
Abstract
EPR oximetry, which enables reliable, accurate, and repeated measurements of the partial pressure of oxygen in tissues, provides a unique opportunity to investigate the role of oxygen in the pathogenesis and treatment of several diseases including cancer, stroke, and heart failure. Building on significant advances in the in vivo application of EPR oximetry for small animal models of disease, we are developing suitable probes and instrumentation required for use in human subjects. Our laboratory has established the feasibility of clinical EPR oximetry in cancer patients using India ink, the only material presently approved for clinical use. We now are developing the next generation of probes, which are both superior in terms of oxygen sensitivity and biocompatibility including an excellent safety profile for use in humans. Further advances include the development of implantable oxygen sensors linked to an external coupling loop for measurements of deep-tissue oxygenations at any depth, overcoming the current limitation of 10 mm. This paper presents an overview of recent developments in our ability to make meaningful measurements of oxygen partial pressures in human subjects under clinical settings.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Considering currently available methodology to measure partial pressure of oxygen (pO2) in tissues in vivo, EPR (electron paramagnetic resonance) oximetry uniquely has the potential to provide direct, reliable, and accurate measurements on a temporal basis (repeated measurements) over long periods of time [1]. At present, EPR technologies and methodologies have been developed thoroughly for use in laboratory animals. However, translation of this capability for useful clinical applications is faced with some constraints and challenges with respect to instrumentation, probe administration, and regulatory issues [2, 3]. Scaling up the magnet and positioning systems to comfortably and safely accommodate human subjects within the active region of measurement has been accomplished. There is also concern that clinical EPR oximetry requires the placement of an exogenous probe in the tissue. The probe, once implanted using a minimally invasive surgical procedure, will stay in the tissue for a desired length of period or left permanently enabling subsequent measurements of pO2 noninvasively and repeatedly, a unique capability that no other technique can match. However, from a regulatory point of view, if the tissues are directly exposed to the probe, this procedure raises safety concerns for use in humans and thus necessitates elaborate studies, which are both expensive and time-consuming in order to get FDA clearance. This paper gives an update of the development of EPR oximetry as a viable clinical tool for measurement of oxygen concentration in humans.
2 Probes for Clinical EPR Oximetry
2.1 India Ink
The potential of India ink as a probe for clinical EPR oximetry has been recognized for some time [4, 5]. India ink has very high sensitivity to oxygen, high stability in tissues, and no clinically significant toxicity. Moreover, it has been approved for clinical use as a tissue marker, which makes it immediately usable for clinical measurements. Pre-clinical and clinical measurements have shown the feasibility and safety of India ink for repeated measurements of pO2 from easily-accessible, subcutaneous sites [6]. Despite the advantage that it is readily usable for clinical applications, India ink has some limitations, including a tendency to diffuse, reducing spatial resolution, and only moderate EPR detection sensitivity. We have therefore focused considerable effort, and made significant progress, on developing complementary alternatives to India ink, using highly oxygen-sensitive materials in biocompatible coatings that can be used in human subjects.
2.2 High-Sensitive Crystalline Probes
Synthetic materials based on lithium phthalocyanine and derivatives [7–10] possess many desirable properties to make them ideally-suited for clinical EPR oximetry. These are well-characterized crystalline particulates that exhibit substantially greater sensitivity to oxygen than India ink. We have developed an array of useful materials having a range of oxygen sensitivity and applicability to a broader range of oxygen levels. We have extensively used these probes in animal models of cancer, heart disease, and wound healing [11–15]. The results show substantially high oxygen sensitivity, spatial resolution, tissue stability, and biocompatibility, which gives these probes great potential and makes them highly promising for use in humans. However, regulatory approvals are required before testing them in humans.
2.3 Polymer-Encapsulated High-Sensitive Crystalline Probes for Safe Use in Humans
The most notable drawback and potential limitation to the use of the crystalline materials for clinical applications is the need to leave them permanently in the tissue, which may present practical barriers for obtaining approval for use in human subjects. Therefore, we are developing an alternative approach for their clinical use. The raw particulates (of 10–100 μm size) are embedded in biocompatible materials that have high oxygen permeability [16, 17]. The probes are effectively shielded from interaction with the biological milieu that could result in biochemical degradation and breakdown, as well as limiting the probability of local and/or systemic toxicity effects from interactions of the probe with the tissues. The implants could be left in the tissue or removed when no longer needed. We have especially used polydimethylsiloxane (PDMS), a silicone polymer with properties desirable for encapsulation of oximetry probes. PDMS is biocompatible, highly flexible, oxygen permeable, and has been used in a wide range of medical device and health-care applications. Furthermore, PDMS has been approved for use in human subjects and is one of the reference materials provided by the National Heart Lung and Blood Institute for standardized biocompatibility testing. We have used PDMS to encapsulate LiNc-BuO and developed the implants in the form of thin films (OxyChip). The efficacy and safety of OxyChip have been well characterized in animal models [17, 18]. We have taken steps to obtain investigational device exemption (IDE) status from FDA for testing the OxyChips in human subjects. The OxyChip implants will be used for oxygen measurements up to a depth of 10 mm.
