or lung function suggests the possibility of ILD, a high-resolution CT is indicated.
There are no consensus guidelines on the management of SLE-PH. In double-blind trials, in which only small numbers of patients (n = 16–35) were enrolled, PH-specific therapy (selective and nonselective endothelin receptor antagonists or phosphodiesterase-5 inhibitors) has demonstrated improvements in clinical and physiologic end points [16]. Data supporting the use of immunosuppressive medications, such as intravenous cyclophosphamide and glucocorticoids, for SLE-PH are limited. In certain retrospective series of small numbers of subjects, investigators have reported a modest physiologic benefit from the use of immunosuppression in combination with vasodilator therapy [24]. In a recent systematic review, elevated mean pulmonary artery pressure, Raynaud’s phenomenon, thrombocytopenia, plexiform lesions, infection, thrombosis, pregnancy, pulmonary vasculitis, and anticardiolipin antibodies were associated with decreased survival among patients with SLE-PH [25]. Overall, SLE-PH has a 75 % 3-year survival [26].
Diffuse Alveolar Hemorrhage
Epidemiology and Clinical Presentation
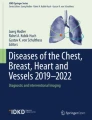
Diffuse alveolar hemorrhage (DAH) is a rare and potentially catastrophic pulmonary manifestation of SLE. In SLE, DAH is the direct consequence of pulmonary capillaritis, defined pathologically by neutrophilic infiltration and destruction of vessel walls [27]. The clinical presentation is often dramatic: patients are often ill appearing with dyspnea and fever. Because hemoptysis occurs in only about 30 % of patients with DAH, its absence far from excludes the diagnosis. Chest imaging is notable for diffuse, bilateral consolidative or ground glass opacities (Fig. 6.1a). Depending on the amount of blood loss, patients may also present with falling hematocrit and/or overt anemia. Nephritis has been reported at the time of DAH presentation [28]. Notably, DAH can lead to pathologic changes in the lungs’ terminal airways (alveoli) that are similar to renal involvement in SLE; immune complexes in addition to blood may be found in the alveolar wall in the setting of DAH [29]. At the time of DAH, high SLE disease activity, high titers of anti-DS DNA antibodies, and low complement C3 levels may be found [30].

(a) shows an axial slice from a chest computed tomography scan from the presented patient at the level of the azygous vein. The image shows bilateral, patchy ground glass opacities confirmed by bronchoalveolar lavage (b) to be due to diffuse alveolar hemorrhage
Management and Prognosis
Catastrophic antiphospholipid antibody syndrome and overlap with primary vasculitides must be excluded, because their management differs from SLE-related DAH. All patients presenting with DAH should be screened for the presence of antiphospholipid, anti-glomerular basement membrane, and antineutrophil cytoplasmic antibodies in addition to serum complement C3, C4, ANA, and anti-DS DNA. Patients should also be evaluated for pulmonary infection as a cause of DAH. Pulse methylprednisolone, 1 g daily for 3 days and changed to 1–2 mg/kg/day oral prednisone over the next few days, is the initial treatment of DAH. Plasma exchange and cytotoxic agents may be used as well. Certain investigators have successfully treated SLE-related DAH with cyclophosphamide or rituximab [28, 31]. In DAH, poor prognostic markers include renal insufficiency, thrombocytopenia, and severity of clinical presentation (i.e., need for mechanical ventilation) [28]. Patients may experience recurrent episodes of DAH; thus, vigilant follow-up is required.
Case Vignette 1
Ms. J. is a 30-year-old African-American woman with long-standing SLE treated with hydroxychloroquine alone. She was found to have elevated antiphospholipid antibodies at the time of SLE diagnosis, but she has no history of arterial or venous thrombosis. She presents now to the emergency department (ED) with 2 days of dyspnea, cough, low-grade fever to 38 °C, and a vague “twinge” in her upper chest bilaterally.
A work-up in the ED shows her room air, resting, peripheral oxygen saturation to be 89 %, and her hematocrit is 30 %, down from 40 % 2 weeks ago. A chest computed tomography scan with contrast rules out acute or chronic pulmonary embolism but demonstrates bilateral, patchy ground glass opacities (Fig. 6.1a). Bronchoscopy with bronchoalveolar lavage (BAL) is performed; return from sequential BAL aliquots is progressively more bloody (Fig. 6.1b).
