
Abstract
Oxidative stress and free radicals have been implicated in the pathophysiology of a number of neuropsychiatric disorders. Both genetic and nongenetic factors have been shown to cause increased cellular levels of reactive oxygen species in subjects with schizophrenia or mood disorder. The above factors are also known to trigger oxidative cellular damage to lipids, proteins, and DNA, which leads to abnormal neural growth and differentiation. In addition, recent evidence suggest that novel therapeutic strategies such as supplementation with antioxidants, ω3 fatty acids, or combination of both might improve the neuroplasticity and can be effective for long-term treatment management of neuropsychiatric disorders. This chapter presents an overview of the recent findings on the potential treatment strategies using antioxidants in schizophrenia and mood disorders.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Bipolar Disorder
- Schizophrenic Patient
- Schizophrenia Patient
- Postpartum Depression
- Bipolar Disorder Patient
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
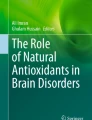
Oxidative stress is defined as higher cellular levels of reactive oxygen species (ROS) than the cellular antioxidant defense. Brain consumes approximately 20 % of the total amount of oxygen in the body. But the enhanced metabolic rate in the brain leads to the generation of excessive levels of ROS. Mostly, oxidative stress-mediated damage of the brain occurs due to higher lipid peroxidation in the cerebrospinal fluid and plasma along with reduced membrane polyunsaturated fatty acids (PUFAs) in the brain and red blood cell (RBC) membranes (Mahadik et al. 2001). Free radicals are produced through a variety of physiological and pathological processes (Fig. 1). The radicals generated from molecular oxygen are generally known as ROS, which include superoxide anion (O2 −), hydroxyl (OH•), hydrogen peroxide (H2O2), singlet oxygen (1O2), and nitric oxide (NO•).

Possible mechanisms involving production and removal of oxygen and nitrogen free radicals in mammalian cells (reprinted with permission from Yao and Keshavan 2011). Molecular oxygen can be converted to superoxide radicals (O2 −•) in the presence of xanthine oxidase (XO). Subsequently, superoxide dismutase (SOD) catalyzes the conversion of superoxide radicals to hydrogen peroxide (H2O2). Catalase (CAT) and glutathione peroxidase (GSH-Px) convert hydrogen peroxide to water. Glutathione (GSH) is utilized by GSH-Px to yield the oxidized form of glutathione (GSSG), which is converted back to GSH by glutathione reductase (GR). Hydrogen peroxide is susceptible to autoxidation to form hydroxyl radicals (OH•), particularly in the presence of metal catalysts such as iron. In addition, nitric oxide (NO), which is the product of a five-electron oxidation of the amino acid l-arginine, can also produce hydroxyl radicals as well as nitrogen dioxide radical. On the other hand, α-tocopherol (vitamin E) has the ability to inhibit lipid peroxidation as a chain-breaking antioxidant. Vitamin E radicals can be recycled back to their native form by ascorbic acid (vitamin C)
Oxidative stress occurs when the production of ROS exceeds the natural antioxidant defense mechanisms, causing damage to macromolecules such as DNA, proteins, and lipids. Cells are protected by antioxidant defense mechanisms that remove these free radicals to prevent oxidative damage. The antioxidant system comprises of different types of functional components such as enzymatic and nonenzymatic antioxidants (Fig. 1). The enzymatic antioxidants comprise of superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GPx), glutathione reductase, and glutathione S transferase. The nonenzymatic antioxidants include reduced glutathione, vitamin C, vitamin E (α-tocopherol), uric acid, carotenoids, flavonoids, ubiquinol, etc.
2 Oxidative Stress in Schizophrenia
Studies suggest that genetic factors, neuronal maldevelopment, impaired neurotransmission, viral infections, environmental factors, and stressors are the main triggers of schizophrenia (Kendler 2003; Jakob and Beckmann 1986; Thome et al. 1998; Carlsson et al. 1999; Kornhuber and Weller 1994; Pearce 2001). Evidence also indicates that mitochondrial pathology and oxidative stress may be the most critical components in the pathophysiology of schizophrenia (Goff et al. 1995; Whatley et al. 1998; Ben-Shachar and Laifenfeld 2004; Bubber et al. 2004; Yao and Keshavan 2011). Lipid peroxidation products, a marker for oxidative stress-mediated damage, were found to be increased in the cerebrospinal fluid and plasma (Mahadik et al. 2001). It has been also observed that oxidative damage leads to reduced membrane PUFAs in the brain and RBC membranes (Mahadik et al. 2001). Moreover, levels of nitric oxide and superoxides (NO‾ and O2‾) as determined indirectly as nitrate (NO‾2) and nitrite (NO‾3) were higher in serum (Taneli et al. 2004), RBC (Herken et al. 2001), and postmortem brain (Yao et al. 2004) samples from schizophrenia subjects.
A significant reduction in plasma total antioxidant status (TAS) has been found in patients with chronic schizophrenia (Yao et al. 1998a) as well as first-episode drug-naive patients with schizophrenia (Li et al. 2011). Individual plasma antioxidants, albumin, bilirubin (Yao et al. 2000), and uric acid (Yao et al. 1998c) were also found lower in schizophrenia subjects. Moreover, decreases in plasma levels of total and reduced GSH, along with altered antioxidant enzyme activities, have been reported in drug-naive first-episode patients with schizophrenia when compared with healthy control subjects (Raffa et al. 2011). Suboticanec et al. (1990) have demonstrated that both plasma and urinary vitamin C levels were lower in chronic schizophrenia subjects, relative to normal controls, even after controlling for diet. McCreadie et al. (1995) found lower ratios of vitamin E to cholesterol in schizophrenic patients compared with normal control subjects. Later, Brown et al. (1998) also reported decreased lipid-corrected vitamin E levels in schizophrenic patients with tardive dyskinesia, relative to healthy controls, but not in patients without dyskinesia. Decreased levels of GSH, ascorbic acid, and plasma vitamin E levels were also found in erythrocytes from schizophrenic patients compared with healthy subjects (Surapaneni 2007).
