
Abstract
Pulmonary arterial hypertension (PAH) is a severe disease characterized by pulmonary vascular remodeling, increased pulmonary vascular resistance (PVR), progressive arterial stiffening, and ultimately right ventricular (RV) failure and death. Despite state-of-the-art therapy and recent advances in our understanding of the molecular mechanisms and genetic determinants of disease, morbidity and mortality remain unacceptably high. Vascular remodeling in PAH is characterized by endothelial dysfunction with release of vasoactive mediators, growth factors, and cytokines; smooth muscle cell hyperplasia and hypertrophy with medial wall thickening; and adventitial fibroblast proliferation, extracellular matrix deposition, and myofibroblast differentiation. Growing evidence through animal and human studies suggests that oxidative stress plays a key role in the pathogenesis of PAH. Oxidative stress in PAH is associated with increased production of reactive oxygen species (ROS) and reactive nitrogen species (RNS), decreased nitric oxide (NO) levels, and mitochondrial dysfunction. Dysregulation of ROS/RNS/NO homeostasis can impair vascular tone and lead to activation of antiapoptotic and pro-proliferative signaling pathways resulting in aberrant vascular remodeling in the lung. Increases in oxidative stress have been demonstrated in animal PH models and PAH patients, and therapies targeting oxidative stress have shown promise in animal models of PH. This chapter will examine the mechanisms of ROS generation in the pulmonary vasculature, review the available animal and human data on the role of oxidative stress in the pathobiology of PAH, and discuss potential therapies targeting oxidative stress for the treatment of patients with PAH.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Pulmonary Vascular Remodeling
- Pulmonary Arterial Smooth Muscle Cells (PASMC)
- Persistent Pulmonary Hypertension Of The Newborn (PPHN)
- PASMC Proliferation
- Nicotine Adenine Dinucleotide Phosphate (NADPH)
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
15.1 Introduction
Pulmonary arterial hypertension (PAH) is a complex and multidisciplinary disorder comprising a series of diseases that result from restricted blood flow through the pulmonary arterial circulation [213, 232]. All of these conditions share a common arterial histopathology characterized by medial hypertrophy, eccentric and concentric intimal fibrosis, and plexiform lesions [114, 213]. The pathophysiology of PAH is not completely understood. Many factors have been shown to be involved in the pathogenesis of PAH, including growth factors, pro-inflammatory molecules, vascular tone mediators, genetic mutations, microRNAs (miRs), and oxidative stress [5, 221, 284]. Currently, the treatment for PAH remains limited and the disease is still associated with a poor long-term prognosis [221]. Growing evidence suggests that reactive oxygen species (ROS) and oxidative stress play a pathogenic role in PAH and some antioxidants appear to be useful in various forms of pulmonary hypertension (PH) [373].
15.2 Pulmonary Arterial Hypertension
15.2.1 Epidemiology
PAH was previously considered a rare disease with an unknown frequency, but in 2006 a French registry reported a prevalence of 15 per million [158, 232]. The most common cause found in this study was idiopathic pulmonary arterial hypertension (IPAH) accounting for 39.2 % of the cases, followed by anorexigen exposure, connective tissue disease, congenital heart diseases (CHDs), portal hypertension, and HIV infection [158]. The Scottish morbidity record found a prevalence of 52 cases per million in an adult population [273]. In both studies, PAH was more common in the female population [158]. According to the Centers for Disease Control and Prevention (CDC), deaths attributed to PH varied between 11,000 and 16,000 per year between 1980 and 2002 [159].
15.2.2 Diagnosis and Pathological Findings
15.2.2.1 Signs and Symptoms
The main symptoms found in patients with PH are dyspnea on exertion (around 60 % of patients), fatigue, angina pectoris, syncope, palpitations, and lower extremity edema [232]. Clinical signs include accentuated pulmonary component of S2 audible at the apex (90 % of patients with IPAH), early systolic click, mid-systolic ejection murmur, left parasternal lift, right ventricular (RV) S4, and increased jugular “a” wave [232]. In more advanced stages of the disease, other signs may be seen, including a holosystolic murmur that increases with inspiration, increased jugular “v” waves, pulsatile hepatomegaly, hepatojugular reflex, peripheral edema, ascites, low pulse pressure, and cool extremities [232]. These usually indicate right ventricular (RV) failure [230]. The main chest X-ray finding suggesting PH is enlargement of main and hilar pulmonary arterial shadows accompanied by attenuation of peripheral pulmonary vascular markings [213, 230]. Electrocardiographic findings that should raise the suspicion of PH include right axis deviation, signs of RV hypertrophy (tall R wave in RV leads and R/S ratio <1 in V5 and V6), and right atrial enlargement (tall p wave in leads II, III, and aVF and frontal p axis of more than 75°) [213, 230, 232].
15.2.2.2 Diagnosis and Classification
PAH is defined as a mean pulmonary arterial pressure (mPAP) greater than 25 mmHg at rest with a normal pulmonary capillary wedge pressure (PCWP) of 15 mmHg or less and a pulmonary vascular resistance (PVR) greater than 3 Wood units [232]. Screening is crucial in all patients with risk factors for PAH, such as bone morphogenetic protein receptor 2 (BMPR2) mutation, first-degree relative with BMPR2 mutation, history of anorexigen intake (fenfluramine), HIV infection, portal hypertension, CHD with systemic-to-pulmonary shunt, systemic sclerosis, recent acute pulmonary embolism, and sickle cell disease (SCD) [232]. If clinical, radiologic, and electrocardiographic findings raise the suspicion of PH, a Doppler echocardiogram is the screening test of choice, providing an estimate of the RV systolic pressure and RV function, as well as allowing identification of potential cardiac causes of PH [230, 232]. Common echocardiographic findings seen in patients with PAH include enlargement of right-sided chambers, abnormal surface of the interventricular septum, and underfilled left atrium and left ventricle [232]. The European Society of Cardiology (ESC) and the European Respiratory Society (ERS) proposed a series of arbitrary criteria for establishing the presence of PH based on echocardiographic findings that have been shown to correlate with PH on right heart catheterization (RHC) (Table 15.1) [125]. In cases where a tricuspid regurgitation profile cannot be determined by conventional echocardiography, intravenous saline or encapsulated microbubble contrast agents can be administered to enhance the signal [147, 232]. Patients with abnormal echocardiograms, including RV systolic pressure greater than 40 mmHg, should be further evaluated [232].
When continuing evaluation of these patients, all causes of PH (including PAH and non-PAH causes) must be considered in order to guide proper management [232]. The revised WHO classification of PH (Dana Point 2008) is shown in Table 15.2 [317]. Although all of the secondary causes of PH should be evaluated before establishing the diagnosis of PAH, excluding chronic thromboembolic pulmonary hypertension (CTEPH) is particularly important because the management of these patients is very different, as some patients may be eligible for surgical treatment [248], and this condition may coexist in the presence of other risk factors for PAH such as scleroderma [232]. The screening test of choice for ruling out CTEPH is the ventilation/perfusion lung scan, since a normal result virtually rules out this condition [148, 232, 248]. Despite the usefulness of the V/Q scan in patients without underlying lung disease, pulmonary multidetector CT angiography (MDCTA) is now considered the gold standard for the diagnosis of CTEPH because it allows identification of thrombosis, concomitant lung changes, and can aid in the diagnosis of pulmonary embolism in patients with preexisting lung disease [176]. Even though Doppler echocardiography aids in the detection of possible PH, the only way to confirm the diagnosis is through RHC [232, 248]. Once left ventricular or valvular disease (Group 2), lung disease (Group 3), and CTEPH (Group 4) are excluded, a RHC showing a mPAP greater than 25 mmHg and a PVR greater than 3 Wood units with a normal PCWP <15 mmHg confirm the presence of PAH, which means that it remains a diagnosis of exclusion [232].
The most recent classification of PH was established in the fourth World Symposium on Pulmonary Hypertension that was held in Dana Point in 2008 [317]. Patients with PAH should be classified into one of the five groups shown in Table 15.2 [317].
15.2.2.2.1 Idiopathic Pulmonary Arterial Hypertension and Heritable Pulmonary Arterial Hypertension: Groups 1.1 and 1.2
IPAH is sporadic and unrelated to any family history or identified risk factor [317]. Heritable PAH is diagnosed when there are mutations of genes that have been identified as having a strong association with the PAH phenotype, such as the BMPR2 gene, which is present in 70 % of heritable cases. Other mutations that have been identified in patients with PAH are located in the activin receptor-like kinase type 1 (ALK1) or endoglin (ENG) genes [248, 317]. Some studies have also suggested that mutations in the Smad proteins and caveolin-1 (CAV1) genes may also predispose to PAH [9, 18, 28, 259, 316]. It is critical that these patients get involved in a comprehensive program that includes genetic testing, counseling, and discussion of risks and benefits [21, 317].
15.2.2.2.2 Drug and Toxin-Induced PAH: Group 1.3
Drug and toxin-induced PAH is further classified depending on the strength of the association between the exposure and the presence of disease, but the main substances that have been found to have a strong association with PAH are anorexigens (aminorex, fenfluramine) and toxic rapeseed oil. Other agents that have been related to PAH include cocaine, phenylpropanolamine, St. John’s Wort, chemotherapeutic medications, selective serotonin reuptake inhibitors (SSRIs), and amphetamines [317]. However, further studies are needed to establish the true association of these latter substances.
15.2.2.2.3 Associated with PAH: Group 1.4
Associated with PAH (APAH) includes connective tissue disorders, congenital systemic-to-pulmonary shunts, portal hypertension, HIV infection, schistosomiasis, and chronic hemolytic anemia [232].
15.2.2.2.3.1 PAH Associated with Connective Tissue Diseases: Group 1.4.1
The presence of PAH has been well established in systemic sclerosis, with an estimated prevalence of 7–12 % and is associated with poor prognosis in this group of patients [138, 248, 253]. The presence of PAH has also been reported in systemic lupus erythematosus (SLE) and mixed connective tissue disease, but the exact prevalence has not been determined [317]. Other mechanisms may be involved in the induction of PH in these patients, such as left heart dysfunction, lung fibrosis, and primary cardiac involvement, which highlights the importance of determining the true cause of PH with RHC.
15.2.2.2.3.2 PAH Associated with HIV Infection: Group 1.4.2
The presence of PAH in patients with HIV infection is rare, with a prevalence of 0.5 % [28, 317]. Clinical, hemodynamic, and histological findings are very similar to those seen in IPAH patients [28, 317]. Concomitant PAH in patients with HIV significantly worsens their prognosis [243].
15.2.2.2.3.3 Porto-pulmonary Hypertension: Group 1.4.3
PAH associated with an increase in the pressure of the portal circulation is classified as porto-pulmonary hypertension (POPH) [248]. Some prospective studies have shown a prevalence of 5–6 % in patients with advanced liver disease [303]. POPH is also a predictor of poor prognosis, since these patients are usually not eligible for liver transplantation due to the high perioperative morbidity and mortality that have been documented in this population [303]. RHC should be performed to accurately diagnose PAH, since other factors, such as fluid overload and diastolic dysfunction, may elevate the pressure of the pulmonary vasculature in patients with portal hypertension [317].
15.2.2.2.3.4 Congenital Heart Diseases: Group 1.4.4
PAH is a fairly common complication of CHD in patients that have left-to-right shunts [81, 317]. It is estimated that 4–15 % of patients with CHD will develop PAH [81] and the most common anomalies associated with PAH are ventricular septal defects (VSD) [104]. Patients with CHD who develop PAH are classified into four groups: Eisenmenger’s syndrome, PAH associated with systemic-to-pulmonary shunts, PAH with small defects, and PAH after corrective cardiac surgery [81, 317]. Eisenmenger’s syndrome is the most severe form of PAH in this context, where there is a reversal of the initial shunt to a right-to-left shunt, where deoxygenated blood is being returned to the systemic circulation and cyanosis ensues along with other potential complications such as blood hyperviscosity, hemostasis, stroke, and endocarditis [81].
15.2.2.2.3.5 Schistosomiasis: Group 1.4.5
Before the Dana Point classification of PH, schistosomiasis was listed under the subgroup of chronic thrombotic or thromboembolic disease. Nevertheless, recent evidence has shown that the obstructive mechanism of schistosoma eggs plays a minor role in the induction of PH in this group of patients, and clinical and pathological findings resemble those of IPAH [248, 317]. Although the exact mechanisms responsible for the induction of PH in patients with schistosomiasis remain largely unknown, the inflammatory response to the schistosoma antigens with the release of cytokines that have also been proven to be upregulated in IPAH, as well as the presence of hepatosplenic disease and portal hypertension likely plays an important role [133]. For these reasons, schistosomiasis is now listed under Group 1 of the Dana Point Classification [248, 317].
15.2.2.2.3.6 Chronic Hemolytic Anemia: Group 1.4.6
PAH has been identified as a complication of many hemolytic anemias including SCD, thalassemia, hereditary spherocytosis, stomacytosis, and microangiopathic hemolytic anemia [317]. Histological findings seen in IPAH have been commonly described in patients with SCD [317]. However, the true prevalence of PAH in these patients remains unknown since most epidemiological studies have defined the presence of PH in terms of echocardiography rather than RHC [317]. Such studies have documented a prevalence of 20–30 % in patients with SCD and 10–75 % in patients with thalassemia [219]. The pathophysiology of PAH induced by hemolysis is not entirely understood, but mechanisms such as inactivation of nitric oxide (NO) by free hemoglobin, depletion of l-arginine in the presence of elevated arginase, and increased endothelin-1 (ET-1) responses have been described [110, 250, 301].
Pulmonary veno-occlusive disease (PVOD) and pulmonary capillary hemangiomatosis (PCH) are rare conditions that were included in Group 1 of the most recent WHO classification of PH (Dana Point 2008) [317]. This inclusion was based on the similarities of PVOD/PCH and PAH regarding histologic findings, clinical presentation, risk factors, and potential for inheritance [317]. Nevertheless, they are still considered separate conditions classified as 1′ (Table 15.2) [317].
As discussed above, PAH is a diagnosis of exclusion and both PAH and non-PAH causes of PH may overlap. Therefore, it is crucial to evaluate and classify patients based on their etiology of PH and WHO group (Table 15.2), and confirm that the elevated pressure is limited exclusively to the pulmonary arterial system [90]. This can only be accomplished with a RHC, which remains an indispensable tool in the assessment of patients with PH [90]. Additionally, this test gives further information that is useful to determine prognosis, such as the severity of the hemodynamic impairment and the vasoreactivity of the pulmonary circulation [125]. The diagnostic PH algorithm established by the American College of Cardiology Foundation/American Heart Association Task Force (ACCF/AHA) experts can be found in Fig. 15.1 [125, 232].

Diagnostic algorithm for pulmonary hypertension. Reproduced with permission from [125]
15.2.2.3 Gold Standard and Pathological Findings
The gold standard for the diagnosis of PAH is the RHC since it is defined by hemodynamic criteria [125, 232]. Lung biopsy in patients with PAH is not recommended, since it has a high morbidity and mortality in this group of patients and is unlikely to change the diagnosis or treatment [125]. Therefore, the natural history of vascular lesions that occur in PAH is not entirely known because biopsies are not regularly obtained in these patients [232]. Arterial abnormalities seen in histological studies of patients with PAH include intimal hyperplasia, inflammation, adventitial proliferation, medial hypertrophy, thrombosis in situ, abnormal muscularization of nonmuscular precapillary arteries, and plexiform arteriopathy [232, 284].
15.2.2.4 Prognosis
Despite a better understanding of the pathophysiological mechanisms involved in PAH and the improvement in treatment options, the long-term prognosis remains poor [232]. Data from the French Network on Pulmonary Hypertension Registry revealed a survival rate of 83 % (95 % CI 72–95 %) at 1 year, 57 % (95 % CI 57–79 %) at 2 years, and 58 % at 3 years [158].
15.2.3 Pathophysiology
PH results from an increase in PVR and restriction in blood flow through the pulmonary vascular circulation, finally leading to altered right heart function [232]. Elevation of PVR and decreases in pulmonary vascular compliance cause increased RV afterload, which ultimately results in adaptive RV hypertrophy [221]. If the pressure overload persists, the RV eventually dilates and becomes dysfunctional, leading to increase in RV contraction time, asynchrony, and decreased RV stroke volume [221]. All of the latter changes result in underfilling of the left ventricle (LV) and subsequent reduction in cardiac output [126, 221, 223].
The main cause of elevated PVR is the reduction in luminal cross section due to vascular remodeling, which results from altered cell growth, apoptosis, migration, and production of extracellular matrix [5, 232]. Various stimuli can induce vascular remodeling, including mechanical forces (changes in transmural pressure, stretch, shear stress), inflammatory cytokines, serotonin (5-hydroxytryptamine [5-HT]), hypoxia, growth factors, angiotensin II (AT-II), endothelin-1 (ET-1), increased serine elastase activity, and increased production of ROS [5]. All of these stimuli induce changes in different cells that are responsible for the changes seen in vascular remodeling, mainly endothelial cells (EC) and smooth muscle cells (SMC) [5].
15.2.3.1 Pulmonary Arterial Endothelial Cells
Pulmonary arterial endothelial cells (PAEC) that are exposed to injury caused by the various stimuli mentioned above may become dysfunctional and respond in ways that contribute to vascular remodeling [5]. This remodeling occurs through the release of agents that stimulate proliferation of pulmonary arterial smooth muscle cells (PASMC), such as platelet-derived growth factor (PDGF) and fibroblast growth factor-2 (FGF-2) and/or failure to produce factors that suppress proliferation of PASMC, such as apelin [284]. Furthermore, PAEC from patients with IPAH have increased expression of the Tie2 receptor, which results in increased production of 5-HT and subsequent PASMC proliferation (Fig. 15.2) [5, 91, 284]. Moreover, dysfunctional PAEC seen in PH generate less nitric oxide (NO) as a result of uncoupling of endothelial NO synthase (eNOS), which ultimately leads to an increase in the production of ROS, particularly superoxide (Fig. 15.2) [5]. The effect of ROS in pulmonary vascular remodeling is further discussed in the next section. Uncoupling of eNOS is related to low levels of enzymatic cofactors l-arginine and tetrahydrobiopterin (BH4) [200]. l-Arginine depletion results from the upregulation of arginase, which has been documented both in animal and human EC exposed to different stimuli, including hypoxia, lipopolysaccharide (LPS), shear stress, and inflammatory cytokines [105]. Increased asymmetric dimethylarginine (ADMA) has also been found to be elevated in patients with PH [5, 312]. ADMA is an endogenous analogue of l-arginine and competes for the substrate binding site of eNOS, which can further contribute to the uncoupling of the enzyme [5, 284]. ADMA has also been shown to contribute to mitochondrial dysfunction through the increase of uncoupling protein-2 (UCP2), which leads to augmented mitochondrial ROS (mROS) production and decreased ATP synthesis (Fig. 15.2) [5, 329].

Overview of mechanisms involved in the pathogenesis of PAH. Diverse stimuli result in endothelial dysfunction and abnormal PASMC proliferation. Decreased NO production in PAEC due to eNOS uncoupling attenuates relaxation of PASMC and promotes vasoconstriction. Factors that contribute to eNOS uncoupling include decreased arginine, increased ADMA, enhanced arginase activity, low BH4, and disruption of the zinc tetrathiolate (ZnS4) cluster. The eNOS uncoupling not only results in lower NO levels but also increases ROS production. Upregulation of NADPH oxidase subunits further contributes to the generation of ROS. Altered function of potassium Kv channels in PASMC leads to membrane depolarization and opening of voltage-dependent calcium channels. Influx of calcium ions stimulates additional release of Ca2+ from the SR. Increased [Ca2+]cyt and upregulated membrane receptors (5-HT, ET-1, leukotrienes) decrease apoptosis and stimulate cell proliferation. Increased Ang-1 downregulates BMPR1A in PAEC and enhances 5-HT production, promoting PASMC contraction and proliferation. As a result of BMPRII mutations, PASMC display dysfunctional BMP signaling pathways, which normally inhibit cell proliferation and stimulate cell apoptosis. Mitochondrial dysfunction leads to increased ROS production and is evidenced by the low levels of SOD2, high levels of UCP2, and impaired function of complexes I and II. Increased activity of XO also results in higher production of ROS. Increased expression of the STAT3/Pim1/Src/NFAT axis and suppression of miR-204 also promote cellular proliferation and reduce apoptosis. TGF-β and BMP4 increase the expression of miR-143/miR-145 through the stimulation of Myocd and MRTF-A, respectively. These miRNAs inhibit KLF4 which ultimately results in enhanced contractile gene expression. PAEC pulmonary arterial endothelial cells, eNOS endothelial nitric oxide synthase, NADPH nicotinamide adenine dinucleotide phosphate, TGF-β transforming growth factor β, TGFRI type I receptor for TGF-β, TGFRII type II receptor for TGF-β, BH 4 tetrahydrobiopterin, ADMA asymmetric dimethylarginine, DDAH2 dimethylaminohydrolase-2, TIE2 tyrosine protein kinase receptor, Ang-1 angiopoietin, BMP bone morphogenetic protein, BMPR1A BMP receptor 1A, BMPRI BMP type I receptor, BMPRII BMP type II receptor, 5-HT 5-hydroxytryptamine, PASMC pulmonary arterial smooth muscle cells, VDCC voltage-dependent calcium channel, PIP2 phosphatidylinositol 4,5-bisphosphate, PLC phospholipase C, IP3 inositol triphosphate, DAG diacylglycerol, PKC protein kinase C, ROC receptor-operated calcium channel, SR sarcoplasmic reticulum, Kv channel voltage-gated potassium channel, SOD2 superoxide dismutase 2, UCP2 uncoupling protein-2, HIF-1α hypoxia-inducible factor α, XO xanthine oxidase, RAGE receptor for advanced glycation endproducts, AGE advanced glycation endproducts, RTK receptor tyrosine kinase, PDGF platelet-derived growth factor, VEGF vascular endothelial growth factor, STAT3 signal transducer and activator, NFAT nuclear factor of activated T-cells, MRTF myocardin-related transcription factor, Myocd myocardin, KLF4 Krüppel-like factor 4
In addition to decreased synthesis of the vasodilator NO, dysfunctional endothelial cells also produce lower levels of prostacyclin, and higher levels of vasoactive substances such as ET-1, AT-II, and thromboxane A2 (TXA2), and growth factors, namely PDGF, transforming growth factor β (TGF-β), FGF-2, and vascular endothelial growth factor (VEGF) [5, 100, 227, 361]. All of these may stimulate PASMC proliferation in vascular remodeling [5]. Finally, PAEC from patients with PAH seem to have increased glycolytic activity and a highly proliferative response to growth factors, which contributes to the formation of plexiform lesions [5, 284, 382]. PAEC seen in these lesions exhibit increased levels of hypoxia-inducible factor (HIF) subunits (HIF-1α and HIF-1β), which induce VEGF under hypoxic conditions [5, 342].
Elevated expression of VEGF and VEGF receptor 2 (VEGFR2) has been documented in plexiform lesions of patients with PAH [221, 342]. VEGF promotes survival and suppresses apoptosis in PAEC [221, 305]. However, mice and rats exposed to hypoxia combined with the VEGFR2 inhibitor, SU5416, develop PAH [221, 353]. Moreover, VEGF is decreased in the monocrotaline (MCT) rat model of PAH, which correlates with early endothelial injury. Overexpression of VEGF also protects against chronic hypoxia and MCT exposure, and VEGFR inhibition results in initial EC apoptosis with subsequent selection of EC clones that are resistant to apoptosis and form angio-obliterative lesions [221, 353]. Therefore, VEGF appears to play a crucial role in angiogenesis and EC growth after vascular injury. Other factors associated with plexiform lesions are angiopoietin 1, 5-lipoxygenase, survivin, and Ki-67 [5, 129, 131, 375]. However, the exact mechanisms responsible for the formation of plexiform lesions are not completely understood [5].
15.2.3.2 Pulmonary Arterial Smooth Muscle Cells
Many pathologic changes take place in the SMC layer of PAs during vascular remodeling. Proximal vessels usually undergo significant hypertrophy, while smaller resistance vessels commonly show hyperplasia [5, 231, 238]. Matrix protein deposition is also a characteristic feature of the muscular layer of PAs in PAH, where SMC seem to acquire a more synthetic, rather than contractile, phenotype, with larger endoplasmic reticula and Golgi apparatus, and increased production of collagen and elastin [5, 238]. Muscularization of otherwise nonmuscular blood vessels results from differentiation of pericytes into SMC and hypertrophy of SMC precursor cells [5, 284].
Factors that have been identified in the induction of SMC hypertrophy include bone morphogenetic protein 4 (BMP4), TGF-β1, 5-HT, ET-1, inhibition of glycogen synthase kinase 3β (GSK-3β), and activation of p70S6 kinase [5, 174]. Abnormal activation of transcription factors (HIF-1α and nuclear factor of activated T-cells [NFAT]), increased expression of survivin and PDGF, calcium overload, mitochondrial hyperpolarization, and decreased expression of voltage-gated potassium channels (Kv) all contribute to the increased survival and decreased apoptosis of PASMC seen in PAH (Fig. 15.2) [221, 232].
Finally, in vitro studies have shown that PASMC from PAH patients have higher mRNA and protein levels of Notch 3 and HES-5 [221]. Notch participates in vasculogenesis, angiogenesis, and differentiation of vascular SMC [11, 221]. HES-5, a target gene for Notch 3, is exclusively expressed in adult SMC and may be involved in SMC maturation and proliferation [53, 96, 221, 279].
15.2.3.3 Neointima Formation
The formation of a layer of cells and extracellular matrix between the endothelium and the internal elastic lamina occurs in severe PH [5, 387]. The neointima is composed of myofibroblasts that express SM markers such as smooth muscle α-actin and vimentin [5]. These cells lack markers of highly differentiated SMC, such as SM-myosin heavy chain, and do not exhibit EC markers either [5, 387]. The exact origin of these cells is unclear. They may originate in stem cells, transdifferentiation of endothelial cells, migration of SMC from the media, or migration of adventitial fibroblasts [5, 284]. This currently remains a subject of intense study [284].
