
Abstract
Squamous cell carcinoma of the penis (SCCP) has behaved similarly to squamous cell carcinoma in other parts of the skin. Stage is important in the treatment of primary lesion. Pathological factors with a known prognostic value, other than lymph node metastasis, are tumor thickness, grade, histological type, lymphovascular embolization, and stage. The histological grade of penile carcinoma, including SCCP usual type, should attend the protocol based on the American Joint Committee on Cancer.
Apart from the carcinogens, oncoviruses such as human papillomavirus (HPV) and Epstein-Barr virus (EBV) can help to cause penile cancers. The mechanism by which HPV promotes cancer is not affecting the genes. HPV encodes for E6 and E7 proteins that are able to bind to two important tumor suppressor proteins, p53 and pRB, respectively, inactivating them.
By conventional cytogenetics, only four karyotypes were described for penile carcinoma. The rarity of karyotype description is due to technical difficulties related to the low mitotic index, contamination of primary cultures, and the occurrence of large areas of necrosis in the tumor. The frequency of DNA aneuploidy showed correlation with histological type of invasive squamous cell carcinoma of the penis. Epidermoid tumors of various organs can be originated from similar genetic alterations. MYC numerical aberrations and c-MYC protein expression were determined and correlated with the clinicopathological parameters and the HPV infection status of the patients. A significant association between MYC gains and tumor progression and poor outcome was demonstrated. These findings were independent of HPV infection. Protein c-MYC expression was increased in samples with HPV infection, probably reflecting direct activation of MYC. A gain in the region 5p15 appears very interesting, because the gene hTERT was mapped on this region. This gene codes for the major protein of the catalytic site of telomerase, the enzyme that stabilizes the telomeres of chromosomes.
Disruption of p53 function is very a common genetic event in many cancers, and there are many ways to cause it. The prognostic significance of p53, Ki-67, PCNA, E-cadherin, and Matrix metalloproteases-9 (MMP-9) was evaluated in SSCP tumors. Tumor embolization and the expression of p53 are independent predictors of metastasis. The comparison of the prognostic value of PCNA and Ki-67 revealed that there was a correlation between the expression of both and the presence of lymph node metastasis.
Telomerase activity was measured in samples of SSCP by the Telomeric Repeat Amplification Protocol (TRAP), a PCR-based assay with fluorescence label. In some patients, it was also possible to measure the activity of telomerase in the region adjacent to the tumor, either skin or corpus cavernous, which were free of tumor cells according to histopathological analysis. These results indicated that telomerase is reactivated either in normal tissues or adjacent tissues of SCCP.
Expression of two members of Bcl-2 family (the antiapoptotic Bcl-2 and the proapoptotic Bax) was analyzed in 16 SCCP using Western blot. Bcl-2 and Bax were completely imbalanced when the tumor, adjacent to either skin or corpus cavernous, was compared in the same way. This means that the adjacent tissues are at least under the influence of the tumor.
The mutations in RAS and PIK3CA were mutually exclusive, suggesting that deregulation of either the phosphatidylinositol 3-kinase or ras pathway would be sufficient for the development and progression of penile carcinoma.
In general, the studies that have searched for DNA methylation of tumor suppressor genes in SSCP also addressed other questions related to gene expression control (in special HPV infection), reflecting the complexity of this issue. Publications analyzed DNA methylation status of several gene promoters.
Proteins from plasma of 36 healthy subjects (controls) were compared to 25 plasmas from patients with SCCP. Two peptides were identified by an MALDI-TOF-TOF as fragments of C3 and C4a/b complement proteins. The conclusion was that fragments C3 and C4 a/b are less expressed in comparison with healthy subjects as the disease progresses. TA-4 antigen, also known as SSC antigen, was originally isolated from patients showing squamous cell carcinoma of the uterine cervix. Later it was shown that TA-4 values were elevated in serum of metastatic SSCP patients.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Penile Cancer
- Telomeric Repeat Amplification Protocol
- Verrucous Carcinoma
- Telomeric Repeat Amplification Protocol
- Penile Carcinoma
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Pathology
Squamous cell carcinoma of the penis (SCCP) has behaved similarly to squamous cell carcinoma in other parts of the skin. This tumor represents the most common malignant neoplasm that can be developed anywhere on the penis, affecting shaft and distal segment as glans, coronal sulcus, and foreskin. That distal sites shelter SCCP most frequently (Fig. 4.1).

Penile cancer. Exophytic lesion
Stage is important in the treatment of primary lesion. In a study with 196 patients, a local extension of the primary tumor into corpora cavernosa was found in 44.9 % of patients. The corpus spongiosum and urethra were involved in 21.4 and 35.2 % of cases, respectively [1].
Pathological factors with a known prognostic value, other than lymph node metastasis, are tumor thickness, grade, histological type, lymphovascular embolization, and stage [2, 3].
The rate of depth invasion is significantly high when the thickness is more than 5 mm. The histological grade of penile carcinoma, including SCCP usual type, should attend the protocol based on the American Joint Committee on Cancer, TNM, 7th edition [4]:
-
(G1) Well-differentiated carcinoma, tumors with a minimal deviation from the morphology of normal/hyperplastic squamous epithelium (Fig. 4.2)
Fig. 4.2 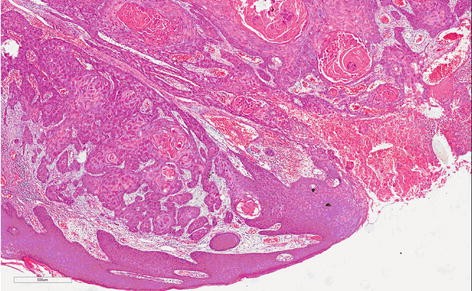
Usual grade 1, well-differentiated SCC. Proliferation of mature epithelial cells with basal atypia forming nets. Abundant centralized keratin pearl
-
(G2) Moderately differentiated carcinoma constitutes the great part of the cases; tumors show a more disorganized growth as compared to grade 1 lesions, increased nucleus-cytoplasm ratio, evident mitoses, and, although present, less prominent keratinization (Fig. 4.3)
Fig. 4.3 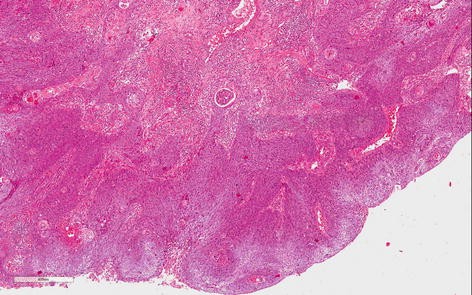
Usual grade 2, moderately differentiated SCC. Less keratin and cell differentiation than grade 1. Irregular infiltrative borders, nuclear atypia, evident mitosis
-
(G3) Poorly differentiated carcinomas are tumors showing any proportion of anaplastic cells, identified as solid sheets or irregular small aggregates, cords, or nests of cells with little or no keratinization, high nucleus-cytoplasm ratio, thick nuclear membranes, nuclear pleomorphism, clumped chromatin, prominent nucleoli, and numerous mitoses (Fig. 4.4)
Fig. 4.4 
(a) Usual grade 3, poorly differentiated SCC. Prominent stromal desmoplastic tissue involved solids nets and irregular small aggregates of anaplastic cells. Individual keratinized cells are present. (b) Usual grade 3, poorly differentiated SCC. Sheets, cords, and small aggregates of anaplastic squamous cells, isolated keratinized cells, nuclear pleomorphism, hyperchromatin, prominent nucleoli, and numerous mitoses



A tumor should be graded according to the least differentiated component. Any proportion of grade 3 should be distinguished in the description. Patients with well-differentiated carcinoma have a higher 10-year survival rate than those with moderately and poorly differentiated carcinoma (P < 0.0001 and P = 0.006) [5].
Lymphovascular embolization and absent koilocytosis have proved to be independent prognostic factors for the risk of lymphatic metastasis. Patients with koilocytosis and without lymphovascular embolization had better 5-year survival [1].
SCCP can be seen as usual SCCP type or constituting the variant forms or subtypes sometimes associated with HPV. Basically the grossly usual SCCP shows itself either as a flat, an endophytic, or as an exophytic tumor (cauliflower appearance), white-gray and firm tumor with necrosis foci. Microscopically it consists of squamous cell proliferation that may infiltrate superficially or profoundly penile tissues and/or projecting outside itself with variable degrees of cytological atypia, mitotic figures, and keratin that can be seen as mild or prominent keratinized cell [6, 7].
Variations of squamous cell carcinoma or subtypes can be seen forming two groups: high-grade and low-grade groups. The high-grade tumors (basaloid and sarcomatoid) frequently are associated with deeper invasion, recurrence of tumors, lymph node metastasis, and significant mortality rate [8]. Low-grade variants (papillary, warty, and verrucous) have mild to moderate morbidity features and better survive rate [9]. The following are a short description of them:
Basaloid carcinoma (BC) is a high-grade subtype associated to HPV and can be seen as flat, endophytic, or papillar [10]. Macroscopic features are ulcerated lesion, flat or slightly elevated, and firm. Microscopy is infiltrated tumor made of cell nests with few cytoplasm and basophilic nuclei, centered by comedonecrosis. Nucleus is oval or round, pleomorphic and hyperchromatic, with inconspicuous nucleoli and numerous mitoses (Fig. 4.5).


