
Abstract
Gastric varices are present in about 20 % of cirrhotic patients with a low incidence of bleeding (10–36 %) but high rebleeding rates (34–89 %). The classification according to their location has an important role in the management. No guidelines are available for primary prophylaxis of gastric variceal bleeding but cyanoacrylate glue seems to be more effective than beta-blockers. Treatment of acute hemorrhage may be performed by tissue adhesives injection, thrombin injection, endoscopic sclerotherapy, variceal band, and loop ligation. In case of failure to control acute bleeding, rescue radiologic approaches include TIPS, balloon-occluded retrograde transvenous obliteration (BRTO), balloon-occluded endoscopic injection sclerotherapy (BOIS), balloon-occluded antegrade transvenous obliteration (BATO). Surgery may be indicated only when all other techniques have failed in patients with Child-Turcotte-Pugh class A cirrhosis or in patients who live at a great distance from centers that can adequately manage variceal bleeding. In the setting of secondary prophylaxis endoscopic therapy is better than drug therapy and the use of tissue adhesive is the modality of choice; there are also clear recommendations for the routine use of radiologic techniques, such as TIPS, BRTO, and BO-EIS. Ectopic varices (EcV) are dilated portosystemic collateral veins located in sites other than the gastroesophageal region and their bleeding constitutes 1–5 % of all variceal bleeds in patients with intrahepatic portal hypertension and 20–30 % of those with extrahepatic portal hypertension. No primary or secondary prophylaxis for EcV is recommended. The management of acute ectopic variceal bleed requires a multidisciplinary approach that includes pharmacological, endoscopic, and angiographic methods with surgery for highly selected cases.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Portal hypertension is characterized by the presence of varices, the most common being esophageal varices. At the same time the presence of varices in stomach (gastric varices) and other sites (called ectopic varices) are other features of portal hypertension. Gastric varices (GV) are found in 20 % of patients with portal hypertension [1]. Ectopic varices (EcV) are dilated portosystemic collaterals located at unusual sites other than the gastroesophageal region; they constitute 1–5 % of all variceal bleeds in patients with intrahepatic portal hypertension, and 20–30 % of those with extrahepatic portal hypertension [2].
The hemodynamics of gastric varices differ from esophageal varices in that they do not correlate with HVPG, bleeding from GV is more severe with high mortality, and treatment is often challenging [3]. Varices developing at unusual sites, i.e., ectopic varices, are difficult to localize and manage because of their varied clinical presentations [4]. Hence, algorithms and stepwise management of these patients are needed.
Gastric Varices
Incidence and Prevalence
Gastric varices (GV) are found in 20 % of patients with portal hypertension [1]. The location of GV has important role in the management. The 2-year incidence of variceal bleeding from IGV1 and GOV2 type were higher (78 % and 54 %, respectively) than the lesser curve (GOV1) varices (28 %) [1]. IGV2 bleed only rarely (9 %) [1]. The overall rebleeding rate of gastric varices after complete variceal obliteration is variable and ranges from 10 to 42 % [5]. With the advancement in endoscopic technique and salvage therapy, the 6 weeks mortality from acute gastroesophageal variceal bleed has decreased from 40 % to approximately 15 % in recent years but mortality related to failure to control bleeding or early rebleeding (i.e., within the first 5 days after the initial bleeding episode) still remains high (up to 30–40 %) [6, 7].
Diagnosis
Gastric varices are diagnosed by endoscopy. Endoscopic ultrasound (EUS) is the test of choice for differentiation of GV from the gastric mucosal folds [8]. Alternatively, transabdominal ultrasound with Doppler, computed tomography (CT) scan with contrast, magnetic resonance angiography, portovenography, and interventional angiography can identify GV [9].
Classification
The most widely used classification system is Sarin’s classification as shown in Fig. 14.1. This has been recommended for use by APASL, AASLD, and BAVENO guidelines and by expert panels because it is easy to use, has good correlation with Pathophysiology, and guides therapy [10–12]. This classifies GVs on the basis of their location in the stomach and their relationship with EVs.

Sarin’s classification of gastric varices
Management
Primary Prophylaxis
Although primary prophylaxis has been studied and well established in managing esophageal varices, no guidelines are available for gastric varices. The hemodynamics of gastric varices differs from esophageal varices in that large gastric varices may develop at lower portal pressures due to the presence of gastrosystemic shunts. As gastric variceal bleed is more severe than bleeding from esophageal varices and associated with high mortality, primary prophylaxis should be considered for patients at high risk for bleeding (suggested to be those with an annual risk of ≥16 %) [13]. The therapeutic options include beta-blocker and/or cyanoacrylate glue. Data on primary prophylaxis for GV are very few. One recent RCT of primary prophylaxis by Mishra et al. [3] included 30 patients endoscopically treated with tissue adhesive, 27 patients treated with beta-blockers and 30 patients left untreated (p = 0.003). The overall bleeding rates were 10 % for patients treated with cyanoacrylate, 38 % for those on beta-blockers and 53 % for untreated patients. Overall mortality rates were 7 %, 17 %, and 26 %, respectively (p = 0.113).
Risk Factors for Gastric Variceal Hemorrhage include [3, 14–16]:
-
Location of gastric varices (IGV1 > GOV2 > GOV1)
-
Size of fundal varices (large > medium > small)
-
Severity of liver failure (Child class C > B > A)
-
Presence of red colour sign(RCS) over gastric varices
-
Concomitant hepatocellular carcinoma
-
Presence of portal hypertensive gastropathy
-
MELD score ≥ 17
Thus, patients with high risk gastric varices should receive primary prophylaxis. Cyanoacrylate injection should be the first line of treatment for primary prophylaxis of “high risk” GV. Whether combined treatment with cyanoacrylate injection and beta-blockers has any added advantages over either of treatment given alone needs to be studied.
Acute Variceal Bleed
Incidence of bleeding from gastric varices is relatively low (10–36 %). The rebleeding rate after control of acute bleeding is high (34–89 %) depending upon the treatment modality and subsequent follow-up protocol [17].
Clinical presentations of variceal bleed are hematemesis and/or melena and are described as next:
-
Acute variceal bleed: defined [10] as the bleed in a known or suspected case of portal hypertension, with the presence of hematemesis within 24 h of presentation, and/or ongoing melena, with last melanic stool within 24 h. The time of presentation is considered as T0 and any subsequent bout of hematemesis from T0 to 48 h of T0 will be considered as part of the same episode of acute variceal bleeding. Any bleeding occurring after 48 h will be considered as rebleeding.
-
Active bleeding: It is defined [10] based upon endoscopic finding as the presence of spurting or oozing from the varix. It is a predictor of failure to control bleed and early rebleed.
-
Recent bleed: Any clinically significant bleed occurring in the past 6 weeks of presentation [10].
-
Past bleed: A clinically significant bleed occurring more than 6 weeks prior to presentation [10].
The amount of blood loss should be quantified based upon the history and clinical presentation as this indirectly decides the urgency of the situation, guides therapy, and predicts the outcome. The patient should be assessed for the amount of blood loss as per history (amount of loss, passage of clots, vomiting in emergency room) and clinical signs (hypotension, tachycardia, diaphoresis, and mental state).
A protocol-based stepwise approach for acute gastric variceal bleeding is the key for optimal outcome. We propose the following algorithmic approach:
-
Step 1—resuscitation: It is the cornerstone to the success of endotherapy and survival. Initial resuscitative measures include protection of airway, breathing, and circulation.
-
Airway protection: Elective intubation prior to endotherapy should be done in patients with massive uncontrolled variceal bleeding, hepatic encephalopathy (grade III and IV), aspiration pneumonia, and in cases where there is difficulty in maintaining oxygen saturation above 90 % [10].
-
Fluid replacement: Colloids are preferred for volume resuscitation and crystalloids, particularly saline, should be avoided. The preferred maintenance fluid should be dextrose. The aim of volume replacement is to maintain systolic blood pressure around 90–100 mmHg, heart rate below 100 beats per minute, CVP 1–5 mmHg, diuresis of 40 mL/h.
-
Blood volume: Target hemoglobin level of around 8 g/dL and a hematocrit value of 24 %, depending on other factors, such as patient’s comorbidities, age, hemodynamic status, and the presence of ongoing bleeding [12]. Packed red blood cells (PRBC) is the preferred blood component. The existing data in the literature demonstrate that correction of coagulation parameters and thrombocytopenia has no role in the management of acute variceal bleed. The use of recombinant activated factor VII (rFVIIa) in cirrhotic patients with acute variceal bleeding is not recommended. The promising role of thromboelastogram (TEG) in the peri-transplant period can be extrapolated for TEG-guided correction of coagulopathy.