15.2.3.4 Changes in the Adventitia
PAH is associated with thickening and disorganization of the pulmonary adventitia, with excessive activation of adventitial metalloproteases [232]. In patients with PAH related to collagen vascular diseases such as scleroderma, the adventitia appears markedly remodeled [5]. Activation of fibroblasts by different stimuli can induce a phenotypic change in these cells, altering their structure and functional behavior [5]. An example of this is the induction of a contractile phenotype in fibroblasts by TGF-β1 and TGF-β2 [5, 387]. The activation and proliferation of fibroblasts and myofibroblasts result in thickening of the adventitia in PH, and some studies have shown that these changes precede remodeling of the intima and SMC layer, which suggests that the initial detection of vascular injury might take place in the adventitia [5, 146].
15.2.3.5 Genes and Transcription Factors Involved in PAH
Genes associated with PAH have helped to identify potential mechanisms involved in the pathogenesis of the disease. Studies have shown that approximately 70 % of patients with heritable pulmonary arterial hypertension (HPAH) and 10–20 % of patients with IPAH are heterozygous for a mutation in BMPR2, which is a member of the TGF-β superfamily of growth factor receptors [284]. HPAH is inherited in an autosomal dominant fashion with incomplete penetrance and genetic anticipation [232]. The impaired function of the BMPR2 results in a loss of function of the SMAD signaling pathway, causing proliferation and decreased apoptosis of PASMC in response to TGF-β and BMP2 (Fig. 15.2) [232]. On the other hand, BMPR2 impairment in EC results in increased susceptibility to apoptosis, which alters the normal migration and survival of EC needed in angiogenesis and regeneration of damaged blood vessels (Fig. 15.2) [85, 284]. Abnormal BMPR2 signaling has also been associated with increased ET-1 production in human lung microvascular EC [221, 324].
Recently, signal transducer and activator of transcription 3 (STAT3) has been shown to participate in aberrant PASMC proliferation [221, 272]. IL-6, TGF-β, PDGF, VEGF, ET-1, and AT-II can activate STAT3, which in turn increases the expression of Pim1 (Fig. 15.2) [221, 272, 390]. PIM1 promotes the activation of NFAT, increasing cytokine secretion, enhancing PASMC proliferation, and suppressing PASMC apoptosis (Fig. 15.2) [221, 287]. STAT3 has also been implicated in induction of survivin expression through activation of Krüppel-like factor 5 (KLF5) and in downregulation of eNOS expression (Fig. 15.2) [74, 221].
Moreover, studies have shown that mice with deletion of the peroxisome proliferator-activator receptor gamma (PPAR-γ) gene develop spontaneous PAH [136], and mutations in this gene have also been identified in patients with severe PH [5, 12, 284]. PPAR-γ participates in the antiproliferative effect of BMP2 signaling in PASMC, which is BMPR2/PPAR-γ/ApoE dependent [8, 140, 221]. The receptor of advanced glycation end products (RAGE) is an upstream target of PPAR-γ in PAH, and has been shown to activate STAT3 and downregulate BMPR2 and PPAR-γ in PAH-PASMC (Fig. 15.2) [221, 236]. Furthermore, BMP2-mediated survival of PAEC depends on the formation of a nuclear complex between β-catenin and PPAR-γ [8]. One of the transcriptional targets of this complex is apelin, which is reduced in patients with IPAH [8]. Apelin promotes PAEC survival and migration, and suppresses PASMC growth [284]. Apelin-deficient PAEC have increased apoptosis and promote PASMC proliferation [8, 221]. Other genes that have been associated with the PAH phenotype include ALK1, ENG, and CAV1 [18, 59, 142, 218, 221].
15.2.3.6 MicroRNAs Involved in PAH
miRs are now of great interest in the study of diseases that display abnormal cell growth, since they are involved in various posttranscriptional regulatory mechanisms [221]. In PAH, only few miRs have been identified as being abnormally expressed [221]. Downregulation of miR-204 in PAH-PASMC was found to correlate with PAH severity and higher cell proliferation [74]. It was shown that downregulated levels of miR-204 enhance a constitutive activation of Src and STAT3, leading to an increase in PASMC proliferation (Fig. 15.2) [74]. Additionally, downregulation of miR-204 appears to upregulate IL-6 secretion, which in turn downregulates BMPR2 and further contributes to the proliferative phenotype of PAH-PASMC [221, 272]. IL-6 is a potent activator of STAT3, which means that these interactions result in a feed-forward loop between miR-204 downregulation and STAT3 (Fig. 15.2) [221].
Src and p53 pathways regulate the organization of miR-145 and miR-143, which are involved in SMC differentiation and proliferation [221, 283]. TGF-β and BMP4 stimulate the expression of myocardin (Myocd) and Myocd-related transcription factor A (MRTF-A), respectively. These factors in turn activate miR-143 and miR-145 transcription, resulting in decreased KLF4 expression and promotion of contractile gene expression in SMC (Fig. 15.2) [83, 221]. Plexiform and concentric lesions seen in patients with PAH display abnormal expression of miR-143/miR-145 and mice exposed to hypoxia show elevated levels of miR-145 [54, 221].
In PAEC, expression of miR-126 appears to be dysregulated specifically in plexiform lesions [36, 221]. This miR plays an important role in neovascularization, EC proliferation, and vascular integrity, and regulates factors involved in apoptosis and modulation of cell cycle arrest [221, 355, 391]. Other miRs that have been found to contribute to the pathogenesis of PAH include miR-150, which is reduced in patients with PAH and is associated with decreased NK cells and B1 cell expansion; miR-210, the miR most highly upregulated by hypoxia [195, 221]; miR-21, which is highly upregulated in hypoxia and appears to participate in abnormal proliferation and migration of PASMC [221]; and miR-17, which is also upregulated in hypoxia, and targets p21 and Janus kinase (JAK1) impairing angiogenic functions of endothelial cells [221]. miRs remain a subject of intense study, since they are regarded as useful biomarkers, prognostic tools, and potential targets for future therapies [221].
15.3 Oxidative Stress and PAH
Several studies have implicated oxidative stress in the pathogenesis of PAH. Oxidative and nitrosative stress are characterized by an imbalance between oxidant and antioxidant production that can lead to downstream cell and tissue damage. Oxidative stress in PAH is associated with increased production of ROS and reactive nitrogen species (RNS), decreased nitric oxide (NO) levels, and mitochondrial dysfunction. Dysregulation of ROS/RNS/NO homeostasis can impair vascular tone and lead to activation of antiapoptotic and mitogenic pathways resulting in cell hyperproliferation and obliteration of the vasculature in PAH.
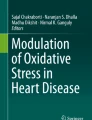
ROS are produced from oxygen during normal metabolic processes. ROS can be characterized as either free radicals, reactive molecules with one or more unpaired electrons, or nonradicals, molecules which share unpaired electrons between two free radicals [34] (Table 15.3). Hydroxyl radical (•OH) is considered the most reactive free radical in biological systems [335]. In the lung, ROS can be generated by alveolar epithelial cells, endothelial cells, alveolar macrophages, neutrophils, and eosinophils. In the pulmonary vasculature, ROS can be produced by complexes in the cell membrane, within mitochondria and peroxisomes, and from within the cytoplasm. The major enzymatic sources of ROS include uncoupled eNOS, xanthine oxidase (XO), nicotine adenine dinucleotide phosphate (NADPH) oxidase (NOX), and mitochondrial electron transport enzymes (Fig. 15.3). RNS are various nitrogen-containing species (Table 15.3) that can alter protein function via S-nitrosylation, tyrosine nitration, and glutathionylation. NO is the predominant source of nitrosative stress and, at high concentrations, can react with ROS to generate other RNS, including peroxynitrite, ONOO‾.

Overview of the mechanisms involved in ROS production and antioxidant mechanisms that counterbalance this oxidative stress. eNOS uncoupling due to decreased arginine, increased ADMA, enhanced arginase activity, low BH4, and disruption of the zinc tetrathiolate (ZnS4) cluster results in increased production of superoxide. Upregulation of NADPH oxidase subunits and xanthine oxidase further contributes to the generation of ROS. Superoxide dismutase catalyzes the conversion of superoxide to hydrogen peroxide. Hydrogen peroxide is reduced by catalase and glutathione peroxidase. XO xanthine oxidase, SOD2 superoxide dismutase 2, UCP2 uncoupling protein-2, HIF-1α hypoxia-inducible factor α, BH 4 tetrahydrobiopterin, ADMA asymmetric dimethylarginine, DDAH2 dimethylaminohydrolase-2, NADPH nicotinamide adenine dinucleotide phosphate, SOD superoxide dismutase, GPx glutathione peroxidase, GSSG glutathione disulfide
15.3.1 Mediators and Molecular Mechanisms of Oxidative Stress in PAH
15.3.1.1 Nitric Oxide Dysregulation
NO is a gaseous lipophilic free radical and primary pulmonary vasodilator produced and released by the endothelium. In addition to regulating vascular tone, NO attenuates platelet aggregation and inhibits vascular SMC proliferation and migration within the vascular wall [404]. NO is biosynthesized during the conversion of the amino acid l-arginine to l-citrulline by a family of enzymes called nitric oxide synthases (NOS). Three different isoforms of NOS have been identified including neuronal NOS (nNOS), inducible NOS (iNOS/NOS2), and endothelial NOS (eNOS). The production of NO by NOS requires NADPH and O2, as well as the cofactors tetrahydrobiopterin (BH4), flavin adenine dinucleotide (FAD), flavin mononucleotide (FMN), and Ca2+/calmodulin (CaM) [52, 220] (Fig. 15.4).

Nitric oxide signaling in PAH. Oxidative stress and nitric oxide (NO) dysregulation in the pathogenesis of PAH. (1) Biosynthesis of NO from the amino acid l-arginine by the enzyme endothelial nitric oxide synthases (eNOS) with l-citrulline as a side product and important cofactors such tetrahydrobiopterin (BH4), calcium, and heme. (2) Uncoupling of eNOS—when cofactors are limited and there is production of ROS, superoxide (O2 •‾) and hydrogen peroxide (H2O2). (3) Binding of NO to its target protein, soluble guanylate cyclase (sGC) and conversion of guanosine triphosphate (GTP) to cGMP resulting in blood vessel dilation (4). (5) Cleavage of cGMP by PDE5 into 5′GMP leading to inhibition of NO signaling resulting in vessel contraction
After release from endothelial cells, NO binds to soluble guanylate cyclase (sGC) in vascular cells and converts guanosine triphosphate (GTP) to cGMP, which leads to activation of downstream cGMP-dependent signaling [77, 270]. cGMP is a transient signaling molecule, as it is rapidly cleaved by phosphodiesterases (PDEs), predominantly PDE5, into 5′GMP, thereby inhibiting NO signaling (Fig. 15.4). Although eNOS-derived NO is primarily responsible for endothelium-dependent vasodilation, iNOS has also been shown to regulate pulmonary vascular tone [111, 113].
In mice, deletion of eNOS results in systemic hypertension [157] and mild PH [326], while eNOS overexpression leads to systemic hypotension [130, 265]. Exposure of eNOS-deficient mice to chronic hypoxia exacerbates PH and right ventricular hypertrophy (RVH) [327] and administration of inhaled NO attenuates hypoxia-induced PH, RVH, and vascular remodeling in rats [192, 297, 300]. In addition, recent findings demonstrate that endothelial-like progenitor cells (ELPC) expressing eNOS reverse MCT-induced PH [395] and attenuate right ventricular systolic pressure (RVSP) and pulmonary arterial muscularization in a lung lobectomy model of PH [366]. Taken together, these findings suggest a critical role for dysregulation of eNOS-derived NO in the pathogenesis of PAH.
While there is general consensus that NO signaling is impaired in PAH, it remains unclear whether this is primarily due to reduced synthesis, decreased bioavailability, decreased responsiveness, or increased consumption of NO. Some studies have demonstrated attenuated bioavailability of NO via hemoglobin and superoxide scavenging [154] or by increased hemolysis in fatal PAH [156].
15.3.1.2 eNOS Regulation
NO synthesis and bioavailability in the pulmonary vasculature are dependent upon the regulation of eNOS [60]. eNOS expression is controlled by two regulatory regions, the positive regulatory domains I and II, and its transcription is regulated by many cofactors acting by complex cis and trans interactions [309]. Additionally, methylation of nucleotides in those regions specifies vascular endothelial cell expression of eNOS [55]. Following eNOS protein translation, its compartmentalization activity is regulated by phosphorylation of specific serine and threonine residues [42, 43, 69, 194, 252], as well as additional posttranslational modifications (myristoylation and palmitoylation) which allow for eNOS localization to the plasma membrane and subsequent targeting to caveolae [263], where caveolin-1 (cav-1) regulates intracellular NO signaling [255].
In addition to the Cav-1/caveolae trafficking system [145, 255, 302], the chaperon Hsp90 has also been identified as a regulator of eNOS activity by its rapid binding upon EC activation [386]. One possible mechanism of this regulation is through interaction of eNOS and Hsp90 with CaM. Following VEGF stimulation of EC, there is disruption of the Ca2+/CaM-dependent eNOS/cav-1 complex and promotion of Hsp90 and eNOS association. The Hsp90/eNOS complex is then triggered for VEGF-activated Akt-dependent phosphorylation of eNOS [49, 336]. Prolonged exposure of cells to Ca2+ results in degradation of eNOS and Hsp90, followed by a decrease in NO production [19]. It has also been shown that Hsp90 as an adaptor protein binds eNOS to sGC, allowing cGMP signaling to take place and facilitating responses to NO donors [350, 386].
15.3.1.3 Uncoupling of eNOS in PAH
In addition to impaired NO signaling in the pathobiology of PAH, “eNOS uncoupling” in conditions of substrate/cofactor deficiency or RNS production in the setting of NO excess can lead to decreases in NO bioavailability and increases in oxidative stress with downstream alterations in vascular tone and aberrant vascular remodeling. eNOS uncoupling can occur in the setting of BH4 or l-arginine deficiency [196, 200] and results in a shift from NO synthesis to other ROS production with resultant endothelial dysfunction [72] (Fig. 15.4). All three isoforms of NOS contain an oxygenase and a reductase domain, each of which has its own catalytic activity. The oxygenase domain has binding sites for heme and BH4, while the reductase domain has binding sites for FAD, FMN, and NADPH. Both domains are linked by the binding site for CaM, an important regulator of NOS function.
For the formation of NO from l-arginine, eNOS requires the critical cofactor BH4, which stabilizes the dimeric structure of eNOS and facilitates binding of l-arginine [73]. When BH4 levels are insufficient, “eNOS uncoupling” may result with activation of the reductase domain and transfer of electrons to O2, rather than l-arginine, and production of superoxide (O2 •‾) [51] (Fig. 15.4). BH4 can be oxidized by ROS to BH2, a competitive BH4 antagonist [130], which shifts eNOS enzymatic activity towards superoxide production [183]. Deficiency of BH4 in a mouse model led to spontaneous development of PH under normoxic conditions as well as exaggerated hypoxia-induced PH, vascular remodeling, and RVH, which was secondary to reduced NOS activity and increased superoxide production associated with reduced BH4 levels [183]. Furthermore, overexpression of GTP-cyclohydrolase 1, the rate-limiting enzyme in BH4 biosynthesis, prevented PH in mice, and exogenous supplementation of BH4 attenuated MCT-induced PH and muscularization of distal pulmonary arteries in rats [120, 180]. Additionally, the BH4 analogue, acetyl-7,7-dimethyl-7,8-dihydropterin, improved NO-mediated pulmonary artery dilation and induced eNOS expression in the endothelium of rats with hypoxia-induced PH [196].
Further support for eNOS uncoupling in the pathogenesis of PAH comes from Cav-1-deficient mice that develop PH [222, 396] due to increased superoxide [179] and peroxynitrite production and tyrosine nitration-dependent impairment of protein kinase G (PKG) activity secondary to increased eNOS activity and NO levels [398]. Importantly, PH in Cav-1-knockout (KO) mice can be reversed with NOS inhibition and prevented with BH4 administration in Cav-1-deficient neonatal mice [376, 377].
Uncoupling of eNOS can also occur in the setting of limited l-arginine availability. Although intracellular concentrations of l-arginine typically far exceed what is necessary for NO production [60], arginase can metabolize l-arginine to l-ornithine and urea, and compete with NOS for substrate. Arginase is upregulated in the lungs of mice exposed to hypoxia [173], as well as in hypoxia-exposed SMC [61], and is increased in EC of PAH patients [381]. Increases in arginase lead to endothelial dysfunction [306, 381], increases in EC and SMC proliferation [205], as well as increases in collagen deposition [186]. Inhibition of arginase decreases SMC and EC proliferation [67], and attenuates pulmonary vascular remodeling in an animal PH model [67]. Increased levels of l-arginine have also been implicated in the development of PAH in patients with SCD [154]. In addition to limiting NO availability, increased arginase and enhanced synthesis of ornithine have also been implicated in SMC remodeling and PH [144, 266].
l-Arginine availability can also be influenced by endogenous methylarginines, specifically l-monomethlyl arginine (l-NMMA) and ADMA, which are produced through posttranslational methylation of amino acids in arginine [14, 372] and compete with l-arginine for the binding site on eNOS [51]. Both l-NMMA and ADMA are eliminated largely through active metabolism by dimethylarginine dimethylaminohydrolase (DDAH) [204]. Levels of ADMA are increased in animal models of PH [17, 241] and have been associated with increased oxidative stress and endothelial dysfunction [334]. Furthermore, DDAH levels are reduced in animal models of PH [17, 241] and DDAH1 overexpression in mice has been shown to decrease the sustained phase of hypoxic pulmonary vasoconstriction (HPV) via activation of the NO-sCG pathway [24]. Additionally, levels of ADMA are increased in the plasma of patients with pediatric and idiopathic PAH [132, 280] and also have been associated with increased pulmonary vascular pressures in decompensated heart failure patients in the intensive care unit [312].
15.3.1.4 NO Reactions with Other ROS: Formation of RNS
Nitrosative stress has also been implicated in the pathogenesis of PAH. NO is the main RNS produced within cells and can react with other ROS such as superoxide to generate peroxynitrite anion (ONOO‾). Peroxynitrite is a potent oxidant that nitrates tyrosine residues and can lead to formation of other extremely reactive RNS such as nitrogen dioxide, nitrosoperoxycarbonate anion, nitrite, and nitrate. These RNS can lead to significant alterations in protein structure and function, lipid peroxidation, nucleic acid damage, and cell death. Nitrotyrosine, a product of tyrosine nitration and marker of peroxynitrite, is upregulated in the endothelium and PASMC of rats subjected to chronic hypoxia [87, 167] and hypoxia-induced peroxynitrite production has been shown to increase proliferation in PASMC [3]. Peroxynitrite-mediated tyrosine nitration has also been shown to inactivate prostacyclin synthase leading to reduced levels of prostaglandin I2 [401], eNOS uncoupling, as well as inhibition of PKG [4, 397]. In addition, peroxynitrite can activate many signaling pathways involved in cell proliferation including ERK and protein kinase C [3]. Moreover, treatment of newborn rats with a ONOO‾ decomposition catalyst, 5,10,15,20-tetrakis(4-sulfonatophenyl) porphyrinato iron(III) (FeTPPS), attenuated chronic hypoxia-induced PH and decreased proliferation in neonatal PASMC [32].
In addition to tyrosine nitration, RNS can also induce S-nitrosylation and glutathionylation of regulatory proteins that may alter protein function and downstream signaling. Notably, NO can induce S-nitrosylation through formation of dinitrogen trioxide that can covalently link NO to free thiol groups on cysteine residues within proteins leading to formation of S-nitrosothiols. Several S-nitrosylation targets may play an important role in modulating oxidative stress and vascular remodeling in PAH including eNOS, sGC, hemoglobin, mitochondrial complex I, NOX, and cyclooxygenase (COX)-2 [224]. The functional effects of S-nitrosylation of several of these key proteins promote vasodilation and decrease oxidative stress, although S-nitrosylation of sGC and eNOS may inhibit NO-mediated effects on vascular tone. In red blood cells (RBC), hypoxia impairs S-nitrosylation of hemoglobin and deficiency of S-nitrosohemoglobin (SNO-Hb) is associated with exaggerated HPV and increased pulmonary arterial pressures [233]. Furthermore, restoration of SNO-Hb levels by ethyl nitrite inhalation enhanced vasorelaxation and improved hemodynamics and oxygenation in PAH patients [233]. Although S-nitrosylation-induced vascular alterations appear to be protective in PAH, the role of S-nitrosothiols in the pathogenesis of PAH remains incompletely understood.
15.3.1.5 Xanthine Oxidase
Xanthine oxidoreductase (XOR) is a critical source of intracellular ROS. It catalyzes the terminal two steps of purine degradation, from hypoxanthine to xanthine and then to uric acid, with release of O2 •‾ and H2O2 (Fig. 15.3). It primarily exists in cells as a dehydrogenase reducing NAD+ to NADH, but in the setting of inflammation, oxidation of cysteine residues or limited proteolysis converts xanthine dehydrogenase into xanthine oxidase (XO). XO transfers substrate-derived electrons to O2, generating O2 •‾ and H2O2. H2O2 is a major ROS product of XOR action under normal and pathophysiological conditions [7, 335] and has been shown to regulate many pathways involved in vascular remodeling including proliferation and Ca2+ signaling [143, 356, 389]. H2O2 has also been shown to contribute to superoxide production and decreased NO via activation of NOX [208, 400], eNOS uncoupling in an NOX-dependent manner [16, 46], and limiting access to BH4. Furthermore, H2O2 has been shown to inhibit the activity of extracellular superoxide dismutase (EC-SOD) in PASMC and treatment with catalase (which catalyzes decomposition of H2O2) enhances EC-SOD activity and decreases superoxide levels in a model of persistent pulmonary hypertension of the newborn (PPHN) [363].
XOR is upregulated in the lung and serum of rats exposed to chronic hypoxia and treatment with allopurinol, an XO inhibitor, attenuates hypoxia-induced PH, pulmonary vascular remodeling, and RVH [151, 167]. In addition, XO activity is increased in the plasma of patients with IPAH [124, 321], suggesting a role for XOR-mediated ROS in the pathogenesis of PAH.
15.3.1.6 NADPH Oxidases
ROS produced by oxidases such as NOX are considered a major contributor to oxidative and nitrosative stress in the lungs and pulmonary vasculature [7, 82], and have been shown to play an important role in dysregulation of vascular tone in the setting of hypoxia [118, 211]. The parenchymal family of NOXs includes NOX1, NOX3, NOX4, NOX5, DUOX1, and DUOX2 and the phagocyte NOX includes gp91phox (NOX2). Only NOX1, NOX2, and NOX4 are found in the human vasculature and generate ROS by electron transfer from NADPH to oxygen to generate O2 •‾ that can be further converted to H2O2 by cellular superoxide dismutases (SODs). For enzymatic function, each NOX requires several adaptor subunits. In endothelial cells, NOX2 is constitutively associated with p22phox and, after stimulation, p47phox is phosphorylated followed by recruitment of p67phox, p40phox, and Rac1 to the NOX2 complex where it is then able to generate O2 •‾ [20] (Fig. 15.3).
In the pulmonary vasculature, NOX1, NOX2, and NOX4, as well as the subunits p22phox p47phox, p67phox, and p40phox are expressed in the lung and pulmonary arteries of mice [246]; however, NOX4 is the predominant NOX upregulated by hypoxia in PASMC [245, 246], PAEC [260], and pulmonary artery adventitial fibroblasts [207]. In addition, p22phox and NOX4 have recently been shown to be upregulated in PASMC in a lamb model of pulmonary hypertension of the newborn (PPHN) [362]. Knockdown of NOX4 decreased ROS production and attenuated proliferation in PASMC and pulmonary artery adventitial fibroblasts [207, 245, 246], as well as increased apoptosis in adventitial fibroblasts [207]. In addition, knockdown of NOX4 increased EC-SOD activity as well as attenuated increases in cyclin D1 and NF-κB in PPHN-PASMC [362]. Furthermore, NOX4-derived ROS have been shown to mediate hypoxia-induced decreases in Kv channel current and increase Kv1.5 channel oxidation in PASMC [245].
NOX4 has also been shown to be upregulated by TGF-β in PASMC [328]. TGF-β significantly induced NOX4 expression and ROS in human PASMC in a Smad2/3-dependent manner that was attenuated by diphenylene iodonium, an NADPH inhibitor, knockdown of NOX4 by siRNA, and transfection of dominant negative Smad2/3 plasmids. In addition, TGF-β stimulation induced NOX4-dependent increases in proliferation in PASMC and, furthermore, led to increases in contractile protein expression that was redox- but not NOX4 dependent. Furthermore, NOX4 has been shown to be significantly upregulated in the lungs of PAH patients compared with healthy donor control lungs [246].
NOX1 and NOX2 have also been shown to play a potential role in the pathogenesis of PAH. In a chronic hypoxia-induced PH model in mice, deficiency of NOX2 reduced hypoxia-induced ROS production, pulmonary artery vasoreactivity, and attenuated hypoxia-induced increases in RVSP, pulmonary vascular remodeling, and RVH [211]. Interestingly, in a rat MCT-induced PH model, PASMC isolated from MCT-treated rats had increased expression of NOX1 and enhanced superoxide production. Knockdown of NOX1 reduced superoxide production as well as attenuated MCT-induced increases in SOD2, cyclin D1, and phosphorylation of ERK. Furthermore, knockdown of NOX1 attenuated proliferation and migration of PASMC from MCT-treated rats [348].
NOXs have also been shown to play an important role in the endothelium in response to hypoxia [122, 405]. PAEC exposed to hypoxia-reoxygenation had significant release of H2O2 compared with control cells and inhibition of NOX with diphenyliodonium attenuated H2O2 production in response to hypoxia-reoxygenation [405]. In addition, acute hypoxic vasoconstriction (HPV) was attenuated in p47phox-deficient mice and ex vivo treatment with an NOX inhibitor significantly reduced HPV in isolated perfused rabbit lungs [371]. Although human data on the role of NOX regulation in the pathobiology of PAH is limited, there is strong animal data supporting an important role for NOX-derived ROS in the pathogenesis of PAH. Further study in patients is warranted to elucidate the role of NOX in human PAH and to determine whether NOX represents an effective pathway for therapeutic targeting in PAH.