(a) High-grade SCC, basaloid subtype (panoramic vision). Endophytic infiltrative tumor of basaloid cells. (b) High-grade SCC, basaloid variant group. Note irregularity of the tumor nets with ragged basal membrane showing its aggressiveness. Cells present poor cytoplasm, great oval or round basophilic nuclei with prominent nucleolus, and atypical mitoses. (c) Basaloid SCC subtype. Tumor shows papillary appearance. Comedonecrosis involved by basaloid cells
Sarcomatoid carcinoma (SC) is a primary spindle-cell squamous carcinoma, rare in penis, similar to a sarcomatous tumor, aggressive with deep structural infiltration, poor prognosis, associated with lymphatic, and hematogenous spread (Fig. 4.6). Metastatic disease develops in a high percentage of cases. Distant tumor metastases occur mainly in lung, skin, bone, and pericardium and pleura [11, 12].


(a) Spindle-cell carcinoma, high-grade group. Ulcerated tumor presents fusiform cells similar to those present in other sarcomatous tumors. (b and c) Sarcomatoid SCC. Groups of squamous and isolated brown cells were stained by 34BE12 keratin
Warty carcinoma (WC) is a morphologically distinct verruciformis tumor with features of HPV-related lesions [13]. HPV attacks the squamous epithelium and produces nuclear atypia, binucleation, and koilocytosis (identified by a large halo around cellular nuclei) (Fig. 4.7).

(a) Warty carcinoma, low-grade variant. The keratin fills up the space between acanthotics cells columns with long and large papillae. (b) HPV-related warty carcinoma exhibiting darker band of basaloid tumor cells deep in the tumor and present area with clear cells and koilocytosis
Papillary carcinoma (PC) is a papillary well-differentiated carcinoma which can invade stromal tissue until deep structures but with rare lymph node involvement. The prognosis is good and tumor is associated with lichen sclerosus [9]. Grossly it is an exophytic white-gray and firm tumor. Microscopy is complex and simple papillae with fibrovascular core and hyperkeratosis.
Verrucous carcinoma (VC) is generally a large lesion (average 4 cm) with exophytic papillary growth, frequently softy, ulcerated sometimes purulent, and foul smelling tumor. Tumor can be seen anywhere on the penis, frequently on the glans and foreskin. A specific etiologic factor is not described. Microscopically, the presence of well-differentiated characteristics frequently makes hard differential diagnostics, mainly with condyloma accuminatum and well-differentiated SCC. Superficially, hyperkeratosis, acanthosis, and papillomatosis are seen, and it excavates through the normal tissue and slowly invades continuous structures (Fig. 4.8). Regional lymph node metastases are rare and distant metastases have not been reported [14].

(a) Verrucous carcinoma, low-grade variant. Tumor not associated with HPV represented by well-differentiated squamous cells with thin and long papillae containing fibrovascular cores and hyperkeratosis. (b) Verrucous carcinoma, low-grade variant. The round tumor board of squamous cell is present in stromal tissue configuring nest with single basal cells involved by inflammatory infiltrated. Inside keratinized material
Genetics
Introduction
Cancer is a disease caused by our own genes’ deregulation. Cancer cells divide indefinitely as a consequence of a deep genetic expression turning. This occurs step by step or mutation by mutation until the cell reaches the point of no return, ignoring the cell cycle checkpoints. Environmental risk factors causing mutagenesis and the failure of the mechanisms of genome repair combine to promote mutations in the key genes that control the cell cycle progress.
The key genes in the carcinogenesis process are the proto-oncogenes and the tumor suppressor genes. In normal cells, proto-oncogenes are responsible for promoting the cell growth. When altered or mutated, they become oncogenes and then can contribute to indefinitely cell division. The tumor suppressor genes that are normally present in our cells can lose their capacity of controlling the processes of cell growth and cell death (called apoptosis) when they are mutated or deleted.
Damage in the key genes that control the cell cycle is caused by many factors. Carcinogens are a class of substances that are directly responsible for promoting cancer. Tobacco, asbestos, arsenic, radiation such as gamma and x-rays, the sun (UV rays), and compounds in car exhaust fumes are all examples of carcinogens [15–18]. When our bodies are exposed to carcinogens, free radicals are formed that try to steal electrons from other molecules in the body. These free radicals damage cells and affect their ability to function normally.
Apart from the carcinogens, oncoviruses such as human papillomavirus (HPV) and Epstein-Barr virus (EBV) can help to cause penile cancers [19, 20]. The mechanism by which HPV promotes cancer is not affecting the genes. HPV encodes for E6 and E7 proteins that are able to bind to two important tumor suppressor proteins, p53 and pRB, respectively, inactivating them [21]. EBV is widely distributed in human population; however, the exact role of EBV in the development of penile cancer is not understood. A possible cooperation between EBV and HPV in the process of penile carcinogenesis should be considered [20].
Cytogenetics and Flow Cytometry Findings
Genes made of DNA are organized in a complex nuclear structure called chromosomes. A normal human cell contains 46 chromosomes. In cancer cells, chromosome rearrangements and the alteration of chromosome number can be detected with the application of cytogenetic techniques. Chromosomes in metaphase can be fixed on slides and can be observed under a microscope. The karyotype is the picture of the chromosomes from one metaphase that is arranged according to the standard classification.
In contrast to most tumors, publications about karyotype alterations in squamous cell carcinoma of the penis (SSCP) are uncommon. By conventional cytogenetics only four karyotypes were described for penile carcinoma. The rarity of karyotype description is due to technical difficulties related to the low mitotic index, contamination of primary cultures, and the occurrence of large areas of necrosis in the tumor.
The first SSCP karyotype description [22] was from a Chinese patient showing moderately differentiated SSCP (stage II). Several inguinal lymph nodes were palpable. Thirty metaphases showed the stemline karyotype 46,XY,del(2)(q33q36),der(4)t(4;?)(p16;?),der(5;15)(q10;q10),der(8)t(8;?13)(q21;?),-13,- 13,-15,+3mar. Twelve cells had the stemline pattern with additional chromosome aberrations. Chromosomes 17, 22, and Y were usually lost, whereas chromosome 14 was frequently trisomic. Five to eight markers were observed in each cell of this population. Eight polyploid cells with poor chromosome spreading were also observed. The other three described karyotypes were from Brazilian cases. The next and second karyotype description [23] was obtained from an SSCP patient who presents an advanced poorly differentiated invasive carcinoma. Cytogenetic analysis of 11 cells obtained from fresh biopsy revealed a complex karyotype nearly tetraploid: 88, XY, + der. X, t (X; ?), (q28; ?), + del. (1), (p36), + 1, + 1, + 1, + 2, + 2, + 3, + 3, + 4, + 5, + 5, + 5, + 9, + 9, + 10, + 10, + 11, + 11, + 12, + 12, + 13, + 14, + 14, + 15, + 15, + 15, + der. 16, t (1; 16), (q24; p12), + 16, + 17, + 17, + 17, + 18, + 18, + 19, + 19, + 20, + 20, + 21, + 21, + mar 2, + mar 2 (Fig. 4.9). Polyploidy was confirmed by flow cytometry (Fig. 4.10). Besides the polyploidy, translocation involving chromosomes 1 and 16 and the appearance of additional genetic material on the X chromosome and isochromosome of the short arm of chromosome 10 were remarkable.

Complete karyotype from the tumoral cells of a patient with poorly differentiated penile carcinoma, including a partial karyotype showing an isochromosome i (10) (q10) (From Ornellas et al. [23])

Distribution pattern of the nuclear DNA content (near-tetraploid tumor). (a) Gated events displayed in identified singlet nucleus populations. (b) Singlet nucleus fluorescence intensity showing a near-tetraploid population and the diploid reference cells (From Ornellas et al. [23])
In contrast, the karyotypes of two early-stage SSCP patients showed no polyploidy [24]. One patient, with clinical stage T2N2MX, presented a moderately differentiated carcinoma of the penis, with a DNA pattern diploid. Cytogenetic analysis of 43 cells showed no cytogenetic alteration. The other patient, with clinical stage T3N1MX, presented also a moderately differentiated penile carcinoma. Cytogenetic analysis of 11 cells showed an altered karyotype (49,XY, dup(1)(q21q32), i(1)(q10), -3, add(11)(q23), del (12)(p12),+i(18)(q10), +3 mar) with a DNA pattern hyperdiploid (Figs. 4.11 and 4.12). Although few, these karyotype descriptions suggest the possibility of the patients’ present different tumors with different behaviors and that polyploidy could be a characteristic of advanced SSCP. Patient with normal karyotype had probably submicroscopic changes responsible for tumor development. In the future, a combination of cytogenetic, molecular, and histopathological stage and grade analyses will contribute to decisions on the classification of a particular solid tumor, leading to better predictive and prognostic information.