-
Antibiotics: Short-term antibiotic prophylaxis is mandatory as it reduces bacterial infections [18], variceal rebleeding, and death [19]. Quinolones and third-generation cephalosporins for a period of 5–7 days post-bleeding is recommended.
-
Vasoactive drugs: The existing evidence for the use of vasoactive drugs in acute gastric variceal bleeding is limited. The efficacy of these drugs in controlling acute esophageal variceal bleed favors their use in the setting of acute GV bleed. RCTs comparing different pharmacological agents (vasopressin, somatostatin, terlipressin, and octreotide) have shown no differences regarding control of hemorrhage and early rebleeding, but vasopressin is associated with a higher incidence of adverse events [20]. The clinical efficacy of terlipressin versus placebo has been assessed in seven RCTs, and in a meta-analysis which showed that terlipressin significantly reduced the incidence of failure to control bleeding and mortality [21]. Terlipressin is the only pharmacologic agent that has been shown to reduce mortality (about 34 % reduction). Vasoactive drug treatment should be continued for 2–5 days.
-
Balloon tamponade: Balloon tamponade is used as a bridge to definitive therapy. It is indicated in case of massive bleeding until endoscopy is done or after endoscopic therapy in case of failure to control bleeding until salvage treatment with TIPS/BRTO (transjugular intrahepatic portosystemic shunt/balloon-occluded retrograde transvenous obliteration) can be performed. Balloon tamponade is highly effective and hemostasis can be achieved in 80 % of cases, but has very high rebleeding rates if used as the sole therapy. Owing to its larger gastric balloon (600 mL), the Linton-Nachlas tube is more desirable for gastric variceal bleeding than the Sengstaken-Blakemore tube (200 mL). Careful placement is essential, especially in the sedated patient to reduce the risk of esophageal perforation from the inadvertent inflation of the gastric balloon in the esophagus.
-
-
Step 2—emergency endoscopy in AVB: Diagnosis of acute gastric variceal bleeding is done by upper GI endoscopy. The endoscopic findings and definitions for management of acute gastric variceal bleed are shown in Table 14.1. Endoscopic therapy is the only established, initial, and often the definitive treatment for acute gastric variceal bleed. Presence of high blood flow in the GVs, underlying shunt leading to profuse bleeding and rapid deterioration despite aggressive resuscitation suggest rapid and urgent endoscopic therapy. Accordingly, once the patient becomes hemodynamically stable endoscopic treatment (EVL, glue, and thrombin) should be done as soon as possible: preferably the door-to-scope time should be less than 6 h as suggested by APASL guideline [10]. The choice of endoscopic therapy used often depends on local availability and expertise. It is advisable to use large channel (6 mm) therapeutic UGI endoscope to be able to do rapid suction and cleaning. The patient position is often important and several maneuvers, such as turning the patient to the right lateral decubitus, or placing the patient in a nearly sitting posture, are helpful to ensure a clean fundus, in order to be able to achieve good vision and proper injection or band placement.
Table 14.1 The definitions for management of acute gastric variceal bleed -
Tissue adhesive/glue/cyanoacrylate/histoacryl: Endoscopic variceal obliteration (EVO) is done by using tissue adhesives like N-butyl-2-cyanoacrylate and 2-octyl-cyanoacrylate, the former being used more commonly. The standard forward viewing endoscope is used, with its tip lubricated (acetone), using a disposable sclerotherapy needle primed with saline, sterile water, or dextrose. 1 mL aliquots of undiluted cyanoacrylate are injected. As the needle is withdrawn, a steady stream of water flush must be maintained. Initial hemostasis rates are up to 90 % in most series. Tissue adhesive injection is considered the endoscopic treatment of choice because of superior hemostasis rate and lower rebleeding rate, and is comparable to TIPS in achieving initial hemostasis as shown in Table 14.2. Complications are well known but rare, and include Thromboembolic phenomena (splenic, renal, pulmonary, cerebral, spinal, and coronary), sticking of the needle in the varix, gastric ulceration, retro-gastric abscess, visceral fistula formation, bacteremia/sepsis, and rarely death. Embolic and thrombotic phenomena are associated with larger volume of glue injection and it is recommended not to exceed 2 mL per session [22]. However, higher volumes could be injected (2 mL/column) if more than one columns are to be injected. Repeat sessions should be performed after about 4 weeks, until endoscopic obliteration is achieved. The obturation of the varices is assessed by blunt palpation using the hub of the same injector with the needle retracted. EUS is useful to identify residual flow [8]. Rebleeding rates after cyanoacrylate injection vary from 7 to 65 % (with most of the larger series reporting rates below 15 %) and is often seen in patients with associated portal vein thrombosis (Table 14.2) [5, 23–26].
Table 14.2 Available randomized controlled trial studies of endoscopic treatment for gastric varices -
Thrombin: Thrombin is a locally acting hemostatic agent that converts fibrinogen to a fibrin clot and also helps in platelet aggregation. It is available as a sterile, lyophilized powder, pooled from human plasma donors. After reconstitution, it is injected through a disposable sclerotherapy needle with a standard gastroscope in aliquots of 1 mL (each mL = 250 U) and hemostasis occurs within 60 s. The average dose of injected thrombin is somewhere between 1,500 and 2,000 U [17]. The results of the use of thrombin in different studies are shown in Table 14.3 [27–32].
Table 14.3 Use of thrombin in different studies Thrombin injection is highly effective with initial hemostasis rates >90 % and rebleeding rates varying from 0 to 50 %. Procedure and injection-related side effects are infrequent. The drawbacks of thrombin are the cost, anaphylactic reaction (presently uncommon since human preparations have replaced the previously used bovine preparations), and risk of transmission of viruses.
-
Endoscopic sclerotherapy: Endoscopic use of sclerosants (ethanolamine oleate or polidocanol) similarly to what is done for esophageal varices is another option. During acute GV bleeding, EVS (endoscopic variceal sclerotherapy) achieves immediate control of bleeding in 60–100 % of cases but is associated with unacceptably high rebleeding rates of up to 90 % [33]. EVS achieves variceal eradication in 40–70 % of all GV patients treated electively [34], but according to Sarin et al. [33] the success rate is dependent upon the location of varices: eradication rates of 95 % can be achieved with GOV1, but the technique is less effective for GOV2 and IGV1. Multiple studies including RCTs showed that EVS is less effective in the treatment of GV than of EV, probably due to the high-volume blood flow through the GV compared with the EV. This may result in rapid flushing away of the sclerosant in the bloodstream, which may require large amounts of sclerosant, leading to a higher rate of side effects, such as retrosternal and abdominal pain, and fever [1]. Rebleeding after elective EVS was <20 % with GOV1 and GOV2 but high in patients with IGV1 (53 %). Most bleeds were due to ulcers at the injection site [1].
To summarize: EVS is effective and appropriate for acute GOV1 bleeding but is less effective for fundal varices (GOV2 or IGV1), as a consequence, the use of cyanoacrylate glue is the first choice if available, and EVS should be considered as an alternative.
-
Variceal band and loop ligation: Endoscopic variceal ligation is the gold standard endoscopic therapy for esophageal varices but is less effective for gastric varices due to: (1) thick mucosa overlying the varices, with difficulty in suction during band ligation; (2) larger size of varices which causes difficulties in sucking the varices in the suction hood of the banding device; (3) development of post-EVL ulcer bleeding which may be fatal because of the underlying hemodynamic alterations; (4) the overall higher rebleeding and recurrence rates of varices (lesser degree of deep fibrosis of the varices) [35].
EVL with nylon or stainless steel snares or standard rubber bands has been used. GV smaller than 2 cm in diameter can be ligated with standard rubber bands, whereas larger diameter GV requires the use of larger detachable snares [36].
Only one RCT by Lo et al. [23] compared the use of EVL using rubber bands against EVO and showed that EVL was less effective than EVO in controlling acute GV bleeding (45 % vs. 87 %) and had a higher rebleeding rate (54 % vs. 31 %). The eradication rates of EVL and EVO were comparable (45 % vs. 51 %).