15.3.1.7 Mitochondria-Derived ROS
Mitochondria are an additional source of ROS production that may play a role in the pathogenesis of PAH [99]. PAH has been reported in patients with genetic alterations in mitochondrial genes [322, 349] and there is growing recognition that metabolic aberrations and mitochondrial dysfunction exist in PASMC and PAEC isolated from patients with PAH [40, 117, 235, 382]. ROS are generated in mitochondria during the electron transport chain when electrons flowing down the redox gradient prematurely react at complexes I and III with O2 to generate O2 •‾ [98, 103, 370]. There is also data to suggest that complex II may be a source of mROS generation in the lungs from hypoxic mice and the hearts isolated from MCT-treated rats [267, 292]. Additional ROS can be generated in mitochondria from superoxide by manganese SOD2 that catalyzes rapid conversion of O2 •‾ to diffusible H2O2 (Fig. 15.3), which can serve as a signaling molecule and regulate transcription factors such as HIF-1α [57, 137, 235] and sulfhydryl-rich voltage-gated potassium Kv channels [155], which have been shown to play a critical role in PAH.
Debate exists as to whether hypoxia increases or decreases mROS and, furthermore, whether mROS promote or protect against pulmonary vascular remodeling [98, 368]. Previous work has demonstrated that hypoxia increases mROS, Ca2+ influx, and PASMC contractility and that inhibition of the electron transport chain attenuates increases in Ca2+ and HPV [56, 106, 290, 359]. In addition, hypoxia-induced increases in mROS have also been shown to enhance PASMC proliferation via opening of mitochondrial K+ ATP channels and overproduction of H2O2 [155]. Furthermore, a recent study demonstrates that redox signaling in PASMC in response to hypoxia is dependent upon subcellular mitochondrial compartment location [358].
While supraphysiologic levels of mROS can lead to oxidative damage and cellular dysfunction, mROS are critical regulators of vascular tone and sustained decreases in mROS may lead to upregulation of transcription factors and signaling pathways that promote aberrant vascular remodeling in PAH. Emerging data suggest that mitochondrial function is impaired in PAH and that cellular metabolism is shifted towards glycolysis leading to enhanced cellular proliferation and resistance to apoptosis, similar to cancer cells (i.e., the Warburg effect) [39, 347]. This has been attributed to decreased mROS production, inhibition of Kv channels with subsequent increases in Ca2+ signaling, and activation of HIF-1α and NFAT which promote proliferation and suppress apoptosis [40, 41, 240, 369].
Reduced levels of mROS have been found in animals models of PH including the fawn-hooded rat (FHR) that spontaneously develops PAH [40] and MCT-treated rats [235]. Additionally, PASMC isolated from PAH patients have decreased Kv1.5 expression, increased intracellular Ca2+ concentrations [Ca2+]i, increased mitochondrial membrane potential, and activation of NFAT [41]. Inhibition of NFAT with VIVIT or cyclosporine restored Kv1.5 expression, decreased [Ca2+]i, and reversed mitochondrial hyperpolarization leading to decreased proliferation and increased apoptosis in PAH-PASMC [41].
In addition, treatment with dichloroacetate (DCA), a pyruvate dehydrogenase kinase (PDK) inhibitor that enhances oxidative phosphorylation, improved mortality and hemodynamics, as well as reversed vascular remodeling and RVH in MCT-treated and chronic hypoxia-exposed rats [235, 239]. DCA was found to reverse MCT-induced vascular remodeling by restoring Kv1.5 expression, depolarizing mitochondria, increasing H2O2 production, and inducing apoptosis in PASMC [235, 239]. Furthermore, mitochondrial survivin, a cytoprotective protein that promotes tumorigenesis and inhibits apoptosis in cancer cells [94], has also been shown to be upregulated in MCT-treated rats and in pulmonary arteries of PAH patients [234]. Adenoviral transfection of a dominant negative survivin mutant increased Kv channel current, depolarized mitochondria, attenuated proliferation, and increased apoptosis in PASMC. Intratracheal administration of the survivin mutant in vivo improved hemodynamics and survival and attenuated vascular remodeling in MCT-treated rats [234]. Although conflicting data exists in animal models, mitochondrial-derived ROS clearly play an important role in the pulmonary vasculature and mitochondrial dysfunction is increasingly recognized as contributing to the pathobiology of PAH. Future studies are necessary to evaluate whether mitochondrial-based therapies have efficacy in animal models of PH and patients with PAH.
15.3.1.8 Lipid Peroxidation and Isoprostanes
Lipid peroxidation has recently been recognized as an additional source of ROS during pulmonary vascular dysfunction [251]. Isoprostanes, chemically stable isomers of prostanoids, are formed when ROS products (particularly peroxynitrite) react with unsaturated bonds of membrane lipids such as arachidonic acid [168]. As isomers of prostaglandins (PG), they can act on several cell types within the pulmonary vasculature via specific prostanoid receptors, including the thromboxane A2 receptor (TP), and PGE2 and PGF2α receptors (EP and FP) [109, 169]. In PASMC and EC, isoprostanes can be released in response to stimulation with growth factors (PDGF, TGF-β), pro-inflammatory cytokines (TNF-α, interferon-γ, IL-1β), as well as by ROS (H2O2 and O2 •‾) [168]. This can lead to activation of signaling pathways downstream of prostanoid receptors including RhoA/ROCK, phospholipase C (PLC), and cyclic AMP/protein kinase A [168], resulting in vasoconstriction and release of other vasoconstrictors, including endothelin-1 (ET-1) from endothelial cells and PASMC [167, 388].
Isoprostane levels have been shown to be elevated in the lung in animal models of hypoxia- and hyperoxia-induced PH [166, 178]. In addition, inhibition of the TP receptor has been shown to reduce ET-1 production in PASMC, as well as attenuate RVH and lung smooth muscle-α actin expression in a hyperoxia neonatal rat model [166]. Urinary levels of isoprostaglandin F2α type-III (iPF2α-III), a stable lipid peroxidation product indicative of oxidative stress [298], are significantly elevated in patients with PAH compared with controls [75, 296], as well as in patients with BMPR2 mutations regardless of disease status [201]. Furthermore, while urinary levels of iPF2α-III inversely correlate with vasoreactivity to inhaled NO [75], increased urinary iPF2α-III levels directly correlate with hemodynamic and clinical response to epoprostenol [296], and recently have been found to be independently associated with mortality in PAH patients [76]. Although future studies in animal models and patients will be necessary to further elucidate the role of isoprostanes in PAH, emerging data suggest that isoprostanes may play a role in the pathogenesis of PAH and may serve as a possible lipid peroxidation biomarker in PAH patients.
15.3.2 Oxidative Stress and Animal Models of PH
15.3.2.1 Hypoxia-Induced PH Model
Oxidative stress has been implicated in the pathogenesis of PAH in several animal models of PH (Table 15.4). In the chronic hypoxia model of PH, hypoxia has been shown to induce ROS/RNS production with observed increases in lung superoxide [260], phosphatidylcholine hydroperoxide (PCOOH) [151], isoprostanes [178], nitrotyrosine [87, 167], and oxidized glutathione (GSSG) [261]. Hypoxia has also been shown to increase expression of ROS generators including eNOS [112], NOX2 [211], NOX4 [245, 246], XO [151, 167], and, in some studies, mROS [56, 357, 359]. In addition, hypoxia decreases expression of the antioxidant EC-SOD (SOD3) in the lungs of mice [261] and in pulmonary arteries from calves exposed to chronic hypoxia [143]. Furthermore, several studies have demonstrated efficacy of antioxidants (e.g., N-acetyl cysteine) [198], inhibitors of ROS-producing enzymes (e.g., allopurinol) [26, 151, 167], peroxynitrite decomposition catalysts [32], and SOD mimetics [351] in hypoxia-induced PH rodent models [151, 199, 260], suggesting oxidative stress contributes significantly to the pathogenesis of hypoxia-induced PH.
In the hypoxia-induced PH model in newborn pigs, increases in oxidative stress were observed after 3 days of hypoxia with increases in isoprostanes in pulmonary resistance arteries [88]. Additionally, NOX1 and p67phox were increased and SOD1 was decreased in pulmonary arteries from pigs raised in hypoxia for 3 or 10 days. Furthermore, inhibition of NOX with apocynin or treatment with an SOD mimetic + polyethylene glycol-catalase attenuated acetylcholine vascular responses of pulmonary arteries from hypoxia-exposed pigs [88].
15.3.2.2 Monocrotaline-Induced PH Model
In the MCT model, increases in isoprostanes [177] and NOX1 [348] have been observed in rats and increased NOX4 expression was reported in mice exposed to MCT [311]. Additionally, while increases in antioxidants SOD, catalase, and glutathione peroxidase have been reported in the lungs [97, 172], decreases in SOD1 and SOD2 have been observed in RV homogenates from MCT-treated rats [292]. Adenoviral overexpression of EC-SOD in MCT-treated rats decreased lung tissue levels of 8-isoprostane and attenuated RVSP and pulmonary vascular remodeling [177]. Furthermore, several antioxidants [291, 393] and resveratrol [269] have shown benefit in the MCT-induced PH model in rats.
15.3.2.3 SU5416-Hypoxia PH Model
In the Sugen hypoxia model, rats treated with SU5416 followed by exposure to chronic hypoxia had significantly increased expression of nitrotyrosine and heme oxygenase 1 (HO-1) in the lung compared with controls [352], in contrast to the RV where levels of HO-1 were decreased following Sugen hypoxia [38]. Treatment with protandim, a nuclear factor erythroid 2-related factor 2 (Nrf2) activator which induces antioxidant expression (e.g., HO-1, SOD), prevented RV failure and fibrosis; however, it did not attenuate pulmonary vascular remodeling [37].
15.3.2.4 Pulmonary Hypertension of the Newborn Model
Increases in oxidative stress have also been demonstrated in the newborn lamb PPHN model where animals undergo prenatal ligation of the ductus arteriosus [48, 325, 362], as well as a CHD model where a surgical shunt between the aorta and pulmonary artery is created in prenatal lambs [135]. In the PPHN model, newborn lambs that had undergone ductus arteriosus ligation in utero demonstrated increased levels of superoxide, decreased SOD expression/activity, as well as increased p67phox expression in pulmonary arteries [48]. Treatment of PPHN lambs with recombinant SOD1 enhanced pulmonary vascular responses to inhaled NO with greater decreases in PVR, suggesting a critical role for NOX-mediated ROS and potential efficacy of SOD in PPHN [325]. A more recent study demonstrated increased NOX4 and p22phox and decreased EC-SOD in the lungs and PASMC from PPHN lambs [362]. Similarly, in the neonatal shunt model, shunted lambs demonstrated elevated superoxide levels and increased expression of Rac and p45phox in the lung, as well as eNOS uncoupling, further supporting the role of NOX and eNOS in ROS generation in animal models of PH [135].
15.3.2.5 Fawn-Hooded Rat Model
The FHR, a strain in which PAH occurs spontaneously, has provided critical information on the role of mitochondrial dysfunction in the pathogenesis of PAH. The FHR has an autosomal recessive disorder similar to Hermansky–Pudlak syndrome characterized by dysfunction of several organs including systemic hypertension, pulmonary fibrosis, renal disease, as well as platelet and coagulation dysfunction [193]. As described above, PASMC isolated from FHR have decreased ROS, decreased SOD2 expression, as well as marked mitochondrial abnormalities, normoxic activation of HIF-1α, and inhibition of Kv1.5 channels [40]. In addition, PASMC from FHR demonstrate a shift in metabolism from oxidative phosphorylation to glycolysis despite adequate oxygen [293]. Overexpression of SOD2 in PASMC from FHR restored Kv1.5 expression and inactivated HIF-1α, and treatment of FHR with an SOD mimetic (metalloporphyrin Mn(III)tetrakis (4-benzoic acid) porphyrin) improved hemodynamics and exercise capacity, as well as decreased vascular remodeling [15].
15.3.2.6 Genetic Models of PH
Genetic models have offered the opportunity to further evaluate the role of ROS in pulmonary vascular remodeling and the development of PAH. Several genetically modified mice that develop PH have recently been associated with increases in oxidative stress. Transgenic (TG) mice with a mutation in the cytoplasmic tail of BMPR2 have increased lung levels of lipid peroxidation products, isoprostanes, and isofurans, and transfection of rat vascular SMC with BMPR2 mutants increases superoxide and peroxide production compared with wild type (WT) BMPR2-transfected cells [116, 201]. Mutations in ALK1, which encode an endothelial-specific receptor of the TGF-β superfamily and are associated with hereditary hemorrhagic telangiectasia (HHT) and PAH [141, 142], have also been associated with increased oxidative stress [170]. Mice heterozygous for ALK1, that develop PH as they age, have increased ROS in the lungs (iPF2α-III, H2O2) at 12 weeks of age secondary to increased eNOS uncoupling, and treatment with tempol, an SOD mimetic, prevents increases in RVSP and RVH in ALK1+/− mice [170]. In addition, TG mice overexpressing ET-1 in the endothelium, that develop hypertrophic vascular remodeling and have impaired vascular relaxation, have enhanced vascular NOX activity and increased expression of gp91phox [13], suggesting these TG mice have increased oxidative stress.
Genetic models of SOD have provided additional insight into oxidative stress and ROS scavenging in animal models of PH. Mice lacking mitochondrial manganese SOD (MnSOD, SOD2) have severe mitochondrial injury with central nervous system and cardiac injury leading to significant postnatal mortality [202]. Mice deficient in intracellular copper-zinc SOD (CuZnSOD, SOD1) or extracellular SOD (EC-SOD, SOD3) have increased oxidative stress as measured by urinary isoprostanes and plasma thiobarbituric acid-reactive (TBARS) levels, and mice deficient for both SOD1 and SOD3 have additional increases in oxidant stress markers [310]. The absence of SOD1 has recently been reported to be associated with the development of spontaneous PH and is dependent on NFAT activation in PASMC [286]. SOD1-deficient mice have elevated superoxide levels and develop significant increases in RVSP under normoxic conditions. Spontaneous PH in SOD1-deficient mice is attenuated by selective inhibition of NFAT as well as tempol, an SOD mimetic, which prevents NFAT activation in SOD1-knockout mice [286]. Although SOD3-knockout mice do not develop spontaneous PH, the absence of SOD3 exacerbates hypoxia-induced PH with significant increases in RV pressures, RVH, and vascular remodeling compared with WT mice [380]. Similarly, a loss-of-function SOD3 mutation in rats leads to increased TBARS and nitrotyrosine in the lung, as well as exaggerated PH and RVH following MCT, which is attenuated by the SOD mimetic Mn(III)TmPyP [380].
Transgenic overexpression of SOD1 [330] and SOD3 [6, 177, 261] protects against oxidative stress and overexpression of SOD3 has been shown to both attenuate [261] and reverse established PH in response to chronic hypoxia [6], as well as attenuate MCT-induced PH [177], and PH secondary to bleomycin-induced fibrosis [346]. Interestingly, in both the chronic hypoxia-induced PH model and in the bleomycin model of secondary PH, overexpression of EC-SOD in the lung attenuated upregulation of the transcription factor early growth factor-1 (Egr-1) [261, 346]. EC-SOD also decreased TGF-β induction in the bleomycin model [346] and prevented eNOS downregulation in the rat MCT model [177]. Additionally, PAs from EC-SOD knockout mice have enhanced vasoconstriction in response to 5-hydroxytryptamine (5-HT), while PAs from transgenic mice overexpressing EC-SOD have decreased superoxide production and attenuated 5-HT-induced vasoconstriction [210].
The caveolin-1-knockout mouse also provides additional evidence that oxidative and nitrosative stress play a role in the pathobiology of PAH. Mice deficient in cav-1 develop PH spontaneously with significant increases in PA pressures and RVH compared with WT control mice [396], and restoration of endothelial cell-specific cav-1 in knockout animals rescues the PH phenotype [254]. The absence of cav-1 leads to increased activation of eNOS [376], NO-dependent peroxynitrite production, and tyrosine nitration of PKG, which can be reversed by PKG overexpression [397]. Furthermore, inhibition of eNOS with l-NAME [376, 398] or BH4 treatment [377] prevents PH in cav-1-knockout mice. Additionally, mice deficient in both cav-1 and eNOS are protected from the development of PH [398].
15.3.3 Oxidative Stress and Human PAH
Several studies have demonstrated increases in oxidative stress in patients with PAH. As described above, elevated levels of urinary iPF2α-III have been demonstrated in PAH patients [75, 296] and recently have been shown to be independently associated with survival in PAH [76]. Additional studies have demonstrated increased levels of plasma malondialdehyde (MDA) [124, 162] and xanthine oxidase [124, 321], as well as decreased EC-SOD [124] and glutathione peroxidase activity [162] in the plasma of PAH patients. Increases in oxidative stress markers have also been demonstrated in plasma from patients with chronic obstructive pulmonary disease (COPD) and secondary PH [175], and in children with congenital portosystemic venous shunts at risk of developing PH [257]. Furthermore, oxidative posttranslational modification of albumin has been shown in patients with both idiopathic PAH and PAH secondary to SCD [262].
Increases in oxidative stress have also been demonstrated in lung tissue from PAH patients [225]. Immunohistochemical staining demonstrated increased staining for nitrotyrosine and 8-hydroxy guanosine, a marker of oxidative DNA damage, in lung tissue from PAH patients compared with controls [47]. Levels of the eicosanoid metabolites, 5-oxo-eicosatetraenoic acid (5-oxo-ETE) and 5-hydroxyeicosatetraenoic acid (5-HETE), were also found to be elevated in lung tissue from PAH patients not on prostacyclin and secondary PH patients [47]. In addition, lung tissue homogenates from PAH patients had decreased SOD activity and levels of SOD2 compared with control lungs [47]. Furthermore, SOD and glutathione peroxidase activity were also decreased in airway epithelial cells and lysates from bronchial tissue obtained from explanted PAH lungs compared with controls [225]. Taken together, substantial evidence from animal models and human PAH samples suggest that oxidative stress plays a critical role in the pathogenesis of PAH.
15.3.4 ROS and Mechanisms of Pulmonary Vascular Remodeling
Several mechanisms have been identified by which oxidative stress can mediate the vascular alterations observed in PAH. ROS have been shown to alter the balance of vasoactive mediators, enhance calcium signaling, upregulate growth factors, and induce pro-proliferative signaling pathways, all of which can contribute to enhanced vasoconstriction and pulmonary vascular remodeling in PAH. XO-derived O2 metabolites have been shown to significantly increase thromboxane B2 levels 30-fold while only minimally increase PGI2 levels, leading to enhanced vasoconstriction in isolated perfused rabbit lungs [337]. In addition, peroxynitrite has been shown to inactivate PGI2 synthase and reduce levels of PGI2 [401]. ROS have also been shown to upregulate endothelin-converting enzyme-1 [215] and induce ET-1 expression in endothelial cells [66] and, furthermore, ET-1 has been shown to stimulate PASMC proliferation via increases in superoxide production [360]. Additionally, H2O2 has been shown to promote eNOS uncoupling leading to decreases in NO and further increases in ROS [46, 400]. Taken together, several studies suggest that oxidative stress leads to an imbalance in vascular mediators with release of potent vasoconstrictors that can overwhelm the effects of endothelial-derived vasodilators and promote enhanced vasoconstriction and vascular remodeling in PAH.
ROS have also been shown to enhance Ca2+ mobilization [209] and Ca2+ sensitization in PASMC [50, 171, 185], and therefore may play a critical role in enhanced contraction and proliferation of PASMC in PAH. H2O2 leads to release of Ca2+ from inositol 1,4,5-trisphosphate (IP3)-gated sarcoplasmic reticulum stores in PASMC [209] via activation of phospholipase C-γ1 [356] and conversion of phosphatidylinositol 4,5-bisphosphate into diacylglycerol and IP3. Calcium mobilization by H2O2 in PASMC [209] and sustained constriction of rat intrapulmonary arteries (IPA) have also been shown to be dependent on ryanodine-sensitive intracellular Ca2+ stores [276]. In addition, superoxide has been shown to activate Rho A/Rho-kinase (ROCK) leading to increased phosphorylation of myosin light chain (MLC), Ca2+ sensitization, and vasoconstriction in rat pulmonary arteries [185]. Similarly, hypoxia- and ET-1-induced ROS production enhance Ca2+ sensitization via activation of Rho A/ROCK signaling in PASMC [50, 171].
mROS production has also been implicated in pulmonary vascular remodeling as discussed above. Numerous studies have demonstrated that hypoxia increases mROS, Ca2+ influx, and PASMC contractility [56, 106, 290, 359]. However, more recent studies suggest that decreases in mROS lead to inhibition of Kv channels, membrane depolarization, activation of voltage-gated Ca2+ channels, and increases in cytosolic Ca2+ concentration ([Ca2+]) which lead to increased vasoconstriction, enhanced proliferation, and suppression of apoptosis [40, 41, 240, 369].
ROS can also increase expression of several growth factors and enhance pro-proliferative signaling pathways that play a critical role in vascular remodeling in PAH. ROS have been shown to activate latent TGF-β [27] and TGF-β can further induce ROS via induction of NOX4 leading to enhanced proliferation and contraction in PASMC [328]. ROS can also induce PASMC expression of FGF-2 [35] which is upregulated in a lamb model of increased pulmonary blood flow and PH [361]. VEGF expression is also upregulated by ROS in PASMC [31] and is dependent on TGF-β activation of NADPH and ROS generation [226]. In addition, hypoxia has been shown to upregulate VEGF expression in pulmonary artery endothelial cells [212], and both H2O2 [249] and hypoxia have been shown to increase PDGF expression in endothelial cells [191].
ROS can also activate signaling pathways and transcription factors that regulate cellular proliferation, growth, and apoptosis leading to enhanced proliferation and growth of PASMC, PAEC, and fibroblasts, as well as matrix deposition in the pulmonary arterial wall. ROS have been shown to activate the G protein Ras leading to recruitment of phosphatidylinositol 3′kinase (PI3K) and activation of downstream signaling pathways involved in cell survival and hypertrophy, including Akt/protein kinase B and ERK1/2 [89, 344]. H2O2 has also been shown to upregulate the p38 mitogen-activated protein kinase (MAPK) pathway [343] and induce Src-dependent JNK activation in vascular SMC [389], as well as Src-dependent activation of big MAPK1 (BMK1/ERK5) in fibroblasts [1]. Peroxynitrite can also stimulate proliferation of PAEC and PASMC via activation of the Ras-Raf-MEK-ERK pathway as well as via protein kinase C [3].
ROS have also been shown to modulate key transcription factors that play a role in PAH and that regulate genes involved in the cell cycle and cell growth. H2O2 and hypoxia have been shown to upregulate transcription of peroxisome proliferator-activated receptor-γ coactivator-1 protein-α (PGC-1α), a transcriptional coactivator and critical regulator of mitochondrial biogenesis [163]. In PASMC, hypoxia has been shown to induce PGC-1α expression via PI3K/Akt signaling and activate mitochondrial biogenesis via NRF-1 and TFAM [288]. Additionally, knockdown of PGC-1α inhibits hypoxia-induced cyclin expression and proliferation of PASMC [288], suggesting that ROS-induced PGC-1α may play a key role in regulating mitochondrial biogenesis and vascular remodeling in PAH. XO-derived ROS have also been shown to upregulate Egr-1 via ERK1/2 in PASMC, which has been shown to play an important role in animal models of PH [92, 203, 345]. Furthermore, ROS have been shown to induce NFAT expression [181], a critical transcription factor linked to PASMC proliferation and vascular remodeling which plays a key role in the pathogenesis of PAH [33, 84, 286]. Interestingly, NFAT has recently been linked to the development of spontaneous PH in SOD1-deficient mice suggesting a critical role for NFAT in mediating ROS-induced PAH [286].
15.4 Antioxidants in PAH
Drugs that are currently available for the management of PAH include calcium channel blockers, prostanoids, endothelin-1 receptor antagonists, and PDE5 inhibitors, which lie outside the scope of this review [247]. Even though there have been significant advances in the understanding of PAH pathogenesis and new therapeutic options available for treatment, PAH remains incurable and patients eventually progress to right heart failure and death [247]. Present therapeutic approaches have been developed based on the imbalance in endothelium-derived vasoactive mediators that exists in patients with PAH [247]. Growing evidence of the importance of oxidative stress in the pathogenesis of PAH has led to the identification of new therapeutic targets. Antioxidant strategies for the treatment of PH have been recently classified into four groups: enzymatic ROS scavengers and regulators, small chemical ROS scavengers, inhibitors of ROS generation, and Nrf2 activators [332]. Additional strategies include eNOS uncoupling agents and mitochondria-active agents.
15.4.1 Enzymatic ROS Scavengers and Regulators
Enzymatic ROS scavengers and regulators include SOD, catalase, glutathione peroxidase, glutathione reductase, glutaredoxin, thioredoxin, thioredoxin reductase, peroxiredoxin, and sulfiredoxin. These enzymatic scavengers exist naturally in human cells and act synergistically in order to protect tissues against free radical damage [62].
15.4.1.1 Superoxide Dismutase
SOD is one of the most important enzymatic antioxidants in the body and is ubiquitously expressed [5, 62]. All three isoforms (SOD1, SOD2, SOD3) act by catalyzing the rapid conversion of O2 •‾ into H2O2 (Fig. 15.3) [5]. SOD has been shown to be downregulated in animal models of PH and PAH patients [5], and administration of SOD has been shown to be beneficial in animal models of PH. Steinhorn et al. found that treatment with recombinant human SOD (rhSOD) in sheep with PPHN reduced PVR in vivo and enhanced relaxation responses of pulmonary arteries to exogenous NO ex vivo [325]. Farrow et al. also showed that rhSOD increases eNOS expression and restores its function, decreases generation of ROS, and increases BH4 in PPHN lambs [115]. The effect of SOD administration in human PAH has not been studied.
15.4.1.2 Catalase
The enzyme catalase is also key in the antioxidant machinery of cells and is of particular importance during high levels of oxidative stress, since it has a very high turnover number [5]. Catalase exerts its antioxidant action by converting hydrogen peroxide into water and oxygen (Fig. 15.3) [5]. Data regarding the role and expression of catalase during PH is variable, with increased activity reported in MCT-treated rats [172], decreased levels in lambs with PH secondary to increased postnatal pulmonary blood flow [313], and no difference reported in humans with IPAH [225]. Studies to evaluate the effect of exogenous catalase in animal PH models have revealed variable results. Goats pre-treated with intravenous catalase and subjected to endotoxin infusions displayed minimal attenuation of PH compared with controls [229]. However, endotoxin-exposed sheep pre-treated with intraperitoneal catalase had attenuated elevation of pulmonary pressures compared to untreated controls [242]. Wedgwood et al. evaluated the effect of catalase on isolated pulmonary arteries from PPHN lambs and found a normalization of the vasodilator responses to exogenous NO [364]. They also demonstrated that intratracheal administration of catalase to PPHN lambs enhanced SOD3 activity and improved oxygenation [363]. Thibeault et al. evaluated the effect of intratracheal injection of liposome-encapsulated catalase in a rat model of hyperoxia, finding reduction in vascular and parenchymal damage caused by oxygen toxicity [340]. The role of catalase in treatment for human PAH is not clear and further studies are needed to determine potential benefit [5].