Increased SOD activities have been reported in RBC of schizophrenic patients (Abdalla et al. 1986; Reddy et al. 1991; Yao et al. 1998b). A recent study did not find any change in plasma SOD activity in drug-naive first-episode schizophrenic patients compared to control subjects (Raffa et al. 2011). However, a meta-analysis showed that SOD activity was significantly decreased in the disorganized type of schizophrenia patients versus healthy controls (Zhang et al. 2010). A significant increase in GPx activity but decrease in CAT activity was found in plasma samples from drug-naive first-episode schizophrenic patients compared to control subjects (Raffa et al. 2011). Moreover, GPx activity was found to be lower in neuroleptic-treated chronic schizophrenia patients (Stoklasova et al. 1986), in drug-free female schizophrenia patients (Abdalla et al. 1986), and in neuroleptic-naive psychotic children (Golse et al. 1977). Schizophrenia patients had significantly lower RBC GPx activity than controls (Othmen et al. 2008). Zhang et al. (1998) have reported higher plasma GPx activities in long-term neuroleptic-free as well as neuroleptic-naïve schizophrenic patients, while Yao et al. (1999) did not find any significant difference between chronic schizophrenic patients and normal subjects. Decrease in CAT activity was also observed in clinically stable patients with schizophrenia and their unaffected siblings (Othmen et al. 2008). However, CAT activity was found unchanged in erythrocytes and plasma of drug-free schizophrenic patients (Yao et al. 1998b; Yao et al. 1999). A recent meta-analysis reported no significant difference in CAT activity between schizophrenia and control subjects (Zhang et al. 2010).
Inflammatory responses induced by proinflammatory T cells provide a source of free radicals that leads to damage of proteins, lipids, and nucleic acids in neuronal cells. Increased cytokine (IL-1β, IL-6, TNF-α) levels are known to generate ROS in the cells. A microarray gene analysis of T cells from schizophrenia patients showed prominent transcript alterations in cell cycle machinery, intracellular signaling, metabolism, and oxidative stress, suggesting that altered T cell response might induce oxidative stress in schizophrenia (Craddock et al. 2007).
3 Oxidative Stress in Bipolar Disorder
Bipolar disorder is a major mood disorder affecting an estimated 1–3 % of the population (Belmaker 2004; Kupfer 2005; Merikangas et al. 2007). Oxidative stress has also been implicated in the pathophysiology of bipolar disorder. Several studies have reported that bipolar disorder patients have significant alterations in antioxidant enzymes, lipid peroxidation, and nitric oxide levels; however, the results are conflicting. A meta-analysis by Andreazza et al. (2008) found that bipolar disorder patients have increased lipid peroxidation and increased NO levels but failed to find significant changes in GPx activity in bipolar disorder (Andreazza et al. 2009). An earlier study has found lower levels of SOD and catalase in bipolar disorder patients (Ranjekar et al. 2003). However, the above data was not in agreement with the findings by Kuloglu et al. (2002), where an increase in SOD levels with no changes in GPx was found in bipolar patients. Serum levels of NO and SOD were found significantly higher in bipolar disorder patients, with a correlation between the number of the manic episodes and NO levels (Savas et al. 2006). A recent review by Marazziti et al. (2012) indicated that mitochondrial dysfunction could contribute to cell metabolism errors and apoptosis in disorders such as schizophrenia and bipolar disorder.
4 Oxidative Stress in Major Depression
Major depression is characterized by significantly lower plasma levels of a number of key antioxidants, such as vitamin E, zinc, and coenzyme Q10, as well as lower glutathione peroxidase activity (Maes et al. 2011). A significant association has been found between depression and polymorphisms in genes involved in oxidative pathways such as manganese superoxide dismutase and catalase (Maes et al. 2011). Galecki et al. (2009) showed increases in CAT activity levels during acute episodes of depression, whereas Kodydkova et al. (2009) demonstrated decreases in GPx activity from female patients with depression. Such reduced levels of GPx were further shown in postmortem prefrontal cortex samples from patients with major depression and schizophrenia (Gawryluk et al. 2011).
In addition, accumulating evidence exists that demonstrates the presence of membrane fatty acid defects in patients with major depression (Hibbeln and Salem 1995; Peet et al. 1998; Edwards et al. 1998). Specifically, an increased ratio of 5,8,11,14-eicosatetraenoic acid (arachidonic acid, AA) to 5,8,11,14,17-eicosapentaenoic acid (EPA) and decreased levels of ω-3 fatty acids have been observed in the serum and RBC lipids of depressive patients. Furthermore, the AA/EPA ratio in serum and RBC membrane phospholipids was correlated positively with the severity of illness (Maes et al. 1996; Seko et al. 1997). The above findings are consistent with the epidemiological studies demonstrating an association between decreased ω-3 fatty acid consumption and increased rates of depression (Hibbeln and Salem 1995). Patients with major depression may have an abnormal intake of ω-3 fatty acids (Edwards et al. 1998; Hibbeln 1998).
Both ω-6 and ω-3 PUFAs are involved the regulation of inflammatory response system. The ω-6 PUFAs, particularly AA, have the proinflammatory features, since AA is the precursor of proinflammatory eicosanoids, prostaglandin E2 (PGE2), and leukotriene B4 (LTB4) and the increase production of interleukin-1 (IL-1), tumor necrosis factor-α (TNF-α), and IL-6 (Soyland et al. 1994; Tashiro et al. 1998). On the other hand, the ω-3 PUFAs, EPA, and docosahexaenoic acid (DHA) suppress the production of AA-derived eicosanoids, thus having anti-inflammatory and immunosuppressive effects (Calder 1998). Several groups have reported that ω-3 PUFA-enriched diets (e.g., fish oil) can lead to partial replacement of AA by EPA in inflammatory cell membranes and significantly reduce the ex vivo production of proinflammatory cytokines (Soyland et al. 1994; Calder 1998; James et al. 2000). Therefore, an imbalance of ω-6/ω-3 PUFAs may result in an increased production of proinflammatory cytokines. Smith (1991) proposed that abnormal fatty acid composition might be related to the inflammatory response system underlying pathophysiology of major depression. Further, Maes et al. (2000) have substantiated the role of ω-3 PUFAs in predicting the response of proinflammatory cytokines to psychological stress.
5 Antioxidant Supplementation as Adjunctive Therapy
In the above sections, we have discussed the role of free radicals and antioxidant enzymes in the pathophysiology of schizophrenia, bipolar disorder, and major depression. Accumulating evidence from clinical, preclinical, and epidemiological studies suggests that many of the antioxidant compounds possess neuroprotective and anti-inflammatory properties and could be considered as important adjunctive therapy for schizophrenia (Pillai 2008). We discuss below a few important antioxidants for their therapeutic potential in the above neuropsychiatric disorders.
5.1 Antioxidant Interventions in Schizophrenia
The section below will discuss the recent findings in studies using antioxidants as adjunctive therapeutics in schizophrenia. The major compounds explored in the treatment of schizophrenia for their antioxidant potential are vitamins, N-acetylcysteine (NAC), and ω-3 fatty acids.