-
Role of EUS: EUS along with color Doppler has been shown to be more sensitive than conventional endoscopy for detecting gastric varices. Iwase et al. [37] showed that linear Doppler EUS easily detects the persistence of blood flow in gastric varices after cyanoacrylate therapy and suggests a higher risk for recurrent bleeding. An interesting study by Lee et al. [8], in patients with acute GV bleeding compared “on-demand” cyanoacrylate injection for recurrent bleeding (n = 47) with scheduled biweekly EUS-guided glue injection till obliteration of all residual varices (n = 54). The study showed that repeated sessions on a scheduled basis significantly reduced the risk of late rebleeding compared with the on-demand approach (19 % vs. 45 %). In a prospective case series [38] of 5 patients with bleeding gastric varices, EUS-guided injection of cyanoacrylate directed at the perforating veins achieved hemostasis in all patients, with no cases of recurrent bleeding over a 10-month follow-up. Variceal eradication was successful in 2 patients after 1 session and in 3 patients after 2 sessions (mean 1.6).
In another study using a novel approach, transesophageal EUS-guided coil embolization and cyanoacrylate injection [39] of gastric fundal varices reduced the amount of glue and the number of sessions needed for complete EVO, with control of acute bleeding in all cases. Among 24 patients with a mean follow-up of 193 days (range 24–589 days), gastric fundal varices were obliterated after a single treatment session in 23 (96 %) and no rebleeding was attributed to GV. There were no procedure-related complications and no symptoms or signs of CYA glue embolization.
Thus EUS is an important tool and its use is expanding in the management. It easily: (1) localizes GV; (2) differentiates GV from other bleeding mucosal lesions; (3) detects perforating veins; (4) can guide the injection of sclerosants, glue or thrombin, dictating both the amount and the site when adequate visualization by conventional endoscopy is not possible due to active ongoing bleeding; (5) can detect, during follow-up, residual varices, perforating veins, and collaterals to guide further sessions of endoscopic therapy and may decrease the risk of rebleeding.
-
-
Step 3—salvage radiologic therapies: After failure to control bleeding during endoscopy salvage, rescue radiologic interventions are the next option. As per the APASL guideline [10], second look endoscopy should be performed after initial failure to control bleeding or early rebleeding and balloon tamponade should be used as a bridge until definitive therapy is started.
Salvage radiologic approaches include TIPS, BRTO, BO-EIS (balloon-occluded endoscopic injection sclerotherapy), and BATO (balloon-occluded antegrade transvenous obliteration).
-
TIPS: The principle behind the use of TIPS is the reduction of portal pressure by creating a portosystemic bypass. TIPS is indicated in two situations, i.e., (1) in acute variceal bleeding as a rescue therapy and (2) to prevent recurrent bleeding after initial endoscopic therapy. See Fig. 14.2a–g.
Fig. 14.2 
(a–g) A 40-year-old male with alcoholic cirrhosis presented with acute variceal hemorrhage. Urgent endoscopy revealed small esophageal varices with active bleeding from GOV2. Glue was injected and hemostatis was achieved but the patient again rebled within 48 h of admission. Abdominal CT scan revealed large (a, b, c) paraesophageal and gastric varices (arrow in (d)). The patient underwent a TIPS procedure (e). Portal venography post stent placement demonstrated persistent filling of the large gastric varices (arrow in (f)) despite adequate reduction in the portal pressure. These varices were successfully embolized with glue (arrow in (g))
Patients presenting with acute gastric variceal bleeding may have HVPG <12 mmHg (which is defined as the lower limit for variceal bleeding/clinically significant portal hypertension for esophageal varices) in the majority of cases. In patients with pre-TIPS HVPG of <12 mmHg, the decrease in gradient after TIPS does not affect the risk for rebleeding, whereas it has been shown that in patients with pre-TIPS HVPG >12 mmHg the risk for rebleeding is significantly reduced [8]. Sanyal et al. [40] showed that patients undergoing TIPS for gastric variceal bleeding had a spontaneous gastro-renal shunt (GRS) in 67 % of cases (4 of 6 patients) and in half of the patients (6 of 12) the varices failed to resolve. Ryan et al. [35] found that in 2 patients with large GV associated with a spontaneous GRS, having pre-TIPS HVPG < 12 mmHg, the post-TIPS gradient was marginally reduced (only by 1 mmHg) and TIPS had no effect on blood flow through the GV in this group of patients. Thus, the efficacy of TIPS in preventing GV rebleeding in a subgroup of patients with low HPVG and GRS needs further studies [26].
Control of acute GV bleeding with TIPS can be achieved in up to 95 % of patients and is comparable to cyanoacrylate and thrombin [35]. On follow-up the 1-year rebleeding rate is between 10 and 30 %, the incidence of new-onset encephalopathy is 3–18 %, and the overall 1-year survival varies between 58 and 80 %, which mainly depend upon the severity of the underlying liver disease. The technical success rate of TIPS is up to 100 % in most of the series and some studies suggested that covered stents might have a survival advantage and possibly lower encephalopathy over bare stents.
Studies have shown that bare stent dysfunction occurs in 30–80 and 47–90 % of patients by 1 and 2 years post-TIPS, respectively [4]. Doppler ultrasound is 70 % sensitive and 90 % specific in predicting stent dysfunction and surveillance at 6 months intervals with this technique is adequate. Some centers suggested to perform portal angiography for surveillance every 6 months as this technique is highly sensitive and allows concomitant therapeutic intervention if necessary [35].
Thus to summarize TIPS has an important role in the management of bleeding gastric varices as a rescue therapy, but in places where cyanoacrylate is readily available, it should probably be used after failed endoscopic therapy. Appropriate patient selection as well as severity of the underlying liver disease is critical, and cost-effectiveness of the procedure along with availability of TIPS in a resource poor setting should be taken into consideration.
-
Balloon-occluded retrograde transvenous obliteration: BRTO is a vascular interventional technique performed in patients with a GRS, in which a balloon catheter is advanced from a transfemoral (systemic venous) approach and positioned and inflated to occlude the GRS near its base at the left renal vein. After balloon occlusion, sclerosant is injected; stagnation of the sclerosant within the shunt and in the gastric varices leads to the obliteration of the varices. Preprocedural imaging is important to ascertain the presence and diameter of the shunt, so that a balloon whose diameter will match the diameter of the shunt can be selected [41].
BRTO is feasible only in patients with a known GRS (which is present in 85 % of patients with GV). In a study of acute bleeding, hemostasis was achieved by BRTO in 100 % (16/16) of patients and the rebleeding rate was 0 % during almost 2 years of follow-up, with a high eradication rate. The most common complications reported are hemoglobinuria, abdominal pain, transient fever, pleural effusion, transient worsening of liver biochemistry, shock, and atrial fibrillation. Long-term complications are worsening of EV in up to 50 % of patient, the appearance of ectopic intestinal varices or rectal varices and extension of thrombus to the portal vein and renal vein. Chikamori et al. [42] showed that the incidence of worsening of esophageal varices was significantly reduced when BRTO was preceded by partial splenic embolization (PSE) (9 % vs. 45 %), without any differences in gastric variceal disappearance rates or survival. See Fig. 14.3a–d.
Fig. 14.3 
(a–d) A case of gastric variceal bleed had undergone BRTO. The upper panels (a, b) show preprocedure CT with gastric varices and gastro-renal shunt. (c, d) Show BRTO intraprocedure image and 3 month post-BRTO follow-up CT with residual varices and lipiodol
In patients with GV bleeding and uncontrolled ascites and/or hepatic hydrothorax, or high-risk esophageal varices, consideration of TIPS with BRTO is advisable to simultaneously achieve portal decompression [41].
-
Balloon-occluded endoscopic injection sclerotherapy: This is another approach which does not require a GRS. The portal vein is cannulated by a transhepatic route and the GRS (if present) is cannulated via the transfemural route through the left renal vein. Through the portal vein, the smaller veins supplying the varices are occluded with coils and the main supplying vein is also occluded with a balloon. The varices are then injected with sclerosant endoscopically. After treatment, the catheters remain in situ for 24 h to permit maximal sclerosis of the varices. This is a potentially effective means of eradicating GV, it seems similar to BRTO in terms of safety and efficacy, and has some added advantage in that it can be performed in patients without GRS [35].
-
Balloon-occluded antegrade transvenous obliteration: BATO in which a balloon catheter is advanced from a transhepatic (portal venous) approach and positioned and inflated in the left gastric vein (LGV) or coronary vein near its origin at the main portal vein (PV). PTE (percutaneous transhepatic embolization), trans-TIPS BATO are used in the absence of GRS or when technical difficulty arises in approaching the variceal columns [41].