15.4.2 Small Chemical ROS Scavengers
15.4.2.1 Dietary Antioxidants
15.4.2.1.1 Vitamin C
Ascorbic acid is an excellent reducing agent, capable of donating an electron to oxidizing radicals such as hydroxyl, alkoxyl, peroxyl, thiol, and tocopheroxyl [101]. This makes vitamin C a good antioxidant and a substance of interest for the treatment of many diseases. Interestingly, reversible PH secondary to vitamin C deficiency and clinical scurvy has been described [197, 237]. Furthermore, low levels of ascorbate have been observed in patients with high altitude PH [22], suggesting a potential beneficial role of vitamin C in PAH. Xiang et al. investigated the effect of vitamin C supplementation in broilers with pulmonary hypertension syndrome (PHS) induced by low temperatures [379]. Vitamin C supplementation reduced PHS incidence and attenuated the percentage of thick-walled peripheral lung vessels and associated muscularization of pulmonary arterioles [379]. Paradoxically, however, Walton et al. found that broilers with PHS secondary to low temperatures and fed with flax seed oil had higher incidence of PHS when vitamins C and E were added to the diet [354]. On the other hand, Belaiba et al. showed that vitamin C inhibits the production of ROS and HIF-1α protein, as well as the increase of VEGF mRNA in PASMC stimulated with thrombin or CoCl2 in vitro [31]. No clinical trials have explored the effects of vitamin C on PH in humans. One clinical trial found no benefit of vitamin C supplementation in the prevention of acute mountain sickness [23]. Currently, there are two ongoing clinical trials registered in the NIH that aim to determine the use of antioxidants, including vitamin C, as prophylaxis for acute mountain sickness (NCT01182792, NCT01571687).
15.4.2.1.2 Tocopherols
Vitamin E is the most important lipophilic antioxidant in the lung and plays a key role in scavenging hydroxyperoxyl radicals produced during lipid peroxidation [189, 341]. Severe oxidative stress leads to increased concentration of vitamin E in the lung [189]. Patients with IPAH appear to have decreased levels of α-tocopherol in the plasma and vitamin E levels have been shown to correlate with pulmonary function better than other antioxidants [278, 308]. These findings suggest that there is a mobilization of vitamin E from other tissues to reach adequate levels in the lung [189]. There is limited and variable evidence on the effect of vitamin E in models of PH. In a model of broilers with PHS induced by cool temperatures, high dietary vitamin E attenuated mitochondrial dysfunction [161], lowered PHS-induced mortality, and improved antioxidant capacity [44]. However, a subsequent study demonstrated no mortality benefit of vitamin E supplementation in broilers with PHS [45]. Additional studies found that α-tocopherol [182] and vitamin E failed to improve RVH in broilers with PHS, nor improved cardiopulmonary performance or NOS activity in isolated pulmonary arteries [216]. Further studies are needed to further elucidate the effects of vitamin E in PAH.
15.4.2.1.3 Carotenoids
The antioxidant activity of carotenoids is due to their multiple conjugated double bonds, which makes them susceptible to oxidative cleavage [314]. The antioxidant properties of vitamin A have been of great interest in the study of many diseases, including lung cancer [123]. The role of retinol in lung development, vasculogenesis, and angiogenesis has been well documented [304, 307]. In PH, it has been demonstrated that patients with IPAH have reduced levels of retinoic acid, and treatment of hPASMC with this vitamin suppressed 5-HT-induced cell growth in vitro [278]. In a rat hypoxia model, treatment with all-trans retinoic acid (ATRA) significantly reduced muscularization of peripheral PAs and medial wall thickness of small muscular arteries; however, it did not attenuate PH or RVH [392]. Similarly, in MCT-induced PH in rats, Swamidas et al. found that dietary retinol resulted in less vascular inflammation in the lung and RV, but did not improve RVH [333]. Conversely, Qin et al. found that ATRA treatment in rats with MCT-induced PH lowered mPAP and inhibited collagen accumulation and MMP1 mRNA overexpression in the lungs [281]. No clinical trials have evaluated the benefits of carotenoids in human PAH.
15.4.2.1.4 Flavonoids
The antioxidant properties of flavonoids have been well documented in vitro [217]. They act through different mechanisms including chelation of metal ions, stimulation of antioxidant enzymes, and inhibition of enzymes that increase oxidative stress [80]. The benefits of flavonoids have been evaluated in a wide array of pathologies, including cardiovascular diseases, type II diabetes, neurodegenerative diseases, and cancer [217]. Many investigators have been interested in the effects that flavonoids may have on oxidative stress in PH. In rat models of MCT-induced PH, administration of flavonoids, such as quercetin and genistein, has been shown to decrease mPAP, RVSP, RVH, medial wall thickness, and neomuscularization of PAs, as well as inhibit hPASMC proliferation and progression to right heart failure [127, 150, 228]. In rats exposed to hypoxia, puerarin was shown to lower levels of ET-1 and type I collagen, enhance the activity of SOD, and improve pulmonary vascular remodeling [206]. Similarly, breviscapine was shown to decrease mPAP, RVH, and vascular remodeling as well as decrease fractalkine and Rho-kinase mRNA expression in a rat hypoxia model [63, 383]. In addition, genistein was shown to inhibit the mean change in tension caused by ET-1 in IPA of rats previously exposed to chronic hypoxia [367]. Finally, genistein has been shown to significantly attenuate PH, activate eNOS, restore endothelial function, and decrease vascular remodeling in broilers with PH [384]. No clinical trials have yet explored the effects of flavonoid administration in patients with PAH.
15.4.2.1.5 Resveratrol
Resveratrol is commonly found in foods such as grapes, plums, and peanuts, and has become a substance of interest because of its potential benefits in cardiovascular disease and cancer [86]. Resveratrol exerts its antioxidant effects possibly through scavenging superoxide radicals formed in the mitochondria, inhibiting lipid peroxidation, and competing with coenzyme Q to decrease the oxidative chain complex [86]. Other antioxidant mechanisms of resveratrol include upregulation of antioxidant enzymes, decrease in NOX levels, and regulation of GTP-cyclohydrolase 1, which increases BH4 levels and reverses eNOS uncoupling [378]. In the rat MCT-induced PH model, resveratrol attenuates elevation in RVSP, RVH, and thickening of IPAs [79, 268, 269]. In addition, resveratrol normalizes alterations in BMP receptors and SMAD signaling molecules, upregulates NOX subunits, and attenuates expression of IL-6, IL-1β, TNF-α, PDGF-α, PDGF-β, MCP-1, iNOS, and ICAM-1 in vivo. Furthermore, resveratrol prevented proliferation of PASMC after PDGF stimulation, and inhibited cytokine-induced NF-κβ activation in PASMC in vitro [79]. Finally, Chun et al. also showed that resveratrol reduced mPAP and monocyte chemoattractant protein-1 expression in rats with PH induced by infusion of autologous blood clot in the PA [68].
15.4.2.2 Gases
15.4.2.2.1 Nitric Oxide
Currently, inhaled NO is indicated for the treatment of term or near-term neonates with hypoxemic respiratory failure associated with PH, and is clinically used in acute vasoreactivity testing in the cardiac catheterization laboratory in patients with PAH [2, 29]. Inhaled NO has also been shown to be beneficial in patients that undergo surgery for CHDs or heart transplant [160]. There have been non-controlled observational clinical studies that show improved PVR and PAP and minimal adverse events in patients with PAH treated with long-term inhaled NO [29, 58, 164, 274, 275, 319]. However, there are still concerns about the potential risks of long-term inhaled NO therapy in PAH patients, including rebound PH upon sudden discontinuation, and toxicity due to production of NO2 and methemoglobin [29, 160]. Further clinical trials are needed to determine the safety profile of inhaled NO in the treatment of PAH.
Most of the rationale behind the studies of inhaled NO in the treatment of PAH are based on the fact that NO is a selective pulmonary vasodilator, rather than the role it may play as antioxidant. However, recent studies have demonstrated that inhaled NO increases antioxidant defenses, decreases DNA damage, and improves lung inflammation in rabbits exposed to conventional mechanical ventilation [119, 299]. In addition, inhaled NO treatment in infants with hypoxemic respiratory failure reduced oxidative stress biomarkers, namely MDA and total glutathione [139]. The potential antioxidant mechanisms of NO are very complex, since this molecule is also involved in the production of RNS and nitrosative stress, as discussed in previous sections. Nevertheless, recent studies have shown that NO participates in scavenging of lipid peroxyl radicals, and some RNS such as ONOO‾ might even participate in cell signaling pathways that activate cellular antioxidants resulting in cytoprotective, rather than cytotoxic, effects [271].
15.4.2.2.2 Hydrogen Sulfide
The toxic effects of excessive hydrogen sulfide (H2S) inhalation have been well documented and include pulmonary edema, bronchiolitis, reactive airways disease, pulmonary interstitial fibrosis, and death [64]. Its main mechanism of toxicity is due to inhibition of cytochrome oxidase and other cellular respiratory enzymes, which is dependent on concentration and duration of exposure [64]. However, H2S is produced endogenously in the lung and studies have now shown potential benefits of H2S or H2S donors in the treatment of chronic pulmonary diseases including COPD, asthma, and PH [64]. Antioxidant mechanisms of H2S include increasing glutathione levels and activation of Nrf2 with subsequent upregulation of antioxidant response elements [277].
H2S levels have been shown to be low in rats exposed to hypoxia [282], and in patients with acute exacerbations of COPD who have elevated PAP, compared to those with normal PASP [65]. Treatment of hypoxia-exposed rats with an H2S donor, sodium hydrosulfide (NaHS), reduces mPAP and RVH [365], decreases vascular remodeling, and enhances total antioxidant capacity compared with controls [282]. Similarly, administration of NaHS to broilers exposed to hypoxia significantly reduced PH compared with untreated controls [385]. In addition, H2S has been shown to relax rat aortic arteries and inhibit vascular SMC proliferation in vitro [102, 152, 282, 394]. Additionally, H2S or injected NaHS has been shown to be protective in mouse lung injury models [121]. Investigations of H2S still remain in a preclinical phase.
15.4.2.2.3 Carbon Monoxide
Carbon monoxide (CO) is very well known for its toxic effects both in chronic cigarette smoke exposure or acute intoxication [128]. The interest in the role of CO as a therapeutic gas is relatively recent and has been based on observations that, at low doses, CO may have cytoprotective properties involving inhibition of inflammatory and proliferative signals [128]. The anti-inflammatory effects of CO have been shown in many in vivo and in vitro studies [128, 244], but its antioxidant properties are less known. In fact, some studies have found that CO inhibits cytochrome c oxidase in the mitochondria, increasing accumulation of electrons within the electron transport chain resulting in increased generation of ROS in this organelle [402]. In contrast, other studies have shown that CO inhibits NOX, limiting ROS production [323].
Low dose CO has been shown to be protective in the FHR model, as well as in the hypoxia and MCT-induced PH rat models [403]. Daily treatment with 1 h of inhaled CO at 250 ppm protected FHRs from the development of spontaneous PH and prevented both hypoxia and MCT-induced increases in RVSP, RVH, and pulmonary vascular remodeling [403]. Although effects on ROS were not assessed, CO was found to attenuate PASMC proliferation, decrease apoptosis, and induce eNOS expression in PAEC [403]. In addition, CO has been shown to attenuate PVR elevation in hypoxemic sheep [256], and decrease vascular remodeling in iliac arteries in a porcine model of balloon angioplasty [285]. CO has also been shown to have protective effects in other lung diseases including bleomycin-induced fibrosis [399], lung transplantation [187, 188], and ventilator-induced lung injury [95, 149, 244]. Furthermore, treatment of ex-smoking COPD patients with CO inhalation decreased sputum eosinophils and improved responses to methacholine testing [30]. Further studies are needed to determine the efficacy of CO in patients with PAH, as well as to elucidate the role of CO in modulating oxidative stress in PAH.
15.4.2.3 Antioxidant Enzyme Mimetics
Substances that mimic the functions of antioxidant enzymes can also be used to counteract oxidative stress in the pulmonary vasculature. The antioxidant enzyme mimetics investigated have the same mechanism of action previously described for the enzymes that they emulate.
15.4.2.3.1 MnTE-2-PyP
MnSOD mimetics have high selectivity for mitochondria and decrease superoxide levels in the mitochondrial matrix, increasing the levels of diffusible H2O2 [98]. The SOD mimetic MnTE-2-PyP has been shown to be protective in a mouse model of hypoxia-induced PH [351]. Treatment of mice with MnTE-2-PyP attenuated hypoxia-induced increases in RVSP, RVH, and pulmonary vascular remodeling [351]. Furthermore, MnTE-2-PyP attenuated hypoxia-induced NALP3 inflammasome activation, caspase cleavage, and IL-1β and IL-18 production [351]. Other Mn porphyrin-based SOD mimetics have demonstrated similar efficacy in the MCT model and FHR [380].
15.4.2.3.2 Tempol
Tempol is also an SOD mimetic that has been studied in various animal models of PH. In rats exposed to chronic hypoxia, tempol normalized RVSP and reduced RVH [108], while combined treatment with tempol and tadalafil significantly prevented elevation in RVSP and RV dP/dt(max) and reduced oxidative stress in rats exposed to acute hypoxia [289]. In addition, tempol has been found to inhibit LY83583-mediated constriction of rat IPAs [185], reduce hypoxia-induced SMC proliferation and remodeling in rat PAs, as well as inhibit lung ROS production [184]. Furthermore, treatment with tempol attenuated PH in a sheep model [320], and prevented spontaneous development of PH in ALK1+/− mice [170]. Tempol has not yet been evaluated in any clinical trial.
15.4.2.3.3 Ebselen
There is minimal information on the use of the glutathione peroxidase mimetic ebselen in PH; however, recent studies suggest that ebselen may have protective effects in the pulmonary vasculature. Ebselen has been shown to attenuate hypoxia and peroxynitrite-induced proliferation of PASMC in vitro [3]. In addition, ebselen has been shown to decrease the sustained phase of hypoxic vasoconstriction of IPAs in rats [71]. More studies are needed to better understand the effects of ebselen on the pulmonary vasculature and determine whether ebselen has efficacy in animal models of PH.
15.4.3 Inhibitors of ROS Generation
15.4.3.1 Inhibitors of Oxidases
Inhibitors of oxidases include inhibitors of NOX, xanthine oxidase, and monoamine oxidase. These substances function by blocking the main enzymes that produce ROS in cells.
15.4.3.1.1 NADPH Oxidase Inhibitors
NOX inhibitors are perhaps the most studied of all the oxidase inhibitors tested in PH. Apocynin, an NADPH inhibitor, attenuates hypoxia-induced PH and vascular remodeling in lectin-like oxidized low-density lipoprotein receptor (LOX-1) transgenic mice that have enhanced ROS in response to hypoxia [264]. In addition, apocynin was shown to attenuate cold-induced PH and PA remodeling in rats [78], and restored pulmonary artery endothelial function and vascular responses in diabetic rats [214]. In lambs with PPHN induced by ductus arteriosus ligation, it has also been shown that apocynin significantly improves oxygenation, enhances PA relaxation and eNOS expression, and improves angiogenic activity of PAEC [339, 363]. Furthermore, in rat PASMC, apocynin reverses hypoxia-induced decreases in Kv current density [245], and suppresses U46619-induced inhibition of Kv currents [70].
15.4.3.1.2 Xanthine Oxidase Inhibitors
Allopurinol has been the mainstay of treatment for gout for many years and has recently become of great interest in the study of ischemic heart disease, chronic heart failure, and inflammatory diseases. In mice and rats exposed to hypoxia, allopurinol has been shown to decrease superoxide production, reduce PH, attenuate vascular remodeling, and alleviate the increased RVSP and RVH [26, 151, 167]. In addition, Shen et al. found that isolated rat lungs exposed to hypoxic challenges had attenuated HPV when treated with allopurinol ex vivo [315].
15.4.3.2 Iron Chelators
Iron normally exists in cells in the form of ferric ions (Fe3+), which can react with superoxide releasing highly reactive hydroxyl radicals. These radicals can cause lipid peroxidation, DNA oxidation, and protein oxidation [374]. Based on this rationale, it has been suggested that iron chelation may have a potential benefit on oxidative stress in the lung, but most investigations have failed to support this hypothesis. Treatment of rats exposed to chronic hypoxia with desferroxamine prevented PH and vascular remodeling in vivo, and inhibited human PASMC growth in vitro [374]. However, human studies have demonstrated that healthy volunteers exposed to desferroxamine develop increased PVR [25], and hypoxia-induced pulmonary vasoconstriction is enhanced by desferroxamine in healthy volunteers [318]. In addition, recent studies have found decreased iron levels in patients with IPAH and iron supplementation is now being evaluated as a potential treatment in this group of patients [153, 294]. Further studies are needed to better understand the role of iron in PAH pathogenesis.
15.4.4 Nrf2 Activators
Nrf2 promotes gene expression of antioxidant response element (ARE)-regulated antioxidant enzymes in response to oxidative stress [165]. Nrf2 is held in the cytoplasm by an inhibitor, and activation of the PKC signaling by oxidative stress leads to activation and translocation of Nrf2 to the nucleus with subsequent activation of ARE-regulated genes [165]. Nrf activators act by eliciting this response and increasing the level of ARE-regulated antioxidant enzymes in cells. Protandim, an Nrf2 activator prevented the development of right ventricular failure and fibrosis in the Sugen hypoxia rat model of PH, although it did not prevent the angio-obliterative vascular remodeling [352]. In addition, Nrf2-knockout mice develop exaggerated RVH in response to hypoxia, and the Nrf2 activator olipraz attenuates RVH and vascular remodeling in wild type, but not Nrf2-deficient, mice exposed to hypoxia [107]. Future studies on the potential benefits of Nrf2 activators in the treatment of PAH are necessary.
15.4.5 Tetrahydrobiopterin
The role of tetrahydrobiopterin (BH4) in oxidative stress and eNOS uncoupling has been reviewed in previous sections. Deficiency of this cofactor has been associated with development of PH and IPF in animal models [10, 183, 338]. Sapropterin dihydrochloride (pharmaceutical preparation of BH4) has been used in the treatment of hyperphenylalanemia [295]. Interest in the possible benefits of BH4 supplementation for the treatment of PH is now increasing. Administration of BH4 to MCT-treated rats attenuated PH and vascular remodeling [120, 180], as well as decreased HPV and increased NO synthesis in isolated lung preparations [120, 190]. In addition, while BH4 did not improve endothelial dysfunction of IPAs in a porcine model of PPHN [258], treatment of PAEC from PPHN lambs decreased apoptosis, improved angiogenesis, increased NO and eNOS dimer formation, and decreased superoxide production [338]. Furthermore, treatment with sapropterin dihydrochloride, in addition to sildenafil and/or endothelin receptor antagonists, in 18 patients with PAH or inoperable CTEPH was well tolerated and improved 6-min walk distance, although did not significantly alter NO synthesis or oxidative stress [295]. As BH4 supplements have been proven to be safe in humans, they represent an interesting therapeutic alternative for the treatment of PAH, but further studies are needed to determine their true efficacy.
15.4.6 Mitochondria-Activating Drugs and Mitochondria-Targeting Antioxidants
The hyperproliferative and antiapoptotic phenotype of PASMC observed in PAH is associated with mitochondrial suppression, altered glucose metabolism, and decreased mROS production [98]. These mechanisms are described in detail in previous sections.
15.4.6.1 Mitochondria-Targeting Antioxidants
There has been recent interest in therapeutic strategies that specifically target mitochondria in order to restore their normal function. The fact that this organelle is negatively charged has led to the development of strategies that increase mitochondrial selectivity such as the use of a positively charged ion, namely triphenylphosphonium (TPP+), to deliver vitamin antioxidants [98]. One of the agents that uses this cation as vehicle and has been studied in vascular diseases is MitoQ, a ubiquinone analogue of the mitochondrial electron transport chain [98]. Treatment of spontaneously hypertensive rats with MitoQ protected against the development of hypertension, improved endothelial function, and decreased cardiac hypertrophy [134]. In addition, the mitochondrial-targeted SOD mimetic mitoTEMPO decreased mitochondrial superoxide production, reduced cellular NOX activity, restored NO expression, improved endothelial-dependent relaxation, and attenuated hypertension in mice exposed to angiotensin II infusion [93].
15.4.6.2 Mitochondrial-Activating Therapies
DCA and trimetazidine (TMZ) stimulate mitochondria and regulate metabolic substrate entry into the TCA cycle [98]. DCA also inhibits PDK, which ultimately results in the inhibition of normoxic HIF-1α production and increases in pro-apoptotic factors, reducing abnormal cell proliferation [98]. Several studies in animal PH models have demonstrated that DCA stimulates glucose oxidation, reduces mPAP, and decreases medial wall thickening of PAs [40, 98, 136, 235, 239, 331]. An early-phase clinical trial of DCA in PAH is currently being completed [98] (NCT01083524). TMZ has also been shown to increase glucose oxidation, suppress fatty acid oxidation, restore perfusion to distal PAs, and reverse established PH in animal models [98, 331]. Finally, phenylbutyrate (PBA), a chemical chaperone which prevents disruption of the ER-mitochondrial unit, has recently been shown to attenuate PH, vascular remodeling, and RVH in both hypoxia-induced PH in mice and in MCT-induced PH in rats [98].
15.5 Conclusions
This review highlights the important role that oxidative stress and aberrant NO signaling play in the pathogenesis of PAH and emphasizes the mechanisms of ROS-induced pulmonary vascular remodeling in PAH. Although significant progress has been made in understanding the pathogenesis of PAH, currently available therapies that target the imbalance of vasoactive mediators do not improve mortality in PAH patients. Emerging studies implicate oxidative stress as a key mechanism in the pathobiology of PAH and therapies targeting ROS generation have shown efficacy in animal models of PH. Growing evidence of the importance of oxidative stress in the pathogenesis of PAH has led to the identification of potential new therapeutic targets in PAH. New approaches to target oxidative stress include ROS scavengers, inhibitors of ROS generation, Nrf2 activators, mitochondria-activating drugs, and eNOS recoupling agents. Developing novel therapeutics to target oxidative stress in PAH is an active and exciting area of research. Although human data is currently limited, antioxidant therapeutics may hold promise in the future for treatment of PAH.