Distribution pattern of nuclear DNA content (aneuploid tumor). (a, b) Hyperdiploid cell line was identified. (c) Singlet nuclear fluorescence intensity showing a hyperdiploid population with DNA index of 1.15 and the diploid reference cells (c, From Ornellas et al. [24])

Hyperdiploid moderately differentiated squamous cell carcinoma of the penis with chromosomal alterations. G-banded karyotype showed 49,XY, dup(1)(q21q32), i(1)(q10), 23,add(11)(q23), del(12)(p12),1i(18)(q10),13mar. Primary culture revealed 11 metaphases (From Ornellas et al. [24])
Flow cytometry is a technique for counting and examining microscopic particles, such as cells and chromosomes, by suspending them in a stream of fluid and passing them by an electronic detection apparatus. A chromosome counting performed by flow cytometry [25] from 90 SSCP patients showed that ploidy in these tumors is proportional to the degree of cellular differentiation. The frequency of DNA aneuploidy showed correlation with histological type of invasive squamous cell carcinoma of the penis. Preliminary analysis of these cases suggested that patients with high DNA index may be at increased risk of metastatic involvement and highlights that aneuploidy seems to be a risk factor for metastatic dissemination [25].
An original molecular cytogenetics study of penile carcinoma [26] was performed by comparative genomic hybridization (CGH). The CGH technique has a great advantage over conventional cytogenetics since it is not necessary to make the primary culture of tumor cells for obtaining slides with chromosome preparations. Only DNA extraction from the tissues is necessary. This technique generates a genomic map that leads to the discovery of chromosomal regions greatly amplified in tumors as well as regions in which there were large deletions. The procedure requires different fluorochromes for labeling of DNA that was extracted from a tumor (tumor DNA), and DNA was extracted from one tissue tumor-free (normal DNA). The tumor and normal DNAs compete for hybridization in normal chromosomes, and regions with large chromosomal amplifications or deletions in chromosomes are distinguished by a computer program associated with a fluorescence microscope according to the difference of intensity of labeled tumor and normal DNA which hybridized to normal chromosomes.
DNA samples from 26 SSCP cases were assayed by CGH; six tumors were well-differentiated invasive tumors and the other 20 tumors moderately differentiated. The changes observed were similar to those described in other squamous cell carcinomas, such as oral and nasopharynx. This finding indicates that epidermoid tumors of various organs can be originated from similar genetic alterations. The regions of gene amplification observed most common were 8q24, 16p11-12, 20q11-13, 22q, 19q13, and 5p15, and the regions with the most frequent deletions were 13q21-22, 4q21-23, and along the X chromosome. In the region 8q24, the proto-oncogene MYC that encodes for transcription factor showing a helix-loop-helix leucine zipper protein domain has been mapped. The friendly MYC regulates expression of numerous target genes that control key cellular functions, including cell growth and cell cycle progression. MYC also has a critical role in DNA replication. Any kind of deregulation on MYC leads to constitutive MYC activity promotes carcinogenesis.
In 79 cases of SSCP including 11 in situ and 68 invasive carcinomas, MYC numerical aberrations and c-MYC protein expression were determined and correlated with the clinicopathological parameters and the HPV infection status of the patients [27]. The MYC cytogenetic profile was evaluated by fluorescence in situ hybridization (FISH) and c-MYC protein by immunohistochemistry (IHC). HPV was detected by polymerase chain reaction amplification (PCR). MYC gains were found to increase gradually as penile squamous cell carcinoma progresses from in situ to invasive. A significant association between MYC gains and tumor progression and poor outcome was demonstrated (p < 0.05). These findings were independent of HPV infection. Protein c-MYC expression was increased in samples with HPV infection, probably reflecting direct activation of MYC.
Gain in the region 5p15 appears very interesting, because the gene hTERT was mapped on this region. This gene codes for the major protein of the catalytic site of telomerase, the enzyme that stabilizes the telomeres of chromosomes. The stabilization of the end of the chromosomes (telomeres) is critical for promoting immortality. This result can be correlated with the study of analysis of telomerase activity in 51 samples of penile cancer [28]. In addition, gain in region 5p15 was also found in 3/7 men with cutaneous squamous cell carcinoma that were studied by array CGH [29], suggesting that this genetic event could also occur within this histological type.
Tissue and Molecular Alterations
TP53 Tumor Suppressor Gene (p53 Protein)
In an editorial of “Molecule of the Year,” p53 was described as: “The molecule p53 is a good guy when it is functioning correctly” [30]. This interpretation suggests that the normal p53 plays a role in controlling cell growth, and when mutated, the surveillance capability of the protein is eliminated and cancer can grow.
When discovered, [31] p53 was just a cellular partner bond to the simian virus 40 large T antigen. After the cloning of the gene TP53, p53 was dismissed as an oncogenic protein and recognized as a tumor suppressor that is very frequently mutated in human cancer. Since then more functions for p53 have been revealed [32]. It acts as a transcription factor induced by stress/DNA damage, promoting cell cycle arrest, apoptosis, and senescence, and also regulates cytokines that are required for embryo implantation and metabolic pathways. In addition, p53 promotes oxidative phosphorylation and dampens glycolysis in cells [33] and has a key role in regulating cell growth and autophagy, thereby helping to coordinate the cell’s response to nutrient starvation. An altered metabolism can contribute to malignant transformation as cancer cells [34].
Disruption of p53 function is a very common genetic event in many cancers, and there are many ways to cause it. The most common type of mutation causing inactivation of p53 is the missense mutation in the binding domain [35]. However, the SCCP might face another reality due to the common HPV infection [19, 20]. HPV encodes for E6 and E7 proteins that bind to p53 and pRb, respectively, leading to uncontrolled cell division and reduced apoptosis. In this situation, in spite of gene TP53 being intact, p53 is blocked by E6.
One study [36] with Chinese patients analyzed p53 accumulation by immunohistochemistry in a series of 42 primary penile carcinomas (seven verrucous carcinomas, 14 well-differentiated, 15 moderately differentiated, and six poorly differentiated squamous cell carcinomas) using the p53 protein-specific mouse monoclonal antibody on paraffin sections. The mutant p53 protein frequently accumulates within the cell and can be viewed on fixed tissues by immunohistochemistry with the application of specific antibodies. However, the determination of specific mutations must be detected by DNA sequencing. The p53 protein was detected in 40 % (17 cases) of the tumors. The p53 staining was not observed in six cases of penile warts nor in seven cases of verrucous carcinomas. Positive p53 staining was identified only in the less differentiated tumor cells in the periphery of the tumor cell nests in all the cases. The noninvasive dysplastic epithelium next to the tumors could also be positive for p53 protein. Furthermore, 100 % of the human papillomavirus (HPV)-positive cases showed positive p53 staining. The authors concluded that p53 accumulation is present in penile squamous cell carcinomas and adjacent noninvasive tumor cells. In agreement, another immunohistochemistry study identified the accumulation of p53 in two cases of HPV-positive (6 or 11) invasive carcinoma [37]. One of the cases carried a mutation in TP53 revealed by DNA sequencing. In contrast, another study did not detect the accumulation of p53 in 25 cases of carcinoma in situ [38]. Therefore, according to these reports, it seems that mutant p53 could play a role in the progression of malignancy into invasion, but this remains controversial. Biopsies of penile lesions were obtained for diagnostic purposes from 13 with 1 to 3 therapy-resistant genital warts or intraepithelial neoplasias. In addition, 4 archival specimens of SSCP were obtained. In the specimens, presence of HPV DNA was assayed by in situ hybridization and PCR analysis, and p53 accumulation was determined by immunohistochemistry. At the molecular level mutations in the DNA binding domain (exons 4–8) of TP53 were assayed in gel by single-strand conformation polymorphism (SSCP) after amplification by polymerase chain reaction (PCR). Band shifts were sequenced to detect possible mutations [39]. No correlation between p53 accumulation and HPV status was found. No mutations in the binding domain of TP53 were found in any of the lesions. The authors concluded that accumulation of p53 did not indicate existence of TP53 mutation in male genital warts, premalignant lesions, or malignant squamous cell carcinomas.
The accumulation of p53 and p21 (another tumor suppressor protein) in 49 SSCP cases was investigated by immunohistochemistry [40]. The accumulation of p21 and p53 was noted in 40 and 89 %, respectively, of the 47 patients with primary penile carcinoma with squamous differentiation. Positive p21 and p53 expression was also seen in two cases of Paget disease. Staining for p21 was often weak and was found in the suprabasal region of carcinomas with squamous differentiation, while p53 expression was seen in the basal region of squamous cell carcinomas. Preinvasive lesions also showed p21 and p53 expression. An inverse correlation between p53 and p21 expression (p53(+)/p21(−) or p53(−)/p21(+)) was noted in half of the squamous cell carcinomas, 4 of 5 verrucous carcinomas, 2 of 3 basaloid squamous cell carcinomas, and 1 spindle-cell carcinoma. The other cases did not show this correlation. Therefore, p21 and p53 expression seems to be independent in SCCP. The relationship between expression-positive/expression-negative p53 and p21 did not show a direct correlation with histological subtypes and staging. However, a strong association between positivity for HPV16 and p21 was found.