5.1.1 Vitamins
Vitamin C and vitamin E are the well-studied essential nutrients that function as the major chain-breaking antioxidants. They are the first line of defense against lipid peroxidation and protecting cell membranes from free radical damage in the human body. It has been shown that the oral supplementation of vitamin C with atypical antipsychotic reverses ascorbic acid levels, reduces oxidative stress, and improves BPRS score in schizophrenic patients (Dakhale et al. 2005). Arvindakshan et al. (2003) also reported reduction in BPRS and PANSS and increase in Henrich’s quality of life score after supplementation with ω-3 fatty acids, vitamin E, and vitamin C. It has been suggested that a combination of a hydrophobic agent such as vitamin E, to protect membranes, and a hydrophilic agent such as vitamin C in intracellular protection provides complete antioxidant defense (Mahadik et al. 2001). A number of studies have used vitamin E as a supplement in chronic schizophrenic patients with TD (reviewed by Yao and Keshavan 2011). Supranormal doses of vitamin E have been safely and effectively used to reduce the severity of TD. Several studies, albeit with relatively small sample sizes, have reported decreases in the severity of dyskinesia by vitamin E treatment (Peet et al. 1993; Elkashef and Wyatt 1999; Adler et al. 1993) though there are some contradictory findings (Corrigan et al. 1993; Shriqui et al. 1992).
5.2 N-Acetylcysteine (NAC)
NAC is the precursor of glutathione, which is known to restore the primary endogenous antioxidant GSH and maintain the oxidative balance in the cell. In addition, NAC has been also shown to scavenge oxidants directly, particularly the reduction of the hydroxyl radical and hypochlorous acid (Aruoma et al. 1989). A number of studies have tested the efficacy of NAC as an adjunctive therapy in schizophrenia (Berk et al. 2008a; Bulut et al. 2009; Dodd et al. 2008; Dean et al. 2011). The above studies have suggested that NAC seems to be a safe, effective, tolerable, and affordable adjunctive antioxidant molecule for the treatment of schizophrenia.
5.2.1 Omega-3 Fatty Acid
Membrane deficits have been well documented in subjects with schizophrenia (Mahadik and Yao 2006; Yao and Keshavan 2011). Therefore, boosting the lower levels of membrane phospholipid EPUFAs, predominantly AA (20:4n-6, ω6-EPUFA) and DHA (22:6n-3, ω3-EPUFA), by dietary supplementation is an attractive approach to protect the membrane from cellular damage in schizophrenia. A recent study has shown that high intake of fish, ω-3 or ω-6 PUFA has a lower rate of schizophrenic symptoms in women (Hedelin et al. 2010). Long-chain ω-3 fatty acids have been shown to reduce the risk of progression to psychotic disorder, particularly in the early stages of illness, and may propose a safe and efficacious adjunctive strategy to prevent from psychiatric condition (Amminger et al. 2010). Thus, ω-3 fatty acids provide numerous health benefits to a variety of psychiatric symptoms (Perica and Delas 2011). Taken together, the above findings suggest the therapeutic potential of ω-3 fatty acid in the treatment of schizophrenia.
In addition to the above compounds, a number of other antioxidants such as glutathione (Berk et al. 2008b), rutin (Bishnoi et al. 2007), Ginkgo biloba (Singh et al. 2010), melatonin (Ortiz et al. 2008; Maldonado et al. 2009), hydroxytyrosol (Young et al. 2007), caffeic acid phenethyl ester (Ozyurt et al. 2007), resveratrol and quercetin (Dietrich-Muszalska and Olas 2009), and lycopene (Rao and Rao 2004) have also been suggested as alternative treatments in schizophrenia (reviewed by Bošković et al. 2011).
5.3 Antioxidant Interventions in Bipolar Disorder
As discussed above, alterations in lipid peroxidation and antioxidant enzymes have been found in subjects with bipolar disorder. In an effort to find the therapeutic potential of antioxidants in bipolar disorder, NAC has been extensively used as adjunctive therapy in bipolar disorder. A recent systematic review of clinical trials showed that adjunct treatment of NAC with standard pharmacotherapies for bipolar disorder shows positive evidence with large effect sizes (Sarris et al. 2011). NAC as an add-on treatment was found to be beneficial in few individuals in relationship to mood and functional outcomes (Magalhães et al. 2011). It has been suggested that long-chain ω-3 fatty acid supplementation has therapeutic potential to improve the disease condition of both major depression and bipolar disorder (McNamara 2013). Increase in brain-derived neurotrophic factor (BDNF) expression following ω-3 fatty acids has been suggested as a possible mechanism that may mediate at least in part the enhancing effects of ω-3 fatty acids in bipolar disorder (Balanzá-Martínez et al. 2011). Frangou et al. (2006) reported a significant improvement in depressive symptoms with ethyl-EPA (ethyl-eicosapentaenoic acid) treatment compared with placebo in subjects with bipolar disorder. In addition, an open-label study with supplementation of 1.5–2 g/day of the ω-3 fatty acids for up to 6 months showed significant improvement in depressive symptoms in bipolar disorder subjects (Osher et al. 2005). Significant changes in mania and depression were reported in an open-label study supplemented with 360 mg of EPA per day and 1,560 mg of DHA (docosahexaenoic acid) per day for 6 weeks in juvenile bipolar disorder subjects (Clayton et al. 2009). Thus, ω-3 fatty acids’ intervention represents a promising therapeutic strategy for bipolar disorder.
5.4 Antioxidant Interventions in Major Depression
5.4.1 Omega-3 Fatty Acids
Increased ratio of ω-6/ω-3 PUFAs may contribute to an increased incidence of coronary artery disease (CAD) (Smith 1991; Linscheer and Vergroesen 1988). Moreover, it is now recognized that MDD is robustly associated with an increased risk of CAD. Thus, the increased ratio of ω-6/ω-3 PUFAs may be responsible for the association between MDD and CAD (Maes et al. 1996; Linscheer and Vergroesen 1988). The administration of ω-3 PUFAs has a demonstrated efficacy in reducing cardiac events and triglycerides with minimal side effects (O’Keefe and Harris 2000). The beneficial effect of dietary and supplemental ω-3 fatty acids on CAD was further supported by a recent meta-analysis of 11 randomized controlled trials of both EPA + DHA and alpha-linolenic acid (Bucher et al. 2002). Several potential mechanisms including hypotriglyceridemic, antithrombogenic, antiarrhythmic, and antiatherogenic properties might be responsible for the protective effect of ω-3 fatty acids on CAD (Connor 2000).