The details of the available studies on BRTO used for GV bleeding are shown in Table 14.4 [42–49].
Table 14.4 The detail of the available studies on BRTO used for GV bleeding In conclusion, BRTO is a very effective form of treatment for gastric varices in patients with large gastrosystemic shunts in whom there is failure to control acute gastric variceal bleed; who are poor candidates for TIPS, such as patients with a thrombosed portal vein, hepatic encephalopathy, or a low HVPG; who have large high risk gastric varices for secondary prophylaxis after initial endoscopic therapy.
-
-
Step 4—surgical therapies: Surgery is currently considered only as salvage therapy when endoscopic, medical, and radiologic therapies fail in patients with Child-Turcotte-Pugh class A cirrhosis or in patients who live at a great distance from centers that can manage variceal bleeding adequately [6]. Surgical therapies for acute GV bleeding are shown in Table 14.5.
Table 14.5 Surgical therapies for acute GV bleeding and on follow-up With rapidly evolving technology, advances in endoscopic approach and use of EUS to assess the vascular anatomy and EUS-guided GVO, and the availability of salvage radiological procedures such BRTO and TIPS, surgery is falling out of favor. Etiology of portal hypertension, severity of liver disease, response to prior treatment, and the possibility of future liver transplantation must be considered while considering surgical management. Hassab’s operation is a useful technique in which devascularization of the upper stomach along with splenectomy is performed and can be effective in acute gastric variceal bleeding with poor liver function [50–53].


Secondary Prophylaxis
Medical Therapies
There is little evidence for the use of drugs for secondary prevention. Few studies have shown the efficacy of drug therapy for the prevention of GV rebleeding after successful endoscopic variceal obturation [54]. In a study by Mishra et al. [26] the GV rebleeding rate in the cyanoacrylate group was significantly lower than in the beta-blocker group (15 % vs. 55 %, p = 0.004) and the mortality rate was lower (3 % vs. 25 %, p = 0.026) during a median follow-up of 26 months. The median baseline and follow-up HVPG in the cyanoacrylate group were 15 (10–23) and 17 (11–24) mmHg (p = 0.001) and for the beta-blocker group 14 (11–24) and 13 (8–25) mmHg (p = 0.003).
Thus, drug therapy with beta-blocker should be continued: (1) if it is well tolerated; (2) in the presence of concomitant esophageal varices or of a documented HVPG greater than 12 mmHg as an adjunct to endoscopic therapy.
Endoscopic Therapies
After the index bleeding, secondary prophylaxis with endoscopic therapy is better than drug therapy and the use of tissue adhesive is the modality of choice. To conclude, repeated tissue adhesive injection until obliteration of GV with or without beta-blocker is the ideal secondary prophylaxis. In resource poor setting, due to unavailability of facilities or lack of expertise for glue injection, GV sclerotherapy or band ligation may be considered, keeping in mind the high risk of rebleeding.
Interventional Radiologic Approach
There are clear recommendations for the routine use of these techniques for secondary prophylaxis of GV bleeding. The options include TIPS, BRTO, and BO-EIS. All these modalities achieve good control of acute bleeding as well as very minimal rebleeding. The preferences for such therapies include (1) TIPS to be considered in cases with HVPG > 12; (2) BRTO for cases with low portal pressure (HVPG < 12 mmHg), presence of PVT, or large GRS; and (3) BO-EIS when it is difficult to perform BRTO [41].
Partial Splenic Embolization
Splenectomy or PSE per se or prior to BRTO has been considered as a modality for GV bleeding, to prevent rapid progression of esophageal varices. The procedure involves super-selective catheterization and embolization of the intrasplenic arterial branches, usually with polyvinyl alcohol particles. PSE leads to reduction of portal venous pressure, reduction in splenic size with improvement of the hypersplenism-induced thrombocytopenia, enhanced hepatic function, and reduced encephalopathy [17]. As far as secondary prophylaxis against GV rebleeding is concerned, patients have been followed in four case series showing an 80 % reduction in bleeding rates with follow-up times ranging from 3 to 50 months. Post-embolization syndrome is almost universal with abdominal pain, fever, nausea, and anorexia.
Overall, the literature is limited in quality, but, given the potential benefits of PSE, further investigation is warranted to allow evidence-based evaluation of its use in the treatment of GV.
An algorithmic approach to gastric variceal bleed is shown in Fig. 14.4.

Algorithm for GV bleed management
Conclusions
Gastric variceal bleeding is associated with high morbidity and mortality rates. Early detection and control of bleeding are important. The patient should be started with vasoactive drugs (door to needle time within 30 min) and early endoscopy after initial hemodynamic stabilization (door to scope time <6 h) is recommended. Endoscopic variceal obturation by glue is the method of choice followed by repeated session every 4 weeks until complete obliteration of varices. Rescue therapies include TIPS or BRTO. Surgery has a limited role for selected subgroups. Secondary prophylaxis with beta-blocker and endoscopic therapy is ideal.
Ectopic Varices
Incidence and Prevalence
EcV are dilated portosystemic collateral veins located in sites other than the gastroesophageal region [4]. They constitute 1–5 % of all variceal bleeds in patients with intrahepatic portal hypertension and 20–30 % of those with extrahepatic portal hypertension [2]. EcV are rare and are a challenge to the clinician because of the difficulty in their management and the high mortality secondary to their initial bleeding (up to 40 %) [26, 40].
Site of Distribution
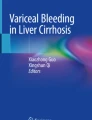
EcV are defined on the basis of their location (Table 14.6). They can occur in the stomach (isolated gastric varices—IGV2 of Sarin’s classification), the duodenum, jejunum, ileum, colon, rectum, at peristomal sites, in the biliary tree, peritoneum, umbilicus, falciform ligament, bare area of the liver, splenic ligament, urinary bladder, right diaphragm, ovary, vagina, and testis. The distribution of varices is difficult to quantify due to difficulty in their diagnosis and unusual location. Data regarding the incidence and/or severity of bleeding in each site are not currently available and only center-based case series were available. The duodenum is the most common site (17–40 %) [55–57]; other relatively common locations are the small intestine (4–18 %) [58–60], the colon (3.5–14 %) [57–61], the rectum (8–40 %) [62], the peritoneum (9 %) [57], and peristomal areas (5.8 %) [58]. The other rare sites are vagina, ovary, and gall bladder. Familial cases of EcV have also been reported [63]. See Fig. 14.5.

Top row: Duodenal ectopic varices in a patient of EHPVO with portal biliopathy. The sent in CBD is visible. Middle row: Jejunal duplication cyst with jejuna ectopic varices at the ostia presenting with recurrent bleed, underwent balloon enteroscopy and sclerotherapy. Bottom row: A cirrhotic with recurrent lower GI bleed from rectal varices, underwent glue injection for the same
Classification
A classification was proposed by us depending upon the location of varices and is shown in Table 14.6.
Management
Clinical Presentation
The majority of EcV are detected during routine endoscopy or colonoscopy or during angiography performed for some other reason in asymptomatic patients. The clinical presentation of EcV is variable and reported in Table 14.7 [4].
When to Suspect Ectopic Variceal Bleed?
Presentation with hematemesis or hematochezia is the most common. EcV bleeding should also be suspected when a patient with portal hypertension shows a sudden fall in Hb >2 g, tachycardia, sweating or hemodynamic instability, abdominal pain, increase in abdominal girth, rising lactate, and no obvious source of bleeding is identified [2, 4]. Small intestinal ectopic variceal bleed should be suspected when patients present with a triad of portal hypertension, hematochezia without hematemesis, and previous history of abdominal surgery [64].
Diagnosis of Ectopic Varices
The diagnosis depends upon the location of ectopic varices. Luminal EcV are often diagnosed by endoscopy.
Endoscopy remains the best method of diagnosing IGV2, duodenal varices as well as rectal varices. Lower GI bleeding should be attributed to rectal varices based on three criteria: rectal varices and the presence of fresh blood in the rectum, sigmoid colon free of fresh blood, and the absence of hemorrhoids or colopathy. At ileocolonoscopy, 18 % of patients with liver cirrhosis and/or portal hypertension have ileal varices [61]. Double Balloon Enteroscopy (DBE) can visualize the whole small bowel and perform necessary endoscopic interventions [64, 65], thus DBE has both diagnostic and therapeutic potential.