2.4 Implantable Oxygen Sensors (ImOS) for Deep-Tissue Oximetry
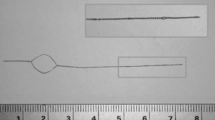
The penetration depth of conventional resonators at L-band frequencies (approximately 1.2 GHz) is limited due to non-resonant absorption of microwave energy and hence they are not capable of making measurements deeper than 10 mm in tissues. To overcome this limitation, we have developed a new class of resonators called implantable resonators capable of deep-tissue pO2 measurements anywhere in the body, and at multiple sites, simultaneously [19–21]. The implantable resonator-based oxygen sensors (ImOS) are assembled with thin twisted enameled copper wires (thickness: 0.15 mm) as transmission lines and contain two sets of loops, a sensory loop of 0.2- to 0.3-mm diameter at one end and a coupling loop of about 10-mm diameter at the other end [21]. The sensory loop is loaded with the oximetry probe embedded in a gas-permeable polymer material. The entire ImOS is coated with a biocompatible polymer. The sensory tip is surgically implanted in the desired tissue and the coupling loop is placed subcutaneously and coupled inductively to an external loop resonator of the EPR spectrometer during measurements. The total length of the transmission line can be anywhere from a few mm to more than 20 cm, depending on measurement depth that is needed. The ImOS can also be prepared to have multiple sensory tips to enable oximetry from multiple sites, simultaneous. Results using animals have shown substantial advantages of the ImOS with respect to EPR signal intensity and repeated measurements at deep sites when compared to traditional oximetry [19, 21]. FDA clearance for the use of implantable resonators in humans is expected to be less problematic.
2.5 Multisite Oximetry
Traditional EPR oximetry provides average pO2 estimates based on the summed signals detected from spins within the sensitive volume of the resonator. In order to provide additional spatial resolution of pO2 within the tissues, we have developed procedures for simultaneous spatially-resolved measurements from multiple implants, as well as implantable resonators with multiple sensory tips that are spatially distributed within the tissue [19, 20]. The multi-site measurement technique uses magnetic field gradients to spectrally distinguish their respective signals. Multisite oximetry has been demonstrated in a number of applications including rodent models of brain tumor and stroke [19, 20].
3 First Clinical Oximetry Data
We have demonstrated that oxygen measurements can be made in human subjects in superficial tumors using India ink, the only currently approved material for use in human subjects [6]. Extensive pre-clinical and clinical developments have shown the feasibility and safety of repeated oxygen measurements for easily-accessible, subcutaneous sites. EPR oximetry measurements in human subjects are performed using the clinical whole-body EPR spectrometer consisting of a 420-Gauss permanent magnet, magnetic field modulation and sweep coils, RF detection system including surface-loop resonators, and computer control [6]. The spectrometer operates at an L-band frequency (approximately 1.2 GHz), where a practical compromise between RF penetration depth and EPR sensitivity is achieved. At this frequency RF penetration depths of approximately 10 mm are achieved. So far, we have obtained pO2 data in superficial tumors at different sites in 14 patients, in subcutaneous foot tissues of nine normal volunteers, and one patient in a post-operative irradiated field [22].
The experimental procedure was purposely simple, using an approach to make the measurements under conditions that could readily be incorporated into normal clinical processes [6]. The India ink was inserted into the tumors or other tissues of interest in the outpatient clinic, with optional local anesthesia and using sterile procedures. A 21- to 23-gauge hypodermic needle and 30-gauge tuberculin syringe were used to insert 10–25 μl of sterilized India ink (a slurry of 200 mg/ml of Printex-U carbon black in 0.9 % NaCl and 1.25 % carboxymethylcellulose), whose response to oxygen had been well calibrated in vitro and in vivo in animals. One to five days later, a baseline measurement was made and then the subject was given 100 % oxygen to breathe through a regular simple face mask. EPR measurements were made continuously while breathing 100 % oxygen and then when the patient returned to breathing room air. For foot measurements in normal subjects, an additional period was included where compression was applied to temporarily suspend blood supply to the tissue and induce hypoxia [6]. These procedures took less than an hour in total and were very well tolerated by all subjects. The data obtained from the small number of tumor types led to the following conclusions: (1) The tumors varied considerably in their baseline pO2, which ranged from 0 to 10 Torr; (2) The subjects varied considerably as to whether their tumors responded to increased oxygen in the breathing gas (4 out of 14 did not respond); (3) The amount of the increase in tumor oxygen varied widely among the responders (3–100 Torr). Even with such a limited amount of data, these results indicate that the ability to make repeated measurements of oxygen in tumors could be quite useful clinically.