In addition, there have been promising results for the use of low-dose ethyl-EPA in treatment-resistant unipolar depression (Peet and Horrobin 2002; Emsley et al. 2003). The effect appears to be specific to EPA, and not DHA (Marangell et al. 2003; Ross et al. 2007; Martins 2009). There also appear to be dose-specific effects; high-dose EPA may not be effective (EPA 6 g/day) (Post et al. 2003). Of particular note is the onset of response with EPA. Peet and Horrobin (2002) found significant reduction in severity of depressed mood as early as 2 weeks and maximally at 4 weeks. Emsley et al. (2003) found significant treatment response at 4 weeks. Thus, response to EPA occurs relatively rapidly. This may be important in managing patients who are not responding to conventional treatments and remain at risk for complications of depression, such as suicide. In the above placebo-controlled trials, there were no dropouts due to EPA-related side effects. An additional advantage is that EPA is not known to alter levels of psychotropic drugs used in treatment of depression. Epidemiological data suggests that there is an inverse relation between risk of depression and postpartum depression and fish consumption (Hibbeln and Salem 1995).
Recently, a meta-analysis study has shown that supplements containing EPA ≥ 60 % of total EPA + DHA, in a dose range of 200–2,200 mg/d of EPA in excess of DHA, were effective against primary depression (Sublette et al. 2011), which is in accordance with an early meta-regression analysis from those double-blind placebo-controlled clinical trials by Ross et al. (2007). On the other hand, another recent systematic review and meta-analyses by Bloch and Hannestad (2011) indicated only a small, nonsignificant, benefit of ω-3 fatty acids treatment in major depression. However, Martins et al. (2012) questioned the validity of their conclusions on the basis of inclusion/exclusion criteria, study subgroup selection, strategy for selecting outcome measures, standard mean difference estimates, and choice of effect modifiers.
5.4.2 Zinc Supplement
Zinc is an essential metal, which plays an important role in improving depressive symptoms (Maes et al. 2011). Zinc has been found to have antidepressive effects by normalizing antioxidant concentrations (Maes et al. 2011). People with depression have significantly lower serum zinc levels than controls (Maes et al. 1994; McLoughlin and Hodge 1990. The transport of zinc to the brain occurs by crossing the blood–brain and blood–cerebrospinal fluid barriers, concentrating in areas such as the hippocampus, amygdala, and neocortex (Frederickson et al. 2000; Takeda and Tamano 2009). Zinc plays an essential role in adult hippocampal neurogenesis and synaptogenesis (Szewczyk et al. 2011). Chronic zinc treatment in high doses is required to increase BDNF mRNA and protein levels in the frontal cortex, while the hippocampus BDNF expression increased with lower, more acute doses of zinc (Cichy et al. 2009; Franco et al. 2008; Nowak et al. 2004; Sowa-Kucma et al. 2008). Earlier studies found that zinc can also regulate nerve growth factor (NGF) directly via the modulation of the zinc binding site (Szewczyk et al. 2011). The induction of NGF by zinc might serve to support neuron survival (Chen and Liao 2003; Mocchegiani et al. 2005).
5.4.3 N-Acetylcysteine (NAC)
In addition to schizophrenia and bipolar disorder, low levels of glutathione (GSH) were also found in postmortem prefrontal cortex from patients with depression (Gawryluk et al. 2011). As described above, the use of NAC in restoring GSH levels has been well established (Dodd et al. 2008). Previously, Berk et al. (2008a) have shown that NAC treatment caused a significant improvement on the Montgomery–Asberg Depression Rating Scale (MADRS) and most secondary scales at end point. A recent open-label study by this same research group also found a robust decrease in depression scores with NAC treatment in 149 individuals with moderate depression for 2 months (Berk et al. 2011).
6 Conclusion
Given the complex pathophysiology of the neuropsychiatric disorders, it is difficult to suggest that a single mechanism could explain the diversity of impairments found in these disorders. As discussed above, a large body of studies provides compelling evidence to show that oxidative stress plays an important role in the pathophysiology of schizophrenia, bipolar disorder, and major depression. However, the biochemical mechanisms underlying these psychiatric disorders remain unclear. A number of studies have suggested that important relationships exist between redox signaling molecules and neuroplasticity-related molecules. For example, neurotrophic factors such as BDNF are known to rescue cerebellar granule neurons from oxidative stress-mediated cellular damage (Skaper et al. 1998). In addition, both peripheral and brain levels of neurotrophins are lower in subjects with schizophrenia or mood disorder (Pillai 2008). It would be important to determine whether increases in oxidative stress lead to reductions in neurotrophin levels in these psychiatric disorders. As oxidative stress is known to disturb the neuroplasticity, attempts to normalize such impairments are of great therapeutic value in psychiatry research. A few such studies using antioxidants as adjunctive therapy have shown promising leads in the treatment of schizophrenia and mood disorder. However, additional studies using large number of subjects are required to identify further viable therapeutic strategies to restore the oxidative stress-induced cellular, molecular, and behavioral deficits. Such studies will provide exciting opportunity for the treatment and long-term management of neuropsychiatric disorders.