Alterations in p53 protein were also identified in 22 of 63 (35 %) patients with epidermoid tumors and invasive penile stage pT2-4 N1-3 MX [41]. The presence or absence of p53 in the nucleus has been correlated in primary lesions and nodal metastasis in 20 patients. Of these 20 patients (90 %), 18 agreed on the levels of p53 expression in primary lesions and nodal metastasis. Two patients have only p53 expression in nodal metastasis.
The impact of p53 as a prognostic marker was investigated in 82 SSCP patients undergoing penile amputation and bilateral inguinal lymphadenectomy [2]. Immunoreactivity of p53 was studied with other clinicopathological parameters, and HPV DNA was detected by PCR using generic primers. Nuclear accumulation of p53 was detected in 34 of 82 samples (41.5 %). Clinical lymph node N stage, lymphatic and venous embolization by neoplastic cells, and p53 positivity were significantly associated with lymph node metastasis. Multivariate analysis revealed that only lymphatic embolization and p53 positivity were independent factors for lymph node metastasis. Patients with negative p53 had significantly better 5- and 10-year overall survival than those in whom tumors stained positive for p53. When tumors were p53 positive and HPV DNA positive, overall survival was worse.
The prognostic significance of p53, Ki-67, E-cadherin, and Matrix metalloproteases-9 (MMP-9) was evaluated in SSCP tumors of 73 Chinese patients who have penile amputation and regional lymphadenectomy [42]. The expression of molecular markers was determined by immunohistochemistry. By multivariate analysis, tumor embolization and the expression of p53 were independent predictors of metastasis. In stage T1 tumors, high expression of p53 was significantly associated with metastasis and poor survival.
Telomerase Activity
A telomere is the “cap” at the end of chromosomes. It is composed of repetitive DNA sequences and specialized proteins that protect the end of the chromosome from degradation of genes near the ends of chromosomes. The loss of telomeric DNA sequences that occur in each cell division rules the process of cell aging or senescence. Very short telomeres trigger the cell death process, so that they act as a “molecular clock” that determines the lifetime of a cell. Cell immortalization depends on stopping telomeric DNA degradation by the reactivation of telomerase that adds DNA sequence repeats (“TTAGGG” in all vertebrates) to the 3’ end of DNA strands in the telomere.
Telomerase, a ribonucleoprotein enzyme, carries its own RNA molecule, which is used as a template for elongating telomeres, which are shortened after each replication cycle. The activity mode of telomerase resembles the activity of the reverse transcriptase enzyme of the retrovirus. The existence of a compensatory mechanism for telomere shortening was first predicted by biologist Alexey Olovnikov in 1973 [43] who also suggested the telomere hypothesis of aging and the telomere’s connections to cancer. Telomerase was discovered by Carol W. Greider and Elizabeth Blackburn in 1984 in the ciliate Tetrahymena [44]. In humans, telomerase activity usually is detected during embryogenesis, in germ cells, stem cells, and B and T lymphocytes.
Telomerase activity was measured in 48 samples of SSCP and three penile verrucous carcinomas [28] by the Telomeric Repeat Amplification Protocol (TRAP), a PCR-based assay with fluorescence label. In some patients, it was also possible to measure the activity of telomerase in the region adjacent to the tumor, either skin or corpus cavernous, which were free of tumor cells according to histopathological analysis. Among the specimens of invasive carcinomas, 41/48 (85.4 %) showed positive telomerase activity, and three samples of verrucous carcinoma were also positive. The results of adjacent tissues were more surprising; 9/11 (81.8 %) of the adjacent skin samples and 8/10 (80 %) of corpus cavernous adjacent samples also were positive for telomerase activity. As controls, five samples of skin and corpus cavernous of prostate cancer patients were tested negative for telomerase activity. These results indicated that telomerase was reactivated in normal tissues or adjacent tissues of SCCP. This could be happening due to angiogenesis/invasion or inflammation next to the tumor. The original TRAP assay [45] used radioactivity labeling for the detection of amplified telomeric DNA sequences that were previously polymerized by a telomerase extract from the tissues. In addition, the activity of telomerase was detected in other case, a 46-year-old man with a penile giant condyloma acuminatum [46]. This information may be valuable for evaluating the degree of malignancy of giant condyloma acuminatum and in obtaining a differential diagnosis between the benign and malignant cases.
Bax and Bcl-2 Apoptotic Proteins
Apoptosis or programmed cell death is a physiological mechanism, characterized by specific morphological and biochemical changes such as cell shrinkage, chromatin condensation, protein cleavage, DNA breakdown, and phagocytosis. Biochemical events lead to characteristic cell changes (morphology) and death. Many proteins have been identified to play a role in apoptosis.
Bcl-2 family consists of approximately 15 members, some of which are antiapoptotic while others are proapoptotic. The first Bcl-2 gene was identified because of its involvement in B-cell malignancies, and it is located on chromosome segment 18q21.3; Bcl-2 stands for B-cell lymphoma/leukemia-2 gene [47]. The Bcl-2 family of proteins can be identified by the presence of the domains BH1 to BH4. Most antiapoptotic members contain, at least, the BH1 and BH2 domains, while the proapoptotic Bcl-2 family members have the four BH domains.
Expression of two members of Bcl-2 family (the antiapoptotic Bcl-2 and the proapoptotic Bax) was analyzed in 16 SCCP (tumor-free adjacent skin tissue and corpus cavernous) comparing with five controls (skin and corpus cavernous) using Western blot (a technique for identifying a particular protein using antibodies after electrophoretic separation in a gel and transfer to a membrane). It was observed that the proteins Bcl-2 and Bax showed a clear homogeneous expression pattern in normal skin and corpus cavernous; Bcl-2 expression was higher than Bax’s. However, Bcl-2 and Bax were completely imbalanced when the tumor, adjacent either skin or corpus cavernous, was compared in the same way. This means that the adjacent tissues are at least under the influence of the tumor. The Bcl-2/Bax results are in agreement with the results of the analysis of telomerase activity [28].
Oncogenes
Alterations in the cellular growing signaling pathways downstream of growth receptors caused by oncogenes are one of the most common events in various cancers. This, in part, is because these receptors control two major signaling pathways (RAS and PI3K pathways). RAS is a family of related proteins with GTPase activity, which are involved in transmitting signals within cells (cellular signal transduction). When RAS activity is under control, cell growth and division occur normally. Mutations in RAS that prevents GTP hydrolysis, let ras protein on permanently, resulting in overactivity that can ultimately lead to cancer. RAS is the most common oncogene in human cancer and was the first to be discovered in the human genome in the early 1980s [48].
Mutations in RAS leading to overexpression are found in 20–25 % of all human tumors and up to 90 % in certain types of cancer. Yet, only one study was published reporting mutations of RAS family members in 28 SSCP cases [49]. In this study, single-stranded conformational and direct DNA sequencing were performed to evaluate mutations in HRAS, KRAS, and NRAS. In addition, mutations in PIK3CA, PTEN, and BRAF oncogenes were also evaluated. Considering all oncogenes that were surveyed, missense mutations were found in 11 of the 28 penile cancer samples (39 %), including 1 (3 %) mutation in KRAS (G12S) and 2 (7 %) mutations in HRAS (G12S and a Q61L). HRAS and KRAS mutations were found in larger and more advanced tumors. In addition, 8 (29 %) mutations (E542K or E545K) were identified in the PIK3CA. The mutations in RAS and PIK3CA were mutually exclusive, suggesting that deregulation of either the phosphatidylinositol 3-kinase or ras pathway would be sufficient for the development and progression of penile carcinoma.
Genes Silenced by DNA Methylation
Regulation of gene expression includes a wide range of mechanisms acting at either the transcriptional initiation, or at mRNA level, or at protein posttranslational modification. At transcriptional level, epigenetic changes such as DNA methylation at the promoter act to silence gene expression. Gene promoter hypermethylation plays a major role in cancer through transcriptional silencing of critical tumor suppressor genes.
In general, the studies that have searched for DNA methylation of tumor suppressor genes in SSCP also addressed other questions related to gene expression control (in special HPV infection), reflecting the complexity of this issue. However, all of them applied the methylation-specific PCR (MSP) method for assaying. In this reaction, the DNA is modified by sodium bisulfite, converting all unmethylated cytosines to uracil. But those cytosines that are methylated (5-methylcytosine) are resistant to this modification and remain as cytosine. Primers for subsequent amplification can be designed to distinguish methylated from unmethylated DNA in bisulfite-modified DNA, taking advantage of the sequence differences resulting from bisulfite modification. MSP requires only small quantities of DNA and is sensitive to 0.1 % methylated alleles of a given CpG island locus [50].