Pulmonary Embolism
Antiphospholipid antibodies (APLAs) are a heterogeneous group of autoantibodies that include anticardiolipin antibodies, lupus anticoagulant, and anti-glycoprotein-I antibodies. APLAs occur in around 1/3 of SLE patients [32]. When compared with SLE patients without a lupus anticoagulant or anticardiolipin antibodies, those with these antibodies are much more likely (six times and 2.5 times) to develop deep venous thrombosis (DVT) or pulmonary embolism (PE) [33]. Moreover, lupus anticoagulant positivity is associated with a 50 % chance of DVT within 20 years of SLE diagnosis [34]. Interestingly, male gender is an independent predictor for thrombosis in SLE and, in addition to hypertension, is an important risk factor for thrombosis, even in the absence of APLAs [32].
As with the majority of pulmonary emboli, PE in SLE nearly always results from lower extremity DVT; intracardiac thrombi are a rare occurrence in SLE, even among those with APLA syndrome [35]. In SLE patients presenting with dyspnea and/or chest pain, particularly if they are seropositive for APLAs, PE must be part of the differential diagnosis. Bilateral lower extremity venous Doppler ultrasound, screen for APLAs, and CT angiogram should be considered for further work-up of PE.
Acute Reversible Hypoxemia
In this extremely rare entity, patients with SLE develop the abrupt onset of potentially profound hypoxemia. The cause is leuko-aggregation within pulmonary vessels [36, 37]. Substantially elevated blood levels of C3a suggest complement activation that plays a pivotal role. Treatment includes glucocorticoids and aspirin. Prognosis is believed to be favorable.
Parenchymal Compartment
Interstitial Lung Disease and Pneumonitis
Epidemiology
Clinically apparent ILD is far less common in SLE than in other connective tissue diseases, occurring in 1–15 % of SLE patients [38]. Although parenchymal abnormalities may occur in the setting of SLE, they are often not the direct consequence of the autoimmune aspect of the disease [39]. For example, an SLE patient presenting with radiographic opacities is much more likely to have infection than fibro/inflammatory parenchymal disease.
Clinical Presentation and Risk Factors
Patients with SLE-related ILD (SLE-ILD) typically present with exertional dyspnea and possibly a nonproductive cough. Because dyspnea is reported in nearly two-thirds of all-comers with SLE, it may be attributed to causes other than ILD, thus delaying the diagnosis of ILD until its later stages [40]. This may, in part, explain why two-thirds of patients with SLE-ILD have auscultatory crackles on chest examination upon presentation of ILD [41]. Clubbing and peripheral cyanosis, signs not infrequently observed in idiopathic pulmonary fibrosis, are rarely found in SLE-ILD [41]. Few predictors of SLE-ILD exist. Patients with long-standing disease (>10 years of disease duration), those with Raynaud’s phenomenon, seropositivity for anti-(U1) RNP antibodies, sclerodactyly, and abnormal nailfold capillary loops are associated with radiographic evidence of ILD [41, 42]. Patients with an older age of SLE onset (>50 years of age) are significantly more likely than those with a younger age of onset to develop ILD [43]. Serologic abnormalities associated with SLE-ILD include a high levels of high-sensitivity C-reactive protein, cryoglobulins, hypocomplementemia, and serum lupus erythematosus cells [38].
Evaluation and Diagnosis
The diagnosis of SLE-ILD relies on a combination of clinical features, chest imaging, histopathology, and lung physiology. Before rending a diagnosis of SLE-ILD, it is important to exclude other causes of ILD including medication-related. Disease-modifying medications used in SLE such as methotrexate, leflunomide, imuran, tumor necrosis factor inhibitors, rituximab, cyclophosphamide, and sulfasalazine have been associated with the development of ILD. In addition, screening for environmental or occupational exposures must be undertaken (e.g., silica, asbestos, beryllium, dust, mold, bird feathers) [44]. It is also important to exclude overlapping disorders that may lead to ILD (sarcoidosis, other connective tissue disorders).