Abbreviations
- 1O2 :
-
Singlet oxygen
- AA:
-
Arachidonic acid
- BDNF:
-
Brain-derived neurotrophic factor
- BPRS:
-
Brief psychiatric rating scale
- CAD:
-
Coronary artery disease
- CAT:
-
Catalase
- DHA:
-
Docosahexaenoic acid
- EPA:
-
Eicosapentaenoic acid
- ethyl-EPA:
-
Ethyl-eicosapentaenoic acid
- GPx:
-
Glutathione peroxidase
- GSH:
-
Glutathione
- H2O2 :
-
Hydrogen peroxide
- IL-1:
-
Interleukin-1
- IL-6:
-
Interleukin-6
- LTB4 :
-
Leukotriene B4
- MADRS:
-
Montgomery–Asberg Depression Rating Scale
- MDD:
-
Major depressive disorder
- NAC:
-
N-Acetylcysteine
- NGF:
-
Nerve growth factor
- NO‾:
-
Nitric oxide
- NO‾2 :
-
Nitrate
- NO‾3 :
-
Nitrite
- NO•:
-
Nitric oxide
- O2 − :
-
Superoxide anion
- OH•:
-
Hydroxyl
- PANSS:
-
Positive and Negative Syndrome Scale
- PGE2 :
-
Prostaglandin E2
- PUFAs:
-
Polyunsaturated fatty acids
- RBC:
-
Red blood cell
- ROS:
-
Reactive oxygen species
- SOD:
-
Superoxide dismutase
- TAS:
-
Total antioxidant status
- TD:
-
Tardive dyskinesia
- TNF-α:
-
Tumor necrosis factor-α
References
Abdalla DS, Manteiro HP, Olivera JA, Bechara EJ (1986) Activities of superoxide dismutase and glutathione peroxidase in schizophrenic and manic depressive patients. Clin Chem 32:805–807
Adler LA, Peselow E, Rotrosen J, Duncan E, Lee M, Rosenthal M, Angrist B (1993) Vitamin E treatment of tardive dyskinesia. Am J Psychiatry 150:1405–1407
Amminger GP, Schäfer MR, Papageorgiou K, Klier CM, Cotton SM, Harrigan SM, Mackinnon A, McGorry PD, Berger GE (2010) Long-chain omega-3 fatty acids for indicated prevention of psychotic disorders: a randomized, placebo-controlled trial. Arch Gen Psychiatry 67:146–154
Andreazza AC, Kauer-Sant’anna M, Frey BN, Bond DJ, Kapczinski F, Young LT, Yatham LN (2008) Oxidative stress markers in bipolar disorder: a meta-analysis. J Affect Disord 111:135–144
Andreazza AC, Kapczinski F, Kauer-Sant’Anna M, Walz JC, Bond DJ, Goncalves CA, Young LT, Yatham LN (2009) 3-Nitrotyrosine and glutathione antioxidant system in patients in the early and late stages of bipolar disorder. J Psychiatry Neurosci 34:263–271
Aruoma OI, Halliwell B, Hoey BM et al (1989) The antioxidant action of N-acetylcysteine: its reaction with hydrogen peroxide, hydroxyl radical, superoxide, and hypochlorous acid. Free Radic Biol Med 6:593–597
Arvindakshan M, Sitasawad S, Debsikdar V, Ghate M, Evans D, Horrobin DF, Bennett C, Ranjekar PK, Mahadik SP (2003) Essential polyunsaturated fatty acid and lipid peroxide levels in never-medicated and medicated schizophrenia patients. Biol Psychiatry 53:56–64
Balanza-Martinez V, Fries GR, Colpo GD, Silveira PP, Portella AK, Tabares-Seisdedos R, Kapczinski F (2011) Therapeutic use of omega-3 fatty acids in bipolar disorder. Expert Rev Neurother 11:1029–1047
Belmaker RH (2004) Bipolar disorder. N Engl J Med 351:476–486
Ben-Shachar D, Laifenfeld D (2004) Mitochondria, synaptic plasticity, and schizophrenia. Int Rev Neurobiol 59:273–296
Berk M, Copolov D, Dean O, Lu K, Jeavons S, Schapkaitz I, Anderson-Hunt M, Judd F, Katz F, Katz P, Ording-Jespersen S, Little J, Conus P, Cuenod M, Do KQ, Bush AI (2008a) N-acetyl cysteine as a glutathione precursor for schizophrenia–a double-blind, randomized, placebo-controlled trial. Biol Psychiatry 64:361–368
Berk M, Ng F, Dean O, Dodd S, Bush AI (2008b) Glutathione: a novel treatment target in psychiatry. Trends Pharmacol Sci 29:346–351
Berk M, Dean O, Cotton SM, Gam CS, Kapczinski F, Fernandes BS, Kohlmann K, Jeavons S, Hewitt K, Allwang C, Cobb H, Bush AI, Schapkaitz I, Dodd S, Malhi GS (2011) The efficacy of N-acetylcysteine as an adjunctive treatment in bipolar depression: an open label trial. J Affect Disord 135:389–394
Bishnoi M, Chopra K, Kulkarni S (2007) Protective effect of rutin, a polyphenolic flavonoid against haloperidol-induced orofacial dyskinesia and associated behavioural, biochemical and neurochemical changes. Fundam Clin Pharmacol 21:521–529
Bloch MH, Hannestad J (2011) Omega-3 fatty acids for the treatment of depression: systematic review and meta-analysis. Mol Psychiatry. doi:10.1038/mp.2011.100 [Epub ahead of print]
Bošković M, Vovk T, Plesnicar BK, Grabnar I (2011) Oxidative stress in schizophrenia. Curr Neuropharmacol 9:301–312
Brown K, Reid A, White T, Henderson T, Hukin S, Johnstone C, Glen A (1998) Vitamin E, lipids, and lipid peroxidation products in tardive dyskinesia. Biol Psychiatry 43:863–867
Bubber P, Tang J, Haroutunian V, Xu H, Davis KL, Blass JP, Gibson GE (2004) Mitochondrial enzymes in schizophrenia. J Mol Neurosci 24(2):315–321
Bucher HC, Hengstler P, Schindler C et al (2002) N-3 polyunsaturated fatty acids in coronary heart disease: a meta-analysis of randomized controlled trials. Am J Med 112:298–304
Bulut M, Savas HA, Altindag A, Virit O, Dalkilic A (2009) Beneficial effects of N-acetylcysteine in treatment resistant schizophrenia. World J Biol Psychiatry 10:626–628
Calder PC (1998) Immunoregulatory and anti-inflammatory effects of n-3 polyunsaturated fatty acids. Braz J Med Biol Res 31:467–490
Carlsson A, Waters N, Carlsson ML (1999) Neurotransmitter interactions in schizophrenia–therapeutic implications. Biol Psychiatry 46:1388–1395
Chen CJ, Liao SL (2003) Neurotrophic and neurotoxic effects of zinc on neonatal cortical neurons. Neurochem Int 42:471–479
Cichy A, Sowa-Kucma M, Legutko B, Pomierny-Chamiolo L, Siwek A, Piotrowska A, Szewczyk B, Poleszak E, Pilc A, Nowak G (2009) Zinc-induced adaptive changes in NMDA/glutamatergic and serotonergic receptors. Pharmacol Rep 61:1184–1191
Clayton EH, Hanstock TL, Hirneth SJ, Kable CJ, Garg ML, Hazell PL (2009) Reduced mania and depression in juvenile bipolar disorder associated with long-chain omega-3 polyunsaturated fatty acid supplementation. Eur J Clin Nutr 63:1037–1040
Connor WE (2000) Importance of n-3 fatty acids in health and disease. Am J Clin Nutr 71:171S–175S