Two publications from the same group [51, 52] analyzed DNA methylation status of several gene promoters. A total of 26 SSCP tumors from Japanese men were assayed for HPV, TP53 alterations, and methylation promoter regions [50]. HPV DNA was detected in 3/26 patients (11.5 %). Overexpression of p53 was observed in 13/26 patients (50 %), and TP53 mutations were detected in 4 /26 patients (15.4 %). The frequencies of methylation in the promoter gene regions were as follows: DAPK, 26.9 % (7/26); FHIT, 88.4 % (23/26); MGMT, 19.2 % (5/26); p14, 3.8 % (1/26); p16, 23.1 % (6/26); RAR-beta, 23.1 % (6/26); RASSF1A, 11.5 % (3/26); and RUNX3, 42.3 % (11/26). FHIT gene promoter methylation was the highest, suggesting that it plays an important role in the pathogenesis of SSCP. Absence of Fhit protein expression was associated with promoter hypermethylation [52]. FHIT has a role in the regulation of apoptosis and the cell cycle, which may be lost upon promoter hypermethylation.
The HPV types, the methylation status in the promoter region of thrombospondin-1 (TSP-1), RAS association domain family 1A (RASSF1-A), and p16 genes and expression of TSP-1, CD31, p16, and p53 proteins were analyzed by reverse line blot, methylation-specific polymerase chain reaction, and immunohistochemistry, respectively, in 24 SSCP [53]. As results, HPV infection was detected in 11 of 24 cases (46 %), and TSP-1, RASSF1-A, and p16 genes were hypermethylated in 46, 42, and 38 % of the tumors, respectively. TSP-1 hypermethylation was associated with unfavorable histological grade (grade 3; p = 0.033), vascular invasion (p = 0.023), weak expression of TSP-1 protein (p = 0.041), and shorter overall survival (p = 0.04). TSP-1 expression was not associated with microvessel density. However, RASSF1-A hypermethylation was more frequent in T1 tumors (P = 0.01), and p16 hypermethylation was not associated with any of the tested variables except for absence of p16 expression (p = 0.022).
A study was performed on 53 SSCP to gain more insight into the mechanisms that may be involved in disruption of the p16INK4A/cyclin D/Rb pathway that functions as cell cycle regulatory proteins [54]. To that end, human papillomavirus (HPV) presence, p16 expression and promoter methylation, and expression of the BMI-1 polycomb gene product were studied. Only 9/53 carcinomas (17 %) revealed positivity with methylation-specific primers. The frequency of p16 promoter methylation was higher in HPV DNA-negative tumors (21 %) than in HPV-positive cases (10 %). Overall data indicated that p16/cyclin D/Rb pathway could become disrupted by either HPV E7 or by methylation of the p16 promoter or by overexpression of the BMI-1 polycomb gene product.
At Metastasis
Metastasis is a multiple step process by which cancer cells spread to other parts of the body. This can happen when cancer cells invade nearby normal tissue, or when they reach the lymphatic system and the bloodstream to spread to other parts of the body. The starting point for metastasis is when cancer cells break away from the primary tumor and attach to and degrade proteins that make up the surrounding extracellular matrix (ECM), which separates the tumor from adjoining tissues. By degrading these proteins, cancer cells are able to breach the ECM and escape. In addition to that, angiogenesis stimulates the growth of new blood vessels to obtain a blood supply. A blood supply is needed to obtain the oxygen and nutrients necessary for continued tumor growth. Some gene products that are implicated in the basis of metastasis have been studied in SSCP.
E-cadherins are cell adhesion molecules that are expressed in normal epithelia. Downregulation of E-cadherins is involved in the mechanism of metastasis, allowing cancer cells to detach from primary site. Matrix metalloproteases (MMPs) are enzymes that degrade type IV collagen in the basal membrane and are involved in the invasion mechanism. An increase in expression of MMPs is expected in the process of metastasis. E-cadherin and MMP-2 and MMP-9 were assayed by immunohistochemistry in SSCP tumors from 125 Brazilian patients [55]. Several parameters (age, race, disease evolution time, venereal background, clinical and pathological stage, tumor thickness, differentiation grade, venous and lymphatic embolization, koilocytosis, type of invasion, lymph node metastases, and survival) were assessed. On univariate analysis, lower E-cadherin immunoreactivity was associated with a greater risk of lymph node metastases, while higher MMP-9 immunoreactivity was considered an independent risk factor for disease recurrence. Another study has concluded that the less differentiated tumors are associated with the overexpression of MMPs [56]. In addition, lower E-cadherin immunoreactivity was reported in 45 % of SSCP Chinese cases and has been correlated with a greater risk of lymph node metastasis [42].
Prostaglandin E2 (PGE2) plays a role in invasiveness and metastasis. The synthesis of PGE2 from arachidonic acid requires the action of two isoenzymes in sequence. Cyclooxygenase (COX-1 and COX-2) catalyzes the synthesis of PGH2, which is converted, in turn, by microsomal prostaglandin E synthase (mPGES-1) to PGE2. In general, COX-1 is constitutively expressed and COX-2 is only expressed following induction by cytokines, growth factors, oncogenes, and tumor promoters. An investigation about COX-2 or mPGES-1 expression was performed in 7 in situ carcinomas and in 6 SSCP tumors [57]. Immunohistochemistry and Western blotting were used to evaluate the expression of COX-2 and mPGES-1 in benign and malignant lesions including metastases to lymph nodes. The expression of intratumoral PGE2 was quantified by enzyme immunoassay. Reverse transcription PCR was used to determine the expression of each of the four known receptors (EP(1–4)) for PGE2. Because HPV has been linked to the development of SSC, COX-2 overexpression was measured in SSCP in an HPV16 transgenic mouse. Immunohistochemistry demonstrated increased expression of COX-2 and mPGES-1 in dysplasia, in situ carcinoma, invasive SCC, and metastases to lymph nodes. Immunoblot analysis confirmed that COX-2 and mPGES-1 were consistently overexpressed in SSCP. PGE2 and all four of the PGE2 receptor subtypes were detected in each of the tumor samples. Elevated levels of COX-2 were also detected in SCC arising in an HPV16 transgenic mouse. Although limited in a number of cases, this study has shown the importance of COX-2 and mPGES-1 upregulation in SSCP.
Ki-67, a Proliferation Marker
Ki-67 is a nuclear protein encoded by MKI67 gene. This protein is considered as a cellular marker for proliferation and was associated with ribosomal RNA transcription [58]. The fact that the Ki-67 protein is present during all active phases of the cell cycle (G1, S, G2, and mitosis), but is absent from resting cells (G0), makes it an excellent marker for determining the so-called growth fraction of a given cell population [59]. Ki-67 expression seems to be tissue type dependent based on studies performed by immunohistochemistry. Ki-67 expression was found higher in basaloid carcinomas and lower in verrucous carcinomas in study assaying the expression of DNA topoisomerase I and II (Topo I and II) to pursue the possibility of future chemotherapy regimens for SCCP [60]. Additionally, lower expression of Ki-67 (as well as p16) could differentiate penile verrucous carcinoma from usual type squamous cell carcinoma. Probably, the lower Ki-67 expression is reflecting the slow-growing nature of verrucous tumors [61].
The prognostic significance of Ki-67 index has been investigated by immunohistochemistry. In a study with 44 SSCP tumors, the mean Ki-67 labeling index indicated an association with advanced local tumor stage, nodal metastasis, and clinical disease progression, but the difference between tumors with and without metastasis did not reach statistical significance [62]. Ki-67 was evaluated (in combination with other molecular makers – p53, E-cadherin, and MMP-9) as the presence of lymph node metastasis and survival in 73 Chinese SSCP tumors. High expression of Ki-67 was found in 26/73 (36 %) of the tumors. No significant difference was observed in inguinal metastases or in the 3-year survival rates between patients with low and high Ki-67 expression [61].
However, a different result was obtained when Ki-67 expression (also known as MIB-1) was evaluated in combination with another proliferation marker (proliferating cell nuclear antigen – PCNA) in 125 SSCP tumors [63]. In a univariate analysis, lower Ki-67 expression, the presence of lymphovascular permeation, clinically positive lymph nodes, tumor thickness greater than 5 mm, and infiltration of cavernous bodies were correlated with lymph node metastasis. However, the independent factors for lymph node metastasis risk were Ki-67 and PCNA, lymphovascular permeation, and clinical nodal stage. Independent variables for disease-free survival were urethra infiltration and the presence of lymph node metastasis. For death risk evaluation, the independent variables were age, lymph node metastasis, and clinical stage. In agreement, another study showed positive correlation between high Ki-67 expression and metastasis [64]. Four of 28 patients who were tested showed a weak Ki-67 expression, without displaying lymph node metastasis. Among 17 patients showing an intermediate Ki-67 index, eight exhibited metastases, while in all seven patients with a strong expression of Ki-67 lymph node metastases were found. The median Ki-67 expression in metastatic lesions was significantly different (50.3 %) from tumors without lymph node metastasis (31.8 %) (p = 0.024). Furthermore, a correlation between presence of HPV DNA and strong Ki-67 expression was found (p = 0.009).