Although a surgical lung biopsy is the gold standard method to diagnose ILD, it is usually not performed. The most common histologic pattern of SLE-ILD is nonspecific interstitial pneumonia (NSIP); less common patterns include organizing pneumonia (OP), lymphoid interstitial pneumonia (LIP), usual interstitial pneumonia (UIP), desquamative interstitial pneumonia (DIP), and diffuse alveolar damage (DAD) [45]. In lieu of an invasive investigational approach, a high-resolution chest computed tomography (HRCT) scan in combination with restrictive physiology (a reduced forced vital capacity (FVC), total lung capacity, and/or diffusing capacity of carbon monoxide (DLCO) on pulmonary function tests (PFTs)) and/or compatible clinical features can clinch the diagnosis of ILD. However, clinicians must be vigilant to exclude ILD mimics such as DAH, drug toxicity congestive heart failure, uremia, or infection.
Management and Prognosis
Treatment for SLE-ILD is based largely on expert opinion. High-dose oral corticosteroids (1 mg/kg body weight of oral prednisone, up to 60 mg, or its equivalent) and a steroid-sparing agent, often cyclophosphamide (daily oral of 1–2 mg/kg depending on renal function and age of patient or intravenous equivalent), are initiated for severe ILD. Mild to moderate forms of ILD are sometimes treated initially with moderate doses of corticosteroids with either azathioprine or mycophenolate mofetil. Tapering of corticosteroid therapy is often guided by favorable clinical, physiologic, and/or radiographic response.
Case Vignette 2
Mrs. D. is a 58-year-old African-American female, never smoker, with SLE diagnosed 10 years ago. She has no other medical problems; she takes no medications associated with the development of pulmonary fibrosis; she owns no pets; she has no exposures, including feathers or dusts. Over the last 18 months, she has noticed gradually increasing exertional dyspnea and nonproductive cough. A slice from a chest computed tomography scan, shown in Fig. 6.2, confirms the presence of pulmonary fibrosis.

A slice through the lower lungs from Mrs. D’s chest computed tomography scan shows an interesting pattern of lower zone-, peripheral-, and subpleural-predominant fibrosis
Lupus Pneumonitis and Its Association with ILD
Lupus pneumonitis (LP) is probably best characterized as an acute interstitial pneumonia (AIP)-like reaction in a patient with SLE. It is a highly fatal syndrome characterized by acute onset of fever, pleuritic chest pain, and tachypnea; up to 50 % mortality rate is seen with this rare condition. It is often accompanied with auscultatory crackles, and hemoptysis may rarely occur. Chest imaging usually reveals bilateral opacities [46]. If alveolar hemorrhage is found, we prefer the term DAH and reserve the term LP for cases in which an AIP-like reaction is the cause of the patient’s acute decompensation. Pneumonitis may be a precursor to chronic ILD in a subset of patients [46]. In one case series, 3 of 12 patients with pneumonitis progressed to chronic ILD, despite treatment with high-dose corticosteroids. In both LP and SLE-ILD, immune complexes, lymphocytic aggregates, and vascular pathology are common [46].
Physiology Impairment: Restrictive Lung Disease and Shrinking Lung Syndrome
Restrictive Lung Disease
Epidemiology
PFT abnormalities in SLE are very common and can occur in patients who are not suspected to have lung involvement [47, 48]. In a study of 43 SLE patients, 88 % had pulmonary dysfunction with the most common abnormality being a reduction in DLCO (72 %), followed by restrictive (49 %) or obstructive (9 %) patterns on PFT [48]. In a study of 70 non-smoking SLE patients, the majority of whom were asymptomatic with a normal chest radiograph, 67 % had an isolated reduction in DLCO, and 6 % had a restrictive pattern [49]. In another study of 110 Japanese SLE patients, an abnormal DLCO and restrictive changes were found in 47 % and 8 % of patients, respectively; only 13 % of patients with PFT abnormalities had other clinical and/or radiographic evidence for lung involvement [50].
Shrinking Lung Syndrome
Clinical Presentation
Dyspnea and physiologic restriction, in the absence of parenchymal disease on chest imaging, are major features of shrinking lung syndrome (SLS). In the original report of SLS by Hoffbrand and colleagues, SLS was characterized by unexplained dyspnea, small lung volumes, and restrictive lung physiology, with or without diaphragmatic elevation, in the absence of interstitial, alveolar, or vascular pulmonary disease [51].