Corrigan FM, Van Rhijn AG, Mackay AV, Skinner ER, Horrobin DF (1993) Vitamin E treatment of tardive dyskinesia (letter). Am J Psychiatry 150:991–992
Craddock RM, Lockstone HE, Rider DA, Wayland MT, Harris LJ, McKenna PJ, Bahn S (2007) Altered T-cell function in schizophrenia: a cellular model to investigate molecular disease mechanisms. PLoS One 2:e692
Dakhale GN, Khanzode SD, Khanzode SS, Saoji A (2005) Supplementation of vitamin C with atypical antipsychotics reduces oxidative stress and improves the outcome of schizophrenia. Psychopharmacology (Berl) 182:494–498
Dean OM, van den Buuse M, Berk M, Copolov DL, Mavros C, Bush AI (2011) N-acetyl cysteine restores brain glutathione loss in combined 2-cyclohexene-1-one and D-amphetamine-treated rats: relevance to schizophrenia and bipolar disorder. Neurosci Lett 499:149–153
Dietrich-Muszalska A, Olas B (2009) Inhibitory effects of polyphenol compounds on lipid peroxidation caused by antipsychotics (haloperidol and amisulpride) in human plasma in vitro. World J Biol Psychiatry 11:276–281
Dodd S, Dean O, Copolov DL, Malhi GS, Berk M (2008) N-acetylcysteine for antioxidant therapy: pharmacology and clinical utility. Expert Opin Biol Ther 8:1955–1962
Edwards R, Peet M, Shay J, Horrobin DF (1998) Omega-3 polyunsaturated fatty acid levels in the diet and in red blood cell membranes of depressed patients. J Affect Disord 48:149–155
Elkashef AM, Wyatt RJ (1999) Tardive dyskinesia: possible involvement of free radicals and treatment with vitamin E. Schizophr Bull 25:731–740
Emsley R, Oosthuizen P, van Rensburg SJ (2003) Clinical potential of omega-3 fatty acids in the treatment of schizophrenia. CNS Drugs 17:1081–1091
Franco JL, Posser T, Brocardo PS, Trevisan R, Uliano-Silva M, Gabilan NH, Santos AR, Leal RB, Rodrigues AL, Farina M, Dafre AL (2008) Involvement of glutathione, ERK1/2 phosphorylation and BDNF expression in the antidepressant-like effect of zinc in rats. Behav Brain Res 188:316–323
Frangou S, Lewis M, McCrone P (2006) Efficacy of ethyl-eicosapentaenoic acid in bipolar depression: randomised double-blind placebo-controlled study. Br J Psychiatry 188:46–50
Frederickson CJ, Suh SW, Silva D, Thompson RB (2000) Importance of zinc in the central nervous system: the zinc-containing neuron. J Nutr 130:1471S–1483S
Galecki P, Szemraj J, Bienkiewicz M, Florkowski A, Galecka E (2009) Lipid peroxidation and antioxidant protection in patients during acute depressive episodes and in remission after fluoxetine treatment. Pharmacol Rep 61:436–447
Gawryluk JW, Wang JF, Andreazza AC, Shao L, Young LT (2011) Decreased levels of glutathione, the major brain antioxidant, in post-mortem prefrontal cortex from patients with psychiatric disorders. Int J Neuropsychopharmacol 14:123–130
Goff DC, Tsai G, Beal MF, Coyle JT (1995) Tardive dyskinesia and substrates of energy metabolism in CSF. Am J Psychiatry 152:1730–1736
Golse B, Debray-Ritzen P, Puget K, Michelson AM (1977) Analysis of platelet superoxide dismutase 1 in the development of childhood psychoses. Nouv Presse Med 6:2449
Hedelin M, Löf M, Olsson M, Lewander T, Nilsson B, Hultman CM, Weiderpass E (2010) Dietary intake of fish, omega-3, omega-6 polyunsaturated fatty acids and vitamin D and the prevalence of psychotic-like symptoms in a cohort of 33,000 women from the general population. BMC Psychiatry 10:38
Herken H, Uz E, Ozyurt H, Akyol O (2001) Red blood cell nitric oxide levels in patients with schizophrenia. Schizophr Res 52:289–290
Hibbeln JR (1998) Fish consumption and major depression. Lancet 351:1213
Hibbeln JR, Salem N (1995) Dietary polyunsaturated fatty acid and depression: when cholesterol does not satisfy. Am J Clin Nutr 62:1–9
Jakob H, Beckmann H (1986) Prenatal developmental disturbances in the limbic allocortex in schizophrenics. J Neural Transm 65:303–326
James MJ, Gibson RA, Cleland LG (2000) Dietary polyunsaturated fatty acids and inflammatory mediator production. Am J Clin Nutr 71:343S–348S
Kendler KS (2003) The genetics of schizophrenia: chromosomal deletions, attentional disturbances, and spectrum boundaries. Am J Psychiatry 160:1549–1553
Kodydkova J, Vavrova L, Zeman M, Jirak R, Macasek J, Stankova B, Tvrzicka E, Zak A (2009) Antioxidative enzymes and increased oxidative stress in depressive women. Clin Biochem 42:1368–1374
Kornhuber J, Weller M (1994) Current status of biochemical hypotheses in the pathogenesis of schizophrenia. Nervenarzt 65:741–754
Kuloglu M, Ustundag B, Atmaca M, Canatan H, Tezcan AE, Cinkilinc N (2002) Lipid peroxidation and antioxidant enzyme levels in patients with schizophrenia and bipolar disorder. Cell Biochem Funct 20:171–175
Kupfer DJ (2005) The increasing medical burden in bipolar disorder. JAMA 293:2528–2530
Li XF, Zheng YL, Xiu MH, da Chen C, Kosten TR, Zhang XY (2011) Reduced plasma total antioxidant status in first-episode drug-naive patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry 35:1064–1067
Linscheer WG, Vergroesen AJ (1988) Lipids. In: Shils ME, Young VR (eds) Modern nutrition in health and disease. Lea and Febiger, Philadelphia, pp 72–107
Maes M, D’Haese PC, Scharpé S, D’Hondt P, Cosyns P, De Broe ME (1994) Hypozincemia in depression. J Affect Disord 31:135–140
Maes M, Smith R, Christophe A, Cosyns P, Desnyder R, Meltzer HY (1996) Fatty acid composition in major depression: decreased ω3 fractions in cholesteryl esters and increased c20:4ω6/c20:5ω3 ratio in cholesteryl esters and phospholipids. J Affect Disord 38:35–46
Maes M, Christophe A, Bosmans E, Lin A, Neels H (2000) In humans, serum polyunsaturated fatty acid levels predict the response of proinflammatory cytokines to psychologic stress. Biol Psychiatry 47:910–920
Maes M, Galecki P, Chang YS, Berk M (2011) A review on the oxidative and nitrosative stress (O&NS) pathways in major depression and their possible contribution to the (neuro)degenerative processes in that illness. Prog Neuropsychopharmacol Biol Psychiatry 35:676–692