The expressions of Ki-67 and cyclin D1 were investigated [65] in 21 SSCP tissues and in premalignant lesions of the penis (7 lichen sclerosus, 5 condyloma acuminatum, and 2 erythroplasia of Queyrat) and correlated with clinicopathological parameters and patient survival. Cyclin D plays an important role in regulating the progression of cells through the G1 phase of the cell cycle. Cyclin D1 overexpression was found in 13/21 SSCP (61.9 %) and in one case of erythroplasia of Queyrat. Strong reactivity for Ki-67 was found in 16 (76.2 %) SSCP, 3 condyloma acuminatum, and 1 case of erythroplasia of Queyrat. A tendency for an association between cyclin D1 expression and tumor differentiation (p = 0.07) but not the level of tumor invasion (p = 0.50) was found. The Ki-67 expression was notably increased with the advance of tumor grade, but the difference did not reach a statistically significant level (p = 0.46). A slight tendency towards a relationship between Ki-67 and cyclin D1 protein expression was observed (p = 0.32). Two patients relapsed and one died from the disease over a median follow-up period of 4.6 years (range 0.1–10.3 years). Ki-67 and cyclin D1 overexpression were in parallel, supporting the concept that cyclin D1 serves as a cell cycle activator.
PCNA, Proliferation Cell Nuclear Antigen
PCNA is a protein found in the nucleus of cells and is a cofactor of DNA polymerase delta. PCNA is important for both DNA synthesis and DNA repair because it shows further exonuclease activity. Since the exonuclease activity is proofreading, it is expected to play a significant role in the maintenance of the fidelity of mammalian DNA replication. Due to its properties, PCNA was originally identified as an antigen that is expressed in the nuclei of cells during the DNA synthesis phase of the cell cycle (S) [66]. PCNA antigen is, therefore, a marker of proliferation that competes with Ki-67.
PCNA expression was assayed by immunohistochemistry [67] and compares to biological aggressiveness (stage and grade) of 50 SSCP tumors from patients who underwent surgical penile amputation (total or partial). Fifteen of them required associated inguinal lymphadenectomy due to suspicion of lymph node metastasis. A diffuse and strong pattern of staining (high level) was found in 18/34 well-differentiated, 10/12 moderately differentiated, and 4/4 undifferentiated tumors. All tumors with metastasis were strong staining, including 4/18 well-differentiated and 4/10 moderately differentiated tumors exhibiting such pattern of staining. There was a positive relation between the strong staining of PCNA and the tumor staging (p = 0.003), but not with grading (p = 0.06). The authors argued that PCNA seemed to be an independent marker to guide medical management. Two years later, a complementary paper was published [68] that included data on p53. In this comparison p53 “won” as a prognostic marker. In a univariate analysis, PCNA staining showed association only with nodal metastasis (p = 0.04), while p53 staining exhibited correlation with tumor pT stage (p = 0.0005), grade (p = 0.02), lymphatic spread (p = 0.02), and cause-specific survival (p = 0.003). Multivariate analysis showed that p53 immunoreactivity was the only factor with prognostic significance for disease progression and cause-specific survival. Tumor pT stage, grade, and PCNA staining have no significance for nodal metastases and cause-specific death.
The comparison of the prognostic value of PCNA and Ki-67 [63] revealed that there was a correlation between the expression of both and the presence of lymph node metastasis. However, PCNA and Ki-67 immunohistochemical expression did not have a relationship with survival and death risk.
Circulating Proteins Markers
Proteomics is the large-scale study of proteins and is associated traditionally with displaying a large number of proteins from a given cell line or organism. Curiously, there is no strict linear relationship between genes and the protein complement or “proteome” of a cell. Proteomics is complementary to genomics, because it focuses on the gene products, which are the active agents in cells.
There are two strategies for finding protein biomarkers in tissues or in biological fluids. Several possible biomarkers have been identified using a gel-based approach in bidimensional electrophoresis (with and without stable isotopic labeling) and mass spectrometry. However, since this approach is very laborious and time-consuming, a new method has been developed to solve this problem. ClinProt matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF), which is based on affinity bead-based prefractionation of proteome, has recently emerged to fill in this gap. This method is fast and quite suitable for the following step that is the accurate mass determination by mass spectrometry (MS) [69]. ClinProt MALDI-TOF uses different chemical chromatographic surfaces on an outer layer of magnetic beads (such as Cu or cation coated) to selectively purify certain subsets of proteins, allowing unbound impurities to be removed by washing with buffers. Proteins bound to the magnetic beads are then eluted, diluted, and directly analyzed. Bioinformatics algorithms are used to align and integrate hundreds of mass data points from large numbers of samples, helping the resolution of complex mixtures. This is especially important for plasma proteomics, because plasma contains high abundance proteins (e.g., albumin, immunoglobulins) that could mask the presence of the secreted tumor protein markers which are found more diluted.
With the application of a ClinProt MALDI-TOF platform, proteins from plasma of 36 healthy subjects (controls) were compared to 25 plasmas from patients with SCCP [70]. The peptides were enriched by super-paramagnetic microparticles functionalized with a hydrophobic C8 coating, separating peptides and proteins according to their hydrophobicity. A cluster of two peptides was able to discriminate patients from control subjects. Cross-validation analysis using the whole casuistic showed 62.5 and 86.76 % sensitivity and specificity, respectively. The cluster also showed very high sensitivity (100 %) and specificity (97 %) for SCCP patients that died due to the disease. Furthermore, patients with lymph node involvement presented sensitivity and specificity of 80 and 97 %, respectively.
The two peptides were identified by an MALDI-TOF-TOF as fragments of C3 and C4a/b complement proteins. The conclusion was that fragments C3 and C4 a/b are less expressed in comparison with healthy subjects as the disease progresses. This finding is very promising in comparison to a previously described circulating SSCP marker, TA-4 antigen, also known as SSC antigen [71]. This antigen was originally isolated from patients showing squamous cell carcinoma of the uterine cervix, and later it was shown [59] that TA-4 values were elevated in serum of metastatic SSCP patients. However, TA-4 has shown limited value in the primary prediction of occult lymph node metastases because its levels increased significantly only after massive lymph node involvement or metastatic disease had occurred [72].
Summary
Pathological factors with a known prognostic value, other than lymph node metastasis, are tumor thickness, grade, histological type, lymphovascular embolization, and stage.
Oncoviruses such as human papillomavirus (HPV) and Epstein-Barr virus (EBV) can help to cause penile cancers. HPV encodes for E6 and E7 proteins that are able to bind to two important tumor suppressor proteins, p53 and pRB, respectively, inactivating them.
In penile cancer, the rarity of karyotype description is due to technical difficulties related to the low mitotic index, contamination of primary cultures, and the occurrence of large areas of necrosis in the tumor. The frequency of DNA aneuploidy showed correlation with histological type of invasive squamous cell carcinoma of the penis.
A significant association between MYC gains and tumor progression and poor outcome was demonstrated. These findings were independent of HPV infection. Protein c-MYC expression was increased in samples with HPV infection, probably reflecting direct activation of MYC.
The prognostic significance of p53, Ki-67, PCNA, E-cadherin, and Matrix metalloproteases-9 (MMP-9) was evaluated in SCCP tumors. Tumor embolization and the expression of p53 are independent predictors of metastasis. The comparison of the prognostic value of PCNA and Ki-67 revealed that there was a correlation between the expression of both and the presence of lymph node metastasis.
Among the specimens of invasive carcinomas, 85.4 % showed positive telomerase activity. In some patients it was also possible to measure the activity of telomerase in the region adjacent to the tumor, which was free of tumor cells according to histopathological analysis. These results indicated that telomerase was reactivated either in normal tissues or adjacent tissues of SCCP.
Bcl-2 and Bax were completely imbalanced when the tumor, adjacent either skin or corpus cavernous, was compared in the same way. This means that the adjacent tissues are at least under the influence of the tumor.
The mutations in RAS and PIK3CA were mutually exclusive, suggesting that deregulation of either the phosphatidylinositol 3-kinase or ras pathway would be sufficient for the development and progression of penile carcinoma.
Fragments of C3 and C4a/b complement proteins are less expressed in plasma of SCCP patients in comparison with healthy subjects as the disease progresses.
TA-4 antigen, also known as SCC antigen, was elevated in serum of metastatic SCCP patients. However, this antigen has shown limited value in the primary prediction of occult lymph node metastases.
References
Ornellas AA, Nóbrega BLB, Chin EWK, Wisnescky A, Silva PCB, Schwindt ABS. Prognostic factors in invasive squamous cell carcinoma of the penis: analysis of 196 patients treated in Brazilian National Cancer Institute. J Urol. 2008;180:1354–9.
Lopes A, Bezerra AL, Pinto CA, Serrano SV, de Mello CA, Villa LL. p53 as a new prognostic factor for lymph node metastasis in penile carcinoma: analysis of 82 patients treated with amputation and bilateral lymphadenectomy. J Urol. 2002;168:81–6.