Epidemiology and Risk Factors
SLS is often considered a rare manifestation of SLE, occurring in 0.5 % of patients [52]. In a recent study of 110 consecutively enrolled SLE patients systematically evaluated for the presence of pulmonary involvement, a surprising 10 % of patients met the definition of SLS [53]. The higher frequency of SLS compared with prior reports may in part be due to the fact that in that study SLE patients were screened with PFTs and chest imaging for the presence of parenchymal lung involvement. In this study, greater disease duration, seropositivity for anti-RNP antibodies, and a history of pleuritis were independently associated with SLS in a multivariate analysis [53]. The exact cause of SLS remains unclear, but some data suggest progressive impairment in diaphragmatic excursion from weakness is the main contributing factor [54].
Management
There is limited information on the management and prognosis of SLS. Corticosteroids (moderate to high doses), cytotoxic agents, biologic therapies (rituximab), theophylline, and high-dose beta-agonists have all been used to successfully treat this condition [54].
Case Vignette 3
Ms. P. is a 40-year-old white female with several years of malar rash, photosensitivity, Raynaud’s phenomenon, and oral ulcers who was diagnosed with SLE 2 years ago when recalcitrant cough brought her to medical attention. Over the last 2 years, she has noticed gradually increasing exertional dyspnea.
A posteroanterior chest radiograph showed small lung volumes characteristic for SLS (Fig. 6.3). A chest computed tomography scan showed no parenchymal or pleural abnormalities. Seated, her FVC is 1.7 L, which is 45 % of the predicted value based on her age, height, and weight. Supine, her FVC is 1.2 L, which represents a 29 % decline from seated. Her maximal inspiratory pressure (MIP) is only 30 % of the predicted value. Results from a maximal cardiopulmonary exercise test are in Table 6.2. Note the failure in her ability to recruit tidal volume (Vt) as the test progresses; minute ventilation increases throughout exercise only because her respiratory rate climbs excessively. The constellation of findings supports a diagnosis of SLS.

Posteroanterior chest radiograph reveals small lung volumes
Pleural Compartment
Epidemiology and Clinical Presentation
Pleuritis (with or without pleural effusion) is the most common SLE-related pulmonary manifestation and part of the classification criteria for SLE [55]. In large observational cohorts from Europe and Canada, nearly a third of prospectively followed SLE patients developed clinically identifiable pleuritis, whereas up to 2/3 will have involvement at autopsy [24, 56, 57]. Disease duration, late age of diagnosis of SLE (after age 50 years), greater cumulative damage, and concomitant seropositivity for anti-RNP and anti-Sm antibodies are factors that increased the risk of pleuritis by nearly twofold [57, 58]. Pleuritic chest pain is the most common symptom, but patients may also report cough, dyspnea, and fever.
Evaluation, Prognosis, and Management
A pleural rub may be heard on physical examination, and chest imaging may reveal pleural effusion(s). Pleural effusions are often bilateral and small; rarely, effusions from SLE disease activity involve more than 2/3 of the lung fields [24]. Before diagnosing SLE-related pleuritis, other causes of a pleural effusion in SLE, such as cardiac or renal failure, must be excluded [59]. A thoracentesis and/or pleural biopsy is not necessary to diagnose an effusion and are rarely performed. These procedures may be performed when there is a concern for infection, blood in the pleural space, or malignancy.
The majority of SLE-related pleural effusions are not life-threatening and respond favorably to treatment with nonsteroidal anti-inflammatory drugs, for mild or asymptomatic effusions, and/or oral corticosteroids at a dose of 20–40 mg daily, for moderate to severe effusions [60]. Treatment can be discontinued in 3–4 weeks depending on clinical response. Pleurodesis may be considered in refractory, treatment-resistant cases [61].
Airways Compartment and Larynx
Large and/or small airways may be affected by SLE. Bronchiectasis can be seen in SLE, but is often an incidental finding on chest imaging; its clinical significance in this population is not known [62]. Inflammatory (e.g., lymphocytic) bronchiolitis may occur. Obliterative bronchiolitis (OB) is an uncommon manifestation of SLE that presents with cough and dyspnea. It is associated with severe, often progressive, airways obstruction (a reduced ratio of forced expiratory volume in 1 s to FVC), air trapping (that is often nicely accentuated on expiratory imaging), but usually a normal DLCO on PFT [63, 64]. Although various agents have been tried, no regimen has been proved effective [65, 66]. Borrowing from the lung transplantation literature, clinicians often prescribe OB patients macrolide antibiotics, because of their putative anti-inflammatory and perhaps antifibrotic effects.