References
Abe J, Takahashi M, Ishida M, Lee JD, Berk BC (1997) c-Src is required for oxidative stress-mediated activation of big mitogen-activated protein kinase 1. J Biol Chem 272(33):20389–20394
Abman SH (2013) Inhaled nitric oxide for the treatment of pulmonary arterial hypertension. Handb Exp Pharmacol 218:257–276
Agbani EO, Coats P, Wadsworth RM (2011) Acute hypoxia stimulates intracellular peroxynitrite formation associated with pulmonary artery smooth muscle cell proliferation. J Cardiovasc Pharmacol 57(5):584–588
Aggarwal S, Gross CM, Kumar S, Datar S, Oishi P, Kalkan G, Schreiber C, Fratz S, Fineman JR, Black SM (2011) Attenuated vasodilatation in lambs with endogenous and exogenous activation of cGMP signaling: role of protein kinase G nitration. J Cell Physiol 226(12):3104–3113
Aggarwal S, Gross CM, Sharma S, Fineman JR, Black SM (2013) Reactive oxygen species in pulmonary vascular remodeling. Compr Physiol 3(3):1011–1034
Ahmed MN, Zhang Y, Codipilly C, Zaghloul N, Patel D, Wolin M, Miller EJ (2012) Extracellular superoxide dismutase overexpression can reverse the course of hypoxia-induced pulmonary hypertension. Mol Med 18:38–46
Al Ghouleh I, Khoo NK, Knaus UG, Griendling KK, Touyz RM, Thannickal VJ, Barchowsky A, Nauseef WM, Kelley EE, Bauer PM, Darley-Usmar V, Shiva S, Cifuentes-Pagano E, Freeman BA, Gladwin MT, Pagano PJ (2011) Oxidases and peroxidases in cardiovascular and lung disease: new concepts in reactive oxygen species signaling. Free Radic Biol Med 51(7):1271–1288
Alastalo TP, Li M, Perez Vde J, Pham D, Sawada H, Wang JK, Koskenvuo M, Wang L, Freeman BA, Chang HY, Rabinovitch M (2011) Disruption of PPARγ/β-catenin-mediated regulation of apelin impairs BMP-induced mouse and human pulmonary arterial EC survival. J Clin Invest 121(9):3735–3746
Aldred MA, Vijayakrishnan J, James V, Soubrier F, Gomez-Sanchez MA, Martensson G, Galie N, Manes A, Corris P, Simonneau G, Humbert M, Morrell NW, Trembath RC (2006) BMPR2 gene rearrangements account for a significant proportion of mutations in familial and idiopathic pulmonary arterial hypertension. Hum Mutat 27(2):212–213
Almudever P, Milara J, De Diego A, Serrano-Mollar A, Xaubet A, Perez-Vizcaino F, Cogolludo A, Cortijo J (2013) Role of tetrahydrobiopterin in pulmonary vascular remodelling associated with pulmonary fibrosis. Thorax 68(10):938–948
Alva JA, Iruela-Arispe ML (2004) Notch signaling in vascular morphogenesis. Curr Opin Hematol 11(4):278–283
Ameshima S, Golpon H, Cool CD, Chan D, Vandivier RW, Gardai SJ, Wick M, Nemenoff RA, Geraci MW, Voelkel NF (2003) Peroxisome proliferator-activated receptor gamma (PPARγ) expression is decreased in pulmonary hypertension and affects endothelial cell growth. Circ Res 92(10):1162–1169
Amiri F, Virdis A, Neves MF, Iglarz M, Seidah NG, Touyz RM, Reudelhuber TL, Schiffrin EL (2004) Endothelium-restricted overexpression of human endothelin-1 causes vascular remodeling and endothelial dysfunction. Circulation 110(15):2233–2240
Anthony S, Leiper J, Vallance P (2005) Endogenous production of nitric oxide synthase inhibitors. Vasc Med 10(suppl 1):S3–S9
Archer SL, Marsboom G, Kim GH, Zhang HJ, Toth PT, Svensson EC, Dyck JR, Gomberg-Maitland M, Thebaud B, Husain AN, Cipriani N, Rehman J (2010) Epigenetic attenuation of mitochondrial superoxide dismutase 2 in pulmonary arterial hypertension: a basis for excessive cell proliferation and a new therapeutic target. Circulation 121(24):2661–2671
Ardanaz N, Pagano PJ (2006) Hydrogen peroxide as a paracrine vascular mediator: regulation and signaling leading to dysfunction. Exp Biol Med 231(3):237–251
Arrigoni FI, Vallance P, Haworth SG, Leiper JM (2003) Metabolism of asymmetric dimethylarginines is regulated in the lung developmentally and with pulmonary hypertension induced by hypobaric hypoxia. Circulation 107(8):1195–1201
Austin ED, Ma L, LeDuc C, Berman Rosenzweig E, Borczuk A, Phillips JA, Palomero T, Sumazin P, Kim HR, Talati MH, West J, Loyd JE, Chung WK (2012) Whole exome sequencing to identify a novel gene (caveolin-1) associated with human pulmonary arterial hypertension. Circ Cardiovasc Genet 5(3):336–343
Averna M, Stifanese R, De Tullio R, Passalacqua M, Salamino F, Pontremoli S, Melloni E (2008) Functional role of HSP90 complexes with endothelial nitric-oxide synthase (eNOS) and calpain on nitric oxide generation in endothelial cells. J Biol Chem 283(43):29069–29076
Babior BM (2000) The NADPH oxidase of endothelial cells. IUBMB Life 50(4–5):267–269
Badesch DB, Champion HC, Sanchez MA, Hoeper MM, Loyd JE, Manes A, McGoon M, Naeije R, Olschewski H, Oudiz RJ, Torbicki A (2009) Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol 54(1 suppl):S55–S66
Bailey DM, Dehnert C, Luks AM, Menold E, Castell C, Schendler G, Faoro V, Gutowski M, Evans KA, Taudorf S, James PE, McEneny J, Young IS, Swenson ER, Mairbaurl H, Bartsch P, Berger MM (2010) High-altitude pulmonary hypertension is associated with a free radical-mediated reduction in pulmonary nitric oxide bioavailability. J Physiol 588(pt 23):4837–4847
Baillie JK, Thompson AA, Irving JB, Bates MG, Sutherland AI, Macnee W, Maxwell SR, Webb DJ (2009) Oral antioxidant supplementation does not prevent acute mountain sickness: double blind, randomized placebo-controlled trial. QJM 102(5):341–348
Bakr A, Pak O, Taye A, Hamada F, Hemeida R, Janssen W, Gierhardt M, Ghofrani HA, Seeger W, Grimminger F, Schermuly RT, Witzenrath M, Brandes RP, Huang N, Cooke JP, Weissmann N, Sommer N (2013) Effects of dimethylarginine dimethylaminohydrolase-1 overexpression on the response of the pulmonary vasculature to hypoxia. Am J Respir Cell Mol Biol 49(3):491–500
Balanos GM, Dorrington KL, Robbins PA (2002) Desferrioxamine elevates pulmonary vascular resistance in humans: potential for involvement of HIF-1. J Appl Physiol 92(6):2501–2507
Baliga RS, Milsom AB, Ghosh SM, Trinder SL, Macallister RJ, Ahluwalia A, Hobbs AJ (2012) Dietary nitrate ameliorates pulmonary hypertension: cytoprotective role for endothelial nitric oxide synthase and xanthine oxidoreductase. Circulation 125(23):2922–2932
Barcellos-Hoff MH, Dix TA (1996) Redox-mediated activation of latent transforming growth factor-β1. Mol Endocrinol 10(9):1077–1083
Barnett CF, Hsue PY (2013) Human immunodeficiency virus-associated pulmonary arterial hypertension. Clin Chest Med 34(2):283–292
Barst RJ, Channick R, Ivy D, Goldstein B (2012) Clinical perspectives with long-term pulsed inhaled nitric oxide for the treatment of pulmonary arterial hypertension. Pulm Circ 2(2):139–147
Bathoorn E, Slebos DJ, Postma DS, Koeter GH, van Oosterhout AJ, van der Toorn M, Boezen HM, Kerstjens HA (2007) Anti-inflammatory effects of inhaled carbon monoxide in patients with COPD: a pilot study. Eur Respir J 30(6):1131–1137
BelAiba RS, Djordjevic T, Bonello S, Flugel D, Hess J, Kietzmann T, Gorlach A (2004) Redox-sensitive regulation of the HIF pathway under non-hypoxic conditions in pulmonary artery smooth muscle cells. Biol Chem 385(3–4):249–257
Belik J, Stevens D, Pan J, McIntyre BA, Kantores C, Ivanovska J, Xu EZ, Ibrahim C, Panama BK, Backx PH, McNamara PJ, Jankov RP (2010) Pulmonary vascular and cardiac effects of peroxynitrite decomposition in newborn rats. Free Radic Biol Med 49(8):1306–1314
Bierer R, Nitta CH, Friedman J, Codianni S, de Frutos S, Dominguez-Bautista JA, Howard TA, Resta TC, Bosc LV (2011) NFATc3 is required for chronic hypoxia-induced pulmonary hypertension in adult and neonatal mice. Am J Physiol Lung Cell Mol Physiol 301(6):L872–L880
Birben E, Sahiner UM, Sackesen C, Erzurum S, Kalayci O (2012) Oxidative stress and antioxidant defense. World Allergy Organ J 5(1):9–19
Black SM, DeVol JM, Wedgwood S (2008) Regulation of fibroblast growth factor-2 expression in pulmonary arterial smooth muscle cells involves increased reactive oxygen species generation. Am J Physiol Cell Physiol 294(1):C345–C354
Bockmeyer CL, Maegel L, Janciauskiene S, Rische J, Lehmann U, Maus UA, Nickel N, Haverich A, Hoeper MM, Golpon HA, Kreipe H, Laenger F, Jonigk D (2012) Plexiform vasculopathy of severe pulmonary arterial hypertension and microRNA expression. J Heart Lung Transplant 31(7):764–772
Bogaard HJ, Natarajan R, Henderson SC, Long CS, Kraskauskas D, Smithson L, Ockaili R, McCord JM, Voelkel NF (2009) Chronic pulmonary artery pressure elevation is insufficient to explain right heart failure. Circulation 120(20):1951–1960
Bogaard HJ, Natarajan R, Mizuno S, Abbate A, Chang PJ, Chau VQ, Hoke NN, Kraskauskas D, Kasper M, Salloum FN, Voelkel NF (2010) Adrenergic receptor blockade reverses right heart remodeling and dysfunction in pulmonary hypertensive rats. Am J Respir Crit Care Med 182(5):652–660
Bonnet S, Archer SL, Allalunis-Turner J, Haromy A, Beaulieu C, Thompson R, Lee CT, Lopaschuk GD, Puttagunta L, Bonnet S, Harry G, Hashimoto K, Porter CJ, Andrade MA, Thebaud B, Michelakis ED (2007) A mitochondria-K+ channel axis is suppressed in cancer and its normalization promotes apoptosis and inhibits cancer growth. Cancer Cell 11(1):37–51
Bonnet S, Michelakis ED, Porter CJ, Andrade-Navarro MA, Thebaud B, Bonnet S, Haromy A, Harry G, Moudgil R, McMurtry MS, Weir EK, Archer SL (2006) An abnormal mitochondrial-hypoxia inducible factor-1α-Kv channel pathway disrupts oxygen sensing and triggers pulmonary arterial hypertension in fawn hooded rats: similarities to human pulmonary arterial hypertension. Circulation 113(22):2630–2641
Bonnet S, Rochefort G, Sutendra G, Archer SL, Haromy A, Webster L, Hashimoto K, Bonnet SN, Michelakis ED (2007) The nuclear factor of activated T cells in pulmonary arterial hypertension can be therapeutically targeted. Proc Natl Acad Sci U S A 104(27):11418–11423
Boo YC, Kim HJ, Song H, Fulton D, Sessa W, Jo H (2006) Coordinated regulation of endothelial nitric oxide synthase activity by phosphorylation and subcellular localization. Free Radic Biol Med 41(1):144–153
Boo YC, Sorescu GP, Bauer PM, Fulton D, Kemp BE, Harrison DG, Sessa WC, Jo H (2003) Endothelial NO synthase phosphorylated at SER635 produces NO without requiring intracellular calcium increase. Free Radic Biol Med 35(7):729–741
Bottje W, Enkvetchakul B, Moore R, McNew R (1995) Effect of α-tocopherol on antioxidants, lipid peroxidation, and the incidence of pulmonary hypertension syndrome (ascites) in broilers. Poult Sci 74(8):1356–1369
Bottje WG, Erf GF, Bersi TK, Wang S, Barnes D, Beers KW (1997) Effect of dietary dl-α-tocopherol on tissue α- and γ-tocopherol and pulmonary hypertension syndrome (ascites) in broilers. Poult Sci 76(11):1506–1512
Boulden BM, Widder JD, Allen JC, Smith DA, Al-Baldawi RN, Harrison DG, Dikalov SI, Jo H, Dudley SC Jr (2006) Early determinants of H2O2-induced endothelial dysfunction. Free Radic Biol Med 41(5):810–817
Bowers R, Cool C, Murphy RC, Tuder RM, Hopken MW, Flores SC, Voelkel NF (2004) Oxidative stress in severe pulmonary hypertension. Am J Respir Crit Care Med 169(6):764–769
Brennan LA, Steinhorn RH, Wedgwood S, Mata-Greenwood E, Roark EA, Russell JA, Black SM (2003) Increased superoxide generation is associated with pulmonary hypertension in fetal lambs: a role for NADPH oxidase. Circ Res 92(6):683–691
Brouet A, Sonveaux P, Dessy C, Balligand JL, Feron O (2001) Hsp90 ensures the transition from the early Ca2+-dependent to the late phosphorylation-dependent activation of the endothelial nitric-oxide synthase in vascular endothelial growth factor-exposed endothelial cells. J Biol Chem 276(35):32663–32669
Broughton BR, Jernigan NL, Norton CE, Walker BR, Resta TC (2010) Chronic hypoxia augments depolarization-induced Ca2+ sensitization in pulmonary vascular smooth muscle through superoxide-dependent stimulation of RhoA. Am J Physiol Lung Cell Mol Physiol 298(2):L232–L242
Bruckdorfer R (2005) The basics about nitric oxide. Mol Aspects Med 26(1–2):3–31
Bruckdorfer R (2005) Nitric oxide in physiology and pathology. Mol Aspects Med 26(1–2):1–2
Campos AH, Wang W, Pollman MJ, Gibbons GH (2002) Determinants of Notch-3 receptor expression and signaling in vascular smooth muscle cells: implications in cell-cycle regulation. Circ Res 91(11):999–1006
Caruso P, Dempsie Y, Stevens HC, McDonald RA, Long L, Lu R, White K, Mair KM, McClure JD, Southwood M, Upton P, Xin M, van Rooij E, Olson EN, Morrell NW, MacLean MR, Baker AH (2012) A role for miR-145 in pulmonary arterial hypertension: evidence from mouse models and patient samples. Circ Res 111(3):290–300
Chan Y, Fish JE, D’Abreo C, Lin S, Robb GB, Teichert AM, Karantzoulis-Fegaras F, Keightley A, Steer BM, Marsden PA (2004) The cell-specific expression of endothelial nitric-oxide synthase: a role for DNA methylation. J Biol Chem 279(33):35087–35100
Chandel NS, Maltepe E, Goldwasser E, Mathieu CE, Simon MC, Schumacker PT (1998) Mitochondrial reactive oxygen species trigger hypoxia-induced transcription. Proc Natl Acad Sci U S A 95(20):11715–11720
Chandel NS, McClintock DS, Feliciano CE, Wood TM, Melendez JA, Rodriguez AM, Schumacker PT (2000) Reactive oxygen species generated at mitochondrial complex III stabilize hypoxia-inducible factor-1α during hypoxia: a mechanism of O2 sensing. J Biol Chem 275(33):25130–25138
Channick RN, Hoch RC, Newhart JW, Johnson FW, Smith CM (1994) Improvement in pulmonary hypertension and hypoxemia during nitric oxide inhalation in a patient with end-stage pulmonary fibrosis. Am J Respir Crit Care Med 149(3 pt 1):811–814
Chaouat A, Coulet F, Favre C, Simonneau G, Weitzenblum E, Soubrier F, Humbert M (2004) Endoglin germline mutation in a patient with hereditary haemorrhagic telangiectasia and dexfenfluramine associated pulmonary arterial hypertension. Thorax 59(5):446–448
Chatterjee A, Black SM, Catravas JD (2008) Endothelial nitric oxide (NO) and its pathophysiologic regulation. Vascul Pharmacol 49(4–6):134–140
Chen B, Calvert AE, Cui H, Nelin LD (2009) Hypoxia promotes human pulmonary artery smooth muscle cell proliferation through induction of arginase. Am J Physiol Lung Cell Mol Physiol 297(6):L1151–L1159
Chen KH, Lai YL, Chen MJ (2012) Oxygen radicals and substance P in perinatal hypoxia-exaggerated, monocrotaline-induced pulmonary hypertension. Chin J Physiol 55(2):82–90
Chen XJ, Cheng DY, Yang L, Xia XQ, Guan J (2006) Effect of breviscapine on fractalkine expression in chronic hypoxic rats. Chin Med J (Engl) 119(17):1465–1468
Chen Y, Wang R (2012) The message in the air: hydrogen sulfide metabolism in chronic respiratory diseases. Respir Physiol Neurobiol 184(2):130–138
Chen YH, Yao WZ, Geng B, Ding YL, Lu M, Zhao MW, Tang CS (2005) Endogenous hydrogen sulfide in patients with COPD. Chest 128(5):3205–3211
Cheng TH, Shih NL, Chen SY, Loh SH, Cheng PY, Tsai CS, Liu SH, Wang DL, Chen JJ (2001) Reactive oxygen species mediate cyclic strain-induced endothelin-1 gene expression via Ras/Raf/extracellular signal-regulated kinase pathway in endothelial cells. J Mol Cell Cardiol 33(10):1805–1814
Cho WK, Lee CM, Kang MJ, Huang Y, Giordano FJ, Lee PJ, Trow TK, Homer RJ, Sessa WC, Elias JA, Lee CG (2013) IL-13 receptor α2-arginase 2 pathway mediates IL-13-induced pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 304(2):L112–L124
Chun C, Yang W, Xueding C, Qi Z, Xiaoying H, Honglei X, Fangyou Y, Chan C, Yuanyuan L, Weixi Z, Dan Y, Zhoucang Z, Lehe Y, Cheng D, Liangxing W (2012) Resveratrol downregulates acute pulmonary thromboembolism-induced pulmonary artery hypertension via p38 mitogen-activated protein kinase and monocyte chemoattractant protein-1 signaling in rats. Life Sci 90(19–20):721–727
Church JE, Fulton D (2006) Differences in eNOS activity because of subcellular localization are dictated by phosphorylation state rather than the local calcium environment. J Biol Chem 281(3):1477–1488
Cogolludo A, Frazziano G, Cobeno L, Moreno L, Lodi F, Villamor E, Tamargo J, Perez-Vizcaino F (2006) Role of reactive oxygen species in Kv channel inhibition and vasoconstriction induced by TP receptor activation in rat pulmonary arteries. Ann N Y Acad Sci 1091:41–51
Connolly MJ, Prieto-Lloret J, Becker S, Ward JP, Aaronson PI (2013) Hypoxic pulmonary vasoconstriction in the absence of pretone: essential role for intracellular Ca2+ release. J Physiol 591(pt 18):4473–4498
Cosentino F, Barker JE, Brand MP, Heales SJ, Werner ER, Tippins JR, West N, Channon KM, Volpe M, Luscher TF (2001) Reactive oxygen species mediate endothelium-dependent relaxations in tetrahydrobiopterin-deficient mice. Arterioscler Thromb Vasc Biol 21(4):496–502. doi:10.1161/01.atv.21.4.496
Cosentino F, Luscher TF (1999) Tetrahydrobiopterin and endothelial nitric oxide synthase activity. Cardiovasc Res 43(2):274–278
Courboulin A, Paulin R, Giguere NJ, Saksouk N, Perreault T, Meloche J, Paquet ER, Biardel S, Provencher S, Cote J, Simard MJ, Bonnet S (2011) Role for miR-204 in human pulmonary arterial hypertension. J Exp Med 208(3):535–548
Cracowski JL, Cracowski C, Bessard G, Pepin JL, Bessard J, Schwebel C, Stanke-Labesque F, Pison C (2001) Increased lipid peroxidation in patients with pulmonary hypertension. Am J Respir Crit Care Med 164(6):1038–1042
Cracowski JL, Degano B, Chabot F, Labarere J, Schwedhelm E, Monneret D, Iuliano L, Schwebel C, Chaouat A, Reynaud-Gaubert M, Faure P, Maas R, Renversez JC, Cracowski C, Sitbon O, Yaici A, Simonneau G, Humbert M (2012) Independent association of urinary F2-isoprostanes with survival in pulmonary arterial hypertension. Chest 142(4):869–876
Crosswhite P, Sun Z (2010) Nitric oxide, oxidative stress and inflammation in pulmonary arterial hypertension. J Hypertens 28(2):201–212
Crosswhite P, Sun Z (2013) Inhibition of phosphodiesterase-1 attenuates cold-induced pulmonary hypertension. Hypertension 61(3):585–592
Csiszar A, Labinskyy N, Olson S, Pinto JT, Gupte S, Wu JM, Hu F, Ballabh P, Podlutsky A, Losonczy G, de Cabo R, Mathew R, Wolin MS, Ungvari Z (2009) Resveratrol prevents monocrotaline-induced pulmonary hypertension in rats. Hypertension 54(3):668–675
Czaplinska M, Czepas J, Gwozdzinski K (2012) Structure, antioxidative and anticancer properties of flavonoids. Postepy Biochem 58(3):235–244
D’Alto M, Mahadevan VS (2012) Pulmonary arterial hypertension associated with congenital heart disease. Eur Respir Rev 21(126):328–337
Damico R, Zulueta JJ, Hassoun PM (2012) Pulmonary endothelial cell NOX. Am J Respir Cell Mol Biol 47(2):129–139
Davis-Dusenbery BN, Chan MC, Reno KE, Weisman AS, Layne MD, Lagna G, Hata A (2011) Down-regulation of Kruppel-like factor-4 (KLF4) by microRNA-143/145 is critical for modulation of vascular smooth muscle cell phenotype by transforming growth factor-β and bone morphogenetic protein 4. J Biol Chem 286(32):28097–28110
de Frutos S, Spangler R, Alo D, Bosc LV (2007) NFATc3 mediates chronic hypoxia-induced pulmonary arterial remodeling with α-actin up-regulation. J Biol Chem 282(20):15081–15089
de Jesus Perez VA, Alastalo TP, Wu JC, Axelrod JD, Cooke JP, Amieva M, Rabinovitch M (2009) Bone morphogenetic protein 2 induces pulmonary angiogenesis via Wnt-β-catenin and Wnt-RhoA-Rac1 pathways. J Cell Biol 184(1):83–99
de la Lastra CA, Villegas I (2007) Resveratrol as an antioxidant and pro-oxidant agent: mechanisms and clinical implications. Biochem Soc Trans 35(pt 5):1156–1160
Demiryurek AT, Karamsetty MR, McPhaden AR, Wadsworth RM, Kane KA, MacLean MR (2000) Accumulation of nitrotyrosine correlates with endothelial NO synthase in pulmonary resistance arteries during chronic hypoxia in the rat. Pulm Pharmacol Ther 13(4):157–165
Dennis KE, Aschner JL, Milatovic D, Schmidt JW, Aschner M, Kaplowitz MR, Zhang Y, Fike CD (2009) NADPH oxidases and reactive oxygen species at different stages of chronic hypoxia-induced pulmonary hypertension in newborn piglets. Am J Physiol Lung Cell Mol Physiol 297(4):L596–L607
Deora AA, Win T, Vanhaesebroeck B, Lander HM (1998) A redox-triggered ras-effector interaction. Recruitment of phosphatidylinositol 3′-kinase to Ras by redox stress. J Biol Chem 273(45):29923–29928
Desai AA, Machado RF (2011) Diagnostic and therapeutic algorithm for pulmonary arterial hypertension. Pulm Circ 1(1):122–124
Dewachter L, Adnot S, Fadel E, Humbert M, Maitre B, Barlier-Mur AM, Simonneau G, Hamon M, Naeije R, Eddahibi S (2006) Angiopoietin/Tie2 pathway influences smooth muscle hyperplasia in idiopathic pulmonary hypertension. Am J Respir Crit Care Med 174(9):1025–1033
Dickinson MG, Bartelds B, Molema G, Borgdorff MA, Boersma B, Takens J, Weij M, Wichers P, Sietsma H, Berger RM (2011) Egr-1 expression during neointimal development in flow-associated pulmonary hypertension. Am J Pathol 179(5):2199–2209
Dikalova AE, Bikineyeva AT, Budzyn K, Nazarewicz RR, McCann L, Lewis W, Harrison DG, Dikalov SI (2010) Therapeutic targeting of mitochondrial superoxide in hypertension. Circ Res 107(1):106–116
Dohi T, Beltrami E, Wall NR, Plescia J, Altieri DC (2004) Mitochondrial survivin inhibits apoptosis and promotes tumorigenesis. J Clin Invest 114(8):1117–1127
Dolinay T, Szilasi M, Liu M, Choi AM (2004) Inhaled carbon monoxide confers antiinflammatory effects against ventilator-induced lung injury. Am J Respir Crit Care Med 170(6):613–620
Domenga V, Fardoux P, Lacombe P, Monet M, Maciazek J, Krebs LT, Klonjkowski B, Berrou E, Mericskay M, Li Z, Tournier-Lasserve E, Gridley T, Joutel A (2004) Notch3 is required for arterial identity and maturation of vascular smooth muscle cells. Genes Dev 18(22):2730–2735
Dorfmuller P, Chaumais MC, Giannakouli M, Durand-Gasselin I, Raymond N, Fadel E, Mercier O, Charlotte F, Montani D, Simonneau G, Humbert M, Perros F (2011) Increased oxidative stress and severe arterial remodeling induced by permanent high-flow challenge in experimental pulmonary hypertension. Respir Res 12:119
Dromparis P, Michelakis ED (2013) Mitochondria in vascular health and disease. Annu Rev Physiol 75:95–126
Dromparis P, Sutendra G, Michelakis ED (2010) The role of mitochondria in pulmonary vascular remodeling. J Mol Med 88(10):1003–1010
Dschietzig T, Richter C, Bartsch C, Bohme C, Heinze D, Ott F, Zartnack F, Baumann G, Stangl K (2001) Flow-induced pressure differentially regulates endothelin-1, urotensin II, adrenomedullin, and relaxin in pulmonary vascular endothelium. Biochem Biophys Res Commun 289(1):245–251
Du J, Cullen JJ, Buettner GR (2012) Ascorbic acid: chemistry, biology and the treatment of cancer. Biochim Biophys Acta 1826(2):443–457
Du J, Hui Y, Cheung Y, Bin G, Jiang H, Chen X, Tang C (2004) The possible role of hydrogen sulfide as a smooth muscle cell proliferation inhibitor in rat cultured cells. Heart Vessels 19(2):75–80
Duchen MR (1999) Contributions of mitochondria to animal physiology: from homeostatic sensor to calcium signalling and cell death. J Physiol 516(pt 1):1–17
Duffels MG, Engelfriet PM, Berger RM, van Loon RL, Hoendermis E, Vriend JW, van der Velde ET, Bresser P, Mulder BJ (2007) Pulmonary arterial hypertension in congenital heart disease: an epidemiologic perspective from a Dutch registry. Int J Cardiol 120(2):198–204