Soria JC, Fizazi K, Piron D, Kramar A, Geraulet A, Haie-Meder C, et al. Squamous cell carcinoma of the penis: multivariate analysis of prognostic factors and natural history in a monocentric study with a conservative policy. Ann Oncol. 1997;8:1089–98.
Velazquez EF, Amin MB, Epstein JI, Grignon DJ, Humphrey PA, Pettaway CA, Renshaw AA, Reuter VE, Srigley JR, Cubilla AL. Protocol for the examination of specimens from patients with carcinoma of the penis. Arch Pathol Lab Med. 2010;134:923–9.
Ornellas AA, Chin EWK, Nóbrega BLB, Wisnescky A, Koifman N, Quirino R. Surgical treatment of invasive squamous cell carcinoma of the penis: Brazilian National Cancer Institute long-term experience. J Surg Oncol. 2008;97:487–95.
Ferrándiz PC, de Torres I, García PV. Penile squamous cell carcinoma. Actas Dermosifiliogr. 2012;103(6):478–87.
Mosconi AM, Roila F, Gatta G, Theodore C. Cancer of the penis. Crit Rev Oncol Hematol. 2005;53(2):165–77.
Guimarães GC, Cunha IW, Soares FA, Lopes A, Torres J, Chaux A, Velazquez EF, Ayala G, Cubilla AL. Penile squamous cell carcinoma clinicopathological features, nodal metastasis and outcome in 333 cases. J Urol. 2009;182(2):528–34.
Chaux A, Reuter V, Lezcano C, Velazquez EF, Torres J, Cubilla AL. Comparison of morphologic features and outcome of resected recurrent and nonrecurrent squamous cell carcinoma of the penis: a study of 81 cases. Am J Surg Pathol. 2010;33(9):1299–306.
Cubilla AL, Lloveras B, Alemany L, Alejo M, Vidal A, Kasamatsu E, Clavero O, Alvarado-Cabrero I, Lynch C, Velasco-Alonso J, Ferrera A, Chaux A, Klaustermeier J, Quint W, de Sanjosé S, Muñoz N, Bosch FX. Basaloid squamous cell carcinoma of the penis with papillary features: a clinicopathologic study of 12 cases. Am J Surg Pathol. 2012;36(6):869–75.
Velasquez EF, Melamed J, Barrreto JF, Aguero F, Cubilla AL. Sarcomatoid carcinoma of the penis: a clinico-patholocical study of 14 cases. Am J Surg Pathol. 2005;29(9):1152–8.
Lont AP, Gallee MPW, Snijders P, Horenblas S. Sarcomatoid squamous cell carcinoma of the penis: a clinical and pathological study of 5 cases. J Urol. 2004;172(3):932–5.
Bezerra AL, Lopes A, Landman G, Alencar GN, Torloni H, Villa LL. Clinicopathologic features and human papillomavirus dna prevalence of warty and squamous cell carcinoma of the penis. Am J Surg Pathol. 2001;25(5):673–8.
Chuanyu S, Ke X, Jie Z, Guowei X, Zujun F, Qiang D. Surgical treatment for 11 cases of penile verrucous carcinoma. Ann Dermatol. 2011;23(3):346–9.
Secretan B, Straif K, Baan R, Grosse Y, El Ghissassi F, Bouvard V, Benbrahim-Tallaa L, Guha N, Freeman C, Galichet L, Cogliano V, WHO International Agency for Research on Cancer Monograph Working Group. A review of human carcinogens–Part E: tobacco, areca nut, alcohol, coal smoke, and salted fish. Lancet Oncol. 2009;10(11):1033–4.
Straif K, Benbrahim-Tallaa L, Baan R, Grosse Y, Secretan B, El Ghissassi F, Bouvard V, Guha N, Freeman C, Galichet L, Cogliano V, WHO International Agency for Research on Cancer Monograph Working Group. A review of human carcinogens–part C: metals, arsenic, dusts, and fibres. Lancet Oncol. 2009;10(5):453–4.
El Ghissassi F, Baan R, Straif K, Grosse Y, Secretan B, Bouvard V, Benbrahim-Tallaa L, Guha N, Freeman C, Galichet L, Cogliano V, WHO International Agency for Research on Cancer Monograph Working Group. A review of human carcinogens–part D: radiation. Lancet Oncol. 2009;10(8):751–2.
Baan R, Grosse Y, Straif K, Secretan B, El Ghissassi F, Bouvard V, Benbrahim-Tallaa L, Guha N, Freeman C, Galichet L, Cogliano V, WHO International Agency for Research on Cancer Monograph Working Group. A review of human carcinogens–Part F: chemical agents and related occupations. Lancet Oncol. 2009;10(12):1143–4.
Scheiner MA, Campos MM, Ornellas AA, Chin EW, Ornellas MH, Andrada-Serpa MJ. Human papillomavirus and penile cancers in Rio de Janeiro, Brazil: HPV typing and clinical features. Int Braz J Urol. 2008;34:467–74.
Afonso LA, Moyses N, Alves G, Ornellas AA, Passos MR, Oliveira Ldo H, Cavalcanti SM. Prevalence of human papillomavirus and Epstein-Barr virus DNA in penile cancer cases from Brazil. Mem Inst Oswaldo Cruz. 2012;107(1):18–23.
Buitrago-Pérez A, Garaulet G, Vázquez-Carballo A, Paramio JM, García-Escudero R. Molecular signature of HPV-induced carcinogenesis: pRb, p53 and gene expression profiling. Curr Genomics. 2009;10(1):26–34.
Xiao S, Feng XL, Shi YH, Liu QZ, Li P. Cytogenetic abnormalities in a squamous cell carcinoma of the penis. Cancer Genet Cytogenet. 1992;64(2):139–41.
Ornellas AA, Ornellas MH, Simões F, Soares R, Campos MM, Harab RC, Silva MLM. Cytogenetic analysis of an invasive, poorly differentiated squamous cell carcinoma of the penis. Cancer Genet Cytogenet. 1998;101:78–80.
Ornellas AA, Ornellas MH, Otero L, Simões F, Campos MM, Harab RC, Silva MLM. Karyotypic findings in two cases of moderately differentiated squamous cell carcinoma of the penis. Cancer Genet Cytogenet. 1999;115:77–9.
Ornellas AA, Campos MM, Ornellas MH, Wisnescky A, Koifman N, Harab RC. Cancer du pénis: étude dela ploïdie par cytométrie de flux chez 90 patients. Progrès Urol. 2000;10:72–7.
Alves G, Heller A, Fiedler W, Campos MM, Claussen U, Ornellas AA, Liehr T. Genetic imbalances in 26 penile SSC cases. Genes Chromosomes Cancer. 2001;31(1):48–53.
Masferrer E, Ferrándiz-Pulido C, Lloveras B, Masferrer-Niubò M, Espinet B, Salido M, Rodríguez-Rivera M, Alemany L, Placer J, Gelabert A, Servitje O, García-Patos V, Pujol RM, Toll A. MYC copy number gains are associated with poor outcome in penile squamous cell carcinoma. J Urol. 2012;188(5):1965–71.
Alves G, Fiedler W, Guenther E, Nascimento P, Campos MM, Ornellas AA. Determination of telomerase activity in squamous cell carcinoma of the penis. Int J Oncol. 2001;18(1):67–70.
Salgado R, Toll A, Espinet B, González-Roca E, Barranco CL, Serrano S, Solé F, Pujol RM. Analysis of cytogenetic abnormalities in squamous cell carcinoma by array comparative genomic hybridization. Actas Dermosifiliogr. 2008;99(3):199–206.
Koshland Jr DE. Molecule of the year. Science. 1993;262(5142):1953.
Lane DP, Crawford LV. T antigen is bound to a host protein in SV40-transformed cells. Nature. 1979;278(5701):261–3.
Levine AJ, Oren M. The first 30 years of p53: growing ever more complex. Nat Rev Cancer. 2009;9(10):749–58.
Vazquez A, Liu J, Zhou Y, Oltvai Z. Catabolic efficiency of aerobic glycolysis: the Warburg effect revisited. BMC Syst Biol. 2010;4:58. doi:10.1186/1752-0509-4-58. PMC 2880972. PMID 20459610.
Vousden KH, Ryan KM. p53 and metabolism. Nat Rev Cancer. 2009;9(10):691–700.
Petitjean A, Mathe E, Kato S, Ishioka C, Tavtigian SV, Hainaut P, Olivier M. Impact of mutant p53 functional properties on TP53 mutation patterns and tumor phenotype: lessons from recent developments in the IARC TP53 database. Hum Mutat. 2007;28(6):622–9.
Lam KY, Chan AC, Chan KW, Leung ML, Srivastava G. Expression of p53 and its relationship with human papillomavirus in penile carcinomas. Eur J Surg Oncol. 1995;21:613–6.
Pilotti S, Donghi R, D’Amato L, et al. HPV detection and p53 alteration in squamous cell verrucous malignancies of the lower genital tract. Diagn Mol Pathol. 1993;2:248–56.