Laryngeal involvement is an uncommon manifestation of SLE, often presenting with hoarseness and dyspnea. In a review of 97 SLE patients with laryngeal involvement, there were various pathologic changes found, from mild ulcerations to subglottic stenosis, but laryngeal edema and vocal chord paralysis were more frequently observed, at a rate of 28 % and 11 %, respectively [67]. It results from varying levels of upper airway mucosal inflammation and is responsive to treatment with oral corticosteroids. In rare circumstances, mucosal inflammation is accompanied by edema and can lead to airway obstruction [68].
How to Approach the Evaluation of a Patient with SLE Who Presents with Dyspnea
In any patient with SLE who presents with a respiratory complaint, particularly dyspnea, infection must be excluded. The concern for infection is heightened further in the dyspneic patient who is receiving chronic immunomodulatory therapy. It should be recognized that patients on glucocorticoids alone, or in combination with an immunomodulatory agent, may not manifest classic symptoms of infection, so a high index of suspicion for infection by typical (bacteria) and atypical (Mycobacteria, fungi, Pneumocystis) agents must be maintained. Bronchoscopy should be considered in any patient on immune-suppressing drugs who is found to have opacities on chest imaging. Besides confirming or ruling out pulmonary infection, as demonstrated in the representative case discussed, findings at bronchoscopy may prove useful for identifying the true cause of a patient’s symptoms (e.g., DAH). If infection is confidently ruled out, consideration is given to other potential etiologies for dyspnea; top on the list, particularly in an SLE patient with risk factors for thromboembolism (e.g., hypercoagulable state or history of thromboembolism), is PE. In the appropriate scenario, a CT angiogram, with or without a lower extremity venous duplex with Doppler ultrasound, can be useful for confirming or ruling out thromboembolic disease. The added benefit to performing CT angiogram is that it shows the lung parenchyma as well as the vasculature. However, because of the intravenous contrast given and the technique-mandated lower lung volumes used for a CT angiogram, the lung parenchyma will be more radiodense than on a high-resolution CT scan; this can make discerning whether ground glass opacities are present or not quite challenging. Depending on the acuity of symptoms, PFTs and an assessment of peripheral oxygen saturation (SpO2) during exertion may add important information that can be used to help direct the evaluation. The DLCO may be elevated in DAH and reduced in the setting of interstitial lung disease or PH. Pulmonary vascular disease should be considered—and its presence assessed—in any patient with otherwise unexplained dyspnea or exertion-induced oxygen desaturation (SpO2 decline ≥ 4 from resting value, even if nadir during exertion remains >90 %).
The SLE Patient Without Respiratory Complaints and the One with Known SLE-Related Pulmonary Complications
There are no data to guide the practitioner on whether and how to evaluate an SLE patient who has no respiratory complaints. Mild abnormalities on spirometry and/or diffusion capacity testing are common in asymptomatic SLE patients; most often, these abnormalities remain stable over time. It is our practice to use imaging and other testing as appropriate for the clinical scenario and not to “screen” asymptomatic SLE patients. However, patients should have a chest radiograph before the start of a disease-modifying medication, particularly before methotrexate is initiated, to rule out any underlying preexisting parenchymal disease. Our approach to following the patient with known SLE-related pulmonary complications varies depending on the particular complication present. For example, we routinely evaluate patients with SLE-ILD every 3–4 months in clinic with spirometry, DLCO, and an assessment of their functional status and exertion-related oxygen requirements.
Concluding Remarks
Pulmonary involvement is common during the disease course of SLE and can involve any part of the respiratory tract. It is important to identify the underlying etiology when pulmonary involvement occurs; clinicians need to particularly be vigilant in excluding other etiologies, such as infections, before attributing the manifestation to SLE. Being mindful of the clinical context, including the serologic profile of the patient, may help support the diagnosis of specific SLE-related pulmonary manifestations. Management of pulmonary manifestations is based largely on clinical experience and case series; studies in large cohorts and/or clinical trials are needed to establish effective therapies for pulmonary disease in SLE.