Durante W (2013) Role of arginase in vessel wall remodeling. Front Immunol 4:111
Duranteau J, Chandel NS, Kulisz A, Shao Z, Schumacker PT (1998) Intracellular signaling by reactive oxygen species during hypoxia in cardiomyocytes. J Biol Chem 273(19):11619–11624
Eba S, Hoshikawa Y, Moriguchi T, Mitsuishi Y, Satoh H, Ishida K, Watanabe T, Shimizu T, Shimokawa H, Okada Y, Yamamoto M, Kondo T (2013) The nuclear factor erythroid 2-related factor 2 activator oltipraz attenuates chronic hypoxia-induced cardiopulmonary alterations in mice. Am J Respir Cell Mol Biol 49(2):324–333
Elmedal B, de Dam MY, Mulvany MJ, Simonsen U (2004) The superoxide dismutase mimetic, tempol, blunts right ventricular hypertrophy in chronic hypoxic rats. Br J Pharmacol 141(1):105–113
Elmhurst JL, Betti PA, Rangachari PK (1997) Intestinal effects of isoprostanes: evidence for the involvement of prostanoid EP and TP receptors. J Pharmacol Exp Ther 282(3):1198–1205
Ergul S, Brunson CY, Hutchinson J, Tawfik A, Kutlar A, Webb RC, Ergul A (2004) Vasoactive factors in sickle cell disease: in vitro evidence for endothelin-1-mediated vasoconstriction. Am J Hematol 76(3):245–251
Fagan KA, Fouty BW, Tyler RC, Morris KG Jr, Hepler LK, Sato K, LeCras TD, Abman SH, Weinberger HD, Huang PL, McMurtry IF, Rodman DM (1999) The pulmonary circulation of homozygous or heterozygous eNOS-null mice is hyperresponsive to mild hypoxia. J Clin Invest 103(2):291–299
Fagan KA, Morrissey B, Fouty BW, Sato K, Harral JW, Morris KG Jr, Hoedt-Miller M, Vidmar S, McMurtry IF, Rodman DM (2001) Upregulation of nitric oxide synthase in mice with severe hypoxia-induced pulmonary hypertension. Respir Res 2(5):306–313
Fagan KA, Tyler RC, Sato K, Fouty BW, Morris KG Jr, Huang PL, McMurtry IF, Rodman DM (1999) Relative contributions of endothelial, inducible, and neuronal NOS to tone in the murine pulmonary circulation. Am J Physiol 277(3 pt 1):L472–L478
Farber HW, Loscalzo J (2004) Pulmonary arterial hypertension. N Engl J Med 351(16):1655–1665
Farrow KN, Lakshminrusimha S, Reda WJ, Wedgwood S, Czech L, Gugino SF, Davis JM, Russell JA, Steinhorn RH (2008) Superoxide dismutase restores eNOS expression and function in resistance pulmonary arteries from neonatal lambs with persistent pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 295(6):L979–L987
Fessel JP, Flynn CR, Robinson LJ, Penner NL, Gladson S, Kang CJ, Wasserman DH, Hemnes AR, West JD (2013) Hyperoxia synergizes with mutant bone morphogenic protein receptor 2 to cause metabolic stress, oxidant injury, and pulmonary hypertension. Am J Respir Cell Mol Biol 49(5):778–787
Fijalkowska I, Xu W, Comhair SA, Janocha AJ, Mavrakis LA, Krishnamachary B, Zhen L, Mao T, Richter A, Erzurum SC, Tuder RM (2010) Hypoxia inducible-factor 1α regulates the metabolic shift of pulmonary hypertensive endothelial cells. Am J Pathol 176(3):1130–1138
Fike CD, Dikalova A, Slaughter JC, Kaplowitz MR, Zhang Y, Aschner JL (2013) Reactive oxygen species-reducing strategies improve pulmonary arterial responses to nitric oxide in piglets with chronic hypoxia-induced pulmonary hypertension. Antioxid Redox Signal 18(14):1727–1738
Fioretto JR, Campos FJ, Ronchi CF, Ferreira AL, Kurokawa CS, Carpi MF, Moraes MA, Bonatto RC, Defaveri J, Yeum KJ (2012) Effects of inhaled nitric oxide on oxidative stress and histopathological and inflammatory lung injury in a saline-lavaged rabbit model of acute lung injury. Respir Care 57(2):273–281
Francis BN, Wilkins MR, Zhao L (2010) Tetrahydrobiopterin and the regulation of hypoxic pulmonary vasoconstriction. Eur Respir J 36(2):323–330
Francis RC, Vaporidi K, Bloch KD, Ichinose F, Zapol WM (2011) Protective and detrimental effects of sodium sulfide and hydrogen sulfide in murine ventilator-induced lung injury. Anesthesiology 115(5):1012–1021
Fresquet F, Pourageaud F, Leblais V, Brandes RP, Savineau JP, Marthan R, Muller B (2006) Role of reactive oxygen species and gp91phox in endothelial dysfunction of pulmonary arteries induced by chronic hypoxia. Br J Pharmacol 148(5):714–723
Fritz H, Kennedy D, Fergusson D, Fernandes R, Doucette S, Cooley K, Seely A, Sagar S, Wong R, Seely D (2011) Vitamin A and retinoid derivatives for lung cancer: a systematic review and meta analysis. PLoS One 6(6):e21107
Gabrielli LA, Castro PF, Godoy I, Mellado R, Bourge RC, Alcaino H, Chiong M, Greig D, Verdejo HE, Navarro M, Lopez R, Toro B, Quiroga C, Diaz-Araya G, Lavandero S, Garcia L (2011) Systemic oxidative stress and endothelial dysfunction is associated with an attenuated acute vascular response to inhaled prostanoid in pulmonary artery hypertension patients. J Card Fail 17(12):1012–1017
Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G (2009) Guidelines for the diagnosis and treatment of pulmonary hypertension: The Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 30:2493–2537
Gan C, Lankhaar JW, Marcus JT, Westerhof N, Marques KM, Bronzwaer JG, Boonstra A, Postmus PE, Vonk-Noordegraaf A (2006) Impaired left ventricular filling due to right-to-left ventricular interaction in patients with pulmonary arterial hypertension. Am J Physiol Heart Circ Physiol 290(4):H1528–H1533
Gao H, Chen C, Huang S, Li B (2012) Quercetin attenuates the progression of monocrotaline-induced pulmonary hypertension in rats. J Biomed Res 26(2):98–102
Gentile MA (2011) Inhaled medical gases: more to breathe than oxygen. Respir Care 56(9):1341–1357; discussion 1357–1349
Giaid A, Yanagisawa M, Langleben D, Michel RP, Levy R, Shennib H, Kimura S, Masaki T, Duguid WP, Stewart DJ (1993) Expression of endothelin-1 in the lungs of patients with pulmonary hypertension. N Engl J Med 328(24):1732–1739
Gielis JF, Lin JY, Wingler K, Van Schil PE, Schmidt HH, Moens AL (2011) Pathogenetic role of eNOS uncoupling in cardiopulmonary disorders. Free Radic Biol Med 50(7):765–776
Golpon HA, Geraci MW, Moore MD, Miller HL, Miller GJ, Tuder RM, Voelkel NF (2001) HOX genes in human lung: altered expression in primary pulmonary hypertension and emphysema. Am J Pathol 158(3):955–966
Gorenflo M, Zheng C, Werle E, Fiehn W, Ulmer HE (2001) Plasma levels of asymmetrical dimethyl-L-arginine in patients with congenital heart disease and pulmonary hypertension. J Cardiovasc Pharmacol 37(4):489–492
Graham BB, Bandeira AP, Morrell NW, Butrous G, Tuder RM (2010) Schistosomiasis-associated pulmonary hypertension: pulmonary vascular disease: the global perspective. Chest 137(6 suppl):20S–29S
Graham D, Huynh NN, Hamilton CA, Beattie E, Smith RA, Cocheme HM, Murphy MP, Dominiczak AF (2009) Mitochondria-targeted antioxidant MitoQ10 improves endothelial function and attenuates cardiac hypertrophy. Hypertension 54(2):322–328
Grobe AC, Wells SM, Benavidez E, Oishi P, Azakie A, Fineman JR, Black SM (2006) Increased oxidative stress in lambs with increased pulmonary blood flow and pulmonary hypertension: role of NADPH oxidase and endothelial NO synthase. Am J Physiol Lung Cell Mol Physiol 290(6):L1069–L1077
Guignabert C, Alvira CM, Alastalo TP, Sawada H, Hansmann G, Zhao M, Wang L, El-Bizri N, Rabinovitch M (2009) Tie2-mediated loss of peroxisome proliferator-activated receptor-γ in mice causes PDGF receptor-β-dependent pulmonary arterial muscularization. Am J Physiol Lung Cell Mol Physiol 297(6):L1082–L1090
Guzy RD, Hoyos B, Robin E, Chen H, Liu L, Mansfield KD, Simon MC, Hammerling U, Schumacker PT (2005) Mitochondrial complex III is required for hypoxia-induced ROS production and cellular oxygen sensing. Cell Metab 1(6):401–408
Hachulla E, Gressin V, Guillevin L, Carpentier P, Diot E, Sibilia J, Kahan A, Cabane J, Frances C, Launay D, Mouthon L, Allanore Y, Tiev KP, Clerson P, de Groote P, Humbert M (2005) Early detection of pulmonary arterial hypertension in systemic sclerosis: a French nationwide prospective multicenter study. Arthritis Rheum 52(12):3792–3800
Hamon I, Fresson J, Nicolas MB, Buchweiller MC, Franck P, Hascoet JM (2005) Early inhaled nitric oxide improves oxidative balance in very preterm infants. Pediatr Res 57(5 pt 1):637–643
Hansmann G, de Jesus Perez VA, Alastalo TP, Alvira CM, Guignabert C, Bekker JM, Schellong S, Urashima T, Wang L, Morrell NW, Rabinovitch M (2008) An antiproliferative BMP-2/PPARγ/apoE axis in human and murine SMCs and its role in pulmonary hypertension. J Clin Invest 118(5):1846–1857
Harrison RE, Berger R, Haworth SG, Tulloh R, Mache CJ, Morrell NW, Aldred MA, Trembath RC (2005) Transforming growth factor-β receptor mutations and pulmonary arterial hypertension in childhood. Circulation 111(4):435–441
Harrison RE, Flanagan JA, Sankelo M, Abdalla SA, Rowell J, Machado RD, Elliott CG, Robbins IM, Olschewski H, McLaughlin V, Gruenig E, Kermeen F, Halme M, Raisanen-Sokolowski A, Laitinen T, Morrell NW, Trembath RC (2003) Molecular and functional analysis identifies ALK-1 as the predominant cause of pulmonary hypertension related to hereditary haemorrhagic telangiectasia. J Med Genet 40(12):865–871
Hartney T, Birari R, Venkataraman S, Villegas L, Martinez M, Black SM, Stenmark KR, Nozik-Grayck E (2011) Xanthine oxidase-derived ROS upregulate Egr-1 via ERK1/2 in PA smooth muscle cells; model to test impact of extracellular ROS in chronic hypoxia. PLoS One 6(11):e27531
Haven CA, Olson JW, Arcot SS, Gillespie MN (1992) Polyamine transport and ornithine decarboxylase activity in hypoxic pulmonary artery smooth muscle cells. Am J Respir Cell Mol Biol 7(3):286–292
Head BP, Patel HH, Insel PA (2014) Interaction of membrane/lipid rafts with the cytoskeleton: impact on signaling and function: membrane/lipid rafts, mediators of cytoskeletal arrangement and cell signaling. Biochim Biophys Acta 1838(2):532–545
Herrmann J, Samee S, Chade A, Rodriguez Porcel M, Lerman LO, Lerman A (2005) Differential effect of experimental hypertension and hypercholesterolemia on adventitial remodeling. Arterioscler Thromb Vasc Biol 25(2):447–453
Hinderliter AL, Willis PW, Long WA, Clarke WR, Ralph D, Caldwell EJ, Williams W, Ettinger NA, Hill NS, Summer WR, de Boisblanc B, Koch G, Li S, Clayton LM, Jöbsis MM, Crow JW (2003) Frequency and severity of tricuspid regurgitation determined by Doppler echocardiography in primary pulmonary hypertension. Am J Cardiol 91(8):1033–1037
Hoeper MM, Mayer E, Simonneau G, Rubin LJ (2006) Chronic thromboembolic pulmonary hypertension. Circulation 113(16):2011–2020
Hoetzel A, Dolinay T, Vallbracht S, Zhang Y, Kim HP, Ifedigbo E, Alber S, Kaynar AM, Schmidt R, Ryter SW, Choi AM (2008) Carbon monoxide protects against ventilator-induced lung injury via PPAR-γ and inhibition of Egr-1. Am J Respir Crit Care Med 177(11):1223–1232
Homma N, Morio Y, Takahashi H, Yamamoto A, Suzuki T, Sato K, Muramatsu M, Fukuchi Y (2006) Genistein, a phytoestrogen, attenuates monocrotaline-induced pulmonary hypertension. Respiration 73(1):105–112
Hoshikawa Y, Ono S, Suzuki S, Tanita T, Chida M, Song C, Noda M, Tabata T, Voelkel NF, Fujimura S (2001) Generation of oxidative stress contributes to the development of pulmonary hypertension induced by hypoxia. J Appl Physiol 90(4):1299–1306
Hosoki R, Matsuki N, Kimura H (1997) The possible role of hydrogen sulfide as an endogenous smooth muscle relaxant in synergy with nitric oxide. Biochem Biophys Res Commun 237(3):527–531
Howard LS, Watson GM, Wharton J, Rhodes CJ, Chan K, Khengar R, Robbins PA, Kiely DG, Condliffe R, Elliott CA, Pepke-Zaba J, Sheares K, Morrell NW, Davies R, Ashby D, Gibbs JS, Wilkins MR (2013) Supplementation of iron in pulmonary hypertension: rationale and design of a phase II clinical trial in idiopathic pulmonary arterial hypertension. Pulm Circ 3(1):100–107
Hsu LL, Champion HC, Campbell-Lee SA, Bivalacqua TJ, Manci EA, Diwan BA, Schimel DM, Cochard AE, Wang X, Schechter AN, Noguchi CT, Gladwin MT (2007) Hemolysis in sickle cell mice causes pulmonary hypertension due to global impairment in nitric oxide bioavailability. Blood 109(7):3088–3098
Hu HL, Zhang ZX, Chen CS, Cai C, Zhao JP, Wang X (2010) Effects of mitochondrial potassium channel and membrane potential on hypoxic human pulmonary artery smooth muscle cells. Am J Respir Cell Mol Biol 42(6):661–666
Hu W, Jin R, Zhang J, You T, Peng Z, Ge X, Bronson RT, Halperin JA, Loscalzo J, Qin X (2010) The critical roles of platelet activation and reduced NO bioavailability in fatal pulmonary arterial hypertension in a murine hemolysis model. Blood 116(9):1613–1622
Huang PL, Huang Z, Mashimo H, Bloch KD, Moskowitz MA, Bevan JA, Fishman MC (1995) Hypertension in mice lacking the gene for endothelial nitric oxide synthase. Nature 377(6546):239–242
Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, Yaici A, Weitzenblum E, Cordier J-F, Chabot F, Dromer C, Pison C, Reynaud-Gaubert M, Haloun A, Laurent M, Hachulla E, Simonneau G (2006) Pulmonary arterial hypertension in France. Am J Respir Crit Care Med 173(9):1023–1030
Hyduk A, Croft JB, Ayala C, Zheng K, Zheng ZJ, Mensah GA (2005) Pulmonary hypertension surveillance–United States, 1980–2002. Morb Mortal Wkly Rep Surveill Summ 54(5):1–28
Ichinose F, Roberts JD Jr, Zapol WM (2004) Inhaled nitric oxide: a selective pulmonary vasodilator: current uses and therapeutic potential. Circulation 109(25):3106–3111
Iqbal M, Cawthon D, Wideman RF Jr, Bottje WG (2001) Lung mitochondrial dysfunction in pulmonary hypertension syndrome. II. Oxidative stress and inability to improve function with repeated additions of adenosine diphosphate. Poult Sci 80(5):656–665
Irodova NL, Lankin VZ, Konovalova GK, Kochetov AG, Chazova IE (2002) Oxidative stress in patients with primary pulmonary hypertension. Bull Exp Biol Med 133(6):580–582
Irrcher I, Ljubicic V, Hood DA (2009) Interactions between ROS and AMP kinase activity in the regulation of PGC-1α transcription in skeletal muscle cells. Am J Physiol Cell Physiol 296(1):C116–C123
Ivy DD, Parker D, Doran A, Parker D, Kinsella JP, Abman SH (2003) Acute hemodynamic effects and home therapy using a novel pulsed nasal nitric oxide delivery system in children and young adults with pulmonary hypertension. Am J Cardiol 92(7):886–890
Jaiswal AK (2004) Nrf2 signaling in coordinated activation of antioxidant gene expression. Free Radic Biol Med 36(10):1199–1207
Jankov RP, Belcastro R, Ovcina E, Lee J, Massaeli H, Lye SJ, Tanswell AK (2002) Thromboxane A2 receptors mediate pulmonary hypertension in 60 % oxygen-exposed newborn rats by a cyclooxygenase-independent mechanism. Am J Respir Crit Care Med 166(2):208–214
Jankov RP, Kantores C, Pan J, Belik J (2008) Contribution of xanthine oxidase-derived superoxide to chronic hypoxic pulmonary hypertension in neonatal rats. Am J Physiol Lung Cell Mol Physiol 294(2):L233–L245
Janssen LJ (2008) Isoprostanes and lung vascular pathology. Am J Respir Cell Mol Biol 39(4):383–389
Janssen LJ, Tazzeo T (2002) Involvement of TP and EP3 receptors in vasoconstrictor responses to isoprostanes in pulmonary vasculature. J Pharmacol Exp Ther 301(3):1060–1066
Jerkic M, Kabir MG, Davies A, Yu LX, McIntyre BA, Husain NW, Enomoto M, Sotov V, Husain M, Henkelman M, Belik J, Letarte M (2011) Pulmonary hypertension in adult Alk1 heterozygous mice due to oxidative stress. Cardiovasc Res 92(3):375–384
Jernigan NL, Walker BR, Resta TC (2008) Reactive oxygen species mediate RhoA/Rho kinase-induced Ca2+ sensitization in pulmonary vascular smooth muscle following chronic hypoxia. Am J Physiol Lung Cell Mol Physiol 295(3):L515–L529
Jin HF, Du SX, Zhao X, Wei HL, Wang YF, Liang YF, Tang CS, Du JB (2008) Effects of endogenous sulfur dioxide on monocrotaline-induced pulmonary hypertension in rats. Acta Pharmacol Sin 29(10):1157–1166
Jin Y, Calvert TJ, Chen B, Chicoine LG, Joshi M, Bauer JA, Liu Y, Nelin LD (2010) Mice deficient in Mkp-1 develop more severe pulmonary hypertension and greater lung protein levels of arginase in response to chronic hypoxia. Am J Physiol Heart Circ Physiol 298(5):H1518–H1528
Jones R, Jacobson M, Steudel W (1999) α-smooth-muscle actin and microvascular precursor smooth-muscle cells in pulmonary hypertension. Am J Respir Cell Mol Biol 20(4):582–594
Joppa P, Petrasova D, Stancak B, Dorkova Z, Tkacova R (2007) Oxidative stress in patients with COPD and pulmonary hypertension. Wien Klin Wochenschr 119(13–14):428–434
Junqueira FP, Lima CM, Coutinho AC Jr, Parente DB, Bittencourt LK, Bessa LG, Domingues RC, Marchiori E (2012) Pulmonary arterial hypertension: an imaging review comparing MR pulmonary angiography and perfusion with multidetector CT angiography. Br J Radiol 85(1019):1446–1456
Kamezaki F, Tasaki H, Yamashita K, Tsutsui M, Koide S, Nakata S, Tanimoto A, Okazaki M, Sasaguri Y, Adachi T, Otsuji Y (2008) Gene transfer of extracellular superoxide dismutase ameliorates pulmonary hypertension in rats. Am J Respir Crit Care Med 177(2):219–226
Kantores C, McNamara PJ, Teixeira L, Engelberts D, Murthy P, Kavanagh BP, Jankov RP (2006) Therapeutic hypercapnia prevents chronic hypoxia-induced pulmonary hypertension in the newborn rat. Am J Physiol Lung Cell Mol Physiol 291(5):L912–L922
Karuppiah K, Druhan LJ, Chen CA, Smith T, Zweier JL, Sessa WC, Cardounel AJ (2011) Suppression of eNOS-derived superoxide by caveolin-1: a biopterin-dependent mechanism. Am J Physiol Heart Circ Physiol 301(3):H903–H911
Katusic ZS (2001) Vascular endothelial dysfunction: does tetrahydrobiopterin play a role? Am J Physiol Heart Circ Physiol 281(3):H981–H986
Ke Q, Li J, Ding J, Ding M, Wang L, Liu B, Costa M, Huang C (2006) Essential role of ROS-mediated NFAT activation in TNF-α induction by crystalline silica exposure. Am J Physiol Lung Cell Mol Physiol 291(2):L257–L264
Khajali F, Fahimi S (2010) Influence of dietary fat source and supplementary α-tocopheryl acetate on pulmonary hypertension and lipid peroxidation in broilers. J Anim Physiol Anim Nutr 94(6):767–772
Khoo JP, Zhao L, Alp NJ, Bendall JK, Nicoli T, Rockett K, Wilkins MR, Channon KM (2005) Pivotal role for endothelial tetrahydrobiopterin in pulmonary hypertension. Circulation 111(16):2126–2133
Klemm DJ, Majka SM, Crossno JT Jr, Psilas JC, Reusch JE, Garat CV (2011) Reduction of reactive oxygen species prevents hypoxia-induced CREB depletion in pulmonary artery smooth muscle cells. J Cardiovasc Pharmacol 58(2):181–191
Knock GA, Snetkov VA, Shaifta Y, Connolly M, Drndarski S, Noah A, Pourmahram GE, Becker S, Aaronson PI, Ward JP (2009) Superoxide constricts rat pulmonary arteries via Rho-kinase-mediated Ca2+ sensitization. Free Radic Biol Med 46(5):633–642
Kobs RW, Chesler NC (2006) The mechanobiology of pulmonary vascular remodeling in the congenital absence of eNOS. Biomech Model Mechanobiol 5(4):217–225
Kohmoto J, Nakao A, Kaizu T, Tsung A, Ikeda A, Tomiyama K, Billiar TR, Choi AM, Murase N, McCurry KR (2006) Low-dose carbon monoxide inhalation prevents ischemia/reperfusion injury of transplanted rat lung grafts. Surgery 140(2):179–185
Kohmoto J, Nakao A, Stolz DB, Kaizu T, Tsung A, Ikeda A, Shimizu H, Takahashi T, Tomiyama K, Sugimoto R, Choi AM, Billiar TR, Murase N, McCurry KR (2007) Carbon monoxide protects rat lung transplants from ischemia-reperfusion injury via a mechanism involving p38 MAPK pathway. Am J Transplant 7(10):2279–2290
Kolleck I, Sinha P, Rustow B (2002) Vitamin E as an antioxidant of the lung: mechanisms of vitamin E delivery to alveolar type II cells. Am J Respir Crit Care Med 166(12 pt 2):S62–S66
Koubsky K, Durisova J, Mikova D, Herget J (2013) Chronic hypoxia inhibits tetrahydrobiopterin-induced NO production in rat lungs. Respir Physiol Neurobiol 185(3):547–552
Kourembanas S, Hannan RL, Faller DV (1990) Oxygen tension regulates the expression of the platelet-derived growth factor-B chain gene in human endothelial cells. J Clin Invest 86(2):670–674
Kouyoumdjian C, Adnot S, Levame M, Eddahibi S, Bousbaa H, Raffestin B (1994) Continuous inhalation of nitric oxide protects against development of pulmonary hypertension in chronically hypoxic rats. J Clin Invest 94(2):578–584
Kuijpers MH, Gruys E (1984) Spontaneous hypertension and hypertensive renal disease in the fawn-hooded rat. Br J Exp Pathol 65(2):181–190
Kukreja RC, Xi L (2007) eNOS phosphorylation: a pivotal molecular switch in vasodilation and cardioprotection? J Mol Cell Cardiol 42(2):280–282
Kulshreshtha R, Davuluri RV, Calin GA, Ivan M (2008) A microRNA component of the hypoxic response. Cell Death Differ 15(4):667–671
Kunuthur SP, Milliken PH, Gibson CL, Suckling CJ, Wadsworth RM (2011) Tetrahydrobiopterin analogues with NO-dependent pulmonary vasodilator properties. Eur J Pharmacol 650(1):371–377
Kupari M, Rapola J (2012) Reversible pulmonary hypertension associated with vitamin C deficiency. Chest 142(1):225–227
Lachmanová V, Hnilicková O, Povýsilová V, Hampl V, Herget J (2005) N-acetylcysteine inhibits hypoxic pulmonary hypertension most effectively in the initial phase of chronic hypoxia. Life Sci 77(2):175–182
Lai YL, Wu HD, Chen CF (1998) Antioxidants attenuate chronic hypoxic pulmonary hypertension. J Cardiovasc Pharmacol 32(5):714–720
Landmesser U, Dikalov S, Price SR, McCann L, Fukai T, Holland SM, Mitch WE, Harrison DG (2003) Oxidation of tetrahydrobiopterin leads to uncoupling of endothelial cell nitric oxide synthase in hypertension. J Clin Invest 111(8):1201–1209
Lane KL, Talati M, Austin E, Hemnes AR, Johnson JA, Fessel JP, Blackwell T, Mernaugh RL, Robinson L, Fike C, Roberts LJ II, West J (2011) Oxidative injury is a common consequence of BMPR2 mutations. Pulm Circ 1(1):72–83
Lebovitz RM, Zhang H, Vogel H, Cartwright J Jr, Dionne L, Lu N, Huang S, Matzuk MM (1996) Neurodegeneration, myocardial injury, and perinatal death in mitochondrial superoxide dismutase-deficient mice. Proc Natl Acad Sci U S A 93(18):9782–9787
Lee SJ, Smith A, Guo L, Alastalo TP, Li M, Sawada H, Liu X, Chen ZH, Ifedigbo E, Jin Y, Feghali-Bostwick C, Ryter SW, Kim HP, Rabinovitch M, Choi AM (2011) Autophagic protein LC3B confers resistance against hypoxia-induced pulmonary hypertension. Am J Respir Crit Care Med 183(5):649–658
Leiper J, Nandi M, Torondel B, Murray-Rust J, Malaki M, O’Hara B, Rossiter S, Anthony S, Madhani M, Selwood D, Smith C, Wojciak-Stothard B, Rudiger A, Stidwill R, McDonald NQ, Vallance P (2007) Disruption of methylarginine metabolism impairs vascular homeostasis. Nat Med 13(2):198–203
Li H, Meininger CJ, Kelly KA, Hawker JR Jr, Morris SM Jr, Wu G (2002) Activities of arginase I and II are limiting for endothelial cell proliferation. Am J Physiol Regul Integr Comp Physiol 282(1):R64–R69
Li JW, Chen P, Guan XQ, Gong YS, Yang PL (2008) Inhibition of puerarin on pulmonary hypertension in rats with hypoxia and hypercapnia. China J Chin Mater Med 33(5):544–549