Ranki A, Lassus J, Niemi KM. Relation of p53 tumor suppressor protein expression to human papillomavirus (HPV) DNA and to cellular atypia in male genital warts and in premalignant lesions. Acta Derm Venereol. 1995;75:180–6.
Castren K, Vahakangas K, Heikkinen E, Ranki A. Absence of p53 mutations in benign and pre-malignant male genital lesions with over-expressed p53 protein. Int J Cancer. 1998;77:674–8.
Lam KY, Chan KW. Molecular pathology and clinicopathologic features of penile tumors: with special reference to analyses of p21 and p53 expression and unusual histologic features. Arch Pathol Lab Med. 1999;123:895–904.
Seigne JD, Ornellas AA, Faria P. Altered expression of the retinoblastoma (Rb) and P53 tumor suppressor genes in squamous cell carcinoma of the penis. J Urol. 1997;157(suppl):46.
Zhu Y, Zhou XY, Yao XD, Dai B, Ye DW. The prognostic significance of p53, Ki-67, epithelial cadherin and matrix metalloproteinase-9 in penile squamous cell carcinoma treated with surgery. BJU Int. 2007;100(1):204–8.
Olovnikov AM. A theory of marginotomy. The incomplete copying of template margin in enzymic synthesis of polynucleotides and biological significance of the phenomenon. J Theor Biol. 1973;41(1):181–90.
Greider CW, Blackburn EH. Identification of a specific telomere terminal transferase activity in Tetrahymena extracts. Cell. 1985;43(2 Pt 1):405–13.
Kim NW, Piatyszek MA, Prowse KR, Harley CB, West MD, Ho PL, Coviello GM, Wright WE, Weinrich SL, Shay JW. Specific association of human telomerase activity with immortal cells and cancer. Science. 1994;266(5193):2011–5.
Ikeda R, Kobayashi Y, Shiroma K, Suzuki K, Ueda Y. Telomerase activity in giant condyloma acuminatum. Urol Int. 2000;65(4):220–3.
Tsujimoto Y, Cossman J, Jaffe E, Croce CM. Involvement of the bcl-2 gene in human follicular lymphoma. Science. 1985;228(4706):1440–3.
Malumbres M, Barbacid M. RAS oncogenes: the first 30 years. Nat Rev Cancer. 2003;3(6):459–65.
Andersson P, Kolaric A, Windahl T, Kirrander P, Söderkvist P, Karlsson MG. PIK3CA, HRAS and KRAS gene mutations in human penile cancer. J Urol. 2008;179:2030–4.
Herman JG, Graff JR, Myöhänen S, Nelkin BD, Baylin SB. Methylation-specific PCR: a novel PCR assay for methylation status of CpG islands. Proc Natl Acad Sci U S A. 1996;93(18):9821–6.
Yanagawa N, Osakabe M, Hayashi M, Tamura G, Motoyama T. Detection of HPV-DNA, p53 alterations, and methylation in penile squamous cell carcinoma in Japanese men. Pathol Int. 2008;58(8):477–82.
Yanagawa N, Osakabe M, Hayashi M, Tamura G, Motoyama T. Frequent epigenetic silencing of the FHIT gene in penile squamous cell carcinomas. Virchows Arch. 2008;452(4):377–82.
Guerrero D, Guarch R, Ojer A, Casas JM, Ropero S, Mancha A, Pesce C, Lloveras B, Garcia-Bragado F, Puras A. Hypermethylation of the thrombospondin-1 gene is associated with poor prognosis in penile squamous cell carcinoma. BJU Int. 2008;102(6):747–55.
Ferreux E, Lont AP, Horenblas S, Gallee MP, Raaphorst FM, von Knebel Doeberitz M, Meijer CJ, Snijders PJ. Evidence for at least three alternative mechanisms targeting the p16INK4A/cyclin D/Rb pathway in penile carcinoma, one of which is mediated by high-risk human papillomavirus. J Pathol. 2003;201(1):109–18.
Campos RS, Lopes A, Guimarães GC, Carvalho AL, Soares FA. E-cadherin, MMP-2, and MMP-9 as prognostic markers in penile cancer: analysis of 125 patients. Urology. 2006;67(4):797–802.
Soares FA, da Cunha IW, Guimarães GC, Nonogaki S, Campos RS, Lopes A. The expression of metaloproteinases-2 and −9 is different according to the patterns of growth and invasion in squamous cell carcinoma of the penis. Virchows Arch. 2006;449(6):637–46.
Golijanin D, Tan JY, Kazior A, Cohen EG, Russo P, Dalbagni G, Auborn KJ, Subbaramaiah K, Dannenberg AJ. Cyclooxygenase-2 and microsomal prostaglandin E synthase-1 are overexpressed in squamous cell carcinoma of the penis. Clin Cancer Res. 2004;10(3):1024–31.
Bullwinkel J, Baron-Lühr B, Lüdemann A, Wohlenberg C, Gerdes J, Scholzen T. Ki-67 protein is associated with ribosomal RNA transcription in quiescent and proliferating cells. J Cell Physiol. 2006;206(3):624–35.
Scholzen T, Gerdes J. The Ki-67 protein: from the known and the unknown. J Cell Physiol. 2000;182(3):311–22.
Berney DM, Stankiewicz E, Adlan AM, Kudahetti S, Biedrzycki OJ, Hadway P, Watkin N, Corbishley C. DNA topoisomerase I and II alpha expression in penile carcinomas: assessing potential tumour chemosensitivity. BJU Int. 2008;102(8):1040–4.
Stankiewicz E, Kudahetti SC, Prowse DM, Ktori E, Cuzick J, Ambroisine L, Zhang X, Watkin N, Corbishley C, Berney DM. HPV infection and immunochemical detection of cell-cycle markers in verrucous carcinoma of the penis. Mod Pathol. 2009;22(9):1160–8.
Berdjis N, Meye A, Nippgen J, Dittert D, Hakenberg O, Baretton GB, Wirth MP. Expression of Ki-67 in squamous cell carcinoma of the penis. BJU Int. 2005;96(1):146–8.
Guimarães GC, Leal ML, Campos RS, Zequi Sde C, da Fonseca FP, da Cunha IW, Soares FA, Lopes A. Do proliferating cell nuclear antigen and MIB-1/Ki-67 have prognostic value in penile squamous cell carcinoma? Urology. 2007;70(1):137–42.
Protzel C, Knoedel J, Zimmermann U, Woenckhaus C, Poetsch M, Giebel J. Expression of proliferation marker Ki67 correlates to occurrence of metastasis and prognosis, histological subtypes and HPV DNA detection in penile carcinomas. Histol Histopathol. 2007;22(11):1197–204.
Papadopoulos O, Betsi E, Tsakistou G, Frangoulis M, Kouvatseas G, Anagnostakis D, Kouvidou C. Expression of cyclin D1 and Ki-67 in squamous cell carcinoma of the penis. Cancer Res. 2007;27(4B):2167–74.
Leonardi E, Girlando S, Serio G, Mauri FA, Perrone G, Scampini S, Dalla Palma P, Barbareschi M. PCNA and Ki67 expression in breast carcinoma: correlations with clinical and biological variables. J Clin Pathol. 1992;45(5):416–9.
Martins ACP, Faria SM, Velludo MAL, Cologna AJ, Suaid HJ, Tucci Jr S. Carcinoma of the penis: the value of proliferating cellular antigen (PCNA). Braz J Urol. 2000;26(1):38–42.
Martins AC, Faria SM, Cologna AJ, Suaid HJ, Tucci Jr S. Immunoexpression of p53 protein and proliferating cell nuclear antigen in penile carcinoma. J Urol. 2002;167(1):89–92.
Cheng AJ, Chen LC, Chien KY, Chen YJ, Chang JT, Wang HM, Liao CT, Chen IH. Oral cancer plasma tumor marker identified with bead-based affinity-fractionated proteomic technology. Clin Chem. 2005;51(12):2236–44.
Ornellas P, Ornellas AA, Chinello C, Gianazza E, Mainini V, Cazzaniga M, Pereira DA, Sandim V, Cypriano AS, Koifman L, da Silva PC, Alves G, Magni F. Downregulation of C3 and C4A/B complement factor fragments in plasma from patients with squamous cell carcinoma of the penis. Int Braz J Urol. 2012;38(6):739–49.
Wishnow KI, Johnson DE, Fritsche H. Squamous cell carcinoma antigen (TA-4) in penile carcinoma. Urology. 1990;36(4):315–7.
Hungerhuber E, Schlenker B, Schneede P, Stief CG, Karl A. Squamous cell carcinoma antigen correlates with tumor burden but lacks prognostic potential for occult lymph node metastases in penile cancer. Urology. 2007;70(5):975–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Ornellas, A.A., Alves, G., Schwindt, A.B.d.S. (2014). Pathology and Genetics. In: Culkin, D. (eds) Management of Penile Cancer. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0461-7_4
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0461-7_4
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-0460-0
Online ISBN: 978-1-4939-0461-7
eBook Packages: MedicineMedicine (R0)