References
Pines A, et al. Pleuro-pulmonary manifestations of systemic lupus erythematosus: clinical features of its subgroups. Prognostic and therapeutic implications. Chest. 1985;88(1):129–35.
Bernatsky S, et al. Mortality in systemic lupus erythematosus. Arthritis Rheum. 2006;54(8):2550–7.
Moore KL, Agur A, Dalley AF. Essential Clinical Anatomy. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2010.
Azad AK, et al. Cough in systemic lupus erythematosus. Mymensingh Med J. 2013;22(2):300–7.
Zhang XJ, et al. Association of gastroesophageal factors and worsening of forced vital capacity in systemic sclerosis. J Rheumatol. 2013;40(6):850–8.
Marie I, et al. Esophageal involvement and pulmonary manifestations in systemic sclerosis. Arthritis Rheum. 2001;45(4):346–54.
Marie I, et al. Polymyositis and dermatomyositis: short term and longterm outcome, and predictive factors of prognosis. J Rheumatol. 2001;28(10):2230–7.
Savarino E, et al. [Possible connection between gastroesophageal reflux and interstitial pulmonary fibrosis in patients with systemic sclerosis]. Recenti Prog Med. 2009;100(11):512–6.
Fagundes MN, et al. Esophageal involvement and interstitial lung disease in mixed connective tissue disease. Respir Med. 2009;103(6):854–60.
Symmons DP, Gabriel SE. Epidemiology of CVD in rheumatic disease, with a focus on RA and SLE. Nat Rev Rheumatol. 2011;7(7):399–408.
Sinicato NA, da Silva Cardoso PA, Appenzeller S. Risk factors in cardiovascular disease in systemic lupus erythematosus. Curr Cardiol Rev. 2013;9(1):15–9.
Wolfe F, et al. Fibromyalgia, systemic lupus erythematosus (SLE), and evaluation of SLE activity. J Rheumatol. 2009;36(1):82–8.
Palagini L, et al. Depression and systemic lupus erythematosus: a systematic review. Lupus. 2013;22(5): 409–16.
Donmez S, et al. Autoimmune rheumatic disease associated symptoms in fibromyalgia patients and their influence on anxiety, depression and somatisation: a comparative study. Clin Exp Rheumatol. 2012;30(6 Suppl 74):65–9.
Peppercorn MA, Docken WP, Rosenberg S. Esophageal motor dysfunction in systemic lupus erythematosus. Two cases with unusual features. JAMA. 1979;242(17):1895–6.
Dhala A. Pulmonary arterial hypertension in systemic lupus erythematosus: current status and future direction. Clin Dev Immunol. 2012;2012:854941.
Simonneau G, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009; 54(1 Suppl):S43–54.
Badesch DB, et al. Medical therapy for pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest. 2004;126(1 Suppl):35S–62.
Kamel SR, et al. Asymptomatic pulmonary hypertension in systemic lupus erythematosus. Clin Med Insights Arthritis Musculoskelet Disord. 2011;4:77–86.
Luo YF, et al. Frequency of pleural effusions in patients with pulmonary arterial hypertension associated with connective tissue diseases. Chest. 2011; 140(1):42–7.
Lian F, et al. Clinical features and independent predictors of pulmonary arterial hypertension in systemic lupus erythematosus. Rheumatol Int. 2012;32(6):1727–31.
Kishida Y, et al. Pulmonary venoocclusive disease in a patient with systemic lupus erythematosus. J Rheumatol. 1993;20(12):2161–2.
Galie N, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J. 2009; 30(20):2493–537.
Swigris JJ, et al. Pulmonary and thrombotic manifestations of systemic lupus erythematosus. Chest. 2008;133(1):271–80.
Chow SL, et al. Prognostic factors for survival in systemic lupus erythematosus associated pulmonary hypertension. Lupus. 2012;21(4):353–64.
Condliffe R, et al. Connective tissue disease-associated pulmonary arterial hypertension in the modern treatment era. Am J Respir Crit Care Med. 2009;179(2):151–7.