Magalhaes PV, Dean OM, Bush AI, Copolov DL, Malhi GS, Kohlmann K, Jeavons S, Schapkaitz I, Anderson-Hunt M, Berk M (2011) N-acetylcysteine for major depressive episodes in bipolar disorder. Rev Bras Psiquiatr 33:374–378
Mahadik SP, Yao JK (2006) Phospholipids in schizophrenia. In: Lieberman JA, Stroup TS, Perkins DO (eds) Textbook of schizophrenia. The American Psychiatric Publishing, Inc., Washington, DC, pp 117–135
Mahadik SP, Evans D, Lal H (2001) Oxidative stress and role of antioxidant and omega-3 essential fatty acid supplementation in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry 25:463–493
Maldonado MD, Reiter RJ, Perez-San-Gregorio MA (2009) Melatonin as a potential therapeutic agent in psychiatric illness. Hum Psychopharmacol 24:391–400
Marangell LB, Martinez JM, Zboyan HA, Kertz B, Kim HF, Puryear LJ (2003) A double-blind, placebo-controlled study of the omega-3 fatty acid docosahexaenoic acid in the treatment of major depression. Am J Psychiatry 160:996–998
Marazziti D, Baroni S, Picchetti M, Landi P, Silvestri S, Vatteroni E, Catena Dell’Osso M (2012) Psychiatric disorders and mitochondrial dysfunctions. Eur Rev Med Pharmacol Sci 16:270–275
Martins JG (2009) EPA but not DHA appears to be responsible for the efficacy of omega-3 long chain polyunsaturated fatty acid supplementation in depression: evidence from a meta-analysis of randomized controlled trials. J Am Coll Nutr 28:525–542
Martins JG, Bentsen H, Puri BK (2012) Eicosapentaenoic acid appears to be the key omega-3 fatty acid component associated with efficacy in major depressive disorder: a critique of Bloch and Hannestad and updated meta-analysis. Mol Psychiatry. doi:10.1038/mp.2012.25
McCreadie RG, MacDonald E, Wiles D, Campbell G, Paterson JR (1995) The Nithsdale Schizophrenia Surveys. XIV: plasma lipid peroxide and serum vitamin E levels in patients with and without tardive dyskinesia, and in normal subjects. Br J Psychiatry 167:610–617
McLoughlin IJ, Hodge JS (1990) Zinc in depressive disorder. Acta Psychiatr Scand 82:451–453
McNamara RK (2013) Long-chain omega-3 fatty acid deficiency in mood disorders: rationale for treatment and prevention. Curr Drug Discov Technol 10:233–244
Merikangas KR, Ames M, Cui L, Stang PE, Ustun TB, Von Korff M, Kessler RC (2007) The impact of comorbidity of mental and physical conditions on role disability in the US adult household population. Arch Gen Psychiatry 64:1180–1188
Mocchegiani E, Bertoni-Freddari C, Marcellini F, Malavolta M (2005) Brain, aging and neurodegeneration: role of zinc ion availability. Prog Neurobiol 75:367–390
Nowak G, Legutko B, Szewczyk B, Papp M, Sanak M, Pilc A (2004) Zinc treatment induces cortical brain-derived neurotrophic factor gene expression. Eur J Pharmacol 492:57–59
O’Keefe JH, Harris WS (2000) From inuit to implementation: omega-3 fatty acids come of age. Mayo Clin Proc 75:607–614
Ortiz GG, Benitez-King GA, Rosales-Corral SA, Pacheco-Moises FP, Velazquez-Brizuela IE (2008) Cellular and biochemical actions of melatonin which protect against free radicals: role in neurodegenerative disorders. Curr Neuropharmacol 6:203–214
Osher Y, Bersudsky Y, Belmaker RH (2005) Omega-3 eicosapentaenoic acid in bipolar depression: report of a small open-label study. J Clin Psychiatry 66:726–729
Othmen L, Mechri A, Fendri C, Bost M, Chazot G, Gaha L, Kerkeni A (2008) Altered antioxidant defense system in clinically stable patients with schizophrenia and their unaffected siblings. Prog Neuropsychopharmacol Biol Psychiatry 32:155–159
Ozyurt B, Ozyrut H, Akpolat N, Erdogan H, Sarsilmaz M (2007) Oxidative stress in prefrontal cortex of ret exposed to MK-801 and protective effects of CAPE. Prog Neuropsychopharmacol Biol Psychiatry 31:832–838
Pearce BD (2001) Schizophrenia and viral infection during neurodevelopment: a focus on mechanisms. Mol Psychiatry 6:634–646
Peet M, Horrobin DF (2002) A dose-ranging study of the effects of ethyl-eicopentaenoic acid in patients with on-going depression in spite of apparently adequate treatment with standard drugs. Arch Gen Psychiatry 59:913–919
Peet M, Laugharne J, Rangarajan N, Reynolds GP (1993) Tardive dyskinesia, lipid peroxidation, and sustained amelioration with vitamin E treatment. Int Clin Psychopharmacol 8:151–153
Peet M, Murphy B, Shay J, Horrobin DF (1998) Depletion of omega-3 fatty acid levels in red blood cell membranes of depressive patients. Biol Psychiatry 43:315–319
Perica MM, Delas I (2011) Essential fatty acids and psychiatric disorders. Nutr Clin Pract 26:409–425
Pillai A (2008) Brain-derived neurotropic factor/TrkB signaling in the pathogenesis and novel pharmacotherapy of schizophrenia. Neurosignals 16:183–193
Post RM, Leverich GS, Altshuler LL et al (2003) An overview of recent findings of the Stanley Foundation Bipolar Network (Part I). Bipolar Disord 5:310–319
Raffa M, Atig F, Mhalla A, Kerkeni A, Mechri A (2011) Decreased glutathione levels and impaired antioxidant enzyme activities in drug-naïve first-episode schizophrenic patients. BMC Psychiatry 11:124
Ranjekar PK, Hinge A, Hegde MV, Ghate M, Kale A, Sitasawad S, Wagh UV, Debsikdar VB, Mahadik SP (2003) Decreased antioxidant enzymes and membrane essential polyunsaturated fatty acids in schizophrenic and bipolar mood disorder patients. Psychiatry Res 121:109–122
Rao A, Rao L (2004) Lycopene and human health. Curr Top Nutraceut Res 2:127–136
Reddy R, Sahebarao MP, Mukherjee S, Murthy JN (1991) Enzymes of the antioxidant defense system in chronic schizophrenic patients. Biol Psychiatry 30:409–412
Ross BM, Seguin J, Sieswerda LE (2007) Omega-3 fatty acids as treatments for mental illness: which disorder and which fatty acid? Lipids Health Dis 6:21
Sarris J, Mischoulon D, Schweitzer I (2011) Adjunctive nutraceuticals with standard pharmacotherapies in bipolar disorder: a systematic review of clinical trials. Bipolar Disord 13:454–465