In one study [65], video capsule endoscopy (VCE) demonstrated small intestinal varices in 8.1 % of patients with portal hypertension. VCE has no procedure-related side effects and is noninvasive, it can detect small varices that are not seen at endoscopy, and the overall concordance between endoscopy and VCE was 96.9 and 90.6 % for the diagnosis of varices and gastropathy, respectively [66]. However, DBE was considered better than capsule endoscopy due to added therapeutic capability.
EUS has been found to be superior to endoscopy to diagnose rectal varices [37]. EUS can be used to better localize and differentiate EcV from other bleeding mucosal lesions [67, 68].
Computed tomography (CT) and angiography can detect bleeding duodenal varices if they are massive [69]. Angiographic evaluation of EcV can be performed either by direct visualization of the venous system through transhepatic portography or by indirect visualization of the venous phase after splenic and/or mesenteric arteriography. It provides information about splenic vein patency. Transhepatic portal venography has been used to confirm EcV by finding abnormal splanchnic vessels feeding from either the superior or the inferior mesenteric vein [70].
Percutaneous Doppler ultrasound can detect peristomal collaterals and may be used to guide variceal sclerotherapy. Choi et al. [71] have described the use of multislice helical CT to detect stomal varices.
Other modalities include Technetium-99 m red blood cell scintigraphy, CT angiography, CT enteroclysis, and laparotomy [2].
The algorithmic approach to diagnose EcV is shown in Fig. 14.6.

Algorithm for ectopic variceal bleed management
Stepwise Approach in Management of Ectopic Variceal Bleeding
As there is no established guideline, and the management is center-specific, based on experience and expert opinion and mostly extrapolated from the existing guidelines for acute variceal bleeding management. Here we suggest a stepwise approach to such cases as outlined next.
-
Step 1—initial management: The initial step for management includes general supportive measures, i.e., appropriate resuscitation with crystalloid or other blood products, according to the APASL guidelines, the goals are to maintain systolic blood pressure at least at 90–100 mmHg, and the heart rate below 100 beats/min, with a hemoglobin level around 7–8 g/dL (hematocrit of 21–24). Prophylactic antibiotics should be given.
Pharmacotherapy with vasoactive drugs should be initiated as soon as the diagnosis of EcV bleed is made or suspected. Somatostatin or its analogue octreotide may be beneficial and should be continued for 3–5 days after confirmation of the diagnosis [72]. Octreotide has been shown to be effective in the control of bleeding colonic varices [73]. Terlipressin use should be considered but no definite recommendation for the dose or frequency of administration is available at present.
-
Step 2—endoscopic interventions: Once the patient is hemodynamically stable, emergency upper GI endoscopy should be performed. The door to scope time should be less than 6 h [10]. If endoscopy fails to show the source of GI bleeding, colonoscopy after a rapid preparation with polyethylene glycol solution delivered via a nasogastric tube should be the second step of investigation. In areas beyond the reach of conventional endoscopic procedures, enteroscopy can be performed electively [10].
The endoscopic stigmata for bleeding EcV include—finding a spurting vessel, signs of recent bleed such as a “white nipple” or an adherent clot (Level of evidence 3b, Grade C) [10] and endoscopic management with band ligation [74, 75] or endoscopic sclerotherapy [76, 77] or glue injection should be done as discussed in detail next. The various endoscopic approaches include:
-
Injection sclerotherapy: The endoscopic injection of ethanolamine oleate, bucrylate [78–80], and thrombin [81, 82] is being used with variable success rate for bleeding varices in the duodenum [77, 83] and small bowel and also for controlling the bleeding from peristomal varices with no injury to the stoma from the sclerosant [83]. Cyanoacrylate and thrombin are promising in the management of gastric and EcV with high hemostasis and low rebleeding rates [84]. The risks associated with cyanoacrylate include endoscope damage, and thromboembolic complications [84] but the use of thrombin as an alternative is technically easy to administer without major complications [32]. However, there have been no randomized trials to directly compare the efficacy of thrombin vs. cyanoacrylate.
-
Band ligation: Although EVL is the treatment of choice for esophageal varices, this treatment [67, 75, 85, 86] is successful in halting bleeding but of limited use when the EcV are larger than 15 mm. EVL does not obliterate the feeding vessel. Because of the occurrence of post-banding deep ulcers and consequent risk of bleed, of the difficulty in band deployment in the acute setting because of limited visibility from the banding hood, and since there are case reports of accidental banding of the major papilla leading to biliary obstruction [87], the use of EVL in ectopic variceal bleed is not indicated.
-
Clipping: Clipping can be easily applied but has the potential of further increasing bleeding with drawbacks similar to those of banding [88]. The success rate of this technique has not been evaluated in controlled trials and its use is dependent on individual expertise, location of the EcV, and technical feasibility.
-
EUS: EUS is an important tool for diagnosis, differentiation and guiding the therapy both in the acute setting and on follow-up. It easily localizes and differentiates EcV from other bleeding mucosal lesions [68, 89]. In patients with rectal varices, EUS is more sensitive than routine endoscopy—the EcV are seen as round or ovoid, tortuous, anechoic structures with an increase in the size of submucosal and perirectal vessels without associated wall thickening or without necessarily detecting the presence of perforating veins [90–92]. EUS can guide the injection of sclerosants, glue or thrombin, and help deciding both the amount and the site for injection, or the deployment of coils when adequate visualization is not possible due to active ongoing bleed [93, 94]. EUS is also useful in the follow-up of the varices after endoscopic therapy, as it can detect residual varices, perforating veins, and collaterals; EUS can also guide further session of endoscopic therapy and may decrease the risk of bleeding [8].
-
-
Step 3—interventional radiology techniques (rescue therapies): TIPS is an attractive option based on the principle of decreasing portal pressure as the underlying cause of bleeding EcV is increased portal pressure [95–98]. In a case series, TIPS led to a decreased need for repeated procedures in patients with EcV, including peristomal varices, with rebleeding rates in this group averaging 23 and 31 % at 1 and 2 years, respectively [98]. In a series of 28 patients by Kochar et al. [99], TIPS achieved 100 % initial hemostasis in all patients with ectopic variceal bleed. The rate of rebleeding was 21 % (5 out of 28). Of these, two were due to shunt dysfunction. TIPS with concomitant variceal embolization is preferred to reduce rebleeding. TIPS use should be considered taking into account the risk of hepatic decompensation and encephalopathy [100] and may not be suitable for EcV caused by focal venous obstruction.
BRTO is another option. In a case series by Watanabe et al. [58] BRTO was shown to be successful in occlusion of the feeding vessels in EcV.
PTO is another rarely performed procedure in which coil embolization of the veins draining into the EcV is performed by transhepatic route. Use of PTO for duodenal varices [101], rectal varices [102], jejunal varices (using transhepatic portovenous angioplasty and stenting) [103], and for the treatment of peristomal varices has been reported.
-
Step 4—surgical interventions: If endoscopic techniques and interventional radiologic procedures fail to control bleeding or are not feasible, surgery is the next step for management. It is preferred in patients with Child-Pugh A cirrhosis and in patients with an EHPVO.
The various options include surgical resection or ligation of ectopic bleeding varices [104, 105], splenectomy for EcV secondary to splenic vein thrombosis from chronic pancreatitis [106, 107]. Minor interventions include simple oversewing of duodenal varices through a duodenotomy [108] duodenal dearterialization and stapling, circumferential-stapled anoplasty [109].
In patients with peristomal varices, local measures such as the initial application of manual pressure and positioning the patient in a recumbent position are usually effective. Ligation or cautery is also effective if bleeding vessels are visible [84]. An attempt for surgical revision or relocation of the stoma is usually ineffective and recurrence of bleeding is common. Portosystemic shunt surgery is highly successful in control of bleeding [110, 111] and has the lowest incidence of rebleeding and need for additional procedures compared with other interventions [112], but at the same time the increased operative risk from the underlying liver disease and a potential for hepatic decompensation are matters of concern.
In rectal varices, surgical staples have been used successfully [113, 114]. Depending on the cause and degree of liver dysfunction, liver transplantation may be the last resort for correcting the underlying PHT with restoration of normal liver function.
Rupture of an intraperitoneal varix is a rare entity and a high index of suspicion is required for diagnosing it as described in Fig. 14.1. Surgical exploration attempting to locate and ligate the bleeding varix may represent the only option [115].
The stepwise approach adopted from Sarin and Kumar et al. is shown in Figs. 14.7a–f and 14.8a–f.