Fishbein GA, Fishbein MC. Lung vasculitis and alveolar hemorrhage: pathology. Semin Respir Crit Care Med. 2011;32(3):254–63.
Martinez-Martinez MU, Abud-Mendoza C. Predictors of mortality in diffuse alveolar haemorrhage associated with systemic lupus erythematosus. Lupus. 2011;20(6):568–74.
Hughson MD, et al. Alveolar hemorrhage and renal microangiopathy in systemic lupus erythematosus. Arch Pathol Lab Med. 2001;125(4):475–83.
Chen GX, Dong Y, Ju ZB. [A clinical analysis of 32 patients with diffuse alveolar hemorrhage in diffuse connective tissue diseases]. Zhonghua Nei Ke Za Zhi. 2008;47(5):362–5.
Narshi CB, et al. Rituximab as early therapy for pulmonary haemorrhage in systemic lupus erythematosus. Rheumatology (Oxford). 2010;49(2):392–4.
Tektonidou MG, et al. Risk factors for thrombosis and primary thrombosis prevention in patients with systemic lupus erythematosus with or without antiphospholipid antibodies. Arthritis Rheum. 2009;61(1): 29–36.
Wahl DG, et al. Risk for venous thrombosis related to antiphospholipid antibodies in systemic lupus erythematosus—a meta-analysis. Lupus. 1997;6(5):467–73.
Somers E, Magder LS, Petri M. Antiphospholipid antibodies and incidence of venous thrombosis in a cohort of patients with systemic lupus erythematosus. J Rheumatol. 2002;29(12):2531–6.
Pardos-Gea J, et al. Cardiac manifestations other than valvulopathy in antiphospholipid syndrome: long-time echocardiography follow-up study. Int J Rheum Dis 2013 Oct 17. doi:10.1111/1756-185X.12191 [Epub ahead of print].
Martinez-Taboada VM, et al. Acute reversible hypoxemia in systemic lupus erythematosus: a new syndrome or an index of disease activity? Lupus. 1995;4(4):259–62.
Abramson SB, et al. Acute reversible hypoxemia in systemic lupus erythematosus. Ann Intern Med. 1991;114(11):941–7.
Mittoo S, Fischer A, Strand V, Meehan R, Swigris JJ. Systemic lupus erythematosus-related interstitial lung disease. Curr Rheumatol Rev. 2010;6(2):99–107.
Quadrelli SA, et al. Pulmonary involvement of systemic lupus erythematosus: analysis of 90 necropsies. Lupus. 2009;18(12):1053–60.
Hellman DB, et al. Dyspnea in ambulatory patients with SLE: prevalence, severity, and correlation with incremental exercise testing. J Rheumatol. 1995;22(3): 455–61.
Eisenberg H, et al. Diffuse interstitial lung disease in systemic lupus erythematosus. Ann Intern Med. 1973;79(1):37–45.
ter Borg EJ, et al. Clinical associations of antiribonucleoprotein antibodies in patients with systemic lupus erythematosus. Semin Arthritis Rheum. 1990;20(3): 164–73.
Ward MM, Polisson RP. A meta-analysis of the clinical manifestations of older-onset systemic lupus erythematosus. Arthritis Rheum. 1989;32(10):1226–32.
Schwaiblmair M, et al. Drug induced interstitial lung disease. Open Respir Med J. 2012;6:63–74.
Galie N, et al. Guidelines on diagnosis and treatment of pulmonary arterial hypertension. Rev Esp Cardiol. 2005;58(5):523–66.
Matthay RA, et al. Pulmonary manifestations of systemic lupus erythematosus: review of twelve cases of acute lupus pneumonitis. Medicine (Baltimore). 1975;54(5):397–409.
Groen H, et al. Pulmonary function in systemic lupus erythematosus is related to distinct clinical, serologic, and nailfold capillary patterns. Am J Med. 1992;93(6):619–27.
Silberstein SL, et al. Pulmonary dysfunction in systemic lupus erythematosus: prevalence classification and correlation with other organ involvement. J Rheumatol. 1980;7(2):187–95.
Andonopoulos AP, et al. Pulmonary function of nonsmoking patients with systemic lupus erythematosus. Chest. 1988;94(2):312–5.
Nakano M, et al. Pulmonary diffusion capacity in patients with systemic lupus erythematosus. Respirology. 2002;7(1):45–9.