Li S, Tabar SS, Malec V, Eul BG, Klepetko W, Weissmann N, Grimminger F, Seeger W, Rose F, Hanze J (2008) NOX4 regulates ROS levels under normoxic and hypoxic conditions, triggers proliferation, and inhibits apoptosis in pulmonary artery adventitial fibroblasts. Antioxid Redox Signal 10(10):1687–1698
Li WG, Miller FJ Jr, Zhang HJ, Spitz DR, Oberley LW, Weintraub NL (2001) H2O2-induced O2 production by a non-phagocytic NAD(P)H oxidase causes oxidant injury. J Biol Chem 276(31):29251–29256
Lin MJ, Yang XR, Cao YN, Sham JS (2007) Hydrogen peroxide-induced Ca2+ mobilization in pulmonary arterial smooth muscle cells. Am J Physiol Lung Cell Mol Physiol 292(6):L1598–L1608
Liu JQ, Folz RJ (2004) Extracellular superoxide enhances 5-HT-induced murine pulmonary artery vasoconstriction. Am J Physiol Lung Cell Mol Physiol 287(1):L111–L118
Liu JQ, Zelko IN, Erbynn EM, Sham JS, Folz RJ (2006) Hypoxic pulmonary hypertension: role of superoxide and NADPH oxidase (gp91phox). Am J Physiol Lung Cell Mol Physiol 290(1):L2–L10
Liu Y, Cox SR, Morita T, Kourembanas S (1995) Hypoxia regulates vascular endothelial growth factor gene expression in endothelial cells. Identification of a 5′ enhancer. Circ Res 77(3):638–643
Longo DL, Harrison TR (2012) Harrison’s principles of internal medicine, 18th edn. McGraw-Hill, New York
Lopez-Lopez JG, Moral-Sanz J, Frazziano G, Gomez-Villalobos MJ, Flores-Hernandez J, Monjaraz E, Cogolludo A, Perez-Vizcaino F (2008) Diabetes induces pulmonary artery endothelial dysfunction by NADPH oxidase induction. Am J Physiol Lung Cell Mol Physiol 295(5):L727–L732
Lopez-Ongil S, Saura M, Zaragoza C, Gonzalez-Santiago L, Rodriguez-Puyol M, Lowenstein CJ, Rodriguez-Puyol D (2002) Hydrogen peroxide regulation of bovine endothelin-converting enzyme-1. Free Radic Biol Med 32(5):406–413
Lorenzoni AG, Ruiz-Feria CA (2006) Effects of vitamin E and L-arginine on cardiopulmonary function and ascites parameters in broiler chickens reared under subnormal temperatures. Poult Sci 85(12):2241–2250
Lu MF, Xiao ZT, Zhang HY (2013) Where do health benefits of flavonoids come from? Insights from flavonoid targets and their evolutionary history. Biochem Biophys Res Commun 434(4):701–704
Machado RD, Eickelberg O, Elliott CG, Geraci MW, Hanaoka M, Loyd JE, Newman JH, Phillips JA, Soubrier F, Trembath RC, Chung WK (2009) Genetics and genomics of pulmonary arterial hypertension. J Am Coll Cardiol 54(1 suppl):S32–S42
Machado RF, Gladwin MT (2010) Pulmonary hypertension in hemolytic disorders: pulmonary vascular disease: the global perspective. Chest 137(6 suppl):30S–38S
Madigan M, Zuckerbraun B (2013) Therapeutic potential of the nitrite-generated NO pathway in vascular dysfunction. Front Immunol 4:174
Malenfant S, Neyron AS, Paulin R, Potus F, Meloche J, Provencher S, Bonnet S (2013) Signal transduction in the development of pulmonary arterial hypertension. Pulm Circ 3(2):278–293
Maniatis NA, Shinin V, Schraufnagel DE, Okada S, Vogel SM, Malik AB, Minshall RD (2008) Increased pulmonary vascular resistance and defective pulmonary artery filling in caveolin-1−/− mice. Am J Physiol Lung Cell Mol Physiol 294(5):L865–L873
Marcus JT, Gan CT, Zwanenburg JJ, Boonstra A, Allaart CP, Gotte MJ, Vonk-Noordegraaf A (2008) Interventricular mechanical asynchrony in pulmonary arterial hypertension: left-to-right delay in peak shortening is related to right ventricular overload and left ventricular underfilling. J Am Coll Cardiol 51(7):750–757
Maron BA, Tang SS, Loscalzo J (2013) S-nitrosothiols and the S-nitrosoproteome of the cardiovascular system. Antioxid Redox Signal 18(3):270–287
Masri FA, Comhair SA, Dostanic-Larson I, Kaneko FT, Dweik RA, Arroliga AC, Erzurum SC (2008) Deficiency of lung antioxidants in idiopathic pulmonary arterial hypertension. Clin Transl Sci 1(2):99–106
Mata-Greenwood E, Grobe A, Kumar S, Noskina Y, Black SM (2005) Cyclic stretch increases VEGF expression in pulmonary arterial smooth muscle cells via TGF-β1 and reactive oxygen species: a requirement for NAD(P)H oxidase. Am J Physiol Lung Cell Mol Physiol 289(2):L288–L289
Mata-Greenwood E, Meyrick B, Steinhorn RH, Fineman JR, Black SM (2003) Alterations in TGF-β1 expression in lambs with increased pulmonary blood flow and pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 285(1):L209–L221
Matori H, Umar S, Nadadur RD, Sharma S, Partow-Navid R, Afkhami M, Amjedi M, Eghbali M (2012) Genistein, a soy phytoestrogen, reverses severe pulmonary hypertension and prevents right heart failure in rats. Hypertension 60(2):425–430
Maunder RJ, Winn RK, Gleisner JM, Hildebrandt J, Harlan JM (1988) Effect of intravenous catalase on the pulmonary vascular response to endotoxemia in goats. J Appl Physiol 64(2):697–704
McGoon M, Gutterman D, Steen V, Barst R, McCrory DC, Fortin TA, Loyd JE, American College of Chest Physicians (2004) Screening, early detection, and diagnosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 126(1 suppl):14S–34S
McKenzie JC, Clancy J Jr, Klein RM (1984) Autoradiographic analysis of cell proliferation and protein synthesis in the pulmonary trunk of rats during the early development of hypoxia-induced pulmonary hypertension. Blood Vessels 21(2):80–89
McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, Mathier MA, McGoon MD, Park MH, Rosenson RS, Rubin LJ, Tapson VF, Varga J, American College of Cardiology Foundation Task Force on Expert Consensus Documents, American Heart Association, American College of Chest Physicians, American Thoracic Society, Inc., Pulmonary Hypertension Association (2009) ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J Am Coll Cardiol 53(17):1573–1619
McMahon TJ, Ahearn GS, Moya MP, Gow AJ, Huang YC, Luchsinger BP, Nudelman R, Yan Y, Krichman AD, Bashore TM, Califf RM, Singel DJ, Piantadosi CA, Tapson VF, Stamler JS (2005) A nitric oxide processing defect of red blood cells created by hypoxia: deficiency of S-nitrosohemoglobin in pulmonary hypertension. Proc Natl Acad Sci U S A 102(41):14801–14806
McMurtry MS, Archer SL, Altieri DC, Bonnet S, Haromy A, Harry G, Bonnet S, Puttagunta L, Michelakis ED (2005) Gene therapy targeting survivin selectively induces pulmonary vascular apoptosis and reverses pulmonary arterial hypertension. J Clin Invest 115(6):1479–1491
McMurtry MS, Bonnet S, Wu X, Dyck JR, Haromy A, Hashimoto K, Michelakis ED (2004) Dichloroacetate prevents and reverses pulmonary hypertension by inducing pulmonary artery smooth muscle cell apoptosis. Circ Res 95(8):830–840
Meloche J, Courchesne A, Barrier M, Carter S, Bisserier M, Paulin R, Lauzon-Joset JF, Breuils-Bonnet S, Tremblay E, Biardel S, Racine C, Courture C, Bonnet P, Majka SM, Deshaies Y, Picard F, Provencher S, Bonnet S (2013) Critical role for the advanced glycation end-products receptor in pulmonary arterial hypertension etiology. J Am Heart Assoc 2(1):e005157
Mertens MT, Gertner E (2011) Rheumatic manifestations of scurvy: a report of three recent cases in a major urban center and a review. Semin Arthritis Rheum 41(2):286–290
Meyrick B, Reid L (1980) Hypoxia-induced structural changes in the media and adventitia of the rat hilar pulmonary artery and their regression. Am J Pathol 100(1):151–178
Michelakis ED, Hampl V, Nsair A, Wu X, Harry G, Haromy A, Gurtu R, Archer SL (2002) Diversity in mitochondrial function explains differences in vascular oxygen sensing. Circ Res 90(12):1307–1315
Michelakis ED, Thebaud B, Weir EK, Archer SL (2004) Hypoxic pulmonary vasoconstriction: redox regulation of O2-sensitive K+ channels by a mitochondrial O2-sensor in resistance artery smooth muscle cells. J Mol Cell Cardiol 37(6):1119–1136
Millatt LJ, Whitley GS, Li D, Leiper JM, Siragy HM, Carey RM, Johns RA (2003) Evidence for dysregulation of dimethylarginine dimethylaminohydrolase I in chronic hypoxia-induced pulmonary hypertension. Circulation 108(12):1493–1498
Milligan SA, Hoeffel JM, Goldstein IM, Flick MR (1988) Effect of catalase on endotoxin-induced acute lung injury in unanesthetized sheep. Am Rev Respir Dis 137(2):420–428
Mirrakhimov AE, Ali AM, Barbaryan A, Prueksaritanond S (2013) Human immunodeficiency virus and pulmonary arterial hypertension. ISRN Cardiol 2013:903454
Mitchell LA, Channell MM, Royer CM, Ryter SW, Choi AM, McDonald JD (2010) Evaluation of inhaled carbon monoxide as an anti-inflammatory therapy in a nonhuman primate model of lung inflammation. Am J Physiol Lung Cell Mol Physiol 299(6):L891–L897
Mittal M, Gu XQ, Pak O, Pamenter ME, Haag D, Fuchs DB, Schermuly RT, Ghofrani HA, Brandes RP, Seeger W, Grimminger F, Haddad GG, Weissmann N (2012) Hypoxia induces Kv channel current inhibition by increased NADPH oxidase-derived reactive oxygen species. Free Radic Biol Med 52(6):1033–1042
Mittal M, Roth M, Konig P, Hofmann S, Dony E, Goyal P, Selbitz AC, Schermuly RT, Ghofrani HA, Kwapiszewska G, Kummer W, Klepetko W, Hoda MA, Fink L, Hanze J, Seeger W, Grimminger F, Schmidt HH, Weissmann N (2007) Hypoxia-dependent regulation of nonphagocytic NADPH oxidase subunit NOX4 in the pulmonary vasculature. Circ Res 101(3):258–267
Montani D, Chaumais MC, Guignabert C, Gunther S, Girerd B, Jais X, Algalarrondo V, Price LC, Sitbon O, Simonneau G, Humbert M (2014) Targeted therapies in pulmonary arterial hypertension. Pharmacol Ther 141(2):172–191
Montani D, Gunther S, Dorfmuller P, Perros F, Girerd B, Garcia G, Jais X, Savale L, Artaud-Macari E, Price LC, Humbert M, Simonneau G, Sitbon O (2013) Pulmonary arterial hypertension. Orphanet J Rare Dis 8(1):97
Montisano DF, Mann T, Spragg RG (1992) H2O2 increases expression of pulmonary artery endothelial cell platelet-derived growth factor mRNA. J Appl Physiol 73(6):2255–2262
Morris CR, Kato GJ, Poljakovic M, Wang X, Blackwelder WC, Sachdev V, Hazen SL, Vichinsky EP, Morris SM Jr, Gladwin MT (2005) Dysregulated arginine metabolism, hemolysis-associated pulmonary hypertension, and mortality in sickle cell disease. JAMA 294(1):81–90
Morrow JD, Roberts LJ (2002) The isoprostanes: their role as an index of oxidant stress status in human pulmonary disease. Am J Respir Crit Care Med 166(12 pt 2):S25–S30
Mount PF, Kemp BE, Power DA (2007) Regulation of endothelial and myocardial NO synthesis by multi-site eNOS phosphorylation. J Mol Cell Cardiol 42(2):271–279
Mukerjee D, St George D, Coleiro B, Knight C, Denton CP, Davar J, Black CM, Coghlan JG (2003) Prevalence and outcome in systemic sclerosis associated pulmonary arterial hypertension: application of a registry approach. Ann Rheum Dis 62(11):1088–1093
Murata T, Lin MI, Huang Y, Yu J, Bauer PM, Giordano FJ, Sessa WC (2007) Reexpression of caveolin-1 in endothelium rescues the vascular, cardiac, and pulmonary defects in global caveolin-1 knockout mice. J Exp Med 204(10):2373–2382
Murata T, Sato K, Hori M, Ozaki H, Karaki H (2002) Decreased endothelial nitric-oxide synthase (eNOS) activity resulting from abnormal interaction between eNOS and its regulatory proteins in hypoxia-induced pulmonary hypertension. J Biol Chem 277(46):44085–44092
Nachar RA, Pastene CM, Herrera EA, Riquelme RA, Sanhueza EM, Troncoso S, Llanos AJ (2001) Low-dose inhaled carbon monoxide reduces pulmonary vascular resistance during acute hypoxemia in adult sheep. High Alt Med Biol 2(3):377–385
Nagasaka H, Okano Y, Aizawa M, Miida T, Yorifuji T, Tajima G, Sakura N, Takatani T, Sanayama Y, Sugamoto K, Mayumi M, Kobayashi K, Hirano K, Takayanagi M, Tsukahara H (2010) Altered metabolisms of mediators controlling vascular function and enhanced oxidative stress in asymptomatic children with congenital portosystemic venous shunt. Metabolism 59(1):107–113
Nandi M, Leiper J, Arrigoni F, Hislop A, Vallance P, Haworth S (2006) Developmental regulation of GTP-CH1 in the porcine lung and its relationship to pulmonary vascular relaxation. Pediatr Res 59(6):767–772
Nasim MT, Ogo T, Ahmed M, Randall R, Chowdhury HM, Snape KM, Bradshaw TY, Southgate L, Lee GJ, Jackson I, Lord GM, Gibbs JS, Wilkins MR, Ohta-Ogo K, Nakamura K, Girerd B, Coulet F, Soubrier F, Humbert M, Morrell NW, Trembath RC, Machado RD (2011) Molecular genetic characterization of SMAD signaling molecules in pulmonary arterial hypertension. Hum Mutat 32(12):1385–1389
Nisbet RE, Bland JM, Kleinhenz DJ, Mitchell PO, Walp ER, Sutliff RL, Hart CM (2010) Rosiglitazone attenuates chronic hypoxia-induced pulmonary hypertension in a mouse model. Am J Respir Cell Mol Biol 42(4):482–490
Nozik-Grayck E, Suliman HB, Majka S, Albietz J, Van Rheen Z, Roush K, Stenmark KR (2008) Lung EC-SOD overexpression attenuates hypoxic induction of Egr-1 and chronic hypoxic pulmonary vascular remodeling. Am J Physiol Lung Cell Mol Physiol 295(3):L422–L430
Odhiambo A, Perlman DH, Huang H, Costello CE, Farber HW, Steinberg MH, McComb ME, Klings ES (2007) Identification of oxidative post-translational modification of serum albumin in patients with idiopathic pulmonary arterial hypertension and pulmonary hypertension of sickle cell anemia. Rapid Commun Mass Spectrom 21(14):2195–2203
Oess S, Icking A, Fulton D, Govers R, Muller-Esterl W (2006) Subcellular targeting and trafficking of nitric oxide synthases. Biochem J 396(3):401–409
Ogura S, Shimosawa T, Mu S, Sonobe T, Kawakami-Mori F, Wang H, Uetake Y, Yoshida K, Yatomi Y, Shirai M, Fujita T (2013) Oxidative stress augments pulmonary hypertension in chronically hypoxic mice overexpressing the oxidized LDL receptor. Am J Physiol Heart Circ Physiol 305(2):H155–H162
Ohashi Y, Kawashima S, Hirata K, Yamashita T, Ishida T, Inoue N, Sakoda T, Kurihara H, Yazaki Y, Yokoyama M (1998) Hypotension and reduced nitric oxide-elicited vasorelaxation in transgenic mice overexpressing endothelial nitric oxide synthase. J Clin Invest 102(12):2061–2071
Olson JW, Altiere RJ, Gillespie MN (1984) Prolonged activation of rat lung ornithine decarboxylase in monocrotaline-induced pulmonary hypertension. Biochem Pharmacol 33(22):3633–3637
Paddenberg R, Goldenberg A, Faulhammer P, Braun-Dullaeus RC, Kummer W (2003) Mitochondrial complex II is essential for hypoxia-induced ROS generation and vasoconstriction in the pulmonary vasculature. Adv Exp Med Biol 536:163–169
Paffett ML, Hesterman J, Candelaria G, Lucas S, Anderson T, Irwin D, Hoppin J, Norenberg J, Campen MJ (2012) Longitudinal in vivo SPECT/CT imaging reveals morphological changes and cardiopulmonary apoptosis in a rodent model of pulmonary arterial hypertension. PLoS One 7(7):e40910
Paffett ML, Lucas SN, Campen MJ (2012) Resveratrol reverses monocrotaline-induced pulmonary vascular and cardiac dysfunction: a potential role for atrogin-1 in smooth muscle. Vascul Pharmacol 56(1–2):64–73
Palmer RM, Rees DD, Ashton DS, Moncada S (1988) L-arginine is the physiological precursor for the formation of nitric oxide in endothelium-dependent relaxation. Biochem Biophys Res Commun 153(3):1251–1256
Patel HH, Zhang S, Murray F, Suda RY, Head BP, Yokoyama U, Swaney JS, Niesman IR, Schermuly RT, Pullamsetti SS, Thistlethwaite PA, Miyanohara A, Farquhar MG, Yuan JX, Insel PA (2007) Increased smooth muscle cell expression of caveolin-1 and caveolae contribute to the pathophysiology of idiopathic pulmonary arterial hypertension. FASEB J 21(11):2970–2979
Paulin R, Courboulin A, Meloche J, Mainguy V, Dumas de la Roque E, Saksouk N, Cote J, Provencher S, Sussman MA, Bonnet S (2011) Signal transducers and activators of transcription-3/pim1 axis plays a critical role in the pathogenesis of human pulmonary arterial hypertension. Circulation 123(11):1205–1215
Peacock AJ, Murphy NF, McMurray JJ, Caballero L, Stewart S (2007) An epidemiological study of pulmonary arterial hypertension. Eur Respir J 30(1):104–109
Perez-Penate G, Julia-Serda G, Pulido-Duque JM, Gorriz-Gomez E, Cabrera-Navarro P (2001) One-year continuous inhaled nitric oxide for primary pulmonary hypertension. Chest 119(3):970–973
Perez-Penate GM, Julia-Serda G, Ojeda-Betancort N, Garcia-Quintana A, Pulido-Duque J, Rodriguez-Perez A, Cabrera-Navarro P, Gomez-Sanchez MA (2008) Long-term inhaled nitric oxide plus phosphodiesterase 5 inhibitors for severe pulmonary hypertension. J Heart Lung Transplant 27(12):1326–1332
Pourmahram GE, Snetkov VA, Shaifta Y, Drndarski S, Knock GA, Aaronson PI, Ward JP (2008) Constriction of pulmonary artery by peroxide: role of Ca2+ release and PKC. Free Radic Biol Med 45(10):1468–1476
Predmore BL, Kondo K, Bhushan S, Zlatopolsky MA, King AL, Aragon JP, Grinsfelder DB, Condit ME, Lefer DJ (2012) The polysulfide diallyl trisulfide protects the ischemic myocardium by preservation of endogenous hydrogen sulfide and increasing nitric oxide bioavailability. Am J Physiol Heart Circ Physiol 302(11):H2410–H2418
Preston IR, Tang G, Tilan JU, Hill NS, Suzuki YJ (2005) Retinoids and pulmonary hypertension. Circulation 111(6):782–790
Proweller A, Pear WS, Parmacek MS (2005) Notch signaling represses myocardin-induced smooth muscle cell differentiation. J Biol Chem 280(10):8994–9004
Pullamsetti S, Kiss L, Ghofrani HA, Voswinckel R, Haredza P, Klepetko W, Aigner C, Fink L, Muyal JP, Weissmann N, Grimminger F, Seeger W, Schermuly RT (2005) Increased levels and reduced catabolism of asymmetric and symmetric dimethylarginines in pulmonary hypertension. FASEB J 19(9):1175–1177
Qin Y, Zhou A, Ben X, Shen J, Liang Y, Li F (2001) All-trans retinoic acid in pulmonary vascular structural remodeling in rats with pulmonary hypertension induced by monocrotaline. Chin Med J (Engl) 114(5):462–465
Qingyou Z, Junbao D, Weijin Z, Hui Y, Chaoshu T, Chunyu Z (2004) Impact of hydrogen sulfide on carbon monoxide/heme oxygenase pathway in the pathogenesis of hypoxic pulmonary hypertension. Biochem Biophys Res Commun 317(1):30–37
Quintavalle M, Elia L, Condorelli G, Courtneidge SA (2010) MicroRNA control of podosome formation in vascular smooth muscle cells in vivo and in vitro. J Cell Biol 189(1):13–22
Rabinovitch M (2012) Molecular pathogenesis of pulmonary arterial hypertension. J Clin Invest 122(12):4306–4313
Raman KG, Barbato JE, Ifedigbo E, Ozanich BA, Zenati MS, Otterbein LE, Tzeng E (2006) Inhaled carbon monoxide inhibits intimal hyperplasia and provides added benefit with nitric oxide. J Vasc Surg 44(1):151–158
Ramiro-Diaz JM, Nitta CH, Maston LD, Codianni S, Giermakowska W, Resta TC, Gonzalez Bosc LV (2013) NFAT is required for spontaneous pulmonary hypertension in superoxide dismutase 1 knockout mice. Am J Physiol Lung Cell Mol Physiol 304(9):L613–L625
Rao A, Luo C, Hogan PG (1997) Transcription factors of the NFAT family: regulation and function. Annu Rev Immunol 15:707–747
Rao J, Li J, Liu Y, Lu P, Sun X, Sugumaran PK, Zhu D (2012) The key role of PGC-1α in mitochondrial biogenesis and the proliferation of pulmonary artery vascular smooth muscle cells at an early stage of hypoxic exposure. Mol Cell Biochem 367(1–2):9–18
Rashid M, Kotwani A, Fahim M (2012) Long-acting phosphodiesterase 5 inhibitor, tadalafil, and superoxide dismutase mimetic, tempol, protect against acute hypoxia-induced pulmonary hypertension in rats. Hum Exp Toxicol 31(6):626–636
Rathore R, Zheng YM, Niu CF, Liu QH, Korde A, Ho YS, Wang YX (2008) Hypoxia activates NADPH oxidase to increase [ROS]i and [Ca2+]i through the mitochondrial ROS-PKCepsilon signaling axis in pulmonary artery smooth muscle cells. Free Radic Biol Med 45(9):1223–1231
Redout EM, van der Toorn A, Zuidwijk MJ, van de Kolk CW, van Echteld CJ, Musters RJ, van Hardeveld C, Paulus WJ, Simonides WS (2010) Antioxidant treatment attenuates pulmonary arterial hypertension-induced heart failure. Am J Physiol Heart Circ Physiol 298(3):H1038–H1047
Redout EM, Wagner MJ, Zuidwijk MJ, Boer C, Musters RJ, van Hardeveld C, Paulus WJ, Simonides WS (2007) Right-ventricular failure is associated with increased mitochondrial complex II activity and production of reactive oxygen species. Cardiovasc Res 75(4):770–781
Rehman J, Archer SL (2010) A proposed mitochondrial-metabolic mechanism for initiation and maintenance of pulmonary arterial hypertension in fawn-hooded rats: the Warburg model of pulmonary arterial hypertension. Adv Exp Med Biol 661:171–185
Rhodes CJ, Wharton J, Howard L, Gibbs JS, Vonk-Noordegraaf A, Wilkins MR (2011) Iron deficiency in pulmonary arterial hypertension: a potential therapeutic target. Eur Respir J 38(6):1453–1460
Robbins IM, Hemnes AR, Gibbs JS, Christman BW, Howard L, Meehan S, Cabrita I, Gonzalez R, Oyler T, Zhao L, Du RH, Mendes LA, Wilkins MR (2011) Safety of sapropterin dihydrochloride (6r-bh4) in patients with pulmonary hypertension. Exp Lung Res 37(1):26–34
Robbins IM, Morrow JD, Christman BW (2005) Oxidant stress but not thromboxane decreases with epoprostenol therapy. Free Radic Biol Med 38(5):568–574
Roberts JD Jr, Roberts CT, Jones RC, Zapol WM, Bloch KD (1995) Continuous nitric oxide inhalation reduces pulmonary arterial structural changes, right ventricular hypertrophy, and growth retardation in the hypoxic newborn rat. Circ Res 76(2):215–222
Roberts LJ, Morrow JD (2000) Measurement of F(2)-isoprostanes as an index of oxidative stress in vivo. Free Radic Biol Med 28(4):505–513
Ronchi CF, Ferreira AL, Campos FJ, Kurokawa CS, Carpi MF, Moraes MA, Bonatto RC, Yeum KJ, Fioretto JR (2013) Interactive effects of mechanical ventilation, inhaled nitric oxide and oxidative stress in acute lung injury. Respir Physiol Neurobiol 190c:118–123
Roos CM, Frank DU, Xue C, Johns RA, Rich GF (1996) Chronic inhaled nitric oxide: effects on pulmonary vascular endothelial function and pathology in rats. J Appl Physiol 80(1):252–260
Rother RP, Bell L, Hillmen P, Gladwin MT (2005) The clinical sequelae of intravascular hemolysis and extracellular plasma hemoglobin: a novel mechanism of human disease. JAMA 293(13):1653–1662
Ryter SW, Choi AM (2008) Caveolin-1: a critical regulator of pulmonary vascular architecture and nitric oxide bioavailability in pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 294(5):L862–L864
Safdar Z, Bartolome S, Sussman N (2012) Portopulmonary hypertension: an update. Liver Transpl 18(8):881–891
Saito A, Sugawara A, Uruno A, Kudo M, Kagechika H, Sato Y, Owada Y, Kondo H, Sato M, Kurabayashi M, Imaizumi M, Tsuchiya S, Ito S (2007) All-trans retinoic acid induces in vitro angiogenesis via retinoic acid receptor: possible involvement of paracrine effects of endogenous vascular endothelial growth factor signaling. Endocrinology 148(3):1412–1423
Sakao S, Tatsumi K (2011) The effects of antiangiogenic compound SU5416 in a rat model of pulmonary arterial hypertension. Respiration 81(3):253–261
Sasaki A, Doi S, Mizutani S, Azuma H (2007) Roles of accumulated endogenous nitric oxide synthase inhibitors, enhanced arginase activity, and attenuated nitric oxide synthase activity in endothelial cells for pulmonary hypertension in rats. Am J Physiol Lung Cell Mol Physiol 292(6):L1480–L1487
Schmidt AF, Goncalves FL, Regis AC, Gallindo RM, Sbragia L (2012) Prenatal retinoic acid improves lung vascularization and VEGF expression in CDH rat. Am J Obstet Gynecol 207(1):76.e25–76.e32