Savas HA, Gergerlioglu HS, Armutcu F, Herken H, Yilmaz HR, Kocoglu E, Selek S, Tutkun H, Zoroglu SS, Akyol O (2006) Elevated serum nitric oxide and superoxide dismutase in euthymic bipolar patients: impact of past episodes. World J Biol Psychiatry 7:51–55
Seko C, Ninno N, Nakamura K (1997) Relation between fatty acid composition in blood and depressive symptoms in the elderly. Jpn J Hyg 52:330
Shriqui CL, Bradwejn J, Annable L, Jones BD (1992) Vitamin E in the treatment of tardive dyskinesia: a double-blind placebo-controlled study. Am J Psychiatry 149:391–393
Singh V, Singh SP, Chan K (2010) Review and meta-analysis of usage of ginkgo as an adjunct therapy in chronic schizophrenia. Int J Neuropsychopharmacol 13:257–271
Skaper SD, Floreani M, Negro A, Facci L, Giusti P (1998) Neurotrophins rescue cerebellar granule neurons from oxidative stress-mediated apoptotic death: selective involvement of phosphatidylinositol 3-kinase and the mitogen-activated protein kinase pathway. J Neurochem 70:1859–1868
Smith RS (1991) The macrophage theory of depression. Med Hypotheses 35:298–306
Sowa-Kucma M, Legutko B, Szewczyk B, Novak K, Znojek P, Poleszak E, Papp M, Pilc A, Nowak G (2008) Antidepressant-like activity of zinc: further behavioral and molecular evidence. J Neural Transm 115:1621–1628
Soyland E, Lea T, Sandstand B, Drevon A (1994) Dietary supplementation with very long-chain n-3 fatty acids in man decreases expression of the interleukin-2 receptor (CD25) on mitogen-stimulated lymphocytes from patients with inflammatory skin disease. Eur J Clin Invest 24:236–242
Stoklasova A, Zapletalek M, Kudrnova K, Randova Z (1986) Glutathione peroxidase activity in the blood in chronic schizophrenia. Sb Ved Pr Lek Fak Karlovy Univerzity Hradci Kralove Suppl 29:103–108
Sublette ME, Ellis SP, Geant AL, Mann JJ (2011) Meta-analysis of the effects of eicosapentaenoic acid (EPA) in clinical trials in depression. J Clin Psychiatry 72:1577–1584
Suboticanec K, Folnegovic V, Korbar M, Mestrovic B, Buzina R (1990) Vitamin C status in chronic schizophrenia. Biol Psychiatry 28:959–966
Surapaneni K (2007) Status of lipid peroxidation, glutathione, ascorbic acid, vitamin E and antioxidant enzymes in schizophrenic patients. J Clin Diagn Res 1:39–44
Szewczyk B, Kubera M, Nowak G (2011) The role of zinc in neurodegenerative inflammatory pathways in depression. Prog Neuropsychopharmacol Biol Psychiatry 35:693–701
Takeda A, Tamano H (2009) Insight into zinc signaling from dietary zinc deficiency. Brain Res Rev 62:33–44
Taneli F, Pirildar S, Akdeniz F, Uyanik BS, Ari Z (2004) Serum nitric oxide metabolite levels and the effect of antipsychotic therapy in schizophrenia. Arch Med Res 35:401–405
Tashiro T, Yamamori H, Takagi K, Hayashi N, Furukawa K, Nakajima N (1998) N-3 versus n-6 polyunsaturated fatty acids in critical illness. Nutrition 14:551–553
Thome J, Foley P, Riederer P (1998) Neurotrophic factors and the maldevelopmental hypothesis of schizophrenic psychoses. Review article. J Neural Transm 105:85–100
Whatley SA, Curti D, Das Gupta F, Ferrier IN, Jones S, Taylor C, Marchbanks RM (1998) Superoxide, neuroleptics and the ubiquinone and cytochrome b5 reductases in brain and lymphocytes from normals and schizophrenic patients. Mol Psychiatry 3:227–237
Yao JK, Keshavan MS (2011) Antioxidants, redox signaling, and pathophysiology in schizophrenia: an integrative view. Antioxid Redox Signal 15:2011–2035
Yao JK, Reddy R, McElhinny LG, van Kammen DP (1998a) Reduced status of plasma total antioxidant capacity in schizophrenia. Schizophr Res 32:1–8
Yao JK, Reddy R, McElhinny LG, van Kammen DP (1998b) Effect of haloperidol on antioxidant defense system enzymes in schizophrenia. J Psychiatr Res 32:385–391
Yao JK, Reddy R, van Kammen DP (1998c) Reduced level of plasma antioxidant uric acid in schizophrenia. Psychiatry Res 80:29–39
Yao JK, Reddy R, van Kammen DP (1999) Human plasma glutathione peroxidase and symptom severity in schizophrenia. Biol Psychiatry 45:1512–1515
Yao JK, Reddy R, van Kammen DP (2000) Abnormal age-related changes of plasma antioxidant proteins in schizophrenia. Psychiatry Res 97:137–151
Yao JK, Leonard S, Reddy RD (2004) Increased nitric oxide radicals in postmortem brain from patients with schizophrenia. Schizophr Bull 30:923–934
Young J, Wahle K, Boyle S (2007) Cytoprotective effects of phenolic antioxidants and essential fatty acids in human blood monocyte and neuroblastoma cell lines: surrogates for neurological damage in vivo. Prostaglandins Leukot Essent Fatty Acids 78:45–59
Zhang ZX, Yang XG, Xia YM, Chen XS (1998) Progress in the study of mammalian selenoprotein. Sheng Li Ke Xue Jin Zhan 29:29–34
Zhang M, Zhao Z, He L, Wan C (2010) A meta-analysis of oxidative stress markers in schizophrenia. Sci China Life Sci 53:112–124
Acknowledgments
This material is based upon work supported in part by the grants from the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, Biomedical Laboratory R&D [Merit Reviews and Senior Research Career Scientist Award (JKY)], VA Pittsburgh Healthcare System, National Institute of Health [MH58141 (JKY) and MH087857 (AP)], and American Heart Association (JKY). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The contents of this article do not represent the views of the Department of Veterans Affairs or the United States Government.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Pillai, A., Yao, J.K. (2015). Antioxidant Interventions in Neuropsychiatric Disorders. In: Dietrich-Muszalska, A., Chauhan, V., Grignon, S. (eds) Studies on Psychiatric Disorders. Oxidative Stress in Applied Basic Research and Clinical Practice. Humana Press, New York, NY. https://doi.org/10.1007/978-1-4939-0440-2_25
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0440-2_25
Published:
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-4939-0439-6
Online ISBN: 978-1-4939-0440-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)