Hoffbrand BI, Beck ER. “Unexplained” dyspnoea and shrinking lungs in systemic lupus erythematosus. Br Med J. 1965;1(5445):1273–7.
Bertoli AM, Vila LM, Apte M, Fessler BJ, Bastian HM, Reveille JD, Alarcon GS. Systemic lupus erythematosus in a multiethnic US Cohort LUMINA XLVIII: factors predictive of pulmonary damage. Lupus. 2007;16(6):410–7.
Allen D, et al. Evaluating systemic lupus erythematosus patients for lung involvement. Lupus. 2012; 21(12):1316–25.
Carmier D, Diot E, Diot P. Shrinking lung syndrome: recognition, pathophysiology and therapeutic strategy. Expert Rev Respir Med. 2011;5(1):33–9.
Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF, Schaller JG, Talal N, Winchester RJ. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982;25(11):1271–7.
Cervera R, et al. Systemic lupus erythematosus in Europe at the change of the millennium: lessons from the “Euro-Lupus Project”. Autoimmun Rev. 2006; 5(3):180–6.
Mittoo S, et al. Clinical and serologic factors associated with lupus pleuritis. J Rheumatol. 2010;37(4): 747–53.
Boddaert J, et al. Late-onset systemic lupus erythematosus: a personal series of 47 patients and pooled analysis of 714 cases in the literature. Medicine (Baltimore). 2004;83(6):348–59.
Badui E, et al. Cardiovascular manifestations in systemic lupus erythematosus. Prospective study of 100 patients. Angiology. 1985;36(7):431–41.
Winslow WA, Ploss LN, Loitman B. Pleuritis in systemic lupus erythematosus: its importance as an early manifestation in diagnosis. Ann Intern Med. 1958;49(1):70–88.
Glazer M, et al. Successful talc slurry pleurodesis in patients with nonmalignant pleural effusion. Chest. 2000;117(5):1404–9.
Fenlon HM, et al. High-resolution chest CT in systemic lupus erythematosus. AJR Am J Roentgenol. 1996;166(2):301–7.
Weber F, et al. Cyclophosphamide therapy is effective for bronchiolitis obliterans occurring as a late manifestation of lupus erythematosus. Br J Dermatol. 2000;143(2):453–5.
Porter DR. Bronchiolitis obliterans in systemic lupus erythematosus. Ann Rheum Dis. 1992;51(7):927.
Kawahata K, et al. Severe airflow limitation in two patients with systemic lupus erythematosus: effect of inhalation of anticholinergics. Mod Rheumatol. 2008;18(1):52–6.
Godeau B, Cormier C, Menkes CJ. Bronchiolitis obliterans in systemic lupus erythematosus: beneficial effect of intravenous cyclophosphamide. Ann Rheum Dis. 1991;50(12):956–8.
Teitel AD, et al. Laryngeal involvement in systemic lupus erythematosus. Semin Arthritis Rheum. 1992;22(3):203–14.
Karim A, et al. Severe upper airway obstruction from cricoarytenoiditis as the sole presenting manifestation of a systemic lupus erythematosus flare. Chest. 2002; 121(3):990–3.
Cervera R, et al. Systemic lupus erythematosus: clinical and immunologic patterns of disease expression in a cohort of 1,000 patients. The European Working Party on Systemic Lupus Erythematosus. Medicine (Baltimore). 1993;72(2):113–24.
Martinez-Martinez MU, Abud-Mendoza C. Recurrent diffuse alveolar haemorrhage in a patient with systemic lupus erythematosus: long-term benefit of rituximab. Lupus. 2012;21(10):1124–7.
Hariri LP, et al. Acute fibrinous and organizing pneumonia in systemic lupus erythematosus: a case report and review of the literature. Pathol Int. 2010;60(11): 755–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Mittoo, S., Swigris, J.J. (2014). Pulmonary Manifestations of Systemic Lupus Erythematosus (SLE). In: Dellaripa, P., Fischer, A., Flaherty, K. (eds) Pulmonary Manifestations of Rheumatic Disease. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0770-0_6
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0770-0_6
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-0769-4
Online ISBN: 978-1-4939-0770-0
eBook Packages: MedicineMedicine (R0)