Fig. 14.7 
(a–f) Portosystemic collaterals. (a) Paraesophageal. (b) Omental. (c) Retroperitoneal. (d) Umbilical. (e) Paraduodenal. (f) Lienorenal
Fig. 14.8 
(a–f) Portosystemic collaterals. (a) Intrahepatic collaterals and recanalized paraumbilical vein. (b) Pericholecystic. (c) Perirenal. (d) Pericolonic. (e) Perirectal. (f) Perivesical and perirectal with patent inferior mesenteric vein


Prophylaxis
The available literature does not suggest either primary or secondary prophylaxis for the ectopic varices.
Conclusions
Bleeding from EcV is rare and often difficult to diagnose, and hence requires a high index of suspicion and is associated with high mortality (i.e., up to 40 %). Management requires multimodal imaging or repeated endoscopies. The management of acute ectopic variceal bleed requires a multidisciplinary approach that includes pharmacological, endoscopic, and angiographic methods with surgery for highly selected cases. To determine the best treatment modalities and their outcomes, large randomized controlled trials are required.
References
Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology. 1992;16:1343–9.
Sarin SK, Chandan KN. Ectopic varices. Clin Liver Dis. 2012;1(5):167–72.
Mishra SR, Sharma BC, Kumar A, Sarin SK. Primary prophylaxis of gastric variceal 1 bleeding comparing cyanoacrylate injection and beta-blockers: a randomized controlled trial. J Hepatol. 2011;54:1161–7.
Helmy A, Al Kahtani K, Al Fadda M. Updates in the pathogenesis, diagnosis and management of ectopic varices. Hepatol Int. 2008;2:322–34.
Tan PC, Hou MC, Lin HC, Liu TT, Lee FY, Chang FY, et al. A randomized trial of endoscopic treatment of acute gastric variceal hemorrhage: N-butyl-2-cyanoacrylate injection versus band ligation. Hepatology. 2006;43:690–7.
Bendtsen F, Krag A, Mølle S. Treatment of acute variceal bleeding. Dig Liver Dis. 2008;40:328–36.
Hsu YC, Chung CS, Wang HP. Application of endoscopy in improving survival of cirrhotic patients with acute variceal hemorrhage. Int J Hepatol. 2011:1–8.
Lee YT, Chan FKL, Ng EK, Leung VK, Law KB, Yung MY, et al. EUS-guided injection of cyanoacrylate for bleeding gastric varices. Gastrointest Endosc. 2000;52:168–74.
Hashizume M, Akahoshi T, Tomikawa M. Management of gastric varices. J Gastroenterol Hepatol. 2011;26 Suppl 1:102–8.
Sarin SK, Kumar A, Angus PW, Baijal SS, Baik SK, Bayraktar Y et al., For Asian Pacific Association for the Study of the Liver (APASL) Working Party on Portal Hypertension. Diagnosis and management of acute variceal bleeding: Asian Pacific Association for Study of the Liver recommendations. Hepatol Int. 2011;5:607–24.
de Franchis R, Baveno V. Faculty. Revising consensus in portal hypertension. Report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol. 2010;53:762–76.
Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W, Practice Guidelines Committee of the American Association for the Study of Liver Diseases; Practice Parameters Committee of the American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46:922–38.
Matsumoto A, Matsumoto H, Hamamoto N, Kayazawa M. Management of gastric fundal varices associated with a gastrorenal shunt. Gut. 2001;48:440–1.
Watanabe K, Kimura K, Matsutani S, Ohto M, Okuda K. Portal hemodynamics in patients with gastric varices. A study in 230 patients with esophageal and/or gastric varices using portal vein catheterization. Gastroenterology. 1988;95:434–40.
Polio J, Groszmann RJ. Hemodynamic factors involved in the development and rupture of esophageal varices: a pathophysiologic approach to treatment. Semin Liver Dis. 1986;6:318–31.
Kim T, Shijo H, Kokawa H, Tokumitsu H, Kubara K, Ota K, et al. Risk factors for hemorrhage from gastric fundal varices. Hepatology. 1997;25:307–12.
Irani S, Kowdley K, Kozarek R. Gastric varices—an updated review of management. J Clin Gastroenterol. 2011;45:133–48.
Bernard B, Grangé JD, Khac EN, Amiot X, Opolon P, Poynard T. Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: a meta-analysis. Hepatology. 1999;29:1655–61.
Hou MC, Lin HC, Liu TT, Kuo BI, Lee FY, Chang FY, et al. Antibiotic prophylaxis after endoscopic therapy prevents rebleeding in acute variceal hemorrhage: a randomized trial. Hepatology. 2004;39:746–53.
D’Amico G, Pagliaro L, Bosch J. Pharmacological treatment of portal hypertension: an evidence-based approach. Semin Liver Dis. 1999;19:475–505.
Ioannou GN, Doust J, Rockey DC. Systematic review: terlipressin in acute esophageal variceal hemorrhage. Aliment Pharmacol Ther. 2003;17:53–64.
Sarin SK, Primignani M, Agarwal SR. Gastric varices. In: de Franchis R, editor. Portal hypertension. Proceedings of the third Baveno international consensus workshop on definitions, methodology and therapeutic strategies. London: Blackwell Science; 2001. p. 76–96.
Lo GH, Lai KH, Cheng JS, Chen MH, Chiang HT. A prospective, randomized trial of butyl cyanoacrylate injection versus band ligation in the management of bleeding gastric varices. Hepatology. 2001;33:1060–4.
Sarin SK, Jain AK, Jain M, Gupta R. A randomized controlled trial of cyanoacrylate versus alcohol injection in patients with isolated fundic varices. Am J Gastroenterol. 2002;97:1010–5.
Lo GH, Liang HL, Chen WC, Chen MH, Lai KH, Hsu PI, et al. A prospective, randomized controlled trial of transjugular intrahepatic portosystemic shunt versus cyanoacrylate injection in the prevention of gastric variceal rebleeding. Endoscopy. 2007;39:679–85.
Mishra SR, Chander Sharma B, Kumar A, Sarin SK. Endoscopic cyanoacrylate injection versus beta-blocker for secondary prophylaxis of gastric 20 variceal bleed: a randomised controlled trial. Gut. 2010;59:729–35.
Williams SG, Peters RA, Westaby D. Thrombin—an effective treatment for gastric variceal haemorrhage. Gut. 1994;35:1287–9.
Przemioslo RT, McNair A, Williams R. Thrombin is effective in arresting bleeding from gastric variceal hemorrhage. Dig Dis Sci. 1999;44:778–81.
Yang WL, Tripathi D, Therapondos G, Todd A, Hayes PC. Endoscopic use of human thrombin in bleeding gastric varices. Am J Gastroenterol. 2002;97:1381–5.
Heneghan MA, Byrne A, Harrison PM. An open pilot study of the effects of a human fibrin glue for endoscopic treatment of patients with acute bleeding from gastric varices. Gastrointest Endosc. 2002;56:422–6.
Datta D, Vlavianos P, Alisa A, Westaby D. Use of fibrin glue (beriplast) in the management of bleeding gastric varices. Endoscopy. 2003;35:675–8.
Ramesh J, Limdi JK, Sharma V, Makin AJ. The use of thrombin injections in the management of bleeding gastric varices: a single-center experience. Gastrointest Endosc. 2008;68:877–82.
Sarin SK, Lahoti D. Management of gastric varices. Baillieres Clin Gastroenterol. 1992;6:527–48.
Trudeau W, Prindiville T. Endoscopic injection sclerosis in bleeding gastric varices. Gastrointest Endosc. 1986;32:264–8.
Ryan BM, Stockbrugger RW, Ryan MJ. A pathophysiologic, gastroenterologic, and radiologic approach to the management of gastric varices. Gastroenterology. 2004;126:1175–89.
Lee MS, Cho JY, Cheon YK, Ryu CB, Moon JH, Cho YD, et al. Use of detachable snares and elastic bands for endoscopic control of bleeding from large gastric varices. Gastrointest Endosc. 2002;56:83–8.
Iwase H, Suga S, Morise K, Kuroiwa A, Yamagouchi T, Horiuchi Y. Color Doppler endoscopic ultrasonography for the evaluation of gastric varices and endoscopic obliteration with cyanoacrylate glue. Gastrointest Endosc. 1995;41:150–4.
Romero-Castro R, Pellicer-Bautista FJ, Jimenez-Saenz M, Marcos-Sanchez F, Caunedo-Alvarez A, Ortiz-Moyano C, et al. EUS-guided injection of cyanoacrylate in perforating feeding veins in gastric varices: results in 5 cases. Gastrointest Endosc. 2007;66:402–7.