Schunemann HJ, Grant BJ, Freudenheim JL, Muti P, Browne RW, Drake JA, Klocke RA, Trevisan M (2001) The relation of serum levels of antioxidant vitamins C and E, retinol and carotenoids with pulmonary function in the general population. Am J Respir Crit Care Med 163(5):1246–1255
Searles CD (2006) Transcriptional and posttranscriptional regulation of endothelial nitric oxide synthase expression. Am J Physiol Cell Physiol 291(5):C803–C816
Sentman ML, Granstrom M, Jakobson H, Reaume A, Basu S, Marklund SL (2006) Phenotypes of mice lacking extracellular superoxide dismutase and copper- and zinc-containing superoxide dismutase. J Biol Chem 281(11):6904–6909
Seta F, Rahmani M, Turner PV, Funk CD (2011) Pulmonary oxidative stress is increased in cyclooxygenase-2 knockdown mice with mild pulmonary hypertension induced by monocrotaline. PLoS One 6(8):e23439
Shao Z, Wang Z, Shrestha K, Thakur A, Borowski AG, Sweet W, Thomas JD, Moravec CS, Hazen SL, Tang WH (2012) Pulmonary hypertension associated with advanced systolic heart failure: dysregulated arginine metabolism and importance of compensatory dimethylarginine dimethylaminohydrolase-1. J Am Coll Cardiol 59(13):1150–1158
Sharma S, Grobe AC, Wiseman DA, Kumar S, Englaish M, Najwer I, Benavidez E, Oishi P, Azakie A, Fineman JR, Black SM (2007) Lung antioxidant enzymes are regulated by development and increased pulmonary blood flow. Am J Physiol Lung Cell Mol Physiol 293(4):L960–L971
Sharoni Y, Linnewiel-Hermoni K, Khanin M, Salman H, Veprik A, Danilenko M, Levy J (2012) Carotenoids and apocarotenoids in cellular signaling related to cancer: a review. Mol Nutr Food Res 56(2):259–269
Shen CY, Lee JF, Su CL, Wang D, Chen CF (2008) Hypoxia and reoxygenation of the lung tissues induced mRNA expressions of superoxide dismutase and catalase and interventions from different antioxidants. Transplant Proc 40(7):2182–2184
Shintani M, Yagi H, Nakayama T, Saji T, Matsuoka R (2009) A new nonsense mutation of SMAD8 associated with pulmonary arterial hypertension. J Med Genet 46(5):331–337
Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, Elliott CG, Gaine SP, Gladwin MT, Jing ZC, Krowka MJ, Langleben D, Nakanishi N, Souza R (2009) Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 54(1 suppl):S43–S54
Smith TG, Balanos GM, Croft QP, Talbot NP, Dorrington KL, Ratcliffe PJ, Robbins PA (2008) The increase in pulmonary arterial pressure caused by hypoxia depends on iron status. J Physiol 586(pt 24):5999–6005
Snell GI, Salamonsen RF, Bergin P, Esmore DS, Khan S, Williams TJ (1995) Inhaled nitric oxide used as a bridge to heart-lung transplantation in a patient with end-stage pulmonary hypertension. Am J Respir Crit Care Med 151(4):1263–1266
Sousa-Santos O, Neto-Neves EM, Ferraz KC, Sertorio JT, Portella RL, Tanus-Santos JE (2013) The antioxidant tempol decreases acute pulmonary thromboembolism-induced hemolysis and nitric oxide consumption. Thromb Res 132(5):578–583
Spiekermann S, Schenk K, Hoeper MM (2009) Increased xanthine oxidase activity in idiopathic pulmonary arterial hypertension. Eur Respir J 34(1):276
Sproule DM, Dyme J, Coku J, de Vinck D, Rosenzweig E, Chung WK, De Vivo DC (2008) Pulmonary artery hypertension in a child with MELAS due to a point mutation of the mitochondrial tRNA((Leu)) gene (m.3243A > G). J Inherit Metab Dis. doi:10.1007/s10545-007-0735-3
Srisook K, Han SS, Choi HS, Li MH, Ueda H, Kim C, Cha YN (2006) CO from enhanced HO activity or from CORM-2 inhibits both O2– and NO production and downregulates HO-1 expression in LPS-stimulated macrophages. Biochem Pharmacol 71(3):307–318
Star GP, Giovinazzo M, Langleben D (2013) ALK2 and BMPR2 knockdown and endothelin-1 production by pulmonary microvascular endothelial cells. Microvasc Res 85:46–53
Steinhorn RH, Albert G, Swartz DD, Russell JA, Levine CR, Davis JM (2001) Recombinant human superoxide dismutase enhances the effect of inhaled nitric oxide in persistent pulmonary hypertension. Am J Respir Crit Care Med 164(5):834–839
Steudel W, Ichinose F, Huang PL, Hurford WE, Jones RC, Bevan JA, Fishman MC, Zapol WM (1997) Pulmonary vasoconstriction and hypertension in mice with targeted disruption of the endothelial nitric oxide synthase (NOS 3) gene. Circ Res 81(1):34–41
Steudel W, Scherrer-Crosbie M, Bloch KD, Weimann J, Huang PL, Jones RC, Picard MH, Zapol WM (1998) Sustained pulmonary hypertension and right ventricular hypertrophy after chronic hypoxia in mice with congenital deficiency of nitric oxide synthase 3. J Clin Invest 101(11):2468–2477
Sturrock A, Cahill B, Norman K, Huecksteadt TP, Hill K, Sanders K, Karwande SV, Stringham JC, Bull DA, Gleich M, Kennedy TP, Hoidal JR (2006) Transforming growth factor-β1 induces Nox4 NAD(P)H oxidase and reactive oxygen species-dependent proliferation in human pulmonary artery smooth muscle cells. Am J Physiol Lung Cell Mol Physiol 290(4):L661–L673
Sud N, Wells SM, Sharma S, Wiseman DA, Wilham J, Black SM (2008) Asymmetric dimethylarginine inhibits HSP90 activity in pulmonary arterial endothelial cells: role of mitochondrial dysfunction. Am J Physiol Cell Physiol 294(6):C1407–C1418
Sugawara T, Noshita N, Lewen A, Gasche Y, Ferrand-Drake M, Fujimura M, Morita-Fujimura Y, Chan PH (2002) Overexpression of copper/zinc superoxide dismutase in transgenic rats protects vulnerable neurons against ischemic damage by blocking the mitochondrial pathway of caspase activation. J Neurosci 22(1):209–217
Sutendra G, Bonnet S, Rochefort G, Haromy A, Folmes KD, Lopaschuk GD, Dyck JR, Michelakis ED (2010) Fatty acid oxidation and malonyl-CoA decarboxylase in the vascular remodeling of pulmonary hypertension. Sci Transl Med 2(44):44ra58
Suzuki YJ, Steinhorn RH, Gladwin MT (2013) Antioxidant therapy for the treatment of pulmonary hypertension. Antioxid Redox Signal 18(14):1723–1726
Swamidas GP, Basaraba RJ, Baybutt RC (1999) Dietary retinol inhibits inflammatory responses of rats treated with monocrotaline. J Nutr 129(7):1285–1290
Sydow K, Münzel T (2003) ADMA and oxidative stress. Atheroscler Suppl 4(4):41–51
Tabima DM, Frizzell S, Gladwin MT (2012) Reactive oxygen and nitrogen species in pulmonary hypertension. Free Radic Biol Med 52(9):1970–1986
Takahashi S, Mendelsohn ME (2003) Synergistic activation of endothelial nitric-oxide synthase (eNOS) by HSP90 and Akt: calcium-independent eNOS activation involves formation of an HSP90-Akt-CaM-bound eNOS complex. J Biol Chem 278(33):30821–30827
Tate RM, Morris HG, Schroeder WR, Repine JE (1984) Oxygen metabolites stimulate thromboxane production and vasoconstriction in isolated saline-perfused rabbit lungs. J Clin Invest 74(2):608–613
Teng RJ, Du J, Xu H, Bakhutashvili I, Eis A, Shi Y, Pritchard KA Jr, Konduri GG (2011) Sepiapterin improves angiogenesis of pulmonary artery endothelial cells with in utero pulmonary hypertension by recoupling endothelial nitric oxide synthase. Am J Physiol Lung Cell Mol Physiol 301(3):L334–L345
Teng RJ, Eis A, Bakhutashvili I, Arul N, Konduri GG (2009) Increased superoxide production contributes to the impaired angiogenesis of fetal pulmonary arteries with in utero pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 297(1):L184–L195
Thibeault DW, Rezaiekhaligh M, Mabry S, Beringer T (1991) Prevention of chronic pulmonary oxygen toxicity in young rats with liposome-encapsulated catalase administered intratracheally. Pediatr Pulmonol 11(4):318–327
Traber MG, Stevens JF (2011) Vitamins C and E: beneficial effects from a mechanistic perspective. Free Radic Biol Med 51(5):1000–1013
Tuder RM, Chacon M, Alger L, Wang J, Taraseviciene-Stewart L, Kasahara Y, Cool CD, Bishop AE, Geraci M, Semenza GL, Yacoub M, Polak JM, Voelkel NF (2001) Expression of angiogenesis-related molecules in plexiform lesions in severe pulmonary hypertension: evidence for a process of disordered angiogenesis. J Pathol 195(3):367–374
Ushio-Fukai M, Alexander RW, Akers M, Griendling KK (1998) p38 Mitogen-activated protein kinase is a critical component of the redox-sensitive signaling pathways activated by angiotensin II. Role in vascular smooth muscle cell hypertrophy. J Biol Chem 273(24):15022–15029
Ushio-Fukai M, Alexander RW, Akers M, Yin Q, Fujio Y, Walsh K, Griendling KK (1999) Reactive oxygen species mediate the activation of Akt/protein kinase B by angiotensin II in vascular smooth muscle cells. J Biol Chem 274(32):22699–22704
van Albada ME, Bartelds B, Wijnberg H, Mohaupt S, Dickinson MG, Schoemaker RG, Kooi K, Gerbens F, Berger RM (2010) Gene expression profile in flow-associated pulmonary arterial hypertension with neointimal lesions. Am J Physiol Lung Cell Mol Physiol 298(4):L483–L491
Van Rheen Z, Fattman C, Domarski S, Majka S, Klemm D, Stenmark KR, Nozik-Grayck E (2011) Lung extracellular superoxide dismutase overexpression lessens bleomycin-induced pulmonary hypertension and vascular remodeling. Am J Respir Cell Mol Biol 44(4):500–508
Vander Heiden MG, Cantley LC, Thompson CB (2009) Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science 324(5930):1029–1033
Veit F, Pak O, Egemnazarov B, Roth M, Kosanovic D, Seimetz M, Sommer N, Ghofrani HA, Seeger W, Grimminger F, Brandes RP, Schermuly RT, Weissmann N (2013) Function of NADPH oxidase 1 in pulmonary arterial smooth muscle cells after monocrotaline-induced pulmonary vascular remodeling. Antioxid Redox Signal 19(18):2213–2231
Venditti CP, Harris MC, Huff D, Peterside I, Munson D, Weber HS, Rome J, Kaye EM, Shanske S, Sacconi S, Tay S, DiMauro S, Berry GT (2004) Congenital cardiomyopathy and pulmonary hypertension: another fatal variant of cytochrome-c oxidase deficiency. J Inherit Metab Dis 27(6):735–739
Venema RC, Sayegh HS, Arnal JF, Harrison DG (1995) Role of the enzyme calmodulin-binding domain in membrane association and phospholipid inhibition of endothelial nitric oxide synthase. J Biol Chem 270(24):14705–14711
Villegas LR, Kluck D, Field C, Oberley-Deegan RE, Woods C, Yeager ME, El Kasmi KC, Savani RC, Bowler RP, Nozik-Grayck E (2013) Superoxide dismutase mimetic, MnTE-2-PyP, attenuates chronic hypoxia-induced pulmonary hypertension, pulmonary vascular remodeling, and activation of the NALP3 inflammasome. Antioxid Redox Signal 18(14):1753–1764
Voelkel NF, Bogaard HJ, Al Husseini A, Farkas L, Gomez-Arroyo J, Natarajan R (2013) Antioxidants for the treatment of patients with severe angioproliferative pulmonary hypertension? Antioxid Redox Signal 18(14):1810–1817
Voelkel NF, Vandivier RW, Tuder RM (2006) Vascular endothelial growth factor in the lung. Am J Physiol Lung Cell Mol Physiol 290(2):L209–L221
Walton JP, Julian RJ, Squires EJ (2001) The effects of dietary flax oil and antioxidants on ascites and pulmonary hypertension in broilers using a low temperature model. Br Poultry Sci 42(1):123–129
Wang S, Aurora AB, Johnson BA, Qi X, McAnally J, Hill JA, Richardson JA, Bassel-Duby R, Olson EN (2008) The endothelial-specific microRNA miR-126 governs vascular integrity and angiogenesis. Dev Cell 15(2):261–271
Wang XT, McCullough KD, Wang XJ, Carpenter G, Holbrook NJ (2001) Oxidative stress-induced phospholipase C-γ 1 activation enhances cell survival. J Biol Chem 276(30):28364–28371
Waypa GB, Chandel NS, Schumacker PT (2001) Model for hypoxic pulmonary vasoconstriction involving mitochondrial oxygen sensing. Circ Res 88(12):1259–1266
Waypa GB, Marks JD, Guzy R, Mungai PT, Schriewer J, Dokic D, Schumacker PT (2010) Hypoxia triggers subcellular compartmental redox signaling in vascular smooth muscle cells. Circ Res 106(3):526–535
Waypa GB, Marks JD, Mack MM, Boriboun C, Mungai PT, Schumacker PT (2002) Mitochondrial reactive oxygen species trigger calcium increases during hypoxia in pulmonary arterial myocytes. Circ Res 91(8):719–726
Wedgwood S, Dettman RW, Black SM (2001) ET-1 stimulates pulmonary arterial smooth muscle cell proliferation via induction of reactive oxygen species. Am J Physiol Lung Cell Mol Physiol 281(5):L1058–L1067
Wedgwood S, Devol JM, Grobe A, Benavidez E, Azakie A, Fineman JR, Black SM (2007) Fibroblast growth factor-2 expression is altered in lambs with increased pulmonary blood flow and pulmonary hypertension. Pediatr Res 61(1):32–36
Wedgwood S, Lakshminrusimha S, Czech L, Schumacker PT, Steinhorn RH (2013) Increased p22(phox)/Nox4 expression is involved in remodeling through hydrogen peroxide signaling in experimental persistent pulmonary hypertension of the newborn. Antioxid Redox Signal 18(14):1765–1776
Wedgwood S, Lakshminrusimha S, Fukai T, Russell JA, Schumacker PT, Steinhorn RH (2011) Hydrogen peroxide regulates extracellular superoxide dismutase activity and expression in neonatal pulmonary hypertension. Antioxid Redox Signal 15(6):1497–1506
Wedgwood S, Steinhorn RH, Bunderson M, Wilham J, Lakshminrusimha S, Brennan LA, Black SM (2005) Increased hydrogen peroxide downregulates soluble guanylate cyclase in the lungs of lambs with persistent pulmonary hypertension of the newborn. Am J Physiol Lung Cell Mol Physiol 289(4):L660–L666
Wei HL, Zhang CY, Jin HF, Tang CS, Du JB (2008) Hydrogen sulfide regulates lung tissue-oxidized glutathione and total antioxidant capacity in hypoxic pulmonary hypertensive rats. Acta Pharmacol Sin 29(6):670–679
Wei L, Zhu W, Xia L, Yang Y, Liu H, Shen J, Zhu J, Xu Y, Yang Z, Wang C (2013) Therapeutic effect of eNOS-transfected endothelial progenitor cells on hemodynamic pulmonary arterial hypertension. Hypertens Res 36(5):414–421
Weigand L, Sylvester JT, Shimoda LA (2006) Mechanisms of endothelin-1-induced contraction in pulmonary arteries from chronically hypoxic rats. Am J Physiol Lung Cell Mol Physiol 290(2):L284–L290
Weir EK, Archer SL (2006) Counterpoint: hypoxic pulmonary vasoconstriction is not mediated by increased production of reactive oxygen species. J Appl Physiol 101(3):995–998; discussion 998
Weir EK, Lopez-Barneo J, Buckler KJ, Archer SL (2005) Acute oxygen-sensing mechanisms. N Engl J Med 353(19):2042–2055
Weissmann N, Ebert N, Ahrens M, Ghofrani HA, Schermuly RT, Hanze J, Fink L, Rose F, Conzen J, Seeger W, Grimminger F (2003) Effects of mitochondrial inhibitors and uncouplers on hypoxic vasoconstriction in rabbit lungs. Am J Respir Cell Mol Biol 29(6):721–732
Weissmann N, Zeller S, Schafer RU, Turowski C, Ay M, Quanz K, Ghofrani HA, Schermuly RT, Fink L, Seeger W, Grimminger F (2006) Impact of mitochondria and NADPH oxidases on acute and sustained hypoxic pulmonary vasoconstriction. Am J Respir Cell Mol Biol 34(4):505–513
Wojciak-Stothard B, Torondel B, Tsang LY, Fleming I, Fisslthaler B, Leiper JM, Vallance P (2007) The ADMA/DDAH pathway is a critical regulator of endothelial cell motility. J Cell Sci 120(pt 6):929–942
Wong CM, Bansal G, Pavlickova L, Marcocci L, Suzuki YJ (2013) Reactive oxygen species and antioxidants in pulmonary hypertension. Antioxid Redox Signal 18(14):1789–1796
Wong CM, Preston IR, Hill NS, Suzuki YJ (2012) Iron chelation inhibits the development of pulmonary vascular remodeling. Free Radic Biol Med 53(9):1738–1747
Wright L, Tuder RM, Wang J, Cool CD, Lepley RA, Voelkel NF (1998) 5-Lipoxygenase and 5-lipoxygenase activating protein (FLAP) immunoreactivity in lungs from patients with primary pulmonary hypertension. Am J Respir Crit Care Med 157(1):219–229
Wunderlich C, Schmeisser A, Heerwagen C, Ebner B, Schober K, Braun-Dullaeus RC, Schwencke C, Kasper M, Morawietz H, Strasser RH (2008) Chronic NOS inhibition prevents adverse lung remodeling and pulmonary arterial hypertension in caveolin-1 knockout mice. Pulm Pharmacol Ther 21(3):507–515
Wunderlich C, Schober K, Schmeisser A, Heerwagen C, Tausche AK, Steinbronn N, Brandt A, Kasper M, Schwencke C, Braun-Dullaeus RC, Strasser RH (2008) The adverse cardiopulmonary phenotype of caveolin-1 deficient mice is mediated by a dysfunctional endothelium. J Mol Cell Cardiol 44(5):938–947
Xia N, Daiber A, Habermeier A, Closs EI, Thum T, Spanier G, Lu Q, Oelze M, Torzewski M, Lackner KJ, Munzel T, Forstermann U, Li H (2010) Resveratrol reverses endothelial nitric-oxide synthase uncoupling in apolipoprotein E knockout mice. J Pharmacol Exp Ther 335(1):149–154
Xiang RP, Sun WD, Wang JY, Wang XL (2002) Effect of vitamin C on pulmonary hypertension and muscularisation of pulmonary arterioles in broilers. Br Poultry Sci 43(5 suppl):705–712
Xu D, Guo H, Xu X, Lu Z, Fassett J, Hu X, Xu Y, Tang Q, Hu D, Somani A, Geurts AM, Ostertag E, Bache RJ, Weir EK, Chen Y (2011) Exacerbated pulmonary arterial hypertension and right ventricular hypertrophy in animals with loss of function of extracellular superoxide dismutase. Hypertension 58(2):303–309
Xu W, Kaneko FT, Zheng S, Comhair SA, Janocha AJ, Goggans T, Thunnissen FB, Farver C, Hazen SL, Jennings C, Dweik RA, Arroliga AC, Erzurum SC (2004) Increased arginase II and decreased NO synthesis in endothelial cells of patients with pulmonary arterial hypertension. FASEB J 18(14):1746–1748
Xu W, Koeck T, Lara AR, Neumann D, DiFilippo FP, Koo M, Janocha AJ, Masri FA, Arroliga AC, Jennings C, Dweik RA, Tuder RM, Stuehr DJ, Erzurum SC (2007) Alterations of cellular bioenergetics in pulmonary artery endothelial cells. Proc Natl Acad Sci U S A 104(4):1342–1347
Yang L, Zheng BX, Cheng DY, Su QL, Fan LL, Yang YJ, Mu M, Chen WB (2008) The effect of breviscapine on the pulmonary arterial pressure and the expression of Rho-kinase in pulmonary arterioles of hypoxic rats. Chin J Tuberc Respir Dis 31(11):826–830
Yang Y, Nie W, Yuan J, Zhang B, Wang Z, Wu Z, Guo Y (2010) Genistein activates endothelial nitric oxide synthase in broiler pulmonary arterial endothelial cells by an Akt-dependent mechanism. Exp Mol Med 42(11):768–776
Yang Y, Zhang BK, Liu D, Nie W, Yuan JM, Wang Z, Guo YM (2012) Sodium hydrosulfide prevents hypoxia-induced pulmonary arterial hypertension in broilers. Br Poultry Sci 53(5):608–615
Yetik-Anacak G, Catravas JD (2006) Nitric oxide and the endothelium: history and impact on cardiovascular disease. Vascul Pharmacol 45(5):268–276
Yi ES, Kim H, Ahn H, Strother J, Morris T, Masliah E, Hansen LA, Park K, Friedman PJ (2000) Distribution of obstructive intimal lesions and their cellular phenotypes in chronic pulmonary hypertension. A morphometric and immunohistochemical study. Am J Respir Crit Care Med 162(4 pt 1):1577–1586
Yi SL, Kantores C, Belcastro R, Cabacungan J, Tanswell AK, Jankov RP (2006) 8-Isoprostane-induced endothelin-1 production by infant rat pulmonary artery smooth muscle cells is mediated by Rho-kinase. Free Radic Biol Med 41(6):942–949
Yoshizumi M, Abe J, Haendeler J, Huang Q, Berk BC (2000) Src and Cas mediate JNK activation but not ERK1/2 and p38 kinases by reactive oxygen species. J Biol Chem 275(16):11706–11712
Zemskova M, Sahakian E, Bashkirova S, Lilly M (2008) The PIM1 kinase is a critical component of a survival pathway activated by docetaxel and promotes survival of docetaxel-treated prostate cancer cells. J Biol Chem 283(30):20635–20644
Zernecke A, Bidzhekov K, Noels H, Shagdarsuren E, Gan L, Denecke B, Hristov M, Koppel T, Jahantigh MN, Lutgens E, Wang S, Olson EN, Schober A, Weber C (2009) Delivery of microRNA-126 by apoptotic bodies induces CXCL12-dependent vascular protection. Sci Signal 2(100):ra81
Zhang E, Jiang B, Yokochi A, Maruyama J, Mitani Y, Ma N, Maruyama K (2010) Effect of all-trans-retinoic acid on the development of chronic hypoxia-induced pulmonary hypertension. Circ J 74(8):1696–1703
Zhang TT, Cui B, Dai DZ, Su W (2005) CPU 86017, p-chlorobenzyltetrahydroberberine chloride, attenuates monocrotaline-induced pulmonary hypertension by suppressing endothelin pathway. Acta Pharmacol Sin 26(11):1309–1316
Zhao W, Zhang J, Lu Y, Wang R (2001) The vasorelaxant effect of H2S as a novel endogenous gaseous K(ATP) channel opener. EMBO J 20(21):6008–6016
Zhao YD, Courtman DW, Deng Y, Kugathasan L, Zhang Q, Stewart DJ (2005) Rescue of monocrotaline-induced pulmonary arterial hypertension using bone marrow-derived endothelial-like progenitor cells: efficacy of combined cell and eNOS gene therapy in established disease. Circ Res 96(4):442–450
Zhao YY, Liu Y, Stan RV, Fan L, Gu Y, Dalton N, Chu PH, Peterson K, Ross J Jr, Chien KR (2002) Defects in caveolin-1 cause dilated cardiomyopathy and pulmonary hypertension in knockout mice. Proc Natl Acad Sci U S A 99(17):11375–11380
Zhao YY, Malik AB (2009) A novel insight into the mechanism of pulmonary hypertension involving caveolin-1 deficiency and endothelial nitric oxide synthase activation. Trends Cardiovasc Med 19(7):238–242
Zhao YY, Zhao YD, Mirza MK, Huang JH, Potula HH, Vogel SM, Brovkovych V, Yuan JX, Wharton J, Malik AB (2009) Persistent eNOS activation secondary to caveolin-1 deficiency induces pulmonary hypertension in mice and humans through PKG nitration. J Clin Invest 119(7):2009–2018
Zhou Z, Song R, Fattman CL, Greenhill S, Alber S, Oury TD, Choi AM, Morse D (2005) Carbon monoxide suppresses bleomycin-induced lung fibrosis. Am J Pathol 166(1):27–37
Zinkevich NS, Gutterman DD (2011) ROS-induced ROS release in vascular biology: redox-redox signaling. Am J Physiol Heart Circ Physiol 301(3):H647–H653
Zou MH, Cohen R, Ullrich V (2004) Peroxynitrite and vascular endothelial dysfunction in diabetes mellitus. Endothelium 11(2):89–97
Zuckerbraun BS, Chin BY, Bilban M, d’Avila JC, Rao J, Billiar TR, Otterbein LE (2007) Carbon monoxide signals via inhibition of cytochrome c oxidase and generation of mitochondrial reactive oxygen species. FASEB J 21(4):1099–1106
Zuckerbraun BS, Chin BY, Wegiel B, Billiar TR, Czsimadia E, Rao J, Shimoda L, Ifedigbo E, Kanno S, Otterbein LE (2006) Carbon monoxide reverses established pulmonary hypertension. J Exp Med 203(9):2109–2119
Zuckerbraun BS, Stoyanovsky DA, Sengupta R, Shapiro RA, Ozanich BA, Rao J, Barbato JE, Tzeng E (2007) Nitric oxide-induced inhibition of smooth muscle cell proliferation involves S-nitrosation and inactivation of RhoA. Am J Physiol Cell Physiol 292(2):C824–C831
Zulueta JJ, Yu FS, Hertig IA, Thannickal VJ, Hassoun PM (1995) Release of hydrogen peroxide in response to hypoxia-reoxygenation: role of an NAD(P)H oxidase-like enzyme in endothelial cell plasma membrane. Am J Respir Cell Mol Biol 12(1):41–49
Conflict of Interest
The authors report no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Chrobak, I., Haeger, C.M., Maracle, M.E., Fredenburgh, L.E. (2014). Pulmonary Arterial Hypertension and Oxidative Stress. In: Ganguly, N., Jindal, S., Biswal, S., Barnes, P., Pawankar, R. (eds) Studies on Respiratory Disorders. Oxidative Stress in Applied Basic Research and Clinical Practice. Humana Press, New York, NY. https://doi.org/10.1007/978-1-4939-0497-6_15
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0497-6_15
Published:
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-4939-0496-9
Online ISBN: 978-1-4939-0497-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)