These studies demonstrate that the measurements can be made under conditions compatible with usual clinical practice. The observation that a number of tumors did not respond at all to increases in the amount of oxygen in the inspired gas illustrates how misleading it could be to try to evaluate the ability of hyperoxygenation strategies to improve outcomes without being able to detect whether the treatment did actually change pO2 in the tumor [22]. The EPR-based measurements of tumor pO2 values and their variable response to hyperoxygenation treatments also agree with the computerized Eppendorf pO2 histogram data obtained from several studies in human [23].
Foot measurements demonstrated variations in the baseline levels between volunteers and during repeated measurements [6]. Such variations are likely due to acute and gradual changes in the local tissue pO2. In the days immediately following ink injection, near anoxic pO2 levels were observed, which may be due to trauma and acute inflammation associated with the injection. The pO2 values, however, gradually increased to levels near 30 Torr over the following weeks. Compression of the thigh led to near anoxia within the foot tissue, followed immediately by full recovery to the baseline pO2 level as soon as the compression was released. A significant increase in the tissue pO2 was consistently observed during repeated experiments with oxygen breathing in each volunteer. The changes in the tissue oxygenation observed during hyperoxygenation and compression are likely to be useful, as it will provide information not only about the tissue oxygen status, but also functional information about perfusion, diffusion of oxygen into the tissues, and oxygen consumption.
4 Conclusion
The development of in vivo EPR oximetry as a viable clinical tool for repeated, direct measurements of tumor pO2 and other tissues in human subjects in compatibility with clinical practice has continued successfully. With the availability of high-sensitive, bio-safe probes, instrumentation and procedures for multiple site, and deep-tissue measurements it will soon be possible to obtain regulatory approvals and begin to make routine clinical measurements of pO2 in human subjects. These new approaches should significantly expand the applicability of clinical EPR oximetry.
References
Ahmad R, Kuppusamy P (2010) Theory, instrumentation, and applications of electron paramagnetic resonance oximetry. Chem Rev 110:3212–3236
Swartz HM, Khan N, Buckey J, Comi R, Gould L, Grinberg O, Hartford A, Hopf H, Hou H, Hug E, Iwasaki A, Lesniewski P, Salikhov I, Walczak T (2004) Clinical applications of EPR: overview and perspectives. NMR Biomed 17:335–351
Swartz HM, Walczak T (1998) Developing in vivo EPR oximetry for clinical use. Adv Exp Med Biol 454:243–252
Swartz HM, Liu KJ, Goda F, Walczak T (1994) India ink: a potential clinically applicable EPR oximetry probe. Magn Reson Med 31:229–232
Goda F, Liu KJ, Walczak T, O’Hara JA, Jiang J, Swartz HM (1995) In vivo oximetry using EPR and india ink. Magn Reson Med 33:237–245
Williams BB, Khan N, Zaki B, Hartford A, Ernstoff MS, Swartz HM (2010) Clinical electron paramagnetic resonance (EPR) oximetry using india ink. Adv Exp Med Biol 662:149–156
Liu KJ, Gast P, Moussavi M, Norby SW, Vahidi N, Walczak T, Wu M, Swartz HM (1993) Lithium phthalocyanine: a probe for electron paramagnetic resonance oximetry in viable biological systems. Proc Natl Acad Sci U S A 90:5438–5442
Ilangovan G, Manivannan A, Li H, Yanagi H, Zweier JL, Kuppusamy P (2002) A naphthalocyanine-based EPR probe for localized measurements of tissue oxygenation. Free Radic Biol Med 32:139–147
Pandian RP, Parinandi NL, Ilangovan G, Zweier JL, Kuppusamy P (2003) Novel particulate spin probe for targeted determination of oxygen in cells and tissues. Free Radic Biol Med 35:1138–1148
Pandian RP, Dolgos M, Marginean C, Woodward PM, Hammel PC, Manoharan PT, Kuppusamy P (2009) Molecular packing and magnetic properties of lithium naphthalocyanine crystals: hollow channels enabling permeability and paramagnetic sensitivity to molecular oxygen. J Mater Chem 19:4138–4147