Binmoeller KF, Weilert F, Shah JN, Kim J. EUS-guided transesophageal treatment of gastric fundal varices with combined coiling and cyanoacrylate glue injection. Gastrointest Endosc. 2011;74:1019–25.
Sanyal AJ, Freedman AM, Luketic VA, Purdum III PP, Shiffman ML, DeMeo J, et al. The natural history of portal hypertension after transjugular intrahepatic portosystemic shunts. Gastroenterology. 1997;112:889–98.
Saad WEA, Sze YD. Variations of balloon-occluded retrograde transvenous obliteration (BRTO): balloon occluded antegrade transvenous obliteration (BATO) and alternative/adjunctive routes for BRTO. Semin Intervent Radiol. 2011;28:314–24.
Chikamori F, Kuniyoshi N, Kawashima T, Takase Y. Gastric varices with gastrorenal shunt: combined therapy using transjugular retrograde obliteration and partial splenic embolization. AJR Am J Roentgenol. 2008;191:555–9.
Kanagawa H, Mima S, Kouyama H, Gotoh K, Uchida T, Okuda K. Treatment of gastric fundal varices by balloon-occluded retrograde transvenous obliteration. J Gastroenterol Hepatol. 1996;11:51–8.
Kitamoto M, Imamura M, Kamada K, Aikata H, Kawakami Y, Matsumoto A, et al. Balloonoccluded retrograde transvenous obliteration of gastric fundal varices with hemorrhage. AJR Am J Roentgenol. 2002;178:1167–74.
Fukuda T, Hirota S, Sugimura K. Long-term results of balloon-occluded retrograde transvenous obliteration for the treatment of gastric varices and hepatic encephalopathy. J Vasc Interv Radiol. 2001;12:327–36.
Ninoi T, Nishida N, Kaminou T, Sakai Y, Kitayama T, Hamuro M, et al. Balloon-occluded retrograde transvenous obliteration of gastric varices with gastrorenal shunt: long-term follow-up in 78 patients. AJR Am J Roentgenol. 2005;184:1340–6.
Cho SK, Shin SW, Lee IH, Do YS, Choo SW, Park KB, et al. Balloon-occluded retrograde transvenous obliteration of gastric varices: outcomes and complications in 49 patients. AJR Am J Roentgenol. 2007;189:W365–72.
Hong CH, Kim HJ, Park JH, Park DI, Cho YK, Sohn CI, et al. Treatment of patients with gastric variceal hemorrhage: endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occluded retrograde transvenous obliteration. J Gastroenterol Hepatol. 2009;24:372–8.
Akahoshi T, Hashizume M, Tomikawa M, Kawanaka H, Yamaguchi S, Konishi K, et al. Long-term results of balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding and risky gastric varices: a 10-year experience. J Gastroenterol Hepatol. 2008;23:1702–9.
Hashizume M, Tanoue K, Morita M, Ohta M, Tomikawa M, Sugimachi K. Laparoscopic gastric devascularization and splenectomy for sclerotherapy-resistant esophagogastric varices with hypersplenism. J Am Coll Surg. 1998;187:263–70.
Mitsis M, Katsanos KH, Fatouros M, Tsianos EV. Hassabs operation for bleeding gastric varices. Ann Gastroenterol. 2012;25(2):182.
Tomikawa M, Hashizume M, Saku M, Tanoue K, Ohta M, Sugimachi K. Effectiveness of gastric devascularization and splenectomy for patients with gastric varices. J Am Coll Surg. 2000;191:498–503.
Sugo H, Fujiwara N, Yoshimoto J, Miwa K, Ishizaki Y. Additional Hassab’s operation for esophagogastric varices in cirrhotic patients with resectable hepatocellular carcinoma. Hepatogastroenterology. 2008;55:1686–90.
Tripathi D, Ferguson JW, Therapondos G, Plevris JN, Hayes PC. Review article: recent advances in the management of bleeding gastric varices. Aliment Pharmacol Ther. 2006;24:1–17.
Khouqeer F, Morrow C, Jordan P. Duodenal varices as a cause of massive upper gastrointestinal bleeding. Surgery. 1987;102:548–52.
Batoon SB, Zoneraich S. Misdiagnosed anorectal varices resulting in a fatal event. Am J Gastroenterol. 1999;94:3076–7.
Norton ID, Andrews JC, Kamath PS. Management of ectopic varices. Hepatology. 1998;28:1154–8.
Watanabe N, Toyonaga A, Kojima S, Takashimizu S, Oho K, Kokubu S, et al. Current status of ectopic varices in Japan: results of a survey by the Japan Society for Portal Hypertension. Hepatol Res. 2010;40:763–76.
Misra SP, Dwivedi M, Misra V, Gupta M. Ileal varices and portal hypertensive ileopathy in patients with cirrhosis and portal hypertension. Gastrointest Endosc. 2004;60:778–83.
Naveau S, Poynard T, Pauphilet C, Aubert A, Chaput JC. Rectal and colonic varices in cirrhosis. Lancet. 1989;1:624.
Misra SP, Dwivedi M, Misra V, Dharmani S, Kunwar BK, Arora JS. Colonic changes in patients with cirrhosis and in patients with extrahepatic portal vein obstruction. Endoscopy. 2005;37:454–9.
McCormack TT, Bailey HR, Simms JM, Johnson AG. Rectal varices are not piles. Br J Surg. 1984;71:163.
Atin V, Sabas JA, Cotano JR, Madariaga M, Galan D. Familial varices of the colon and small bowel. Int J Colorectal Dis. 1993;8:4–8.
Almadi MA, Almessabi A, Wong P, Ghali PM, Barkun A. Ectopic varices. Gastrointest Endosc. 2011;74:384–8.
Heine GD, Hadithi M, Groenen MJ, Kuipers EJ, Jacobs MA, Mulder CJ. Double-balloon enteroscopy: indications, diagnostic yield, and complications in a series of 275 patients with suspected small-bowel disease. Endoscopy. 2006;38:42–8.
Hekmat H, Al-toma A, Mallant MP, Mulder CJ, Jacobs MA. Endoscopic N-butyl-2-cyanoacrylate (Histoacryl) obliteration of jejunal varices by using the double balloon enteroscope. Gastrointest Endosc. 2007;65(2):350–2.
Akazawa Y, Murata I, Yamao T, Yamakawa M, Kawano Y, Nomura N, et al. Successful management of bleeding duodenal varices by endoscopic variceal ligation and balloon-occluded retrograde transvenous obliteration. Gastrointest Endosc. 2003;58:794–7.
Bhutani MS, Nadella P. Utility of an upper echoendoscope for endoscopic ultrasonography of malignant and benign conditions of the sigmoid/left colon and the rectum. Am J Gastroenterol. 2001;96:3318–22.
Spence RA. The venous anatomy of the lower oesophagus in normal subjects and in patients with varices: an image analysis study. Br J Surg. 1984;71:739–44.
Vangeli M, Patch D, Terreni N, Tibbals J, Watkinson A, Davies N, et al. Bleeding ectopic varices—treatment with transjugular intrahepatic porto-systemic shunt (TIPS) and embolisation. J Hepatol. 2004;41:560–6.
Choi JW, Lee CH, Kim KA, Park CM, Kim JY. Ectopic varices in colonic stoma: MDCT findings. Korean J Radiol. 2006;7:297–9.
Garcia-Tsao G, Sanyal AJ, Grace ND, Carey WD, et al. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Am J Gastroenterol. 2007;102:2086–102.
Chakravarty BJ, Riley JW. Control of colonic variceal haemorrhage with a somatostatin analogue. J Gastroenterol Hepatol. 1996;11:305–6.
Firoozi B, Gamagaris Z, Weinshel EH, Bini EJ. Endoscopic band ligation of bleeding rectal varices. Dig Dis Sci. 2002;47:1502–5.
Bosch A, Marsano L, Varilek GW. Successful obliteration of duodenal varices after endoscopic ligation. Dig Dis Sci. 2003;48:1809–12.
Wang M, Desigan G, Dunn D. Endoscopic sclerotherapy for bleeding rectal varices: a case report. Am J Gastroenterol. 1985;80:779–80.
Barbish AW, Ehrinpreis MN. Successful endoscopic injection sclerotherapy of a bleeding duodenal varix. Am J Gastroenterol. 1993;88:90–2.