Bratasz A, Pandian RP, Ilangovan G, Kuppusamy P (2006) Monitoring oxygenation during the growth of a transplanted tumor. Adv Exp Med Biol 578:375–380
Eubank TD, Roberts RD, Khan M, Curry JM, Nuovo GJ, Kuppusamy P, Marsh CB (2009) Granulocyte macrophage colony-stimulating factor inhibits breast cancer growth and metastasis by invoking an anti-angiogenic program in tumor-educated macrophages. Cancer Res 69:2133–2140
Khan M, Kutala VK, Vikram DS, Wisel S, Chacko SM, Kuppusamy ML, Mohan IK, Zweier JL, Kwiatkowski P, Kuppusamy P (2007) Skeletal myoblasts transplanted in the ischemic myocardium enhance in situ oxygenation and recovery of contractile function. Am J Physiol Heart Circ Physiol 293:H2129–H2139
Khan M, Meduru S, Mohan IK, Kuppusamy ML, Wisel S, Kulkarni A, Rivera BK, Hamlin RL, Kuppusamy P (2009) Hyperbaric oxygenation enhances transplanted cell graft and functional recovery in the infarct heart. J Mol Cell Cardiol 47:275–287
Selvendiran K, Bratasz A, Kuppusamy ML, Tazi MF, Rivera BK, Kuppusamy P (2009) Hypoxia induces chemoresistance in ovarian cancer cells by activation of signal transducer and activator of transcription 3. Int J Cancer 125:2198–2204
Meenakshisundaram G, Eteshola E, Pandian RP, Bratasz A, Lee SC, Kuppusamy P (2009) Fabrication and physical evaluation of a polymer-encapsulated paramagnetic probe for biomedical oximetry. Biomed Microdevices 11:773–782
Meenakshisundaram G, Pandian RP, Eteshola E, Lee SC, Kuppusamy P (2010) A paramagnetic implant containing lithium naphthalocyanine microcrystals for high-resolution biological oximetry. J Magn Reson 203:185–189
Meenakshisundaram G, Eteshola E, Pandian RP, Bratasz A, Selvendiran K, Lee SC, Krishna MC, Swartz HM, Kuppusamy P (2009) Oxygen sensitivity and biocompatibility of an implantable paramagnetic probe for repeated measurements of tissue oxygenation. Biomed Microdevices 11:817–826
Hou H, Dong R, Li H, Williams B, Lariviere JP, Hekmatyar SK, Kauppinen RA, Khan N, Swartz H (2012) Dynamic changes in oxygenation of intracranial tumor and contralateral brain during tumor growth and carbogen breathing: a multisite EPR oximetry with implantable resonators. J Magn Reson 214:22–28
Hou H, Li H, Dong R, Mupparaju S, Khan N, Swartz H (2011) Cerebral oxygenation of the cortex and striatum following normobaric hyperoxia and mild hypoxia in rats by EPR oximetry using multi-probe implantable resonators. Adv Exp Med Biol 701:61–67
Li H, Hou H, Sucheta A, Williams BB, Lariviere JP, Khan MN, Lesniewski PN, Gallez B, Swartz HM (2010) Implantable resonators: a technique for repeated measurement of oxygen at multiple deep sites with in vivo EPR. Adv Exp Med Biol 662:265–272
Swartz HM, Williams BB, Zaki BI, Hartford AC, Jarvis LA, Chen EY, Comi RJ, Ernstoff MS, Hou H, Khan N, Swartz SG, Flood AB, Kuppusamy P (2013) Clinical EPR: unique opportunities and some challenges. Acad Radiol 21:197–206
Vaupel P, Hockel M, Mayer A (2007) Detection and characterization of tumor hypoxia using pO2 histography. Antioxid Redox Signal 9:1221–1235
Acknowledgments
The development and applications of EPR oximetry reported in this manuscript was supported by the following grants from the National Institutes of Health (NIH): P01 EB002180 (HMS), R21 CA121593 (HMS), R21DK072112 (NK), and R01 EB004031 (PK).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media, LLC
About this paper
Cite this paper
Swartz, H.M. et al. (2014). Advances in Probes and Methods for Clinical EPR Oximetry. In: Swartz, H.M., Harrison, D.K., Bruley, D.F. (eds) Oxygen Transport to Tissue XXXVI. Advances in Experimental Medicine and Biology, vol 812. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0620-8_10
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0620-8_10
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-0583-6
Online ISBN: 978-1-4939-0620-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)