Benedetti G, Sablich R, Lacchin T, Masiero A. Endoscopic treatment of bleeding duodenal varices by bucrylate injection. Endoscopy. 1993;25:432–3.
Chen WC, Hou MC, Lin HC, Chang FY, Lee SD. An endoscopic injection with N-butyl-2-cyanoacrylate used for colonic variceal bleeding: a case report and review of the literature. Am J Gastroenterol. 2000;95:540–2.
D’Imperio N, Piemontese A, Baroncini D, Billi P, Borioni D, Dal Monte PP, et al. Evaluation of undiluted N-butyl-2-cyanoacrylate in the endoscopic treatment of upper gastrointestinal tract varices. Endoscopy. 1996;28:239–43.
Rai R, Panzer SW, Miskovsky E, Thuluvath PJ. Thrombin injection for bleeding duodenal varices. Am J Gastroenterol. 1994;89:1871–3.
Sans M, Llach J, Bordas JM, Andreu V, Reverter JC, Bosch J, et al. Thrombin and ethanolamine injection therapy in arresting uncontrolled bleeding from duodenal varices. Endoscopy. 1996;28:403.
Liu Y, Yang J, Wang J, Chai G, Sun G, Wang Z, et al. Clinical characteristics and endoscopic treatment with cyanoacrylate injection in patients with duodenal varices. Scand J Gastroenterol. 2009;44:1012–6.
Spier BJ, Fayyad AA, Lucey MR, Johnson EA, Wojtowycz M, Rikkers L, et al. Bleeding stomal varices: case series and systematic review of the literature. Clin Gastroenterol Hepatol. 2008;6:346–52.
Farid M, El Hoda MA. Anorectal varices endoscopic dilemma. Joint Euro-Asian Congr Endosc Surg. 1997:445–877.
Coelho-Prabhu N, Baron TH, Kamath PS. Endoscopic band ligation of rectal varices: a case series. Endoscopy. 2010;42:173–6.
Silberzweig JE, Atillasoy EO, Sheiner PA, Mitty HA. Biliary obstruction caused by endoscopic band ligation of a duodenal varix. Am J Gastroenterol. 1997;92:1060–2.
Machida T, Sato K, Kojima A, Takezawa J, Sohara N, Kakizaki S, et al. Ruptured duodenal varices after endoscopic ligation of esophageal varices: an autopsy case. Gastrointest Endosc. 2006;63:352–4.
Iwase H, Kyogane K, Suga S, Morise K. Endoscopic ultrasonography with color Doppler function in the diagnosis of rectal variceal bleeding. J Clin Gastroenterol. 1994;19:227–30.
Dhiman RK, Choudhuri G, Saraswat VA, Mukhopadhyay DK, Khan EM, Pandey R, et al. Endoscopic ultrasonographic evaluation of the rectum in cirrhotic portal-hypertension. Gastrointest Endosc. 1993;39:635–40.
Dhiman RK, Choudhuri G, Saraswat VA, Mukhopadhyay DK, Khan EM, Pandey R, et al. Endosonographic, endoscopic, and histologic evaluation of alterations in the rectal venous system in patients with portal hypertension. Gastrointest Endosc. 1999;49:218–27.
Wiechowska-Kozlowska A, Bialek A, Milkiewicz P. Prevalence of ‘deep’ rectal varices in patients with cirrhosis: an EUS-based study. Liver Int. 2009;29:1202–5.
Sharma M, Somasundaram A. Massive lower GI bleed from an endoscopically inevident rectal varices: diagnosis and management by EUS (with videos). Gastrointest Endosc. 2010;72:1106–8.
Levy MJ, Wong Kee Song LM, Kendrick ML, Misra S, Gostout CJ. EUS-guided coil embolization for refractory ectopic variceal bleeding (with videos). Gastrointest Endosc. 2008;67:572–4.
Chevallier P, Motamedi JP, Demuth N, Caroli-Bosc FX, Oddo F, Padovani B. Ascending colonic variceal bleeding: utility of phase-contrast MR portography in diagnosis and follow-up after treatment with TIPS and variceal embolization. Eur Radiol. 2000;10:1280–3.
Cohen GS, Ball DS, Flynn DE. Transjugular transhepatic placement of a superior mesenteric vein stent for small bowel varices. J Vasc Interv Radiol. 1995;6:707–10.
Haskal ZJ, Scott M, Rubin RA, Cope C. Intestinal varices: treatment with the transjugular intrahepatic portosystemic shunt. Radiology. 1994;191:183–7.
Vidal V, Joly L, Perreault P, Bouchard L, Lafortune M, Pomier-Layrargues G. Usefulness of transjugular intrahepatic portosystemic shunt in the management of bleeding ectopic varices in cirrhotic patients. Cardiovasc Intervent Radiol. 2006;29:216–9.
Kochar N, Tripathi D, McAvoy NC, Ireland H, Redhead DN, Hayes PC. Bleeding ectopic varices in cirrhosis: the role of transjugular intrahepatic portosystemic stent shunts. Aliment Pharmacol Ther. 2008;28(3):294–303.
Shibata D, Brophy DP, Gordon FD, Anastopoulos HT, Sentovich SM, Bleday R. Transjugular intrahepatic portosystemic shunt for treatment of bleeding ectopic varices with portal hypertension. Dis Colon Rectum. 1999;42:1581–5.
Menu Y, Gayet B, Nahum H. Bleeding duodenal varices: diagnosis and treatment by percutaneous portography and transcatheter embolisation. Gastrointest Radiol. 1987;12:111–3.
Okazaki H, Higuchi K, Shiba M, Nakamura S, Wada T, Yamamori K, et al. Successful treatment of giant rectal varices by modified percutaneous transhepatic obliteration with sclerosant: report of a case. World J Gastroenterol. 2006;12:5408–11.
Sakai M, Nakao A, Kaneko T, Takeda S, Inoue S, Yagi Y, et al. Transhepatic portal venous angioplasty with stenting for bleeding jejunal varices. Hepatogastroenterology. 2005;52:749–52.
Bhagwat SS, Borwankar SS, Ramadwar RH, Naik AS, Gajaree GI. Isolated jejunal varices. J Postgrad Med. 1995;41:43–4.
Bruet A, Fingerhut A, Lopez Y, Bergue A, Taugourdeau P, Mathe C, et al. Ileal varices revealed by recurrent hematuria in a patient with portal hypertension and Mekong Schistosomiasis. Am J Gastroenterol. 1983;78:346–50.
Bradley III EL. The natural history of splenic vein thrombosis due to chronic pancreatitis: indications for surgery. Int J Pancreatol. 1987;2:87–92.
Cottam DR, Clark R, Hayn E, Shaftan G. Duodenal varices: a novel treatment and literature review. Am Surg. 2002;68:407–9.
McAlister VC, Al-Saleh NA. Duodenal dearterialization and stapling for severe hemorrhage from duodenal varices with portal vein thrombosis. Am J Surg. 2005;189:49–52.
Botterill ID, Jayne DG, Snelling AP, Ambrose NS. Correction of symptomatic ano-rectal varices with circumferential stapled anoplasty. Colorectal Dis. 2002;4:217.
Adson MA, Fulton RE. The ileal stoma and protal hypertension: an uncommon site of variceal bleeding. Arch Surg. 1977;112:501–4.
Cameron AD, Fone DJ. Portal hypertension and bleeding ileal varices after colectomy and ileostomy for chronic ulcerative colitis. Gut. 1970;11:755–9.
Conte JV, Arcomano TA, Naficy MA, Holt RW. Treatment of bleeding stomal varices. Report of a case and review of the literature. Dis Colon Rectum. 1990;33:308–14.
Biswas S, George ML, Leather AJ. Stapled anopexy in the treatment of anal varices: report of a case. Dis Colon Rectum. 2003;46:1284–5.
Kaul AK, Skaife PG. Circumferential stapled procedure for bleeding anorectal varices is an effective treatment–experience in nine patients. Colorectal Dis. 2009;11:420–3.
Aslam N, Waters B, Riely CA. Intraperitoneal rupture of ectopic varices: two case reports and a review of literature. Am J Med Sci. 2008;335:160–2.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Chaudhary, A., Sarin, S.K. (2014). How to Manage Gastric and Ectopic Varices?. In: de Franchis, R., Dell’Era, A. (eds) Variceal Hemorrhage. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0002-2_14
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0002-2_14
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-0001-5
Online ISBN: 978-1-4939-0002-2
eBook Packages: MedicineMedicine (R0)